
Population Pharmacokinetics and Dose Optimization Based on Renal Function of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Rivaroxaban Quantification
2.3. Population Pharmacokinetic Analysis
2.4. Simulations
3. Results
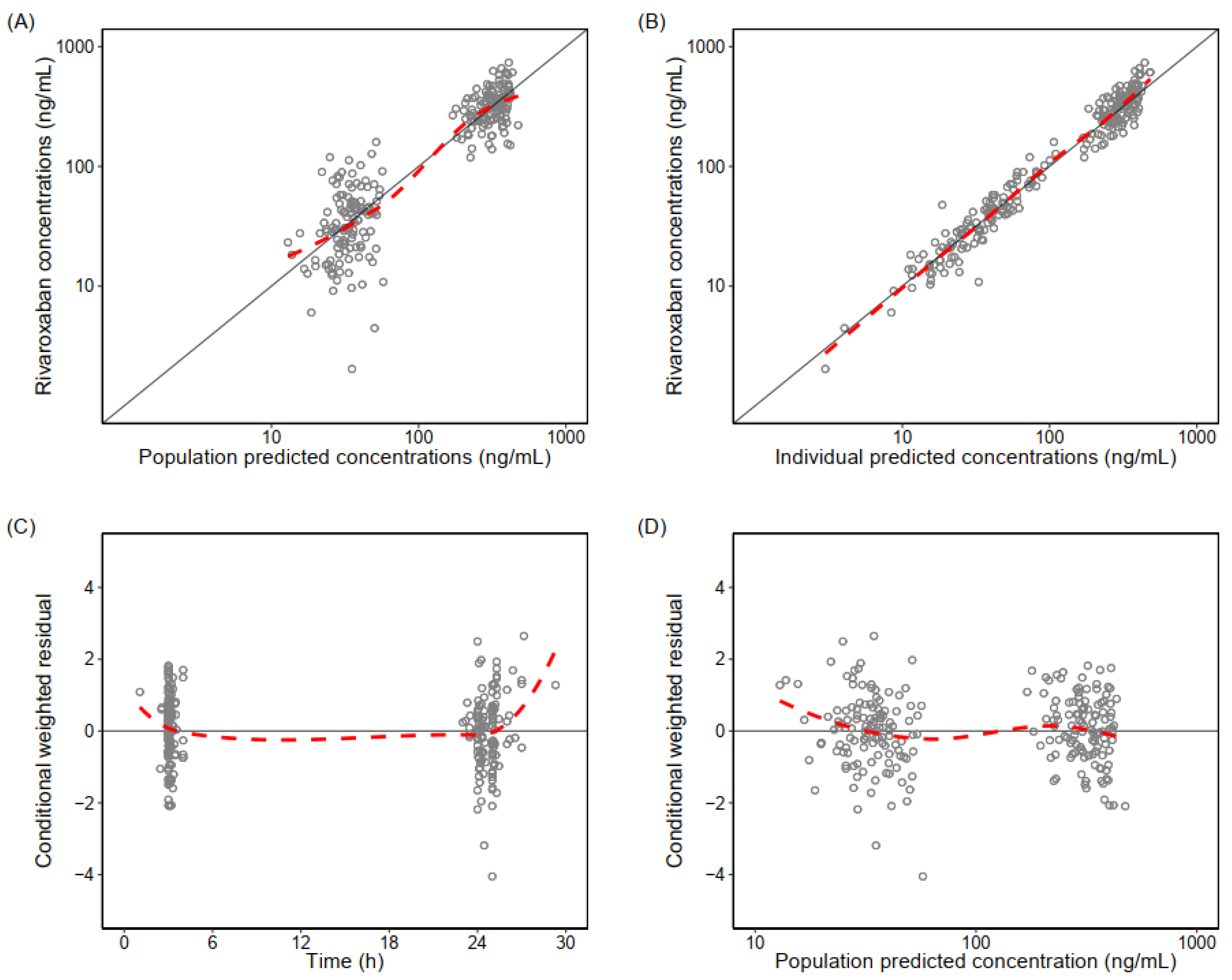
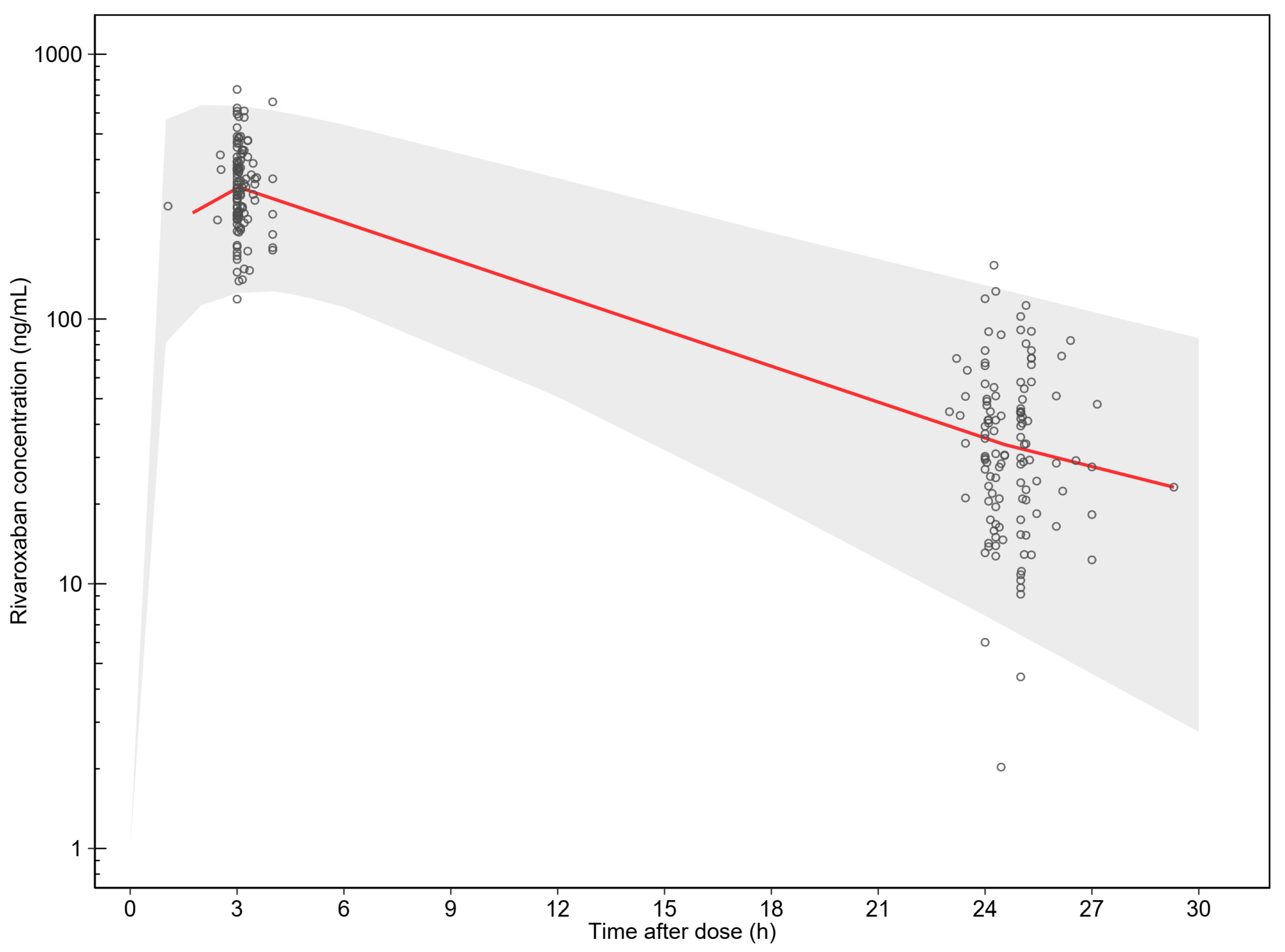
3.1. Population Pharmacokinetic Analysis
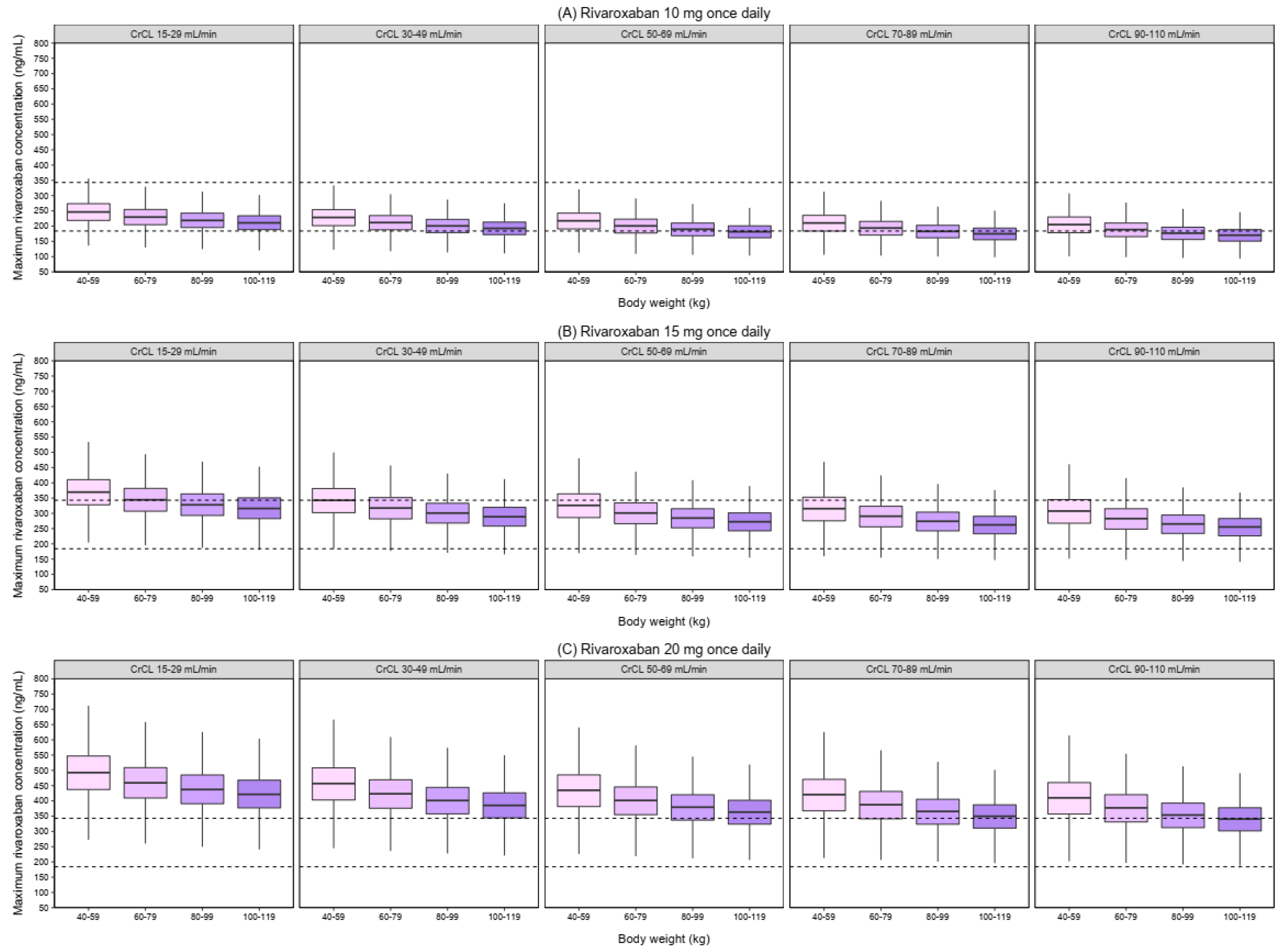
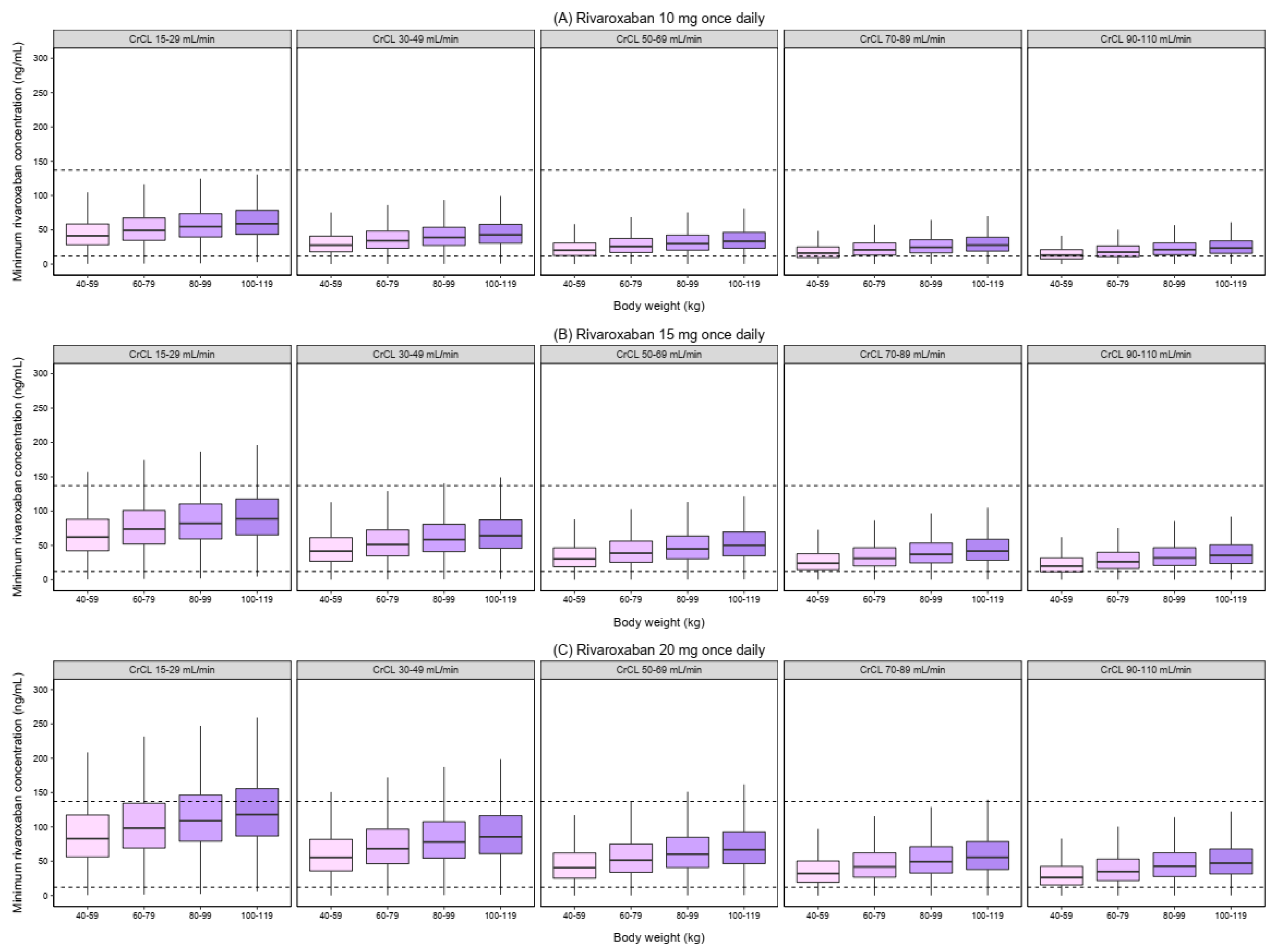
3.2. Simulations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, M.; Matsumoto, M.; Tanahashi, N.; Momomura, S.; Uchiyama, S.; Goto, S.; Izumi, T.; Koretsune, Y.; Kajikawa, M.; Kato, M.; et al. Rivaroxaban vs. warfarin in Japanese patients with atrial fibrillation–the J-ROCKET AF study-. Circ. J. 2012, 76, 2104–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; Shim, J.; Tsai, C.T.; Wang, C.C.; Vilela, G.; Muengtaweepongsa, S.; Kurniawan, M.; Maskon, O.; Fern, H.L.; Nguyen, T.H.; et al. XANAP: A real-world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in atrial fibrillation in Asia. J. Arrhythm. 2018, 34, 418–427. [Google Scholar] [CrossRef] [Green Version]
- Chan, Y.H.; Lee, H.F.; Wang, C.L.; Chang, S.H.; Yeh, C.H.; Chao, T.F.; Yeh, Y.H.; Chen, S.A.; Kuo, C.T. Comparisons of Rivaroxaban Following Different Dosage Criteria (ROCKET AF or J-ROCKET AF Trials) in Asian Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2019, 8, e013053. [Google Scholar] [CrossRef]
- Cuker, A.; Siegal, D.M.; Crowther, M.A.; Garcia, D.A. Laboratory measurement of the anticoagulant activity of the non-vitamin K oral anticoagulants. J. Am. Coll. Cardiol. 2014, 64, 1128–1139. [Google Scholar] [CrossRef] [Green Version]
- Molenaar, P.J.; Dinkelaar, J.; Leyte, A. Measuring Rivaroxaban in a clinical laboratory setting, using common coagulation assays, Xa inhibition and thrombin generation. Clin. Chem. Lab. Med. 2012, 50, 1799–1807. [Google Scholar] [CrossRef]
- Sakaguchi, T.; Osanai, H.; Murase, Y.; Ishii, H.; Nakashima, Y.; Asano, H.; Suzuki, S.; Takefuji, M.; Inden, Y.; Sakai, K. Monitoring of anti-Xa activity and factors related to bleeding events: A study in Japanese patients with nonvalvular atrial fibrillation receiving rivaroxaban. J. Cardiol. 2017, 70, 244–249. [Google Scholar]
