
Pharmacogenetic Analysis of Voriconazole Treatment in Children

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and TDM
2.2. Genotyping
2.3. Data Analysis by Linear Mixed Effects Modelling
3. Results
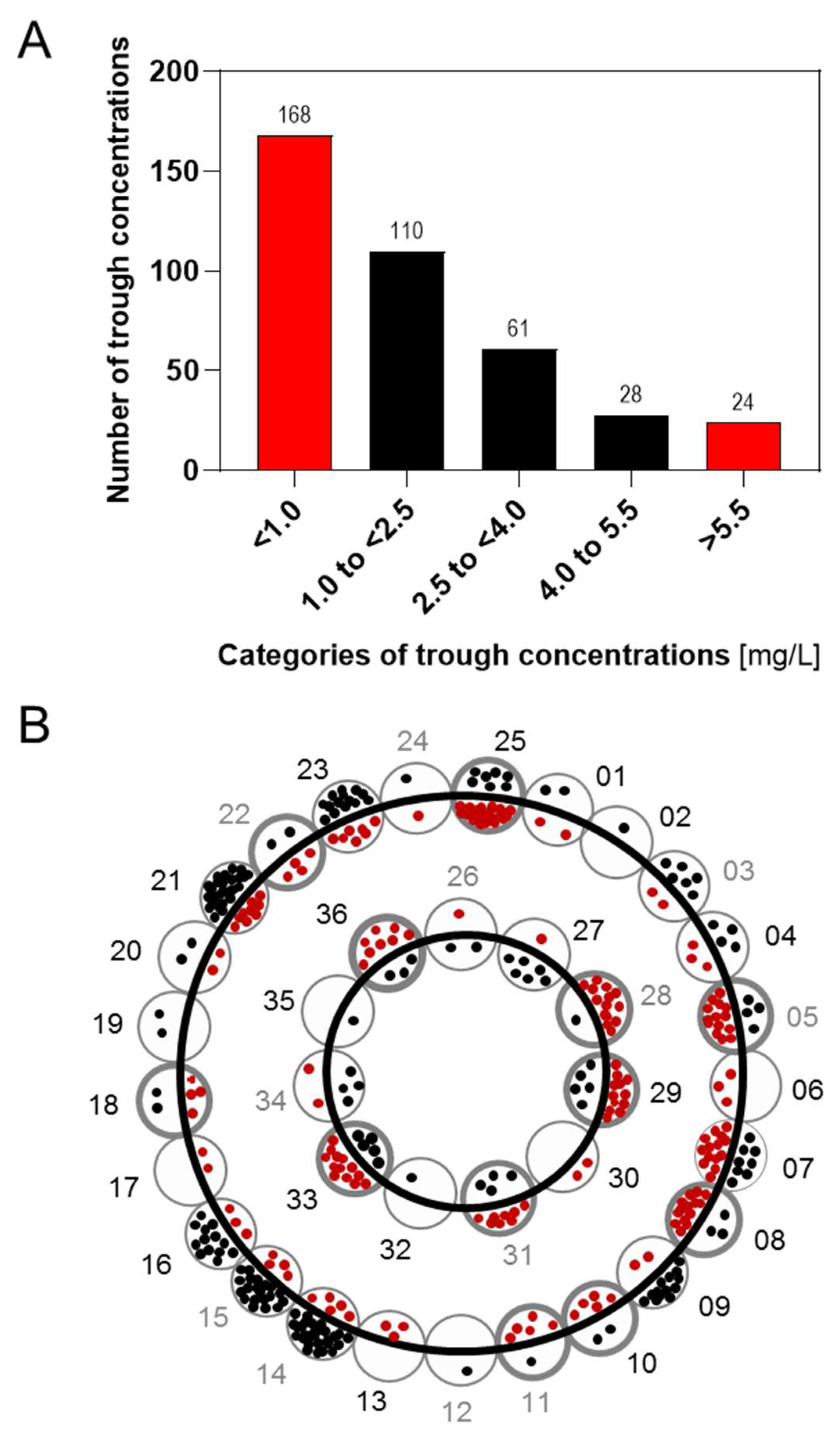
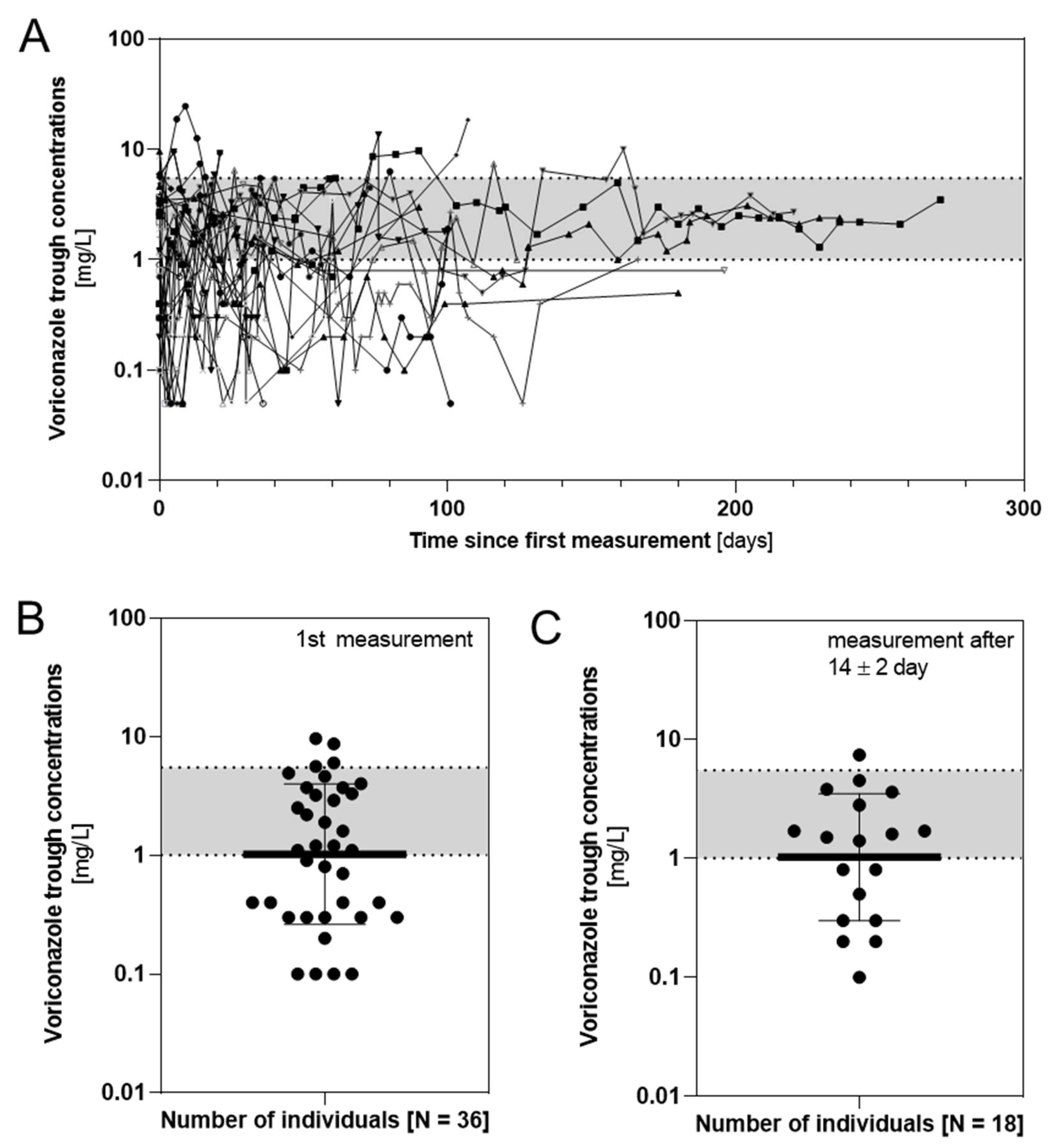
3.1. Population Description and TDM
- 2 to 12 years or 12 to 14 years and <50 kg: 8 mg/kg (7.5 ± 1.6 mg/kg) q12h;
