1. Introduction
Pre-exposure prophylaxis (PrEP) has shown high efficacy against HIV transmission during receptive intercourse [
1]. However, the dosing requirements for insertive sex are not known. TAF is a newer version of TDF and, in combination with FTC, has a smaller pill size than FTC-TDF. Whilst TDF-emtricitabine (FTC) has been evaluated in many trials and risk groups, TAF-FTC PrEP has only been evaluated in one PrEP efficacy clinical trial [
2,
3]. The CHAPS Trial (NCT03986970) aims to optimize on-demand PrEP dosing or both TDF-FTC and TAF-FTC in a pharmacokinetic (PK) and pharmacodynamic (PD) randomized control trial providing oral PrEP prior to voluntary medical male circumcision and evaluating activity using the ex vivo foreskin tissue explant HIV-challenge model [
4]. However, no pre-clinical data were available on the anti-HIV activity of TAF in foreskin tissue to help design this comparative clinical trial.
TAF has potential safety advantages over TDF with fewer renal and bone side effects than TDF. It is converted intracellularly to TFV and phosphorylated to the active TFV–diphosphate (DP) form [
5]. This accounts for four- to seven-fold higher intracellular concentrations of TFV–DP in PBMC than with TDF/FTC [
6,
7,
8,
9]. However, this advantage has not been consistently reported in mucosal tissues. In a single 25 mg dose of TAF study, a large proportion of vaginal and rectal tissue samples had unquantifiable TFV–DP levels, and the metabolite could not be detected beyond 72 h post-dose [
10]. TFV–DP concentrations were approximately 1.3- and 13-fold lower in vaginal and rectal tissue compared with concentrations achieved after administration 300 mg TDF/FTC [
11]. Similarly, in another pharmacokinetic study, TFV–DP was quantifiable in only 33% cervicovaginal tissue samples after a single dose of tenofovir alafenamide, although TFV–DP concentrations did increase after 14 daily doses [
12].
Studies with female genital tract (FGT) models have shown that TAF achieves similar protection against HIV infection at concentrations ~300-fold lower than TFV [
13,
14]. However, none has been carried out for insertive sex. TFV inhibits ex vivo infection of foreskin tissue explants at 1 mg/mL [
15]. However, no studies to date have established a comparison between TFV and TAF in foreskin tissue. Hence, we aimed to define the ex vivo inhibitory concentrations providing pharmacological equivalency between TAF and TFV in foreskin tissue to be used in the CHAPS trial [
4].
2. Materials and Methods
2.1. Reagents and Viral Isolate
TFV and TAF were donated by Gilead Sciences, Inc. (Foster City, CA, USA). A single HIV-1
BaL [
16] stock (
http://www.aidsreagent.org/) (accessed on 19 April 2022) was prepared in activated PBMCs [
17].
2.2. Human Tissue
Two surgically resected foreskins were collected at Charing Cross Hospital, London, UK, and three at Chris Hani Baragwanath Academic Hospital, Soweto, South Africa. Tissues were collected after receiving signed informed consent from all patients through the Imperial College Healthcare Tissue Bank, approved by Research Ethics Committee Wales (IRAS 17/WA/0161), or through the University of the Witwatersrand Human Research Ethics Committee (180906B) and South African Health Products Regulatory authority (SAHPRA) (20181004).
2.3. Cell and Foreskin Tissue Explants Culture
TZM-bl cells [
18,
19,
20] were grown in Dulbecco’s Minimal Essential Medium (DMEM) (Sigma-Aldrich, Inc., St. Louis, MO, USA) containing 10% fetal calf serum (FCS), 2 mM L-glutamine and antibiotics (100 U of penicillin/mL, 100 µg of streptomycin/mL). Cells were tested for mycoplasma contamination and confirmed mycoplasma-free.
Tissues were transported and processed in local sites within 30 min of surgical resection. The tissues were dissected and the outer and inner foreskin specimens were cut into 2–3 mm
3 explants comprising the inner squamous epithelium, lamina propria, dartos layer and preputial skin, as described previously [
15]. Explants were maintained in a non-polarized system in 96-well U-bottom plates with complete high glucose DMEM (containing 10% fetal calf serum, 2 mM
l-glutamine, 100 U of penicillin/mL, 100 µg of streptomycin/mL, 80 µg of gentamicin/mL and 2.5 µg of amphotericin B) at 37 °C in an atmosphere containing 5% CO
2.
2.4. Infectivity and Inhibition Assays
The infectivity of the HIV-1
BaL stock was estimated in TZM-bl cells (by luciferase quantitation of cell lysates; Promega, Madison, WI, USA) and in activated PBMCs (by measurement of p24 antigen content in cell culture supernatants). The extent of luciferase expression was recorded in relative light units (r.l.u), as described previously [
21]. Viral p24 content in the supernatants was measured with HIV-1 p24 ELISA (Innotest HIV antigen ELISA, Fujirebio Europe, Ghent, Belgium), following the manufacturer’s instructions. Viral growth was reported as pg/mL of p24, extrapolated from the p24 kit-supplied standard curve generated by ODs using a sigmoidal dose–response curve (Prism, GraphPad, San Diego, CA, USA). Appropriate dilutions of culture supernatants were applied to ensure that the data were within the 95% interval of the standard OD range.
Inhibition assays were performed using a standardized amount of virus culture supernatant normalized for infectivity. Considering the published data on FGT [
14], TZM-bl cells and explants (one outer and one inner foreskin explant were pooled in each well) were exposed in triplicate to serial dilutions of drug at a constant ratio of 1 TAF to 300 TFV. After 1 h at 37 °C, virus was added to TZM-bl cells (10
3.3 TCID
50/mL) and left for the time of the experiment. Alternatively, tissue explants were challenged with HIV-1
BaL at the HVT (10
4 TCID
50/mL) routinely used to obtain productive infection of explants or at a more biologically relevant LVT (10
2 TCID
50/mL). Ex vivo dosing with TFV and TAF, along with viral challenge of tissue explants, was performed in a non-polarized manner. After 2 h of incubation, explants were washed with PBS, transferred to fresh plates and cultured for 15 days in the absence of inhibitors. Approximately 50% of the supernatants was harvested every 3 to 4 days and replaced with fresh media. Infectivity was evaluated in supernatants by analysis of p24 concentration (Innotest HIV antigen ELISA).
2.5. Bioanalysis
Parallel explant cultures were set up as described for the inhibition assays with the same total incubation times but without viral challenge to measure TAF, TFV and TFV–DP levels in tissues. Quantifications of dosing supernatant (post-3 h incubation), wash solutions (pooled) and 48 h culture supernatant were performed on a SCIEX 5500 triple quadrupole mass spectrometer interfaced with an electrospray ionisation source (AB Sciex Limited, Warrington, UK) operating in SRM and positive ionisation mode. Analyst software (version 1.7) was used for the optimization of tuning parameters and data acquisition. Multiquant (version 3.03) software was used for peak integration and data processing.
