
In Silico Quantification of Intersubject Variability on Aerosol Deposition in the Oral Airway

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. CT Database and Subject Characteristics
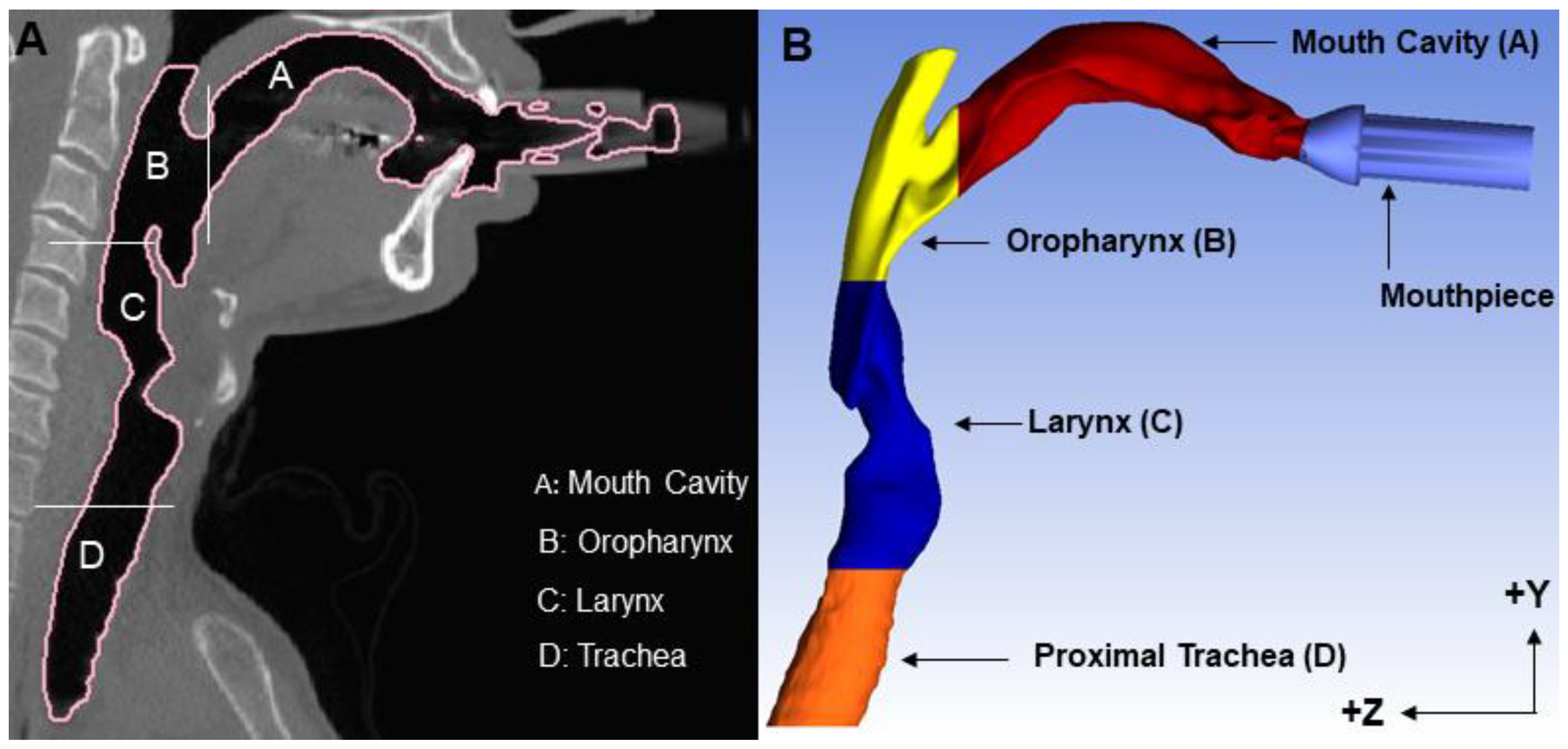
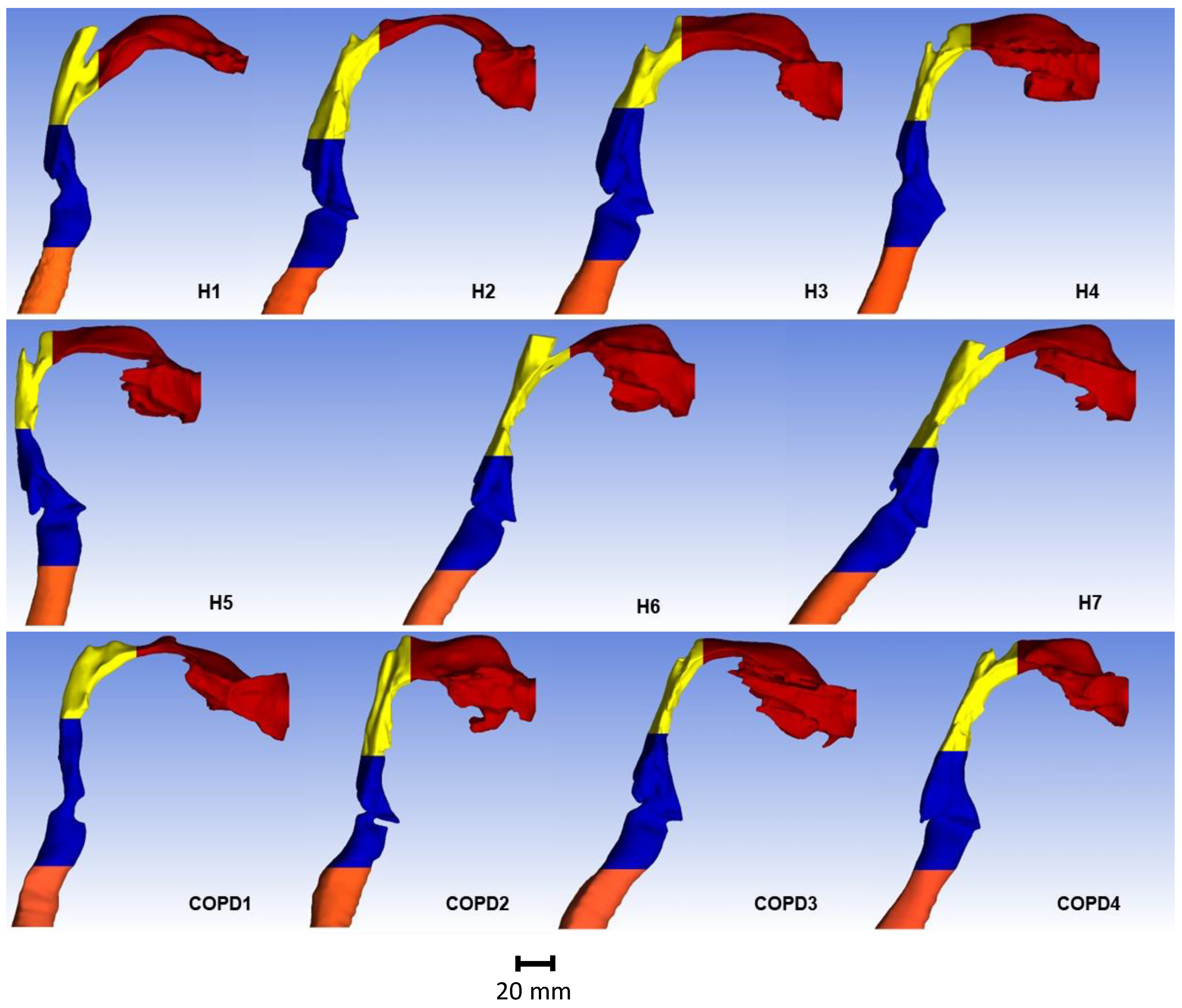
2.2. Reconstruction of Human Upper Airway Geometries
2.3. Computational Fluid-Particle Dynamics (CFPD) Simulations
2.3.1. Flow Simulations
2.3.2. Particle Transport Simulations
2.4. Comparison of Subject-Specific In Silico Predictions with Experimental Results
2.5. Statistical Analysis
3. Results
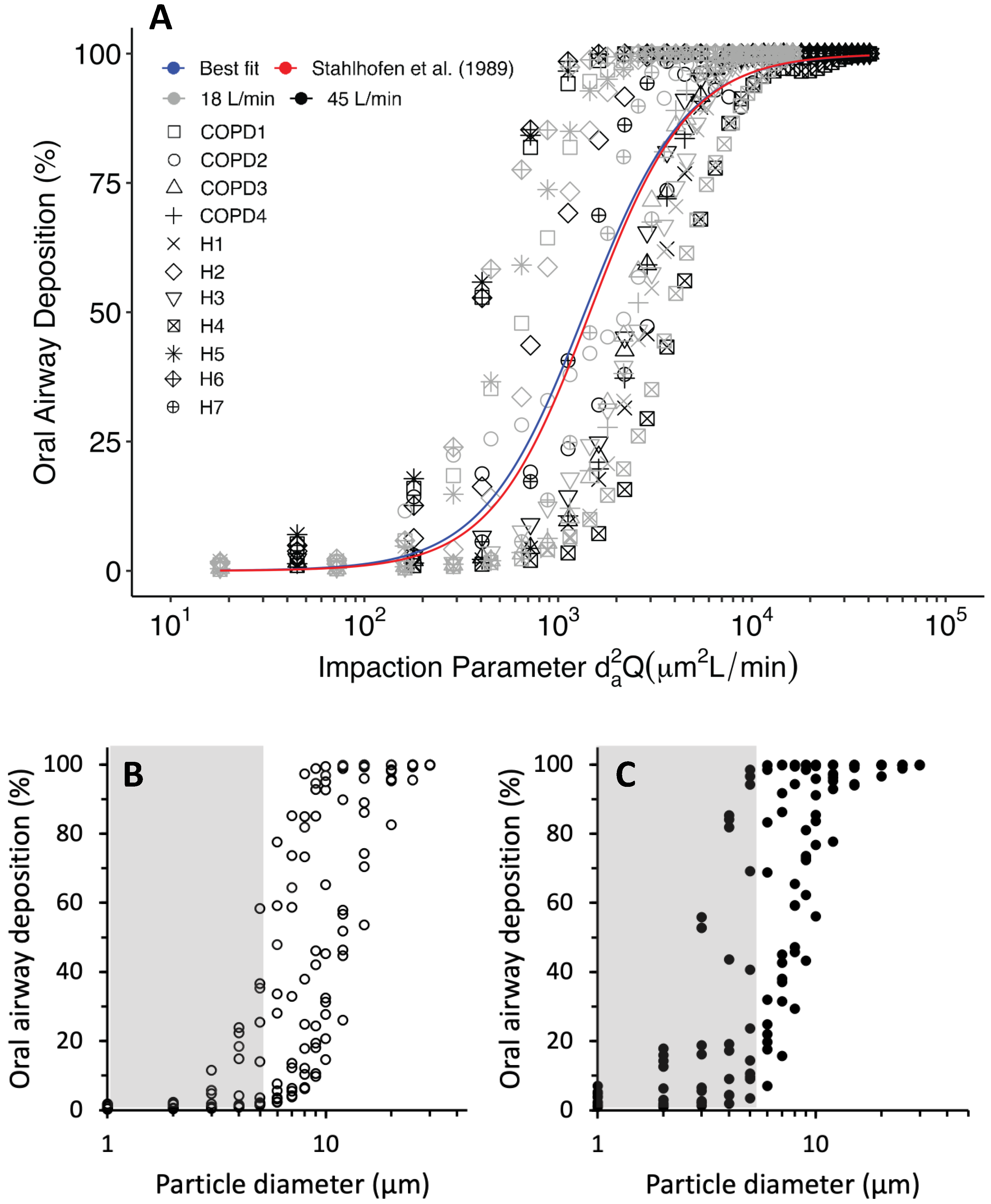
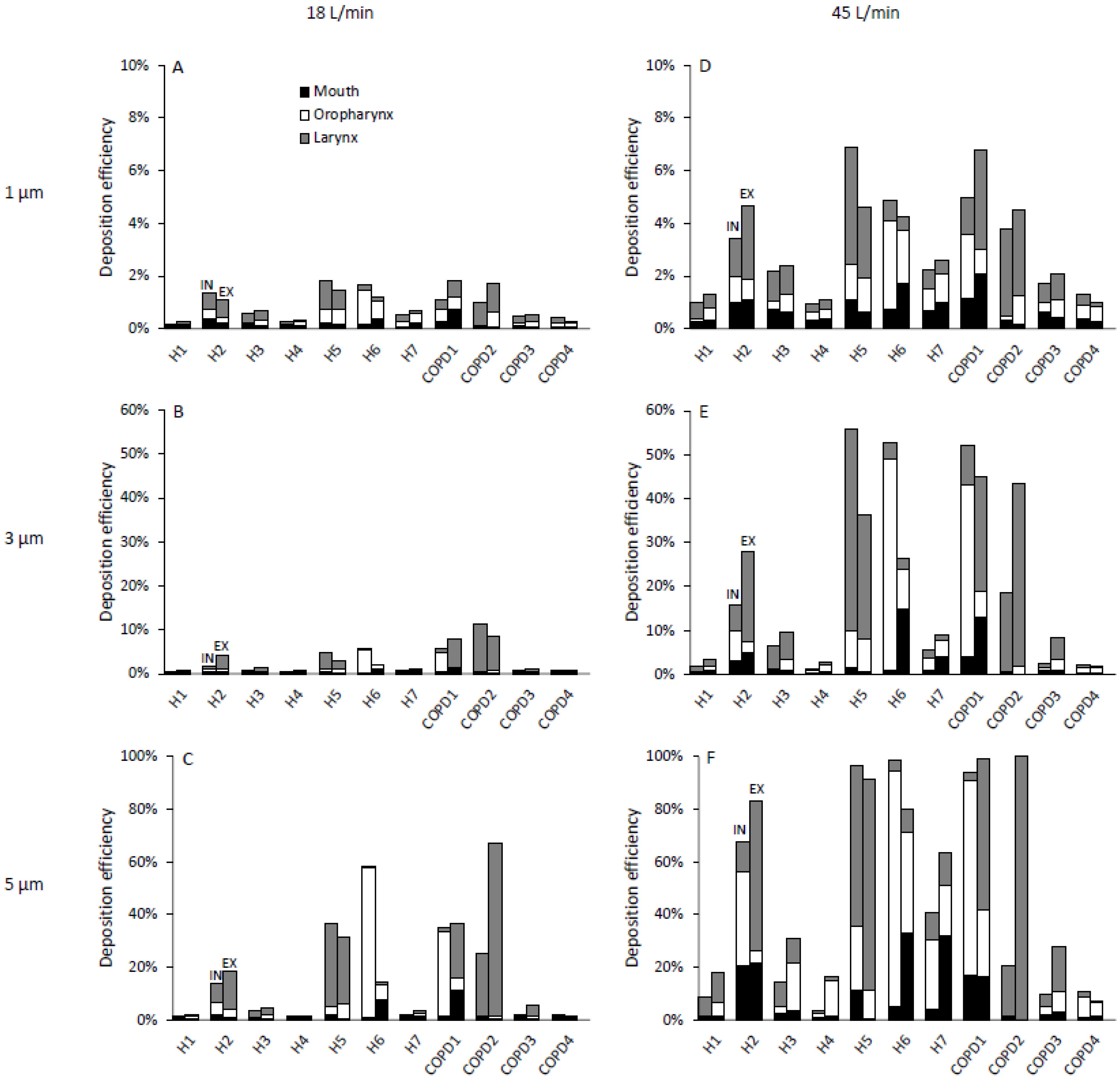
3.1. Total Oral Deposition Efficiency
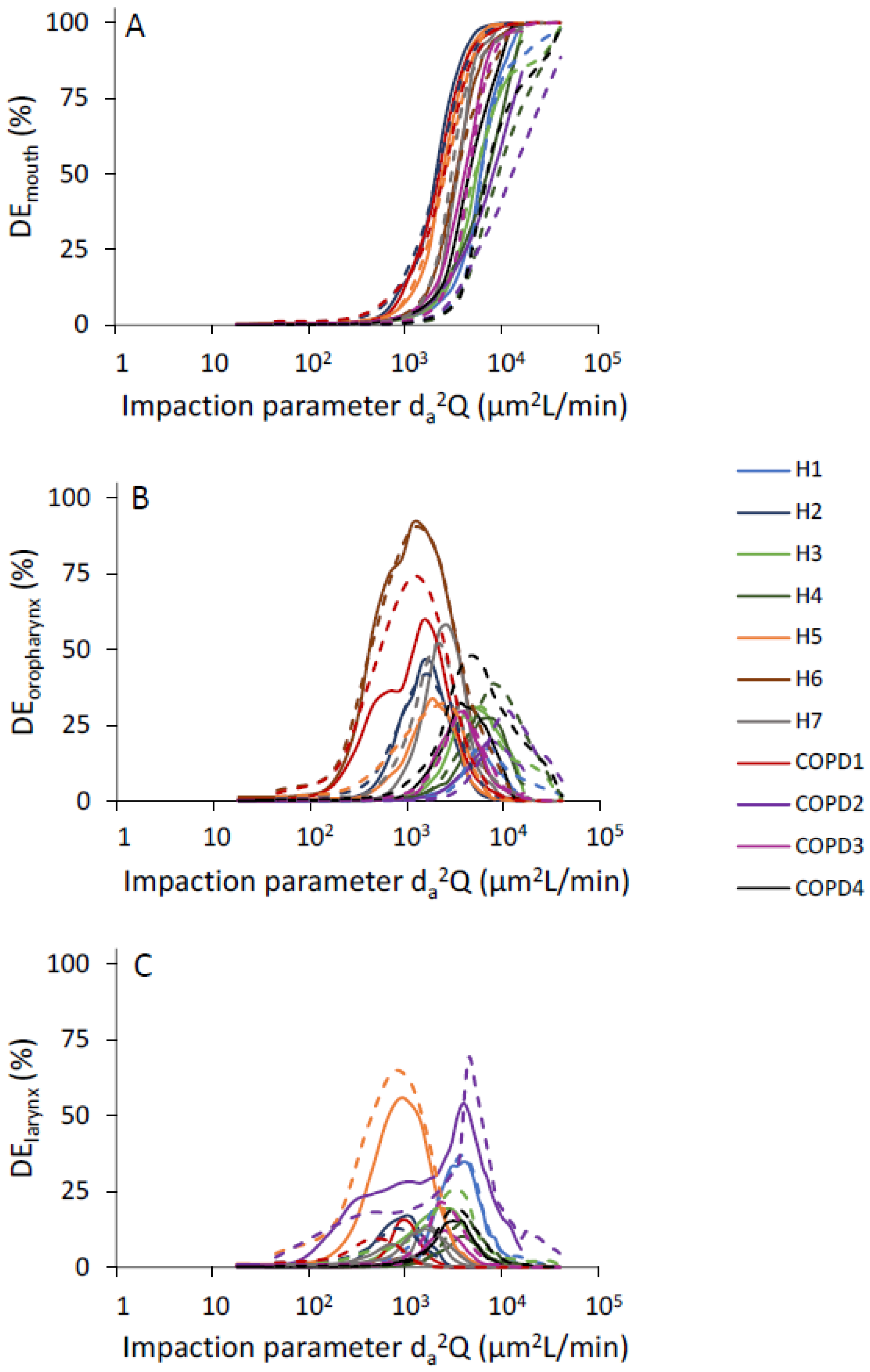
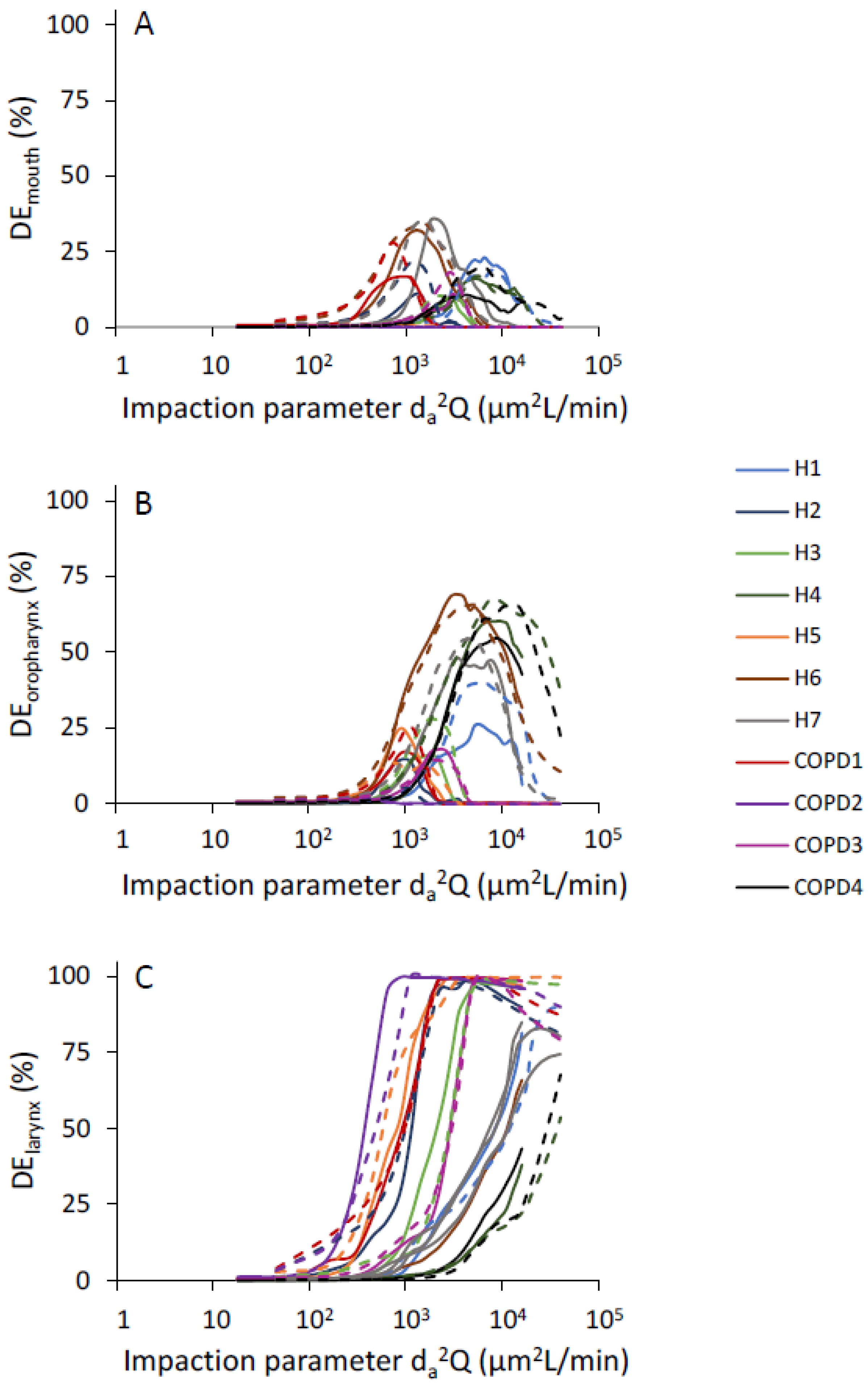
3.2. Effect of Particle Impaction on Regional Deposition
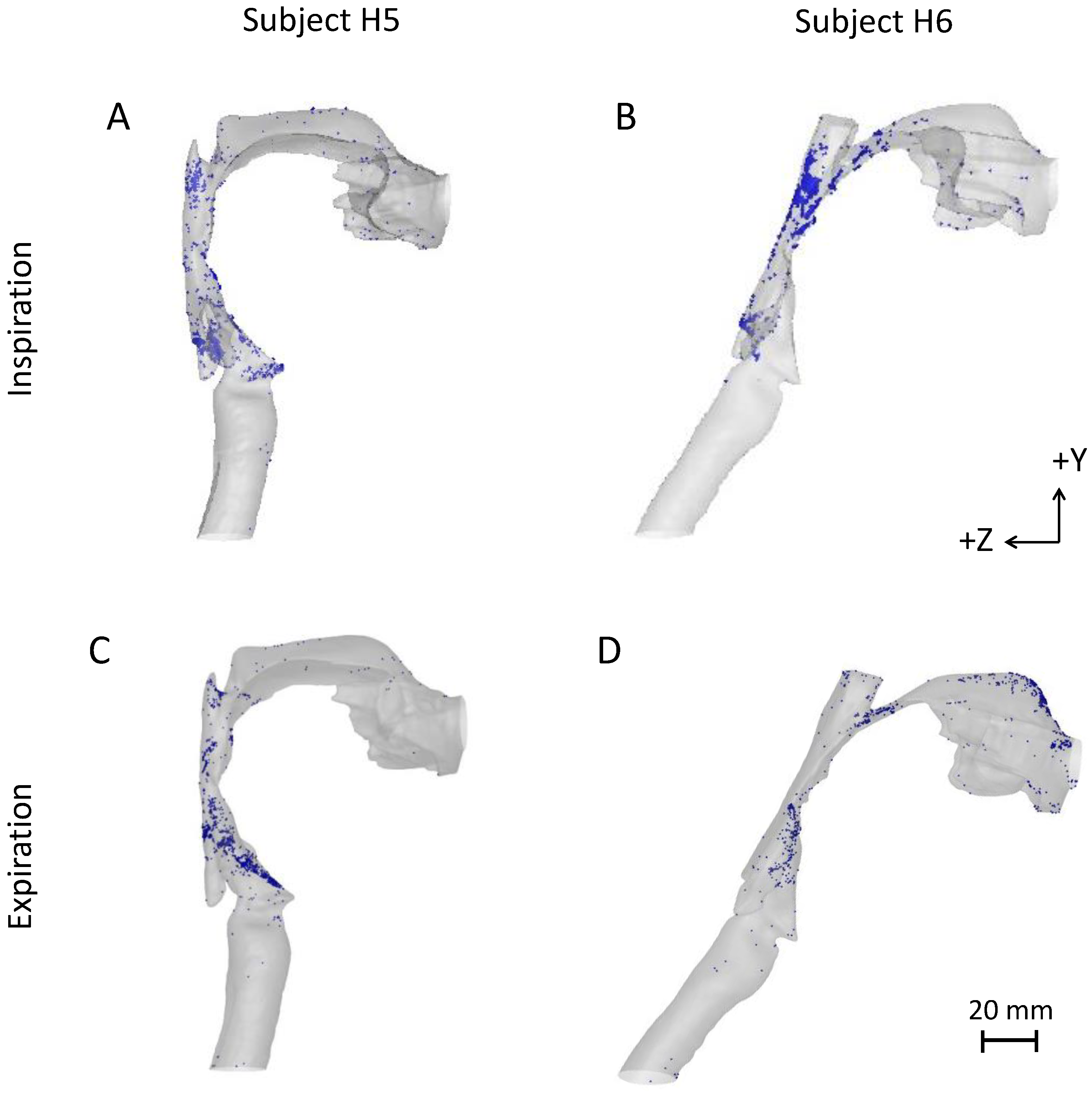
3.3. Comparison of Inspiratory and Expiratory Particle Deposition in the Upper Airway
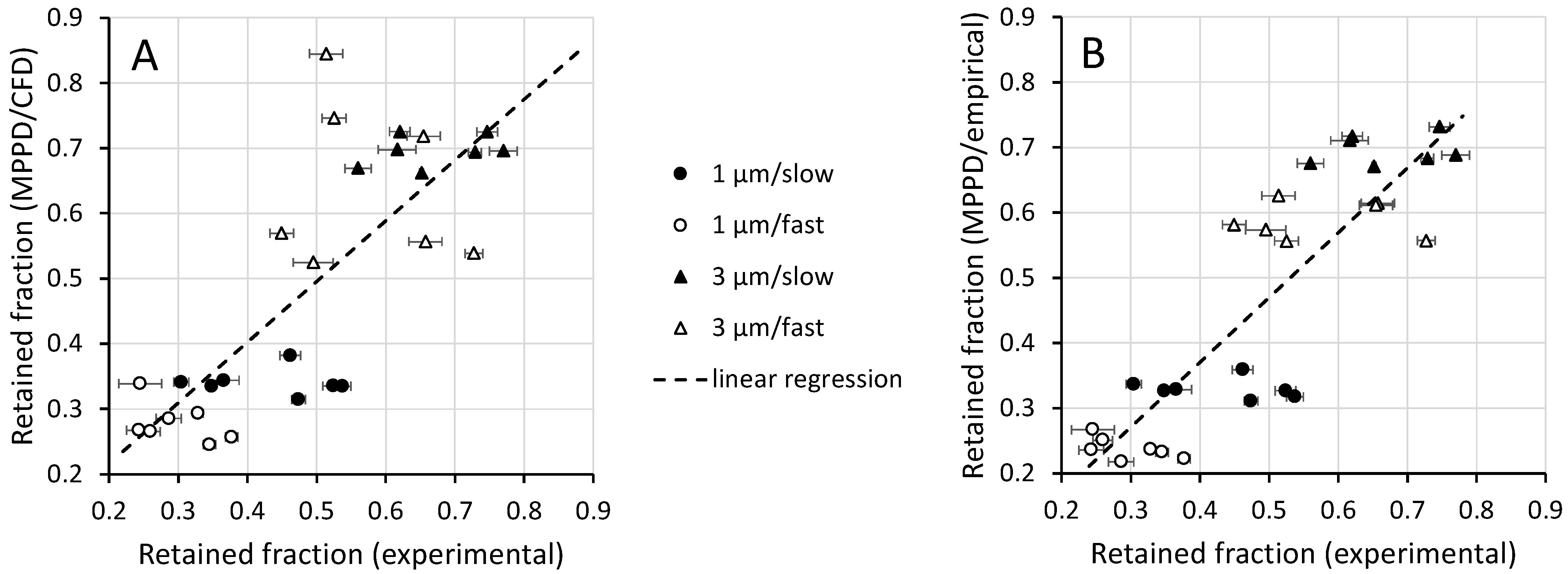
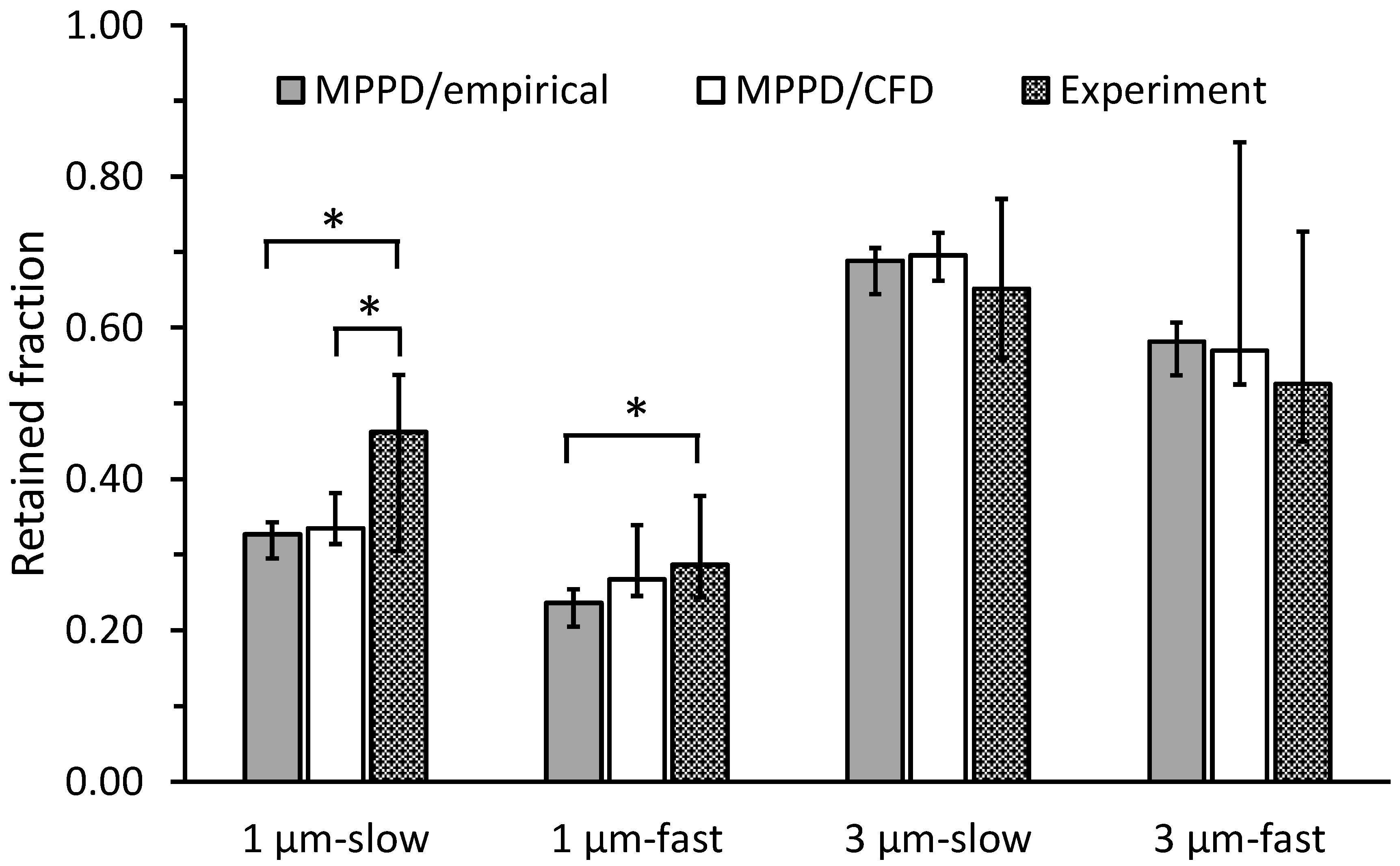
3.4. Comparison of In Silico Predictions with In Vivo Experimental Data
4. Discussion
4.1. Intersubject Variability in Deposition in the Oral Airway
4.2. Differences in Regional Deposition between Inhalation and Exhalation
4.3. Comparison of Whole-Lung Deposition with Experiments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Individual Geometries


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject ID | Volume (cm³) | Surface Area (cm²) |
|---|---|---|
| H1 | 73.70 | 188.18 |
| H2 | 65.32 | 178.55 |
| H3 | 63.88 | 179.94 |
| H4 | 96.34 | 210.22 |
| H5 | 67.92 | 193.32 |
| H6 | 72.51 | 200.18 |
| H7 | 61.28 | 192.96 |
| COPD1 | 52.86 | 149.79 |
| COPD2 | 126.83 | 254.02 |
| COPD3 | 85.53 | 243.09 |
| COPD4 | 87.40 | 220.84 |
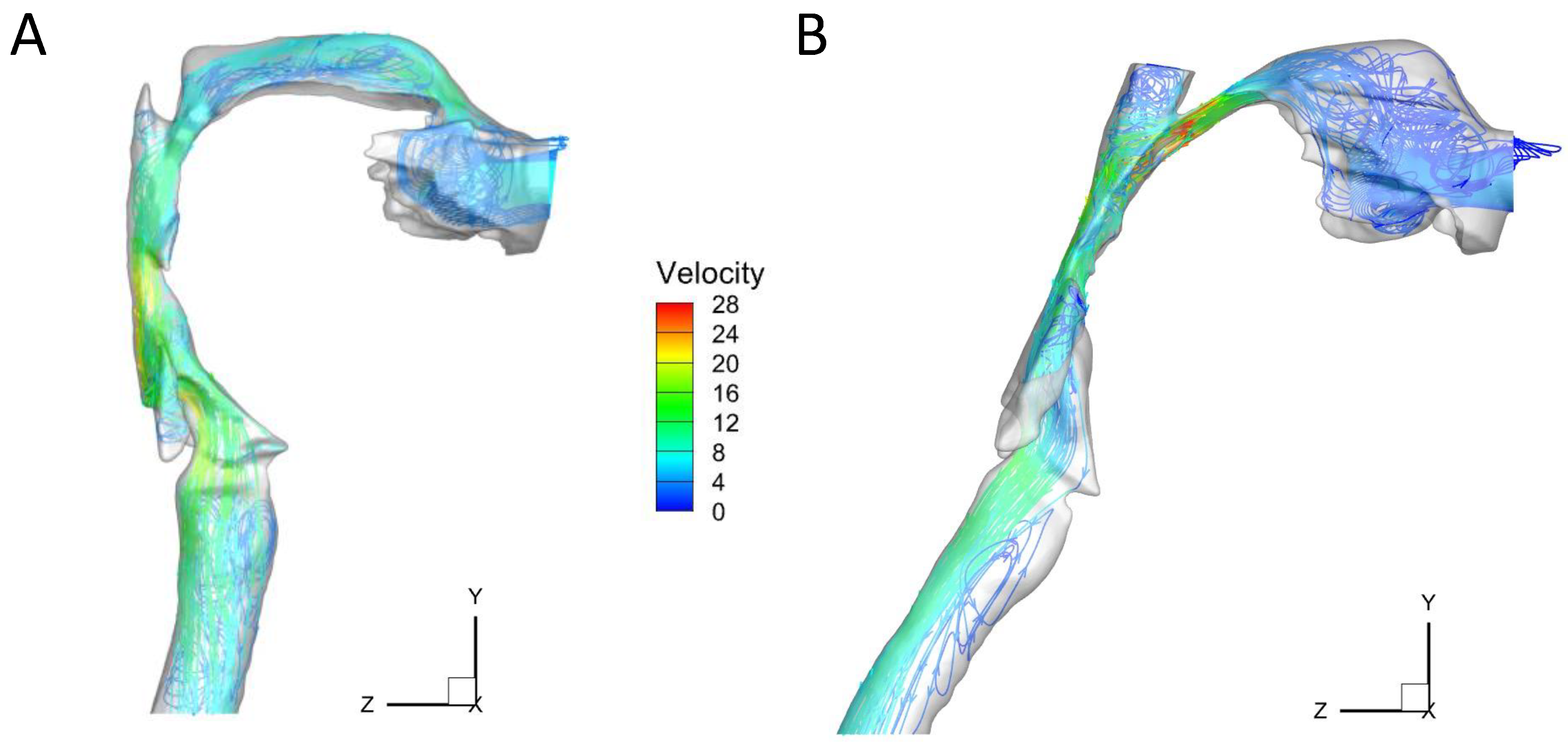
Appendix B. Flow Patterns

References
- Finlay, W.H. The Mechanics of Inhaled Pharmaceutical Aerosols: An Introduction; Academic Press: Amsterdam, NL, USA, 2001. [Google Scholar]
