
Preparation and Characterisation of a Cyclodextrin-Complexed Mānuka Honey Microemulsion for Eyelid Application

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Antibacterial Activity of MH, CYP, and α-CD
2.3. Corneal Tolerability of MH, CYP, and α-CD
2.4. Formulation Development and Characterisation
2.5. Antibacterial Activity of the Formulation
2.5.1. Minimum Bactericidal Concentration
2.5.2. Zone Inhibition Test
2.5.3. Direct Inoculation Assay
2.6. Corneal Tolerability of the Formulation
2.7. Vascular Tolerability of the Formulation
3. Results and Discussion
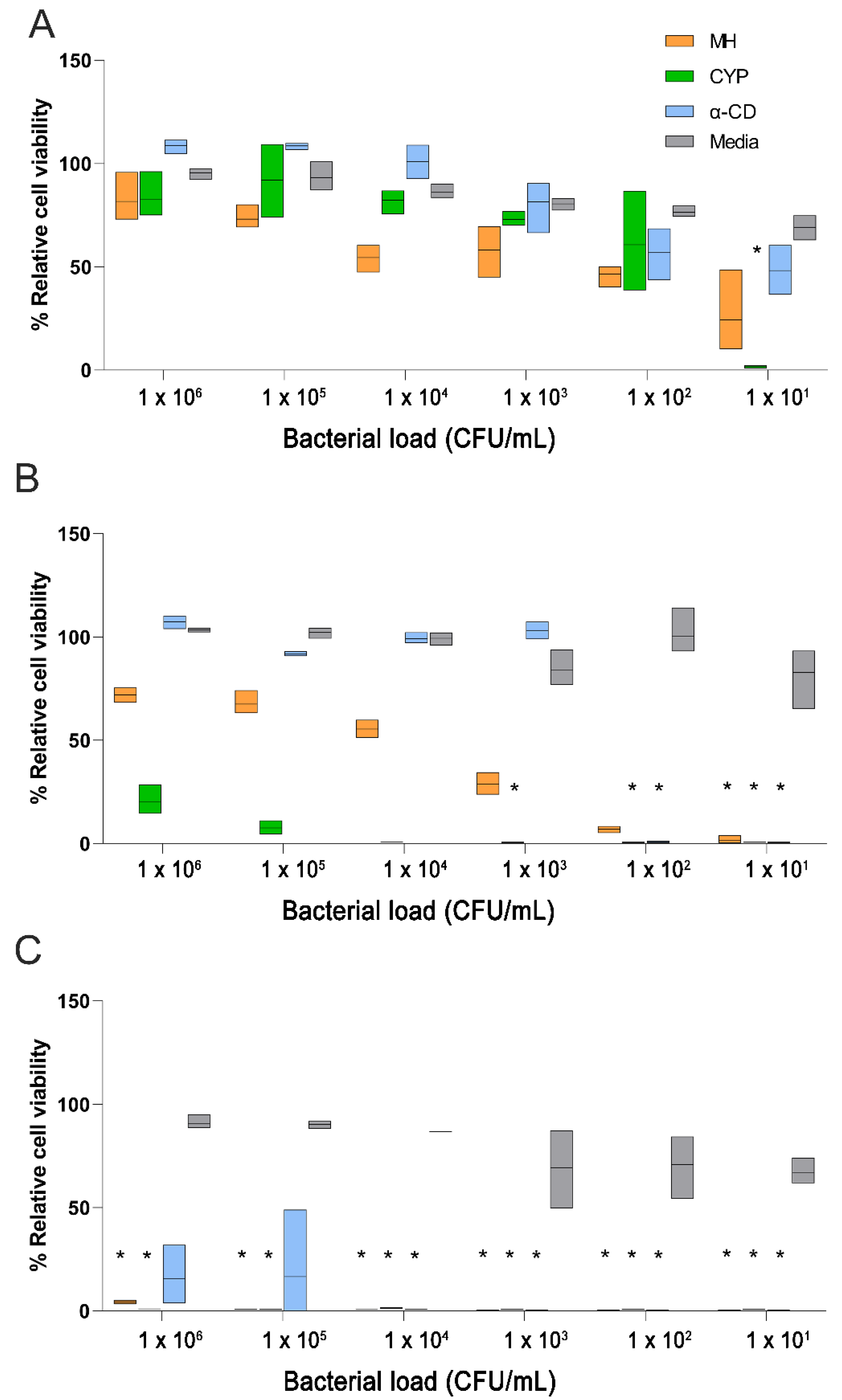
3.1. Antibacterial Activity of MH, CYP, and α-CD
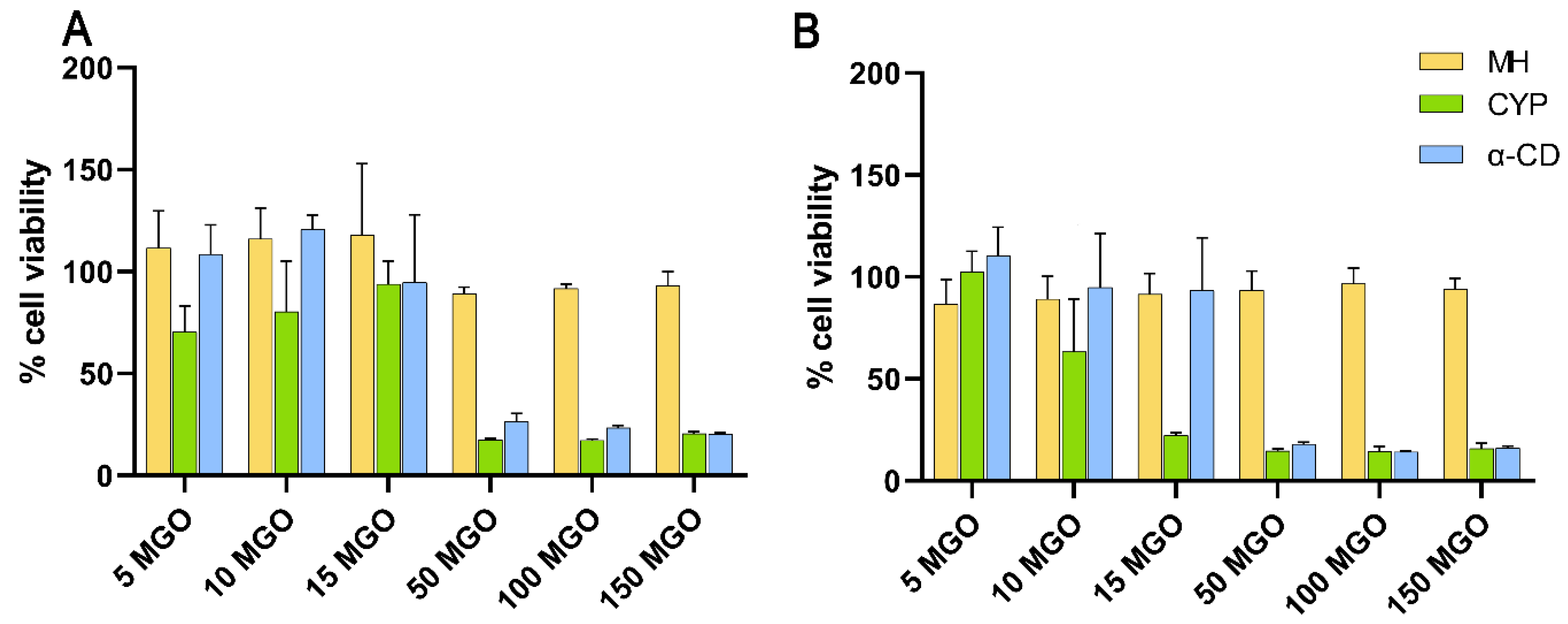
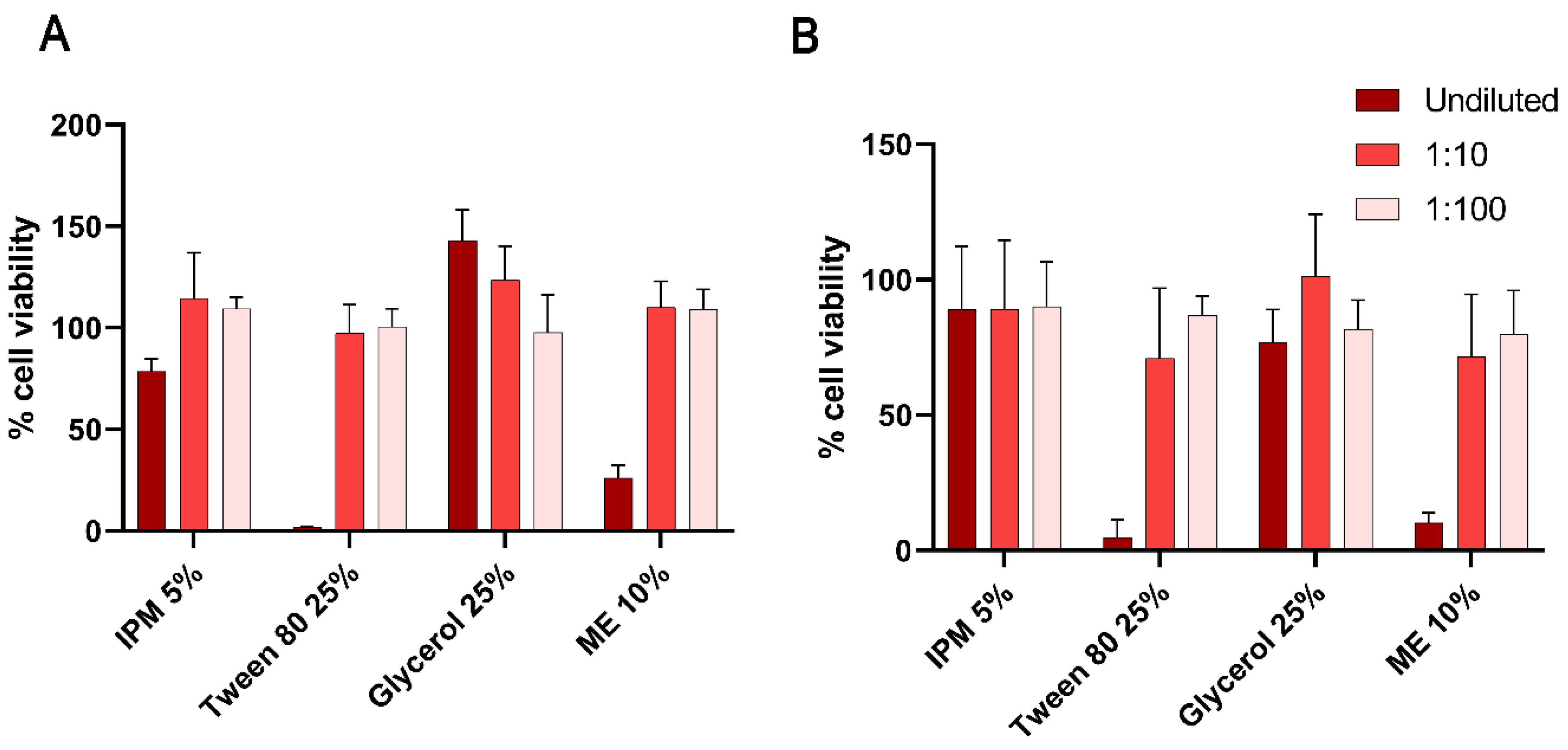
3.2. Corneal Tolerability of MH, CYP, and α-CD
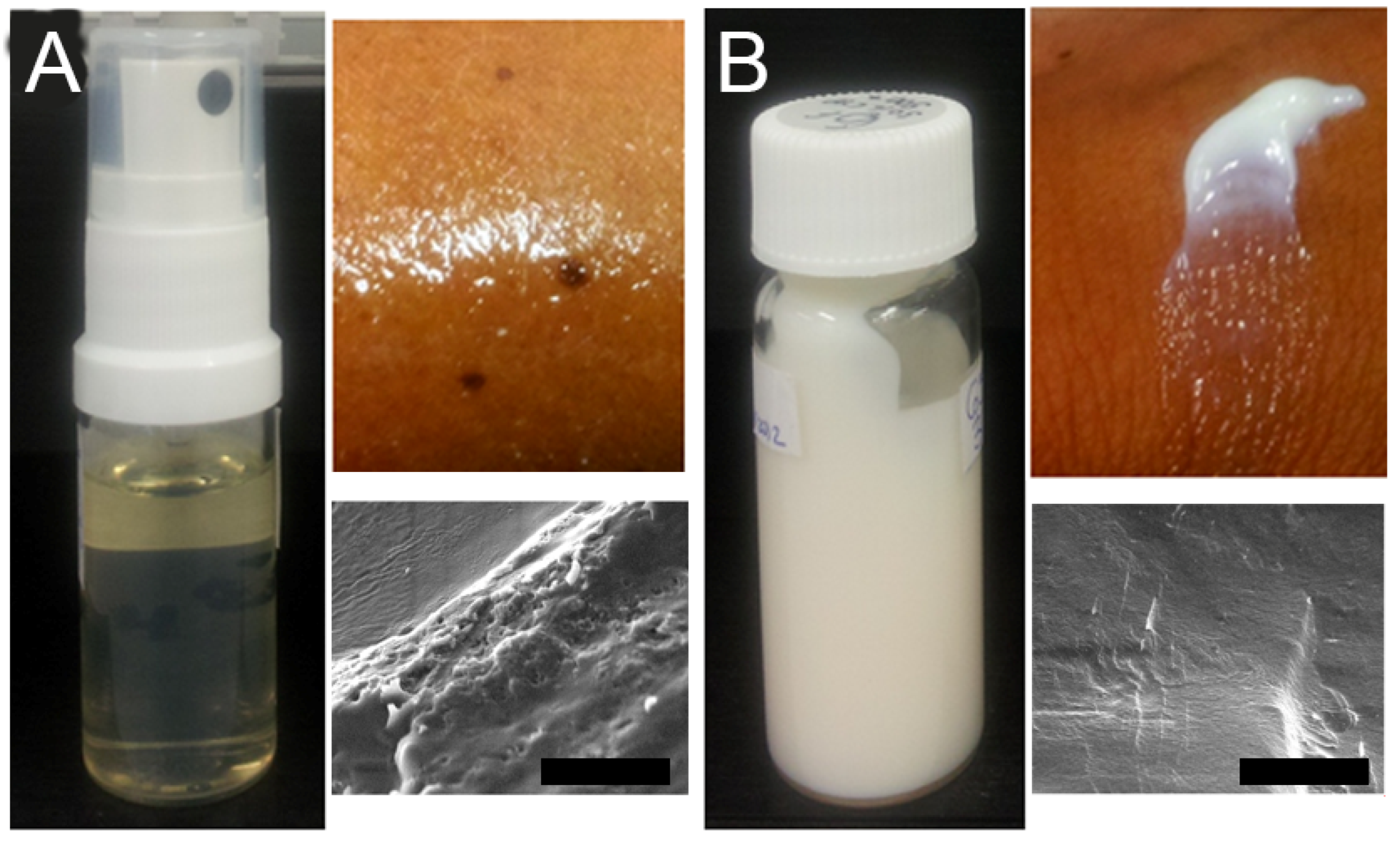
3.3. Formulation Development and Characterisation
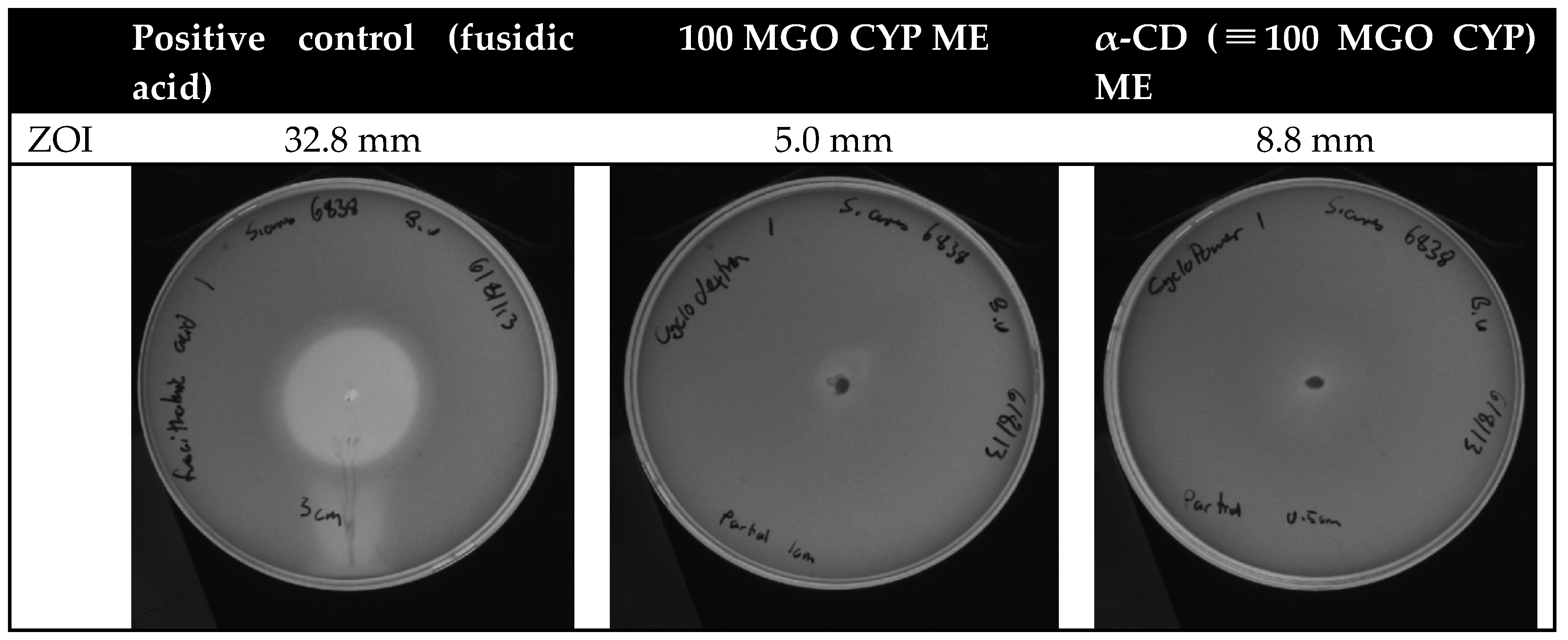
3.4. Antibacterial Activity of the Formulation
3.5. Corneal Tolerability of the Formulation
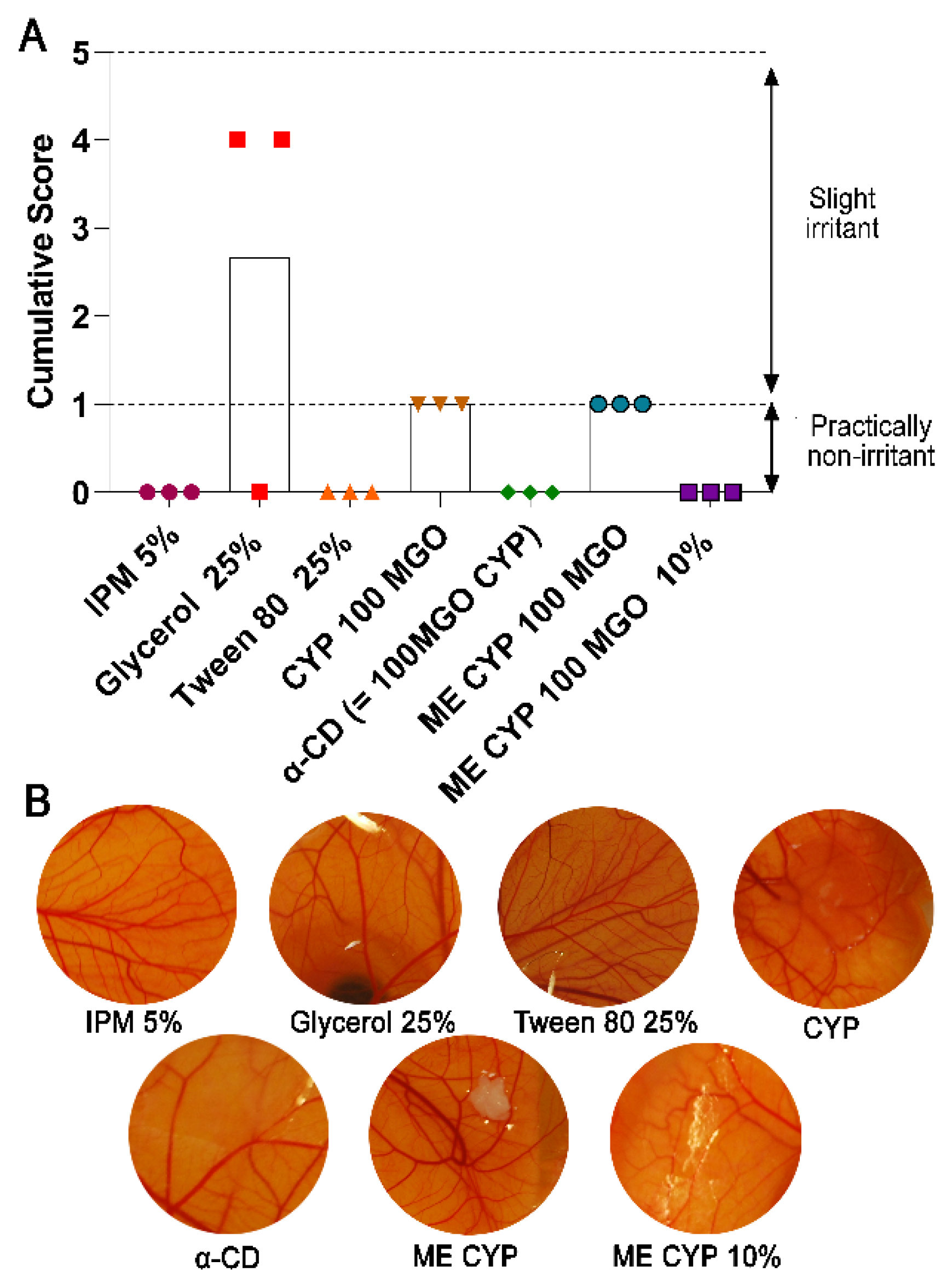
3.6. Vascular Tolerability of the Formulation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carter, D.A.; Blair, S.E.; Cokcetin, N.N.; Bouzo, D.; Brooks, P.; Schothauer, R.; Harry, E.J. Therapeutic Manuka Honey: No Longer So Alternative. Front. Microbiol. 2016, 7, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kot, B.; Sytykiewicz, H.; Sprawka, I.; Witeska, M. Effect of manuka honey on biofilm-associated genes expression during methicillin-resistant Staphylococcus aureus biofilm formation. Sci. Rep. 2020, 10, 13552. [Google Scholar] [CrossRef] [PubMed]
- Balan, P.; Mal, G.; Das, S.; Singh, H. Synergistic and Additive Antimicrobial Activities of Curcumin, Manuka Honey and Whey Proteins. J. Food Biochem. 2016, 40, 647–654. [Google Scholar] [CrossRef]
