
Enhanced Corrosion Resistance and Local Therapy from Nano-Engineered Titanium Dental Implants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
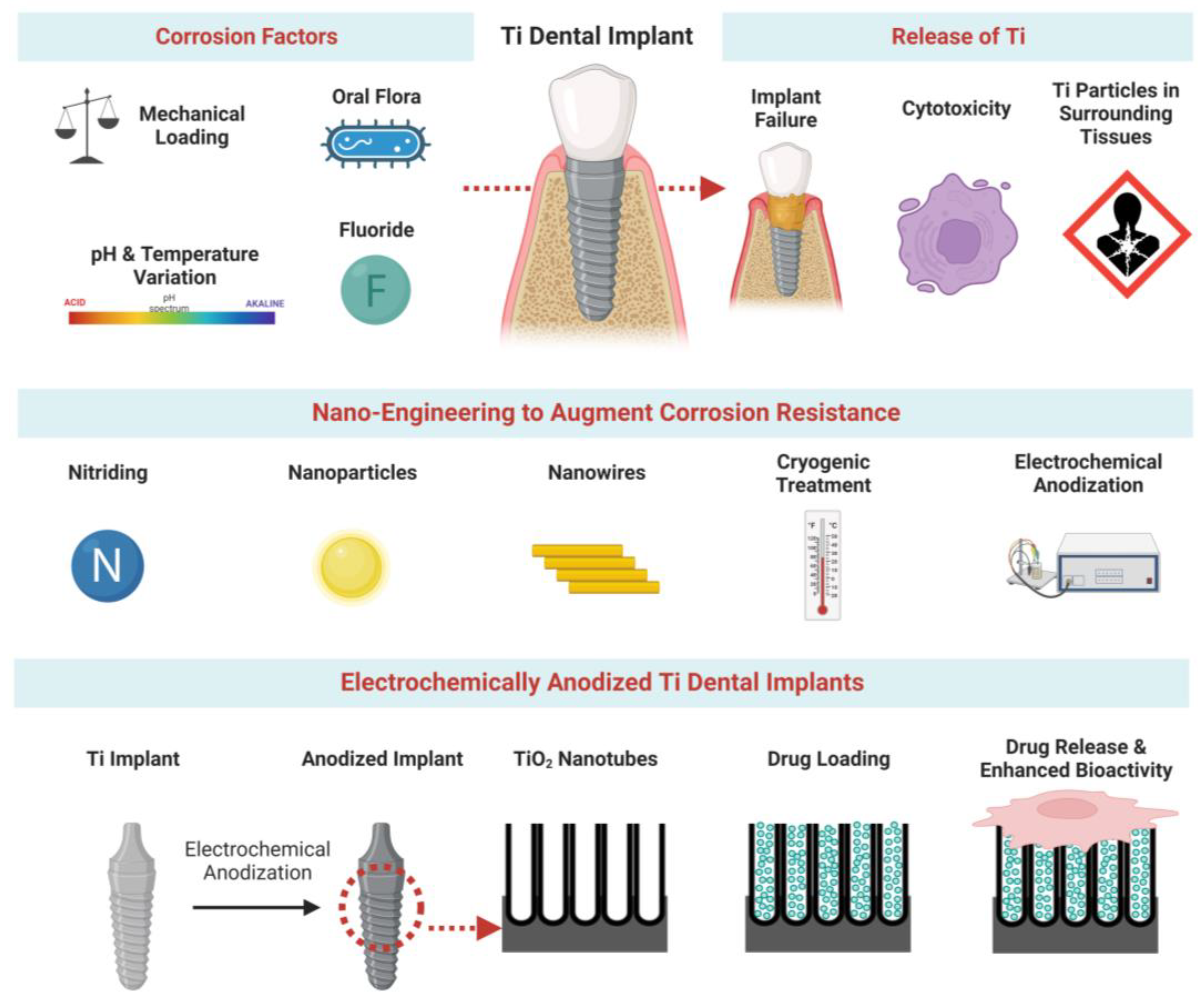
2. Factors Influencing Ti Implant Corrosion
2.1. Key Factors
2.1.1. Mechanical Corrosion
2.1.2. Chemical and Electrochemical Corrosion
2.1.3. Tribocorrosion
2.2. Specific Factors Linked to the Oral Cavity
2.2.1. Mechanical Factors
2.2.2. pH Variations
2.2.3. Oral Contamination
2.2.4. Fluoride Treatments
3. Enhancing Corrosion Resistance
3.1. Alloying and Chemical Modification
3.1.1. Alloying of Titanium
3.1.2. Chemical Coatings and Modifications
3.2. Implant Nano-Engineering
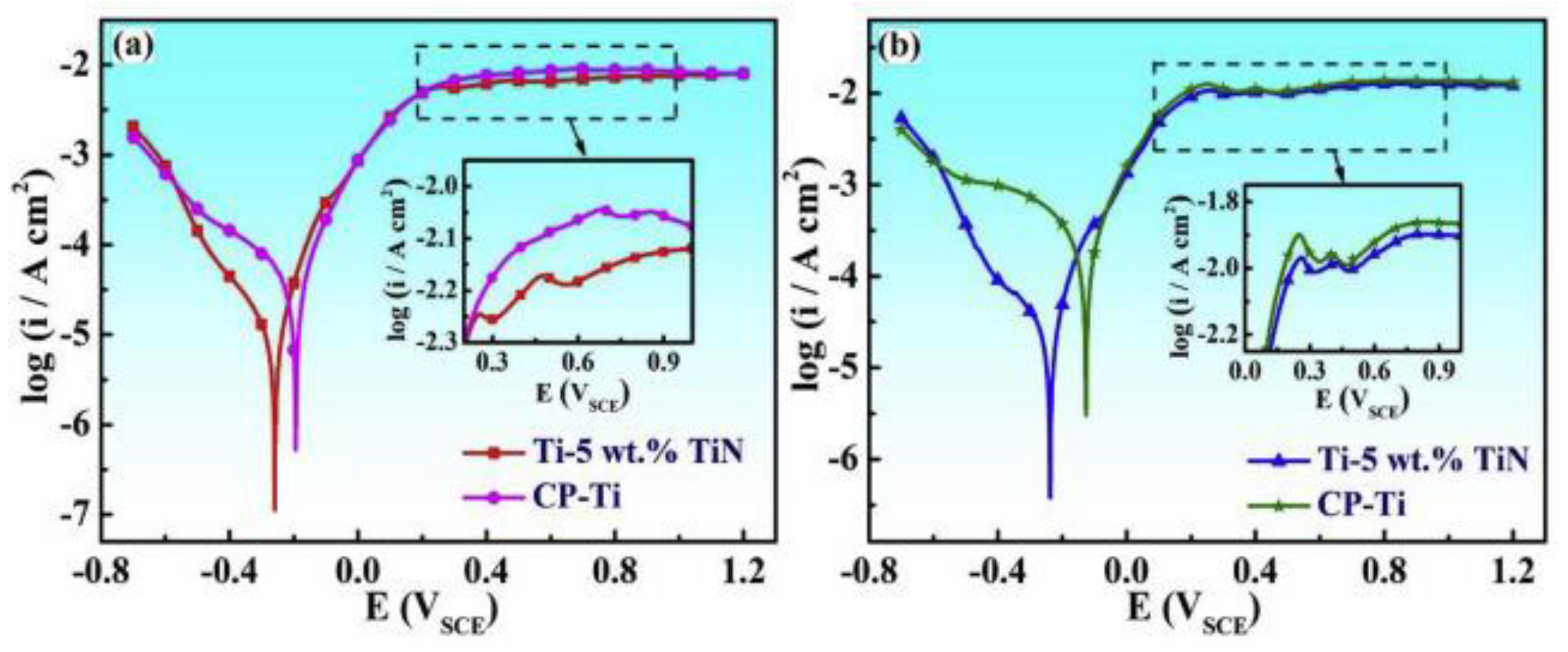
3.2.1. Nitriding for a Nanoparticular TiN Layer
3.2.2. Plasma Spraying of Nanoparticles (NPs)
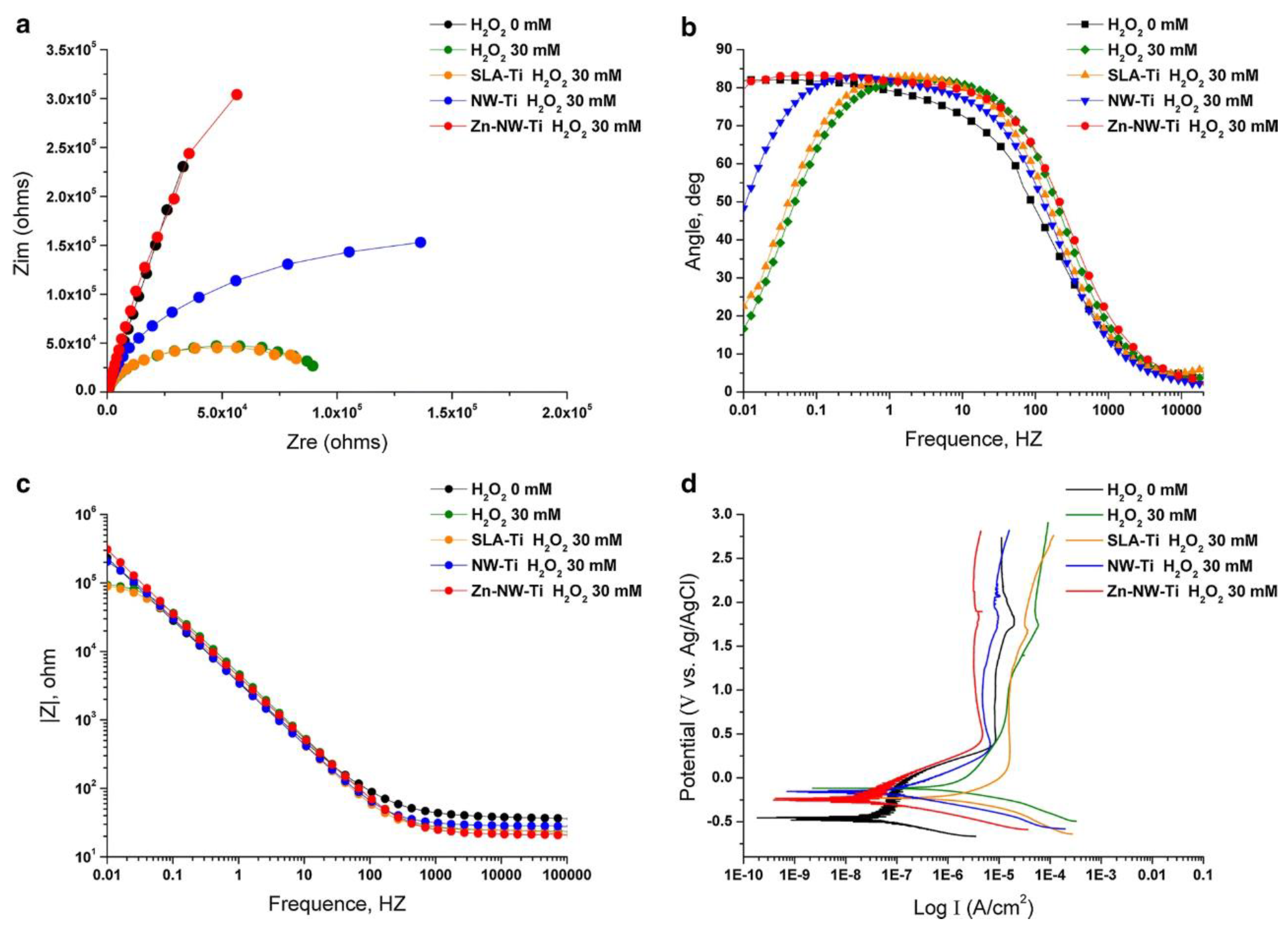
3.2.3. Depositing Nanowires (NWs)
3.3. Refining Grain Size into Nanoscale
3.3.1. Cryogenic Treatment
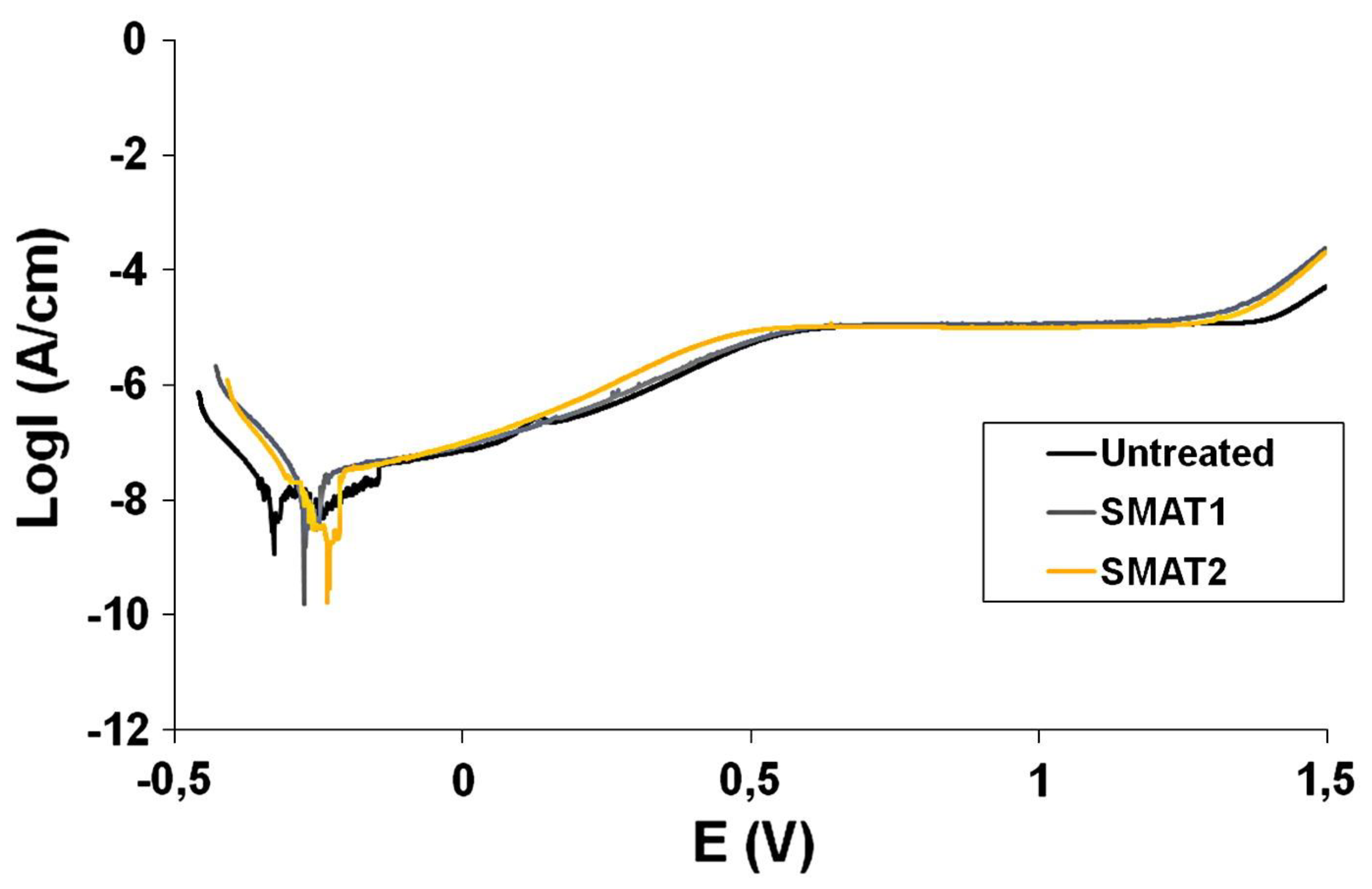
3.3.2. Surface Mechanical Attrition Treatment (SMAT)
4. Electrochemically Anodized Ti Implants
4.1. Anodization of Ti Implants
4.2. Thickened TiO2 Barrier Layer
4.3. Influence of Titania Nanostructure Layer
4.4. Influence of Nanotube Dimensions
4.5. Annealing of Anodized Ti
5. Drug-Releasing Anodized Implants towards Implant Integration
5.1. Enhanced Soft-Tissue Integration
5.2. Enhanced Osseointegration
6. Conclusions and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Orchestrating soft tissue integration at the transmucosal region of titanium implants. Acta Biomater. 2021, 124, 33–49. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and current interpretations of the bone-implant interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, S.; Lee, R. Comparison of peri-implant and periodontal marginal soft tissues in health and disease. Periodontol. 2000 2018, 76, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Wennerberg, A. On osseointegration in relation to implant surfaces. Clin. Implant. Dent. Relat. Res. 2019, 21, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Romanos, G.E.; Fischer, G.A.; Delgado-Ruiz, R. Titanium Wear of Dental Implants from Placement, under Loading and Maintenance Protocols. Int. J. Mol. Sci. 2021, 22, 1067. [Google Scholar] [CrossRef]
- Rashad, A.; Sadr-Eshkevari, P.; Weuster, M.; Schmitz, I.; Prochnow, N.; Maurer, P. Material attrition and bone micromorphology after conventional and ultrasonic implant site preparation. Clin. Oral Implant. Res. 2013, 24, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Race to invade: Understanding soft tissue integration at the transmucosal region of titanium dental implants. Dent. Mater. 2021, 37, 816–831. [Google Scholar] [CrossRef]
- Tanaka, N.; Ichinose, S.; Kimijima, Y.; Mimura, M. Investigation of titanium leak to bone tissue surrounding dental titanium implant: Electron microscopic findings and analysis by electron diffraction. Med. Electron. Microsc. 2000, 33, 96–101. [Google Scholar] [CrossRef]
- Martini, D.; Fini, M.; Franchi, M.; Pasquale, V.D.; Bacchelli, B.; Gamberini, M.; Tinti, A.; Taddei, P.; Giavaresi, G.; Ottani, V.; et al. Detachment of titanium and fluorohydroxyapatite particles in unloaded endosseous implants. Biomaterials 2003, 24, 1309–1316. [Google Scholar] [CrossRef]
- Ivanovski, S.; Bartold, P.M.; Huang, Y.-S. The role of foreign body response in peri-implantitis: What is the evidence? Periodontol. 2000 2022, 90, 176–185. [Google Scholar] [CrossRef]
- Meng, B.; Chen, J.; Guo, D.; Ye, Q.; Liang, X. The effect of titanium particles on rat bone marrow stem cells in vitro. Toxicol. Mech. Methods 2009, 19, 552–558. [Google Scholar] [CrossRef]
- Schulze, C.; Lochner, K.; Jonitz, A.; Lenz, R.; Duettmann, O.; Hansmann, D.; Bader, R. Cell viability, collagen synthesis and cytokine expression in human osteoblasts following incubation with generated wear particles using different bone cements. Int. J. Mol. Med. 2013, 32, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Q.; Zhang, S.-M.; Qiu, J. Surface analysis and corrosion behavior of pure titanium under fluoride exposure. J. Prosthet. Dent. 2020, 124, e231–e239. [Google Scholar] [CrossRef] [PubMed]