Tissue weight (~10 mg) was converted to volume (µL) by dividing by 1.05 g/mL (1.05 mg/µL) and made up to 100 µL with ice-cold methanol and 20 mM EDTA–EGTA (70:30 v/v). Explants were homogenized in 2 mL tubes (1.4 mm ceramic beads) using a MINILYS homogenizer at 4000 rpm for 120 s. Deuterated internal standards (TFV-d6, TAF-d5 and 13C-TFV–DP) were added to all tubes containing 100 µL of homogenate or supernatant prior to solid phase extraction (SPE). Following the addition of 1% formic acid (300 µL), TAF and TFV were extracted using strong cation exchanger SPE cartridges (SOLA SCX (10 mg/mL)). TFV–DP was extracted with a mixture of acetonitrile–formic acid (100 µL; 98:2 v/v) followed by further sample clean-up using polymeric reverse phase SPE (Strata-X 33 µ (30 mg/1 mL)). TAF and TFV were eluted using a reverse phase Synergi Polar C18 column (Phenomenex, Cheshire, UK). The calibration curve ranged between 0.1 and 100 ng/sample (TFV) and 0.05 and 50 ng/sample (TAF). TFV–DP and its internal standard were eluted using a weak anion exchange column (Thermo Biobasic AX, Thermo Fisher Scientific, Waltham, MA, USA). The calibration curve for TFV–DP ranged between 0.07 and 25 ng/sample (sample = 100 µL) on the column.
All analytical methods were validated in accordance with the EMEA guidelines on bioanalytical method validation. The intra- and inter-assay precision (expressed as percent coefficient of variation (%CV)) ranged between 1.91 and 8.62 (TFV) and 3.34 and 9.11 (TFV–DP), and the accuracy (expressed as %Bias) was between −4.08 and 2.83 (TFV) and −4.79 and 5.55, respectively. The average percentage (%) recovery of TFV and TFV–DP from culture media (which was used as a surrogate for a foreskin tissue explant) was 35% and 92%, respectively, and analyte recovery was consistent across the assay calibration range.
2.6. Viability Assay
Viability of tissue explants following exposure to drugs was determined by measuring tetrazolium salt [3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyl-2H-tetrazolium bromide (MTT)] cleavage into a blue product (formazan) by viable cells [
22], as described previously [
23]. Optical density values obtained with a Synergy-HT (BioTek, Winooski, VT, USA) plate reader were corrected for explant dry weight. Untreated tissue was considered as a positive control for viability (100%). Nonoxynol-9 (N-9) (LKT Laboratories Inc., St Paul, MN, USA) at 2%
v/
v was used as a known cytotoxic agent [
24].
2.7. Statistical Analysis
Drug concentrations were quantified using a ng/sample calibration curve and normalised to ng/gram of tissue, or ng/mL of dosing/wash/culture supernatant for TAF and TFV or to pmol/g or pmol/mL, respectively, for TFV–DP. Values below the assay limit of quantification (<LLQ) were expressed as half the LLQ and subsequently normalised to per gram of tissue. Values below the assay limit of detection (LoD) and with no visible chromatographic peak above the baseline were excluded.
p24 values were calculated from sigmoid curve fitted (Prism, GraphPad) fulfilling the criterion of R2 > 0.7. Pearson’s test was used for correlations.