- 12 to 14 years and ≥50 kg or ≥15 years: 4 mg/kg (3.6 ± 1.1 mg/kg) q12h.
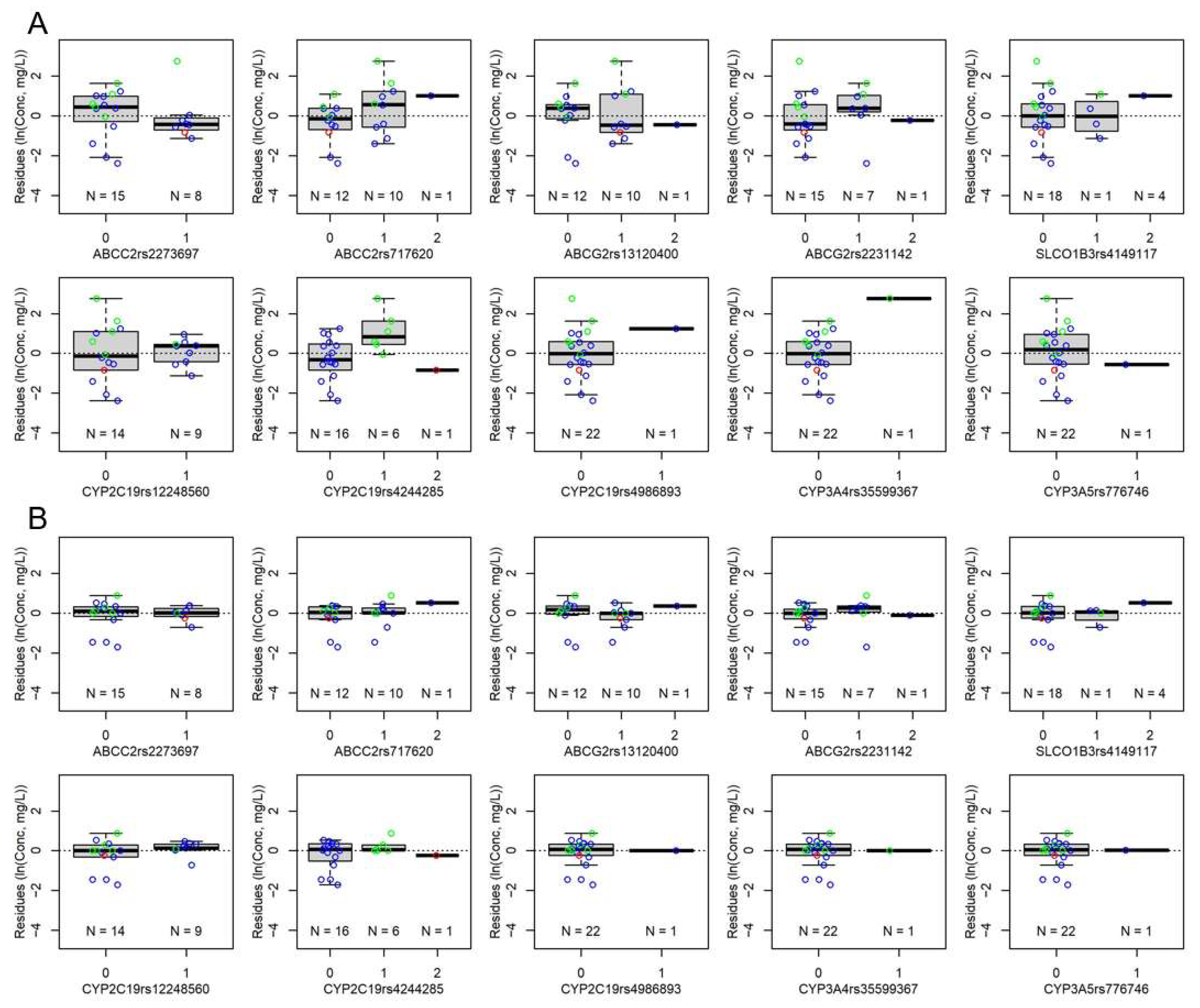
3.2. Genetic Analysis
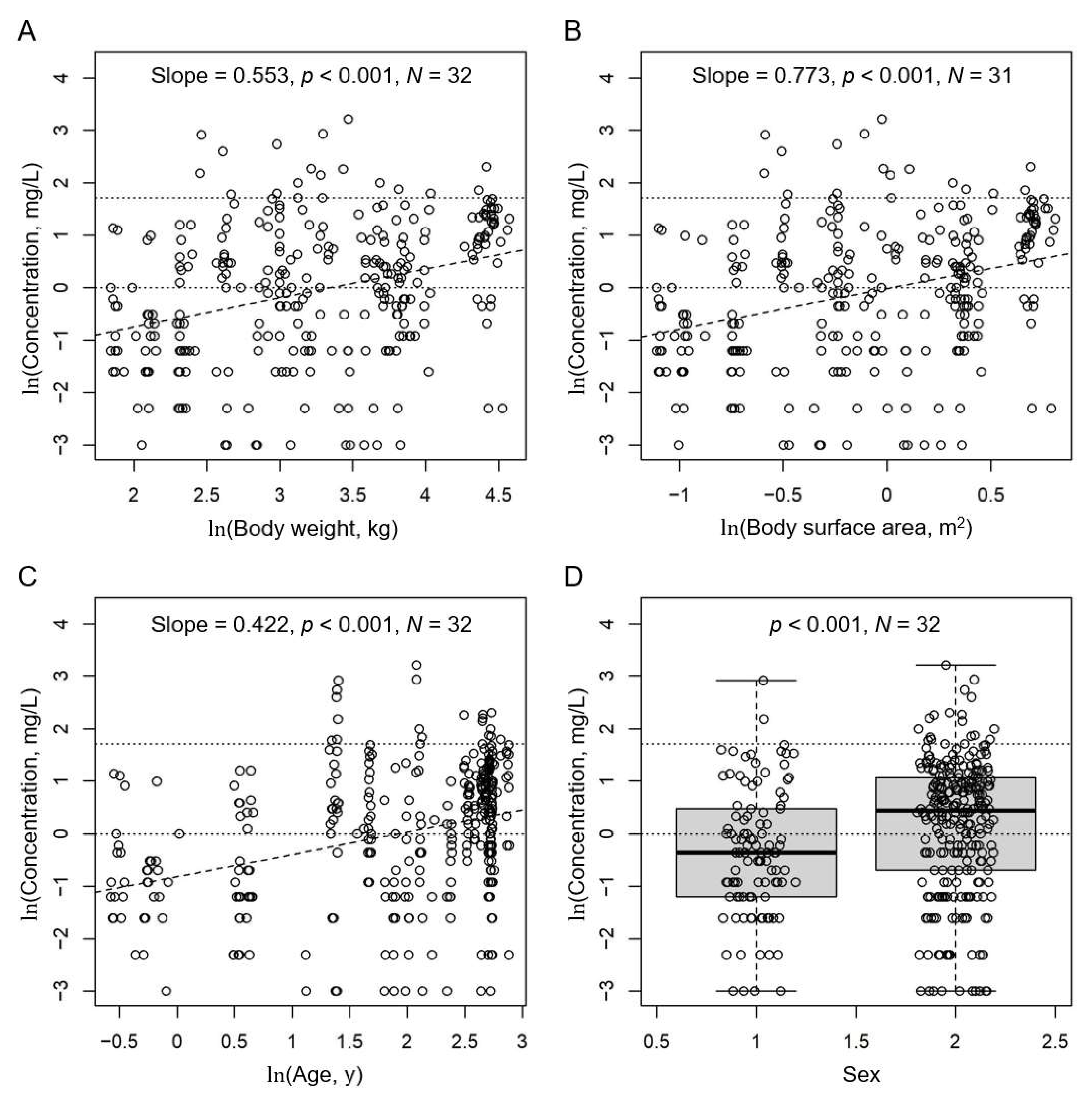
3.3. Covariate Analysis
3.4. Final Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lehrnbecher, T.; Groll, A.H. Invasive fungal infections in the pediatric population. Expert Rev. Anti-Infect. Ther. 2011, 9, 275–278. [Google Scholar] [CrossRef] [Green Version]
- Warris, A.; Lehrnbecher, T.; Roilides, E.; Castagnola, E.; Bruggemann, R.J.M.; Groll, A.H. Escmid-ecmm guideline: Diagnosis and management of invasive aspergillosis in neonates and children. Clin. Microbiol. Infect. 2019, 25, 1096–1113. [Google Scholar] [CrossRef] [Green Version]
- Pfizer. Vfend® Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/vfend-epar-product-information_en.pdf (accessed on 7 January 2020).
