
Monitoring of Ex Vivo Cyclosporin a Activity in Healthy Volunteers Using T Cell Function Assays in Relation to Whole Blood and Cellular Pharmacokinetics
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Whole Blood and Intracellular PK
2.3. Whole Blood Culture and PD Assessments
2.4. Data Analysis
3. Results
3.1. Subject Characteristics and Safety
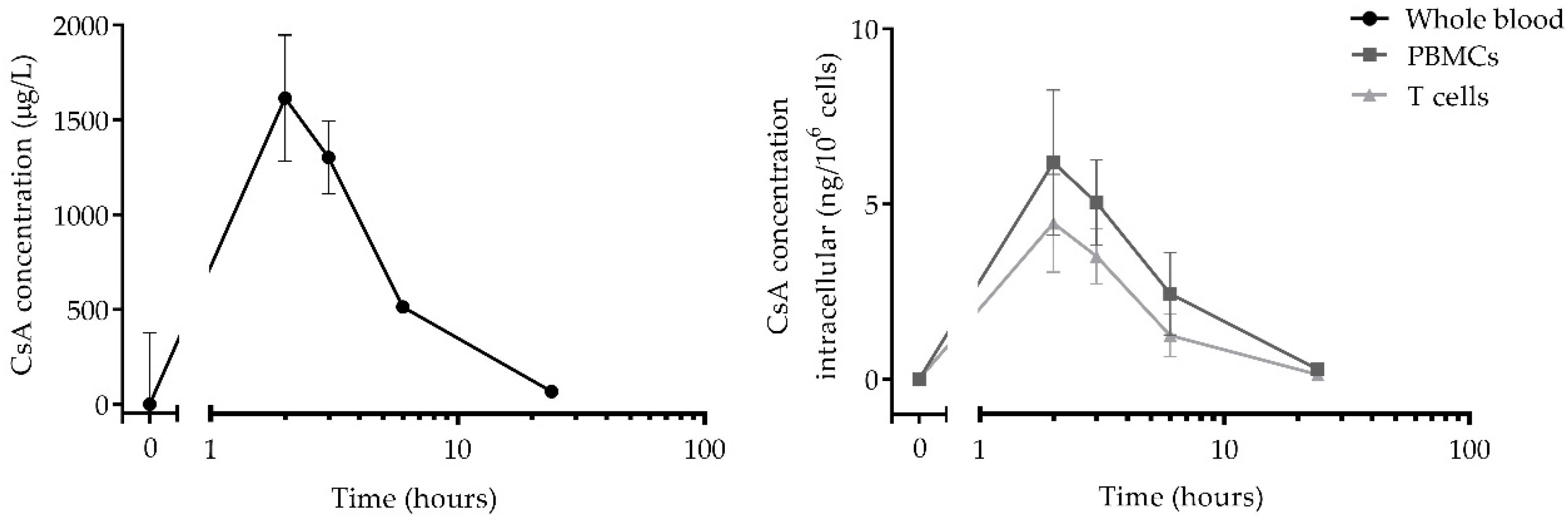
3.2. Pharmacokinetics
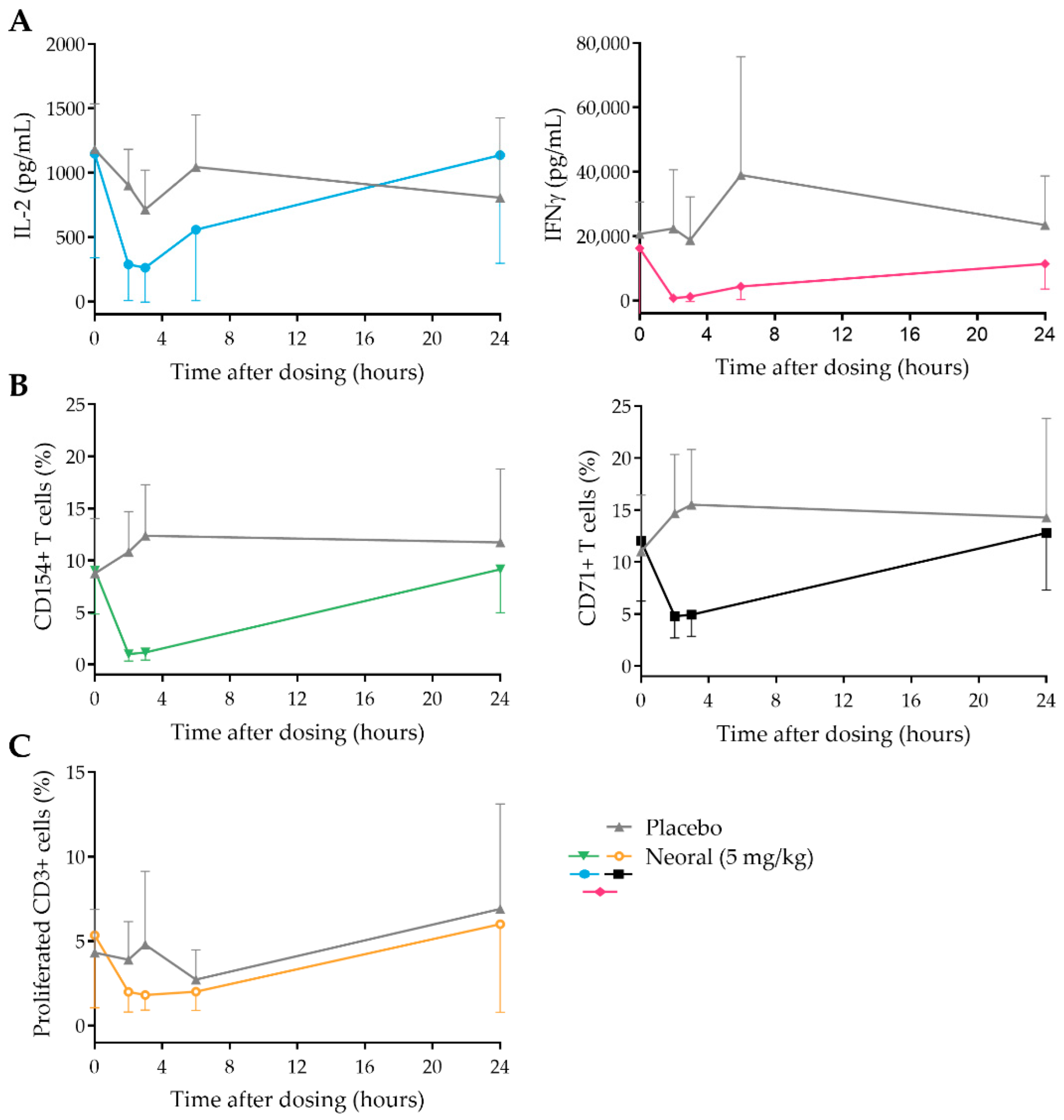
3.3. CsA Strongly Inhibits PD Markers Post-Dose
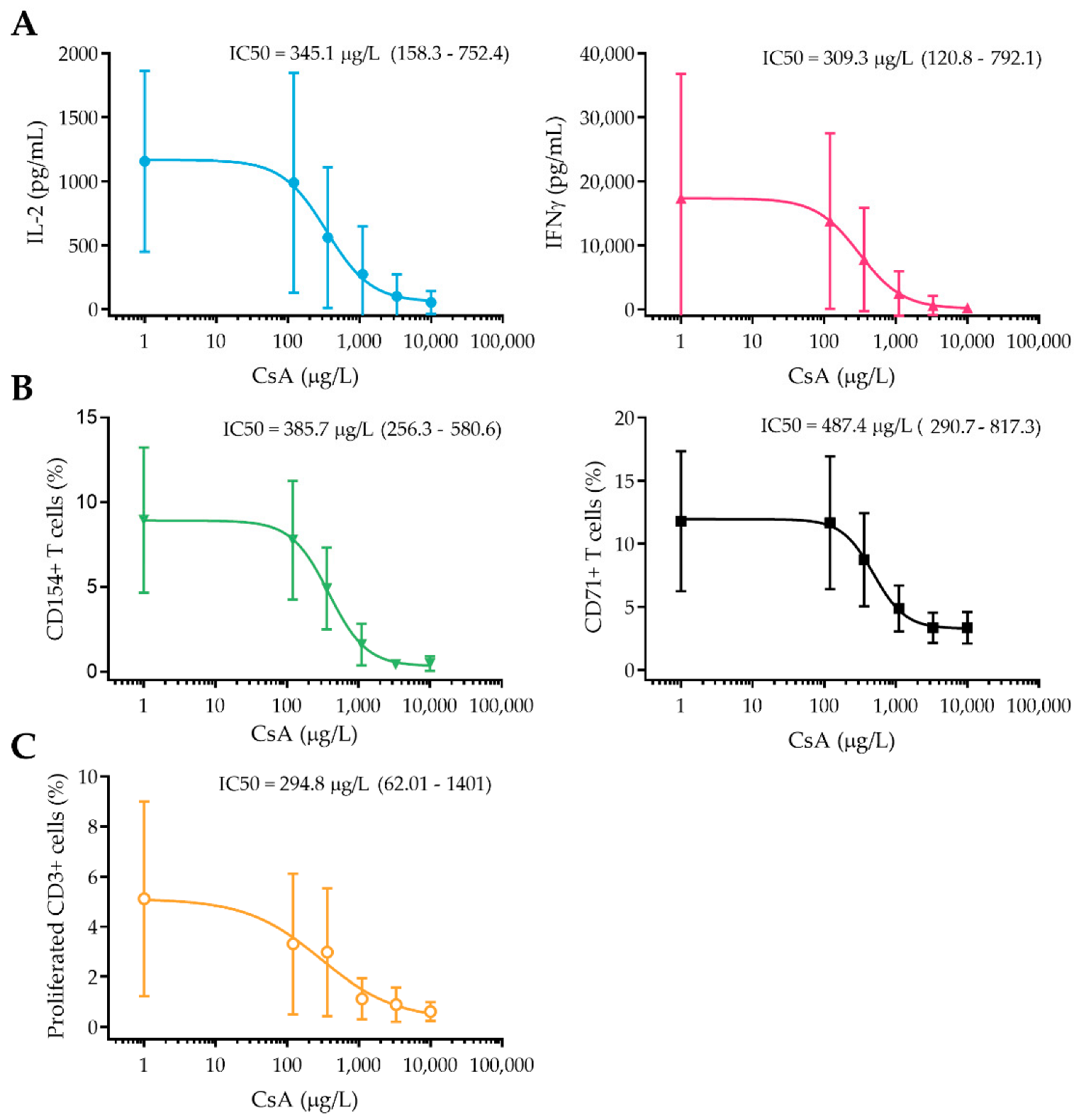
3.4. In Vitro Concentration–Effect Relationship of CsA
3.5. Correlation of In Vitro and Ex Vivo Drug Effect
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farouk, S.S.; Rein, J.L. The Many Faces of Calcineurin Inhibitor Toxicity-What the FK? Adv. Chronic Kidney Dis. 2020, 27, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Brunet, M.; Shipkova, M.; van Gelder, T.; Wieland, E.; Sommerer, C.; Budde, K.; Haufroid, V.; Christians, U.; López-Hoyos, M.; Barten, M.J.; et al. Barcelona Consensus on Biomarker-Based Immunosuppressive Drugs Management in Solid Organ Transplantation. Ther. Drug Monit. 2016, 38 (Suppl. S1), S1–S20. [Google Scholar] [CrossRef]
- Brunet, M.; van Gelder, T.; Åsberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef] [PubMed]
- Francke, M.I.; Hesselink, D.A.; Li, Y.; Koch, B.C.P.; de Wit, L.E.A.; van Schaik, R.H.N.; Yang, L.; Baan, C.C.; van Gelder, T.; de Winter, B.C.M. Monitoring the tacrolimus concentration in peripheral blood mononuclear cells of kidney transplant recipients. Br. J. Clin. Pharmacol. 2021, 87, 1918–1929. [Google Scholar] [CrossRef] [PubMed]