- Testa, S.; Legnani, C.; Antonucci, E.; Paoletti, O.; Dellanoce, C.; Cosmi, B.; Pengo, V.; Poli, D.; Morandini, R.; Testa, R.; et al. Drug levels and bleeding complications in atrial fibrillation patients treated with direct oral anticoagulants. J. Thromb. Haemost. 2019, 17, 1064–1072. [Google Scholar] [CrossRef] [Green Version]
- Jakowenko, N.; Nguyen, S.; Ruegger, M.; Dinh, A.; Salazar, E.; Donahue, K.R. Apixaban and rivaroxaban anti-Xa level utilization and associated bleeding events within an academic health system. Thromb. Res. 2020, 196, 276–282. [Google Scholar] [CrossRef]
- Testa, S.; Paoletti, O.; Legnani, C.; Dellanoce, C.; Antonucci, E.; Cosmi, B.; Pengo, V.; Poli, D.; Morandini, R.; Testa, R.; et al. Low drug levels and thrombotic complications in high-risk atrial fibrillation patients treated with direct oral anticoagulants. J. Thromb. Haemost. 2018, 16, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Nosáľ, V.; Petrovičová, A.; Škorňová, I.; Bolek, T.; Dluhá, J.; Stančiaková, L.; Sivák, Š.; Babálová, L.; Hajaš, G.; Staško, J.; et al. Plasma levels of direct oral anticoagulants in atrial fibrillation patients at the time of embolic stroke: A pilot prospective multicenter study. Eur. J. Clin. Pharmacol. 2022, 78, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Miklič, M.; Mavri, A.; Vene, N.; Söderblom, L.; Božič-Mijovski, M.; Pohanka, A.; Antovic, J.; Malmström, R.E. Intra- and inter-individual rivaroxaban concentrations and potential bleeding risk in patients with atrial fibrillation. Eur. J. Clin. Pharmacol. 2019, 75, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Sennesael, A.L.; Larock, A.S.; Douxfils, J.; Elens, L.; Stillemans, G.; Wiesen, M.; Taubert, M.; Dogné, J.M.; Spinewine, A.; Mullier, F. Rivaroxaban plasma levels in patients admitted for bleeding events: Insights from a prospective study. Thromb. J. 2018, 16, 28. [Google Scholar] [CrossRef]
- Cuker, A. Laboratory measurement of the non-vitamin K antagonist oral anticoagulants: Selecting the optimal assay based on drug, assay availability, and clinical indication. J. Thromb. Thrombolysis 2016, 41, 241–247. [Google Scholar] [CrossRef]