- Feng, Y.; Zhao, J.; Kleinstreuer, C.; Wang, Q.; Wang, J.; Wu, D.H.; Lin, J. An in silico inter-subject variability study of extra-thoracic morphology effects on inhaled particle transport and deposition. J. Aerosol Sci. 2018, 123, 185–207. [Google Scholar] [CrossRef]
- Borgstrom, L.; Olsson, B.; Thorsson, L. Degree of Throat Deposition Can Explain Variability in Lung Deposition of Inhaled Drugs. J. Aerosol Med. 2006, 19, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Byron, P.R.; Hindle, M.; Lange, C.F.; Longest, P.W.; McRobbie, D.; Oldham, M.J.; Olsson, B.; Thiel, C.; Wachtel, H.; Finlay, W.H. In Vivo-in Vitro Correlations: Predicting Pulmonary Drug Deposition from Pharmaceutical Aerosols. J. Aerosol Med. Pulm. Drug Deliv. 2010, 23, S59–S69. [Google Scholar] [CrossRef] [PubMed]
- Vinchurkar, S.; De Backer, L.; Vos, W.; Van Holsbeke, C.; De Backer, J.; De Backer, W. A Case Series on Lung Deposition Analysis of Inhaled Medication Using Functional Imaging Based Computational Fluid Dynamics in Asthmatic Patients: Effect of Upper Airway Morphology and Comparison with in-Vivo Data. Inhal. Toxicol. 2012, 24, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Holbrook, L.T. In silico models of aerosol delivery to the respiratory tract—Development and applications. Adv. Drug Deliv. Rev. 2012, 64, 296–311. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.S. Aerosol Deposition in the Extrathoracic Region. Aerosol Sci. Technol. 2003, 37, 659–671. [Google Scholar] [CrossRef] [Green Version]
- Grgic, B.; Finlay, W.H.; Burnell, P.K.P.; Heenan, A.F. In vitro intersubject and intrasubject deposition measurements in realistic mouth-throat geometries. J. Aerosol. Sci. 2004, 35, 1025–1040. [Google Scholar] [CrossRef]
- Golshahi, L.; Noga, M.L.; Vehring, R.; Finlay, W.H. An In vitro Study on the Deposition of Micrometer-Sized Particles in the Extrathoracic Airways of Adults During Tidal Oral Breathing. Ann. Biomed. Eng. 2013, 41, 979–989. [Google Scholar] [CrossRef]