- Coste, G.; Chabanne, C.; Tron, C.; Lelong, B.; Verdier, M.C.; Roussel, M.; Le Gall, F.; Turlin, B.; Desille-Dugast, M.; Flécher, E.; et al. Blood, cellular, and tissular calcineurin inhibitors pharmacokinetic-pharmacodynamic relationship in heart transplant recipients: The INTRACAR study. Ther. Drug Monit. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Lemaitre, F.; Vethe, N.T.; D’Avolio, A.; Tron, C.; Robertsen, I.; De Winter, B.; Denicolo, A.; Koch, B.C.P.; Venkataramanan, R.; Van Gelder, T.; et al. Measuring Intracellular Concentrations of Calcineurin Inhibitors: Expert Consensus from the International Association of Therapeutic Drug Monitoring and Clinical Toxicology Expert Panel. Ther. Drug Monit. 2020, 42, 665–670. [Google Scholar] [CrossRef]
- Blanchet, B.; Duvoux, C.; Costentin, C.E.; Barrault, C.; Ghaleh, B.; Salvat, A.; Jouault, H.; Astier, A.; Tod, M.; Hulin, A. Pharmacokinetic-pharmacodynamic assessment of tacrolimus in liver-transplant recipients during the early post-transplantation period. Ther. Drug Monit. 2008, 30, 412–418. [Google Scholar] [CrossRef]
- Sellar, K.J.; van Rossum, H.H.; Romijn, F.P.; Smit, N.P.; de Fijter, J.W.; van Pelt, J. Spectrophotometric assay for calcineurin activity in leukocytes isolated from human blood. Anal. Biochem. 2006, 358, 104–110. [Google Scholar] [CrossRef]
- Fukudo, M.; Yano, I.; Masuda, S.; Fukatsu, S.; Katsura, T.; Ogura, Y.; Oike, F.; Takada, Y.; Tanaka, K.; Inui, K. Pharmacodynamic analysis of tacrolimus and cyclosporine in living-donor liver transplant patients. Clin. Pharmacol. Ther. 2005, 78, 168–181. [Google Scholar] [CrossRef]
- Koefoed-Nielsen, P.B.; Karamperis, N.; Jørgensen, K.A. Validation of the calcineurin phosphatase assay. Clin. Chem. 2004, 50, 2331–2337. [Google Scholar] [CrossRef]
- Blanchet, B.; Hulin, A.; Duvoux, C.; Astier, A. Determination of serine/threonine protein phosphatase type 2B PP2B in lymphocytes by HPLC. Anal. Biochem. 2003, 312, 1–6. [Google Scholar] [CrossRef]