- Shima, H.; Miharu, M.; Osumi, T.; Takahashi, T.; Shimada, H. Differences in voriconazole trough plasma concentrations per oral dosages between children younger and older than 3 years of age. Pediatr. Blood Cancer 2010, 54, 1050–1052. [Google Scholar] [CrossRef]
- Kadam, R.S.; Van Den Anker, J.N. Pediatric clinical pharmacology of voriconazole: Role of pharmacokinetic/pharmacodynamic modeling in pharmacotherapy. Clin. Pharmacokinet. 2016, 55, 1031–1043. [Google Scholar] [CrossRef]
- Herbrecht, R. Voriconazole: Therapeutic review of a new azole antifungal. Expert Rev. Anti-Infect. Ther. 2004, 2, 485–497. [Google Scholar] [CrossRef]
- Theuretzbacher, U.; Ihle, F.; Derendorf, H. Pharmacokinetic/pharmacodynamic profile of voriconazole. Clin. Pharmacokinet. 2006, 45, 649–663. [Google Scholar] [CrossRef]
- Steinbach, W.J. Invasive aspergillosis in pediatric patients. Curr. Med. Res. Opin. 2010, 26, 1779–1787. [Google Scholar] [CrossRef]
- Pascual, A.; Calandra, T.; Bolay, S.; Buclin, T.; Bille, J.; Marchetti, O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin. Infect. Dis. 2008, 46, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Karthaus, M.; Lehrnbecher, T.; Lipp, H.P.; Kluge, S.; Buchheidt, D. Therapeutic drug monitoring in the treatment of invasive aspergillosis with voriconazole in cancer patients—An evidence-based approach. Ann. Hematol. 2015, 94, 547–556. [Google Scholar] [CrossRef]
- Park, W.B.; Kim, N.H.; Kim, K.H.; Lee, S.H.; Nam, W.S.; Yoon, S.H.; Song, K.H.; Choe, P.G.; Kim, N.J.; Jang, I.J.; et al. The effect of therapeutic drug monitoring on safety and efficacy of voriconazole in invasive fungal infections: A randomized controlled trial. Clin. Infect. Dis. 2012, 55, 1080–1087. [Google Scholar] [CrossRef] [Green Version]
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic drug monitoring (tdm) of antifungal agents: Guidelines from the british society for medical mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neely, M.; Rushing, T.; Kovacs, A.; Jelliffe, R.; Hoffman, J. Voriconazole pharmacokinetics and pharmacodynamics in children. Clin. Infect. Dis. 2010, 50, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanai, Y.; Hamada, Y.; Kimura, T.; Matsumoto, K.; Takahashi, Y.; Fujii, S.; Nishizawa, K.; Takesue, Y. Optimal trough concentration of voriconazole with therapeutic drug monitoring in children: A systematic review and meta-analysis. J. Infect. Chemother. 2021, 27, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Luong, M.L.; Al-Dabbagh, M.; Groll, A.H.; Racil, Z.; Nannya, Y.; Mitsani, D.; Husain, S. Utility of voriconazole therapeutic drug monitoring: A meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1786–1799. [Google Scholar] [CrossRef]
- Soler-Palacin, P.; Frick, M.A.; Martin-Nalda, A.; Lanaspa, M.; Pou, L.; Rosello, E.; de Heredia, C.D.; Figueras, C. Voriconazole drug monitoring in the management of invasive fungal infection in immunocompromised children: A prospective study. J. Antimicrob. Chemother. 2012, 67, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Silva, F.; Navea, D.; Saias, C.; Torres, J.P.; Catalán, P.; Morales, J. [Analysis of voriconazole serum concentrations and safety profile in pediatric oncology patients]. Rev. Chil. Infectol. 2016, 33, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Troke, P.F.; Hockey, H.P.; Hope, W.W. Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients. Antimicrob. Agents Chemother. 2011, 55, 4782–4788. [Google Scholar] [CrossRef] [Green Version]
- Groll, A.H.; Castagnola, E.; Cesaro, S.; Dalle, J.H.; Engelhard, D.; Hope, W.; Roilides, E.; Styczynski, J.; Warris, A.; Lehrnbecher, T. Fourth european conference on infections in leukaemia (ecil-4): Guidelines for diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or allogeneic haemopoietic stem-cell transplantation. Lancet Oncol. 2014, 15, e327–e340. [Google Scholar] [CrossRef]
- Tucker, L.; Higgins, T.; Egelund, E.F.; Zou, B.; Vijayan, V.; Peloquin, C.A. Voriconazole monitoring in children with invasive fungal infections. J. Pediatr. Pharmacol. Ther. 2015, 20, 17–23. [Google Scholar] [CrossRef]