- Ikeda, K.; Tachibana, H. Clinical implication of monitoring rivaroxaban and apixaban by using anti-factor Xa assay in patients with non-valvular atrial fibrillation. J. Arrhythm. 2016, 32, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Testa, S.; Tripodi, A.; Legnani, C.; Pengo, V.; Abbate, R.; Dellanoce, C.; Carraro, P.; Salomone, L.; Paniccia, R.; Paoletti, O.; et al. Plasma levels of direct oral anticoagulants in real life patients with atrial fibrillation: Results observed in four anticoagulation clinics. Thromb. Res. 2016, 137, 178–183. [Google Scholar] [CrossRef] [Green Version]
- Gulilat, M.; Tang, A.; Gryn, S.E.; Leong-Sit, P.; Skanes, A.C.; Alfonsi, J.E.; Dresser, G.K.; Henderson, S.L.; Rose, R.V.; Lizotte, D.J.; et al. Interpatient Variation in Rivaroxaban and Apixaban Plasma Concentrations in Routine Care. Can. J. Cardiol. 2017, 33, 1036–1043. [Google Scholar] [CrossRef]
- Mueck, W.; Stampfuss, J.; Kubitza, D.; Becka, M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin. Pharmacokinet. 2014, 53, 1–16. [Google Scholar]
- Willmann, S.; Zhang, L.; Frede, M.; Kubitza, D.; Mueck, W.; Schmidt, S.; Solms, A.; Yan, X.; Garmann, D. Integrated Population Pharmacokinetic Analysis of Rivaroxaban Across Multiple Patient Populations. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 309–320. [Google Scholar] [CrossRef]
- Gibson, C.M.; Yuet, W.C. Racial and Ethnic Differences in Response to Anticoagulation: A Review of the Literature. J. Pharm. Pract. 2021, 34, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.F.; Joung, B.; Takahashi, Y.; Lim, T.W.; Choi, E.K.; Chan, Y.H.; Guo, Y.; Sriratanasathavorn, C.; Oh, S.; Okumura, K.; et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb. Haemost. 2022, 122, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Tanigawa, T.; Kaneko, M.; Hashizume, K.; Kajikawa, M.; Ueda, H.; Tajiri, M.; Paolini, J.F.; Mueck, W. Model-based dose selection for phase III rivaroxaban study in Japanese patients with non-valvular atrial fibrillation. Drug Metab. Pharmacokinet. 2013, 28, 59–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, M.; Tanigawa, T.; Hashizume, K.; Kajikawa, M.; Tajiri, M.; Mueck, W. Confirmation of model-based dose selection for a Japanese phase III study of rivaroxaban in non-valvular atrial fibrillation patients. Drug Metab. Pharmacokinet. 2013, 28, 321–331. [Google Scholar] [CrossRef]