- Lu, J.; Turnbull, L.; Burke, C.M.; Liu, M.; Carter, D.A.; Schlothauer, R.C.; Whitchurch, C.B.; Harry, E.J. Manuka-type honeys can eradicate biofilms produced by Staphylococcus aureus strains with different biofilm-forming abilities. PeerJ 2014, 2, e326. [Google Scholar] [CrossRef] [Green Version]
- George, N.M.; Cutting, K.F. Antibacterial Honey (Medihoney™): In-Vitro Activity against Clinical Isolates of MRSA, VRE, and Other Multiresistant Gram-Negative Organisms Including Pseudomonas aeruginosa. Wounds 2007, 19, 231–236. [Google Scholar] [PubMed]
- Blair, S.E.; Cokcetin, N.N.; Harry, E.J.; Carter, D.A. The unusual antibacterial activity of medical-grade Leptospermum honey: Antibacterial spectrum, resistance and transcriptome analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.A.; Jenkins, L.; Henriques, A.F.; Duggan, R.S.; Burton, N.F. Absence of bacterial resistance to medical-grade manuka honey. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1237–1241. [Google Scholar] [CrossRef] [Green Version]
- Johnston, M.; McBride, M.; Dahiya, D.; Owusu-Apenten, R.; Nigam, P.S. Antibacterial activity of Manuka honey and its components: An overview. AIMS Microbiol. 2018, 4, 655–664. [Google Scholar] [CrossRef]
- Salonen, A.; Virjamo, V.; Tammela, P.; Fauch, L.; Julkunen-Tiitto, R. Screening bioactivity and bioactive constituents of Nordic unifloral honeys. Food Chem. 2017, 237, 214–224. [Google Scholar] [CrossRef] [Green Version]
- Mavric, E.; Wittmann, S.; Barth, G.; Henle, T. Identification and quantification of methylglyoxal as the dominant antibacterial constituent of Manuka (Leptospermum scoparium) honeys from New Zealand. Mol. Nutr. Food Red. 2008, 52, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.G.; Herst, P.M.; Harper, J.L. Indigenous New Zealand honeys exhibit multiple anti-inflammatory activities. Innate Immun. 2012, 18, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCulley, J.P.; Dougherty, J.M.; Deneau, D.G. Classification of chronic blepharitis. Ophthalmology 1982, 89, 1173–1180. [Google Scholar] [CrossRef]
