

Focal Photocoagulation as an Adjunctive Therapy to Reduce the Burden of Intravitreal Injections in Macula Edema Patients, the LyoMAC2 Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Outcome Measures
2.4. Statistics
3. Results
3.1. Patients’ Characteristics
3.2. Primary and Secondary Outcomes
3.3. Functional and Anatomical Outcomes According to the Type of IVI Agent
3.4. Functional and Anatomical Outcomes According to the Size of CMA
3.5. Functional and Anatomical Outcomes According to the Cause of ME
3.6. Functional and Anatomical Outcomes According to the Distance between CMA and the Fovea
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhagat, N.; Grigorian, R.A.; Tutela, A.; Zarbin, M.A. Diabetic Macular Edema: Pathogenesis and Treatment. Surv. Ophthalmol. 2009, 54, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Retinal vascular cystoid macular edema: Review and New Theory. Retina 2016, 36, 1823–1842. [Google Scholar] [CrossRef] [PubMed]
- Stitt, A.W.; A Gardiner, T.; Archer, D.B. Histological and ultrastructural investigation of retinal microaneurysm development in diabetic patients. Br. J. Ophthalmol. 1995, 79, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Murakami, T.; Nishijima, K.; Sakamoto, A.; Ota, M.; Horii, T.; Yoshimura, N. Foveal Cystoid Spaces Are Associated with Enlarged Foveal Avascular Zone and Microaneurysms in Diabetic Macular Edema. Ophthalmology 2011, 118, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Bourhis, A.; Girmens, J.-F.; Boni, S.; Pecha, F.; Favard, C.; Sahel, J.-A.; Paques, M. Imaging of macroaneurysms occurring during retinal vein occlusion and diabetic retinopathy by indocyanine green angiography and high resolution optical coherence tomography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 248, 161–166. [Google Scholar] [CrossRef]
- Paques, M.; Philippakis, E.; Bonnet, C.; Falah, S.; Ayello-Scheer, S.; Zwillinger, S.; Girmens, J.-F.; Dupas, B. Indocyanine-green-guided targeted laser photocoagulation of capillary macroaneurysms in macular oedema: A pilot study. Br. J. Ophthalmol. 2017, 101, 170–174. [Google Scholar] [CrossRef]
- Parodi, M.B.; Bondel, E.; Ravalico, G. Capillary Macroaneurysms in Central Retinal Vein Occlusion. Ophthalmologica 1995, 209, 248–250. [Google Scholar] [CrossRef]
- Farías, D.C.; Serrano, R.M.; Gancharov, J.B.; Cuadras, U.D.D.; Sahel, J.; Wiechers, F.G.; Dupas, B.; Paques, M. Indocyanine green angiography for identifying telangiectatic capillaries in diabetic macular oedema. Br. J. Ophthalmol. 2019, 104, 509–513. [Google Scholar] [CrossRef]
- Chaperon, M.; Kodjikian, L.; Agard, E.; Mathis, T.; Billant, J.; El-Chehab, H.; Pradat, P.; Dot, C. Screening of telangiectatic capillaries in chronic macular edema based on multimodal imaging: A study of 101 eyes. LyoMAC1 study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 2501–2508. [Google Scholar] [CrossRef]
- Hamada, M.; Ohkoshi, K.; Inagaki, K.; Ebihara, N.; Murakami, A. Visualization of microaneurysms using optical coherence tomography angiography: Comparison of OCTA en face, OCT B-scan, OCT en face, FA, and IA images. Jpn. J. Ophthalmol. 2018, 62, 168–175. [Google Scholar] [CrossRef]