- Wongcharoen, W.; Pacharasupa, P.; Norasetthada, L.; Gunaparn, S.; Phrommintikul, A. Anti-Factor Xa Activity of Standard and Japan-Specific Doses of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation. Circ. J. 2020, 84, 1075–1082. [Google Scholar] [CrossRef]
- Jonsson, E.N.; Karlsson, M.O. Xpose—An S-PLUS based population pharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput. Methods Programs Biomed. 1999, 58, 51–64. [Google Scholar] [CrossRef]
- Keizer, R.J.; van Benten, M.; Beijnen, J.H.; Schellens, J.H.; Huitema, A.D. Piraña and PCluster: A modeling environment and cluster infrastructure for NONMEM. Comput. Methods Programs Biomed. 2011, 101, 72–79. [Google Scholar] [CrossRef]
- Lindbom, L.; Ribbing, J.; Jonsson, E.N. Perl-speaks-NONMEM (PsN)—A Perl module for NONMEM related programming. Comput. Methods Programs Biomed. 2004, 75, 85–94. [Google Scholar] [CrossRef]
- Gisleskog, P.O.; Karlsson, M.O.; Beal, S.L. Use of prior information to stabilize a population data analysis. J. Pharmacokinet. Pharmacodyn. 2002, 29, 473–505. [Google Scholar] [CrossRef]
- Savic, R.M.; Karlsson, M.O. Importance of shrinkage in empirical bayes estimates for diagnostics: Problems and solutions. AAPS J. 2009, 11, 558–569. [Google Scholar] [CrossRef] [Green Version]
- Phrommintikul, A.; Detnuntarat, P.; Prasertwitayakij, N.; Wongcharoen, W. Prevalence of atrial fibrillation in Thai elderly. J. Geriatr. Cardiol. 2016, 13, 270–273. [Google Scholar] [PubMed]
- Akao, M.; Chun, Y.H.; Wada, H.; Esato, M.; Hashimoto, T.; Abe, M.; Hasegawa, K.; Tsuji, H.; Furuke, K.; Fushimi, A.F.; et al. Current status of clinical background of patients with atrial fibrillation in a community-based survey: The Fushimi AF Registry. J. Cardiol. 2013, 61, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.Q.; Zhang, Y.F.; Ding, H.Y.; Yan, M.M.; Jiao, Z.; Zhong, M.K.; Ma, C.L. Population pharmacokinetic and pharmacodynamic analysis of rivaroxaban in Chinese patients with non-valvular atrial fibrillation. Acta Pharmacol. Sin. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Chen, X.; Wu, T.; Huang, N.; Li, L.; Yuan, D.; Xiang, J.; Wang, N.; Chen, W.; Zhang, J. Population Pharmacokinetics of Rivaroxaban in Chinese Patients with Non-Valvular Atrial Fibrillation: A Prospective Multicenter Study. Clin. Pharmacokinet. 2022, 61, 881–893. [Google Scholar] [CrossRef]
- Lee, H.F.; Chan, Y.H.; Tu, H.T.; Kuo, C.T.; Yeh, Y.H.; Chang, S.H.; Wu, L.S.; See, L.C. The effectiveness and safety of low-dose rivaroxaban in Asians with non-valvular atrial fibrillation. Int. J. Cardiol. 2018, 261, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Wattanaruengchai, P.; Nathisuwan, S.; Rattanavipanon, W.; Chulavatnatol, S.; Kongwatcharapong, J.; Mitsuntisuk, P.; Chaiyasothi, T.; Kritsanapipat, D.; Phrommintikul, A.; Chaiyakunapruk, N.; et al. Prescriber compliance to direct oral anticoagulant labels and impact on outcomes in Thailand. Br. J. Clin. Pharmacol. 2021, 87, 1390–1400. [Google Scholar] [CrossRef]
- Girgis, I.G.; Patel, M.R.; Peters, G.R.; Moore, K.T.; Mahaffey, K.W.; Nessel, C.C.; Halperin, J.L.; Califf, R.M.; Fox, K.A.; Becker, R.C. Population pharmacokinetics and pharmacodynamics of rivaroxaban in patients with non-valvular atrial fibrillation: Results from ROCKET AF. J. Clin. Pharmacol. 2014, 54, 917–927. [Google Scholar] [CrossRef]
- Zhao, N.; Liu, Z.; Xie, Q.; Wang, Z.; Sun, Z.; Xiang, Q.; Cui, Y. A Combined Pharmacometrics Analysis of Biomarker Distribution Under Treatment with Standard- or Low-Dose Rivaroxaban in Real-World Chinese Patients with Nonvalvular Atrial Fibrillation. Front. Pharmacol. 2022, 13, 814724. [Google Scholar] [CrossRef]
- Mueck, W.; Eriksson, B.I.; Bauer, K.A.; Borris, L.; Dahl, O.E.; Fisher, W.D.; Gent, M.; Haas, S.; Huisman, M.V.; Kakkar, A.K.; et al. Population pharmacokinetics and pharmacodynamics of rivaroxaban—An oral, direct factor Xa inhibitor—In patients undergoing major orthopaedic surgery. Clin. Pharmacokinet. 2008, 47, 203–216. [Google Scholar] [CrossRef]
- Barsam, S.J.; Patel, J.P.; Roberts, L.N.; Kavarthapu, V.; Patel, R.K.; Green, B.; Arya, R. The impact of body weight on rivaroxaban pharmacokinetics. Res. Pract. Thromb. Haemost. 2017, 1, 180–187. [Google Scholar] [CrossRef]
