
Preclinical Evaluation of a New Format of 68Ga- and 111In-Labeled Affibody Molecule ZIGF-1R:4551 for the Visualization of IGF-1R Expression in Malignant Tumors Using PET and SPECT

 , ,
, ,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General
2.2. Protein Production
2.3. NODAGA Conjugation
2.4. Radiolabeling
2.5. In Vitro Studies
2.6. In Vivo Studies
3. Results
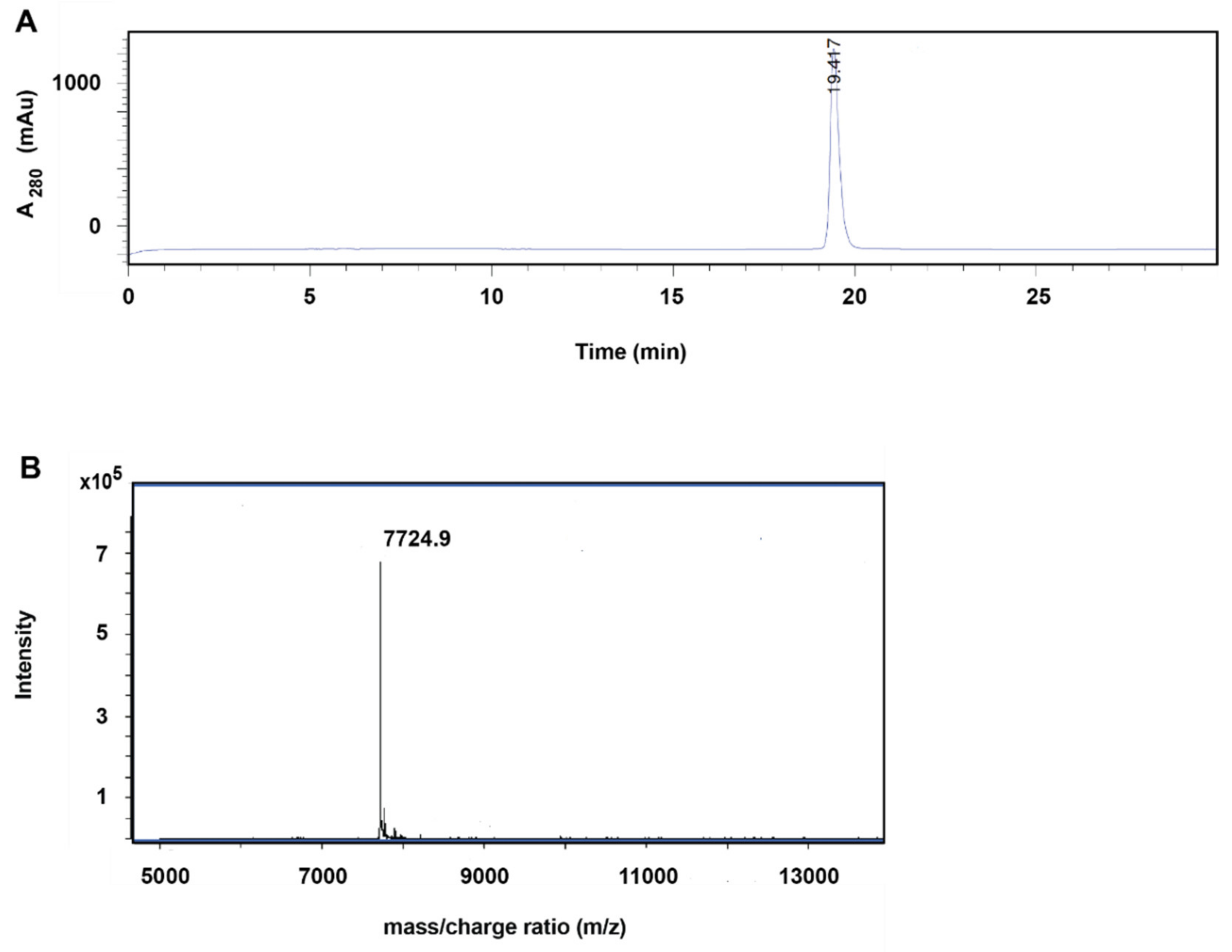
3.1. Production, Purification, and Conjugation
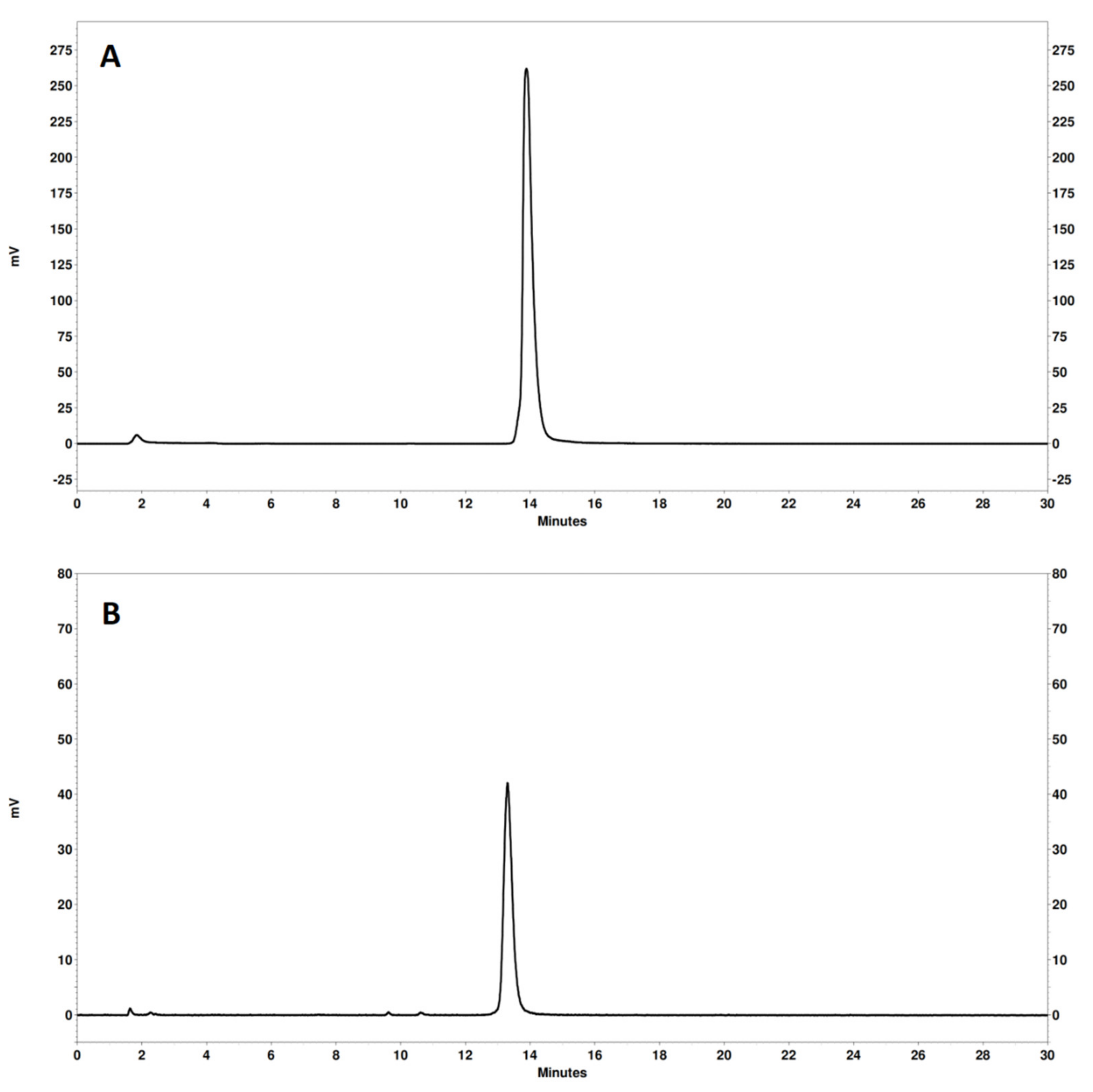
3.2. Radiolabeling
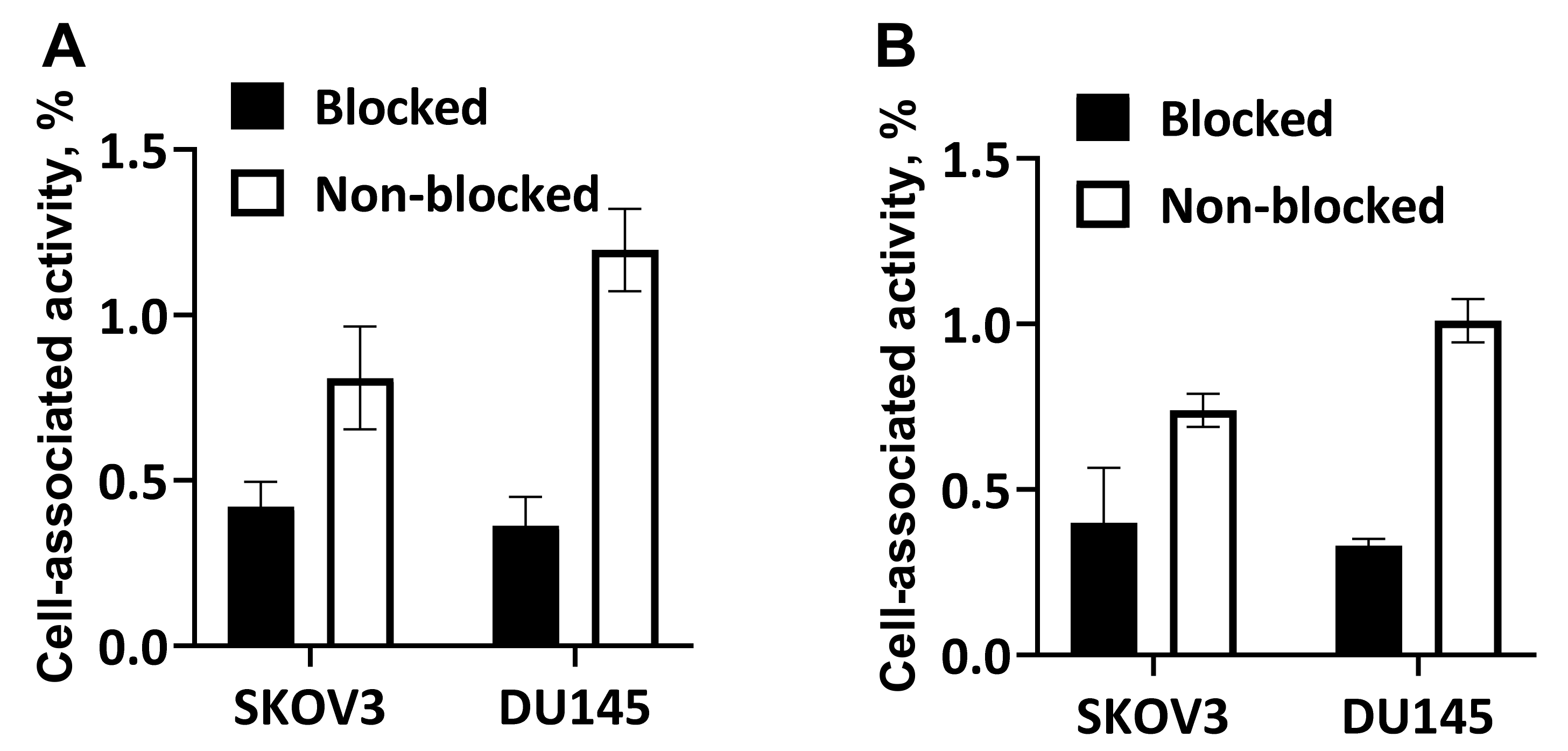
3.3. In Vitro Studies
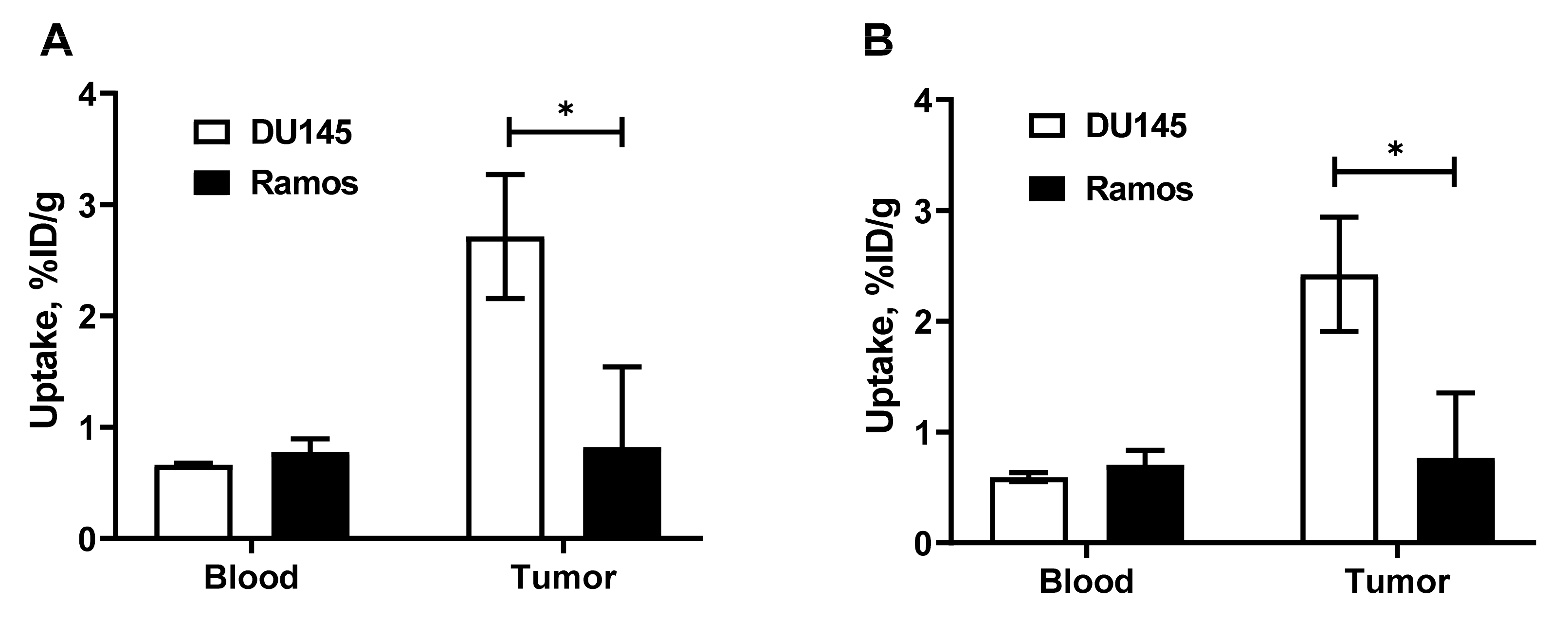
3.4. In Vivo Evaluation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Werner, H.; Bruchim, I. The insulin-like growth factor-I receptor as an oncogene. Arch. Physiol. Biochem. 2009, 115, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Baserga, R. The insulin receptor substrate-1: A biomarker for cancer? Exp. Cell Res. 2009, 315, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Nahta, R.; Yuan, L.X.; Zhang, B.; Kobayashi, R.; Esteva, F.J. Insulin-like growth factor-I receptor/human epidermal growth factor receptor 2 heterodimerization contributes to trastuzumab resistance of breast cancer cells. Cancer Res. 2005, 65, 11118–11128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, H.E.; Gee, J.M.; Hutcheson, I.R.; Nicholson, R.I. Insulin-like growth factor-I receptor signaling and resistance in breast cancer. Expert Rev. Endocrinol. Metab. 2006, 1, 33–46. [Google Scholar] [CrossRef]
- Pienta, K.J.; Bradley, D. Mechanisms underlying the development of androgen-independent prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2006, 12, 1665–1671. [Google Scholar] [CrossRef] [Green Version]
- Ozkan, E.E. Plasma and tissue insulin-like growth factor-I receptor (IGF-IR) as a prognostic marker for prostate cancer and anti-IGF-IR agents as novel therapeutic strategy for refractory cases: A review. Mol. Cell. Endocrinol. 2011, 344, 1–24. [Google Scholar] [CrossRef]
- Vaccaro, V.; Melisi, D.; Bria, E.; Cuppone, F.; Ciuffreda, L.; Pino, M.S.; Gelibter, A.; Tortora, G.; Cognetti, F.; Milella, M. Emerging pathways and future targets for the molecular therapy of pancreatic cancer. Expert Opin. Ther. Targets 2011, 15, 1183–1196. [Google Scholar] [CrossRef]
- Liefers-Visser, J.A.L.; Meijering, R.A.M.; Reyners, A.K.L.; van der Zee, A.G.J.; de Jong, S. IGF system targeted therapy: Therapeutic opportunities for ovarian cancer. Cancer Treat. Rev. 2017, 60, 90–99. [Google Scholar] [CrossRef] [Green Version]
- Iams, W.T.; Lovly, C.M. Molecular Pathways: Clinical Applications and Future Direction of Insulin-like Growth Factor-1 Receptor Pathway Blockade. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2015, 21, 4270–4277. [Google Scholar] [CrossRef] [Green Version]