- Pennington, B.; Alshreef, A.; Flight, L.; Metry, A.; Poku, E.; Hykin, P.; Sivaprasad, S.; Prevost, A.T.; Vasconcelos, J.C.; Murphy, C.; et al. Cost Effectiveness of Ranibizumab vs Aflibercept vs Bevacizumab for the Treatment of Macular Oedema Due to Central Retinal Vein Occlusion: The LEAVO Study. Pharmacoeconomics 2021, 39, 913–927. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.L.; Hutton, D.W.; Stein, J.; Bressler, N.M.; Jampol, L.M.; Glassman, A.R. Diabetic Retinopathy Clinical Research Network Cost-effectiveness of Aflibercept, Bevacizumab, and Ranibizumab for Diabetic Macular Edema Treatment. JAMA Ophthalmol 2016, 134, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Ogura, S.; Yasukawa, T.; Kato, A.; Kuwayama, S.; Hamada, S.; Hirano, Y.; Uemura, A.; Yoshida, M.; Ogura, Y. Indocyanine Green Angiography-Guided Focal Laser Photocoagulation for Diabetic Macular Edema. Ophthalmologica 2015, 234, 139–150. [Google Scholar] [CrossRef]
- Datlinger, F.; Datlinger, A.; Pollreisz, A.; Sacu, S.; Schmidt-Erfurth, U.; Datlinger, P. Intraprocedural OCT monitoring of the immediate treatment response during indocyanine green angiography-guided laser therapy of teleangiectatic capillaries in diabetic macular edema. Sci. Rep. 2022, 12, 2315. [Google Scholar] [CrossRef]
- Roh, H.C.; Lee, C.; Kang, S.W.; Choi, K.J.; Eun, J.S.; Hwang, S. Infrared reflectance image-guided laser photocoagulation of telangiectatic capillaries in persistent diabetic macular edema. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmology 1995, 102, 1425–1433. [CrossRef] [PubMed]
- Elman, M.J.; Ayala, A.; Bressler, N.M.; Browning, D.; Flaxel, C.J.; Glassman, A.R.; Jampol, L.M.; Stone, T.W. Intravitreal Ranibizumab for Diabetic Macular Edema with Prompt versus Deferred Laser Treatment: 5-Year Randomized Trial Results. Ophthalmology 2014, 122, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Holz, F.G.; Boyer, D.S.; Midena, E.; Heier, J.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal Aflibercept for Diabetic Macular Edema. Ophthalmology 2015, 122, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.; Wong, T.Y. Diabetic Macular Edema Treatment Guideline Working Group Management Paradigms for Diabetic Macular Edema. Am. J. Ophthalmol. 2013, 157, 505–513.e8. [Google Scholar] [CrossRef]
- Glanville, J.; Patterson, J.; McCool, R.; Ferreira, A.; Gairy, K.; Pearce, I. Efficacy and safety of widely used treatments for macular oedema secondary to retinal vein occlusion: A systematic review. BMC Ophthalmol. 2014, 14, 7. [Google Scholar] [CrossRef]
- Amoroso, F.; Pedinielli, A.; Colantuono, D.; Jung, C.; Capuano, V.; Souied, E.H.; Miere, A. Selective Photocoagulation of Capillary Macroaneurysms by Navigated Focal Laser. Ophthalmic Surg. Lasers Imaging Retin. 2021, 52, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Na Lee, S.; Chhablani, J.; Chan, C.K.; Wang, H.; Barteselli, G.; El-Emam, S.; Gomez, M.L.; Kozak, I.; Cheng, L.; Freeman, W.R. Characterization of Microaneurysm Closure After Focal Laser Photocoagulation in Diabetic Macular Edema. Am. J. Ophthalmol. 2013, 155, 905–912.e2. [Google Scholar] [CrossRef] [Green Version]
