
Hyaluronic Acid: Its Versatile Use in Ocular Drug Delivery with a Specific Focus on Hyaluronic Acid-Based Polyelectrolyte Complexes

 ,
,  , and
, and
Abstract
:1. Introduction
2. Hyaluronic Acid: “Nature’s Sponge”
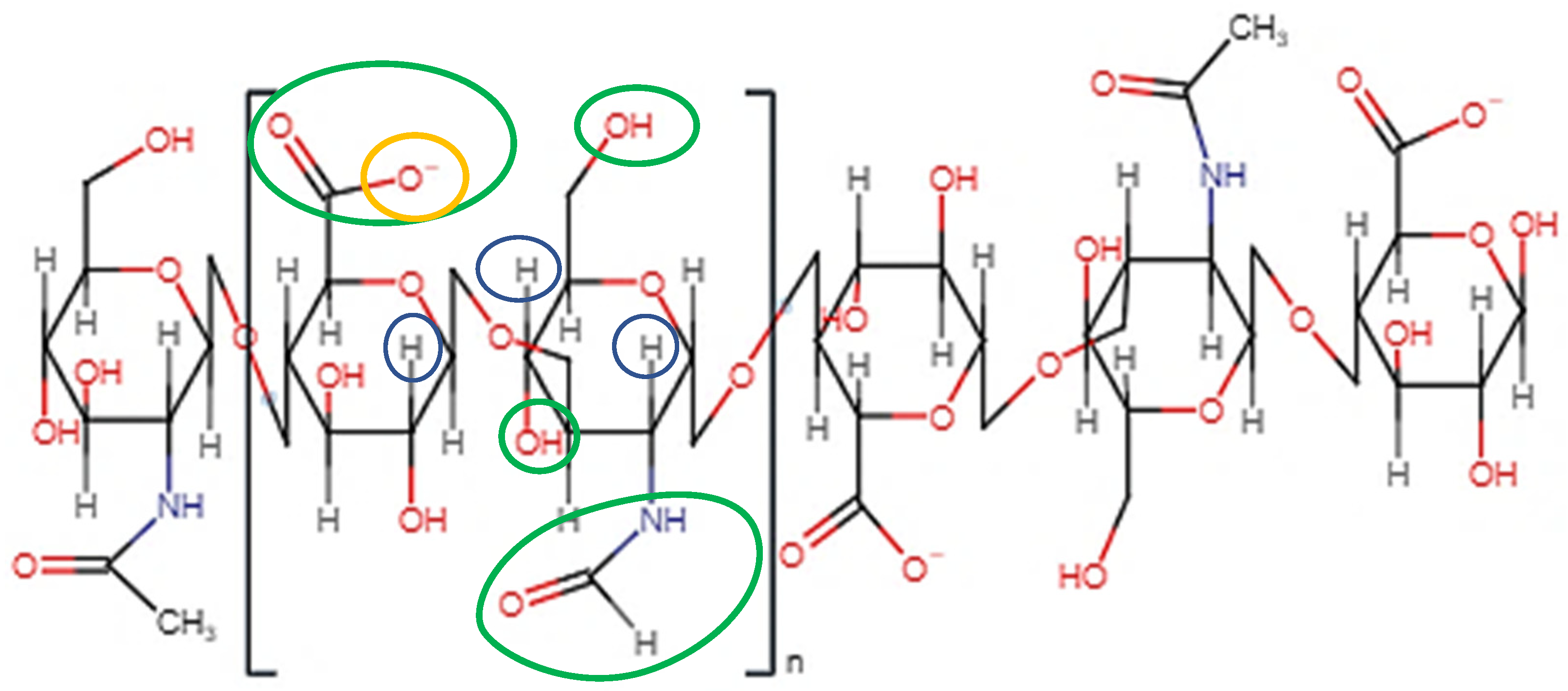
2.1. Molecular Structure
2.2. Ionisation and Rheological Properties
2.3. Biological Properties of HA
2.3.1. HA—A Fundamental Component of Vitreous Humour
2.3.2. HA and Mucoadhesion
2.3.3. HA-CD44 Binding: An Essential Cellular Signalling Mechanism
2.3.4. The Relationship between HA MW and Biological Activity
2.4. Enzymatic Degradation of HA
2.5. Potential Cytotoxicity of HA under Inflammatory Conditions
3. Hyaluronic Acid Biomaterials for Ocular Drug Delivery
3.1. Artificial Tears for Dry Eye Disease
3.2. Eye Drop Formulations—Viscosity, Mucoadhesion, and Solubility Enhancement
3.3. In Situ-Forming Hydrogel Systems
3.3.1. Injectable Formulations
3.3.2. Vitreous Substitutes
3.4. HA-Based Topical Gels
3.5. Contact Lenses: Comfort and Wettability via HA Modification
3.6. HA-Based Nanoformulations
3.6.1. Enhanced Pharmacokinetics of HA-Based Nanoformulations
3.6.2. Cytotoxicity and Safety of HA-Based Nanoformulations
3.7. Clinical Applications of HA-Based Ocular Drug Delivery Systems
4. HA Polyelectrolyte Complexes
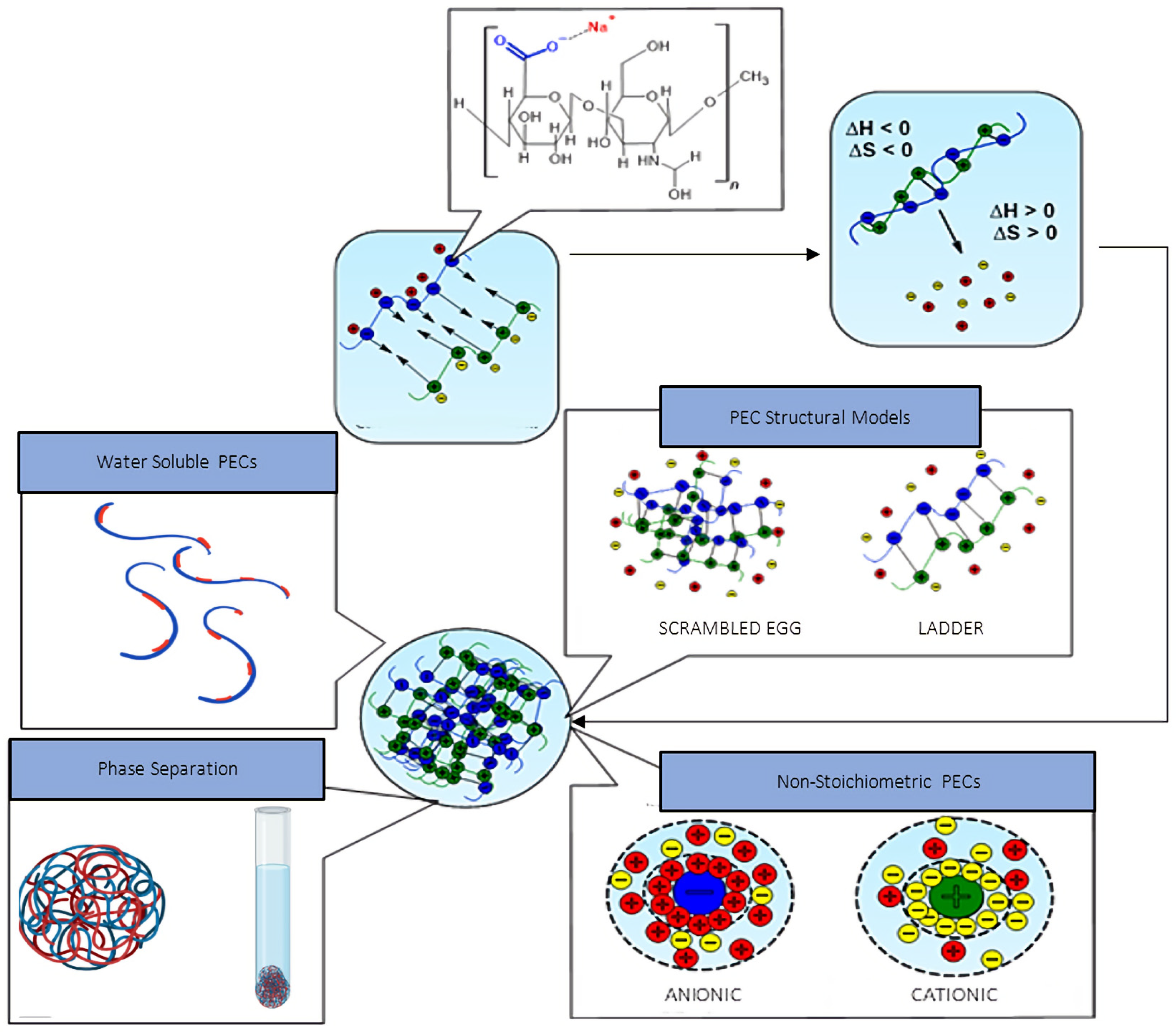
4.1. Polyelectrolyte Complex Assembly Mechanism
4.2. Thermodynamics of Polyelectrolyte Complexation
4.3. Applications of HA Polyelectrolyte Complexes in Ocular Drug Delivery
4.4. HA-PECs: Design Considerations and Critical Quality Attributes
4.4.1. pH
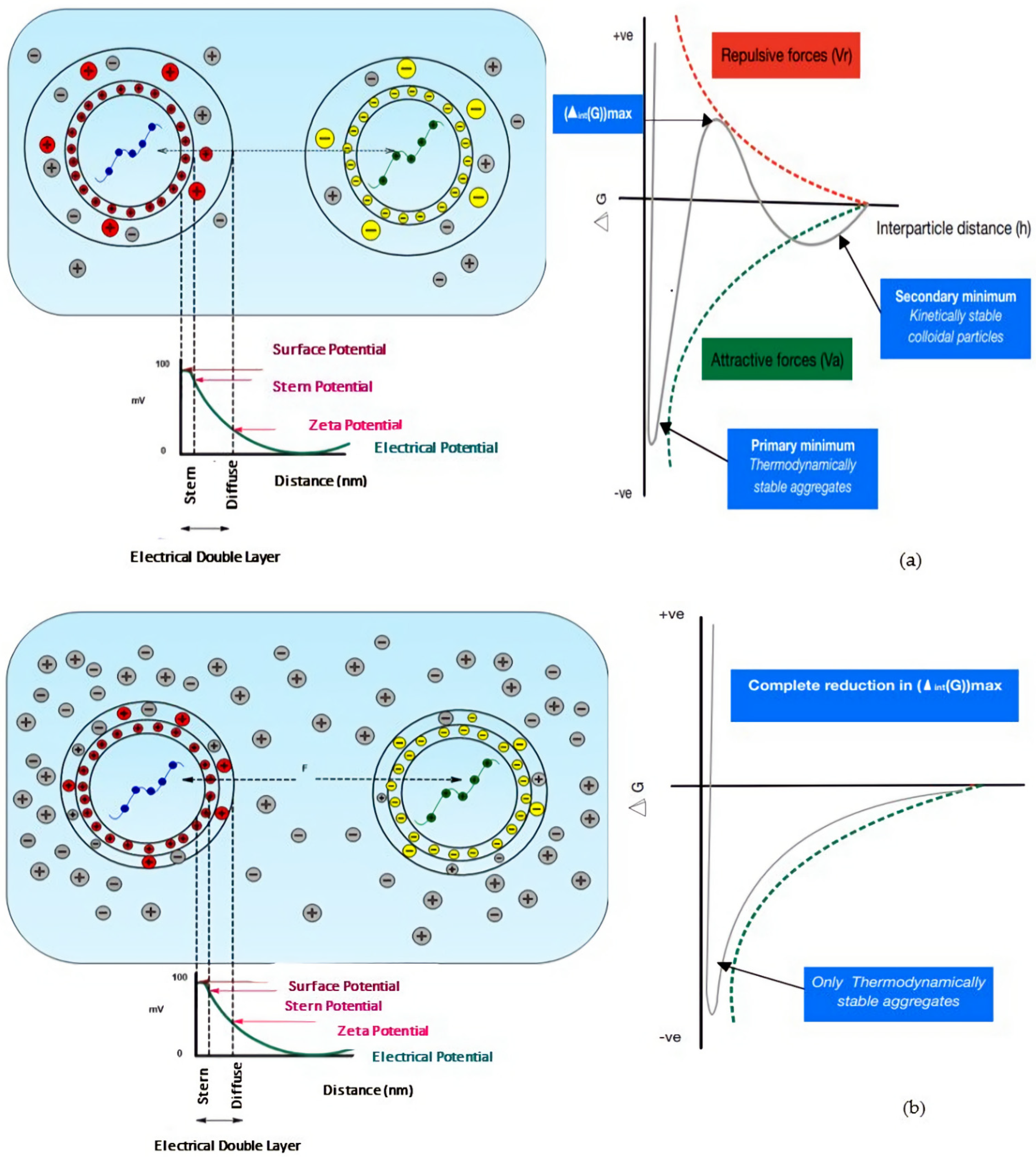
4.4.2. PEC Surface Charge
4.4.3. Ionic Strength and Stability
4.4.4. The Control of Therapeutic Release from PECs
4.4.5. The Influence of HA Concentration and MW
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AMD | Age-related macular degeneration |
| AT | Artificial tears |
| BEVA | Bevacizumab |
| CD44 | Cluster determinant 44 |
| CH | Chitosan |
| CRN | L-carnitine |
| Cx43 | MP Connexin 43 mimetic peptide |
| CyA | Cyclosporine A |
| DEAEM | 2-(diethylamino) ethyl methacrylate |
| DED | Dry eye disease |
| DEX | Dexamethasone |
| DEX-SP | Dexamethasone sodium phosphate |
| DLVO | Derjaguin, Landau, Verwey, and Overbeek |
| ECM | Extracellular matrices |
| EDL | Electrical double layer |
| EGCG | Epigallocatechin gallate |
| EPR | Enhanced permeation and retention |
| FA | Ferulic acid |
| FLZ | Fluconazole |
| GEH | Gelatin–EGCG nanoparticles |
| HA | Hyaluronic acid |
| HABD | HA-binding domain |
| HA–HC | Hyaluronic acid–heavy chain |
| HA-PEC | HA-based polyelectrolyte complexes |
| HC | Heavy chain |
| HCE | Human corneal epithelial |
| HMWHA | High-MW HA |
| HPMC | Hydroxypropyl methylcellulose |
| HYAL | Hyaluronidases |
| IL | Interleukin |
| IOBA-NHC | Spontaneously immortalised normal human conjunctival cell line |
| IOP | Intraocular pressure |
| IVI | Intravitreal injection |
| LMWHA | Low-MW HA |
| LPHNP | Lipid–polymer hybrid nanoparticles |
| LYVE-1 | Lymphatic vessel endothelial HA receptors |
| MCF.HCL | Moxifloxacin hydrochloride |
| MCR | Molar charge ratio |
| MPS | Multipurpose solution |
| mRNA | Messenger RNA |
| MSVI | Moderate-to-severe visual impairment |
| MW | Molecular weight |
| NaHA | Sodium hyaluronate |
| NHA | Native HA |
| ODDS | Ocular drug delivery systems |
| OSDI | Ocular Surface Disease Index |
| PECs | Polyelectrolyte complexes |
| pHEMA | poly-2-hydroxyethyl methacrylate |
| PLGA | Poly(D, L-lactide-co-glycide) |
| PLL | Poly(L-lysine) |
| pNIPAAM | Poly(N-isopropylacrylamide) |
| PTM | Pentamidine isethionate |
| RNS | Reactive nitrogen species |
| ROS | Reactive oxygen species |
| SH | Sodium hyaluronate |
| SIHy | Silicone hydrogel |
| siRNA | Small interfering RNA |
| TFBT | Tear film break-up time |
| TLR | Toll-like receptors |
| TM | Timolol maleate |
| TNF-α | Tumour necrosis factor-α |
| TPP | Tripolyphosphate |
| TRIS | Tris (trimethylsiloxy) methacryloxy propyl silane |
| TSG-6 | Tumour necrosis factor-stimulated gene-6 |
| VEGF-2 | Vascular endothelial growth factor 2 |
| VEGF165 | Vascular endothelial growth factor 165 |
| VEGF | Vascular endothelial growth factor |
| VitE-TPGS | D-α-Tocopherolpolyethylene glycol succinate |
| ZP | Zeta potential |
References
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D. Ocular Drug Delivery: Present Innovations and Future Challenges. J. Pharmacol. Exp. Ther. 2019, 370, 602–624. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Zhang, P.; Li, J. Elucidation of Colloid Performances of Thermosensitive in situ—Forming Ophthalmic Gel Formed by Poloxamer 407 for Loading Drugs. J. Pharm. Sci. 2020, 109, 1703–1713. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; Wang, J.; Li, N. A Novel Thermo-Sensitive Hydrogel-Based on Poly(N-Isopropylacrylamide)/Hyaluronic Acid of Ketoconazole for Ophthalmic Delivery. Artif. Cells Nanomed. Biotechnol. 2018, 46, 1282–1287. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.-H.; Ko, Y.-C.; Chang, Y.-F.; Huang, S.-H.; Liu, C.J.-L. Thermosensitive Chitosan-Gelatin-Based Hydrogel Containing Curcumin-Loaded Nanoparticles and Latanoprost as a Dual-Drug Delivery System for Glaucoma Treatment. Exp. Eye Res. 2019, 179, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Suwannoi, P.; Chomnawang, M.; Tunsirikongkon, A.; Phongphisutthinan, A.; Müller-Goymann, C.C.; Sarisuta, N. TAT-Surface Modified Acyclovir-Loaded Albumin Nanoparticles as a Novel Ocular Drug Delivery System. J. Drug Deliv. Sci. Technol. 2019, 52, 624–631. [Google Scholar] [CrossRef]
- Luis de Redín, I.; Boiero, C.; Martínez-Ohárriz, M.C.; Agüeros, M.; Ramos, R.; Peñuelas, I.; Allemandi, D.; Llabot, J.M.; Irache, J.M. Human Serum Albumin Nanoparticles for Ocular Delivery of Bevacizumab. Int. J. Pharm. 2018, 541, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Terreni, E.; Chetoni, P.; Tampucci, S.; Burgalassi, S.; Al-Kinani, A.A.; Alany, R.G.; Monti, D. Assembling Surfactants-Mucoadhesive Polymer Nanomicelles (ASMP-Nano) for Ocular Delivery of Cyclosporine-A. Pharmaceutics 2020, 12, 253. [Google Scholar] [CrossRef] [Green Version]