- Putnam, C.M. Diagnosis and management of blepharitis: An optometrist’s perspective. Clin. Optom. 2016, 8, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemp, M.A.; Nichols, K.K. Blepharitis in the United States 2009, A Survey-Based Perspective on Prevalence and Treatment. Ocul. Surf. 2009, 7 (Suppl. S2), S1–S14. [Google Scholar] [CrossRef]
- Lindsley, K.; Matsumura, S.; Hatef, E.; Akpek, E.K. Interventions for Chronic blepharitis. Cochrane Database Syst. Rev. 2012, 2012, CD005556. [Google Scholar] [CrossRef] [PubMed]
- Albietz, J.M.; Lenton, L.M. Effect of antibacterial honey on the ocular flora in tear deficiency and meibomian gland disease. Cornea 2006, 25, 1012–1019. [Google Scholar] [CrossRef]
- Frame, K.; Cheung, I.M.Y.; Wang, M.T.M.; Turnbull, P.R.; Watters, G.A.; Craig, J.P. Comparing the in vitro effects of MGO™ Manuka honey and tea tree oil on ocular Demodex viability. Contact Lens Anterior Eye 2018, 41, 527–530. [Google Scholar] [CrossRef]
- Craig, J.P.; Rupenthal, I.D.; Seyfoddin, A.; Cheung, I.M.Y.; Uy, B.; Wang, M.T.M.; Watters, G.A.; Swift, S. Preclinical development of MGO Manuka Honey microemulsion for blepharitis management. BMJ Open Ophthalmol. 2017, 1, e000065. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.P.; Tomlinson, A. Importance of the lipid layer in human tear film stability and evaporation. Optom. Vis. Sci. 1997, 74, 8–13. [Google Scholar] [CrossRef]
- Thakur, S.S.; Solloway, J.; Stikkelman, A.; Seyfoddin, A.; Rupenthal, I.D. Phase transition of a microemulsion upon addition of cyclodextrin—Applications in drug delivery. Pharm. Dev. Technol. 2018, 23, 167–175. [Google Scholar] [CrossRef]