- Speed, V.; Green, B.; Roberts, L.N.; Woolcombe, S.; Bartoli-Abdou, J.; Barsam, S.; Byrne, R.; Gee, E.; Czuprynska, J.; Brown, A.; et al. Fixed dose rivaroxaban can be used in extremes of bodyweight: A population pharmacokinetic analysis. J. Thromb. Haemost. 2020, 18, 2296–2307. [Google Scholar] [CrossRef] [PubMed]
- Esmaeili, T.; Rezaee, M.; Esfahani, M.A.; Davoudian, A.; Omidfar, D.; Rezaee, S. Rivaroxaban population pharmacokinetic and pharmacodynamic modeling in Iranian patients. J. Clin. Pharm. Ther. 2022. [Google Scholar] [CrossRef]
- Kubitza, D.; Becka, M.; Zuehlsdorf, M.; Mueck, W. Body weight has limited influence on the safety, tolerability, pharmacokinetics, or pharmacodynamics of rivaroxaban (BAY 59-7939) in healthy subjects. J. Clin. Pharmacol. 2007, 47, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Kubitza, D.; Becka, M.; Roth, A.; Mueck, W. The influence of age and gender on the pharmacokinetics and pharmacodynamics of rivaroxaban—An oral, direct Factor Xa inhibitor. J. Clin. Pharmacol. 2013, 53, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Konicki, R.; Weiner, D.; Patterson, J.H.; Gonzalez, D.; Kashuba, A.; Cao, Y.C.; Gehi, A.K.; Watkins, P.; Powell, J.R. Rivaroxaban Precision Dosing Strategy for Real-World Atrial Fibrillation Patients. Clin. Transl. Sci. 2020, 13, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Gosselin, R.C.; Adcock, D.M.; Bates, S.M.; Douxfils, J.; Favaloro, E.J.; Gouin-Thibault, I.; Guillermo, C.; Kawai, Y.; Lindhoff-Last, E.; Kitchen, S. International Council for Standardization in Haematology (ICSH) Recommendations for Laboratory Measurement of Direct Oral Anticoagulants. Thromb. Haemost. 2018, 118, 437–450. [Google Scholar] [CrossRef] [Green Version]
- Königsbrügge, O.; Quehenberger, P.; Belik, S.; Weigel, G.; Seger, C.; Griesmacher, A.; Pabinger, I.; Ay, C. Anti-coagulation assessment with prothrombin time and anti-Xa assays in real-world patients on treatment with rivaroxaban. Ann. Hematol. 2015, 94, 1463–1471. [Google Scholar] [CrossRef]