Drug concentrations were log10-transformed and correlated with the corresponding log-transformed p24 level at day 15 of tissue explant culture post-infection for each subject using a Pearson correlation test. p-values were determined using a two-tailed unpaired Student’s t-test, and a p-value < 0.05 was considered statistically significant.
3. Results
3.1. Ex Vivo PK Equivalency in Foreskin Explants
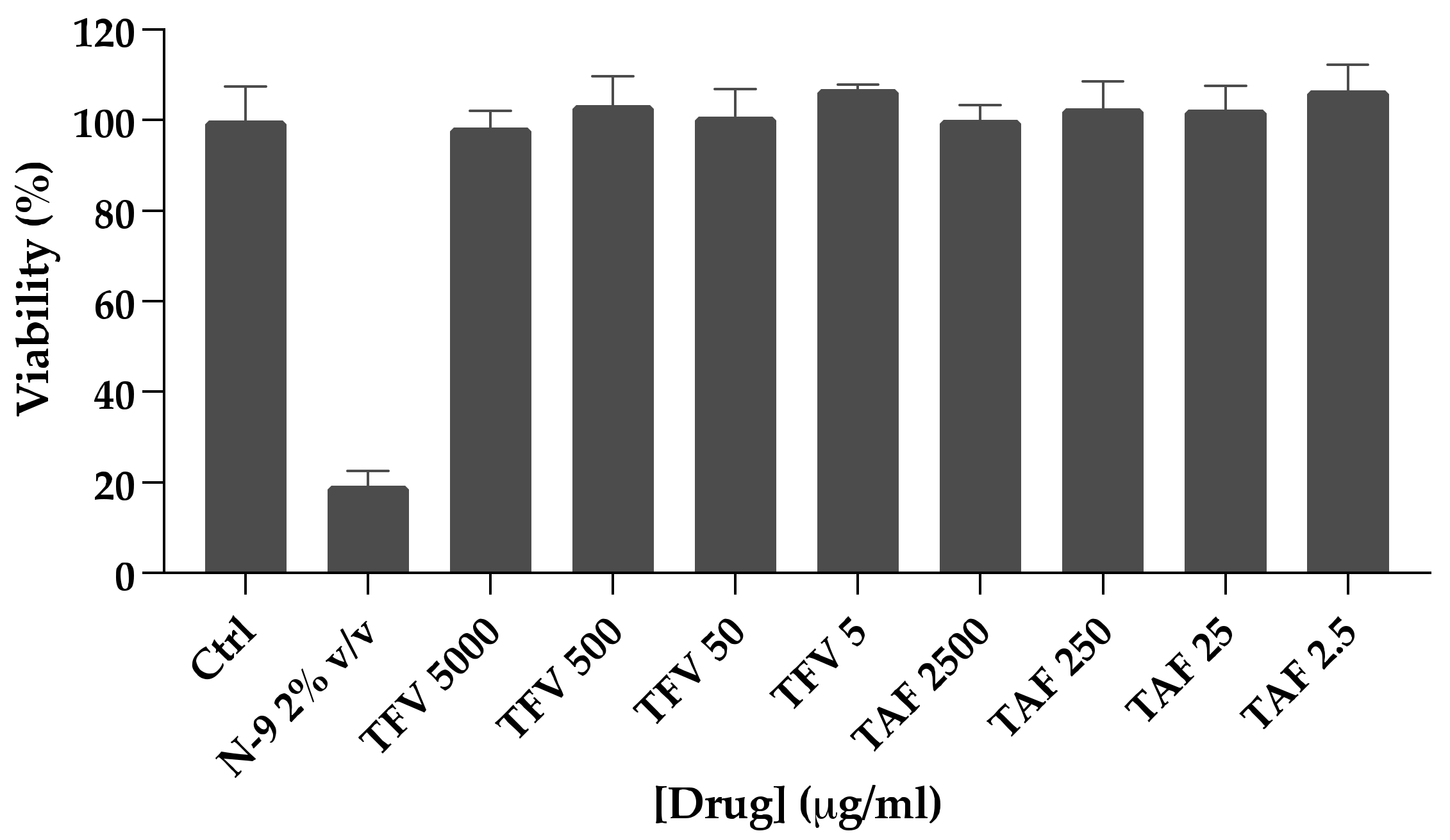
Tissue explants were dosed with the base compounds TAF or TFV. TFV, instead of TDF, was used to mimic the rapid cleavage of the prodrug to TFV in plasma and kidneys following oral dosing. Ex vivo dosing of foreskin explants to TFV or TAF did not induce cytotoxicity at the concentrations tested in this study (
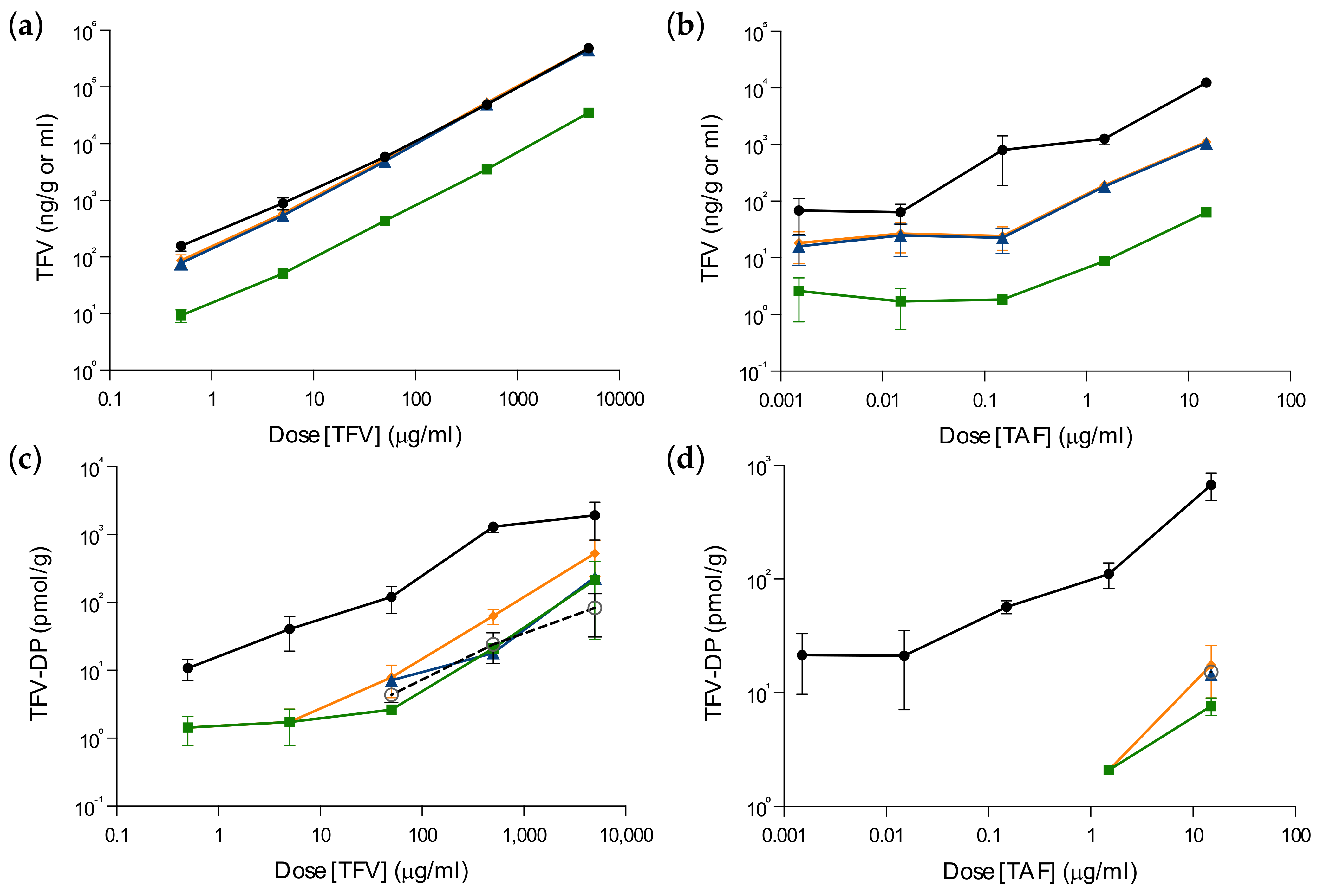
Figure 1). Parent TFV was quantifiable in all foreskin explants after incubation with both TFV and TAF, with approximately five-fold higher levels detected after TAF dosing (
Figure 2a,
Table S1). Following incubation with TFV, excess levels of parent drug (~80% of tissue) were present in the culture supernatants, whereas, with TAF dosing, TFV levels in culture media were on average less than 20% of total TFV in explants (
Figure S1a,b). TAF was undetectable in tissue explants.
Intracellular TFV–DP concentrations in the explants were approximately six-fold higher after ex vivo dosing with 15 µg/mL of TAF compared with an equivalent dose of TFV (
Figure 2b,
Table S2). In both cases, the concentration of TFV–DP achieved in tissue was proportional to dosing (TFV r
2 = 0.710; TAF r
2 = 0.998;
p = 0.017), and there was no evidence of saturation. TFV–DP was unquantifiable in 91% of explants dosed with ≤5 µg/mL (TFV) and 78% dosed with ≤0.15 µg/mL (TAF). TFV and TFV–DP concentrations in tissue were highly correlated following dosing with TFV (r
2 = 0.7905;
p < 0.0001) or with TAF (r
2 = 0.7342;
p < 0.0001) (
Figure 2c,d).
Following incubation with TFV, the summated concentration of TFV–DP measured in the dosing supernatant, culture supernatant and wash solution accounted for 12% (range: 1–29%) of the total amount detected in the tissue explant (
Figure 3c,d). TFV–DP concentrations in culture and wash samples after dosing with TAF were below LLD.
3.2. Inhibitory Activity in Foreskin Explants
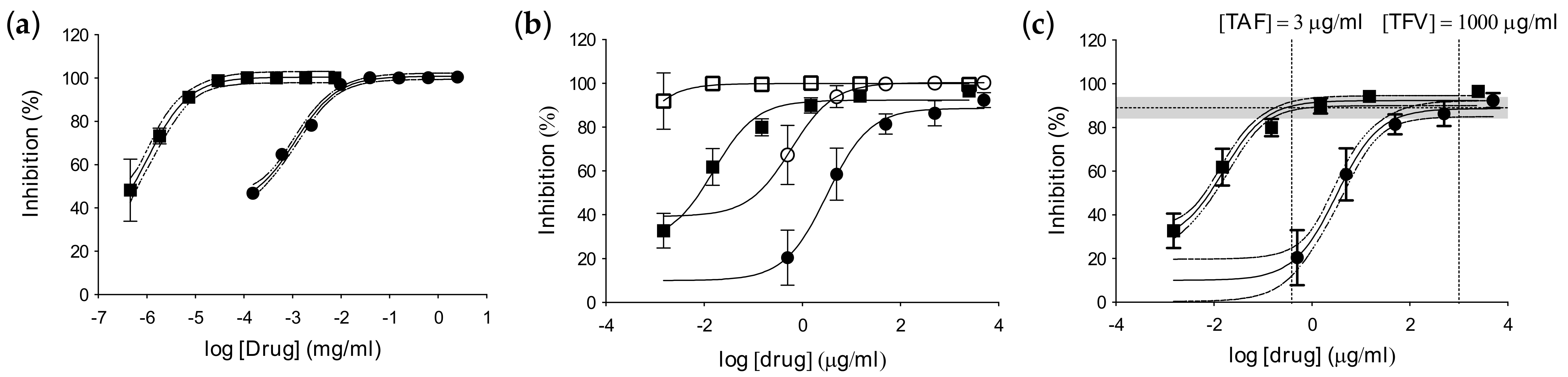
Prior to evaluating the potency of TFV and TAF in tissue explants, we confirmed their activity in TZM-bl cells. As expected, statistically significant greater in vitro activity was observed for TAF (
Figure 4a,
Table 1), with a 50% inhibitory concentration (IC
50) three logs lower (IC
50 = 0.0006 ± 0.0003) than that for TFV (IC
50 = 0.203 ± 0.069) against HIV-1
BaL (
p = 0.0073).
Dose–response curves were obtained for both drugs against HIV-1
BaL at HVT and LVT in foreskin tissue explants and, as observed in TZM-bl cells, TAF was significantly more potent than TFV (against HVT: TFV IC
50 = 3.69 ± 0.61 and TAF IC
50 = 0.018 ± 0.004;
p < 0.0001) (
Figure 4b,
Table 1). Equivalency of ex vivo inhibitory potency was established from 3 µg/mL of TAF and 1 mg/mL of TFV using the dose–response curve against the high viral challenge titer (
Figure 4c).