- Cheng, Y.-S.; Zhou, Y.; Chen, B.T. Particle Deposition in a Cast of Human Oral Airways. Aerosol Sci. Technol. 1999, 31, 286–300. [Google Scholar] [CrossRef]
- Cheng, K.-H.; Cheng, Y.-S.; Yeh, H.-C.; Swift, D.L. Measurements of Airway Dimensions and Calculation of Mass Transfer Characteristics of the Human Oral Passage. J. Biomech. Eng. 1997, 119, 476–482. [Google Scholar] [CrossRef]
- Gallivan, G.J.; Gallivan, K.H.; Gallivan, H.K. Inhaled corticosteroids: Hazardous effects on voice—an update. J. Voice 2007, 21, 101–111. [Google Scholar] [CrossRef]
- DelGaudio, J.M. Steroid inhaler laryngitis: Dysphonia caused by inhaled fluticasone therapy. Arch. Otolaryngol.-Head Neck Surg. 2002, 128, 677–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xi, J.; Yang, T.; Talaat, K.; Wen, T.; Zhang, Y.; Klozik, S.; Peters, S. Visualization of local deposition of nebulized aerosols in a human upper respiratory tract model. J. Vis. 2018, 21, 225–237. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, J.; Hayati, H.; Sperry, T.; Yi, H. Tutorial: Understanding the transport, deposition, and translocation of particles in human respiratory systems using Computational Fluid-Particle Dynamics and Physiologically Based Toxicokinetic models. J. Aerosol Sci. 2021, 151, 105672. [Google Scholar] [CrossRef]
- Wedel, J.; Steinmann, P.; Štrakl, M.; Hriberšek, M.; Ravnik, J. Can CFD establish a connection to a milder COVID-19 disease in younger people? Aerosol deposition in lungs of different age groups based on Lagrangian particle tracking in turbulent flow. Comput. Mech. 2021, 67, 1497–1513. [Google Scholar] [CrossRef] [PubMed]
- Tian, G.; Longest, P.W.; Su, G.; Walenga, R.L.; Hindle, M. Development of a stochastic individual path (SIP) model for predicting the tracheobronchial deposition of pharmaceutical aerosols: Effects of transient inhalation and sampling the airways. J. Aerosol Sci. 2011, 42, 781–799. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Kim, C. Micro-particle transport and deposition in a human oral airway model. J. Aerosol Sci. 2002, 33, 1635–1652. [Google Scholar] [CrossRef]