- Bengani, L.C.; Kobashi, H.; Ross, A.E.; Zhai, H.; Salvador-Culla, B.; Tulsan, R.; Kolovou, P.E.; Mittal, S.K.; Chauhan, S.K.; Kohane, D.S.; et al. Steroid-Eluting Contact Lenses for Corneal and Intraocular Inflammation. Acta Biomater. 2020, 116, 149–161. [Google Scholar] [CrossRef]
- Zhu, Y.; Sheng, Y. Sustained Delivery of Epalrestat to the Retina Using PEGylated Solid Lipid Nanoparticles Laden Contact Lens. Int. J. Pharm. 2020, 587, 119688. [Google Scholar] [CrossRef]
- Ross, A.E.; Bengani, L.C.; Tulsan, R.; Maidana, D.E.; Salvador-Culla, B.; Kobashi, H.; Kolovou, P.E.; Zhai, H.; Taghizadeh, K.; Kuang, L.; et al. Topical Sustained Drug Delivery to the Retina with a Drug-Eluting Contact Lens. Biomaterials 2019, 217, 119285. [Google Scholar] [CrossRef]
- Mun, J.; Mok, J.W.; Jeong, S.; Cho, S.; Joo, C.K.; Hahn, S.K. Drug-Eluting Contact Lens Containing Cyclosporine-Loaded Cholesterol-Hyaluronate Micelles for Dry Eye Syndrome. RSC Adv. 2019, 9, 16578–16585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, H.J.; Kim, D.H.; Chang, W.S.; Vales, T.P.; Kim, J.W.; Kim, K.H.; Kim, J.K. Thermo-Sensitive Nanogel-Laden Bicontinuous Microemulsion Drug-Eluting Contact Lenses. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 107, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Badiee, P.; Varshochian, R.; Rafiee-Tehrani, M.; Abedin Dorkoosh, F.; Khoshayand, M.R.; Dinarvand, R. Ocular Implant Containing Bevacizumab-Loaded Chitosan Nanoparticles Intended for Choroidal Neovascularization Treatment. J. Biomed. Mater. Res. A 2018, 106, 2261–2271. [Google Scholar] [CrossRef]
- Jiang, P.; Chaparro, F.J.; Cuddington, C.T.; Palmer, A.F. Injectable Biodegradable Bi-Layered Capsule for Sustained Delivery of Bevacizumab in Treating Wet Age-Related Macular Degeneration. J. Control. Release 2020, 320, 442–456. [Google Scholar] [CrossRef] [PubMed]
- Blindness and Visual Impairment. Available online: https://www.who.int/en/news-room/fact-sheets/detail/blindness-and-visual-impairment (accessed on 14 October 2019).
- The World Population Prospects: 2015 Revision. Available online: https://www.un.org/en/development/desa/publications/world-population-prospects-2015-revision.html (accessed on 14 October 2019).
- Projected Change in Vision Loss 2020 to 2050. Available online: https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/projected-change/ (accessed on 6 January 2021).
- Adelson, J.D.; Bourne, R.R.A.; Briant, P.S.; Flaxman, S.R.; Taylor, H.R.B.; Jonas, J.B.; Abdoli, A.A.; Abrha, W.A.; Abualhasan, A.; Abu-Gharbieh, E.G.; et al. Causes of Blindness and Vision Impairment in 2020 and Trends over 30 Years, and Prevalence of Avoidable Blindness in Relation to VISION 2020: The Right to Sight: An Analysis for the Global Burden of Disease Study. Lancet Glob. Health 2020, 1, E144–E160. [Google Scholar] [CrossRef]
- Global Age-Related Macular Degeneration Market Will More Than Double in Size by 2028—GlobalData. Available online: https://www.globaldata.com/global-age-related-macular-degeneration-market-will-more-than-double-in-size-by-2028/ (accessed on 11 January 2021).
- Glaucoma Therapeutics Market to Reach USD 11.05 Billion at 6.1% CAGR by 2027; Rising Research on Prostaglandin Analogs, Says Fortune Business InsightsTM. Available online: https://www.globenewswire.com/news-release/2020/09/09/2090664/0/en/Glaucoma-Therapeutics-Market-to-Reach-USD-11-05-Billion-at-6-1-CAGR-by-2027-Rising-Research-on-Prostaglandin-Analogs-says-Fortune-Business-Insights.html (accessed on 2 May 2022).
- Diabetic Retinopathy Market to Reach USD 13.04 Billion by 2026. Available online: https://www.globenewswire.com/news-release/2019/06/06/1865544/0/en/Diabetic-Retinopathy-Market-to-Reach-USD-13-04-billion-By-2026-Reports-And-Data.html (accessed on 2 May 2022).
- Nentwich, M.M.; Ulbig, M.W. Diabetic Retinopathy—Ocular Complications of Diabetes Mellitus. World J. Diabetes 2015, 6, 489. [Google Scholar] [CrossRef]
- García-Quintanilla, L.; Luaces-Rodríguez, A.; Gil-Martínez, M.; Mondelo-García, C.; Maroñas, O.; Mangas-Sanjuan, V.; González-Barcia, M.; Zarra-Ferro, I.; Aguiar, P.; Otero-Espinar, F.J.; et al. Pharmacokinetics of Intravitreal Anti-VEGF Drugs in Age-Related Macular Degeneration. Pharmaceutics 2019, 11, 365. [Google Scholar] [CrossRef] [Green Version]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- del Amo, E.M.; Rimpelä, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic Aspects of Retinal Drug Delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef]
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; et al. Ophthalmic Drug Delivery Systems for the Treatment of Retinal Diseases: Basic Research to Clinical Applications. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5403–5420. [Google Scholar] [CrossRef]
- Meduri, E.; Gillmann, K.; Mansouri, K. Intraocular Pressure Variations After Intravitreal Injections Measured with an Implanted Suprachoroidal Telemetry Sensor. J. Glaucoma 2021, 30, E360–E363. [Google Scholar] [CrossRef] [PubMed]
- Falavarjani, K.G.; Nguyen, Q.D. Adverse Events and Complications Associated with Intravitreal Injection of Anti-VEGF Agents: A Review of Literature. Eye 2013, 27, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrera, F.J.; Wang, D.C.; Reddy, K.; Acharya, G.; Shin, C.S. Challenges and Opportunities for Drug Delivery to the Posterior of the Eye. Drug Discov. Today 2019, 24, 1679–1684. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Samy, K.E.; Bernards, D.A.; Desai, T.A. Recent Advances in Intraocular Sustained-Release Drug Delivery Devices. Drug Discov. Today 2019, 24, 1694–1700. [Google Scholar] [CrossRef]
- Ophthalmic Drugs Market Size, Share & Trends Analysis Report by Disease (Dry Eye, Eye Allergy, Glaucoma, Eye Infection), by Drug Class, by Dosage form, by Route of Administration, by Product Type, by Region, and Segment Forecasts, 2021–2028. Available online: https://www.grandviewresearch.com/industry-analysis/ophthalmic-therapeutics-drug-market (accessed on 2 May 2022).