- Happe, A.; Sielker, S.; Hanisch, M.; Jung, S. The Biological Effect of Particulate Titanium Contaminants of Dental Implants on Human Osteoblasts and Gingival Fibroblasts. Int. J. Oral Maxillofac. Implant. 2019, 34, 673–680. [Google Scholar] [CrossRef]
- Pioletti, D.P.; Takei, H.; Kwon, S.Y.; Wood, D.; Sung, K.L. The cytotoxic effect of titanium particles phagocytosed by osteoblasts. J. Biomed. Mater. Res. 1999, 46, 399–407. [Google Scholar] [CrossRef]
- Mine, Y.; Makihira, S.; Nikawa, H.; Murata, H.; Hosokawa, R.; Hiyama, A.; Mimura, S. Impact of titanium ions on osteoblast-, osteoclast- and gingival epithelial-like cells. J. Prosthodont. Res. 2010, 54, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Saldaña, L.; Barranco, V.; García-Alonso, M.C.; Vallés, G.; Escudero, M.L.; Munuera, L.; Vilaboa, N. Concentration-dependent effects of titanium and aluminium ions released from thermally oxidized Ti6Al4V alloy on human osteoblasts. J. Biomed. Mater. Res. A 2006, 77A, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wong, C.; Xiong, J.; Hodgson, P.; Wen, C. Cytotoxicity of Titanium and Titanium Alloying Elements. J. Dent. Res. 2010, 89, 493–497. [Google Scholar] [CrossRef]
- Wachi, T.; Shuto, T.; Shinohara, Y.; Matono, Y.; Makihira, S. Release of titanium ions from an implant surface and their effect on cytokine production related to alveolar bone resorption. Toxicology 2015, 327, 1–9. [Google Scholar] [CrossRef]
- Cadosch, D.; Al-Mushaiqri, M.S.; Gautschi, O.P.; Meagher, J.; Simmen, H.-P.; Filgueira, L. Biocorrosion and uptake of titanium by human osteoclasts. J. Biomed. Mater. Res. A 2010, 95A, 1004–1010. [Google Scholar] [CrossRef]
- Smith, R.L.; Schwarz, E.M. Are Biologic Treatments a Potential Approach to Wear- and Corrosion-related Problems? Clin. Orthop. Relat. Res. 2014, 472, 3740–3746. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.-J.; Song, Y.-H.; An, J.-H.; Song, H.-J.; Anusavice, K.J. Cytocompatibility of pure metals and experimental binary titanium alloys for implant materials. J. Dent. 2013, 41, 1251–1258. [Google Scholar] [CrossRef]
- Noronha Oliveira, M.; Schunemann, W.V.H.; Mathew, M.T.; Henriques, B.; Magini, R.S.; Teughels, W.; Souza, J.C.M. Can degradation products released from dental implants affect peri-implant tissues? J. Periodontal. Res. 2018, 53, 1–11. [Google Scholar] [CrossRef]
- Batt, J.; Milward, M.; Chapple, I.; Grant, M.; Roberts, H.; Addison, O. TiO(2) nanoparticles can selectively bind CXCL8 impacting on neutrophil chemotaxis. Eur. Cell. Mater. 2018, 35, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, M.; Kelk, P.; Belibasakis, G.N.; Bylund, D.; Molin Thorén, M.; Johansson, A. Titanium ions form particles that activate and execute interleukin-1β release from lipopolysaccharide-primed macrophages. J. Periodontal. Res. 2017, 52, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Frisken, K.; Dandie, G.; Lugowski, S.; Jordan, G. A Study of Titanium Release into Body Organs Following the Insertion of Single Threaded Screw Implants into the Mandibles of Sheep. Aust. Dent. J. 2002, 47, 214–217. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Reichl, F.-X.; Wang, Y.; Michalke, B.; Milz, S.; Yang, Y.; Stolper, P.; Lindemaier, G.; Graw, M.; Hickel, R.; et al. Analysis of titanium and other metals in human jawbones with dental implants–A case series study. Dent. Mater. 2016, 32, 1042–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercan, S.; Bölükbaşı, N.; Bölükbaşı, M.K.; Yayla, M.; Cengiz, S. Titanium Element Level in Peri-Implant Mucosa. Biotechnol. Biotechnol. Equip. 2013, 27, 4002–4005. [Google Scholar] [CrossRef] [Green Version]
- Paknejad, M.; Bayani, M.; Yaghobee, S.; Kharazifard, M.J.; Jahedmanesh, N. Histopathological evaluation of gingival tissue overlying two-stage implants after placement of cover screws. Biotechnol. Biotechnol. Equip. 2015, 29, 1169–1175. [Google Scholar] [CrossRef] [Green Version]