- Ray-Coquard, I.; Haluska, P.; O’Reilly, S.; Cottu, P.H.; Elit, L.; Provencher, D.M.; Beckmann, M.W.; Bosserman, L.D.; Jacod, S.; Houe, V.; et al. A multicenter open-label phase II study of the efficacy and safety of ganitumab (AMG 479), a fully human monoclonal antibody against insulin-like growth factor type 1 receptor (IGF-1R) as second-line therapy in patients with recurrent platinum-sensitive ovarian cancer. J. Clin. Oncol. 2013, 31, 5515. [Google Scholar]
- Konecny, G.E.; Hendrickson, A.; Davidson, T.M.; Winterhoff, B.J.; Ma, S.; Mahner, S.; Sehouli, J.; Fasching, P.A.; Feisel-Schwickardi, G.; Poelcher, M.; et al. Results of TRIO-14, a phase II, multicenter, randomized, placebo-controlled trial of carboplatin-paclitaxel versus carboplatin-paclitaxel-ganitumab in newly diagnosed epithelial ovarian cancer. Gynecol. Oncol. 2021, 163, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Eng, C.; Nowara, E.; Swieboda-Sadlej, A.; Tebbutt, N.C.; Mitchell, E.; Davidenko, I.; Stephenson, J.; Elez, E.; Prenen, H.; et al. Randomized phase Ib/II trial of rilotumumab or ganitumab with panitumumab versus panitumumab alone in patients with wild-type KRAS metastatic colorectal cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 4240–4250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bono, J.S.; Piulats, J.M.; Pandha, H.S.; Petrylak, D.P.; Saad, F.; Aparicio, L.M.; Sandhu, S.K.; Fong, P.; Gillessen, S.; Hudes, G.R.; et al. Phase II randomized study of figitumumab plus docetaxel and docetaxel alone with crossover for metastatic castration-resistant prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 1925–1934. [Google Scholar] [CrossRef] [Green Version]
- Scagliotti, G.V.; Bondarenko, I.; Blackhall, F.; Barlesi, F.; Hsia, T.C.; Jassem, J.; Milanowski, J.; Popat, S.; Sanchez-Torres, J.M.; Novello, S.; et al. Randomized, phase III trial of figitumumab in combination with erlotinib versus erlotinib alone in patients with nonadenocarcinoma nonsmall-cell lung cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.A.; Goldman, B.; Ramanathan, R.K.; Lenz, H.J.; Lowy, A.M.; Whitehead, R.P.; Wakatsuki, T.; Iqbal, S.; Gaur, R.; Benedetti, J.K.; et al. Dual blockade of epidermal growth factor receptor and insulin-like growth factor receptor-1 signaling in metastatic pancreatic cancer: Phase Ib and randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG S0727). Cancer 2014, 120, 2980–2985. [Google Scholar] [PubMed] [Green Version]
- Hanna, N.H.; Dahlberg, S.E.; Kolesar, J.M.; Aggarwal, C.; Hirsch, F.R.; Ramalingam, S.S.; Schiller, J.H. Three-arm, randomized, phase 2 study of carboplatin and paclitaxel in combination with cetuximab, cixutumumab, or both for advanced non-small cell lung cancer (NSCLC) patients who will not receive bevacizumab-based therapy: An Eastern Cooperative Oncology Group (ECOG) study (E4508). Cancer 2015, 121, 2253–2261. [Google Scholar] [PubMed] [Green Version]