- Patel, A. Ocular Drug Delivery Systems: An Overview. World J. Pharmacol. 2013, 2, 47. [Google Scholar] [CrossRef]
- Boddu, S.; Gupta, H.; Patel, S. Drug Delivery to the Back of the Eye Following Topical Administration: An Update on Research and Patenting Activity. Recent Pat. Drug Deliv. Formul. 2014, 8, 27–36. [Google Scholar] [CrossRef]
- Johannsdottir, S.; Jansook, P.; Stefansson, E.; Kristinsdottir, I.M.; Fulop, Z.; Asgrimsdottir, G.M.; Thorsteindsottir, M.; Eiriksson, F.F.; Loftsson, T. Topical Drug Delivery to the Posterior Segment of the Eye: Dexamethasone Concentrations in Various Eye Tissues after Topical Administration for up to 15 Days to Rabbits. J. Drug Deliv. Sci. Technol. 2018, 45, 449–454. [Google Scholar] [CrossRef]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular Drug Delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Rodrigues, G.A.; Lutz, D.; Shen, J.; Yuan, X.; Shen, H.; Cunningham, J.; Rivers, H.M. Topical Drug Delivery to the Posterior Segment of the Eye: Addressing the Challenge of Preclinical to Clinical Translation. Pharm. Res. 2018, 35, 245. [Google Scholar] [CrossRef] [Green Version]
- Pitkänen, L.; Ranta, V.P.; Moilanen, H.; Urtti, A. Permeability of Retinal Pigment Epithelium: Effects of Permeant Molecular Weight and Lipophilicity. Investig. Ophthalmol. Vis. Sci. 2005, 46, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Jumelle, C.; Gholizadeh, S.; Annabi, N.; Dana, R. Advances and Limitations of Drug Delivery Systems Formulated as Eye Drops. J. Control. Release 2020, 321, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Irimia, T.; Ghica, M.V.; Popa, L.; Anuţa, V.; Arsene, A.L.; Dinu-Pîrvu, C.E. Strategies for Improving Ocular Drug Bioavailability and Cornealwound Healing with Chitosan-Based Delivery Systems. Polymers 2018, 10, 1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allyn, M.M.; Luo, R.H.; Hellwarth, E.B.; Swindle-Reilly, K.E. Considerations for Polymers Used in Ocular Drug Delivery. Front. Med. 2022, 8, 787644. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Huh, K.M.; Kang, S.W. Applications of Biomaterials in 3D Cell Culture and Contributions of 3D Cell Culture to Drug Development and Basic Biomedical Research. Int. J. Mol. Sci. 2021, 22, 2491. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Liu, P.Y.; Lin, M.H.; Lu, C.J.; Chou, H.Y.; Nian, C.Y.; Jiang, Y.T.; Hsu, Y.H.H. Applications of Hyaluronic Acid in Ophthalmology and Contact Lenses. Molecules 2021, 26, 2485. [Google Scholar] [CrossRef]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic Acid: A Key Molecule in Skin Aging. Dermato-Endocrinol. 2012, 4, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Vasvani, S.; Kulkarni, P.; Rawtani, D. Hyaluronic Acid: A Review on Its Biology, Aspects of Drug Delivery, Route of Administrations and a Special Emphasis on Its Approved Marketed Products and Recent Clinical Studies. Int. J. Biol. Macromol. 2020, 151, 1012–1029. [Google Scholar] [CrossRef]
- Selyanin, M.A.; Boykov, P.Y.; Khabarov, V.N. Molecular and Supramolecular Structure of Hyaluronic Acid. In Hyaluronic Acid—Preparation, Properties, Application in Biology and Medicine; Polyak, F., Ed.; John Wiley & Sons Ltd.: West Sussex, UK, 2015; Volume 1, pp. 101–104. [Google Scholar]
- Lapčík, L.; Lapčík, L.; de Smedt, S.; Demeester, J.; Chabreček, P. Hyaluronan: Preparation, Structure, Properties, and Applications. Chem. Rev. 1998, 98, 2663–2684. [Google Scholar] [CrossRef]
- Juncan, A.M.; Moisă, D.G.; Santini, A.; Morgovan, C.; Rus, L.L.; Vonica-țincu, A.L.; Loghin, F. Advantages of Hyaluronic Acid and Its Combination with Other Bioactive Ingredients in Cosmeceuticals. Molecules 2021, 26, 4429. [Google Scholar] [CrossRef]
- Bukhari, S.N.A.; Roswandi, N.L.; Waqas, M.; Habib, H.; Hussain, F.; Khan, S.; Sohail, M.; Ramli, N.A.; Thu, H.E.; Hussain, Z. Hyaluronic Acid, a Promising Skin Rejuvenating Biomedicine: A Review of Recent Updates and Pre-Clinical and Clinical Investigations on Cosmetic and Nutricosmetic Effects. Int. J. Biol. Macromol. 2018, 120, 1682–1695. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.R.; Kondiah, P.P.D.; Choonara, Y.E.; du Toit, L.C.; Ally, N.; Pillay, V. Hydrogel Biomaterials for Application in Ocular Drug Delivery. Front. Bioeng. Biotechnol. 2020, 8, 228. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wei, D.; Xu, Y.; Zhu, Q. Hyaluronic Acid in Ocular Drug Delivery. Carbohydr. Polym. 2021, 264, 118006. [Google Scholar] [CrossRef] [PubMed]
- Harrer, D.; Sanchez Armengol, E.; Friedl, J.D.; Jalil, A.; Jelkmann, M.; Leichner, C.; Laffleur, F. Is Hyaluronic Acid the Perfect Excipient for the Pharmaceutical Need? Int. J. Pharm. 2021, 601, 120589. [Google Scholar] [CrossRef] [PubMed]
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic Acid in the Third Millennium. Polymers 2018, 10, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knopf-Marques, H.; Pravda, M.; Wolfova, L.; Velebny, V.; Schaaf, P.; Vrana, N.E.; Lavalle, P. Hyaluronic Acid and Its Derivatives in Coating and Delivery Systems: Applications in Tissue Engineering, Regenerative Medicine and Immunomodulation. Adv. Healthc. Mater. 2016, 5, 2841–2855. [Google Scholar] [CrossRef]
- Gallo, N.; Nasser, H.; Salvatore, L.; Natali, M.L.; Campa, L.; Mahmoud, M.; Capobianco, L.; Sannino, A.; Madaghiele, M. Hyaluronic Acid for Advanced Therapies: Promises and Challenges. Eur. Polym. J. 2019, 117, 134–147. [Google Scholar] [CrossRef]
- Necas, J.; Bartosikova, L.; Brauner, P.; Kolar, J. Hyaluronic Acid (Hyaluronan): A Review. Vet. Med. 2008, 53, 397–411. [Google Scholar] [CrossRef] [Green Version]
- Toole, B.P. Hyaluronan: From Extracellular Glue to Pericellular Cue. Nat. Rev. Cancer 2004, 4, 528–539. [Google Scholar] [CrossRef]
- Fakhari, A.; Berkland, C. Applications and Emerging Trends of Hyaluronic Acid in Tissue Engineering, as a Dermal Filler and in Osteoarthritis Treatment. Acta Biomater. 2013, 9, 7081–7092. [Google Scholar] [CrossRef] [Green Version]
- Dovedytis, M.; Liu, Z.J.; Bartlett, S. Hyaluronic Acid and Its Biomedical Applications: A Review. Eng. Regen. 2020, 1, 102–113. [Google Scholar] [CrossRef]
- Guter, M.; Breunig, M. Hyaluronan as a Promising Excipient for Ocular Drug Delivery. Eur. J. Pharm. Biopharm. 2017, 113, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Yanaki, T.; Yamaguchi, T. Temporary Network Formation of Hyaluronate under a Physiological Condition. 1. Molecular-weight Dependence. Biopolymers 1990, 30, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Kabanov, V.A. Polyelectrolyte Complexes in Solution and in Bulk. Russ. Chem. Rev. 2005, 74, 3–20. [Google Scholar] [CrossRef]
- Insua, I.; Wilkinson, A.; Fernandez-Trillo, F. Polyion Complex (PIC) Particles: Preparation and Biomedical Applications. Eur. Polym. J. 2016, 81, 198–215. [Google Scholar] [CrossRef] [Green Version]
- Khunmanee, S.; Jeong, Y.; Park, H. Crosslinking Method of Hyaluronic-Based Hydrogel for Biomedical Applications. J. Tissue Eng. 2017, 8, 2041731417726464. [Google Scholar] [CrossRef] [Green Version]
- Gatej, I.; Popa, M.; Rinaudo, M. Role of the PH on Hyaluronan Behavior in Aqueous Solution. Biomacromolecules 2005, 6, 61–67. [Google Scholar] [CrossRef]
- Ghosh, S.; Kobal, I.; Zanette, D.; Reed, W.F. Conformational Contraction and Hydrolysis of Hyaluronate in Sodium Hydroxide Solutions. Macromolecules 1993, 26, 4685–4693. [Google Scholar] [CrossRef]
- Morris, E.R.; Rees, D.A.; Welsh, E.J. Conformation and Dynamic Interactions in Hyaluronate Solutions. J. Mol. Biol. 1980, 138, 383–400. [Google Scholar] [CrossRef]
- Maleki, A.; Kjøniksen, A.L.; Nyström, B. Effect of PH on the Behavior of Hyaluronic Acid in Dilute and Semidilute Aqueous Solutions. Macromol. Symp. 2008, 274, 131–140. [Google Scholar] [CrossRef]
- Cowman, M.K.; Matsuoka, S. The Intrinsic Viscosity of Hyaluronan. In Hyaluronan; Elsevier: Amsterdam, The Netherlands, 2002; pp. 75–78. [Google Scholar] [CrossRef]
- Bothner, H.; Wik, O. Rheology of Hyaluronate. Acta Oto-Laryngol. 1987, 104, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Cowman, M.K.; Schmidt, T.A.; Raghavan, P.; Stecco, A. Viscoelastic Properties of Hyaluronan in Physiological Conditions. F1000Research 2015, 4, 622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleland, R.L. Effect of Temperature on the Limiting Viscosity Number of Hyaluronic Acid and Chondroitin 4-sulfate. Biopolymers 1979, 18, 1821–1828. [Google Scholar] [CrossRef]
- Shetty, G.N.; Whelton, R. Ophthalmic Injection of Viscous Formulations—Why Unique Needs Require a Novel Delivery System. ONdrugdelivery 2022, 130, 54–58. [Google Scholar]
- Ng, P.C.; Oliver, J.J. Anatomy of the Eye. In Handbook of Emergency Ophthalmology; Long, B., Koyfman, A., Eds.; Springer: Cham, Switzerland, 2018; pp. 1–12. [Google Scholar] [CrossRef]
- Nickerson, C.S. The Vitreous Humor: Mechanics and Structure. Ph.D. Thesis, California Institute of Technology, Pasadena, CA, USA, 2005. [Google Scholar]
- Moiseev, R.V.; Morrison, P.W.J.; Steele, F.; Khutoryanskiy, V.V. Penetration Enhancers in Ocular Drug Delivery. Pharmaceutics 2019, 11, 321. [Google Scholar] [CrossRef] [Green Version]
- Crowell, S.R.; Wang, K.; Famili, A.; Shatz, W.; Loyet, K.M.; Chang, V.; Liu, Y.; Prabhu, S.; Kamath, A.V.; Kelley, R.F. Influence of Charge, Hydrophobicity, and Size on Vitreous Pharmacokinetics of Large Molecules. Transl. Vis. Sci. Technol. 2019, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Bishop, P. The Biochemical Structure of Mammalian Vitreous. Eye 1996, 10, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Ángeles, G.H.; Nešporová, K. Hyaluronan and Its Derivatives for Ophthalmology: Recent Advances and Future Perspectives. Carbohydr. Polym. 2021, 259, 117697. [Google Scholar] [CrossRef]
- Müller-Lierheim, W.G.K. Why Chain Length of Hyaluronan in Eye Drops Matters. Diagnostics 2020, 10, 511. [Google Scholar] [CrossRef]
- Kwon, M.Y.; Wang, C.; Galarraga, J.H.; Puré, E.; Han, L.; Burdick, J.A. Influence of Hyaluronic Acid Modification on CD44 Binding towards the Design of Hydrogel Biomaterials. Biomaterials 2019, 222, 119451. [Google Scholar] [CrossRef]
- Girish, K.S.; Kemparaju, K. The Magic Glue Hyaluronan and Its Eraser Hyaluronidase: A Biological Overview. Life Sci. 2007, 80, 1921–1943. [Google Scholar] [CrossRef] [PubMed]
- Passi, A.; Vigetti, D. Hyaluronan as Tunable Drug Delivery System. Adv. Drug Deliv. Rev. 2019, 146, 83–96. [Google Scholar] [CrossRef] [PubMed]