- Schroeter, J.D.; Garcia, G.J.; Kimbell, J.S. Effects of surface smoothness on inertial particle deposition in human nasal models. J. Aerosol Sci. 2011, 42, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Darquenne, C.; Lamm, W.J.; Fine, J.M.; Corley, R.A.; Glenny, R.W. Total and regional deposition of inhaled aerosols in supine healthy subjects and subjects with mild-to-moderate COPD. J. Aerosol Sci. 2016, 99, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Tracy, L.F.; Basu, S.; Shah, P.V.; Frank-Ito, D.O.; Das, S.; Zanation, A.M.; Kimbell, J.S. Impact of endoscopic craniofacial resection on simulated nasal airflow and heat transport. Int. Forum Allergy Rhinol. 2019, 9, 900–909. [Google Scholar] [CrossRef]
- Borojeni, A.A.; Garcia, G.J.; Moghaddam, M.G.; Frank-Ito, D.O.; Kimbell, J.S.; Laud, P.W.; Koenig, L.J.; Rhee, J.S. Normative ranges of nasal airflow variables in healthy adults. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Elghobashi, S. On predicting particle-laden turbulent flows. Appl. Sci. Res. 1994, 52, 309–329. [Google Scholar] [CrossRef]
- Frank-Ito, D.O.; Wofford, M.; Schroeter, J.D.; Kimbell, J.S. Influence of Mesh Density on Airflow and Particle Deposition in Sinonasal Airway Modeling. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Jiang, J.; Dong, H.; Zhao, K. Computational modeling and validation of human nasal airflow under various breathing conditions. J. Biomech. 2017, 64, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Prasad, A.K.; Wexler, A.S. Detailed flow patterns in the nasal cavity. J. Appl. Physiol. 2000, 89, 323–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menter, F.R. Two-equation eddy-viscosity turbulence models for engineering applications. AIAA J. 1994, 32, 1598–1605. [Google Scholar] [CrossRef] [Green Version]
- Frank-Ito, D.O.; Cohen, S.M. Orally inhaled drug particle transport in computerized models of laryngotracheal stenosis. Otolaryngol.-Head Neck Surg. 2021, 164, 829–840. [Google Scholar] [CrossRef]
