
Anti PD-1/Anti PDL-1 Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Meta-Analysis of Phase 2/3 Randomized Controlled Trials

Abstract
:1. Introduction
2. Summary
2.1. Question
2.2. Findings
2.3. Meaning
3. Methods
3.1. Data Sources and Searches
3.2. Selection Criteria
3.3. Data Extraction
3.4. Statistical Methods
4. Results
4.1. Study Selection
4.2. Overall Study Population
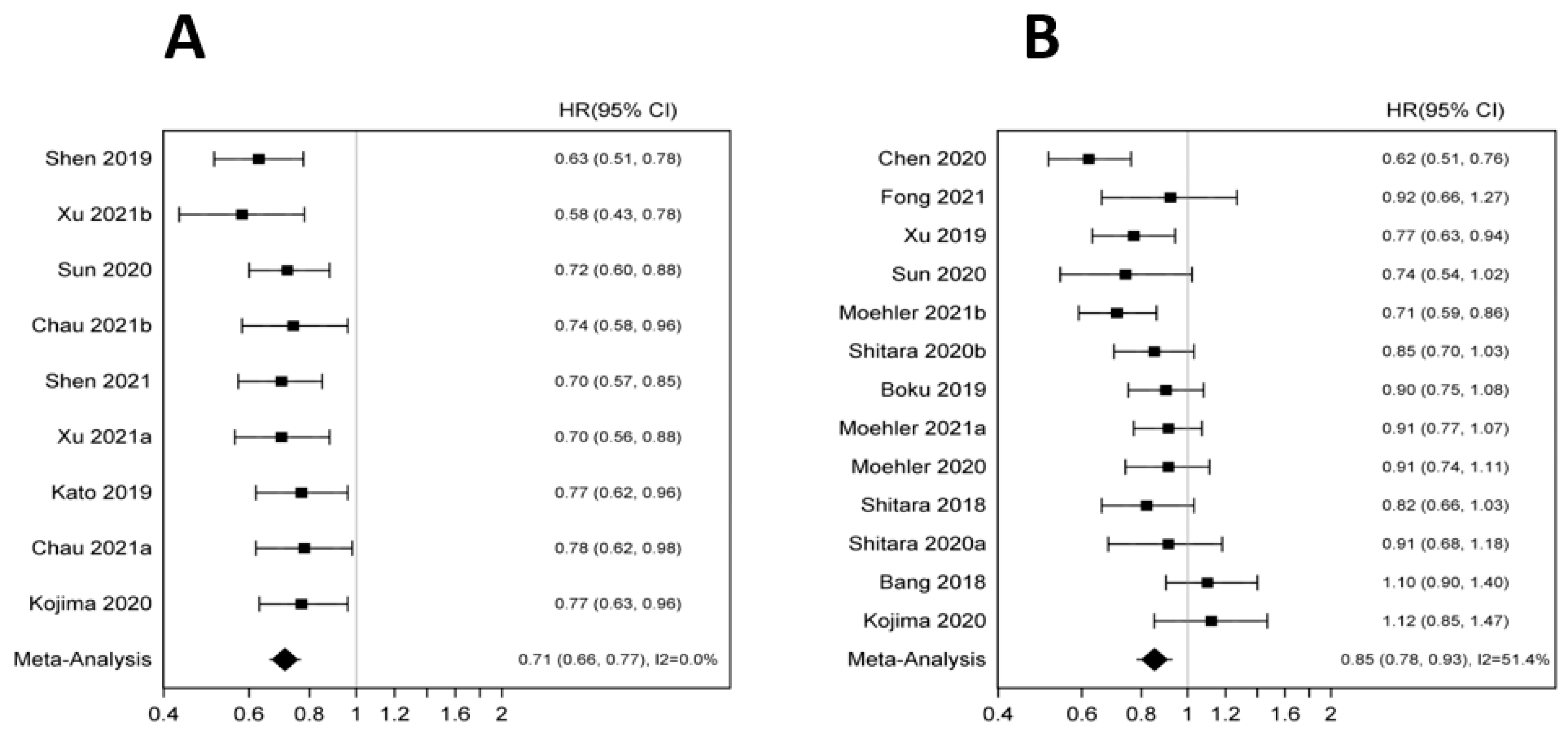
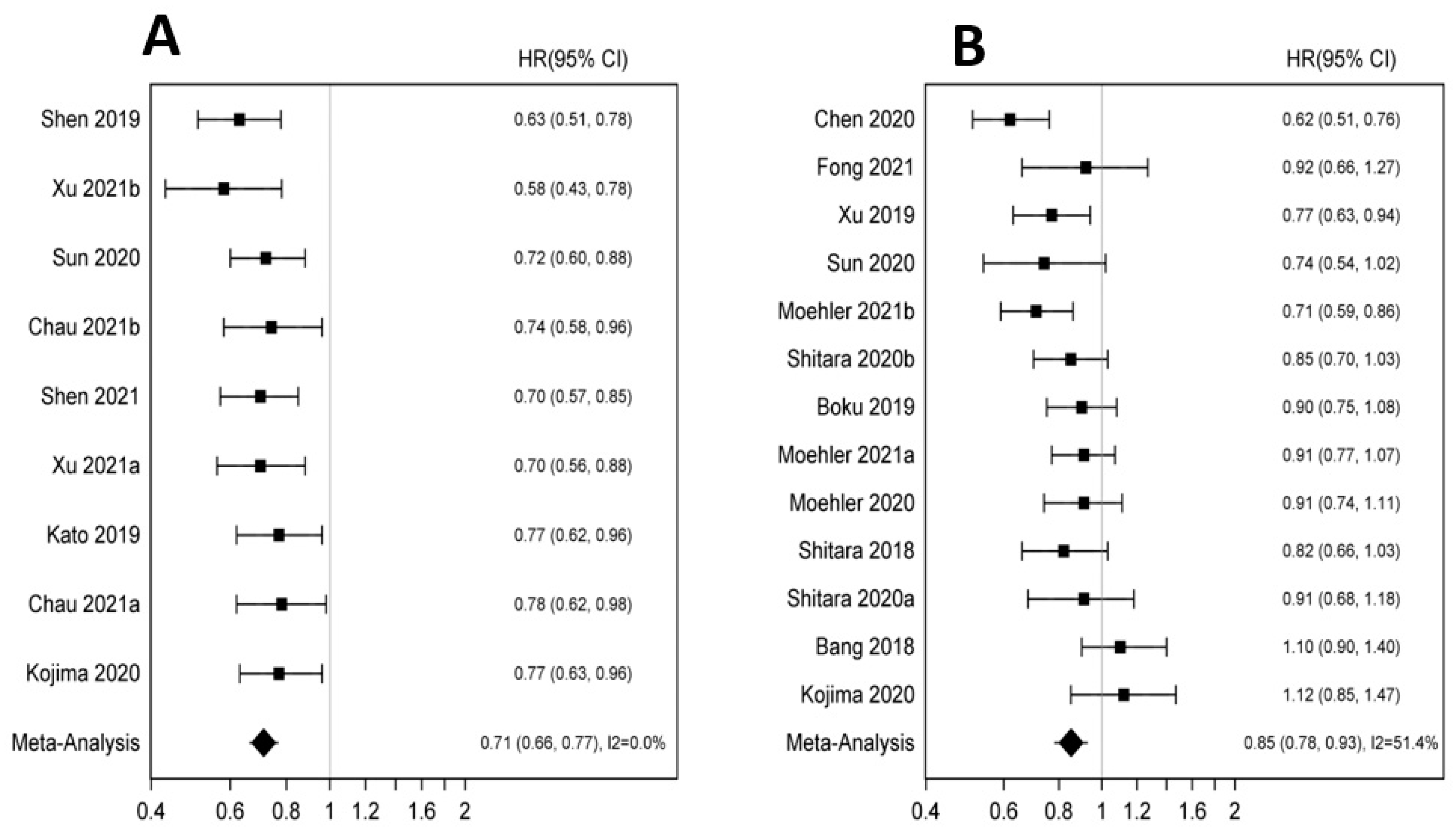
4.3. Anti PD-1/PD-L1 plus Chemotherapy vs. Chemotherapy
4.4. Anti-PD-1/PDL-1 vs. Chemotherapy
4.5. Anti PD-1/PDL-1 vs. Placebo
4.6. Publication Bias
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.-E.; Atmaca, A.; Hegewisch-Becker, S.; Jaeger, D.; Hahnfeld, S.; Rummel, M.J.; Seipelt, G.; Rost, A.; Orth, J.; Knuth, A.; et al. Phase II Trial of Biweekly Infusional Fluorouracil, Folinic Acid, and Oxaliplatin in Patients with Advanced Gastric Cancer. J. Clin. Oncol. 2004, 22, 658–663. [Google Scholar] [CrossRef]
- Catenacci, D.V.; Chao, J.; Muro, K.; Al-Batran, S.E.; Klempner, S.J.; Wainberg, Z.A.; Shah, M.A.; Rha, S.Y.; Ohtsu, A.; Liepa, A.M.; et al. Toward a Treatment Sequencing Strategy: A Systematic Review of Treatment Regimens in Advanced Gastric Cancer/Gastroesophageal Junction Adenocarcinoma. Oncologist 2021, 26, e1704–e1729. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.A. Update on Metastatic Gastric and Esophageal Cancers. J. Clin. Oncol. 2015, 33, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 3, 27–40. [Google Scholar] [CrossRef]
- Sun, J.-M.; Shen, L.; Shah, M.A.; Enzinger, P.; Adenis, A.; Doi, T.; Kojima, T.; Metges, J.-P.; Li, Z.; Kim, S.-B.; et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): A randomised, placebo-controlled, phase 3 study. Lancet 2021, 398, 759–771. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Kawazoe, A.; Yañez, P.; Li, N.; Lonardi, S.; Kolesnik, O.; Barajas, O.; Bai, Y.; Shen, L.; Tang, Y.; et al. The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer. Nature 2021, 600, 727–730. [Google Scholar] [CrossRef]
- Ilson, D.H. Immunotherapy in esophagogastric cancer. Clin. Adv. Hematol. Oncol. 2021, 19, 639–647. [Google Scholar]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 2013, MR000030. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Yang, Z.R.; Sun, F.; Zhan, S.Y. Risk on bias assessment: (2) Revised Cochrane risk of bias tool for individually randomized, parallel group trials (RoB2.0). Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 1285–1291. [Google Scholar] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.-H.; Luo, H.; Lu, J.; Bai, Y.; Mao, T.; Wang, J.; Fan, Q.; Zhang, Y.; Zhao, K.; Chen, Z.; et al. ESCORT-1st: A randomized, double-blind, placebo-controlled, phase 3 trial of camrelizumab plus chemotherapy versus chemotherapy in patients with untreated advanced or metastatic esophageal squamous cell carcinoma (ESCC). J. Clin. Oncol. 2021, 39, 4000. [Google Scholar] [CrossRef]
- Boku, N.; Ryu, M.H.; Kato, K.; Chung, H.C.; Minashi, K.; Lee, K.W.; Cho, H.; Kang, W.K.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of nivolumab in combination with S-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase II trial (ATTRACTION-4). Ann. Oncol. 2019, 30, 250–258. [Google Scholar]
- Xu, R.-H.; Wang, F.; Cui, C.; Yao, J.; Zhang, Y.; Wang, G.; Feng, J.; Yang, S.; Fan, Y.; Shi, J.; et al. 1373MO JUPITER-06: A Randomized, Double-Blind, Phase III Study of Toripalimab Versus Placebo in Combination with First-Line Chemotherapy for Treatment Naive Advanced or Metastatic Esophageal Squamous Cell Carcinoma (ESCC). Ann. Oncol. 2021, 32 (Suppl. 5), S1040–S1075. [Google Scholar] [CrossRef]
- Xu, J.; Jin, Y.; Liu, Y.; Zhou, H.; Wang, Y. Abstract CT213: ORIENT-16: Sintilimab plus XELOX vs placebo plus XELOX as 1st line treatment for unresectable advanced gastric and GEJ adenocarcinoma. Cancer Res. 2019, 79 (Suppl. 13), CT213. [Google Scholar] [CrossRef]
- Lu, Z.; Wang, J.; Shu, Y.; Liu, L.; Kong, L.; Yang, L.; Wang, B.; Sun, G.; Ji, Y.; Cao, G.; et al. Sintilimab versus placebo in combination with chemotherapy as first line treatment for locally advanced or metastatic oesophageal squamous cell carcinoma (ORIENT-15): Multicentre, randomised, double blind, phase 3 trial. BMJ 2022, 377, e068714. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.-J.; Fuchs, C.; Wyrwicz, L.; Lee, K.-W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Doki, Y.; Ajani, J.A.; Kato, K.; Xu, J.; Wyrwicz, L.; Motoyama, S.; Ogata, T.; Kawakami, H.; Hsu, C.-H.; Adenis, A.; et al. Nivolumab Combination Therapy in Advanced Esophageal Squamous-Cell Carcinoma. N. Engl. J. Med. 2022, 386, 449–462. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Ruiz, E.; Van Cutsem, E.; Lee, K.-W.; Wyrwicz, L.; Schenker, M.; Alsina, M.; Ryu, M.-H.; Chung, H.-C.; Evesque, L.; et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef]
