
Phase I Clinical Trial Using [99mTc]Tc-1-thio-D-glucose for Diagnosis of Lymphoma Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiopharmaceutical
2.3. Imaging Protocol
2.4. Evaluation of Distribution and Dosimetry
2.5. Statistics
3. Results
3.1. Safety and Tolerability
3.2. Evaluation of Distribution and Dosimetry
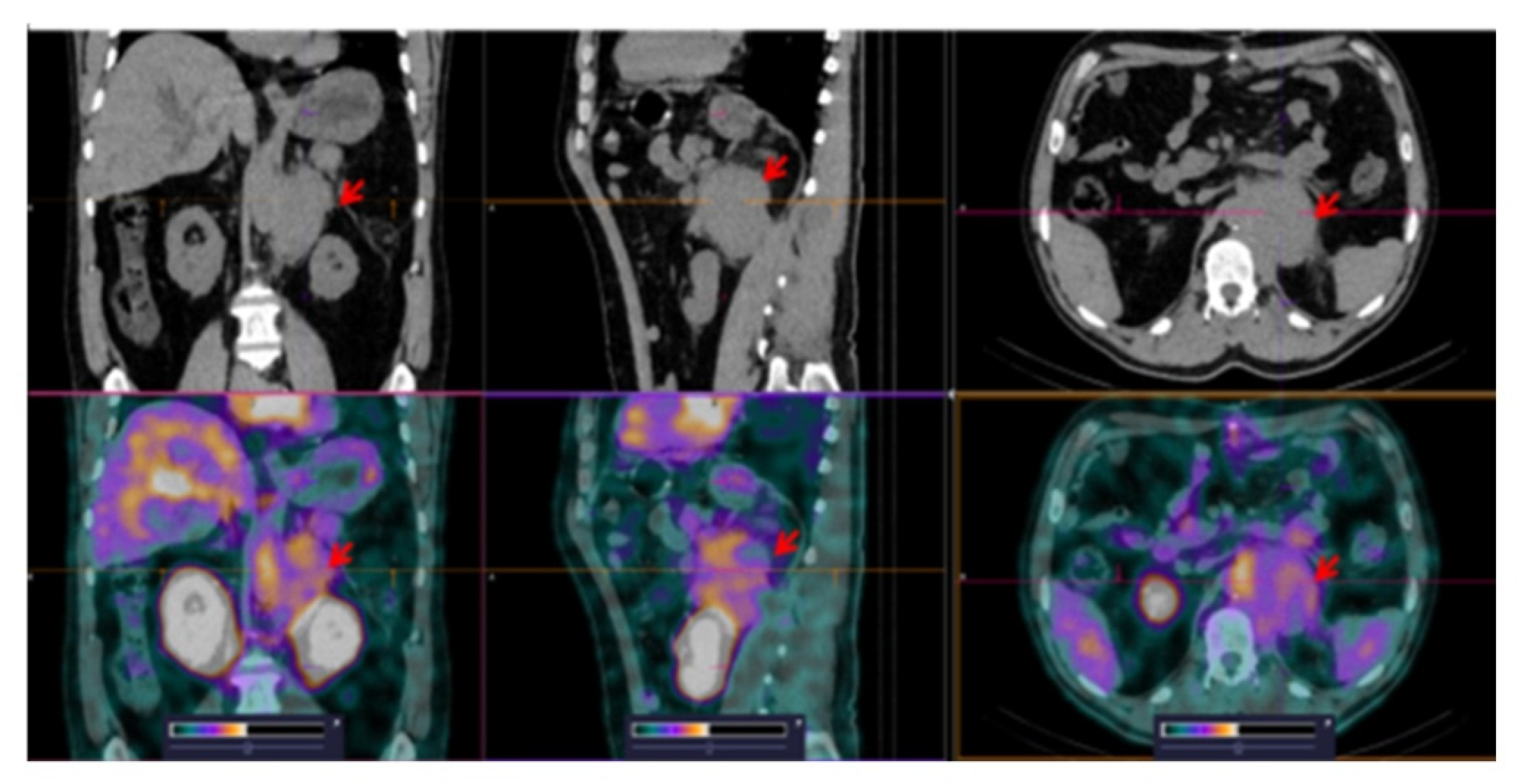
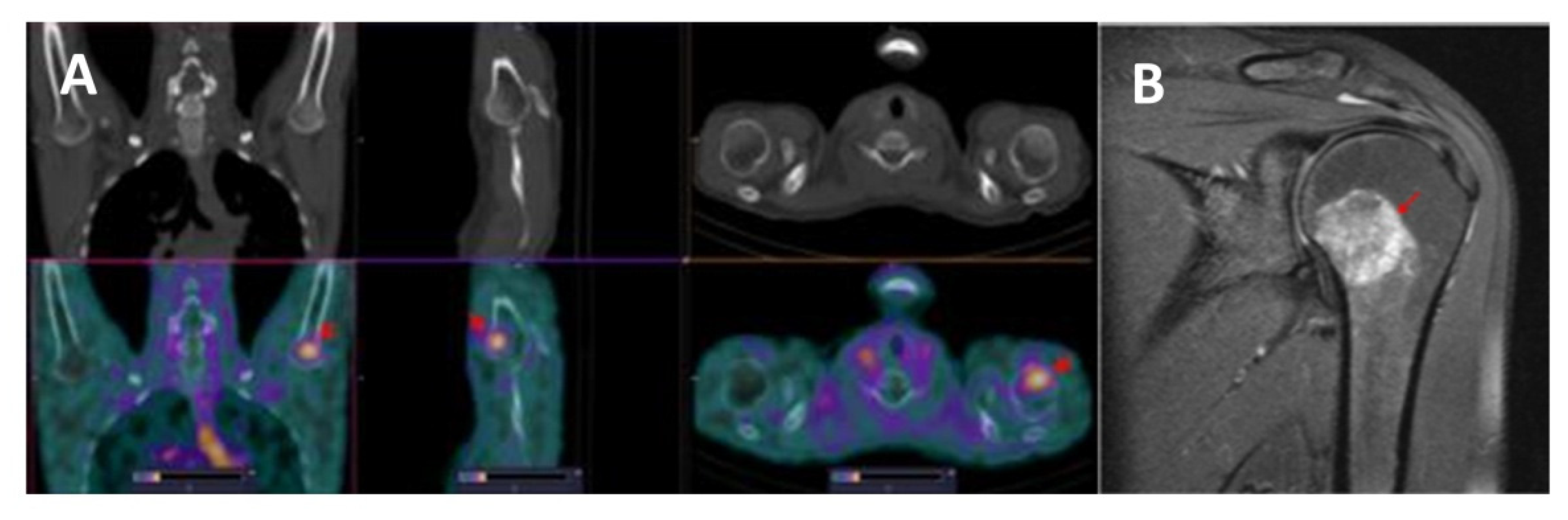
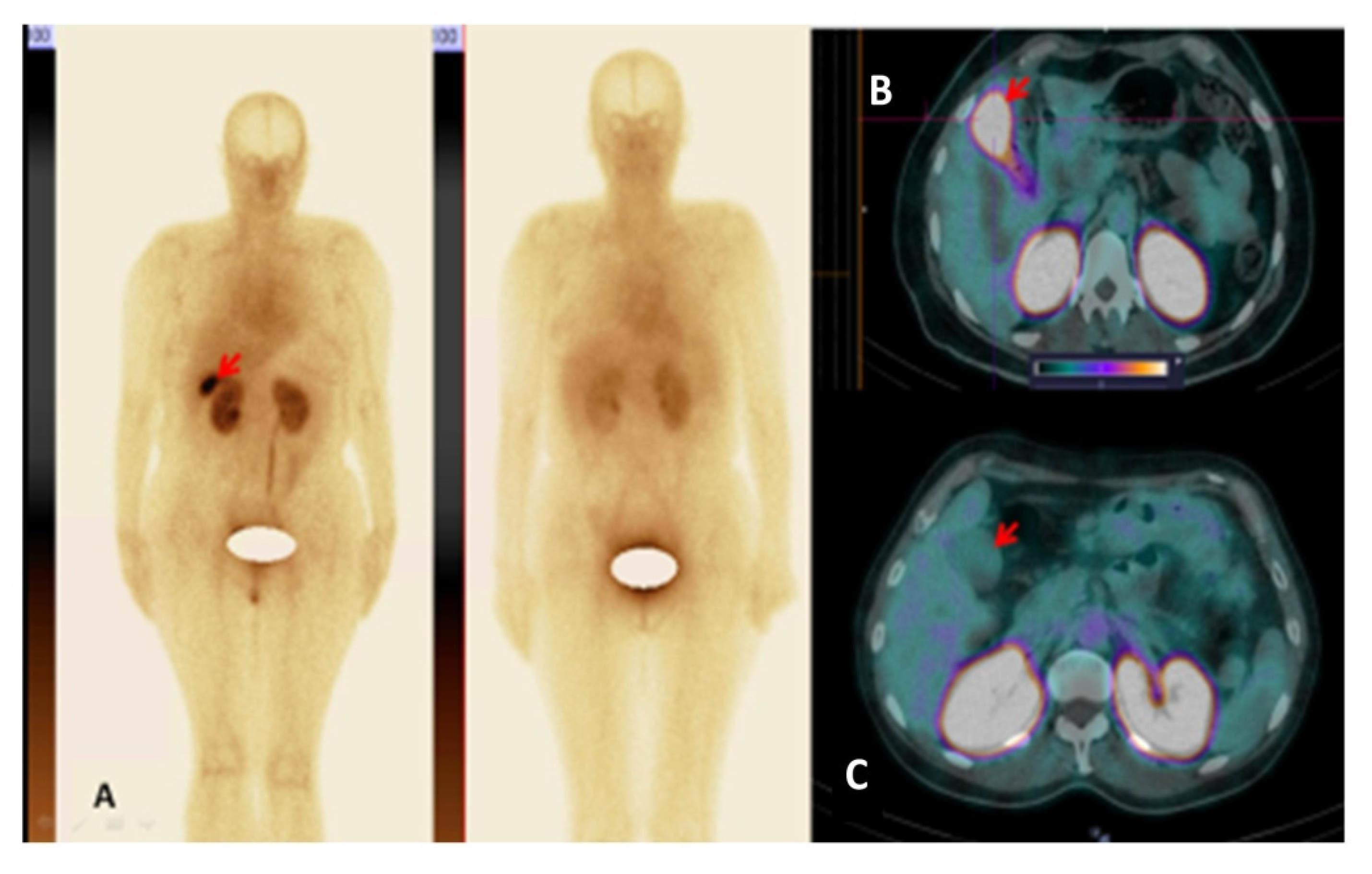
3.3. [99mTc]Tc-TG SPECT/CT Imaging of Nodal and Extranodal Lesions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, stag-ing, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Jun Oh, S.; Ryu, J.S.; Yoon, E.J.; Bae, M.S.; Choi, S.J.; Park, K.B.; Moon, D.H. 99mTc-labeled 1-thio-beta-D-glucose as a new tumor-seeking agent: Synthesis and tumor cell uptake assay. Appl. Radiat. Isot. 2006, 64, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Seidensticker, M.; Ulrich, G.; Muehlberg, F.L.; Pethe, A.; Grosser, O.S.; Steffen, I.G.; Stiebler, M.; Goldschmidt, J.; Smalla, K.H.; Seidensticker, R.; et al. Tumor cell uptake of 99mTc-labeled 1-thio-β-D-glucose and 5-Thio-D-glucose in comparison with 2-Deoxy-2-[18F]fluoro-D-glucose in vitro: Kinetics, dependencies, blockage and cell compartment of accumulation. Mol. Imaging Biol. 2014, 16, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Dapueto, R.; Aguiar, R.; Moreno, M.; Machado, C.M.; Marques, F.; Gambini, J.P.; Chammas, R.; Cabral, P.; Porcal, W. Technetium glucose complexes as potential cancer imaging agents. Bioorganic Med. Chem. Lett. 2015, 25, 4254–4259. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ruan, Q.; Duan, X.; Gan, Q.; Song, X.; Fang, S.; Lin, X.; Du, J.; Zhang, J. Novel 99mTc-labeled glucose derivative for single photon emission computed tomography: A promising tumor imaging agent. Mol. Pharm. 2018, 15, 3417–3424. [Google Scholar] [CrossRef] [PubMed]
- Gan, Q.; Zhang, X.; Ruan, Q.; Fang, S.; Zhang, J. 99mTc-CN7DG: A highly expected SPECT imaging agent of cancer with satisfactory tumor uptake and tumor-to-nontarget ratios. Mol. Pharm. 2021, 18, 1356–1363. [Google Scholar] [CrossRef]
- Ong, L.-C.; Jin, Y.; Song, I.-C.; Yu, S.; Zhang, K. 2-[18f]-2-deoxy-d-glucose (fdg) uptake in human tumor cells is related to the expression of glut-1 and hexokinase ii. Acta Radiol. 2008, 49, 1145–1153. [Google Scholar] [CrossRef]
- Guo, G.F.; Cai, Y.C.; Zhang, B.; Xu, R.H.; Qiu, H.J.; Xia, L.P.; Jiang, W.Q.; Hu, P.L.; Chen, X.X.; Zhou, F.F.; et al. Overexpression of SGLT1 and EGFR in colorectal cancer showing a correlation with the prognosis. Med. Oncol. 2011, 28 (Suppl. S1), 197–203. [Google Scholar] [CrossRef]
- Huber, S.M.; Misovic, M.; Mayer, C.; Rodemann, H.-P.; Dittmann, K. EGFR-mediated stimulation of sodium/glucose cotransport promotes survival of irradiated human A549 lung adenocarcinoma cells. Radiother. Oncol. 2012, 103, 373–379. [Google Scholar] [CrossRef]
- Stasyuk, E.; Sкuridin, V.; Rogov, A.; Zelchan, R.; Sadkin, V.; Varlamova, N.; Nesterov, E. 99mTc-labeled monosaccharide kits: Development methods and quality control. Sci. Rep. 2020, 10, 5121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeltchan, R.; Medvedeva, A.; Sinilkin, I.; Chernov, V.; Stasyuk, E.; Rogov, A.; Il’Ina, E.; Larionova, L.; Skuridin, V. Study of potential utility of new radiopharmaceuticals based on technetium-99m labeled derivative of glucose. AIP Conf. Proc. 2016, 1760, 020072. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.; Kwee, T.C. Value of detecting bone marrow involvement in Hodgkin lymphoma. Br. J. Haematol. 2019, 187, 397–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Wang, X.; Zhang, L.; Yi, X.; Qiao, Y.; Jin, Q. Correlations between maximum standardized uptake value measured via 18F-fluorodeoxyglucose positron emission tomography/computed tomography and clinical variables and biochemical indicators in adult lymphoma. J. Cancer Res. Ther. 2019, 15, 1581–1588. [Google Scholar] [CrossRef] [PubMed]
- Meller, J.; Sahlmann, C.-O.; Scheel, A.K. 18F-FDG PET and PET/CT in fever of unknown origin. J. Nucl. Med. 2007, 48, 35–45. [Google Scholar]
- Yu, J.Q.; Kung, J.W.; Potenta, S.; Xiu, Y.; Alavi, A.; Zhuang, H. Chronic Cholecystitis Detected by FDG-PET. Clin. Nucl. Med. 2004, 29, 496–497. [Google Scholar] [CrossRef]
- Kitazono, M.T.; Colletti, P.M. FDG PET Imaging of Acute Cholecystitis. Clin. Nucl. Med. 2006, 31, 23–24. [Google Scholar] [CrossRef]
- Nasseri, Y.; Ourian, A.J.; Waxman, A.; D’Angolo, A.; Thomson, L.E.; Margulies, D.R. Fluorodeoxyglucose Positron Emission Tomography–Computed Tomography: A Novel Approach for the Diagnosis of Cholecystitis for Equivocal Diagnoses after Ultrasound Imaging. Am. Surg. 2012, 78, 1109–1113. [Google Scholar] [CrossRef]
- Pilkington, P.; Lopci, E.; Adam, J.A.; Kobe, C.; Goffin, K.; Herrmann, K. FDG-PET/CT Variants and Pitfalls in Haematological Malignancies. Semin. Nucl. Med. 2021, 51, 554–571. [Google Scholar] [CrossRef]