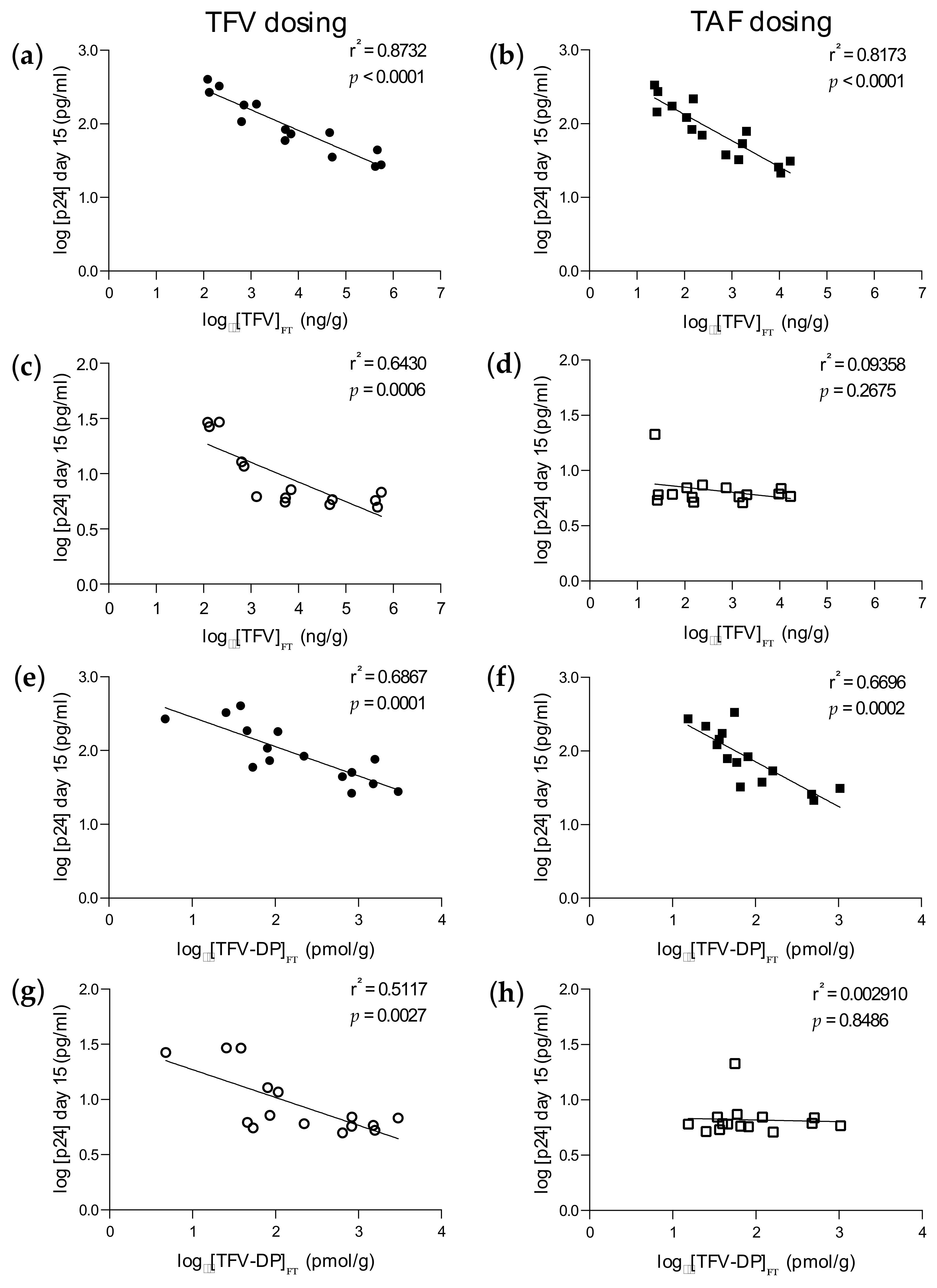
Importantly, statistically significant inverse correlations between ex vivo infectivity levels and drug concentrations were observed for both TFV (
Figure 5a,b) and TFV–DP (
Figure 5e,f) against HVT following ex vivo dosing with TFV (r
2 = 0.8732;
p < 0.0001 for TFV; r
2 = 0.6867;
p = 0.0001 for TFV–DP) and TAF (r
2 = 0.8173;
p < 0.0001 for TFV; r
2 = 0.6696;
p = 0.0002 for TFV–DP). However, significant correlations following LVT challenge were observed with ex vivo TFV dosing (r
2 = 0.6430;
p = 0.0006 for TFV; r
2 = 0.5117;
p = 0.0027 for TFV–DP) (
Figure 5c,g) and not TAF (r
2 = 0.09358;
p = 0.2675 for TFV; r
2 = 0.00291;
p = 0.8486 for TFV–DP) (
Figure 5d,h). We further investigated these correlations by assessing whether a non-linear correlation would be a better fit. Analysis revealed that a non-linear fit was possible for TFV levels in tissues following ex vivo dosing with TFV against LVT challenge (
Figure S1).
4. Discussion
This study showed that higher levels of tenofovir–DP in foreskin explants were obtained following ex vivo dosing with TAF compared to tenofovir. This is in keeping with results obtained from vaginal and rectal tissue [
10,
11,
12]. Our data demonstrated that ex vivo dosing with 15 µg/mL TAF achieved equivalent concentrations of TFV–DP in foreskin tissue (~1000 pmol/gram) to a 1 mg/mL dose of TFV. The highly significant correlations observed between TFV and TFV–DP indicates the physiological relevance of the ex vivo dosing model. The CHAPS trial will confirm the levels of penetration and metabolization of tenofovir and tenofovir alafenamide in foreskin tissue following oral dosing [
4]. The ex vivo inhibitory equivalency observed in foreskin explants was the same as that described in FGT models [
13,
14] and was confirmed by the significant inverse PK–PD correlations.
The lack of ex vivo PK–PD correlation in explants dosed with tenofovir alafenamide and challenged with a low viral titer was due to the limited range of concentrations tested, resulting in an incomplete dose–response curve for tenofovir alafenamide. The four-parameter non-linear fit observed only for the TFV levels in tissue following ex vivo dosing with TFV against ex vivo challenge with LVT could be an artifact due to the limited sample size, and the results from the CHAPS trial will help to clarify this discrepancy.
Both TFV and TAF have been shown to be stable within the time of dosing we used in this study (3 h) in the culture conditions (37 °C in buffered media such as the complete culture media containing DMEM with sodium bicarbonate) [
25,
26]. Furthermore, we do not expect that TFV in the culture supernatants will have degraded, both during the 48 h post-dosing incubation period and at the time of downstream PK analysis. The culture supernatants were harvested and immediately placed in a −80 °C freezer prior to drug quantification analysis. The samples were analyzed within 11 months from the time of collection/harvesting. We have extensive in-house stability data to suggest that TFV remains stable in plasma for a prolonged period (>2 years) when frozen at this temperature, when subjected to heat treatment (2 × 58 °C; 50 min) and following up to three freeze–thaw cycles. Other research groups have demonstrated TFV (plasma) stability for up to 34 months at −80 °C [
27]. Similarly, TFV was shown to be stable (in media) after being left on the bench at ambient temperature for approximately 20 h, and other groups have shown that it is stable in plasma at ambient temperature for up to 144 h [
27]. Drug loss into culture media compared to dosing input levels was higher with tenofovir compared to tenofovir alafenamide and can likely be attributed to the presence of either unabsorbed or unconverted drug, as well as loss from the explants by passive diffusion or active cellular efflux. Consistent with previous observations in FGT tissue and urethral secretions [
10,
28], with the harvesting schedule of this study and despite topical exposure, tenofovir alafenamide was undetectable in foreskin explants, presumably due to the prodrug’s rapid interconversion to tenofovir in tissue. Drug levels in dosing supernatants, wash buffer and culture supernatant samples were expressed as ng/mL of solution, whereas tissue concentrations were derived from a ng/sample calibration curve (i.e., ng per mg of tissue extracted) and subsequently normalized to ng/gram of tissue. We chose to standardize the concentration units for both tissue and solutions based on the assumption that 1 mL is equal to 1 g of tissue, as opposed to using actual values (e.g., ng per mg of tissue explant “on column”), since both tissue weight and volume of the surrounding supernatant/wash solutions harvested from the incubation experiment were variable factors.