- Mombelli, A.; Hashim, D.; Cionca, N. What is the impact of titanium particles and biocorrosion on implant survival and complications? A critical review. Clin. Oral Implant. Res. 2018, 29, 37–53. [Google Scholar] [CrossRef]
- Rakic, M.; Radunovic, M.; Petkovic-Curcin, A.; Tatic, Z.; Basta-Jovanovic, G.; Sanz, M. Study on the immunopathological effect of titanium particles in peri-implantitis granulation tissue: A case–control study. Clin. Oral Implant. Res. 2022, 33, 656–666. [Google Scholar] [CrossRef]
- Allsobrook, O.F.L.; Leichter, J.; Holborow, D.; Swain, M. Descriptive Study of the Longevity of Dental Implant Surgery Drills. Clin. Implant. Dent. Relat. Res. 2011, 13, 244–254. [Google Scholar] [CrossRef]
- Romanos, G.E.; Gaertner, K.; Nentwig, G.H. Long-Term Evaluation of Immediately Loaded Implants in the Edentulous Mandible Using Fixed Bridges and Platform Shifting. Clin. Implant. Dent. Relat. Res. 2014, 16, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Stimmelmayr, M.; Edelhoff, D.; Güth, J.-F.; Erdelt, K.; Happe, A.; Beuer, F. Wear at the titanium–titanium and the titanium–zirconia implant–abutment interface: A comparative in vitro study. Dent. Mater. 2012, 28, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruiz, R.; Romanos, G. Potential causes of titanium particle and ion release in implant dentistry: A systematic review. Int. J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, M.S. Mechanical complications of dental implants. Clin. Oral Implant. Res. 2000, 11, 156–158. [Google Scholar] [CrossRef]
- Apaza-Bedoya, K.; Tarce, M.; Benfatti, C.A.M.; Henriques, B.; Mathew, M.T.; Teughels, W.; Souza, J.C.M. Synergistic interactions between corrosion and wear at titanium-based dental implant connections: A scoping review. J. Periodontal. Res. 2017, 52, 946–954. [Google Scholar] [CrossRef]
- Siddiqui, D.A.; Guida, L.; Sridhar, S.; Valderrama, P.; Wilson, T.G., Jr.; Rodrigues, D.C. Evaluation of oral microbial corrosion on the surface degradation of dental implant materials. J. Periodontol. 2019, 90, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Souza, J.C.M.; Barbosa, S.L.; Ariza, E.A.; Henriques, M.; Teughels, W.; Ponthiaux, P.; Celis, J.-P.; Rocha, L.A. How do titanium and Ti6Al4V corrode in fluoridated medium as found in the oral cavity? An in vitro study. Mater. Sci. Eng. C 2015, 47, 384–393. [Google Scholar] [CrossRef] [Green Version]
- Revathi, A.; Borrás, A.D.; Muñoz, A.I.; Richard, C.; Manivasagam, G. Degradation mechanisms and future challenges of titanium and its alloys for dental implant applications in oral environment. Mater. Sci. Eng. C 2017, 76, 1354–1368. [Google Scholar] [CrossRef]
- Shah, F.A.; Grandfield, K.; Palmquist, A. 9—Laser surface modification and the tissue–implant interface. In Laser Surface Modification of Biomaterials; Vilar, R., Ed.; Woodhead Publishing: Sawston, UK, 2016; pp. 253–280. [Google Scholar]
- Peixoto, C.D.; Almas, K. The implant surface characteristics and peri-implantitis. An evidence-based update. Odontostomatol. Trop. 2016, 39, 23–35. [Google Scholar] [PubMed]
- Mouhyi, J.; Dohan Ehrenfest, D.M.; Albrektsson, T. The Peri-Implantitis: Implant Surfaces, Microstructure, and Physicochemical Aspects. Clin. Implant. Dent. Relat. Res. 2012, 14, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Addison, O.; Baker, S.J.; Davenport, A.J. Lipopolysaccharide inhibits or accelerates biomedical titanium corrosion depending on environmental acidity. Int. J. Oral. Sci. 2015, 7, 179–186. [Google Scholar] [CrossRef]
- Perinetti, G.; Contardo, L.; Ceschi, M.; Antoniolli, F.; Franchi, L.; Baccetti, T.; Di Lenarda, R. Surface corrosion and fracture resistance of two nickel-titanium-based archwires induced by fluoride, pH, and thermocycling. An in vitro comparative study. Eur. J. Orthod. 2012, 34, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiff, N.; Grosgogeat, B.; Lissac, M.; Dalard, F. Influence of fluoride content and pH on the corrosion resistance of titanium and its alloys. Biomaterials 2002, 23, 1995–2002. [Google Scholar] [CrossRef]