- Kobe, C.; Dietlein, M.; Hellwig, D. PET/CT for Lymphoma Post-therapy Response Assessment in Hodgkin Lymphoma and Diffuse Large B-cell Lymphoma. Semin. Nucl. Med. 2018, 48, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Karls, S.; Shah, H.; Jacene, H. PET/CT for Lymphoma Post-therapy Response Assessment in Other Lymphomas, Response Assessment for Autologous Stem Cell Transplant, and Lymphoma Follow-up. Semin. Nucl. Med. 2018, 48, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Patching, S.G. Glucose Transporters at the Blood-Brain Barrier: Function, Regulation and Gateways for Drug Delivery. Mol. Neurobiol. 2016, 54, 1046–1077. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No | Sex | Age (y) | IHC Diagnosis | Stage |
|---|---|---|---|---|
| 1 | Male | 62 | FL | IVA |
| 2 | Male | 39 | HL | IVA |
| 3 | Female | 20 | HL | IIIB |
| 4 | Female | 57 | DLBCL | IVB |
| 5 | Female | 49 | MALT-lymphoma | IIIB |
| 6 | Female | 56 | BLL | IVA |
| 7 | Male | 58 | FL | IVA |
| 8 | Female | 45 | HL | IIA |
| 9 | Male | 68 | DLBCL | IVA |
| 10 | Female | 39 | MZL | IVA |
| 11 | Female | 34 | HL | IIIB * |
| 12 | Female | 61 | DLBCL | IVA |
| Time | Kidney | Liver | Lung | |||
|---|---|---|---|---|---|---|
| Female | Male | Female | Male | Female | Male | |
| 2 h | 5.6 ± 2.7 | 4.0 ± 0.7 | 3.5 ± 1.1 | 3.4 ± 1.0 | 4.0 ± 1.5 | 4.6 ± 1.1 |
| 4 h | 6.5 ± 3.5 | 4.3 ± 0.9 | 3.6 ± 0.8 | 3.2 ± 0.8 | 4.5 ± 2.1 | 4.0 ± 0.9 |
| 6 h | 5.9 ± 3.1 | 3.7 ± 1.3 | 3.9 ± 1.2 | 2.5 ± 0.8 | 3.7 ± 1.2 | 3.1 ± 1.1 |