- Ahmed, M.; Venkataraman, R.; Logar, A.J.; Rao, A.S.; Bartley, G.P.; Robert, K.; Dodson, F.S.; Shapiro, R.; Fung, J.J.; Zeevi, A. Quantitation of immunosuppression by tacrolimus using flow cytometric analysis of interleukin-2 and interferon-gamma inhibition in CD8(-) and CD8(+) peripheral blood T cells. Ther. Drug Monit. 2001, 23, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Albring, A.; Wendt, L.; Harz, N.; Engler, H.; Wilde, B.; Kribben, A.; Lindemann, M.; Schedlowski, M.; Witzke, O. Relationship between pharmacokinetics and pharmacodynamics of calcineurin inhibitors in renal transplant patients. Clin. Transplant. 2015, 29, 294–300. [Google Scholar] [CrossRef]
- Marx, S.; Adam, C.; Mihm, J.; Weyrich, M.; Sester, U.; Sester, M. A Polyclonal Immune Function Assay Allows Dose-Dependent Characterization of Immunosuppressive Drug Effects but Has Limited Clinical Utility for Predicting Infection on an Individual Basis. Front. Immunol. 2020, 11, 916. [Google Scholar] [CrossRef]
- Stalder, M.; Bîrsan, T.; Holm, B.; Haririfar, M.; Scandling, J.; Morris, R.E. Quantification of immunosuppression by flow cytometry in stable renal transplant recipients. Ther. Drug Monit. 2003, 25, 22–27. [Google Scholar] [CrossRef]
- Sommerer, C.; Brunet, M.; Budde, K.; Millán, O.; Guirado Perich, L.; Glander, P.; Meuer, S.; Zeier, M.; Giese, T. Monitoring of gene expression in tacrolimus-treated de novo renal allograft recipients facilitates individualized immunosuppression: Results of the IMAGEN study. Br. J. Clin. Pharmacol. 2021, 87, 3851–3862. [Google Scholar] [CrossRef] [PubMed]
- Zwart, T.C.; Metscher, E.; van der Boog, P.J.M.; Swen, J.J.; de Fijter, J.W.; Guchelaar, H.J.; de Vries, A.P.J.; Moes, D. Volumetric microsampling for simultaneous remote immunosuppressant and kidney function monitoring in outpatient kidney transplant recipients. Br. J. Clin. Pharmacol. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Moes, D.J.; van der Bent, S.A.; Swen, J.J.; van der Straaten, T.; Inderson, A.; Olofsen, E.; Verspaget, H.W.; Guchelaar, H.J.; den Hartigh, J.; van Hoek, B. Population pharmacokinetics and pharmacogenetics of once daily tacrolimus formulation in stable liver transplant recipients. Eur. J. Clin. Pharmacol. 2016, 72, 163–174. [Google Scholar] [CrossRef]