- Kaneko, K.; Yokoyama, K.I.; Moriyama, K.; Asaoka, K.; Sakai, J.I.; Nagumo, M. Delayed fracture of beta titanium orthodontic wire in fluoride aqueous solutions. Biomaterials 2003, 24, 2113–2120. [Google Scholar] [CrossRef]
- Akimoto, T.; Ueno, T.; Tsutsumi, Y.; Doi, H.; Hanawa, T.; Wakabayashi, N. Evaluation of corrosion resistance of implant-use Ti-Zr binary alloys with a range of compositions. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 73–79. [Google Scholar] [CrossRef]
- Han, M.-K.; Hwang, M.-J.; Yang, M.-S.; Yang, H.-S.; Song, H.-J.; Park, Y.-J. Effect of zirconium content on the microstructure, physical properties and corrosion behavior of Ti alloys. Mater. Sci. Eng. A 2014, 616, 268–274. [Google Scholar] [CrossRef]
- Han, M.-K.; Kim, J.-Y.; Hwang, M.-J.; Song, H.-J.; Park, Y.-J. Effect of Nb on the Microstructure, Mechanical Properties, Corrosion Behavior, and Cytotoxicity of Ti-Nb Alloys. Materials 2015, 8, 5986–6003. [Google Scholar] [CrossRef] [Green Version]
- Çaha, I.; Alves, A.C.; Kuroda, P.A.B.; Grandini, C.R.; Pinto, A.M.P.; Rocha, L.A.; Toptan, F. Degradation behavior of Ti-Nb alloys: Corrosion behavior through 21 days of immersion and tribocorrosion behavior against alumina. Corros. Sci. 2020, 167, 108488. [Google Scholar] [CrossRef]
- Coelho, P.G.; de Assis, S.L.; Costa, I.; Thompson, V.P. Corrosion resistance evaluation of a Ca- and P-based bioceramic thin coating in Ti-6Al-4V. J. Mater. Sci. Mater. Med. 2009, 20, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-H.; Chen, Y.-C.; Liao, C.-C.; Lin, L.-W.; Chen, C.-F.; Wang, K.-K.; Chen, S.-T.; Hsueh, Y.-H.; Wu, C.-H.; Ou, S.-F. Improvement in bioactivity and corrosion resistance of Ti by hydroxyapatite deposition using ultrasonic mechanical coating and armoring. Ceram. Int. 2022, 48, 4999–5008. [Google Scholar] [CrossRef]
- Prando, D.; Brenna, A.; Diamanti, M.V.; Beretta, S.; Bolzoni, F.; Ormellese, M.; Pedeferri, M. Corrosion of titanium: Part 2: Effects of surface treatments. J. Appl. Biomater. Funct. Mater. 2018, 16, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti, M.V.; Spreafico, F.C.; Pedeferri, M.P. Production of Anodic TiO2 Nanofilms and their Characterization. Phys. Procedia 2013, 40, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Hongxi, L.; Qian, X.; Xiaowei, Z.; Chuanqi, W.; Baoyin, T. Wear and corrosion behaviors of Ti6Al4V alloy biomedical materials by silver plasma immersion ion implantation process. Thin Solid Film 2012, 521, 89–93. [Google Scholar] [CrossRef]
- Yang, C.-H.; Wang, Y.-T.; Tsai, W.-F.; Ai, C.-F.; Lin, M.-C.; Huang, H.-H. Effect of oxygen plasma immersion ion implantation treatment on corrosion resistance and cell adhesion of titanium surface. Clin. Oral Implant. Res. 2011, 22, 1426–1432. [Google Scholar] [CrossRef]
- Mohan, L.; Anandan, C. Wear and corrosion behavior of oxygen implanted biomedical titanium alloy Ti-13Nb-13Zr. Appl. Surf. Sci. 2013, 282, 281–290. [Google Scholar] [CrossRef]
- Zhang, Y.; Gulati, K.; Li, Z.; Di, P.; Liu, Y. Dental Implant Nano-Engineering: Advances, Limitations and Future Directions. Nanomaterials 2021, 11, 2489. [Google Scholar] [CrossRef]
- Chung, K.H.; Liu, G.T.; Duh, J.G.; Wang, J.H. Biocompatibility of a titanium–aluminum nitride film coating on a dental alloy. Surf. Coat. Technol. 2004, 188-189, 745–749. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, M.; Ahangarani, S.; Esmailian, M.; Shanaghi, A. Investigation on the corrosion behavior and biocompatibility of Ti-6Al-4V implant coated with HA/TiN dual layer for medical applications. Surf. Coat. Technol. 2020, 397, 126044. [Google Scholar] [CrossRef]
- Zhou, S.; Zhao, Y.; Wang, X.; Li, W.; Chen, D.; Sercombe, T.B. Enhanced corrosion resistance of Ti-5 wt.% TiN composite compared to commercial pure Ti produced by selective laser melting in HCl solution. J. Alloy. Compd. 2020, 820, 153422. [Google Scholar] [CrossRef]
- Ananthakumar, R.; Subramanian, B.; Kobayashi, A.; Jayachandran, M. Electrochemical corrosion and materials properties of reactively sputtered TiN/TiAlN multilayer coatings. Ceram. Int. 2012, 38, 477–485. [Google Scholar] [CrossRef]