| 24 h | 7.1 ± 3.7 | 4.5 ± 2.1 | 2.9 ± 1.1 | 2.6 ± 0.5 | 2.7 ± 1.0 | 2.5 ± 0.5 |
| Site | Female Patients | Male Patients |
|---|---|---|
| Testes | 0.01 ± 0.01 | |
| Brain | 0.0017 ± 0.0006 | 0.0012 ± 0.0003 |
| Breasts | 0.002 ± 0.001 | 0.0011 ± 0.0002 |
| Skin | 0.0019 ± 0.0007 | 0.0014 ± 0.0003 |
| Muscle | 0.003 ± 0.001 | 0.0021 ± 0.0005 |
| Red Marrow | 0.003 ± 0.001 | 0.0026 ± 0.0005 |
| Stomach Wall | 0.004 ± 0.001 | 0.0028 ± 0.0005 |
| Small Intestine | 0.005 ± 0.002 | 0.0042 ± 0.0009 |
| LLI Wall | 0.005 ± 0.003 | 0.005 ± 0.003 |
| Thymus | 0.005 ± 0.002 | 0.005 ± 0.001 |
| Thyroid | 0.005 ± 0.002 | 0.004 ± 0.001 |
| Spleen | 0.005 ± 0.002 | 0.0032 ± 0.0006 |
| Pancreas | 0.005 ± 0.002 | 0.0033 ± 0.0004 |
| ULI Wall | 0.005 ± 0.002 | 0.0038 ± 0.0008 |
| Gallbladder Wall | 0.007 ± 0.003 | 0.005 ± 0.001 |
| Liver | 0.007 ± 0.002 | 0.004 ± 0.001 |
| Uterus | 0.007 ± 0.004 | |
| Ovaries | 0.007 ± 0.04 | |
| Heart Wall | 0.008 ± 0.003 | 0.006 ± 0.002 |
| Lungs | 0.008 ± 0.003 | 0.005 ± 0.001 |
| Osteogenic Cells | 0.008 ± 0.003 | 0.006 ± 0.001 |
| Adrenals | 0.009 ± 0.003 | 0.005 ± 0.001 |
| Kidneys | 0.03 ± 0.01 | 0.02 ± 0.01 |
| Urinary Bladder Wall | 0.03 ± 0.04 | 0.05 ± 0.05 |
| Prostate | 0.010 ± 0.006 | |
| Total Body | 0.004 ± 0.002 | 0.0028 ± 0.0005 |
| Effective Dose Equivalent (mSv/MBq) | 0.009 ± 0.005 | 0.02 ± 0.01 |
| Effective Dose (mSv/MBq) | 0.007 ± 0.004 | 0.014 ± 0.009 |
| Patients | Tumor Size cm | SUVmax Tumor | SUVmax Gallbladder | Tumor/ Background 2 h | Tumor/ Background 4 h | Tumor/ Background 6 h |
|---|---|---|---|---|---|---|
| 1. | 8.0 | 3.92 | 4.2 | 4.1 | 4.2 | 2.7 |