- Boast, A.; Curtis, N.; Cranswick, N.; Gwee, A. Voriconazole dosing and therapeutic drug monitoring in children: Experience from a paediatric tertiary care centre. J. Antimicrob. Chemother. 2016, 71, 2031–2036. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, M.O.; Lutsar, I.; Milligan, P.A. Population pharmacokinetic analysis of voriconazole plasma concentration data from pediatric studies. Antimicrob. Agents Chemother. 2009, 53, 935–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, T.J.; Driscoll, T.; Milligan, P.A.; Wood, N.D.; Schlamm, H.; Groll, A.H.; Jafri, H.; Arrieta, A.C.; Klein, N.J.; Lutsar, I. Pharmacokinetics, safety, and tolerability of voriconazole in immunocompromised children. Antimicrob. Agents Chemother. 2010, 54, 4116–4123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, C.; Bierbach, U.; Frenzel, K.; Lange, T.; Basara, N.; Niederwieser, D.; Mauz-Korholz, C.; Preiss, R. Voriconazole pharmacokinetics and safety in immunocompromised children compared to adult patients. Antimicrob. Agents Chemother. 2010, 54, 3225–3232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelink, I.H.; Wolfs, T.; Jonker, M.; de Waal, M.; Egberts, T.C.; Ververs, T.T.; Boelens, J.J.; Bierings, M. Highly variable plasma concentrations of voriconazole in pediatric hematopoietic stem cell transplantation patients. Antimicrob. Agents Chemother. 2013, 57, 235–240. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Zhou, X.; Wu, T.; Jiang, H.; Yang, S.; Zhang, Y. Dose optimisation of voriconazole with therapeutic drug monitoring in children: A single-centre experience in China. Int. J. Antimicrob. Agents 2017, 49, 483–487. [Google Scholar] [CrossRef]
- Narita, A.; Muramatsu, H.; Sakaguchi, H.; Doisaki, S.; Tanaka, M.; Hama, A.; Shimada, A.; Takahashi, Y.; Yoshida, N.; Matsumoto, K.; et al. Correlation of cyp2c19 phenotype with voriconazole plasma concentration in children. J. Pediatr. Hematol. Oncol. 2013, 35, e219–e223. [Google Scholar] [CrossRef]
- Hicks, J.K.; Crews, K.R.; Flynn, P.; Haidar, C.E.; Daniels, C.C.; Yang, W.; Panetta, J.C.; Pei, D.; Scott, J.R.; Molinelli, A.R.; et al. Voriconazole plasma concentrations in immunocompromised pediatric patients vary by cyp2c19 diplotypes. Pharmacogenomics 2014, 15, 1065–1078. [Google Scholar] [CrossRef] [Green Version]
- Chuwongwattana, S.; Jantararoungtong, T.; Prommas, S.; Medhasi, S.; Puangpetch, A.; Sukasem, C. Impact of cyp2c19, cyp3a4, abcb1, and fmo3 genotypes on plasma voriconazole in Thai patients with invasive fungal infections. Pharmacol. Res. Perspect. 2020, 8, e00665. [Google Scholar] [CrossRef]
- Allegra, S.; Fatiguso, G.; Francia, S.; Pirro, E.; Carcieri, C.; Cusato, J.; Nicolo, A.; Avataneo, V.; Perri, G.D.; D’Avolio, A. Pharmacogenetic of voriconazole antifungal agent in pediatric patients. Pharmacogenomics 2018, 19, 913–925. [Google Scholar] [CrossRef]
- Goers, R.; Coman Schmid, D.; Jäggi, V.F.; Paioni, P.; Okoniewski, M.J.; Parker, A.; Bangerter, B.; Georgakopoulou, S.; Sengstag, T.; Bielicki, J.; et al. Swisspk(cdw)—A clinical data warehouse for the optimization of pediatric dosing regimens. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 1578–1587. [Google Scholar] [CrossRef]
- Moriyama, B.; Obeng, A.O.; Barbarino, J.; Penzak, S.R.; Henning, S.A.; Scott, S.A.; Agúndez, J.; Wingard, J.R.; McLeod, H.L.; Klein, T.E.; et al. Clinical pharmacogenetics implementation consortium (cpic) guidelines for cyp2c19 and voriconazole therapy. Clin. Pharmacol. Ther. 2017, 102, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coman Schmid, D.; Crameri, K.; Oesterle, S.; Rinn, B.; Sengstag, T.; Stockinger, H. Sphn—The biomedit network: A secure IT platform for research with sensitive human data. In Digital Personalized Health and Medicine, Proceedings of the 30th Medical Informatics Europe Conference (MIE 2020) (Cancelled), Geneva, Switzerland, 28 April–1 May 2020; Pape-Haugaard, L.B., Lovis, C., Cort Madsen, I., Weber, P., Hostrup Nielsen, P., Scott, P., Eds.; IOS Press: Amsterdam, The Netherlands, 2020; Volume 270, pp. 1170–1174. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Mosteller, R.D. Simplified calculation of body-surface area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [PubMed]
- National Center for Biotechnology Information. ALFA: Allele Frequency Aggregator. Available online: www.ncbi.nlm.nih.gov/snp/docs/gsr/alfa/ (accessed on 22 March 2021).