- Rossi, S.; Fedrizzi, L.; Bacci, T.; Pradelli, G. Corrosion behaviour of glow discharge nitrided titanium alloys. Corros. Sci. 2003, 45, 511–529. [Google Scholar] [CrossRef]
- Kwok, C.T.; Wong, P.K.; Cheng, F.T.; Man, H.C. Characterization and corrosion behavior of hydroxyapatite coatings on Ti6Al4V fabricated by electrophoretic deposition. Appl. Surf. Sci. 2009, 255, 6736–6744. [Google Scholar] [CrossRef]
- Singh, S.; Pandey, K.K.; Islam, A.; Keshri, A.K. Corrosion behaviour of plasma sprayed graphene nanoplatelets reinforced hydroxyapatite composite coatings in simulated body fluid. Ceram. Int. 2020, 46, 13539–13548. [Google Scholar] [CrossRef]
- Richard, C.; Kowandy, C.; Landoulsi, J.; Geetha, M.; Ramasawmy, H. Corrosion and wear behavior of thermally sprayed nano ceramic coatings on commercially pure Titanium and Ti–13Nb–13Zr substrates. Int. J. Refract. Met. Hard Mater. 2010, 28, 115–123. [Google Scholar] [CrossRef]
- Palanivelu, R.; Kalainathan, S.; Ruban Kumar, A. Characterization studies on plasma sprayed (AT/HA) bi-layered nano ceramics coating on biomedical commercially pure titanium dental implant. Ceram. Int. 2014, 40, 7745–7751. [Google Scholar] [CrossRef]
- Palanivelu, R.; Ruban Kumar, A. Scratch and wear behaviour of plasma sprayed nano ceramics bilayer Al2O3-13wt%TiO2/hydroxyapatite coated on medical grade titanium substrates in SBF environment. Appl. Surf. Sci. 2014, 315, 372–379. [Google Scholar] [CrossRef]
- Gulati, K.; Scimeca, J.-C.; Ivanovski, S.; Verron, E. Double-edged sword: Therapeutic efficacy versus toxicity evaluations of doped titanium implants. Drug Discov. Today 2021, 26, 2734–2742. [Google Scholar] [CrossRef]
- Zhu, W.-q.; Shao, S.-y.; Xu, L.-n.; Chen, W.-q.; Yu, X.-y.; Tang, K.-m.; Tang, Z.-h.; Zhang, F.-m.; Qiu, J. Enhanced corrosion resistance of zinc-containing nanowires-modified titanium surface under exposure to oxidizing microenvironment. J. Nanobiotechnol. 2019, 17, 55. [Google Scholar] [CrossRef]
- Manole, C.C.; Dinischiotu, A.; Nica, C.; Demetrescu, I.; Pirvu, C. Influence of electrospun TiO2 nanowires on corrosion resistance and cell response of Ti50Zr alloy. Mater. Corros. 2018, 69, 1609–1619. [Google Scholar] [CrossRef]
- Bhaskar, P.; Dasgupta, A.; Sarma, V.S.; Mudali, U.K.; Saroja, S. Mechanical properties and corrosion behaviour of nanocrystalline Ti–5Ta–1.8Nb alloy produced by cryo-rolling. Mater. Sci. Eng. A 2014, 616, 71–77. [Google Scholar] [CrossRef]
- Tang, J.; Luo, H.; Zhang, Y. Enhancing the surface integrity and corrosion resistance of Ti-6Al-4V titanium alloy through cryogenic burnishing. Int. J. Adv. Manuf. Technol. 2017, 88, 2785–2793. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, C.; Zhang, L. Effects of Cryo-Treatment on Corrosion Behavior and Mechanical Properties of Laser-Welded Commercial Pure Titanium. Mater. Trans. 2014, 55, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Gu, K.-X.; Wang, K.-K.; Zheng, J.-P.; Chen, L.-B.; Wang, J.-J. Electrochemical behavior of Ti–6Al–4V alloy in Hank’s solution subjected to deep cryogenic treatment. Rare. Met. 2018. [Google Scholar] [CrossRef]
- Jelliti, S.; Richard, C.; Retraint, D.; Roland, T.; Chemkhi, M.; Demangel, C. Effect of surface nanocrystallization on the corrosion behavior of Ti–6Al–4V titanium alloy. Surf. Coat. Technol. 2013, 224, 82–87. [Google Scholar] [CrossRef]
- Lin, Y.; Lu, J.; Wang, L.; Xu, T.; Xue, Q. Surface nanocrystallization by surface mechanical attrition treatment and its effect on structure and properties of plasma nitrided AISI 321 stainless steel. Acta Mater. 2006, 54, 5599–5605. [Google Scholar] [CrossRef]
- Huang, R.; Han, Y. The effect of SMAT-induced grain refinement and dislocations on the corrosion behavior of Ti–25Nb–3Mo–3Zr–2Sn alloy. Mater. Sci. Eng. C 2013, 33, 2353–2359. [Google Scholar] [CrossRef]
- Skowron, K.; Wróbel, M.; Mosiałek, M.; Joncour, L.L.; Dryzek, E. Gradient Microstructure Induced by Surface Mechanical Attrition Treatment in Grade 2 Titanium Studied Using Positron Annihilation Spectroscopy and Complementary Methods. Materials 2021, 14, 6347. [Google Scholar] [CrossRef]