- Moran, T.; Felip, E.; Keedy, V.; Borghaei, H.; Shepherd, F.A.; Insa, A.; Brown, H.; Fitzgerald, T.; Sathyanarayanan, S.; Reilly, J.F.; et al. Activity of dalotuzumab, a selective anti-IGF1R antibody, in combination with erlotinib in unselected patients with Non-small-cell lung cancer: A phase I/II randomized trial. Exp. Hematol. Oncol. 2014, 3, 26. [Google Scholar] [CrossRef] [Green Version]
- Sclafani, F.; Kim, T.Y.; Cunningham, D.; Kim, T.W.; Tabernero, J.; Schmoll, H.J.; Roh, J.K.; Kim, S.Y.; Park, Y.S.; Guren, T.K.; et al. A Randomized Phase II/III Study of Dalotuzumab in Combination with Cetuximab and Irinotecan in Chemorefractory, KRAS Wild-Type, Metastatic Colorectal Cancer. J. Natl. Cancer Inst. 2015, 107, djv258. [Google Scholar] [CrossRef] [Green Version]
- Kindler, H.L.; Richards, D.A.; Garbo, L.E.; Garon, E.B.; Stephenson, J.J., Jr.; Rocha-Lima, C.M.; Safran, H.; Chan, D.; Kocs, D.M.; Galimi, F.; et al. A randomized, placebo-controlled phase 2 study of ganitumab (AMG 479) or conatumumab (AMG 655) in combination with gemcitabine in patients with metastatic pancreatic cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 2834–2842. [Google Scholar] [CrossRef]
- Chi, K.N.; Gleave, M.E.; Fazli, L.; Goldenberg, S.L.; So, A.; Kollmannsberger, C.; Murray, N.; Tinker, A.; Pollak, M. A phase II pharmacodynamic study of preoperative figitumumab in patients with localized prostate cancer. Clin. Cancer Res. 2012, 18, 3407–3413. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Spigel, D.R.; Chen, D.; Steins, M.B.; Engelman, J.A.; Schneider, C.P.; Novello, S.; Eberhardt, W.E.E.; Crino, L.; Habben, K.; et al. Randomized phase II study of erlotinib in combination with placebo or R1507, a monoclonal antibody to insulin-like growth factor-1 receptor, for advanced-stage nonsmall- cell lung cancer. J. Clin. Oncol. 2011, 29, 4574–4580. [Google Scholar] [CrossRef] [Green Version]
- Pappo, A.S.; Patel, S.R.; Crowley, J.; Reinke, D.K.; Kuenkele, K.P.; Chawla, S.P.; Toner, G.C.; Maki, R.G.; Meyers, P.A.; Chugh, R.; et al. R1507, a monoclonal antibody to the insulin-like growth factor 1 receptor, in patients with recurrent or refractory Ewing sarcoma family of tumors: Results of a phase II Sarcoma Alliance for Research through Collaboration study. J. Clin. Oncol. 2011, 29, 4541–4547. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Yu, Y.; Darko, I.; Currier, D.; Mayeenuddin, L.H.; Wan, X.; Khanna, C.; Helman, L.J. Addiction to elevated insulin-like growth factor I receptor and initial modulation of the AKT pathway define the responsiveness of rhabdomyosarcoma to the targeting antibody. Cancer Res. 2008, 68, 8039–8048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zha, J.; O’Brien, C.; Savage, H.; Huw, L.Y.; Zhong, F.; Berry, L.; Lewis Phillips, G.D.; Luis, E.; Cavet, G.; Hu, X.; et al. Molecular predictors of response to a humanized anti-insulin-like growth factor-I receptor monoclonal antibody in breast and colorectal cancer. Mol. Cancer Ther. 2009, 8, 2110–2121. [Google Scholar] [CrossRef] [Green Version]