- Franco, P.; De Marco, I. Preparation of non-steroidal anti-inflammatory drug/β-cyclodextrin inclusion complexes by supercritical antisolvent process. J. CO2 Util. 2021, 44, 101397. [Google Scholar] [CrossRef]
- Yan, T.; Ji, M.; Sun, Y.; Yan, T.; Zhao, J.; Zhang, H.; Wang, Z. Preparation and characterization of baicalein/hydroxypropyl-β-cyclodextrin inclusion complex for enhancement of solubility, antioxidant activity and antibacterial activity using supercritical antisolvent technology. J. Incl. Phenom. Macrocycl. Chem. 2020, 96, 285–295. [Google Scholar] [CrossRef]
- Vichai, V.; Kirtikara, K. Sulforhodamine B colorimetric assay for cytotoxicity screening. Nat. Protoc. 2006, 1, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Habib, F.; El-Mahdy, M.; Maher, S. Microemulsions for ocular delivery: Evaluation and characterization. J. Drug Deliv. Sci. Technol. 2011, 21, 485–489. [Google Scholar] [CrossRef]
- Alany, R.G.; Rades, T.; Nicoll, J.; Tucker, I.G.; Davies, N.M. W/O microemulsions for ocular delivery: Evaluation of ocular irritation and precorneal retention. J. Control. Release 2006, 111, 145–152. [Google Scholar] [CrossRef]
- Luepke, N.P. Hen’s egg chorioallantoic membrane test for irritation potential. Food Chem. Toxicol. 1985, 23, 287–291. [Google Scholar] [CrossRef]
- Watters, G.A.; Turnbull, P.R.; Swift, S.; Petty, A.; Craig, J.P. Ocular surface microbiome in meibomian gland dysfunction. Clin. Exp. Ophthalmol. 2017, 45, 105–111. [Google Scholar] [CrossRef]
- Lee, S.H.; Oh, D.H.; Jung, J.Y.; Kim, J.C.; Jeon, C.O. Comparative Ocular Microbial Communities in Humans with and without Blepharitis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5585–5593. [Google Scholar] [CrossRef] [Green Version]