- Mueck, W.; Kubitza, D.; Becka, M. Co-administration of rivaroxaban with drugs that share its elimination pathways: Pharmacokinetic effects in healthy subjects. Br. J. Clin. Pharmacol. 2013, 76, 455–466. [Google Scholar] [CrossRef] [Green Version]
- Zdovc, J.; Petre, M.; Pišlar, M.; Repnik, K.; Mrhar, A.; Vogrin, M.; Potočnik, U.; Grabnar, I. Downregulation of ABCB1 gene in patients with total hip or knee arthroplasty influences pharmacokinetics of rivaroxaban: A population pharmacokinetic-pharmacodynamic study. Eur. J. Clin. Pharmacol. 2019, 75, 817–824. [Google Scholar] [CrossRef]
- Kubitza, D.; Roth, A.; Becka, M.; Alatrach, A.; Halabi, A.; Hinrichsen, H.; Mueck, W. Effect of hepatic impairment on the pharmacokinetics and pharmacodynamics of a single dose of rivaroxaban, an oral, direct Factor Xa inhibitor. Br. J. Clin. Pharmacol. 2013, 76, 89–98. [Google Scholar] [CrossRef]
- Qian, J.; Yan, Y.D.; Yang, S.Y.; Zhang, C.; Li, W.Y.; Gu, Z.C. Benefits and Harms of Low-Dose Rivaroxaban in Asian Patients with Atrial Fibrillation: A Systematic Review and Meta-analysis of Real-World Studies. Front. Pharmacol. 2021, 12, 642907. [Google Scholar] [CrossRef] [PubMed]
- Shimokawa, H.; Yamashita, T.; Uchiyama, S.; Kitazono, T.; Shimizu, W.; Ikeda, T.; Kamouchi, M.; Kaikita, K.; Fukuda, K.; Origasa, H. The EXPAND study: Efficacy and safety of rivaroxaban in Japanese patients with non-valvular atrial fibrillation. Int. J. Cardiol. 2018, 258, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, W.H.; Chao, T.F.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P.; Lip, G.Y.H.; et al. Low-Dose Rivaroxaban and Risks of Adverse Events in Patients with Atrial Fibrillation. Stroke 2019, 50, 2574–2577. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Male, n (%) | 38 (63.3) |
| Age (y), mean (SD) | 69.4 (9.2) |
| Body weight (kg), mean (SD) | 64.0 (14.1) |
| Body mass index (kg/m2), median (Q1, Q3) | 24.2 (21.5, 26.9) |
| Creatinine (mg/dL), mean (SD) | 1.1 (0.3) |
| Creatinine clearance (mL/min), mean (SD) | 59.0 (22.8) |
| CHADS2 score, median (Q1, Q3) | 2 (1, 2) |
| CHA2 DS2-VASC score, median (Q1, Q3) | 3 (2, 4) |
| HAS-BLED score, median (Q1, Q3) | 2 (1, 2) |
| Underlying disease, n (%) | |
| Hypertension | 46 (76.7) |
| Dyslipidemia | 35 (58.3) |
| Diabetes | 16 (26.7) |