- Gualberto, A.; Melvin, C.L.; Dean, A.; Ang, A.L.; Reynolds, J.M.; Lee, A.V.; Terstappen, W.; Haluska, P.; Lipton, A.; Karp, D.D. Characterization of NSCLC patients responding to anti-IGFIR therapy. J. Clin. Oncol. 2008, 26, 8000. [Google Scholar] [CrossRef]
- Jadvar, H.; Chen, X.; Cai, W.; Mahmood, U. Radiotheranostics in Cancer Diagnosis and Management. Radiology 2018, 286, 388–400. [Google Scholar] [CrossRef]
- Moek, K.L.; Giesen, D.; Kok, I.C.; de Groot, D.; Jalving, M.; Fehrmann, R.; Lub-de Hooge, M.N.; Brouwers, A.H.; de Vries, E. Theranostics Using Antibodies and Antibody-Related Therapeutics. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2017, 58 (Suppl. 2), 83S–90S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Sun, X.; Shen, B. Molecular Imaging of IGF-1R in Cancer. Mol. Imaging 2017, 16, 1536012117736648. [Google Scholar] [CrossRef] [Green Version]
- Majo, V.J.; Arango, V.; Simpson, N.R.; Prabhakaran, J.; Kassir, S.A.; Underwood, M.D.; Bakalian, M.; Canoll, P.; John Mann, J.; Dileep Kumar, J.S. Synthesis and in vitro evaluation of [18F]BMS-754807: A potential PET ligand for IGF-1R. Bioorganic Med. Chem. Lett. 2013, 23, 4191–4194. [Google Scholar] [CrossRef] [Green Version]
- Prabhakaran, J.; Dewey, S.L.; McClure, R.; Simpson, N.R.; Tantawy, M.N.; Mann, J.J.; Pham, W.; Kumar, J. In vivo evaluation of IGF1R/IR PET ligand [18F]BMS-754807 in rodents. Bioorganic Med. Chem. Lett. 2017, 27, 941–943. [Google Scholar] [CrossRef] [Green Version]
- Fleuren, E.D.; Versleijen-Jonkers, Y.M.; van de Luijtgaarden, A.C.; Molkenboer-Kuenen, J.D.; Heskamp, S.; Roeffen, M.H.; van Laarhoven, H.W.; Houghton, P.J.; Oyen, W.J.; Boerman, O.C.; et al. Predicting IGF-1R therapy response in bone sarcomas: Immuno-SPECT imaging with radiolabeled R1507. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 7693–7703. [Google Scholar] [CrossRef] [Green Version]
- Heskamp, S.; van Laarhoven, H.W.; Molkenboer-Kuenen, J.D.; Bouwman, W.H.; van der Graaf, W.T.; Oyen, W.J.; Boerman, O.C. Optimization of IGF-1R SPECT/CT imaging using 111In-labeled F(ab’)2 and Fab fragments of the monoclonal antibody R1507. Mol. Pharm. 2012, 9, 2314–2321. [Google Scholar] [CrossRef] [PubMed]