- Swift, S.; Chepulis, L.M.; Uy, B.; Radcliff, F.J. Enhanced antibacterial activity of MGOTM manuka honey complexed with α- cyclodextrin (manuka honey with CycloPowerTM). Funct. Foods Health Dis. 2014, 4, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; Cheng, C.; Yi, H.; Lin, L.; Wu, K. Quantitative Analysis of the Bacteria in Blepharitis with Demodex Infestation. Front. Microbiol. 2018, 9, 1719. [Google Scholar] [CrossRef] [Green Version]
- Thakur, A.; Jain, S.; Pant, A.; Sharma, A.; Kumar, R.; Singla, N.; Suttee, A.; Kumar, S.; Barnwal, R.P.; Katare, O.P.; et al. Cyclodextrin derivative enhances the ophthalmic delivery of poorly soluble Azithromycin. ACS Omega 2022, 7, 23050–23060. [Google Scholar] [CrossRef]
- Inoue, Y.; Suzuki, R.; Murata, I.; Nomura, H.; Isshiki, Y.; Kanamoto, I. Evaluation of Antibacterial Activity Expression of the Hinokitiol/Cyclodextrin Complex against Bacteria. ACS Omega 2020, 5, 27180–27187. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Yuan, Q.; Vriesekoop, F.; Lv, F. Effects of cyclodextrins on the antimicrobial activity of plant-derived essential oil compounds. Food Chem. 2012, 135, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Mao, X.; Sun, Y.; Cui, H. Antibacterial mechanism of artemisinin/beta-cyclodextrins against methicillin-resistant Staphylococcus aureus (MRSA). Microb. Pathog. 2018, 118, 66–73. [Google Scholar] [CrossRef]
- Mourtzinos, I.; Makris, D.P.; Yannakopoulou, K.; Kalogeropoulos, N.; Michali, I.; Karathanos, V.T. Thermal Stability of Anthocyanin Extract of Hibiscus sabdariffa L. in the Presence of β-Cyclodextrin. J. Agric. Food Chem. 2008, 56, 10303–10310. [Google Scholar] [CrossRef]
- Saarinen-Savolainen, P.; Järvinen, T.; Araki-Sasaki, K.; Watanabe, H.; Urtti, A. Evaluation of Cytotoxicity of Various Ophthalmic Drugs, Eye Drop Excipients and Cyclodextrins in an Immortalized Human Corneal Epithelial Cell Line. Pharm. Res. 1998, 15, 1275–1280. [Google Scholar] [CrossRef]