- García-Posadas, L.; Contreras-Ruiz, L.; López-García, A.; Álvarez, S.V.; Maldonado, M.J.; Diebold, Y. Hyaluronan Receptors in the Human Ocular Surface: A Descriptive and Comparative Study of RHAMM and CD44 in Tissues, Cell Lines and Freshly Collected Samples. Histochem. Cell Biol. 2012, 137, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhao, S.; Karnad, A.; Freeman, J.W. The Biology and Role of CD44 in Cancer Progression: Therapeutic Implications. J. Hematol. Oncol. 2018, 11, 64. [Google Scholar] [CrossRef] [Green Version]
- Mochimaru, H.; Takahashi, E.; Tsukamoto, N.; Miyazaki, J.; Yaguchi, T.; Koto, T.; Kurihara, T.; Noda, K.; Ozawa, Y.; Ishimoto, T.; et al. Involvement of Hyaluronan and Its Receptor CD44 with Choroidal Neovascularization. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4410–4415. [Google Scholar] [CrossRef]
- Shen, W.Y.; Yu, M.J.T.; Barry, C.J.; Constable, I.J.; Rakoczy, P.E. Expression of Cell Adhesion Molecules and Vascular Endothelial Growth Factor in Experimental Choroidal Neovascularisation in the Rat. Br. J. Ophthalmol. 1998, 82, 1063–1071. [Google Scholar] [CrossRef] [Green Version]
- Knepper, P.A.; Miller, A.M.; Choi, J.; Wertz, R.D.; Nolan, M.J.; Goossens, W.; Whitmer, S.; Yue, B.Y.J.T.; Ritch, R.; Liebmann, J.M.; et al. Hypophosphorylation of Aqueous Humor SCD44 and Primary Open-Angle Glaucoma. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2829–2837. [Google Scholar] [CrossRef]
- de Oliveira, J.D.; Carvalho, L.S.; Gomes, A.M.V.; Queiroz, L.R.; Magalhães, B.S.; Parachin, N.S. Genetic Basis for Hyper Production of Hyaluronic Acid in Natural and Engineered Microorganisms. Microb. Cell Factories 2016, 15, 119. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Cao, M.; Liu, H.; He, Y.; Xu, J.; Du, Y.; Liu, Y.; Wang, W.; Cui, L.; Hu, J.; et al. The High and Low Molecular Weight Forms of Hyaluronan Have Distinct Effects on CD44 Clustering. J. Biol. Chem. 2012, 287, 43094–43107. [Google Scholar] [CrossRef] [Green Version]
- Wight, T.N. Provisional Matrix: A Role for Versican and Hyaluronan. J. Int. Soc. Matrix Biol. 2017, 60–61, 38–56. [Google Scholar] [CrossRef]
- Stern, R.; Jedrzejas, M.J. The Hyaluronidases: Their Genomics, Structures, and Mechanisms of Action. Chem. Rev. 2006, 106, 818–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cyphert, J.M.; Trempus, C.S.; Garantziotis, S. Size Matters: Molecular Weight Specificity of Hyaluronan Effects in Cell Biology. Int. J. Cell Biol. 2015, 2015, 563818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigetti, D.; Karousou, E.; Viola, M.; Deleonibus, S.; de Luca, G.; Passi, A. Hyaluronan: Biosynthesis and Signaling. Biochim. Et Biophys. Acta Gen. Subj. 2014, 1840, 2452–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestorino, N.; Bełdowski, P.; Martinez-Larrañaga, M.-R.; Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Vet. Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [Green Version]
- Erickson, M.; Stern, R. Chain Gangs: New Aspects of Hyaluronan Metabolism. Biochem. Res. Int. 2012, 2012, 893947. [Google Scholar] [CrossRef] [Green Version]
- Marinho, A.; Nunes, C.; Reis, S. Hyaluronic Acid: A Key Ingredient in the Therapy of Inflammation. Biomolecules 2021, 11, 1518. [Google Scholar] [CrossRef]
- Fan, C.; Wang, H. Connection between Hyaluronic Acid and Toll-Like Receptor in Signal Transduction. In Proceedings of the International Conference in Medical Science and Biological Engineering; Deng, J., Qingjun, L., Eds.; World Scientific: Kowloon, Hong Kong, 2015; pp. 387–393. [Google Scholar] [CrossRef]
- Kotla, N.G.; Bonam, S.R.; Rasala, S.; Wankar, J.; Bohara, R.A.; Bayry, J.; Rochev, Y.; Pandit, A. Recent Advances and Prospects of Hyaluronan as a Multifunctional Therapeutic System. J. Control. Release 2021, 336, 598–620. [Google Scholar] [CrossRef]
- Jiang, D.; Liang, J.; Noble, P.W. Hyaluronan as an Immune Regulator in Human Diseases. Physiol. Rev. 2011, 91, 221–264. [Google Scholar] [CrossRef] [Green Version]
- Petrey, A.C.; de la Motte, C.A. Hyaluronan, a Crucial Regulator of Inflammation. Front. Immunol. 2014, 5, 101. [Google Scholar] [CrossRef] [Green Version]
- Lee-Sayer, S.S.M.; Dong, Y.; Arif, A.A.; Olsson, M.; Brown, K.L.; Johnson, P. The Where, When, How and Why of Hyaluronan Binding by Immune Cells. Front. Immunol. 2015, 6, 150. [Google Scholar] [CrossRef] [Green Version]
- Lardner, E.; van Setten, G.B. Detection of TSG-6-like Protein in Human Corneal Epithelium. Simultaneous Presence with CD44 and Hyaluronic Acid. J. Fr. D’ophtalmologie 2020, 43, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.Y.; Keller, K.E. Hyaluronan Cable Formation by Ocular Trabecular Meshwork Cells. Exp. Eye Res. 2015, 139, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, A.J.; de La Motte, C.A. Hyaluronan Cross-Linking: A Protective Mechanism in Inflammation? Trends Immunol. 2005, 26, 637–643. [Google Scholar] [CrossRef]
- Bora, M.; Mundargi, R.C.; Chee, Y.; Wong, T.T.L.; Venkatraman, S.S. 5-Flurouracil Microencapsulation and Impregnation in Hyaluronic Acid Hydrogel as Composite Drug Delivery System for Ocular Fibrosis. Cogent Med. 2016, 3, 1182108. [Google Scholar] [CrossRef]
- Carlson, E.; Kao, W.W.Y.; Ogundele, A. Impact of Hyaluronic Acid-Containing Artificial Tear Products on Reepithelialization in an In Vivo Corneal Wound Model. J. Ocul. Pharmacol. Ther. 2018, 34, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Wang, Z.; Liu, Y.; Wang, L.; Jiang, Z.; Li, T.; Zhang, W.; Liang, Y. Carboxymethyl Chitosan/Gelatin/Hyaluronic Acid Blended-Membranes as Epithelia Transplanting Scaffold for Corneal Wound Healing. Carbohydr. Polym. 2018, 192, 240–250. [Google Scholar] [CrossRef]
- Saraswathy, K.; Agarwal, G.; Srivastava, A. Hyaluronic Acid Microneedles-Laden Collagen Cryogel Plugs for Ocular Drug Delivery. J. Appl. Polym. Sci. 2020, 137, 49285. [Google Scholar] [CrossRef]
- Ilochonwu, B.C.; Urtti, A.; Hennink, W.E.; Vermonden, T. Intravitreal Hydrogels for Sustained Release of Therapeutic Proteins. J. Control. Release 2020, 326, 419–441. [Google Scholar] [CrossRef]
- Chittasupho, C.; Posritong, P.; Ariyawong, P. Stability, Cytotoxicity, and Retinal Pigment Epithelial Cell Binding of Hyaluronic Acid-Coated PLGA Nanoparticles Encapsulating Lutein. AAPS PharmSciTech 2019, 20, 4. [Google Scholar] [CrossRef]
- Silva, B.; Gonçalves, L.M.; Braz, B.S.; Delgado, E. Chitosan and Hyaluronic Acid Nanoparticles as Vehicles of Epoetin Beta for Subconjunctival Ocular Delivery. Mar. Drugs 2022, 20, 151. [Google Scholar] [CrossRef]
- Agarwal, P.; Craig, J.P.; Rupenthal, I.D. Formulation Considerations for the Management of Dry Eye Disease. Pharmaceutics 2021, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- You, I.C.; Li, Y.; Jin, R.; Ahn, M.; Choi, W.; Yoon, K.C. Comparison of 0.1%, 0.18%, and 0.3% Hyaluronic Acid Eye Drops in the Treatment of Experimental Dry Eye. J. Ocul. Pharmacol. Ther. 2018, 34, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallacara, A.; Vertuani, S.; Panozzo, G.; Pecorelli, A.; Valacchi, G.; Manfredini, S. Novel Artificial Tears Containing Cross-Linked Hyaluronic Acid: An in Vitro Re-Epithelialization Study. Molecules 2017, 22, 2104. [Google Scholar] [CrossRef] [Green Version]
- Graça, A.; Gonçalves, L.M.; Raposo, S.; Ribeiro, H.M.; Marto, J. Useful in Vitro Techniques to Evaluate the Mucoadhesive Properties of Hyaluronic Acid-Based Ocular Delivery Systems. Pharmaceutics 2018, 10, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, T.; Nagata, T.; Kudo, H.; Müller-Lierheim, W.G.K.; van Setten, G.-B.; Dogru, M.; Tsubota, K. The Effects of High Molecular Weight Hyaluronic Acid Eye Drop Application in Environmental Dry Eye Stress Model Mice. Int. J. Mol. Sci. 2020, 21, 3516. [Google Scholar] [CrossRef]
- Manju, S.; Sreenivasan, K. Conjugation of Curcumin onto Hyaluronic Acid Enhances Its Aqueous Solubility and Stability. J. Colloid Interface Sci. 2011, 359, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Oechsner, M.; Keipert, S. Polyacrylic Acid/Polyvinylpyrrolidone Bipolymeric Systems. I. Rheological and Mucoadhesive Properties of Formulations Potentially Useful for the Treatment of Dry-Eye-Syndrome. Eur. J. Pharm. Biopharm. 1999, 47, 113–118. [Google Scholar] [CrossRef]
- Chen, T.; Tseng, C.; Lin, C.-A.; Lin, H.; Venkatesan, P.; Lai, P. Effects of Eye Drops Containing Hyaluronic Acid-Nimesulide Conjugates in a Benzalkonium Chloride-Induced Experimental Dry Eye Rabbit Model. Pharmaceutics 2021, 13, 1366. [Google Scholar] [CrossRef]
- Tredici, C.; Fasciani, R.; Villano, A.; Gambini, G.; Caporossi, A. Efficacy of Eye Drops Containing Crosslinked Hyaluronic Acid and CoQ10 in Restoring Ocular Health Exposed to Chlorinated Water. Eur. J. Ophthalmol. 2020, 30, 430–438. [Google Scholar] [CrossRef]
- White, C.J.; Thomas, C.R.; Byrne, M.E. Bringing Comfort to the Masses: A Novel Evaluation of Comfort Agent Solution Properties. Contact Lens Anterior Eye 2014, 37, 81–91. [Google Scholar] [CrossRef]
- Jansook, P.; Kulsirachote, P.; Asasutjarit, R.; Loftsson, T. Development of Celecoxib Eye Drop Solution and Microsuspension: A Comparative Investigation of Binary and Ternary Cyclodextrin Complexes. Carbohydr. Polym. 2019, 225, 115209. [Google Scholar] [CrossRef] [PubMed]
- Salzillo, R.; Schiraldi, C.; Corsuto, L.; D’Agostino, A.; Filosa, R.; de Rosa, M.; la Gatta, A. Optimization of Hyaluronan-Based Eye Drop Formulations. Carbohydr. Polym. 2016, 153, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Yin, C.; Ma, J.; Tu, J.; Shen, Y. Preparation and Evaluation of Topically Applied Azithromycin Based on Sodium Hyaluronate in Treatment of Conjunctivitis. Pharmaceutics 2019, 11, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Agate, S.; Salem, K.S.; Lucia, L.; Pal, L. Hydrogel-Based Sensor Networks: Compositions, Properties, and Applications—A Review. ACS Appl. Bio Mater. 2021, 4, 140–162. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Mooney, D.J.; Paulson, J.A. Designing Hydrogels for Controlled Drug Delivery. Nat. Rev. Mater. 2016, 1, 16071. [Google Scholar] [CrossRef]
- Trombino, S.; Servidio, C.; Curcio, F.; Cassano, R. Strategies for Hyaluronic Acid-Based Hydrogel Design in Drug Delivery. Pharmaceutics 2019, 11, 407. [Google Scholar] [CrossRef] [Green Version]
- Awwad, S.; Abubakre, A.; Angkawinitwong, U.; Khaw, P.T.; Brocchini, S. In Situ Antibody-Loaded Hydrogel for Intravitreal Delivery. Eur. J. Pharm. Sci. 2019, 137, 104993. [Google Scholar] [CrossRef] [PubMed]