- England, C.G.; Kamkaew, A.; Im, H.J.; Valdovinos, H.F.; Sun, H.; Hernandez, R.; Cho, S.Y.; Dunphy, E.J.; Lee, D.S.; Barnhart, T.E.; et al. ImmunoPET Imaging of Insulin-Like Growth Factor 1 Receptor in a Subcutaneous Mouse Model of Pancreatic Cancer. Mol. Pharm. 2016, 13, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Roopenian, D.C.; Akilesh, S. FcRn: The neonatal Fc receptor comes of age. Nat. Rev. Immunol. 2007, 7, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Garousi, J.; Orlova, A.; Frejd, F.Y.; Tolmachev, V. Imaging using radiolabelled targeted proteins: Radioimmunodetection and beyond. EJNMMI Radiopharm. Chem. 2020, 5, 16. [Google Scholar] [CrossRef]
- Fleuren, E.D.; Versleijen-Jonkers, Y.M.; Heskamp, S.; Roeffen, M.H.; Bouwman, W.H.; Molkenboer-Kuenen, J.D.; van Laarhoven, H.W.; Oyen, W.J.; Boerman, O.C.; van der Graaf, W.T. The strength of small: Improved targeting of insulin-like growth factor-1 receptor (IGF-1R) with F(ab’)₂-R1507 fragments in Ewing sarcomas. Eur. J. Cancer 2013, 49, 2851–2858. [Google Scholar] [CrossRef]
- Cornelissen, B.; McLarty, K.; Kersemans, V.; Reilly, R.M. The level of insulin growth factor-1 receptor expression is directly correlated with the tumor uptake of (111)In-IGF-1(E3R) in vivo and the clonogenic survival of breast cancer cells exposed in vitro to trastuzumab (Herceptin). Nucl. Med. Biol. 2008, 35, 645–653. [Google Scholar] [CrossRef]
- Tolmachev, V.; Orlova, A. Affibody Molecules as Targeting Vectors for PET Imaging. Cancers 2020, 12, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ståhl, S.; Gräslund, T.; Eriksson Karlström, A.; Frejd, F.Y.; Nygren, P.Å.; Löfblom, J. Affibody Molecules in Biotechnological and Medical Applications. Trends Biotechnol. 2017, 35, 691–712. [Google Scholar] [CrossRef] [PubMed]
- Tolmachev, V.; Malmberg, J.; Hofström, C.; Abrahmsén, L.; Bergman, T.; Sjöberg, A.; Sandström, M.; Gräslund, T.; Orlova, A. Imaging of insulinlike growth factor type 1 receptor in prostate cancer xenografts using the affibody molecule 111In-DOTA-ZIGF1R:4551. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2012, 53, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlova, A.; Hofström, C.; Strand, J.; Varasteh, Z.; Sandstrom, M.; Andersson, K.; Tolmachev, V.; Gräslund, T. [99mTc(CO)3]+-(HE)3-ZIGF1R:4551, a new Affibody conjugate for visualization of insulin-like growth factor-1 receptor expression in malignant tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 439–449. [Google Scholar] [CrossRef] [Green Version]
- Wållberg, H.; Orlova, A.; Altai, M.; Hosseinimehr, S.J.; Widström, C.; Malmberg, J.; Ståhl, S.; Tolmachev, V. Molecular design and optimization of 99mTc-labeled recombinant affibody molecules improves their biodistribution and imaging properties. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2011, 52, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Mitran, B.; Altai, M.; Hofström, C.; Honarvar, H.; Sandström, M.; Orlova, A.; Tolmachev, V.; Gräslund, T. Evaluation of 99mTc-Z IGF1R:4551-GGGC affibody molecule, a new probe for imaging of insulin-like growth factor type 1 receptor expression. Amino Acids 2015, 47, 303–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, X.; Cheng, K.; Liu, Y.; Hu, X.; Meng, S.; Cheng, Z. PET imaging of insulin-like growth factor type 1 receptor expression with a 64Cu-labeled Affibody molecule. Amino Acids 2015, 47, 1409–1419. [Google Scholar] [CrossRef] [PubMed]