- Kanai, A.; Alba, R.M.; Takano, T.; Kobayashi, C.; Nakajima, A.; Kurihara, K.; Yokoyama, T.; Fukami, M. The effect on the cornea of alpha cyclodextrin vehicle for cyclosporin eye drops. Transplant. Proc. 1989, 21 Pt 3, 3150–3152. [Google Scholar]
- Irie, T.; Uekama, K. Pharmaceutical applications of cyclodextrins. III. Toxicological issues and safety evaluation. J. Pharm. Sci. 1997, 86, 147–162. [Google Scholar] [CrossRef]
- Róka, E.; Ujhelyi, Z.; Deli, M.; Bocsik, A.; Fenyvesi, É.; Szente, L.; Fenyvesi, F.; Vecsernyés, M.; Váradi, J.; Fehér, P.; et al. Evaluation of the Cytotoxicity of α-Cyclodextrin Derivatives on the Caco-2 Cell Line and Human Erythrocytes. Molecules 2015, 20, 20269–20285. [Google Scholar] [CrossRef] [Green Version]
- Jóhannsdóttir, S.; Kristinsson, J.K.; Fülöp, Z.; Ásgrímsdóttir, G.; Stefánsson, E.; Loftsson, T. Formulations and toxicologic in vivo studies of aqueous cyclosporin A eye drops with cyclodextrin nanoparticles. Int. J. Pharm. 2017, 529, 486–490. [Google Scholar] [CrossRef]
- Loftsson, T.; Stefánsson, E. Cyclodextrins and topical drug delivery to the anterior and posterior segments of the eye. Int. J. Pharm. 2017, 531, 413–423. [Google Scholar] [CrossRef]
- Loftsson, T.; Stefánsson, E. Aqueous eye drops containing drug/cyclodextrin nanoparticles deliver therapeutic drug concentrations to both anterior and posterior segment. Acta Ophthalmol. 2022, 100, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Svirskis, D.; Alany, R.G.; Zargar-Shoshtari, S.; Wu, Z. In-situ phase transition from microemulsion to liquid crystal with the potential of prolonged parenteral drug delivery. Int. J. Pharm. 2012, 431, 130–137. [Google Scholar] [CrossRef]
- Uchino, M.; Tsubota, K. Tear Film Overview. In Encyclopedia of the Eye; Dartt, D.A., Ed.; Academic Press: Oxford, UK, 2010; pp. 263–268. [Google Scholar]