- Gosman, R.E.; Sicard, R.M.; Cohen, S.M.; Frank-Ito, D.O. Comparison of Inhaled Drug Delivery in Patients With One- and Two-level Laryngotracheal Stenosis. Laryngoscope, 2022; Online ahead of print. [Google Scholar]
- Asgharian, B.; Price, O.; Borojeni, A.A.T.; Kuprat, A.P.; Colby, S.; Singh, R.K.; Gu, W.; Corley, R.A.; Darquenne, C. Influence of alveolar mixing and multiple breaths of aerosol intake on particle deposition in the human lungs. J. Aerosol Sci. 2022, 166, 106050. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Rudolf, G.; James, A.C. Intercomparison of experimental regional aerosol deposition data. J. Aerosol Med. 1989, 2, 285–308. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W. Transport and deposition of micro-aerosols in realistic and simplified models of the oral airway. Ann. Biomed. Eng. 2007, 35, 560–581. [Google Scholar] [CrossRef]
- Bennett, W.D. Effect of Respiratory Tract Disease on Particle Deposition. J. Aerosol Med. Pulm. Drug Deliv. 2021, 34, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Darquenne, C. Aerosol deposition in health and disease. J. Aerosol Med. Pulm. Drug Deliv. 2012, 25, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.L.; Lippmann, M. Experimental measurement and empirical modeling of the regional deposition of inhaled particles in humans. Am. Ind. Hyg. Assoc. J. 1980, 41, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M. Regional deposition of particles in the human respiratory tract. In Handbook of Physiology; Lee, D.H.K., Falk, H.L., Murphy, S.D., Geiger, S.R., Eds.; American Physiological Society: Bethesda, MD, USA, 1976; Volume 9, pp. 213–232. [Google Scholar]
- Foord, N.; Black, A.; Walsh, M. Regional deposition of 2.5–7.5 µm diameter inhaled particles in healthy male non-smokers. J. Aerosol Sci. 1978, 9, 343–357. [Google Scholar] [CrossRef]