The mucosal tissue explant model [
29,
30,
31,
32] has limitations, including (i) progressive loss of architecture despite the maintenance of CD4:CD8 T cell ratios and sufficient viability to sustain viral replication for more than 10 days [
33]; (ii) a paucity of data regarding the preservation of immune competence [
30]; (iii) limitation in demonstrating sterilizing protection; and (iv) an inability to metabolize certain prodrugs, such as TFV disoproxil fumarate, which is the formulated version of TFV for oral administration. Despite these limitations, tissue explants are an important tool for basic research [
34,
35,
36,
37,
38,
39] and pre-clinical screening of PrEP regimens [
40] and are increasingly being used in clinical trials for PK–PD assessment [
4,
41,
42,
43,
44,
45,
46,
47,
48,
49,
50,
51,
52,
53,
54,
55]. It has been shown that consistent results can be obtained among different laboratories through protocol standardization [
56] and that the model can be used to refine animal models and increase their predictive power [
57]. Furthermore, in vivo viral replication fitness can be mimicked in mucosal tissue explants [
21,
57,
58] and, following ex vivo challenge, virus has been shown in different mucosal tissue explant models to penetrate the lamina propia with similar kinetics to those observed in vivo [
34,
59,
60].
The primary purpose of this study was to derive suitable and equivalent doses of TAF and TDF to inform the ex vivo PEP dosing in the CHAPS clinical trial and not to specifically define compartmental PK. Thus, the doses used in this study were based on the concentration of TFV that is known to inhibit ex vivo infection of foreskin tissue and not derived from doses administered in vivo. Ex vivo dosing of tissue explants will likely result in higher localized drug concentrations than tissue sampled from orally medicated subjects for a number of reasons, including the ratio of drug-to-tissue surface area, enzymatic activity, incubation time and weight of tissue. Indeed, there is a trend towards lower TFV levels with F–TAF dosing, compared with TDF in cervical/vaginal tissue [
10,
11,
12]. TAF is known to be a substrate of multidrug resistance protein 1 and breast cancer resistance protein, whereas TFV is not. These efflux transporters are expressed within mucosal tissues and may eliminate TAF but not TFV from the localized site in vivo. It is also possible that the inherent activity of such efflux transporters differs in the ex vivo dosing model.
Our study has established ex vivo dosing concentrations to reach PK–PD equivalency between tenofovir alafenamide and tenofovir in foreskin tissue and suggests an improved PK mucosal profile for TAF. Furthermore, it emphasizes the need to assess the pharmacological profile of PrEP candidates in mucosal tissues.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/pharmaceutics14061285/s1, Table S1: Tenofovir concentrations after ex vivo dosing of foreskin explants with tenofovir alafenamide (TAF) and tenofovir (TFV); Table S2: Tenofovir–DP concentrations after ex vivo dosing of foreskin explants with tenofovir alafenamide (TAF) and tenofovir (TFV); Figure S1: Non-linear model of TFV dose and p24 response correlation.
Author Contributions
Conceptualization, C.H., L.E., S.K. and C.C.; methodology, C.H., L.E., S.D.P., A.-D.P. and T.B.S.; validation, C.H. and L.E.; formal analysis, C.H. and L.E.; investigation, C.H., L.E., A.-D.P., T.B.S., L.L., S.D.P., S.M., R.M., T.R. and N.M.; resources, A.-D.P., T.B.S., L.L., N.M., S.K., R.M., T.R. and S.M.; data curation, C.H. and L.E.; writing—original draft preparation, C.H., L.E., C.C., S.K. and J.F.; writing—review and editing, all authors; supervision, C.H.; funding acquisition, C.H., S.K., N.M. and J.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the EDCTP2 program supported by the European Union, grant number RIA2016MC-1616-CHAPS, and through an investigator-led grant from Gilead Sciences.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved through the Imperial College Healthcare Tissue Bank approved by Research Ethics Committee Wales (IRAS 17/WA/0161) or through the University of the Witwatersrand Human Research Ethics Committee (180906B) and South African Health Products Regulatory authority (SAHPRA) (20181004).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available upon request.
Acknowledgments
We thank the CHAPS trial participants, and the CHAPS consortium: Nadia Ahmed, Amara Alieu, Berenice Alinde, Millicent Atujuna, Vincent Basajja, Linda-Gail Bekker, Asiphe Besethi, Francesca Chiodi, Mike Chirenje, Janan Dietrich, Charity Dire, Jeffrey Dorfman, Deirdre Egan, Laura Else, Julie Fox, Clive Gray, Carolina Herrera, Stefanie Hornschuh, Ayoub Kakande, Pon-tiano Kaleebu, Zephyrian Kamushaaga, Charles Kelly, Saye Khoo, Mamakiri Khunwane, Abigail Kubeka, Sophie Lam, Limakatso Lebina, Boitshoko Mahlangu, Joseph Makhura, Nomvuyo Mang-xilana, Neil Martinson, Andrew Moultrie, Susan Mugaba, Richard Muhumuza, Winnie Nabu-keera, Patricia Namubiru, Stephen Nash, Denis Ndekezi, Teacler Nematadzira, Lumka Nobula, Geoffrey Odoch, Kyle O’Hagan, Daniel Opoka, Kennedy Otwombe, Stefan Petkov, Azure-Dee Pillay, Cosnet Lerato Rametse, Elzette Rousseau, Portia Seatlholo, Janet Seeley, Thabiso Seiphetlo, Jennifer Serwanga, Robin Shattock, Andrew Ssemata, Lynda Stranix-Chibanda, Gugulethu Tshabalala, Emily Webb, Helen Weiss. We thank the Liverpool Biomedical Research Centre funded by Liverpool Health Partners for infrastructural support.
Conflicts of Interest
C.H. has received research grants from Gilead. N.M. has received a research grant from Pfizer. S.K. has received research support from ViiV, Gilead and Merck. J.F. has received travel and research grants from Gilead and ViiV. C.C. is employed by Gilead. L.E., S.D.P., A.P., T.S., S.M., R.M., T.R. and L.L. declare no conflict of interest. EDCTP had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. C.C., as a Gilead employee, contributed to the conceptualization of the study and the writing of the manuscript.