- Gulati, K.; Santos, A.; Findlay, D.; Losic, D. Optimizing Anodization Conditions for the Growth of Titania Nanotubes on Curved Surfaces. J. Phys. Chem. C 2015, 119, 16033–16045. [Google Scholar] [CrossRef]
- Gulati, K.; Martinez, R.D.O.; Czerwiński, M.; Michalska-Domańska, M. Understanding the influence of electrolyte aging in electrochemical anodization of titanium. Adv. Colloid Interface Sci. 2022, 302, 102615. [Google Scholar] [CrossRef] [PubMed]
- Chopra, D.; Guo, T.; Ivanovski, S.; Gulati, K. Single-step nano-engineering of multiple micro-rough metals via anodization. Nano Res. 2023, 16, 1320–1329. [Google Scholar] [CrossRef]
- Guo, T.; Oztug, N.A.K.; Han, P.; Ivanovski, S.; Gulati, K. Untwining the topography-chemistry interdependence to optimize the bioactivity of nano-engineered titanium implants. Appl. Surf. Sci. 2021, 570, 151083. [Google Scholar] [CrossRef]
- Li, T.; Gulati, K.; Wang, N.; Zhang, Z.; Ivanovski, S. Bridging the gap: Optimized fabrication of robust titania nanostructures on complex implant geometries towards clinical translation. J. Colloid Interface Sci. 2018, 529, 452–463. [Google Scholar] [CrossRef] [Green Version]
- Guo, T.; Oztug, N.A.K.; Han, P.; Ivanovski, S.; Gulati, K. Old is Gold: Electrolyte Aging Influences the Topography, Chemistry, and Bioactivity of Anodized TiO2 Nanopores. ACS Appl. Mater. Interfaces 2021, 13, 7897–7912. [Google Scholar] [CrossRef]
- Gulati, K.; Li, T.; Ivanovski, S. Consume or Conserve: Microroughness of Titanium Implants toward Fabrication of Dual Micro–Nanotopography. ACS Biomater. Sci. Eng. 2018, 4, 3125–3131. [Google Scholar] [CrossRef] [Green Version]
- Gulati, K.; Moon, H.-J.; Kumar, P.T.S.; Han, P.; Ivanovski, S. Anodized anisotropic titanium surfaces for enhanced guidance of gingival fibroblasts. Mater. Sci. Eng. C 2020, 112, 110860. [Google Scholar] [CrossRef]
- Martinez-Marquez, D.; Gulati, K.; Carty, C.P.; Stewart, R.A.; Ivanovski, S. Determining the relative importance of titania nanotubes characteristics on bone implant surface performance: A quality by design study with a fuzzy approach. Mater. Sci. Eng. C 2020, 114, 110995. [Google Scholar] [CrossRef]
- Gulati, K.; Moon, H.-J.; Li, T.; Sudheesh Kumar, P.T.; Ivanovski, S. Titania nanopores with dual micro-/nano-topography for selective cellular bioactivity. Mater. Sci. Eng. C 2018, 91, 624–630. [Google Scholar] [CrossRef]
- Jayasree, A.; Ivanovski, S.; Gulati, K. ON or OFF: Triggered therapies from anodized nano-engineered titanium implants. J. Control. Release 2021, 333, 521–535. [Google Scholar] [CrossRef]
- Gulati, K.; Kogawa, M.; Maher, S.; Atkins, G.; Findlay, D.; Losic, D. Titania Nanotubes for Local Drug Delivery from Implant Surfaces. In Electrochemically Engineered Nanoporous Materials: Methods, Properties and Applications; Losic, D., Santos, A., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 307–355. [Google Scholar]
- Karambakhsh, A.; Afshar, A.; Malekinejad, P. Corrosion Resistance and Color Properties of Anodized Ti-6Al-4V. J Mater Eng Perform 2012, 21, 121–127. [Google Scholar] [CrossRef]
- Saraswati, W.C.; Anawati, A.; Jujur, I.N.; Gumelar, M.D. Effect of coloring by anodizing on the corrosion behavior of Ti-6Al-4V alloy. AIP Conf. Proc. 2020, 2232, 020004. [Google Scholar] [CrossRef]
- Saji, V.S.; Choe, H.C. Electrochemical corrosion behaviour of nanotubular Ti–13Nb–13Zr alloy in Ringer’s solution. Corros. Sci. 2009, 51, 1658–1663. [Google Scholar] [CrossRef]
- Demetrescu, I.; Pirvu, C.; Mitran, V. Effect of nano-topographical features of Ti/TiO2 electrode surface on cell response and electrochemical stability in artificial saliva. Bioelectrochemistry 2010, 79, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Al-Saady, F.A.A.; Rushdi, S.A.; Abbar, A.H. Improvement the corrosion Behavior of Titanium by Nanotubular Oxide in a simulated saliva solution. IOP Conf. Ser. Mater. Sci. Eng. 2020, 870, 012060. [Google Scholar] [CrossRef]