- Emmett, P.; Aitken, R.; Hannan, W. Measurements of the total and regional deposition of inhaled particles in the human respiratory tract. J. Aerosol Sci. 1982, 13, 549–560. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Gebhart, J.; Heyder, J.; Scheuch, G. New regional deposition data of the human respiratory tract. J. Aerosol Sci. 1983, 14, 186–188. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Gebhart, J.; Heyder, J. Experimental determination of the regional deposition of aerosol particles in the human respiratory tract. Am. Ind. Hyg. Assoc. J. 1980, 41, 385–398. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Gebhart, J.; Heyder, J. Biological variability of regional deposition of aerosol particles in the human respiratory tract. Am. Ind. Hyg. Assoc. J. 1981, 42, 348–352. [Google Scholar] [CrossRef]
- Koullapis, P.G.; Nicolaou, L.; Kassinos, S.C. In silico assessment of mouth-throat effects on regional deposition in the upper tracheobronchial airways. J. Aerosol Sci. 2018, 117, 164–188. [Google Scholar] [CrossRef]
- Verbanck, S.; Kalsi, H.S.; Biddiscombe, M.F.; Agnihotri, V.; Belkassem, B.; Lacor, C.; Usmani, O.S. Inspiratory and expiratory aerosol deposition in the upper airway. Inhal. Toxicol. 2011, 23, 104–111. [Google Scholar] [CrossRef]
- Laube, B.L.; Janssens, H.M.; de Jongh, F.H.C.; Devadason, S.G.; Dhand, R.; Diot, P.; Everard, M.L.; Horvath, I.; Navalesi, P.; Voshaar, T.; et al. What the pulmonary specialist should know about the new inhalation therapies. Eur. Respir. J. 2011, 37, 1308–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, A.C.; Stahlhofen, W.; Rudolf, G.; Köbrich, R.; Briant, J.K.; Egan, M.J.; Nixon, W.; Birchall, A. Annexe D. Deposition of Inhaled Particles. Ann. ICRP 1994, 24, 231–299. [Google Scholar] [CrossRef]
- Li, J.T.; Reed, C.E. Proper use of aerosol corticosteroids to control asthma. Mayo Clin. Proc. 1989, 64, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Williamson, I.J.; Matusiewicz, S.P.; Brown, P.H.; Greening, A.P.; Crompton, G.K. Frequency of voice problems and cough in patients using pressurized aerosol inhaled steroid preparations. Eur. Respir. J. 1995, 8, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.J.; Gefter, W.B.; Pack, A.I.; Hoffman, E.A. Dynamic imaging of the upper airway during respiration in normal subjects. J. Appl. Physiol. 1993, 74, 1504–1514. [Google Scholar] [CrossRef]