- Egbu, R.; Brocchini, S.; Khaw, P.T.; Awwad, S. Antibody Loaded Collapsible Hyaluronic Acid Hydrogels for Intraocular Delivery. Eur. J. Pharm. Biopharm. 2018, 124, 95–103. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, L.C.M.; Lo, A.C.; Chau, Y. Injectable Chemically Crosslinked Hydrogel for the Controlled Release of Bevacizumab in Vitreous: A 6-Month In Vivo Study. Transl. Vis. Sci. Technol. 2015, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Donati, S.; Caprani, S.M.; Airaghi, G.; Vinciguerra, R.; Bartalena, L.; Testa, F.; Mariotti, C.; Porta, G.; Simonelli, F.; Azzolini, C. Vitreous Substitutes: The Present and the Future. BioMed Res. Int. 2014, 2014, 351804. [Google Scholar] [CrossRef]
- Alovisi, C.; Panico, C.; De Sanctis, U.; Eandi, C.M. Vitreous Substitutes: Old and New Materials in Vitreoretinal Surgery. J. Ophthalmol. 2017, 2017, 3172138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Chi, J.; Jiang, Z.; Hu, H.; Yang, C.; Liu, W.; Han, B. A Self-Healing and Injectable Hydrogel Based on Water-Soluble Chitosan and Hyaluronic Acid for Vitreous Substitute. Carbohydr. Polym. 2021, 256, 117519. [Google Scholar] [CrossRef] [PubMed]
- Thakur, S.S.; Shenoy, S.K.; Suk, J.S.; Hanes, J.S.; Rupenthal, I.D. Validation of Hyaluronic Acid-Agar-Based Hydrogels as Vitreous Humor Mimetics for in Vitro Drug and Particle Migration Evaluations. Eur. J. Pharm. Biopharm. 2020, 148, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Rickmann, A.; Wahl, S.; Germann, A.; Stanzel, B.V.; Januschowski, K.; Szurman, P. Alginate-and Hyaluronic Acid–Based Hydrogels as Victreous Substitutes: An in Vitro Evaluation. Transl. Vis. Sci. Technol. 2020, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Jung, M.Y.; Pak, H.J.; Park, J.H.; Kim, M.; Chuck, R.S.; Park, C.Y. Development of a Novel Hyaluronic Acid Membrane for the Treatment of Ocular Surface Diseases. Sci. Rep. 2021, 11, 2351. [Google Scholar] [CrossRef]
- Bao, Z.; Yu, A.; Shi, H.; Hu, Y.; Jin, B.; Lin, D.; Dai, M.; Lei, L.; Li, X.; Wang, Y. Glycol Chitosan/Oxidized Hyaluronic Acid Hydrogel Film for Topical Ocular Delivery of Dexamethasone and Levofloxacin. Int. J. Biol. Macromol. 2021, 167, 659–666. [Google Scholar] [CrossRef]
- Díaz-Tomé, V.; Luaces-Rodríguez, A.; Silva-Rodríguez, J.; Blanco-Dorado, S.; García-Quintanilla, L.; Llovo-Taboada, J.; Blanco-Méndez, J.; García-Otero, X.; Varela-Fernández, R.; Herranz, M.; et al. Ophthalmic Econazole Hydrogels for the Treatment of Fungal Keratitis. J. Pharm. Sci. 2018, 107, 1342–1351. [Google Scholar] [CrossRef]
- Korogiannaki, M.; Zhang, J.; Sheardown, H. Surface Modification of Model Hydrogel Contact Lenses with Hyaluronic Acid via Thiol-Ene “Click” Chemistry for Enhancing Surface Characteristics. J. Biomater. Appl. 2017, 32, 446–462. [Google Scholar] [CrossRef]
- Luensmann, D.; Jones, L. Protein Deposition on Contact Lenses: The Past, the Present, and the Future. Contact Lens Anterior Eye 2012, 35, 53–64. [Google Scholar] [CrossRef]
- Xu, J.; Xue, Y.; Hu, G.; Lin, T.; Gou, J.; Yin, T.; He, H.; Zhang, Y.; Tang, X. A Comprehensive Review on Contact Lens for Ophthalmic Drug Delivery. J. Control. Release 2018, 281, 97–118. [Google Scholar] [CrossRef]
- Musgrave, C.S.A.; Fang, F. Contact Lens Materials: A Materials Science Perspective. Materials 2019, 12, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Beek, M.; Jones, L.; Sheardown, H. Hyaluronic Acid Containing Hydrogels for the Reduction of Protein Adsorption. Biomaterials 2008, 29, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Stapleton, F.; Carnt, N. Microbiology, Lens Care and Maintenance. In Contact Lenses; Phillips, A.J., Speedwell, L., Hough, T., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 16, pp. 65–96. [Google Scholar] [CrossRef]
- Weeks, A.; Boone, A.; Luensmann, D.; Jones, L.; Sheardown, H. The Effects of Hyaluronic Acid Incorporated as a Wetting Agent on Lysozyme Denaturation in Model Contact Lens Materials. J. Biomater. Appl. 2013, 28, 323–333. [Google Scholar] [CrossRef]
- Boone, A.; Heynen, M.; Joyce, E.; Varikooty, J.; Jones, L. Ex Vivo Protein Deposition on Bi-Weekly Silicone Hydrogel Contact Lenses. Optom. Vis. Sci. 2009, 86, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, K.; Drolle, E.; Nakagawa, H.; Hisamura, R.; Ngo, W.; Jones, L. Impact of a Low Molecular Weight Hyaluronic Acid Derivative on Contact Lens Wettability. Contact Lens Anterior Eye 2021, 44, 101334. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Lee, T.R. Contact Angle and Wetting Properties. In Surface Science Techniques; Bracco, G., Holst, B., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 51, pp. 3–34. [Google Scholar] [CrossRef]
- Ali, M.; Byrne, M.E. Controlled Release of High Molecular Weight Hyaluronic Acid from Molecularly Imprinted Hydrogel Contact Lenses. Pharm. Res. 2009, 26, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Shaikh, A.A.; Lakdawala, D.H.; Desai, A.R.; Pandya, M.M.; Singhania, S.S.; Vaidya, R.J.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. Design and Optimization of a Novel Implantation Technology in Contact Lenses for the Treatment of Dry Eye Syndrome: In Vitro and in Vivo Evaluation. Acta Biomater. 2017, 53, 211–221. [Google Scholar] [CrossRef]
- Jiang, S.; Franco, Y.L.; Zhou, Y.; Chen, J. Nanotechnology in Retinal Drug Delivery. Int. J. Ophthalmol. 2018, 11, 1038–1044. [Google Scholar] [CrossRef]
- Gorantla, S.; Rapalli, V.K.; Waghule, T.; Singh, P.P.; Dubey, S.K.; Saha, R.N.; Singhvi, G. Nanocarriers for Ocular Drug Delivery: Current Status and Translational Opportunity. RSC Adv. 2020, 10, 27835–27855. [Google Scholar] [CrossRef]
- Pinto Reis, C.; Neufeld, R.J.; Ribeiro, A.J.; Veiga, F.; Nanoencapsulation, I. Methods for Preparation of Drug-Loaded Polymeric Nanoparticles. Nanomed. Nanotechnol. Biol. Med. 2006, 2, 8–21. [Google Scholar] [CrossRef] [Green Version]
- Vauthier, C.; Bouchemal, K. Methods for the Preparation and Manufacture of Polymeric Nanoparticles. Pharm. Res. 2009, 26, 1025–1058. [Google Scholar] [CrossRef] [PubMed]
- Matha, K.; Lollo, G.; Taurino, G.; Respaud, R.; Marigo, I.; Shariati, M.; Bussolati, O.; Vermeulen, A.; Remaut, K.; Benoit, J.P. Bioinspired Hyaluronic Acid and Polyarginine Nanoparticles for DACHPt Delivery. Eur. J. Pharm. Biopharm. 2020, 150, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kalam, M.A. Development of Chitosan Nanoparticles Coated with Hyaluronic Acid for Topical Ocular Delivery of Dexamethasone. Int. J. Biol. Macromol. 2016, 89, 127–136. [Google Scholar] [CrossRef]
- Grimaudo, M.A.; Concheiro, A.; Alvarez-Lorenzo, C. Crosslinked Hyaluronan Electrospun Nanofibers for Ferulic Acid Ocular Delivery. Pharmaceutics 2020, 12, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.; Chen, Y.S.; Rupenthal, I.D. Hyaluronic Acid Coated Albumin Nanoparticles for Targeted Peptide Delivery to the Retina. Mol. Pharm. 2017, 14, 533–545. [Google Scholar] [CrossRef]
- Liu, D.; Lian, Y.; Fang, Q.; Liu, L.; Zhang, J.; Li, J. Hyaluronic-Acid-Modified Lipid-Polymer Hybrid Nanoparticles as an Efficient Ocular Delivery Platform for Moxifloxacin Hydrochloride. Int. J. Biol. Macromol. 2018, 116, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Amato, G.; Grimaudo, M.A.; Alvarez-Lorenzo, C.; Concheiro, A.; Carbone, C.; Bonaccorso, A.; Puglisi, G.; Musumeci, T. Hyaluronan/Poly-L-Lysine/Berberine Nanogels for Impaired Wound Healing. Pharmaceutics 2020, 13, 34. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Wang, M.-C.; Chen, Z.-Y.; Chiu, W.-Y.; Chen, K.-H.; Lin, I.-C.; Yang, W.-C.V.; Wu, C.-C.; Tseng, C.-L. Gelatin-Epigallocatechin Gallate Nanoparticles with Hyaluronic Acid Decoration as Eye Drops Can Treat Rabbit Dry-Eye Syndrome Effectively via Inflammatory Relief. Int. J. Nanomed. 2018, 13, 7251–7273. [Google Scholar] [CrossRef] [Green Version]
- Rubenicia, A.M.L.; Cubillan, L.D.P.; Sicam, V.A.D.P.; Macabeo, A.P.G.; Villaflores, O.B.; Castillo, A.L. Intraocular Pressure Reduction Effect of 0.005% Latanoprost Eye Drops in a Hyaluronic Acid-Chitosan Nanoparticle Drug Delivery System in Albino Rabbits. Transl. Vis. Sci. Technol. 2021, 10, 2. [Google Scholar] [CrossRef]
- Bongiovì, F.; Fiorica, C.; Palumbo, F.S.; di Prima, G.; Giammona, G.; Pitarresi, G. Imatinib-Loaded Micelles of Hyaluronic Acid Derivatives for Potential Treatment of Neovascular Ocular Diseases. Mol. Pharm. 2018, 15, 5031–5045. [Google Scholar] [CrossRef]
- Apaolaza, P.S.; Busch, M.; Asin-Prieto, E.; Peynshaert, K.; Rathod, R.; Remaut, K.; Dünker, N.; Göpferich, A. Hyaluronic Acid Coating of Gold Nanoparticles for Intraocular Drug Delivery: Evaluation of the Surface Properties and Effect on Their Distribution. Exp. Eye Res. 2020, 198, 14–4835. [Google Scholar] [CrossRef] [PubMed]
- Radwan, S.E.S.; El-Kamel, A.; Zaki, E.I.; Burgalassi, S.; Zucchetti, E.; El-Moslemany, R.M. Hyaluronic-Coated Albumin Nanoparticles for the Non-Invasive Delivery of Apatinib in Diabetic Retinopathy. Int. J. Nanomed. 2021, 16, 4481–4494. [Google Scholar] [CrossRef] [PubMed]
- Osorno, L.L.; Maldonado, D.E.; Whitener, R.J.; Brandley, A.N.; Yiantsos, A.; Medina, J.D.R.; Byrne, M.E. Amphiphilic PLGA-PEG-PLGA Triblock Copolymer Nanogels Varying in Gelation Temperature and Modulus for the Extended and Controlled Release of Hyaluronic Acid. J. Appl. Polym. Sci. 2019, 48678, 48678. [Google Scholar] [CrossRef]
- Devoldere, J.; Wels, M.; Peynshaert, K.; Dewitte, H.; de Smedt, S.C.; Remaut, K. The Obstacle Course to the Inner Retina: Hyaluronic Acid-Coated Lipoplexes Cross the Vitreous but Fail to Overcome the Inner Limiting Membrane. Eur. J. Pharm. Biopharm. 2019, 141, 161–171. [Google Scholar] [CrossRef]
- Moustafa, M.A.; Elnaggar, Y.S.R.; El-Refaie, W.M.; Abdallah, O.Y. Hyalugel-Integrated Liposomes as a Novel Ocular Nanosized Delivery System of Fluconazole with Promising Prolonged Effect. Int. J. Pharm. 2017, 534, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chen, R.; Xu, M.; Qiao, J.; Yan, L.; Guo, X.D. Hyaluronic Acid Modified MPEG-b-PAE Block Copolymer Aqueous Micelles for Efficient Ophthalmic Drug Delivery of Hydrophobic Genistein. Drug Deliv. 2018, 25, 1258–1265. [Google Scholar] [CrossRef] [Green Version]
- Gomes, J.A.P.; Amankwah, R.; Powell-Richards, A. Sodium Hyaluronate (Hyaluronic Acid) Promotes Migration of Human Corneal Epithelial Cells in Vitro. Br. J. Ophthalmol. 2004, 88, 821–825. [Google Scholar] [CrossRef] [Green Version]
- De La Fuente, M.; Seijo, B.; Alonso, M.J. Novel Hyaluronic Acid-Chitosan Nanoparticles for Ocular Gene Therapy. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2016–2024. [Google Scholar] [CrossRef] [Green Version]
- Karpecki, P.M. HA: No Laughing Matter. Available online: https://www.reviewofoptometry.com/article/ha-no-laughing-matter (accessed on 25 June 2022).