- Prasanphanich, A.F.; Nanda, P.K.; Rold, T.L.; Ma, L.; Lewis, M.R.; Garrison, J.C.; Hoffman, T.J.; Sieckman, G.L.; Figueroa, S.D.; Smith, C.J. [64Cu-NOTA-8-Aoc-BBN(7-14)NH2] targeting vector for positron-emission tomography imaging of gastrin-releasing peptide receptor-expressing tissues. Proc. Natl. Acad. Sci. USA 2007, 104, 12462–12467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolmachev, V.; Yim, C.B.; Rajander, J.; Perols, A.; Karlström, A.E.; Haaparanta-Solin, M.; Grönroos, T.J.; Solin, O.; Orlova, A. Comparative Evaluation of Anti-HER2 Affibody Molecules Labeled with 64Cu Using NOTA and NODAGA. Contrast Media Mol. Imaging 2017, 2017, 8565802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofstrom, C.; Orlova, A.; Altai, M.; Wangsell, F.; Graslund, T.; Tolmachev, V. Use of a HEHEHE purification tag instead of a hexahistidine tag improves biodistribution of affibody molecules site-specifically labeled with (99m)Tc, (111)In, and (125)I. J. Med. Chem. 2011, 54, 3817–3826. [Google Scholar] [CrossRef] [PubMed]
- Spang, P.; Herrmann, C.; Roesch, F. Bifunctional Gallium-68 Chelators: Past, Present, and Future. Semin. Nucl. Med. 2016, 46, 373–394. [Google Scholar] [CrossRef] [Green Version]
- Eisenwiener, K.P.; Prata, M.I.; Buschmann, I.; Zhang, H.W.; Santos, A.C.; Wenger, S.; Reubi, J.C.; Mäcke, H.R. NODAGATOC, a new chelator-coupled somatostatin analogue labeled with [67/68Ga] and [111In] for SPECT, PET, and targeted therapeutic applications of somatostatin receptor (hsst2) expressing tumors. Bioconjug. Chem. 2002, 13, 530–541. [Google Scholar] [CrossRef]
- Xu, T.; Ding, H.; Vorobyeva, A.; Oroujeni, M.; Orlova, A.; Tolmachev, V.; Gräslund, T. Drug Conjugates Based on a Monovalent Affibody Targeting Vector Can Efficiently Eradicate HER2 Positive Human Tumors in an Experimental Mouse Model. Cancers 2020, 13, 85. [Google Scholar] [CrossRef]
- Wållberg, H.; Orlova, A. Slow internalization of anti-HER2 synthetic affibody monomer 111In-DOTA-ZHER2:342-pep2: Implications for development of labeled tracers. Cancer Biother. Radiopharm. 