- Darquenne, C.; Elliott, A.R.; Sibille, B.; Smales, E.T.; DeYoung, P.D.; Theilmann, R.J.; Malhotra, A. Upper airway dynamic imaging during tidal breathing in awake and asleep subjects with obstructive sleep apnea and healthy controls. Physiol. Rep. 2018, 6, e13711. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, T.; Kondo, R.; Horiguchi, T. A comparison of posterior pharyngeal wall areas between different tongue positions during inhalation. J. Allergy Clin. Immunol. Pract. 2019, 7, 743.e1–745.e1. [Google Scholar] [CrossRef]
- Horiguchi, T.; Kondo, R. Determination of the preferred tongue position for optimal inhaler use. J. Allergy Clin. Immunol. Pract. 2018, 6, 1039.e3–1041.e3. [Google Scholar] [CrossRef]
- Heenan, A.F.; Finlay, W.H.; Grgic, B.; Pollard, A.; Burnell, P.K.P. An investigation of the relationship between the flow field and regional deposition in realistic extra-thoracic airways. J. Aerosol Sci. 2004, 35, 1013–1023. [Google Scholar] [CrossRef]








| Subject ID | Age, Yr | Weight, kg | Height, cm | BMI | Health Status | FEV1, %pred | FEV1/FVC |
|---|---|---|---|---|---|---|---|
| H1 | 35 | 68.2 | 170 | 23.5 | Healthy | 113 | 0.88 |
| H2 | 52 | 96.8 | 165 | 35.5 | Healthy | 117 | 0.79 |
| H3 | 47 | 88.6 | 183 | 26.5 | Healthy | 85 | 0.74 |
| H4 | 26 | 91.8 | 183 | 27.5 | Healthy | 94 | 0.80 |
| H5 | 34 | 100.0 | 193 | 26.8 | Healthy | 104 | 0.84 |
| H6 | 21 | 54.1 | 168 | 19.2 | Healthy | 89 | 0.73 |
| H7 | 21 | 63.6 | 173 | 21.3 | Healthy | 95 | 0.81 |
| COPD1 | 57 | 70.0 | 164 | 26.1 | COPD | 60 | 0.56 |
| COPD2 | 55 | 65.9 | 178 | 20.8 | COPD | 56 | 0.48 |
| COPD3 | 45 | 83.2 | 180 | 25.6 | COPD | 69 | 0.67 |
| COPD4 | 54 | 83.6 | 187 | 24.0 | COPD | 58 | 0.52 |
| Subject | H1 | H2 | H3 | H4 | H5 | H6 | H7 | ||