- Inagaki, K.; Ohkoshi, K.; Ohde, S.; Deshpande, G.A.; Ebihara, N.; Murakami, A. Comparative efficacy of pure yellow (577-nm) and 810-nm subthreshold micropulse laser photocoagulation combined with yellow (561–577-nm) direct photocoagulation for diabetic macular edema. Jpn. J. Ophthalmol. 2014, 59, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Gatti, V.; Muraca, A.; Brambilla, M.; Villani, E.; Nucci, P.; Rossetti, L.; De Cilla, S. Optical coherence tomography angiography changes after subthreshold micropulse yellow laser in diabetic macular edema. Retina 2020, 40, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Starr, M.R.; Salabati, M.; Mahmoudzadeh, R.; Patel, L.G.; Ammar, M.J.; Hsu, J.; Garg, S.; Ho, A.C.; Kuriyan, A.E. Fluctuations in Central Subfield Thickness Associated With Worse Visual Outcomes in Patients With Diabetic Macular Edema in Clinical Trial Setting. Am. J. Ophthalmol. 2021, 232, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Gibbons, A.; Smiddy, W.E. Cost-Utility of Anti–Vascular Endothelial Growth Factor Treatment for Macular Edema Secondary to Central Retinal Vein Occlusion. Ophthalmol. Retin. 2020, 5, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Curry, B.A.; Sanfilippo, P.G.; Chan, S.; Hewitt, A.W.; Verma, N. Clinical Outcomes of a Treat and Extend Regimen with Intravitreal Aflibercept Injections in Patients with Diabetic Macular Edema: Experience in Clinical Practice. Ophthalmol. Ther. 2020, 9, 87–101. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) or Mean ± SD |
|---|---|
| Female gender | 33 (43.4%) |
| Age, years | 70.8 ± 11.2 |
| Cause of macular edema | |
| Diabetes | 62 (66.6%) |
| RVO | 9 (9.7%) |
| BRVO | 22 (23.7%) |
| Duration of macular edema | 23.9 ± 11 |
| Capillary macroaneurysms | |
| Number (mean) | 1.97 ± 1.11 |
| Largest size (mean), µm | 172 ± 52 |
| Distance to the fovea (mean), µm | 1690 ± 664 |
| Intravitreal injections | |
| Number in the last 6 months (mean) | 2.52 ± 1.43 |
| Number in the last 12 months (mean) | 4.44 ± 2.44 |
| Anti-VEGF agent | 37 (39.8%) |
| Dexamethasone implant | 39 (41.9%) |
| Both | 17 (18.3%) |
| SD-OCT findings | |
| Foveal thickness (mean), µm | 354 (114) |
| Focal edema thickness (mean), µm | 462 (92.7) |
| Primary Outcome | 6 Months before Photocoagulation | 6 Months after Photocoagulation | p | 12 Months before Photocoagulation | 12 Months after Photocoagulation | p |
|---|---|---|---|---|---|---|
| Mean number of injections | 2.52 | 1.52 | <0.001 | 4.44 | 2.95 | <0.001 |
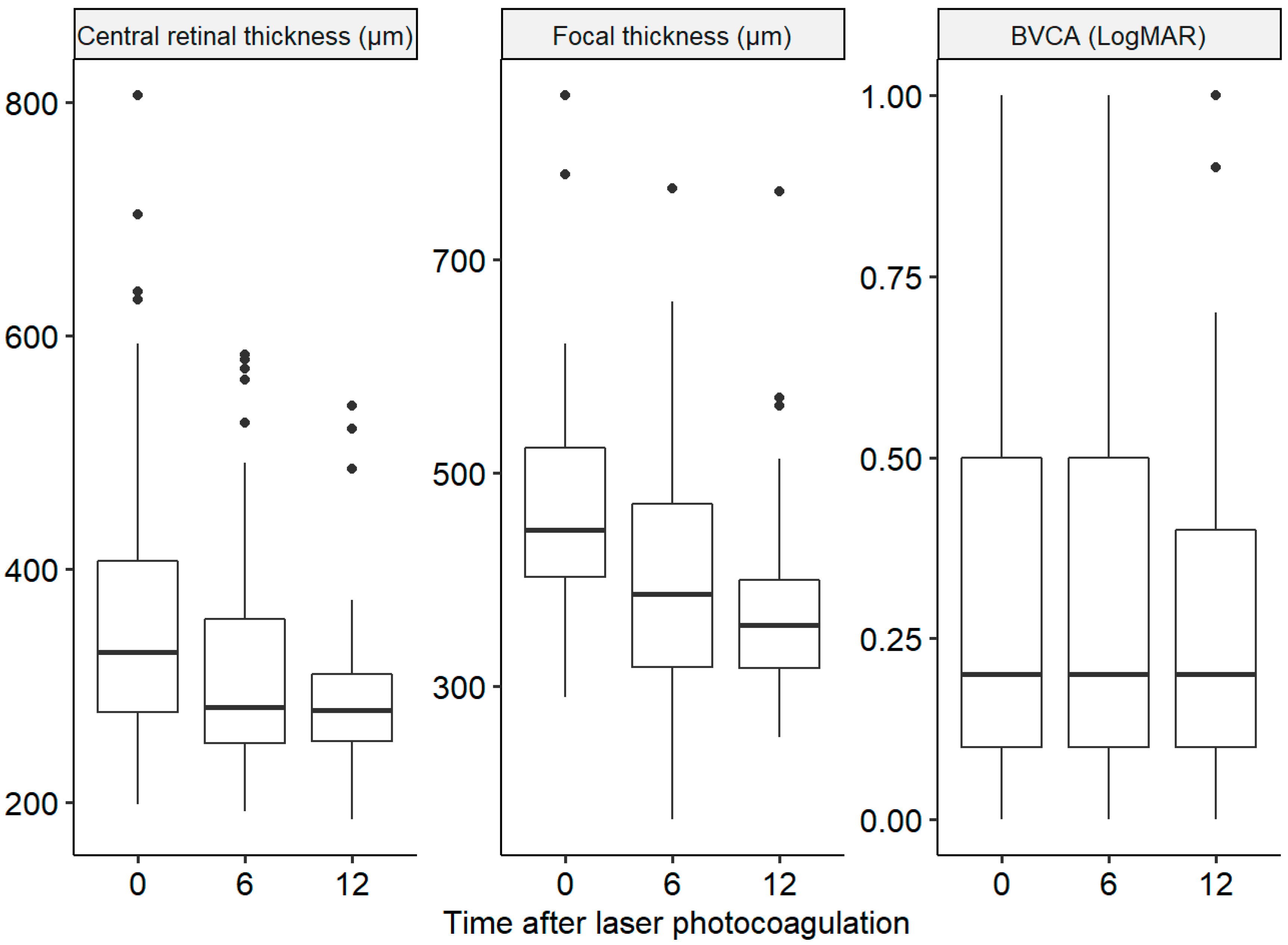
| Secondary outcomes | Baseline | 6 Months after Photocoagulation | p | 12 Months after Photocoagulation | p | |
| Mean best-corrected visual acuity (LogMAR) | 0.32 | 0.31 | 0.95 | 0.30 | 0.16 | |
| Mean foveal thickness (µm) | 354 | 314 | <0.001 | 299 | <0.001 | |
| Mean focal thickness (µm) | 462 | 400 | <0.001 | 399 | <0.001 | |
| Anti-VEGF | ||||||
|---|---|---|---|---|---|---|
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 3.62 | 1.90 | <0.001 | 6.19 | 3.70 | <0.001 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (LogMAR) | 0.22 | 0.25 | 0.35 | 0.24 | 0.80 | |
| Mean foveal thickness (µm) | 301 | 283 | 0.04 | 273 | <0.01 | |
|