- Hynnekleiv, L.; Magno, M.; Vernhardsdottir, R.R.; Moschowits, E.; Tønseth, K.A.; Dartt, D.A.; Vehof, J.; Utheim, T.P. Hyaluronic Acid in the Treatment of Dry Eye Disease. Acta Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Beck, R.; Stachs, O.; Koschmieder, A.; Mueller-Lierheim, W.G.K.; Peschel, S.; van Setten, G.B. Hyaluronic Acid as an Alternative to Autologous Human Serum Eye Drops: Initial Clinical Results with High-Molecular-Weight Hyaluronic Acid Eye Drops. Case Rep. Ophthalmol. 2019, 10, 244–255. [Google Scholar] [CrossRef]
- Labetoulle, M.; Chiambaretta, F.; Shirlaw, A.; Leaback, R.; Baudouin, C. Osmoprotectants, Carboxymethylcellulose and Hyaluronic Acid Multi-Ingredient Eye Drop: A Randomised Controlled Trial in Moderate to Severe Dry Eye. Eye 2017, 31, 1409–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carracedo, G.; Pastrana, C.; Serramito, M.; Rodriguez-Pomar, C. Evaluation of Tear Meniscus by Optical Coherence Tomography after Different Sodium Hyaluronate Eyedrops Instillation. Acta Ophthalmol. 2019, 97, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Fraga, J.; López-De La Rosa, A.; Arauzo, F.B.; Rodríguez, R.U.; González-García, M.J. Efficacy and Safety of 0.2% Hyaluronic Acid in the Management of Dry Eye Disease. Eye Contact Lens 2017, 43, 57–63. [Google Scholar] [CrossRef] [PubMed]
- López-De La Rosa, A.; Pinto-Fraga, J.; Blázquez Arauzo, F.; Rodríguez, R.U.; González-García, M.J. Safety and Efficacy of an Artificial Tear Containing 0.3% Hyaluronic Acid in the Management of Moderate-to-Severe Dry Eye Disease. Eye Contact Lens 2017, 43, 383–388. [Google Scholar] [CrossRef]
- Clinical Evaluation of Visco-Assisted CyPass® Micro-Stent Implantation in Patients with Open Angle Glaucoma. Available online: https://clinicaltrials.gov/ct2/show/NCT02448875 (accessed on 22 June 2022).
- Cazorla-Luna, R.; Martín-Illana, A.; Notario-Pérez, F.; Ruiz-Caro, R.; Veiga, M.D. Naturally Occurring Polyelectrolytes and Their Use for the Development of Complex-Based Mucoadhesive Drug Delivery Systems: An Overview. Polymers 2021, 13, 2241. [Google Scholar] [CrossRef]
- Papagiannopoulos, A. Current Research on Polyelectrolyte Nanostructures: From Molecular Interactions to Biomedical Applications. Macromol 2021, 1, 155–172. [Google Scholar] [CrossRef]
- Yadav, S.; Sharma, A.K.; Kumar, P. Nanoscale Self-Assembly for Therapeutic Delivery. Front. Bioeng. Biotechnol. 2020, 8, 127. [Google Scholar] [CrossRef]
- Kulkarni, A.D.; Vanjari, Y.H.; Sancheti, K.H.; Patel, H.M.; Belgamwar, V.S.; Surana, S.J.; Pardeshi, C.V. Polyelectrolyte Complexes: Mechanisms, Critical Experimental Aspects, and Applications. Artif. Cells Nanomed. Biotechnol. 2016, 44, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- van der Gucht, J.; Spruijt, E.; Lemmers, M.; Stuart, M.A.C. Polyelectrolyte Complexes: Bulk Phases and Colloidal Systems. J. Colloid Interface Sci. 2011, 361, 407–422. [Google Scholar] [CrossRef]
- Shah, S.; Eyler, A.; Tabandeh, S.; Leon, L. Electrostatically Driven Self-Assembled Nanoparticles and Coatings. In Nanoparticles for Biomedical Applications; Chung, E.J., Rinaldi, L., Leon, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 349–370. [Google Scholar] [CrossRef]
- Ou, Z.; Muthukumar, M. Entropy and Enthalpy of Polyelectrolyte Complexation: Langevin Dynamics Simulations. J. Chem. Phys. 2006, 124, 154902. [Google Scholar] [CrossRef]
- Lebovka, N.I. Aggregation of Charged Colloidal Particles. In Polyelectrolyte Complexes in the Dispersed and Solid State I: Principles and Theory; Muller, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 57–97. [Google Scholar]
- Tsuchida, E. Formation of Polyelectrolyte Complexes and Their Structures. J. Macromol. Sci. Part A 1994, 31, 1–15. [Google Scholar] [CrossRef]
- Philipp, B.; Dautzenberg, H.; Linow, K.J.; Kötz, J.; Dawydoff, W. Polyelectrolyte Complexes—Recent Developments and Open Problems. Prog. Polym. Sci. 1989, 14, 91–172. [Google Scholar] [CrossRef]
- Ankerfors, C. Polyelectrolyte Complexes: Preparation, Characterization, and Use for Control of Wet and Dry Adhesion between Surfaces. Ph.D. Thesis, KTH Royal Institute of Technology, Stockholm, Sweden, 2012. [Google Scholar]
- Hartig, S.M.; Greene, R.R.; Dikov, M.M.; Prokop, A.; Davidson, J.M. Multifunctional Nanoparticulate Polyelectrolyte Complexes. Pharm. Res. 2007, 24, 2353–2369. [Google Scholar] [CrossRef]
- Quiñones, J.P.; Peniche, H.; Peniche, C. Chitosan Based Self-Assembled Nanoparticles in Drug Delivery. Polymers 2018, 10, 235. [Google Scholar] [CrossRef] [Green Version]
- van Le, H.; Dulong, V.; Picton, L.; le Cerf, D. Polyelectrolyte Complexes of Hyaluronic Acid and Diethylaminoethyl Dextran: Formation, Stability and Hydrophobicity. Colloids Surf. A Physicochem. Eng. Asp. 2021, 629, 127485. [Google Scholar] [CrossRef]
- Hotze, E.M.; Phenrat, T.; Lowry, G.V. Nanoparticle Aggregation: Challenges to Understanding Transport and Reactivity in the Environment. J. Environ. Qual. 2010, 39, 1909–1924. [Google Scholar] [CrossRef] [Green Version]
- Biorender. BioRender. Available online: https://biorender.com/ (accessed on 17 January 2022).
- Ferreira, L.M.B.; dos Santos, A.M.; Boni, F.I.; dos Santos, K.C.; Robusti, L.M.G.; de Souza, M.P.C.; Ferreira, N.N.; Carvalho, S.G.; Cardoso, V.M.O.; Chorilli, M.; et al. Design of Chitosan-Based Particle Systems: A Review of the Physicochemical Foundations for Tailored Properties. Carbohydr. Polym. 2020, 250, 116968. [Google Scholar] [CrossRef]
- Leite, E.R.; Ribeiro, C. Basic Principles: Thermodynamics and Colloidal Chemistry. In Crystallization and Growth of Colloidal Nanocrystals; Springer: New York, NY, USA, 2012; pp. 7–17. [Google Scholar] [CrossRef]
- Ohshima, H. The Derjaguin—Landau—Verway—Overbeek (DLVO) Theory of Colloidal Stability. In Electrical Phenomena at Interfaces and Bionterfaces—Fundamentals and Applications in Nano-, Bio-, and Environmental Sciences; Ohshima, H., Ed.; John Wiley & Sons Ltd.: New Jersey, NJ, USA, 2012; pp. 27–34. [Google Scholar]
- Mero, A.; Campisi, M. Hyaluronic Acid Bioconjugates for the Delivery of Bioactive Molecules. Polymers 2014, 6, 346–369. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.H.; Jones, S.A.; Forbes, B.; Martin, G.P.; Brown, M.B. Hyaluronan: Pharmaceutical Characterization and Drug Delivery. Drug Deliv. J. Deliv. Target. Ther. Agents 2005, 12, 327–342. [Google Scholar] [CrossRef]
- Meka, V.S.; Sing, M.K.G.; Pichika, M.R.; Nali, S.R.; Kolapalli, V.R.M.; Kesharwani, P. A Comprehensive Review on Polyelectrolyte Complexes. Drug Discov. Today 2017, 22, 1697–1706. [Google Scholar] [CrossRef]
- Grimaudo, M.A.; Amato, G.; Carbone, C.; Diaz-Rodriguez, P.; Musumeci, T.; Concheiro, A.; Alvarez-Lorenzo, C.; Puglisi, G. Micelle-Nanogel Platform for Ferulic Acid Ocular Delivery. Int. J. Pharm. 2020, 576, 118986. [Google Scholar] [CrossRef]
- Kale, N.R.; Dutta, D.; Carstens, W.; Mallik, S.; Quadir, M. Functional Applications of Polyarginine-Hyaluronic Acid-Based Electrostatic Complexes. Bioelectricity 2020, 2, 158–166. [Google Scholar] [CrossRef]
- Malay, Ö.; Yal, D.Ï.; Bat, A.Ï.; Bayraktar, O. Characterisation of Silk Fibroin/Hyaluronic Acid Polyelectrolyte Complex (PEC) Films. J. Therm. Anal. Calorim. 2008, 94, 749–755. [Google Scholar] [CrossRef] [Green Version]
- Deb Nath, S.; Abueva, C.; Kim, B.; Taek, B. Chitosan—Hyaluronic Acid Polyelectrolyte Complex Scaffold Crosslinked with Genipin for Immobilization and Controlled Release of BMP-2. Carbohydr. Polym. 2015, 115, 160–169. [Google Scholar] [CrossRef]