- Singh, A.; Singh, B.P.; Wani, M.R.; Kumar, D.; Singh, J.K.; Singh, V. Effect of anodization on corrosion behaviour and biocompatibility of Cp-titanium in simulated body fluid. Bull. Mater. Sci. 2013, 36, 931–937. [Google Scholar] [CrossRef] [Green Version]
- Uzal, H.; Döner, A. Corrosion Behavior of Titanium Dioxide Nanotubes in Alkaline Solution. Prot. Met. Phys. Chem. Surf. 2020, 56, 311–319. [Google Scholar] [CrossRef]
- Liu, C.; Wang, Y.; Wang, M.; Huang, W.; Chu, P.K. Electrochemical stability of TiO2 nanotubes with different diameters in artificial saliva. Surf. Coat. Technol. 2011, 206, 63–67. [Google Scholar] [CrossRef]
- Huang, Q.; Yang, Y.; Hu, R.; Lin, C.; Sun, L.; Vogler, E.A. Reduced platelet adhesion and improved corrosion resistance of superhydrophobic TiO2-nanotube-coated 316L stainless steel. Colloids Surf. B Biointerfaces 2015, 125, 134–141. [Google Scholar] [CrossRef]
- Ossowska, A.; Zieliński, A.; Olive, J.-M.; Wojtowicz, A.; Szweda, P. Influence of Two-Stage Anodization on Properties of the Oxide Coatings on the Ti–13Nb–13Zr Alloy. Coatings 2020, 10, 707. [Google Scholar] [CrossRef]
- Nogueira, R.P.; Deuzimar Uchoa, J.; Hilario, F.; Santana-Melo, G.F.; de Vasconcellos, L.M.R.; Marciano, F.R.; Roche, V.; Moreira Jorge Junior, A.; Lobo, A.O. Characterization of Optimized TiO(2) Nanotubes Morphology for Medical Implants: Biological Activity and Corrosion Resistance. Int. J. Nanomed. 2021, 16, 667–682. [Google Scholar] [CrossRef] [PubMed]
- Fatichi, A.Z.; de Mello, M.G.; Pereira, K.D.; Antonio, L.G.M.; Luchessi, A.D.; Caram, R.; Cremasco, A. Crystalline phase of TiO2 nanotube arrays on Ti–35Nb–4Zr alloy: Surface roughness, electrochemical behavior and cellular response. Ceram. Int. 2022, 48, 5154–5161. [Google Scholar] [CrossRef]
- Yu, W.Q.; Qiu, J.; Xu, L.; Zhang, F.Q. Corrosion behaviors of TiO2 nanotube layers on titanium in Hank’s solution. Biomed. Mater. 2009, 4, 065012. [Google Scholar] [CrossRef]
- Chopra, D.; Gulati, K.; Ivanovski, S. Understanding and optimizing the antibacterial functions of anodized nano-engineered titanium implants. Acta Biomater. 2021, 127, 80–101. [Google Scholar] [CrossRef] [PubMed]
- Chopra, D.; Jayasree, A.; Guo, T.; Gulati, K.; Ivanovski, S. Advancing dental implants: Bioactive and therapeutic modifications of zirconia. Bioact. Mater. 2022, 13, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Zhang, Y.; Di, P.; Liu, Y.; Ivanovski, S. Research to Clinics: Clinical Translation Considerations for Anodized Nano-Engineered Titanium Implants. ACS Biomater. Sci. Eng. 2022, 8, 4077–4091. [Google Scholar] [CrossRef]
- Gulati, K.; Atkins, G.J.; Findlay, D.M.; Losic, D. Nano-engineered titanium for enhanced bone therapy. In Proceedings of the Biosensing and Nanomedicine, San Diego, CA, USA, 11 September 2013; Volume VI, pp. 28–33. [Google Scholar] [CrossRef] [Green Version]
- Atsuta, I.; Ayukawa, Y.; Kondo, R.; Oshiro, W.; Matsuura, Y.; Furuhashi, A.; Tsukiyama, Y.; Koyano, K. Soft tissue sealing around dental implants based on histological interpretation. J. Prosthodont. Res. 2016, 60, 3–11. [Google Scholar] [CrossRef]
- Atsuta, I.; Yamaza, T.; Yoshinari, M.; Mino, S.; Goto, T.; Kido, M.A.; Terada, Y.; Tanaka, T. Changes in the distribution of laminin-5 during peri-implant epithelium formation after immediate titanium implantation in rats. Biomaterials 2005, 26, 1751–1760. [Google Scholar] [CrossRef]
- Wei, H.; Wu, S.; Feng, Z.; Zhou, W.; Dong, Y.; Wu, G.; Bai, S.; Zhao, Y. Increased fibroblast functionality on CNN2-loaded titania nanotubes. Int. J. Nanomed. 2012, 7, 1091–1100. [Google Scholar] [CrossRef]
- Ma, Q.; Mei, S.; Ji, K.; Zhang, Y.; Chu, P.K. Immobilization of Ag nanoparticles/FGF-2 on a modified titanium implant surface and improved human gingival fibroblasts behavior. J. Biomed. Mater. Res. Part A 2011, 98A, 274–286. [Google Scholar] [CrossRef]