2008, 23, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Honarvar, H.; Jokilaakso, N.; Andersson, K.; Malmberg, J.; Rosik, D.; Orlova, A.; Karlström, A.E.; Tolmachev, V.; Järver, P. Evaluation of backbone-cyclized HER2-binding 2-helix affibody molecule for in vivo molecular imaging. Nucl. Med. Biol. 2013, 40, 378–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.M.; Wittrup, K.D. A modeling analysis of the effects of molecular size and binding affinity on tumor targeting. Mol. Cancer Ther. 2009, 8, 2861–2871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlsson Leitao, C.; Rinne, S.S.; Mitran, B.; Vorobyeva, A.; Andersson, K.G.; Tolmachev, V.; Ståhl, S.; Löfblom, J.; Orlova, A. Molecular Design of HER3-Targeting Affibody Molecules: Influence of Chelator and Presence of HEHEHE-Tag on Biodistribution of 68Ga-Labeled Tracers. Int. J. Mol. Sci. 2019, 20, 1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolmachev, V.; Tran, T.A.; Rosik, D.; Sjöberg, A.; Abrahmsén, L.; Orlova, A. Tumor targeting using affibody molecules: Interplay of affinity, target expression level, and binding site composition. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2012, 53, 953–960. [Google Scholar] [CrossRef] [Green Version]
- Andersson, K.G.; Rosestedt, M.; Varasteh, Z.; Malm, M.; Sandström, M.; Tolmachev, V.; Löfblom, J.; Ståhl, S.; Orlova, A. Comparative evaluation of 111In-labeled NOTA-conjugated affibody molecules for visualization of HER3 expression in malignant tumors. Oncol. Rep. 2015, 34, 1042–1048. [Google Scholar] [CrossRef] [Green Version]
- Garousi, J.; Honarvar, H.; Andersson, K.G.; Mitran, B.; Orlova, A.; Buijs, J.; Löfblom, J.; Frejd, F.Y.; Tolmachev, V. Comparative Evaluation of Affibody Molecules for Radionuclide Imaging of in Vivo Expression of Carbonic Anhydrase IX. Mol. Pharm. 2016, 13, 3676–3687. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protein-Associated Activity | ||
|---|---|---|
| [68Ga]Ga-NODAGA-(HE)3-ZIGF-1R:4551 | [111In]In-NODAGA-(HE)3-ZIGF-1R:4551 | |
| 1000-fold molar excess EDTA | 98.4 ± 0.2% | 98.2 ± 0.5% |
| Control | 98.3 ± 0.2% | 99.4 ± 0.2% |
| [68Ga]Ga-NODAGA-(HE)3-ZIGF-1R:4551 | [111In]In-NODAGA-(HE)3-ZIGF-1R:4551 | ||||
|---|---|---|---|---|---|
| 1 h | 3 h | 1 h | 3 h | 24 h | |
| Blood | 0.6 ± 0.04 | 0.31 ± 0.01 b | 0.66 ± 0.02 | 0.36 ± 0.02 b | 0.077 ± 0.004 |
| Salivary gland | 2.99 ± 0.03 a | 2.3 ± 0.4 | 3.7 ± 0.2 a | 3 ± 0.3 | 1.47 ± 0.04 |
| Lung | 3.9 ± 0.1 a | 3.2 ± 0.2 | 4.19 ± 0.02 a | 3.8 ± 0.2 | 1.8 ± 0.2 |
| Liver | 3.2 ± 0.1 a | 2.7 ± 0.1 b | 3.7 ± 0.1 a | 3.4 ± 0.1 b | 2 ± 0.2 |
| Spleen | 1.8 ± 0.1 | 1.5 ± 0.2 | 2.1 ± 0.1 | 2 ± 0.2 | 1.3 ± 0.2 |
| Pancreas | 2.3 ± 0.1 a | 1.7 ± 0.4 | 2.65 ± 0.04 a | 2.1 ± 0.5 | 1.5 ± 0.1 |
| Stomach | 2.6 ± 0.1 | 2.1 ± 0.1 b | 3.2 ± 0.2 | 2.6 ± 0.1 b | 1.4 ± 0.2 |
| Colon | 2.94 ± 0.03 a | 2.4 ± 0.2 b | 3.4 ± 0.1 a | 3.2 ± 0.2 b | 1.5 ± 0.2 |
| Kidney | 250 ± 11 | 275 ± 25 | 231 ± 7 | 258 ± 26 | 246 ± 23 |
| Tumor | 2.4 ± 0.5 | 2.4 ± 0.1 b | 2.7 ± 0.6 | 2.8 ± 0.2 b | 1.9 ± 0.1 |
| Muscle | 0.45 ± 0.03 | 0.31 ± 0.04 | 0.54 ± 0.02 | 0.4 ± 0.1 | 0.2 ± 0.03 |
| Bone | 0.8 ± 0.1 | 0.7 ± 0.1 | 1 ± 0.1 | 0.9 ± 0.2 | 0.5 ± 0.1 |
| GI * | 3 ± 0.1 a | 2.6 ± 0.2 b | 3.5 ± 0.1 a | 3.2 ± 0.2 b | 1.7 ± 0.2 |