- Wu, D.; Delair, T. Stabilization of Chitosan/Hyaluronan Colloidal Polyelectrolyte Complexes in Physiological Conditions. Carbohydr. Polym. 2015, 119, 149–158. [Google Scholar] [CrossRef]
- Chaharband, F.; Daftarian, N.; Kanavi, M.R.; Varshochian, R.; Hajiramezanali, M.; Norouzi, P.; Arefian, E.; Atyabi, F.; Dinarvand, R. Trimethyl Chitosan-Hyaluronic Acid Nano-Polyplexes for Intravitreal VEGFR-2 SiRNA Delivery: Formulation and in Vivo Efficacy Evaluation. Nanomed. Nanotechnol. Biol. Med. 2020, 26, 102181. [Google Scholar] [CrossRef]
- Silva, B.; Marto, J.; Braz, B.S.; Delgado, E.; Almeida, A.J.; Gonçalves, L. New Nanoparticles for Topical Ocular Delivery of Erythropoietin. Int. J. Pharm. 2020, 576, 119020. [Google Scholar] [CrossRef]
- Carton, F.; Chevalier, Y.; Nicoletti, L.; Tarnowska, M.; Stella, B.; Arpicco, S.; Malatesta, M.; Jordheim, L.P.; Briançon, S.; Lollo, G. Rationally Designed Hyaluronic Acid-Based Nano-Complexes for Pentamidine Delivery. Int. J. Pharm. 2019, 568, 118526. [Google Scholar] [CrossRef]
- Battistini, F.D.; Tártara, L.I.; Boiero, C.; Guzmán, M.L.; Luciani-Giaccobbe, L.C.; Palma, S.D.; Allemandi, D.A.; Manzo, R.H.; Olivera, M.E. The Role of Hyaluronan as a Drug Carrier to Enhance the Bioavailability of Extended Release Ophthalmic Formulations. Hyaluronan-Timolol Ionic Complexes as a Model Case. Eur. J. Pharm. Sci. 2017, 105, 188–194. [Google Scholar] [CrossRef]
- Siyawamwaya, M.; Choonara, Y.E.; Bijukumar, D.; Kumar, P.; du Toit, L.C.; Pillay, V. A Review: Overview of Novel Polyelectrolyte Complexes as Prospective Drug Bioavailability Enhancers. Int. J. Polym. Mater. Polym. Biomater. 2015, 64, 955–968. [Google Scholar] [CrossRef]
- Wu, D.; Zhu, L.; Li, Y.; Zhang, X.; Xu, S.; Yang, G.; Delair, T. Chitosan-Based Colloidal Polyelectrolyte Complexes for Drug Delivery: A Review. Carbohydr. Polym. 2020, 238, 116126. [Google Scholar] [CrossRef]
- Dreffs, A.; Henderson, D.; Dmitriev, A.V.; Antonetti, D.A.; Linsenmeier, R.A. Retinal PH and Acid Regulation during Metabolic Acidosis. Curr. Eye Res. 2018, 43, 902. [Google Scholar] [CrossRef]
- Rawas-Qalaji, M.; Williams, C.A. Advances in Ocular Drug Delivery. Curr. Eye Res. 2012, 37, 345–356. [Google Scholar] [CrossRef]
- Kaur, J.; Kaur, G. Optimization of PH Conditions and Characterization of Polyelectrolyte Complexes between Gellan Gum and Cationic Guar Gum. Polym. Adv. Technol. 2018, 29, 3035–3048. [Google Scholar] [CrossRef]
- Kayitmazer, A.B.; Koksal, A.F.; Kilic Iyilik, E. Complex Coacervation of Hyaluronic Acid and Chitosan: Effects of PH, Ionic Strength, Charge Density, Chain Length and the Charge Ratio. Soft Matter 2015, 11, 8605–8612. [Google Scholar] [CrossRef]
- Pan, W.; Yin, D.-X.; Jing, H.-R.; Chang, H.-J.; Wen, H.; Liang, D.-H. Core-Corona Structure Formed by Hyaluronic Acid and Poly(L-Lysine) via Kinetic Path. Chin. J. Polym. Sci. 2019, 37, 36–42. [Google Scholar] [CrossRef]
- Sukhanova, A.; Bozrova, S.; Sokolov, P.; Berestovoy, M.; Karaulov, A.; Nabiev, I. Dependence of Nanoparticle Toxicity on Their Physical and Chemical Properties. Nanoscale Res. Lett. 2018, 13, 44. [Google Scholar] [CrossRef] [Green Version]
- Dautzenberg, H.; Karibyants, N. Polyelectrolyte Complex Formation in Highly Aggregating Systems. Effect of Salt: Response to Subsequent Addition of NaCl. Macromol. Chem. Phys. 1999, 200, 118–125. [Google Scholar] [CrossRef]
- Zhang, Y.; Yildirim, E.; Antila, H.S.; Valenzuela, L.D.; Sammalkorpi, M.; Lutkenhaus, J.L. The Influence of Ionic Strength and Mixing Ratio on the Colloidal Stability of PDAC/PSS Polyelectrolyte Complexes. Soft Matter 2015, 11, 7392–7401. [Google Scholar] [CrossRef] [Green Version]
- Golchoobi, A.; Khosravi, A.; Modarress, H.; Ahmadzadeh, A. Effect of Charge, Size and Temperature on Stability of Charged Colloidal Nano Particles. Chin. J. Chem. Phys. 2012, 25, 617–624. [Google Scholar] [CrossRef]
- de Vasconcelos, C.L.; Pereira, M.R.; Fonseca, J.L.C. Polyelectrolytes in Solution and the Stabilization of Colloids. J. Dispers. Sci. Technol. 2005, 26, 59–70. [Google Scholar] [CrossRef]
- Koetz, J.; Kosmella, S. Semi Diluted Polyanion-Polycation Systems (Turbid Polyelectrolyte Complexes). In Polyelectrolytes and Nanoparticles; Barth, H.G., Pasch, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 41–43. [Google Scholar]
- Mitsubayashi, K.; Ogasawara, K.; Yokoyama, K.; Takeuchi, T.; Tsuru, T.; Karube, I. Measurement of Tear Electrolyte Concentration and Turnover Rate Using a Flexible Conductimetric Sensor. Technol. Health Care 1995, 3, 117–121. [Google Scholar] [CrossRef] [PubMed]
- van Haeringen, N.J. Clinical Biochemistry of Tears. Surv. Ophthalmol. 1981, 26, 84–96. [Google Scholar] [CrossRef]
- Stahl, U.; Willcox, M.; Stapleton, F. Osmolality and Tear Film Dynamics. Clin. Exp. Optom. 2012, 95, 3–11. [Google Scholar] [CrossRef]
- Li, Q.; Li, X.; Zhao, C. Strategies to Obtain Encapsulation and Controlled Release of Small Hydrophilic Molecules. Front. Bioeng. Biotechnol. 2020, 8, 437. [Google Scholar] [CrossRef]
- Henein, C.; Awwad, S.; Ibeanu, N.; Vlatakis, S.; Brocchini, S.; Khaw, P.T.; Bouremel, Y. Hydrodynamics of Intravitreal Injections into Liquid Vitreous Substitutes. Pharmaceutics 2019, 11, 371. [Google Scholar] [CrossRef] [Green Version]
- Azhdam, A.M.; Goldberg, R.A.; Ugradar, S. In Vivo Measurement of the Human Vitreous Chamber Volume Using Computed Tomography Imaging of 100 Eyes. Transl. Vis. Sci. Technol. 2020, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Schatz, C.; Domard, A.; Viton, C.; Pichot, C. Versatile and Efficient Formation of Colloids of Biopolymer-Based Polyelectrolyte Complexes. Biomacromolecules 2004, 5, 1882–1892. [Google Scholar] [CrossRef]

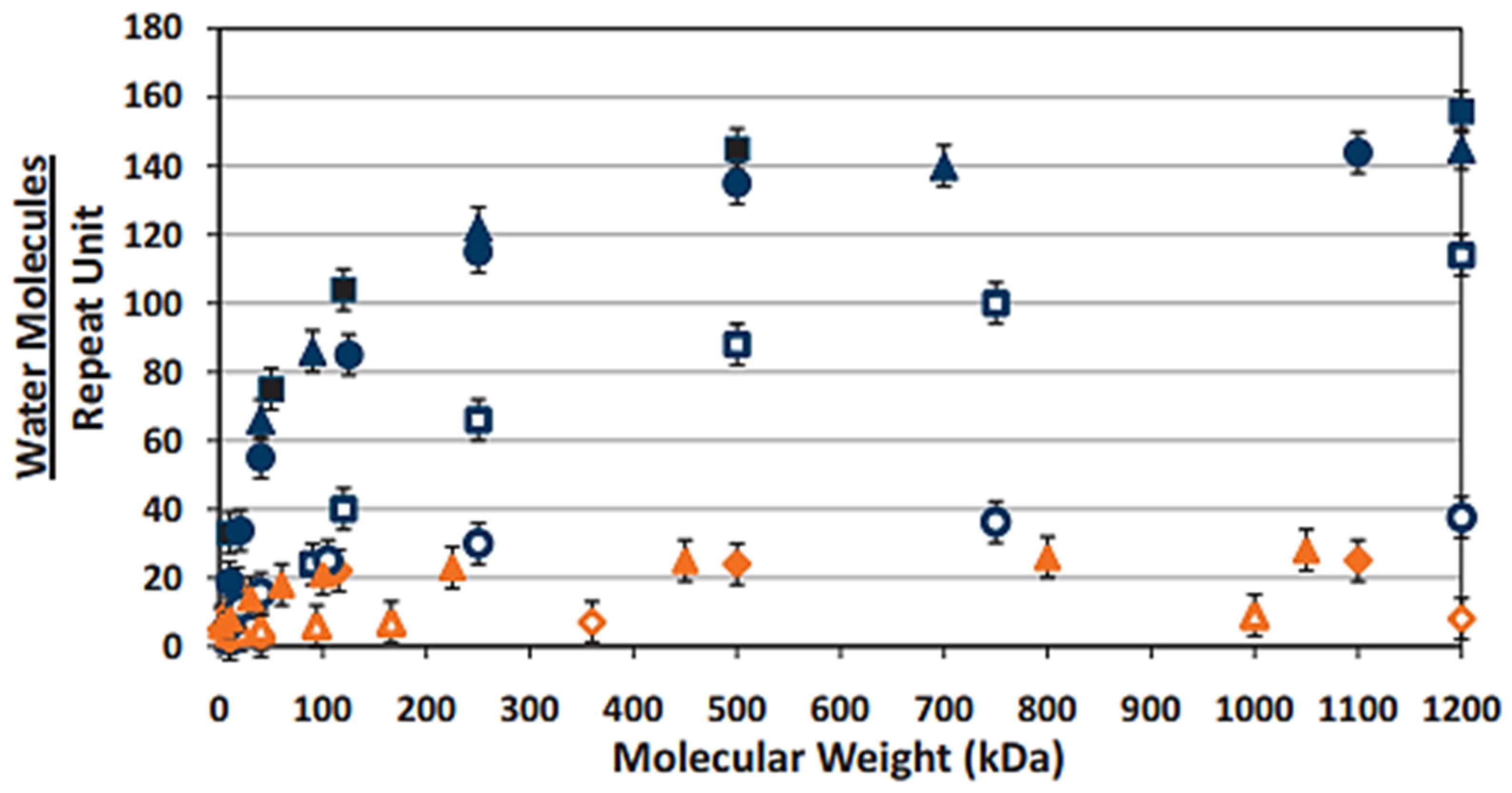
 ) exhibiting superior water retention in comparison to the other polyelectrolyte materials, increases as a function of MW. (
) exhibiting superior water retention in comparison to the other polyelectrolyte materials, increases as a function of MW. (  —dextran sodium sulfate,
—dextran sodium sulfate,  —hydroxypropyl methylcellulose,
—hydroxypropyl methylcellulose,  —dextran,
—dextran,  —carboxymethylcellulose,
—carboxymethylcellulose,  —poly(acrylic acid),
—poly(acrylic acid),  —poly(methacrylic acid),
—poly(methacrylic acid),  —polyvinyl alcohol,
—polyvinyl alcohol,  —polyvinyl pyrrilidone). (Reproduced with permission from Ref. [122]. 2014, White, C.J., Thomas, C.R. and Byrne, M.E. “Bringing comfort to the masses: A novel evaluation of comfort agent solution properties”; published by Contact Lens and Anterior Eye.
) exhibiting superior water retention in comparison to the other polyelectrolyte materials, increases as a function of MW. ( —dextran sodium sulfate, —hydroxypropyl methylcellulose, —dextran, —carboxymethylcellulose, —poly(acrylic acid), —poly(methacrylic acid), —polyvinyl alcohol, —polyvinyl pyrrilidone). (Reproduced with permission from Ref. [122]. 2014, White, C.J., Thomas, C.R. and Byrne, M.E. “Bringing comfort to the masses: A novel evaluation of comfort agent solution properties”; published by Contact Lens and Anterior Eye.
—polyvinyl pyrrilidone). (Reproduced with permission from Ref. [122]. 2014, White, C.J., Thomas, C.R. and Byrne, M.E. “Bringing comfort to the masses: A novel evaluation of comfort agent solution properties”; published by Contact Lens and Anterior Eye.