References
- Molina, J.-M.; Capitant, C.; Spire, B.; Pialoux, G.; Cotte, L.; Charreau, I.; Tremblay, C.; Le Gall, J.-M.; Cua, E.; Pasquet, A.; et al. On-Demand Preexposure Prophylaxis in Men at High Risk for HIV-1 Infection. N. Engl. J. Med. 2015, 373, 2237–2246. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.H.; Molina, J.M.; Thompson, M.A.; Anderson, P.L.; Mounzer, K.C.; De Wet, J.J.; DeJesus, E.; Jessen, H.; Grant, R.M.; Ruane, P.J.; et al. Emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis (DISCOVER): Primary results from a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet 2020, 396, 239–254. [Google Scholar] [CrossRef]
- Ogbuagu, O.; Ruane, P.J.; Podzamczer, D.; Salazar, L.C.; Henry, K.; Asmuth, D.M.; Wohl, D.; Gilson, R.; Shao, Y.; Ebrahimi, R.; et al. Long-term safety and efficacy of emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV-1 pre-exposure prophylaxis: Week 96 results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet HIV 2021, 8, e397–e407. [Google Scholar] [CrossRef]
- Nash, S.; Dietrich, J.; Ssemata, A.S.; Herrera, C.; O’Hagan, K.; Else, L.; Chiodi, F.; Kelly, C.; Shattock, R.; Chirenje, M.; et al. Combined HIV Adolescent Prevention Study (CHAPS): Comparison of HIV pre-exposure prophylaxis regimens for adolescents in sub-Saharan Africa-study protocol for a mixed-methods study including a randomised controlled trial. Trials 2020, 21, 900. [Google Scholar] [CrossRef]
- Lee, W.A.; He, G.X.; Eisenberg, E.; Cihlar, T.; Swaminathan, S.; Mulato, A.; Cundy, K.C. Selective intracellular activation of a novel prodrug of the human immunodeficiency virus reverse transcriptase inhibitor tenofovir leads to preferential distribution and accumulation in lymphatic tissue. Antimicrob. Agents Chemother. 2005, 49, 1898–1906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callebaut, C.; Stepan, G.; Tian, Y.; Miller, M.D. In Vitro Virology Profile of Tenofovir Alafenamide, a Novel Oral Prodrug of Tenofovir with Improved Antiviral Activity Compared to That of Tenofovir Disoproxil Fumarate. Antimicrob. Agents Chemother. 2015, 59, 5909–5916. [Google Scholar] [CrossRef] [Green Version]
- Ruane, P.J.; DeJesus, E.; Berger, D.; Markowitz, M.; Bredeek, U.F.; Callebaut, C.; Zhong, L.; Ramanathan, S.; Rhee, M.S.; Fordyce, M.W.; et al. Antiviral activity, safety, and pharmacokinetics/pharmacodynamics of tenofovir alafenamide as 10-day monotherapy in HIV-1-positive adults. J. Acquir. Immune Defic. Syndr. 2013, 63, 449–455. [Google Scholar] [CrossRef] [Green Version]
- Sax, P.E.; Wohl, D.; Yin, M.T.; Post, F.; DeJesus, E.; Saag, M.; Pozniak, A.; Thompson, M.; Podzamczer, D.; Molina, J.M.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: Two randomised, double-blind, phase 3, non-inferiority trials. Lancet 2015, 385, 2606–2615. [Google Scholar] [CrossRef]
- Sax, P.E.; Zolopa, A.; Brar, I.; Elion, R.; Ortiz, R.; Post, F.; Wang, H.; Callebaut, C.; Martin, H.; Fordyce, M.W.; et al. Tenofovir alafenamide vs. tenofovir disoproxil fumarate in single tablet regimens for initial HIV-1 therapy: A randomized phase 2 study. J. Acquir. Immune Defic. Syndr. 2014, 67, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Cottrell, M.L.; Garrett, K.L.; Prince, H.M.A.; Sykes, C.; Schauer, A.; Emerson, C.W.; Peery, A.; Rooney, J.F.; McCallister, S.; Gay, C.; et al. Single-dose pharmacokinetics of tenofovir alafenamide and its active metabolite in the mucosal tissues. J. Antimicrob. Chemother. 2017, 72, 1731–1740. [Google Scholar] [CrossRef]
- Cottrell, M.L.; Yang, K.H.; Prince, H.M.; Sykes, C.; White, N.; Malone, S.; Dellon, E.S.; Madanick, R.D.; Shaheen, N.J.; Hudgens, M.G.; et al. A Translational Pharmacology Approach to Predicting Outcomes of Preexposure Prophylaxis Against HIV in Men and Women Using Tenofovir Disoproxil Fumarate with or Without Emtricitabine. J. Infect. Dis. 2016, 214, 55–64. [Google Scholar] [CrossRef]
- Thurman, A.R.; Schwartz, J.L.; Cottrell, M.L.; Brache, V.; Chen, B.A.; Cochon, L.; Ju, S.; McGowan, I.; Rooney, J.F.; McCallister, S.; et al. Safety and Pharmacokinetics of a Tenofovir Alafenamide Fumarate-Emtricitabine based Oral Antiretroviral Regimen for Prevention of HIV Acquisition in Women: A Randomized Controlled Trial. EClinicalMedicine 2021, 36, 100893. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, M.; Patel, M.V.; Shen, Z.; Bodwell, J.; Rossoll, R.M.; Wira, C.R. Tenofovir Inhibits Wound Healing of Epithelial Cells and Fibroblasts from the Upper and Lower Human Female Reproductive Tract. Sci. Rep. 2017, 8, 45725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Z.; Rodriguez-Garcia, M.; Patel, M.V.; Bodwell, J.; Wira, C.R. Epithelial Cells and Fibroblasts from the Human Female Reproductive Tract Accumulate and Release TFV and TAF to Sustain Inhibition of HIV Infection of CD4+ T cells. Sci. Rep. 2019, 9, 1864. [Google Scholar] [CrossRef] [PubMed]
- Fischetti, L.; Barry, S.M.; Hope, T.J.; Shattock, R.J. HIV-1 infection of human penile explant tissue and protection by candidate microbicides. AIDS 2009, 23, 319–328. [Google Scholar] [CrossRef]
- Gartner, S.; Markovits, P.; Markovitz, D.M.; Kaplan, M.H.; Gallo, R.C.; Popovic, M. The role of mononuclear phagocytes in HTLV-III/LAV infection. Science 1986, 233, 215–219. [Google Scholar] [CrossRef]
- Gordon, C.J.; Muesing, M.A.; Proudfoot, A.E.; Power, C.A.; Moore, J.P.; Trkola, A. Enhancement of human immunodeficiency virus type 1 infection by the CC-chemokine RANTES is independent of the mechanism of virus-cell fusion. J. Virol. 1999, 73, 684–694. [Google Scholar] [CrossRef] [Green Version]
- Derdeyn, C.A.; Decker, J.M.; Sfakianos, J.N.; Wu, X.; O’Brien, W.A.; Ratner, L.; Kappes, J.C.; Shaw, G.M.; Hunter, E. Sensitivity of human immunodeficiency virus type 1 to the fusion inhibitor T-20 is modulated by coreceptor specificity defined by the V3 loop of gp120. J. Virol. 2000, 74, 8358–8367. [Google Scholar] [CrossRef] [Green Version]