- Kato, K.; Cho, B.C.; Takahashi, M.; Okada, M.; Lin, C.-Y.; Chin, K.; Kadowaki, S.; Ahn, M.-J.; Hamamoto, Y.; Doki, Y.; et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Kojima, T.; Shah, M.A.; Muro, K.; Francois, E.; Adenis, A.; Hsu, C.H.; Doi, T.; Moriwaki, T.; Kim, S.; Lee, S.; et al. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef] [PubMed]
- Moehler, M.; Dvorkin, M.; Boku, N.; Özgüroğlu, M.; Ryu, M.-H.; Muntean, A.S.; Lonardi, S.; Nechaeva, M.; Bragagnoli, A.C.; Coşkun, H.S.; et al. Phase III Trial of Avelumab Maintenance After First-Line Induction Chemotherapy Versus Continuation of Chemotherapy in Patients with Gastric Cancers: Results From JAVELIN Gastric 100. J. Clin. Oncol. 2021, 39, 966–977. [Google Scholar] [CrossRef]
- Shen, L.; Kato, K.; Kim, S.-B.; Ajani, J.A.; Zhao, K.; He, Z.; Yu, X.; Shu, Y.; Luo, Q.; Wang, J.; et al. RATIONALE 302: Randomized, phase 3 study of tislelizumab versus chemotherapy as second-line treatment for advanced unresectable/metastatic esophageal squamous cell carcinoma. J. Clin. Oncol. 2021, 39, 4012. [Google Scholar] [CrossRef]
- Shitara, K.; Özgüroğlu, M.; Bang, Y.J.; Di Bartolomeo, M.; Mandalà, M.; Ryu, M.H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Fong, C.; Patel, B.; Peckitt, C.; Bourmpaki, E.; von Loga, K.; Begum, R.; Davidson, M.; Anandappa, G.; Cafferkey, C.; Watkins, D.J.; et al. Maintenance durvalumab after first-line platinum-based chemotherapy in advanced oesophago-gastric (OG) adenocarcinoma: Results from the PLATFORM trial. J. Clin. Oncol. 2021, 39, 4015. [Google Scholar] [CrossRef]
- Chen, L.-T.; Satoh, T.; Ryu, M.-H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.-S.; Muro, K.; Kang, W.K.; Yeh, K.-H.; et al. A phase 3 study of nivolumab in previously treated advanced gastric or gastroesophageal junction cancer (ATTRACTION-2): 2-year update data. Gastric Cancer 2019, 23, 510–519. [Google Scholar] [CrossRef]
- Chung, H.C.; Bang, Y.J.; Fuchs, C.S.; Qin, S.K.; Satoh, T.; Shitara, K.; Tabernero, J.; van Cutsem, E.; Alsina, M.; Cao, Z.A.; et al. First-line pembrolizumab/placebo plus trastuzumab and chemotherapy in HER2-positive advanced gastric cancer: KEYNOTE-811. Future Oncol. 2021, 17, 491–501. [Google Scholar] [CrossRef]
- Kundel, Y.; Sternschuss, M.; Moore, A.; Perl, G.; Brenner, B.; Goldvaser, H. Efficacy of immune-checkpoint inhibitors in metastatic gastric or gastroesophageal junction adenocarcinoma by patient subgroups: A systematic review and meta-analysis. Cancer Med. 2020, 9, 7613–7625. [Google Scholar] [CrossRef]