- He, H.R.; Sun, J.Y.; Ren, X.D.; Wang, T.T.; Zhai, Y.J.; Chen, S.Y.; Dong, Y.L.; Lu, J. Effects of cyp3a4 polymorphisms on the plasma concentration of voriconazole. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Moriyama, B.; Penzak, S.R.; Klein, T.E.; Caudle, K.E. Response to “pharmacogenetics of voriconazole: Cyp2c19 but also cyp3a4 need to be genotyped”—The role of cyp3a4 and cyp3a5 polymorphisms in clinical pharmacokinetics of voriconazole. Clin. Pharmacol. Ther. 2017, 102, 190. [Google Scholar] [CrossRef]
- Mori, M.; Kobayashi, R.; Kato, K.; Maeda, N.; Fukushima, K.; Goto, H.; Inoue, M.; Muto, C.; Okayama, A.; Watanabe, K.; et al. Pharmacokinetics and safety of voriconazole intravenous-to-oral switch regimens in immunocompromised japanese pediatric patients. Antimicrob. Agents Chemother. 2015, 59, 1004–1013. [Google Scholar] [CrossRef] [Green Version]
- Scott, S.A.; Sangkuhl, K.; Shuldiner, A.R.; Hulot, J.S.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmgkb summary: Very important pharmacogene information for cytochrome p450, family 2, subfamily c, polypeptide 19. Pharmacogenet. Genom. 2012, 22, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Hyland, R.; Jones, B.C.; Smith, D.A. Identification of the cytochrome p450 enzymes involved in the n-oxidation of voriconazole. Drug Metab. Dispos. 2003, 31, 540–547. [Google Scholar] [CrossRef] [Green Version]
- Bachmann, F.; Duthaler, U.; Meyer Zu Schwabedissen, H.E.; Puchkov, M.; Huwyler, J.; Haschke, M.; Krähenbühl, S. Metamizole is a moderate cytochrome p450 inducer via the constitutive androstane receptor and a weak inhibitor of cyp1a2. Clin. Pharmacol. Ther. 2021, 109, 1505–1516. [Google Scholar] [CrossRef]
- Bachmann, F.; Meyer Zu Schwabedissen, H.E.; Duthaler, U.; Krähenbühl, S. Cytochrome p450 1a2 is the most important enzyme for hepatic metabolism of the metamizole metabolite 4-methylaminoantipyrine. Br. J. Clin. Pharmacol. 2022, 88, 1885–1896. [Google Scholar] [CrossRef]
- Espinoza, N.; Galdames, J.; Navea, D.; Farfán, M.J.; Salas, C. Frequency of the cyp2c19*17 polymorphism in a chilean population and its effect on voriconazole plasma concentration in immunocompromised children. Sci. Rep. 2019, 9, 8863. [Google Scholar] [CrossRef] [Green Version]
- Zanger, U.M.; Schwab, M. Cytochrome p450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef] [PubMed]
- Elens, L.; van Gelder, T.; Hesselink, D.A.; Haufroid, V.; van Schaik, R.H. Cyp3a4*22: Promising newly identified cyp3a4 variant allele for personalizing pharmacotherapy. Pharmacogenomics 2013, 14, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Shi, L.; Li, H.; Wang, L.; Zhu, M.; Luo, J.; Zhang, Z. Effect of cyclosporine a and polymorphisms in cyp2c19 and abcc2 on the concentration of voriconazole in patients undergoing allogeneic hematopoietic stem cell transplantation. Xenobiotica 2020, 50, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Zamek-Gliszczynski, M.J.; Taub, M.E.; Chothe, P.P.; Chu, X.; Giacomini, K.M.; Kim, R.B.; Ray, A.S.; Stocker, S.L.; Unadkat, J.D.; Wittwer, M.B.; et al. Transporters in drug development: 2018 itc recommendations for transporters of emerging clinical importance. Clin. Pharmacol. Ther. 2018, 104, 890–899. [Google Scholar] [CrossRef]
- Lempers, V.J.; van den Heuvel, J.J.; Russel, F.G.; Aarnoutse, R.E.; Burger, D.M.; Brüggemann, R.J.; Koenderink, J.B. Inhibitory potential of antifungal drugs on atp-binding cassette transporters p-glycoprotein, mrp1 to mrp5, bcrp, and bsep. Antimicrob. Agents Chemother. 2016, 60, 3372–3379. [Google Scholar] [CrossRef] [Green Version]
- Haenisch, S.; May, K.; Wegner, D.; Caliebe, A.; Cascorbi, I.; Siegmund, W. Influence of genetic polymorphisms on intestinal expression and rifampicin-type induction of abcc2 and on bioavailability of talinolol. Pharmacogenet. Genom. 2008, 18, 357–365. [Google Scholar] [CrossRef]
- Itoda, M.; Saito, Y.; Soyama, A.; Saeki, M.; Murayama, N.; Ishida, S.; Sai, K.; Nagano, M.; Suzuki, H.; Sugiyama, Y.; et al. Polymorphisms in the abcc2 (cmoat/mrp2) gene found in 72 established cell lines derived from japanese individuals: An association between single nucleotide polymorphisms in the 5’-untranslated region and exon 28. Drug Metab. Dispos. 2002, 30, 363–364. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Yin, Y.; Sheng, Q.; Lu, X.; Wang, F.; Lin, Z.; Tian, H.; Xu, A.; Zhang, J. Association of abcc2 -24c>t polymorphism with high-dose methotrexate plasma concentrations and toxicities in childhood acute lymphoblastic leukemia. PLoS ONE 2014, 9, e82681. [Google Scholar] [CrossRef]
- Meyer zu Schwabedissen, H.E.; Kroemer, H.K. In vitro and in vivo evidence for the importance of breast cancer resistance protein transporters (bcrp/mxr/abcp/abcg2). In Drug Transporters; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2011; pp. 325–371. [Google Scholar]
- Allen, J.D.; Schinkel, A.H. Multidrug resistance and pharmacological protection mediated by the breast cancer resistance protein (bcrp/abcg2). Mol. Cancer Ther. 2002, 1, 427–434. [Google Scholar]
- Gupta, A.; Unadkat, J.D.; Mao, Q. Interactions of azole antifungal agents with the human breast cancer resistance protein (bcrp). J. Pharm. Sci. 2007, 96, 3226–3235. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, S.; Zhang, W.; Shi, Z. Polymorphisms of abcg2 and its impact on clinical relevance. Biochem. Biophys. Res. Commun. 2018, 503, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Meyer zu Schwabedissen, H.E.; Kim, R.B. Hepatic oatp1b transporters and nuclear receptors pxr and car: Interplay, regulation of drug disposition genes, and single nucleotide polymorphisms. Mol. Pharm. 2009, 6, 1644–1661. [Google Scholar] [CrossRef] [PubMed]
- Flockhart, D.A.; Oesterheld, J.R. Cytochrome p450-mediated drug interactions. Child Adolesc. Psychiatr. Clin. N. Am. 2000, 9, 43–76. [Google Scholar] [CrossRef]
- Bergogne-Bérézin, E. Clinical role of protein binding of quinolones. Clin. Pharmacokinet. 2002, 41, 741–750. [Google Scholar] [CrossRef]
- UCB-Pharma SA. Keppra® Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/keppra-epar-product-information_en.pdf (accessed on 22 April 2022).