) exhibiting superior water retention in comparison to the other polyelectrolyte materials, increases as a function of MW. ( —dextran sodium sulfate, —hydroxypropyl methylcellulose, —dextran, —carboxymethylcellulose, —poly(acrylic acid), —poly(methacrylic acid), —polyvinyl alcohol, —polyvinyl pyrrilidone). (Reproduced with permission from Ref. [122]. 2014, White, C.J., Thomas, C.R. and Byrne, M.E. “Bringing comfort to the masses: A novel evaluation of comfort agent solution properties”; published by Contact Lens and Anterior Eye.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pH | Ionisation | Stability | Viscosity |
|---|---|---|---|
 | The carboxylate anion primarily exists in its protonated state (COOH). Protonation of the -NH- group of the acetylamine groups may also occur at a pH < 1.6.  | At a pH of <2, cleavage of the β-1-3 and β-1-4 glycosidic bonds via acid hydrolysis occurs. This results in the reformation of the individual monosaccharide units coupled with a decrease in molecular mass. | A significant decrease in HA viscosity occurs within this pH range. pH-induced degradation of the individual HA chains reduces both the rigidity and the extent of interchain entanglement. Suppression of electrostatic repulsion between the COO- anions contributes to the formation of a more densely compact gel state. Below 1.6, a gel-sol transition occurs due to acetylamino group protonation. |
 | The carboxylate anion exists in its deprotonated state (COO−). Electrostatic repulsion between COO- anions allows for hydrophilic domain expansion. Protonation of the -NH- groups is at a minimum. | The stability of the tertiary β sheet structure is enhanced by the formation of an intermolecular hydrogen bond between the hydroxyl and ether groups  and carboxylate anions and acetylamine groups.  Water molecules can also indirectly facilitate the formation of these hydrogen bonds by behaving as bridging molecules. | HA exhibits both viscoelastic and pseudoplastic flow behaviour. Increasing shear rate disrupts hydrogen bonding and hydrophobic interactions, resulting in increased chain flexibility and network degradation. This allows the individual chains to align in the direction of the applied flow, leading to a temporary decrease in viscosity. However, HA is also non-thixotropic. Reformation of the network occurs over time upon removal of the shear stress. |
 | At pH > 12, the COO- anions remain in their deprotonated state. The hydroxyl (OH) atoms also exist as alkoxyl anions due to the removal of the hydrogen atoms via excess hydroxide ions. | Base-catalysed hydrolysis of the β-1-3 and β-1-4 glycosidic bonds occurs. Due to the deprotonation of the hydroxyl groups, the hydrogen bonds responsible for the stabilisation of the tertiary network begin to degrade. | Deformation of the intermolecular hydrogen bonds reduces the rigidity of the backbones of the HA chains. This results in the degradation of the entangled network, coupled with an increase in chain flexibility and mobility. |
| Formulation | Preparation Method | Excipients | Function | HA MW (kDa) | Desired Effect | Therapeutic | Key Findings | Further Investigation | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Nanoparticles | Ionotropic Gelation | Chitosan (CS) and tripolyphoshapte (TPP) | Coating agent | 200 | Improved cellular targeting via receptor-mediated internalisation. | Dexamethasone sodium phosphate (DEX-SP) | Increase in size from 305 ± 14 nm to 386 ± 13 nm and reversal of ZP values from high positive to high negative with HA coating. Coating with HA decreased initial DEX -SP in vitro burst release by approximately 15%. Similar release profiles were obtained between the 1 and 12 h time points. | In vitro/ex vivo mucoadhesion In vitro cytotoxicity analysis In vitro CD44- binding and cellular uptake analysis (study conducted by Matha et al. [156] to investigate HA-CD44 mediated cellular uptake). | [157] |
| Nanofibres | Electrospinning | Polyvinylpyrrolidone | Excipient | 600–1100 | Enhanced ocular bioavailability after conjunctival application. | Ferulic acid (FA) and ε-poly(L-lysine) (ε-PLL) | Crosslinking the HA nanofibres with ε-PLL formed electrostatically cross-linked nanofibre-laden inserts (blank inserts only). Blank and FA-loaded inserts preserved chorioallantoic membrane integrity (embryonated hen’s egg). | Ex vivo conjunctival permeation and retention studies. | [158] |
| Nanoparticles | Desolvation | Human serum albumin | Surface ligand | 120 | Targeted retinal delivery via active CD44 targeting. | Connexin 43 mimetic peptide (Cx43-MP) | The HA-coated nanoparticles exhibited enhanced ex vivo retinal penetration into the outer nuclear layer and retinal pigment epithelium in comparison to the uncoated control group 4 h post-incubation due to high CD44 ligand interaction. 1.2- and 1.5-fold increase in fluorescence intensity in neural retina and retinal pigment epithelium/choroid with HA-coated particles in comparison to the uncoated group. HA-modification exhibited superior ARPE-19 in vitro internalisation in comparison to control. | In vivo permeation studies. In vivo Cx43-MP quantification to determine whether nanoparticle encapsulation prolongs the half-life of Cx43-MP in the vitreal injection site after injection. | [159] |
| Lipid–polymer hybrid nanoparticles (LPHNP) | Ionotropic gelation and thin-film hydration | CS, TPP, Lipoid E 80, cholesterol and DPPE | Surface Ligand | 10 | Enhanced corneal retention and permeability. | Moxifloxacin hydrochloride (MCF.HCL) | The apparent permeability coefficient of the HA-coated LPHNPs through excised rabbit cornea was 3.29- and 1.69-fold higher than those of the MXF commercial product and the uncoated LPHNP formulation. The area under the curve of the HA-coated LPHNPs between 0 and 6 h was 6.74 and 2.56 times higher than that of the commercial MXF product and the control chitosan nanoparticle formulation, respectively. Fluorescent-labelled HA-coated LPHNPs exhibited stronger fluorescence within the corneal and conjunctival tissues of a rabbit model after ex vivo fluorescent imaging analysis. | Although the enhanced precorneal retention of the HA-coated LPHNP formulation was attributed to the mucoadhesive capabilities of HA, no mucoadhesion studies were conducted. In vitro stability studies to evaluate the stability of the HA-coated LPHNPs in comparison to the uncoated LPHNP and control nanoparticle formulations. | [160] |
| Nanogels | Physical crosslinking | ε-PLL | Excipient | 200/700/1200 | General wound healing capabilities. | Berberine | Due to macrogelation and polydispersity index values above 0.3, nanogels formulated with 700 and 1200 kDa HA or HA concentrations above 2 mg/mL were excluded from further characterisation studies. In vitro berberine release was sustained for 24 h after an initial burst release of approximately 50% of the total loaded berberine within 45 min. Blank nanogels exhibited greater efficacy in promoting in vitro wound healing over 48 h in comparison to the berberine-loaded nanogels, which they attributed to the decreased availability of HA as a result of electrostatic interaction with berberine. | A rheological assessment of optimised nanogels. These nanogels were prepared for general wound healing purposes. If designed for corneal wound healing, nanogels exhibiting high viscosity may be beneficial for increasing the retention time and pharmacological profile of the formulation. | [161] |
| Nanoparticles | Self-assembly | Gelatin | Surface ligand | Not Listed | Mucoadhesion to the corneal–conjunctival interface. | Epigallocatechin gallate (EGCG) | HA-coated gelatin–EGCG nanoparticles (GEH) exhibited greater accumulation in human corneal epithelial cells in comparison to control gelatin–EGCG nanoparticles. 100 min after in vivo administration in a murine model, the GEH formulation demonstrated longer retention on the ocular surface in comparison to both the control nanoparticles and an EGCG solution. After twice-daily administrations for three weeks, the GEH formulation restored normal corneal architecture following benzalkonium chloride-induced dry eye syndrome (DES) in a rabbit model. | A study to evaluate the effect of HA MW on the mucoadhesive capabilities and ocular surface retention times of the GEH formulation. | [162] |
| Nanomicelles | Self-assembly | D-α-Tocopherolpolyethylene glycol succinate (VitE-TPGS) and octylphenoxy poly(ethyleneoxy)ethanol | Excipient | 1650 | Mucoadhesion to the corneal surface and prevention of corneal damage caused by surfactant excipients. | Cyclosporine A (CyA) | The addition of HA to the micellar formulation significantly decreased the rate of cyclosporine A elimination from the corneal surface in a rabbit model, as evidenced by an elimination rate constant that was almost 4 times smaller than that of the commercial product (Ikervis®) and a five-fold increase in CyA half-life. | Additional in vivo efficacy studies to determine the effective dose of CyA required to treat DES. The dual efficacy of the nanomicellar formulation in delivering CyA for DES treatment and minimising corneal surface abnormalities via HA-mediated re-epithelisation and wound healing. | [7] |
| Nanoparticles | Ionotropic gelation | CS and TPP | Surface ligand | Not Listed | Mucoadhesion to the corneal and conjunctival surface. | Latanoprost | Treatment with HA-CS-latanoprost link nanoparticles led to a significant reduction in daily IOP measurements (27.3 ± 2.2% reduction) in comparison to a 0.005% latanoprost eye drop and Xalatan® (0.005%) over a three-day treatment period in a rabbit model. | In vivo cytotoxicity and ocular tolerability analysis. In vivo latanoprost release and quantification in rabbit tear fluid and/or the mucus layer. | [163] |
| Nanomicelles | Co-solvent evaporation | HA-ethylenediamine-hexadecyl group derivatives | Excipient | 7.3 | Mucoadhesion and enhanced retention time on the corneal surface. | Imatinib | HA micellar decoration with polyethylene glycol (PEG) and L-carnitine (CRN) improved transcorneal permeation in an in vitro human corneal epithelial cell model and an ex vivo bovine cornea model. Corneal permeation coefficients increased by 10.5 (free HA), 20.5 (HA-PEG), and 16.5 (HA-CRN) times in comparison to an imatinib suspension (0.5 mg/mL). | In vivo imatinib pharmacokinetic analysis. | [164] |
| Nanoparticles | Turkevich method | Gold | Coating agent | 5 | Improved intraocular mobility and targetability. | N/A | Chemical conjugation of thiolated HA to the surface of the gold nanoparticles allowed for enhanced diffusion through retinal explants (from the ganglion cell layer to the photoreceptor layer) in comparison to the uncoated nanoparticles. | Long-term in vitro analysis of antiangiogenic and antioxidant effects of gold nanoparticles. Physicochemical analysis of therapeutic-laden, HA-coated gold nanoparticles. | [165] |
| Nanoparticle | Desolvation | Bovine serum albumin | Coating agent | 1400 | Enhanced binding to CD44 receptors expressed on RPE-19 cells and minimisation of diabetic vascular adverse effects. | Apatinib | In comparison to uncoated nanoparticles (3.55 ± 0.81 fluorescence intensity), the HA-coated nanoparticles exhibited greater retinal accumulation (12.28 ± 1.39 fluorescence intensity) 5 h post-topical administration in a murine diabetic retinopathy model. The viscosity of the experimental mucin increased from 10.5 ± 0.2 cP to 28.42 ± 1.25 cP upon mixing with the HA-coated albumin nanoparticles. The ZP values of the coated nanoparticles also decreased from −37.3 ± 1.8 mV to −11.9 ± 0.8 mV upon incubation with mucin. | Evaluation of increased apatinib-laden HA-coated nanoparticle cellular uptake resulting from CD44-mediated endocytosis. | [166] |
| Nanogels | Mixing of amphiphilic polymers at various mass ratios | PLGA-PEG-PLGA triblock copolymer | Therapeutic | 800 | Extended and controlled release of HA via non-covalent modification. | Fluorescein isothiocyanate-HA | 5–30 kDa and 30–70 kDa PLL chains sustained the release of HA from the nanogels up to 30 days via counterion-mediated overlap of the anionic HA chains and cationic PLL. This prevented excessive swelling of the electrostatic complexes and allowed for a more gradual in vitro release of HA. | In vivo HA release and pharmacodynamic study to ensure that sustained HA release and optical transparency can be obtained in physiological conditions. | [167] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casey-Power, S.; Ryan, R.; Behl, G.; McLoughlin, P.; Byrne, M.E.; Fitzhenry, L. Hyaluronic Acid: Its Versatile Use in Ocular Drug Delivery with a Specific Focus on Hyaluronic Acid-Based Polyelectrolyte Complexes. Pharmaceutics 2022, 14, 1479. https://doi.org/10.3390/pharmaceutics14071479
Casey-Power S, Ryan R, Behl G, McLoughlin P, Byrne ME, Fitzhenry L. Hyaluronic Acid: Its Versatile Use in Ocular Drug Delivery with a Specific Focus on Hyaluronic Acid-Based Polyelectrolyte Complexes. Pharmaceutics. 2022; 14(7):1479. https://doi.org/10.3390/pharmaceutics14071479
Chicago/Turabian StyleCasey-Power, Saoirse, Richie Ryan, Gautam Behl, Peter McLoughlin, Mark E. Byrne, and Laurence Fitzhenry. 2022. "Hyaluronic Acid: Its Versatile Use in Ocular Drug Delivery with a Specific Focus on Hyaluronic Acid-Based Polyelectrolyte Complexes" Pharmaceutics 14, no. 7: 1479. https://doi.org/10.3390/pharmaceutics14071479