- Wang, B.C.; Zhang, Z.J.; Fu, C.; Wang, C. Efficacy and safety of anti-PD-1/PD-L1 agents vs chemotherapy in patients with gastric or gastroesophageal junction cancer: A systematic review and meta-analysis. Medicine 2019, 98, e18054. [Google Scholar] [CrossRef]
- Pala, L.; Conforti, F. The effect of patient sex on the efficacy and safety of anticancer immunotherapy. Expert Opin. Drug Saf. 2021, 20, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wei, Z.; Wang, C.; Chen, W.; He, Y.; Zhang, C. Gender Differences in Gastric Cancer Survival: 99,922 Cases Based on the SEER Database. J. Gastrointest. Surg. 2019, 24, 1747–1757. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Jing, Y.; Li, L.; Mills, G.B.; Diao, L.; Liu, H.; Han, L. Sex-associated molecular differences for cancer immunotherapy. Nat. Commun. 2020, 11, 1779. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.; Giobbie-Hurder, A.; McCleary, N.J.; Ott, P.; Hodi, F.S.; Rahma, O. Efficacy of PD-1 & PD-L1 inhibitors in older adults: A meta-analysis. J. Immunother. Cancer 2018, 6, 26. [Google Scholar] [CrossRef]
- Denson, A.C.; Mahipal, A. Participation of the Elderly Population in Clinical Trials: Barriers and Solutions. Cancer Control 2014, 21, 209–214. [Google Scholar] [CrossRef]
- Talarico, L.; Chen, G.; Pazdur, R. Enrollment of Elderly Patients in Clinical Trials for Cancer Drug Registration: A 7-Year Experience by the US Food and Drug Administration. J. Clin. Oncol. 2004, 22, 4626–4631. [Google Scholar] [CrossRef]
- Sedrak, M.S.; Mohile, S.G.; Sun, V.; Sun, C.-L.; Chen, B.T.; Li, D.; Wong, A.R.; George, K.; Padam, S.; Liu, J.; et al. Barriers to clinical trial enrollment of older adults with cancer: A qualitative study of the perceptions of community and academic oncologists. J. Geriatr. Oncol. 2019, 11, 327–334. [Google Scholar] [CrossRef]
- Athauda, A.; Nankivell, M.; Langley, R.E.; Alderson, D.; Allum, W.; Grabsch, H.I.; Starling, N.; Chau, I.; Cunningham, D. Impact of sex and age on chemotherapy efficacy, toxicity and survival in localised oesophagogastric cancer: A pooled analysis of 3265 individual patient data from four large randomised trials (OE02, OE05, MAGIC and ST03). Eur. J. Cancer 2020, 137, 45–56. [Google Scholar] [CrossRef]
- Fong, C.Y.; Chau, I. Harnessing biomarkers of response to improve therapy selection in esophago-gastric adenocarcinoma. Pharmacogenomics 2021, 22, 703–726. [Google Scholar] [CrossRef]