- Nicolas, J.M.; Collart, P.; Gerin, B.; Mather, G.; Trager, W.; Levy, R.; Roba, J. In vitro evaluation of potential drug interactions with levetiracetam, a new antiepileptic agent. Drug Metab. Dispos. 1999, 27, 250–254. [Google Scholar]
- Hole, K.; Wollmann, B.M.; Nguyen, C.; Haslemo, T.; Molden, E. Comparison of cyp3a4-inducing capacity of enzyme-inducing antiepileptic drugs using 4β-hydroxycholesterol as biomarker. Ther. Drug Monit. 2018, 40, 463–468. [Google Scholar] [CrossRef]
- Patsalos, P.N. Clinical pharmacokinetics of levetiracetam. Clin. Pharmacokinet. 2004, 43, 707–724. [Google Scholar] [CrossRef]
- Strolin Benedetti, M.; Whomsley, R.; Nicolas, J.M.; Young, C.; Baltes, E. Pharmacokinetics and metabolism of 14c-levetiracetam, a new antiepileptic agent, in healthy volunteers. Eur. J. Clin. Pharmacol. 2003, 59, 621–630. [Google Scholar] [CrossRef]
- Li, Z.R.; Wang, C.Y.; Zhu, X.; Jiao, Z. Population pharmacokinetics of levetiracetam: A systematic review. Clin. Pharmacokinet. 2021, 60, 305–318. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SNP-Identifier | Gene | Genetic Variant | Assay ID | * |
|---|---|---|---|---|
| rs2273697 | ABCC2 | c.1249G > A | C__22272980_20 | |
| rs717620 | ABCC2 | c.24C > T | C___2814642_10 | |
| rs13120400 | ABCG2 | c.1194 + 928T > C | C___9510480_10 a | |
| rs2231142 | ABCG2 | c.421C > A | C__15854163_70 | * |
| rs12248560 | CYP2C19 | * 17; g.-806C > T | C___469857_10 | |
| rs28399504 | CYP2C19 | * 4; c.1A > G | C__30634136_10 | |
| rs4244285 | CYP2C19 | * 2; c.681G > A | C__25986767_70 | |
| rs4986893 | CYP2C19 | * 3; c.636G > A | C__27861809_10 | |
| rs35599367 | CYP3A4 | * 22; (intronic) C > T | C__59013445_10 a | * |
| rs10264272 | CYP3A5 | * 6; g.14690G > A | C__30203950_10 | * |
| rs776746 | CYP3A5 | * 3; g.6986A > G | C__26201809_30 | * |
| rs4149117 | SLCO1B3 | c.334G > T | C__25639181_40 |
| Female | 30.6 | % | N = 11 |
|---|---|---|---|
| Male | 69.4 | % | N = 25 |
| Age, median (range) | 10 (0–17) | years | N = 36 |
| Age, mean ± SD | 9.6 ± 5.4 | years | N = 36 |
| Body weight, median (range) | 30.6 (6.5–96.9) | kg | N = 36 |
| Body weight, mean ± SD | 35.5 ± 21.8 | kg | N = 36 |
| Body surface area *, (median (range) | 1.09 (0.33–2.25) | m2 | N = 35 |
| Body surface area *, mean ± SD | 1.13 ± 0.49 | m2 | N = 35 |
| Height, median (range) | 139.5 (62–188) | cm | N = 35 |
| Height, mean ± SD | 133.2 ± 34.0 | cm | N = 35 |
| Voriconazole i.v. | N = 21 | ||
| Voriconazole p.o. | N = 15 | ||
| Confirmed invasive aspergillosis (IA) | N = 23 | ||
| Probable or suspected IA | N = 7 | ||
| Prophylaxis of IA | N = 3 | ||
| Other IFI | N = 3 |
| SNP-Identifier | Gene | Genotype: Number of Individuals/Ctrough Measurements | MAF Observed | MAF Reported * | Χ2 a | Χ2 b | ||
|---|---|---|---|---|---|---|---|---|
| rs2273697 | ABCC2 | GG: 15/135 | GA: 8/105 | AA: 0 | 0.1739 | 0.2014 | 0.601 | 0.610 |
| rs717620 | ABCC2 | CC: 12/143 | CT: 10/96 | TT: 1/1 | 0.2609 | 0.1997 | 0.830 | 0.480 |
| rs13120400 | ABCG2 | TT: 12/140 | TC: 10/83 | CC: 1/17 | 0.2609 | 0.2185 | 0.830 | 0.809 |