| Congestive heart failure | 15 (25.0) |
| Ischemic heart disease | 8 (13.3) |
| Ischemic stroke | 7 (11.7) |
| Concomitant medications, n (%) | |
| Dronedarone | 3 (5.0) |
| Amiodarone | 1 (1.7) |
| Aspirin | 1 (1.7) |
| Clopidogrel | 1 (1.7) |
| Parameters | Final Model (NONMEM) | Bootstrap Analysis (n = 1000 Samples) | ||
|---|---|---|---|---|
| Estimates a [RSE%] | 95% CI * | Median b [RSE%] | 95% CI ** | |
| CL/F (L/h) | 4.19 [3.8%] | 3.88–4.50 | 4.21 [4.08] | 3.88–4.55 |
| V/F (L) | 37.5 [4.7%] | 34.03–40.97 | 37.59 [4.62%] | 34.0–40.8 |
| ka (h−1) | 0.697 [10.7%] | 0.550–0.844 | 0.699 [5.06%] | 0.623–0.764 |
| CrCl on CL/F c | 0.277 [29%] | 0.120–0.434 | 0.277 [35.2%] | 0.054–0.480 |
| WT on V/F d | 0.412 [35.7%] | 0.124–0.70 | 0.413 [28.1%] | 0.149–0.639 |
| IIV of CL/F (%CV) | 21.94 [21.3%] | 16.67–26.24 | 21.24 [14.7%] | 14.8–27.5 |
| IIV of ka (%CV) | 75.91 [10.1%] | 66.39–85.10 | 75.81 [1.08%] | 74.1–78.1 |
| RUV, additive (mg/L) | 0.092 [11.7%] | 0.071–0.114 | 0.0926 [9.44%] | 0.064–0.131 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singkham, N.; Phrommintikul, A.; Pacharasupa, P.; Norasetthada, L.; Gunaparn, S.; Prasertwitayakij, N.; Wongcharoen, W.; Punyawudho, B. Population Pharmacokinetics and Dose Optimization Based on Renal Function of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation. Pharmaceutics 2022, 14, 1744. https://doi.org/10.3390/pharmaceutics14081744
Singkham N, Phrommintikul A, Pacharasupa P, Norasetthada L, Gunaparn S, Prasertwitayakij N, Wongcharoen W, Punyawudho B. Population Pharmacokinetics and Dose Optimization Based on Renal Function of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation. Pharmaceutics. 2022; 14(8):1744. https://doi.org/10.3390/pharmaceutics14081744
Chicago/Turabian StyleSingkham, Noppaket, Arintaya Phrommintikul, Phongsathon Pacharasupa, Lalita Norasetthada, Siriluck Gunaparn, Narawudt Prasertwitayakij, Wanwarang Wongcharoen, and Baralee Punyawudho. 2022. "Population Pharmacokinetics and Dose Optimization Based on Renal Function of Rivaroxaban in Thai Patients with Non-Valvular Atrial Fibrillation" Pharmaceutics 14, no. 8: 1744. https://doi.org/10.3390/pharmaceutics14081744