- Yamashita, K.; Iwatsuki, M.; Harada, K.; Eto, K.; Hiyoshi, Y.; Ishimoto, T.; Nagai, Y.; Iwagami, S.; Miyamoto, Y.; Yoshida, N.; et al. Prognostic impacts of the combined positive score and the tumor proportion score for programmed death ligand-1 expression by double immunohistochemical staining in patients with advanced gastric cancer. Gastric Cancer 2019, 23, 95–104. [Google Scholar] [CrossRef]
- Kulangara, K.; Guerrero, L.; Posch, A.; Boyer, S.; Hanks, D.A.; Carnahan, J.; Wang, J.; Lunceford, J.; Savage, M.; Marton, M.J.; et al. Investigation of PD-L1 expression and response to pembrolizumab (pembro) in gastric cancer (GC) and cervical cancer (CC) using combined positive score (CPS) and tumor proportion score (TPS). J. Clin. Oncol. 2018, 36, 4065. [Google Scholar] [CrossRef]
- Yeong, J.; Lum, H.Y.J.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; Tay, R.Y.K.; Choo, J.R.-E.; Jeyasekharan, A.D.; Miow, Q.H.; Loo, L.-H.; et al. Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy. Gastric Cancer 2022, 25, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Petrelli, F.; Ghidini, A.; Raimondi, A.; Smyth, E.; Pietrantonio, F. Efficacy and activity of PD-1 blockade in patients with advanced esophageal squamous cell carcinoma: A systematic review and meta-analysis with focus on the value of PD-L1 combined positive score. ESMO Open 2022, 7, 100380. [Google Scholar] [CrossRef]
- Zhao, J.J.; Yap, D.W.T.; Chan, Y.H.; Tan, B.K.J.; Teo, C.B.; Syn, N.L.; Smyth, E.C.; Soon, Y.Y.; Sundar, R. Low Programmed Death-Ligand 1-Expressing Subgroup Outcomes of First-Line Immune Checkpoint Inhibitors in Gastric or Esophageal Adenocarcinoma. J. Clin. Oncol. 2022, 40, 392–402. [Google Scholar] [CrossRef]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.-Y.; Andre, F.; et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: A systematic review-based approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef] [PubMed]
- Chao, J.; Fuchs, C.S.; Shitara, K.; Tabernero, J.; Muro, K.; Van Cutsem, E.; Bang, Y.; de Vita, F.; Landers, G.; Yen, C.; et al. Assessment of Pembrolizumab Therapy for the Treatment of Microsatellite Instability-High Gastric or Gastroesophageal Junction Cancer Among Patients in the KEYNOTE-059, KEYNOTE-061, and KEYNOTE-062 Clinical Trials. JAMA Oncol. 2021, 7, 895–902. [Google Scholar] [CrossRef]