| Carcass * | 13.2 ± 0.2 a | 9.6 ± 0.7 b | 15.9 ± 0.4 a | 13.3 ± 1.5 b | 6.2 ± 0.6 |
| [68Ga]Ga-NODAGA-(HE)3-ZIGF-1R:4551 | [111In]In-NODAGA-(HE)3-ZIGF-1R:4551 | ||||
|---|---|---|---|---|---|
| 1 h | 3 h | 1 h | 3 h | 24 h | |
| Blood | 4 ± 0.7 | 7.8 ± 0.2 | 4.1 ± 0.8 | 8 ± 0.6 | 25.1 ± 1.3 |
| Salivary gland | 0.8 ± 0.2 | 1.1 ± 0.1 | 0.7 ± 0.2 | 1 ± 0.1 | 1.3 ± 0.1 |
| Lung | 0.6 ± 0.1 | 0.8 ± 0.1 | 0.6 ± 0.1 | 0.74 ± 0.03 | 1.1 ± 0.1 |
| Liver | 0.8 ± 0.1 | 0.91 ± 0.02 | 0.7 ± 0.1 | 0.84 ± 0.04 | 1 ± 0.1 |
| Spleen | 1.4 ± 0.3 | 1.6 ± 0.1 | 1.3 ± 0.3 | 1.5 ± 0.2 | 1.6 ± 0.2 |
| Pancreas | 1.1 ± 0.2 | 1.5 ± 0.4 | 1 ± 0.2 | 1.4 ± 0.4 | 1.3 ± 0.1 |
| Stomach | 0.9 ± 0.2 | 1.14 ± 0.03 | 0.9 ± 0.1 | 1.1 ± 0.1 | 1.4 ± 0.1 |
| Colon | 0.8 ± 0.2 | 1 ± 0.1 | 0.8 ± 0.2 | 0.9 ± 0.1 | 1.3 ± 0.1 |
| Kidney | 0.010 ± 0.002 | 0.009 ± 0.001 | 0.012 ± 0.002 | 0.011 ± 0.002 | 0.008 ± 0.001 |
| Muscle | 5.3 ± 0.9 | 8 ± 1 | 5 ± 1 | 7.6 ± 1.1 | 10 ± 1.6 |
| Bone | 3 ± 0.9 | 3.5 ± 0.6 | 2.7 ± 0.8 | 3.2 ± 0.7 | 4 ± 0.7 |
| Tumor-to-Blood Ratio | ||||||
|---|---|---|---|---|---|---|
| [111In]In-DOTA-H6-ZIGF-1R:4551 [40] | [99mTc]Tc (CO)3-(HE)3-ZIGF-1R:4551 [41] | [99mTc]Tc-ZIGF-1R:4551-GGGC [43] | [64Cu]Cu-NOTA-ZIGF-1R:4:40 * [44] | [68Ga]Ga-NODAGA-(HE)3-ZIGF-1R:4551 (This Study) | [111In]In-NODAGA-(HE)3-ZIGF-1R:4551 (This Study) | |
| 1 | 1.3 ± 0.2 | 3.1 ± 0.3 | 4.1 ± 0.7 | 4.1 ± 0.8 | ||
| 3 | 7.8 ± 0.2 | 8.0 ± 0.6 | ||||
| 4 | 2.5 ± 0.2 | 3.5 ± 0.7 | 6.2 ± 0.9 | |||
| 8 | 3.3 ± 0.2 | 4.4 ± 0.3 | 7.6 ± 2.3 | |||
| 24 | 5.1 ± 0.3 | 5.4 ± 0.4 | 4.1 ± 0.6 | 25.1 ± 1.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Yu, S.; Xu, T.; Bodenko, V.; Orlova, A.; Oroujeni, M.; Rinne, S.S.; Tolmachev, V.; Vorobyeva, A.; Gräslund, T. Preclinical Evaluation of a New Format of 68Ga- and 111In-Labeled Affibody Molecule ZIGF-1R:4551 for the Visualization of IGF-1R Expression in Malignant Tumors Using PET and SPECT. Pharmaceutics 2022, 14, 1475. https://doi.org/10.3390/pharmaceutics14071475
Liu Y, Yu S, Xu T, Bodenko V, Orlova A, Oroujeni M, Rinne SS, Tolmachev V, Vorobyeva A, Gräslund T. Preclinical Evaluation of a New Format of 68Ga- and 111In-Labeled Affibody Molecule ZIGF-1R:4551 for the Visualization of IGF-1R Expression in Malignant Tumors Using PET and SPECT. Pharmaceutics. 2022; 14(7):1475. https://doi.org/10.3390/pharmaceutics14071475
Chicago/Turabian StyleLiu, Yongsheng, Shengze Yu, Tianqi Xu, Vitalina Bodenko, Anna Orlova, Maryam Oroujeni, Sara S. Rinne, Vladimir Tolmachev, Anzhelika Vorobyeva, and Torbjörn Gräslund. 2022. "Preclinical Evaluation of a New Format of 68Ga- and 111In-Labeled Affibody Molecule ZIGF-1R:4551 for the Visualization of IGF-1R Expression in Malignant Tumors Using PET and SPECT" Pharmaceutics 14, no. 7: 1475. https://doi.org/10.3390/pharmaceutics14071475