- Ujhelyi, Z.; Fenyvesi, F.; Váradi, J.; Fehér, P.; Kiss, T.; Veszelka, S.; Deli, M.; Vecsernyés, M.; Bácskay, I. Evaluation of cytotoxicity of surfactants used in self-micro emulsifying drug delivery systems and their effects on paracellular transport in Caco-2 cell monolayer. Eur. J. Pharm. Sci. 2012, 47, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Arechabala, B.; Coiffard, C.; Rivalland, P.; Coiffard, L.J.; de Roeck-Holtzhauer, Y. Comparison of cytotoxicity of various surfactants tested on normal human fibroblast cultures using the neutral red test, MTT assay and LDH release. J. Appl. Toxicol. 1999, 19, 163–165. [Google Scholar] [CrossRef]
- Spielmann, H.; Kalweit, S.; Liebsch, M.; Wirnsberger, T.; Gerner, I.; Bertram-Neis, E.; Krauser, K.; Kreiling, R.; Miltenburger, H.G.; Pape, W.; et al. Validation study of alternatives to the Draize eye irritation test in Germany: Cytotoxicity testing and HET-CAM test with 136 industrial chemicals. Toxicol. Vitr. 1993, 7, 505–510. [Google Scholar] [CrossRef]
- McNamee, P.; Hibatallah, J.; Costabel-Farkas, M.; Goebel, C.; Araki, D.; Dufour, E.; Hewitt, N.J.; Jones, P.; Kirst, A.; le Varlet, B.; et al. A tiered approach to the use of alternatives to animal testing for the safety assessment of cosmetics: Eye irritation. Regul. Toxicol. Pharmacol. 2009, 54, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.P.; Cruzat, A.; Cheung, I.M.Y.; Watters, G.A.; Wang, M.T.M. Randomized masked trial of the clinical efficacy of MGO Manuka Honey microemulsion eye cream for the treatment of blepharitis. Ocul. Surf. 2020, 18, 170–177. [Google Scholar] [CrossRef]