- Murphy, G.; Pfeiffer, R.; Camargo, M.C.; Rabkin, C.S. Meta-analysis Shows That Prevalence of Epstein–Barr Virus-Positive Gastric Cancer Differs Based on Sex and Anatomic Location. Gastroenterology 2009, 137, 824–833. [Google Scholar] [CrossRef]
- Lima, Á.; Sousa, H.; Medeiros, R.; Nobre, A.; Machado, M. PD-L1 expression in EBV associated gastric cancer: A systematic review and meta-analysis. Discov. Oncol. 2022, 13, 19. [Google Scholar] [CrossRef]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef]
- Dong, Z.; Ni, B.; Yang, L.; Guan, Y.; Zhu, C.; Zhao, E.; Zhao, G.; Xia, X.; Zhang, Z. Efficacy and Safety of Camrelizumab in Combination with Docetaxel + S-1 Sequenced by Camrelizumab+S-1 for Stage III (PD-1+/MSI-H/EBV+/dMMR) Gastric Cancer: Study Protocol for a Single-Center, Prospective, Open-Label, Single-Arm Trial. Front. Surg. 2022, 9, 917352. [Google Scholar] [CrossRef]
- Kim, J.; Kim, B.; Kang, S.Y.; Heo, Y.J.; Park, S.H.; Kim, S.T.; Kang, W.K.; Lee, J.; Kim, K.-M. Tumor Mutational Burden Determined by Panel Sequencing Predicts Survival After Immunotherapy in Patients with Advanced Gastric Cancer. Front. Oncol. 2020, 10, 314. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.H.; Wei, X.; Xu, N.; Shen, L.; Dai, G.; Yuan, X.; Chen, Y.; Yang, S.; Shi, J.; Hu, X.; et al. Safety, efficacy and tumor mutational burden as a biomarker of overall survival benefit in chemo-refractory gastric cancer treated with toripalimab, a PD-1 antibody in phase Ib/II clinical trial NCT02915432. Ann. Oncol. 2019, 30, 1479–1486. [Google Scholar] [CrossRef] [Green Version]
- Fock, K.M.; Ang, T.L. Epidemiology of Helicobacter pylori infection and gastric cancer in Asia. J. Gastroenterol. Hepatol. 2010, 25, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.; Miller, J.; Feng, X.; Gangi, A.; Gong, J.; Burch, M. Racial differences in tumor biology and treatment of gastric cancer in the United States. J. Clin. Oncol. 2021, 39, 174. [Google Scholar] [CrossRef]
- Lin, S.J.; Gagnon-Bartsch, J.A.; Tan, I.B.; Earle, S.; Ruff, L.; Pettinger, K.; Ylstra, B.; Van Grieken, N.; Rha, S.Y.; Chung, H.C.; et al. Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas. Gut 2015, 64, 1721–1731. [Google Scholar] [CrossRef]
- Abnet, C.C.; Arnold, M.; Wei, W.-Q. Epidemiology of Esophageal Squamous Cell Carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef]