| rs2231142 | ABCG2 | CC: 15/161 | CA: 7/47 | AA: 1/32 | 0.1957 | 0.1026 | 0.988 | 0.089 |
| rs12248560 | CYP2C19 | CC: 14/157 | CT: 9/83 | TT: 0 | 0.1957 | 0.2314 | 0.506 | 0.515 |
| rs28399504 | CYP2C19 | AA: 23/240 | AG: 0 | GG: 0 | n.d. | 0.0033 | n.a. | 0.927 |
| rs4244285 | CYP2C19 | GG: 16/161 | GA: 6/64 | AA: 1/15 | 0.1739 | 0.1473 | 0.907 | 0.762 |
| rs4986893 | CYP2C19 | GG: 22/224 | GA: 1/16 | AA: 0 | 0.0217 | 0.0058 | 0.994 | 0.358 |
| rs35599367 | CYP3A4 | CC: 22/237 | CT: 1/3 | TT: 0 | 0.0217 | 0.0462 | 0.994 | 0.732 |
| rs10264272 | CYP3A5 | GG: 23/240 | GA: 0 | AA: 0 | n.d. | 0.0011 | n.a. | 0.975 |
| rs776746 | CYP3A5 | GG: 22/216 | GA: 1/24 | AA: 0 | 0.0217 | 0.0700 | 0.994 | 0.435 |
| rs4149117 | SLCO1B3 | GG: 18/207 | GT: 4/32 | TT: 1/1 | 0.1304 | 0.1411 | 0.535 | 0.563 |
| Parameter | Reference Value for Intercept | Fit Effect | SE | p | Significance a |
|---|---|---|---|---|---|
| Fixed Effects | |||||
| θ1, Intercept (log(Ctrough)) | −2.0763 | 0.4637 | <10−4 | *** | |
| θ2, ln(dose/weight, mg/kg) | ln(1 mg/kg) | 0.8905 | 0.2004 | <10−4 | *** |
| θ3, Δ ln(surface area, m2) | ln(1 m2) | 1.1437 | 0.2388 | <10−5 | *** |
| θ4, ciprofloxacin | No ciprofloxacin | −0.9497 | 0.2925 | 0.0013 | ** |
| θ5, levetiracetam | No levetiracetam | −1.0043 | 0.2850 | 0.00051 | *** |
| θ6, propranolol | No propranolol | −0.5887 | 0.2671 | 0.028 | * |
| θ7, metamizole | No metamizole | −0.1520 | 0.1673 | 0.36 | |
| θ8, ABCC2 rs2273697 | ABCC2 rs2273697 GG | −0.6581 | 0.1708 | 0.00015 | *** |
| θ9, ABCC2 rs717620 | ABCC2 rs717620 CC | 0.4130 | 0.1918 | 0.032 | * |
| θ10, ABCG2 rs2231142 | ABCG2 rs2231142 CC | 0.4481 | 0.1391 | 0.0015 | ** |
| θ11, CYP2C19 rs4244285 | CYP2C19 rs4244285 GG | 0.8990 | 0.1980 | <10−5 | *** |
| θ12, CYP2C19 rs4986893 | CYP2C19 rs4986893 GG | 1.6289 | 0.4302 | 0.00019 | *** |
| θ13, CYP3A4 rs35599367 | CYP3A4 rs35599367 CC | 3.3737 | 0.6203 | <10−6 | *** |
| θ14, metamizole × CYP2C19 rs4244285 | No metamizole, CYP2C19 rs4244285 GG | −0.4911 | 0.2231 | 0.029 | * |
| Random effects distribution (SD) and Residuals | |||||
| ID intercept, n.a.; Residuals, 0.9385 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tilen, R.; Paioni, P.; Goetschi, A.N.; Goers, R.; Seibert, I.; Müller, D.; Bielicki, J.A.; Berger, C.; Krämer, S.D.; Meyer zu Schwabedissen, H.E. Pharmacogenetic Analysis of Voriconazole Treatment in Children. Pharmaceutics 2022, 14, 1289. https://doi.org/10.3390/pharmaceutics14061289
Tilen R, Paioni P, Goetschi AN, Goers R, Seibert I, Müller D, Bielicki JA, Berger C, Krämer SD, Meyer zu Schwabedissen HE. Pharmacogenetic Analysis of Voriconazole Treatment in Children. Pharmaceutics. 2022; 14(6):1289. https://doi.org/10.3390/pharmaceutics14061289
Chicago/Turabian StyleTilen, Romy, Paolo Paioni, Aljoscha N. Goetschi, Roland Goers, Isabell Seibert, Daniel Müller, Julia A. Bielicki, Christoph Berger, Stefanie D. Krämer, and Henriette E. Meyer zu Schwabedissen. 2022. "Pharmacogenetic Analysis of Voriconazole Treatment in Children" Pharmaceutics 14, no. 6: 1289. https://doi.org/10.3390/pharmaceutics14061289