- Xu, R.; Hu, X.; Yu, X.; Wan, S.; Wu, F.; Ouyang, J.; Deng, F. Micro-/nano-topography of selective laser melting titanium enhances adhesion and proliferation and regulates adhesion-related gene expressions of human gingival fibroblasts and human gingival epithelial cells. Int. J. Nanomed. 2018, 13, 5045–5057. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.T.; Tan, H.L.; Duan, Z.L.; Yue, B.; Ma, R.; He, G.; Tang, T.T. Inhibited bacterial biofilm formation and improved osteogenic activity on gentamicin-loaded titania nanotubes with various diameters. Int. J. Nanomed. 2014, 9, 1215–1230. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Wang, H.; Huo, K.; Cui, L.; Zhang, W.; Ni, H.; Zhang, Y.; Wu, Z.; Chu, P.K. Antibacterial nano-structured titania coating incorporated with silver nanoparticles. Biomaterials 2011, 32, 5706–5716. [Google Scholar] [CrossRef]
- Jayasree, A.; Gómez-Cerezo, M.N.; Verron, E.; Ivanovski, S.; Gulati, K. Gallium-doped dual micro-nano titanium dental implants towards soft-tissue integration and bactericidal functions. Mater. Today Adv. 2022, 16, 100297. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Z.; Shen, G.; Zhao, J. Enhanced osteogenic activity and anti-inflammatory properties of Lenti-BMP-2-loaded TiO₂ nanotube layers fabricated by lyophilization following trehalose addition. Int. J. Nanomed. 2016, 11, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Zhang, Z.; Liu, Y.; Li, H.; Wang, N.; Liu, W.; Li, W.; Jin, L.; Wang, J.; Chen, S. Nanotubes Functionalized with BMP2 Knuckle Peptide Improve the Osseointegration of Titanium Implants in Rabbits. J. Biomed. Nanotechnol. 2015, 11, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Albashari, A.A.; He, Y.; Albaadani, M.A.; Xiang, Y.; Ali, J.; Hu, F.; Zhang, Y.; Zhang, K.; Luo, L.; Wang, J.; et al. Titanium Nanotube Modified With Silver Cross-Linked Basic Fibroblast Growth Factor Improves Osteoblastic Activities of Dental Pulp Stem Cells and Antibacterial Effect. Front. Cell Dev. Biol. 2021, 9, 665. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Kogawa, M.; Prideaux, M.; Findlay, D.M.; Atkins, G.J.; Losic, D. Drug-releasing nano-engineered titanium implants: Therapeutic efficacy in 3D cell culture model, controlled release and stability. Mater. Sci. Eng. C 2016, 69, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Roguska, A.; Pisarek, M.; Andrzejczuk, M.; Dolata, M.; Lewandowska, M.; Janik-Czachor, M. Characterization of a calcium phosphate–TiO2 nanotube composite layer for biomedical applications. Mater. Sci. Eng. C 2011, 31, 906–914. [Google Scholar] [CrossRef]
- Yao, Q.; Jiang, Y.; Tan, S.; Fu, X.; Li, B.; Liu, L. Composition and bioactivity of calcium phosphate coatings on anodic oxide nanotubes formed on pure Ti and Ti-6Al-4V alloy substrates. Mater. Sci. Eng. C 2020, 110, 110687. [Google Scholar] [CrossRef]
- Kung, K.-C.; Chen, J.-L.; Liu, Y.-T.; Lee, T.-M. Fabrication and characterization of CaP-coated nanotube arrays. Mater. Chem. Phys. 2015, 153, 110–116. [Google Scholar] [CrossRef]
- Saji, V.S. Recent Updates on Supramolecular-Based Drug Delivery—Macrocycles and Supramolecular Gels. Chem. Rec. 2022, 22, e202200053. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Ramakrishnan, S.; Aw, M.S.; Atkins, G.J.; Findlay, D.M.; Losic, D. Biocompatible polymer coating of titania nanotube arrays for improved drug elution and osteoblast adhesion. Acta Biomater. 2012, 8, 449–456. [Google Scholar] [CrossRef] [PubMed]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, T.; Scimeca, J.-C.; Ivanovski, S.; Verron, E.; Gulati, K. Enhanced Corrosion Resistance and Local Therapy from Nano-Engineered Titanium Dental Implants. Pharmaceutics 2023, 15, 315. https://doi.org/10.3390/pharmaceutics15020315
Guo T, Scimeca J-C, Ivanovski S, Verron E, Gulati K. Enhanced Corrosion Resistance and Local Therapy from Nano-Engineered Titanium Dental Implants. Pharmaceutics. 2023; 15(2):315. https://doi.org/10.3390/pharmaceutics15020315
Chicago/Turabian StyleGuo, Tianqi, Jean-Claude Scimeca, Sašo Ivanovski, Elise Verron, and Karan Gulati. 2023. "Enhanced Corrosion Resistance and Local Therapy from Nano-Engineered Titanium Dental Implants" Pharmaceutics 15, no. 2: 315. https://doi.org/10.3390/pharmaceutics15020315