- Craig, J.P.; Wang, M.T.M.; Ganesalingam, K.; Rupenthal, I.D.; Swift, S.; Loh, C.S.; Weehi, L.T.; Cheung, I.M.Y.; Watters, G.A. Randomised masked trial of the clinical safety and tolerability of MGO Manuka Honey eye cream for the management of blepharitis. BMJ Open Ophthalmol. 2017, 1, e000066. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Dilution in PBS | pH | Osmolarity (mOsmol/kg) |
|---|---|---|---|
| Tween 80 | undiluted | N/A | N/A |
| Tween 80 (25% w/v) | 1:4 | 4.07 ± 0.04 | 474.00 ± 15.10 |
| IPM | undiluted | N/A | N/A |
| IPM (5% w/v) | 1:20 | 7.23 ± 0.05 | 297.00 ± 10.82 |
| Glycerol | undiluted | N/A | N/A |
| Glycerol (25% w/v) | 1:4 | 7.07 ± 0.27 | 3705.67 ± 53.26 |
| ME | undiluted | 4.73 ± 0.04 | * |
| ME | 1:10 | 7.12 ± 0.01 | 611.67 ± 8.74 |
| α-CD (≡100 MGO CYP) | undiluted | 7.27 ± 0.02 | 411.33 ± 10.07 |
| 100 MGO CYP | undiluted | 5.49 ± 0.95 | 1431.00 ± 170.77 |
| 100 MGO CYP ME | undiluted | 4.18 ± 0.02 | * |
| 100 MGO CYP ME | 1:10 | 6.50 ± 0.01 | 587.00 ± 6.08 |
| 100 MGO CYP ME | 1:100 | 7.13 ± 0.01 | 323.33 ± 3.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rupenthal, I.D.; Agarwal, P.; Uy, B.; Kim, J.; Cunningham, A.A.; Seyfoddin, A.; Swift, S.; Craig, J.P. Preparation and Characterisation of a Cyclodextrin-Complexed Mānuka Honey Microemulsion for Eyelid Application. Pharmaceutics 2022, 14, 1493. https://doi.org/10.3390/pharmaceutics14071493
Rupenthal ID, Agarwal P, Uy B, Kim J, Cunningham AA, Seyfoddin A, Swift S, Craig JP. Preparation and Characterisation of a Cyclodextrin-Complexed Mānuka Honey Microemulsion for Eyelid Application. Pharmaceutics. 2022; 14(7):1493. https://doi.org/10.3390/pharmaceutics14071493
Chicago/Turabian StyleRupenthal, Ilva D., Priyanka Agarwal, Benedict Uy, Jaeun Kim, Angela A. Cunningham, Ali Seyfoddin, Simon Swift, and Jennifer P. Craig. 2022. "Preparation and Characterisation of a Cyclodextrin-Complexed Mānuka Honey Microemulsion for Eyelid Application" Pharmaceutics 14, no. 7: 1493. https://doi.org/10.3390/pharmaceutics14071493