- Platt, E.J.; Wehrly, K.; Kuhmann, S.E.; Chesebro, B.; Kabat, D. Effects of CCR5 and CD4 cell surface concentrations on infections by macrophagetropic isolates of human immunodeficiency virus type 1. J. Virol. 1998, 72, 2855–2864. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Decker, J.M.; Liu, H.; Zhang, Z.; Arani, R.B.; Kilby, J.M.; Saag, M.S.; Wu, X.; Shaw, G.M.; Kappes, J.C. Emergence of resistant human immunodeficiency virus type 1 in patients receiving fusion inhibitor (T-20) monotherapy. Antimicrob. Agents Chemother. 2002, 46, 1896–1905. [Google Scholar] [CrossRef] [Green Version]
- Herrera, C.; Cranage, M.; McGowan, I.; Anton, P.; Shattock, R.J. Reverse transcriptase inhibitors as potential colorectal microbicides. Antimicrob. Agents Chemother. 2009, 53, 1797–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slater, T.F.; Sawyer, B.; Straeuli, U. Studies on Succinate-Tetrazolium Reductase Systems. Iii. Points of Coupling of Four Different Tetrazolium Salts. Biochim. Biophys. Acta 1963, 77, 383–393. [Google Scholar] [CrossRef]
- Mesquita, P.M.; Wilson, S.S.; Manlow, P.; Fischetti, L.; Keller, M.J.; Herold, B.C.; Shattock, R.J. Candidate microbicide PPCM blocks human immunodeficiency virus type 1 infection in cell and tissue cultures and prevents genital herpes in a murine model. J. Virol. 2008, 82, 6576–6584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fichorova, R.N.; Tucker, L.D.; Anderson, D.J. The molecular basis of nonoxynol-9-induced vaginal inflammation and its possible relevance to human immunodeficiency virus type 1 transmission. J. Infect. Dis. 2001, 184, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Agrahari, V.; Putty, S.; Mathes, C.; Murowchick, J.B.; Youan, B.B. Evaluation of degradation kinetics and physicochemical stability of tenofovir. Drug Test. Anal. 2015, 7, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Golla, V.M.; Kurmi, M.; Shaik, K.; Singh, S. Stability behaviour of antiretroviral drugs and their combinations. 4: Characterization of degradation products of tenofovir alafenamide fumarate and comparison of its degradation and stability behaviour with tenofovir disoproxil fumarate. J. Pharm. Biomed. Anal. 2016, 131, 146–155. [Google Scholar] [CrossRef]
- Delahunty, T.; Bushman, L.; Robbins, B.; Fletcher, C.V. The simultaneous assay of tenofovir and emtricitabine in plasma using LC/MS/MS and isotopically labeled internal standards. J. Chromatogr. B 2009, 877, 1907–1914. [Google Scholar] [CrossRef] [Green Version]
- Haaland, R.E.; Fountain, J.; Dinh, C.; Lupo, L.D.; Martin, A.; Conway-Washington, C.; Hall, L.; Kelley, C.F.; Garcia-Lerma, J.G.; Heneine, W. Antiretroviral drug exposure in urethral and glans surface sampling of the penis. J. Antimicrob. Chemother. 2021, 76, 2368–2374. [Google Scholar] [CrossRef]
- Berry, N.; Herrera, C.; Cranage, M. Detection, quantification, and characterisation of HIV/SIV. Methods Mol. Biol. 2011, 665, 133–160. [Google Scholar] [CrossRef]
- Grivel, J.C.; Margolis, L. Use of human tissue explants to study human infectious agents. Nat. Protoc. 2009, 4, 256–269. [Google Scholar] [CrossRef]
- Introini, A.; Vanpouille, C.; Grivel, J.C.; Margolis, L. An ex vivo Model of HIV-1 Infection in Human Lymphoid Tissue and Cervico-vaginal Tissue. Bio-Protocol 2014, 4, e1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arakelyan, A.; Fitzgerald, W.; Grivel, J.C.; Vanpouille, C.; Margolis, L. Histocultures (tissue explants) in human retrovirology. Methods Mol. Biol. 2014, 1087, 233–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, P.S.; Elliott, J.; Grivel, J.C.; Margolis, L.; Anton, P.; McGowan, I.; Shattock, R.J. Ex vivo culture of human colorectal tissue for the evaluation of candidate microbicides. AIDS 2006, 20, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Herrera, C.; McRaven, M.D.; Laing, K.G.; Dennis, J.; Hope, T.J.; Shattock, R.J. Early Colorectal Responses to HIV-1 and Modulation by Antiretroviral Drugs. Vaccines 2021, 9, 231. [Google Scholar] [CrossRef]
- Calenda, G.; Villegas, G.; Reis, A.; Millen, L.; Barnable, P.; Mamkina, L.; Kumar, N.; Roberts, K.; Kalir, T.; Martinelli, E.; et al. Mucosal Susceptibility to Human Immunodeficiency Virus Infection in the Proliferative and Secretory Phases of the Menstrual Cycle. AIDS Res. Hum. Retrovir. 2019, 35, 335–347. [Google Scholar] [CrossRef]
- Saba, E.; Origoni, M.; Taccagni, G.; Ferrari, D.; Doglioni, C.; Nava, A.; Lisco, A.; Grivel, J.C.; Margolis, L.; Poli, G. Productive HIV-1 infection of human cervical tissue ex vivo is associated with the secretory phase of the menstrual cycle. Mucosal Immunol. 2013, 6, 1081–1090. [Google Scholar] [CrossRef]
- Nicol, M.R.; Brewers, L.M.; Kashuba, A.D.M.; Sykes, C. The role of menopause in tenofovir diphosphate and emtricitabine triphosphate concentrations in cervical tissue. AIDS 2018, 32, 11–15. [Google Scholar] [CrossRef]
- Fahrbach, K.M.; Barry, S.M.; Anderson, M.R.; Hope, T.J. Enhanced cellular responses and environmental sampling within inner foreskin explants: Implications for the foreskin’s role in HIV transmission. Mucosal Immunol. 2010, 3, 410–418. [Google Scholar] [CrossRef]
- Penn, M.L.; Grivel, J.C.; Schramm, B.; Goldsmith, M.A.; Margolis, L. CXCR4 utilization is sufficient to trigger CD4+ T cell depletion in HIV-1-infected human lymphoid tissue. Proc. Natl. Acad. Sci. USA 1999, 96, 663–668. [Google Scholar] [CrossRef] [Green Version]
- Herrera, C.; Shattock, R.J. Candidate microbicides and their mechanisms of action. Curr. Top. Microbiol. Immunol. 2014, 383, 1–25. [Google Scholar]
- Anton, P.A.; Cranston, R.D.; Kashuba, A.; Hendrix, C.W.; Bumpus, N.N.; Richardson-Harman, N.; Elliott, J.; Janocko, L.; Khanukhova, E.; Dennis, R.; et al. RMP-02/MTN-006: A phase 1 rectal safety, acceptability, pharmacokinetic, and pharmacodynamic study of tenofovir 1% gel compared with oral tenofovir disoproxil fumarate. AIDS Res. Hum. Retrovir. 2012, 28, 1412–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, J.; Tiraboschi, J.M.; Herrera, C.; Else, L.; Egan, D.; Dickinson, L.; Jackson, A.; Olejniczak, N.; Back, D.; Khoo, S.; et al. Brief Report: Pharmacokinetic/Pharmacodynamic Investigation of Single-Dose Oral Maraviroc in the Context of HIV-1 Pre-exposure Prophylaxis. J. Acquir. Immune Defic. Syndr. 2016, 73, 252–257. [Google Scholar] [CrossRef] [PubMed]