Mean focal thickness (µm) | 416 | 358 | <0.01 | 358 | <0.01 | |
| Dexamethasone implant | ||||||
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 1.69 | 1.26 | 0.02 | 3.05 | 2.42 | 0.02 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (LogMAR) | 0.47 | 0.41 | 0.08 | 0.39 | 0.11 | |
| Mean foveal thickness (µm) | 403 | 336 | <0.01 | 317 | <0.01 | |
| Mean focal thickness (µm) | 492 | 427 | <0.01 | 425 | <0.01 | |
| CMA > 150 µm | ||||||
|---|---|---|---|---|---|---|
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 2.30 | 1.40 | <0.001 | 4.05 | 2.84 | <0.01 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (logMAR) | 0.36 | 0.34 | 0.97 | 0.33 | 0.16 | |
| Mean foveal thickness (µm) | 373 | 317 | <0.01 | 309 | <0.01 | |
| Mean focal thickness (µm) | 474 | 401 | <0.01 | 402 | <0.01 | |
| CMA < 150 µm | ||||||
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 2.91 | 1.73 | <0.01 | 5.15 | 3.13 | <0.01 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (logMAR) | 0.26 | 0.26 | 0.95 | 0.25 | 0.60 | |
| Mean foveal thickness (µm) | 319 | 306 | 0.34 | 280 | 0.002 | |
| Mean focal thickness (µm) | 441 | 397 | <0.01 | 395 | <0.01 | |
| Diabetes | ||||||
|---|---|---|---|---|---|---|
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 2.52 | 1.53 | <0.01 | 4.37 | 3.15 | <0.01 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (logMAR) | 0.32 | 0.30 | 0.73 | 0.28 | 0.06 | |
| Mean foveal thickness (µm) | 360 | 319 | <0.01 | 299 | <0.01 | |
| Mean focal thickness (µm) | 476 | 415 | <0.01 | 413 | <0.01 | |
| RVO | ||||||
| 6 months before photocoagulation | 6 months after photocoagulation | p | 12 months before photocoagulation | 12 months after photocoagulation | p | |
| Mean number of injections | 2.51 | 1.48 | <0.01 | 4.58 | 2.59 | <0.01 |
| Baseline | 6 months after photocoagulation | p | 12 months after photocoagulation | p | ||
| Mean BCVA (logMAR) | 0.33 | 0.33 | 0.70 | 0.33 | 0.68 | |
| Mean foveal thickness (µm) | 342 | 302 | 0.02 | 298 | <0.01 | |
| Mean focal thickness (µm) | 436 | 371 | 0.02 | 373 | <0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Séjournet, L.; Kodjikian, L.; Elbany, S.; Allignet, B.; Agard, E.; Chaperon, M.; Billant, J.; Denis, P.; Mathis, T.; Burillon, C.; et al. Focal Photocoagulation as an Adjunctive Therapy to Reduce the Burden of Intravitreal Injections in Macula Edema Patients, the LyoMAC2 Study. Pharmaceutics 2023, 15, 308. https://doi.org/10.3390/pharmaceutics15020308
Séjournet L, Kodjikian L, Elbany S, Allignet B, Agard E, Chaperon M, Billant J, Denis P, Mathis T, Burillon C, et al. Focal Photocoagulation as an Adjunctive Therapy to Reduce the Burden of Intravitreal Injections in Macula Edema Patients, the LyoMAC2 Study. Pharmaceutics. 2023; 15(2):308. https://doi.org/10.3390/pharmaceutics15020308
Chicago/Turabian StyleSéjournet, Lucas, Laurent Kodjikian, Sandra Elbany, Benoit Allignet, Emilie Agard, Mayeul Chaperon, Jérémy Billant, Philippe Denis, Thibaud Mathis, Carole Burillon, and et al. 2023. "Focal Photocoagulation as an Adjunctive Therapy to Reduce the Burden of Intravitreal Injections in Macula Edema Patients, the LyoMAC2 Study" Pharmaceutics 15, no. 2: 308. https://doi.org/10.3390/pharmaceutics15020308