| 2. | 1.8 | 2.23 | 7.1 | 2.5 | 1.6 | 1.4 |
| 3. | 12.0 | 1.3 | - | 2.5 | 1.6 | 1.8 |
| 4. | 3.8 | 4.53 | 2.9 | 1.7 | 1.9 | 1.9 |
| 5. | 3.6 | 3.39 | 20.9 | 3.5 | 1.4 | 1.3 |
| 6. | 4.6 | 3.34 | 4.2 | 3.6 | 1.6 | 1.7 |
| 7. | 5.0 | 2.45 | - | 2.5 | 1.7 | 1.6 |
| 8. | 4.5 | 1.43 | - | 3.8 | 2.5 | 2.8 |
| 9. | 2.8 | 1.89 | - | 2.8 | 1.3 | 1.48 |
| 10. | 8.3 | 1.21 | - | 2.9 | 1.7 | 3.2 |
| 11. | 4.2 | 2.28 | 3.5 | 6.3 | 5.8 | 4.2 |
| 12. | 4.6 | 2.65 | - | 21.9 | 18.3 | 16.1 |
| Mean ± SD | 5 ± 3 | 3 ± 1 | 4.4 ± 1.6 * | 3.3 ± 1.2 ** | 2.3 ± 1.4 ** p = 0.005 *** | 2.1 ± 0.9 ** p = 0.005 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chernov, V.; Dudnikova, E.; Zelchan, R.; Medvedeva, A.; Rybina, A.; Bragina, O.; Goldberg, V.; Muravleva, A.; Sörensen, J.; Tolmachev, V. Phase I Clinical Trial Using [99mTc]Tc-1-thio-D-glucose for Diagnosis of Lymphoma Patients. Pharmaceutics 2022, 14, 1274. https://doi.org/10.3390/pharmaceutics14061274
Chernov V, Dudnikova E, Zelchan R, Medvedeva A, Rybina A, Bragina O, Goldberg V, Muravleva A, Sörensen J, Tolmachev V. Phase I Clinical Trial Using [99mTc]Tc-1-thio-D-glucose for Diagnosis of Lymphoma Patients. Pharmaceutics. 2022; 14(6):1274. https://doi.org/10.3390/pharmaceutics14061274
Chicago/Turabian StyleChernov, Vladimir, Ekaterina Dudnikova, Roman Zelchan, Anna Medvedeva, Anstasiya Rybina, Olga Bragina, Viktor Goldberg, Albina Muravleva, Jens Sörensen, and Vladimir Tolmachev. 2022. "Phase I Clinical Trial Using [99mTc]Tc-1-thio-D-glucose for Diagnosis of Lymphoma Patients" Pharmaceutics 14, no. 6: 1274. https://doi.org/10.3390/pharmaceutics14061274