- McGowan, I.; Cranston, R.D.; Duffill, K.; Siegel, A.; Engstrom, J.C.; Nikiforov, A.; Jacobson, C.; Rehman, K.K.; Elliott, J.; Khanukhova, E.; et al. A Phase 1 Randomized, Open Label, Rectal Safety, Acceptability, Pharmacokinetic, and Pharmacodynamic Study of Three Formulations of Tenofovir 1% Gel (the CHARM-01 Study). PLoS ONE 2015, 10, e0125363. [Google Scholar] [CrossRef] [PubMed]
- Richardson-Harman, N.; Hendrix, C.W.; Bumpus, N.N.; Mauck, C.; Cranston, R.D.; Yang, K.; Elliott, J.; Tanner, K.; McGowan, I.; Kashuba, A.; et al. Correlation between compartmental tenofovir concentrations and an ex vivo rectal biopsy model of tissue infectibility in the RMP-02/MTN-006 phase 1 study. PLoS ONE 2014, 9, e111507. [Google Scholar]
- Richardson-Harman, N.; Mauck, C.; McGowan, I.; Anton, P. Dose-response relationship between tissue concentrations of UC781 and explant infectibility with HIV type 1 in the RMP-01 rectal safety study. AIDS Res. Hum. Retrovir. 2012, 28, 1422–1433. [Google Scholar] [CrossRef] [PubMed]
- Herrera, C.; Lwanga, J.; Lee, M.; Mantori, S.; Amara, A.; Else, L.; Penchala, S.D.; Egan, D.; Challenger, E.; Dickinson, L.; et al. Pharmacokinetic/pharmacodynamic investigation of raltegravir with or without lamivudine in the context of HIV-1 pre-exposure prophylaxis (PrEP). J. Antimicrob. Chemother. 2021, 76, 2129–2136. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.A.; Panther, L.; Marzinke, M.A.; Hendrix, C.W.; Hoesley, C.J.; van der Straten, A.; Husnik, M.J.; Soto-Torres, L.; Nel, A.; Johnson, S.; et al. Phase 1 Safety, Pharmacokinetics, and Pharmacodynamics of Dapivirine and Maraviroc Vaginal Rings: A Double-Blind Randomized Trial. J. Acquir. Immune Defic. Syndr. 2015, 70, 242–249. [Google Scholar] [CrossRef] [Green Version]
- McGowan, I.; Dezzutti, C.S.; Siegel, A.; Engstrom, J.; Nikiforov, A.; Duffill, K.; Shetler, C.; Richardson-Harman, N.; Abebe, K.; Back, D.; et al. Long-acting rilpivirine as potential pre-exposure prophylaxis for HIV-1 prevention (the MWRI-01 study): An open-label, phase 1, compartmental, pharmacokinetic and pharmacodynamic assessment. Lancet HIV 2016, 3, e569–e578. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.A.; Marzinke, M.A.; Bakshi, R.P.; Fuchs, E.J.; Radebaugh, C.L.; Aung, W.; Spiegel, H.M.; Coleman, J.S.; Rohan, L.C.; Hendrix, C.W. Comparison of Dapivirine Vaginal Gel and Film Formulation Pharmacokinetics and Pharmacodynamics (FAME 02B). AIDS Res. Hum. Retrovir. 2017, 33, 339–346. [Google Scholar] [CrossRef]
- Fonsart, J.; Saragosti, S.; Taouk, M.; Peytavin, G.; Bushman, L.; Charreau, I.; Hance, A.; Goldwirt, L.; Morel, S.; Mammano, F.; et al. Single-dose pharmacokinetics and pharmacodynamics of oral tenofovir and emtricitabine in blood, saliva and rectal tissue: A sub-study of the ANRS IPERGAY trial. J. Antimicrob. Chemother. 2017, 72, 478–485. [Google Scholar] [CrossRef]
- Sekabira, R.; McGowan, I.; Yuhas, K.; Brand, R.M.; Marzinke, M.A.; Manabe, Y.C.; Frank, I.; Eron, J.; Landovitz, R.J.; Anton, P.; et al. Higher colorectal tissue HIV infectivity in cisgender women compared with MSM before and during oral preexposure prophylaxis. AIDS 2021, 35, 1585–1595. [Google Scholar] [CrossRef] [PubMed]
- McGowan, I.; Wilkin, T.; Landovitz, R.J.; Wu, C.; Chen, Y.; Marzinke, M.A.; Hendrix, C.W.; Richardson, P.; Eshleman, S.H.; Andrade, A.; et al. The pharmacokinetics, pharmacodynamics, and mucosal responses to maraviroc-containing pre-exposure prophylaxis regimens in MSM. AIDS 2019, 33, 237–246. [Google Scholar] [CrossRef] [PubMed]
- McGowan, I.M.; Kunjara Na Ayudhya, R.P.; Brand, R.M.; Marzinke, M.A.; Hendrix, C.W.; Johnson, S.; Piper, J.; Holtz, T.H.; Curlin, M.E.; Chitwarakorn, A.; et al. An Open-Label Pharmacokinetic and Pharmacodynamic Assessment of Tenofovir Gel and Oral Emtricitabine/Tenofovir Disoproxil Fumarate. AIDS Res. Hum. Retrovir. 2022, 38, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Leyva, F.; Fuchs, E.J.; Bakshi, R.; Carballo-Dieguez, A.; Ventuneac, A.; Yue, C.; Caffo, B.; Du, Y.; Torbenson, M.; Li, L.; et al. Simultaneous Evaluation of Safety, Acceptability, Pericoital Kinetics, and Ex Vivo Pharmacodynamics Comparing Four Rectal Microbicide Vehicle Candidates. AIDS Res. Hum. Retrovir. 2015, 31, 1089–1097. [Google Scholar] [CrossRef] [Green Version]
- Anton, P.A.; Saunders, T.; Elliott, J.; Khanukhova, E.; Dennis, R.; Adler, A.; Cortina, G.; Tanner, K.; Boscardin, J.; Cumberland, W.G.; et al. First phase 1 double-blind, placebo-controlled, randomized rectal microbicide trial using UC781 gel with a novel index of ex vivo efficacy. PLoS ONE 2011, 6, e23243. [Google Scholar] [CrossRef] [Green Version]
- Richardson-Harman, N.; Lackman-Smith, C.; Fletcher, P.S.; Anton, P.A.; Bremer, J.W.; Dezzutti, C.S.; Elliott, J.; Grivel, J.C.; Guenthner, P.; Gupta, P.; et al. Multisite comparison of anti-human immunodeficiency virus microbicide activity in explant assays using a novel endpoint analysis. J. Clin. Microbiol. 2009, 47, 3530–3539. [Google Scholar] [CrossRef] [Green Version]
- Herrera, C.; Cottrell, M.L.; Prybylski, J.; Kashuba, A.D.M.; Veazey, R.S.; García-Pérez, J.; Olejniczak, N.; McCoy, C.F.; Ziprin, P.; Richardson-Harman, N.; et al. The ex vivo pharmacology of HIV-1 antiretrovirals differs between macaques and humans. iScience 2022, 25, 104409. [Google Scholar] [CrossRef]
- Abraha, A.; Nankya, I.L.; Gibson, R.; Demers, K.; Tebit, D.M.; Johnston, E.; Katzenstein, D.; Siddiqui, A.; Herrera, C.; Fischetti, L.; et al. CCR5- and CXCR4-tropic subtype C human immunodeficiency virus type 1 isolates have a lower level of pathogenic fitness than other dominant group M subtypes: Implications for the epidemic. J. Virol. 2009, 83, 5592–5605. [Google Scholar] [CrossRef] [Green Version]
- Dinh, M.H.; Anderson, M.R.; McRaven, M.D.; Cianci, G.C.; McCoombe, S.G.; Kelley, Z.L.; Gioia, C.J.; Fought, A.J.; Rademaker, A.W.; Veazey, R.S.; et al. Visualization of HIV-1 interactions with penile and foreskin epithelia: Clues for female-to-male HIV transmission. PLoS Pathog. 2015, 11, e1004729. [Google Scholar] [CrossRef]
- Hladik, F.; Hope, T.J. HIV infection of the genital mucosa in women. Curr. HIV/AIDS Rep. 2009, 6, 20–28. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}