- Nankivell, B.J.; PʼNg, C.H.; OʼConnell, P.J.; Chapman, J.R. Calcineurin Inhibitor Nephrotoxicity Through the Lens of Longitudinal Histology: Comparison of Cyclosporine and Tacrolimus Eras. Transplantation 2016, 100, 1723–1731. [Google Scholar] [CrossRef]
- Wu, K.H.; Cui, Y.M.; Guo, J.F.; Zhou, Y.; Zhai, S.D.; Cui, F.D.; Lu, W. Population pharmacokinetics of cyclosporine in clinical renal transplant patients. Drug Metab. Dispos. Biol. Fate Chem. 2005, 33, 1268–1275. [Google Scholar] [CrossRef] [Green Version]
- Kees, F.; Bucher, M.; Schweda, F.; Gschaidmeier, H.; Faerber, L.; Seifert, R. Neoimmun versus Neoral: A bioequivalence study in healthy volunteers and influence of a fat-rich meal on the bioavailability of Neoimmun. Naunyn-Schmiedebergs Arch. Pharmacol. 2007, 375, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Lepage, J.M.; Lelong-Boulouard, V.; Lecouf, A.; Debruyne, D.; Hurault de Ligny, B.; Coquerel, A. Cyclosporine monitoring in peripheral blood mononuclear cells: Feasibility and interest. A prospective study on 20 renal transplant recipients. Transplant. Proc. 2007, 39, 3109–3110. [Google Scholar] [CrossRef] [PubMed]
- In’t Veld, A.E.; Grievink, H.W.; Saghari, M.; Stuurman, F.E.; de Kam, M.L.; de Vries, A.P.J.; de Winter, B.C.M.; Burggraaf, J.; Cohen, A.F.; Moerland, M. Immunomonitoring of Tacrolimus in Healthy Volunteers: The First Step from PK- to PD-Based Therapeutic Drug Monitoring? Int. J. Mol. Sci. 2019, 20, 4710. [Google Scholar] [CrossRef] [PubMed]
- Vaeth, M.; Feske, S. NFAT control of immune function: New Frontiers for an Abiding Trooper. F1000Research 2018, 7, 260. [Google Scholar] [CrossRef]