- Coleman, H.G.; Xie, S.-H.; Lagergren, J. The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology 2018, 154, 390–405. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network. Integrated genomic characterization of oesophageal carcinoma. Nature 2017, 541, 169–175. [Google Scholar] [CrossRef]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Number | OS | PFS | >Grade 3 TRAE | TRAE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median, mo | Median, mo | |||||||||||||
| Author | ICI | ICI | SoC | ICI | SoC | HR (95% CI) | P | ICI | SoC | HR (95% CI) | ICI | SoC | ICI | SoC |
| Chau et al., 2021 [19], CHECKMATE 648 | Nivolumab + Chemotherapy | 321 | 324 | 13.2 | 10.7 | 0.74 (0.58–0.96) | 0.0021 | 0.65 (0.46–0.92) | 47.00% | 36.00% | 96.00% | 80.00% | ||
| Xu et al., 2021 [13], ESCORT | Camrelizumab + Chemotherapy | 298 | 298 | 15.3 | 12 | 0.70 (0.56–0.88) | 0.001 | 6.9 | 5.6 | 0.56 (0.46–0.68) | 63.40% | 67.70% | 99.30% | 97% |
| Boku et al., 2019 [14], ATTRACTION 4 | Nivolumab + Chemotherapy | 362 | 362 | 17.45 | 17.15 | 0.90 (0.75–1.08) | 0.257 | 10.45 | 8.34 | 0.68 (0.51–0.90) | 57.10% | 48.60% | 97.80% | 97.50% |
| Shitara et al., 2020 [18], KEYNOTE 062 | Pembrolizumab + Chemotherapy | 257 | 250 | 12.5 | 11.1 | 0.85 (0.70–1.03) | 0.05 | 6.9 | 6.4 | 0.84 (0.70–1.02) | 73.20% | 69.30% | 94.00% | 91.80% |
| Moehler et al., 2021 [5], CHECKMATE 649 | Nivolumab + Chemotherapy | 789 | 792 | 13.8 | 11.6 | 0.71 (0.59–0.86) | 0.0002 | 7.7 | 6.9 | 0.68 (0.56–0.81) | 59.00% | 44.00% | 95.00% | 88.00% |
| Sun et al., 2020 [6], KEYNOTE 590 | Pembrolizumab + Chemotherapy | 373 | 376 | 12.6 | 9.8 | 0.73 (0.62–0.86) | <0.0001 | 6.3 | 5.8 | 0.65 (0.55–0.76) | 86.00% | 83.00% | 100.00% | 99.00% |
| Rui Hua Xu et al., 2021 [15], JUPITER-06 | Toripalimab + Chemotherapy | 257 | 257 | 17 | 11 | 0.58 (0.43–0.78) | 0.00036 | 5.7 | 5.5 | 0.58 (0.46–0.74) | 97.30% | 56.00% | 97.30% | 64.60% |
| Jianming Xu et al., 2019 [16], ORIENT-16 | Sintilimab + Chemotherapy | 327 | 323 | 15.2 | 12.3 | 0.77 (0.63–0.94) | 0.009 | 7.1 | 5.7 | 0.636 (0.525–0.771) | 96.30% | 52.50% | 97.30% | 59.80% |
| Lin Shen et al., 2019 [17], ORIENT-15 | Sintilimab + Chemotherapy | 327 | 332 | 16.7 | 12.5 | 0.628 (0.508–0.777) | <0.0001 | 7.2 | 5.7 | 0.558 (0.461–0.676) | 98.20% | 54.50% | 98.20% | 59.90% |
| Patients Number | Os | PFS | >Grade 3 TRAE | TRAE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median, mo | Median, mo | |||||||||||||
| Author | ICI | ICI | SoC | ICI | SoC | HR (95% CI) | P | ICI | SoC | HR (95% CI) | ICI | SoC | ICI | SoC |