|---|---|---|---|---|---|---|---|---|---|
| FRC (L) | 3.26 | 3.38 | 3.44 | 3.51 | 2.67 | 3.43 | 3.31 | ||
| dp = 1 µm | slow breathing | Qin (L/min) | 19.26 | 19.08 | 19.86 | 17.70 | 18.72 | 17.64 | 18.18 |
| Qex (L/min) | 20.94 | 19.32 | 20.10 | 18.24 | 18.66 | 17.82 | 17.76 | ||
| TV (L) | 1.116 | 1.073 | 1.101 | 0.979 | 1.041 | 0.984 | 1.009 | ||
| fast breathing | Qin (L/min) | 43.56 | 41.40 | 41.94 | 39.18 | 40.56 | 42.90 | 41.16 | |
| Qex (L/min) | 45.30 | 40.02 | 41.64 | 40.50 | 42.18 | 40.02 | 40.74 | ||
| TV (L) | 1.127 | 1.019 | 1.038 | 1.012 | 1.043 | 0.924 | 0.923 | ||
| dp = 2.9 µm | slow breathing | Qin (L/min) | 21.66 | 19.38 | 17.70 | 17.16 | 18.66 | 18.18 | 18.30 |
| Qex (L/min) | 23.16 | 18.96 | 17.94 | 17.70 | 18.00 | 19.26 | 19.14 | ||
| TV (L) | 1.254 | 1.064 | 0.987 | 0.972 | 1.023 | 1.043 | 1.249 | ||
| fast breathing | Qin (L/min) | 45.48 | 44.58 | 39.96 | 37.62 | 40.32 | 40.08 | 40.26 | |
| Qex (L/min) | 49.02 | 44.22 | 39.60 | 41.40 | 40.14 | 39.24 | 41.64 | ||
| TV (L) | 1.164 | 1.135 | 0.994 | 0.993 | 1.035 | 0.900 | 0.901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borojeni, A.A.T.; Gu, W.; Asgharian, B.; Price, O.; Kuprat, A.P.; Singh, R.K.; Colby, S.; Corley, R.A.; Darquenne, C. In Silico Quantification of Intersubject Variability on Aerosol Deposition in the Oral Airway. Pharmaceutics 2023, 15, 160. https://doi.org/10.3390/pharmaceutics15010160
Borojeni AAT, Gu W, Asgharian B, Price O, Kuprat AP, Singh RK, Colby S, Corley RA, Darquenne C. In Silico Quantification of Intersubject Variability on Aerosol Deposition in the Oral Airway. Pharmaceutics. 2023; 15(1):160. https://doi.org/10.3390/pharmaceutics15010160
Chicago/Turabian StyleBorojeni, Azadeh A. T., Wanjun Gu, Bahman Asgharian, Owen Price, Andrew P. Kuprat, Rajesh K. Singh, Sean Colby, Richard A. Corley, and Chantal Darquenne. 2023. "In Silico Quantification of Intersubject Variability on Aerosol Deposition in the Oral Airway" Pharmaceutics 15, no. 1: 160. https://doi.org/10.3390/pharmaceutics15010160