- Boyman, O.; Sprent, J. The role of interleukin-2 during homeostasis and activation of the immune system. Nat. Rev. Immunol. 2012, 12, 180–190. [Google Scholar] [CrossRef]
- Cibrián, D.; Sánchez-Madrid, F. CD69: From activation marker to metabolic gatekeeper. Eur. J. Immunol. 2017, 47, 946–953. [Google Scholar] [CrossRef]
- Létourneau, S.; Krieg, C.; Pantaleo, G.; Boyman, O. IL-2- and CD25-dependent immunoregulatory mechanisms in the homeostasis of T-cell subsets. J. Allergy Clin. Immunol. 2009, 123, 758–762. [Google Scholar] [CrossRef]
- Perrin, S.; Magill, M. The Inhibition of CD40/CD154 Costimulatory Signaling in the Prevention of Renal Transplant Rejection in Nonhuman Primates: A Systematic Review and Meta Analysis. Front. Immunol. 2022, 13, 861471. [Google Scholar] [CrossRef]
- Ponka, P.; Lok, C.N. The transferrin receptor: Role in health and disease. Int. J. Biochem. Cell Biol. 1999, 31, 1111–1137. [Google Scholar] [CrossRef]
- Di Paolo, S.; Teutonico, A.; Infante, B.; Stallone, G.; Schena, A.; Grandaliano, G.; Battaglia, M.; Di Tonno, P.; Schena, F.P. Experience with cyclosporine: Approaching the therapeutic window for C2 levels in maintenance kidney transplant recipients. Transplant. Proc. 2004, 36, 434s–436s. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject characteristics | 5 mg/kg Neoral (n = 12) | Placebo (n = 4) | ||
|---|---|---|---|---|
| Age (range) | 28.9 (21–52) | 25.5 (22–28) | ||
| Gender (female/male) | 4/8 | 2/2 | ||
| BMI (kg/m2), mean (range) | 23.3 (19–26.4) | 24.0 (21.5–27.5) | ||
| System Organ Class/Preferred term | Events | Subjects (%) | Events | Subjects (%) |
| Any events | 32 | 11 (91.7) | 3 | 3 (75.0) |
| Gastrointestinal disorders | 5 | 5 (41.7) | - | - |
| Abdominal pain | 1 | 1 (8.3) | - | - |
| Faeces pale | 1 | 1 (8.3) | - | - |
| Nausea | 2 | 3 (25.0) | - | - |
| General disorders and administration site conditions | 18 | 7 (58.3) | - | - |
| Burning sensation | 1 | 1 (8.3) | - | - |