| Kojima et. al., 2020 [22], KEYNOTE 181 | Pembrolizumab | 314 | 314 | 9.3 | 6.7 | 0.69 (0.52–0.93) | 0.0074 | 2.1 | 3.4 | 1.11 (0.94–1.31) | 18.20% | 40.90% | 64.30% | 86.10% |
| Chau et al., 2021 [19], CHECKMATE 648 | Nivolumab + Ipilimumab | 325 | 324 | 12.8 | 10.7 | 0.78 (0.62–0.98) | 0.011 | 2.9 | 5.6 | 1.26 (1.042–1.52) | 32.00% | 36.00% | 90.00% | 80.00% |
| Bang et. al., 2018 [20] JAVELIN 300 | Avelumab | 185 | 186 | 4.6 | 5 | 1.1 (0.9–1.4) | 0.81 | 1.4 | 2.7 | 1.73 (1.4–2.2) | 9.20% | 31.60% | 48.90% | 74.00% |
| Kato et. al., 2019 [21], ATTRACTION 3 | Nivolumab | 210 | 209 | 10.9 | 8.4 | 0.77 (0.62–0.96) | 0.02 | 1.7 | 3.4 | 1.08 (0.87–1.34) | 18.00% | 63.00% | 66.00% | 95% |
| Shitara et. al., 2020 [22], KEYNOTE 062 | Pembrolizumab | 256 | 250 | 10.6 | 11.1 | 0.91 (0.68–1.18) | NA | 2 | 6.4 | 1.66 (1.37–2.01) | 16.90% | 69.30% | 54.30% | 91.80% |
| Shitara et. al., 2018 [25], KEYNOTE 061 | Pembrolizumab | 296 | 296 | 9.1 | 8.3 | 0.82 (0.66–1.03) | 0.0421 | 1.5 | 4.1 | 1.25 (1.02–1.54) | 14.00% | 35.00% | 53.00% | 84.00% |
| Moehler et. al., 2020 [23], JAVALIN 100 | Avelumab | 249 | 250 | 10.4 | 10.9 | 0.91 (0.74–1.11) | 0.1179 | 3.2 | 4.4 | 1.04 (0.85–1.28) | 12.80% | 32.80% | 61.30% | 77.30% |
| Shen et al., 2021 [24], RATIONALE 302 | Tislelizumab | 256 | 256 | 8.6 | 6.3 | 0.70 (0.57–0.85) | 0.0001 | NA | 18.8.0% | 55.8.0% | 73.30% | 93.80% | ||
| Moehler et. al., 2021 [5], CHECKMATE 649 | Nivolumab + lpilimumab | 409 | 404 | 11.7 | 11.8 | 0.91 (0.77–1.07) | NA | 2.8 | 7.1 | 1.66 (1.40–1.95) | 38.00% | 46.00% | 80.00% | 92.00% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmar, K.; Subramanyam, S.; Attwood, K.; Appiah, D.; Fountzilas, C.; Mukherjee, S. Anti PD-1/Anti PDL-1 Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Meta-Analysis of Phase 2/3 Randomized Controlled Trials. Pharmaceutics 2022, 14, 1953. https://doi.org/10.3390/pharmaceutics14091953
Parmar K, Subramanyam S, Attwood K, Appiah D, Fountzilas C, Mukherjee S. Anti PD-1/Anti PDL-1 Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Meta-Analysis of Phase 2/3 Randomized Controlled Trials. Pharmaceutics. 2022; 14(9):1953. https://doi.org/10.3390/pharmaceutics14091953
Chicago/Turabian StyleParmar, Kanak, Sai Subramanyam, Kristopher Attwood, Duke Appiah, Christos Fountzilas, and Sarbajit Mukherjee. 2022. "Anti PD-1/Anti PDL-1 Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Meta-Analysis of Phase 2/3 Randomized Controlled Trials" Pharmaceutics 14, no. 9: 1953. https://doi.org/10.3390/pharmaceutics14091953