| Fatigue | 5 | 3 (25.0) | - | - |
| Feeling cold | 1 | 1 (8.3) | - | - |
| Feeling hot | 6 | 3 (25.0) | - | - |
| Hyperhidrosis | 1 | 1 (8.3) | - | - |
| Peripheral coldness | 4 | 3 (25.0) | - | - |
| Infections and infestations | 1 | 1 (8.3%) | - | - |
| Candida infection | 1 | 1 (8.3%) | - | - |
| Nervous system disorders | 6 | 6 (50.0) | 3 | 3 (75.0) |
| Dizziness | - | - | 1 | 1 (25.0) |
| Headache | 5 | 5 (41.7) | 2 | 2 (50.0) |
| Somnolence | 1 | 1 (8.3) | - | - |
| Renal and urinary disorders | 1 | 1 (8.3) | - | - |
| Chromaturia | 1 | 1 (8.3) | - | - |
| Respiratory, thoracic, and mediastinal disorders | 1 | 1 (8.3) | - | - |
| Nasopharyngitis | 1 | 1 (8.3) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
in ’t Veld, A.E.; Jansen, M.A.A.; Huisman, B.W.; Schoonakker, M.; de Kam, M.L.; Moes, D.J.A.R.; van Poelgeest, M.I.E.; Burggraaf, J.; Moerland, M. Monitoring of Ex Vivo Cyclosporin a Activity in Healthy Volunteers Using T Cell Function Assays in Relation to Whole Blood and Cellular Pharmacokinetics. Pharmaceutics 2022, 14, 1958. https://doi.org/10.3390/pharmaceutics14091958
in ’t Veld AE, Jansen MAA, Huisman BW, Schoonakker M, de Kam ML, Moes DJAR, van Poelgeest MIE, Burggraaf J, Moerland M. Monitoring of Ex Vivo Cyclosporin a Activity in Healthy Volunteers Using T Cell Function Assays in Relation to Whole Blood and Cellular Pharmacokinetics. Pharmaceutics. 2022; 14(9):1958. https://doi.org/10.3390/pharmaceutics14091958
Chicago/Turabian Stylein ’t Veld, Aliede E., Manon A. A. Jansen, Bertine W. Huisman, Mascha Schoonakker, Marieke L. de Kam, Dirk Jan A. R. Moes, Mariëtte I. E. van Poelgeest, Jacobus Burggraaf, and Matthijs Moerland. 2022. "Monitoring of Ex Vivo Cyclosporin a Activity in Healthy Volunteers Using T Cell Function Assays in Relation to Whole Blood and Cellular Pharmacokinetics" Pharmaceutics 14, no. 9: 1958. https://doi.org/10.3390/pharmaceutics14091958