
Dose–Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Ethical Approval
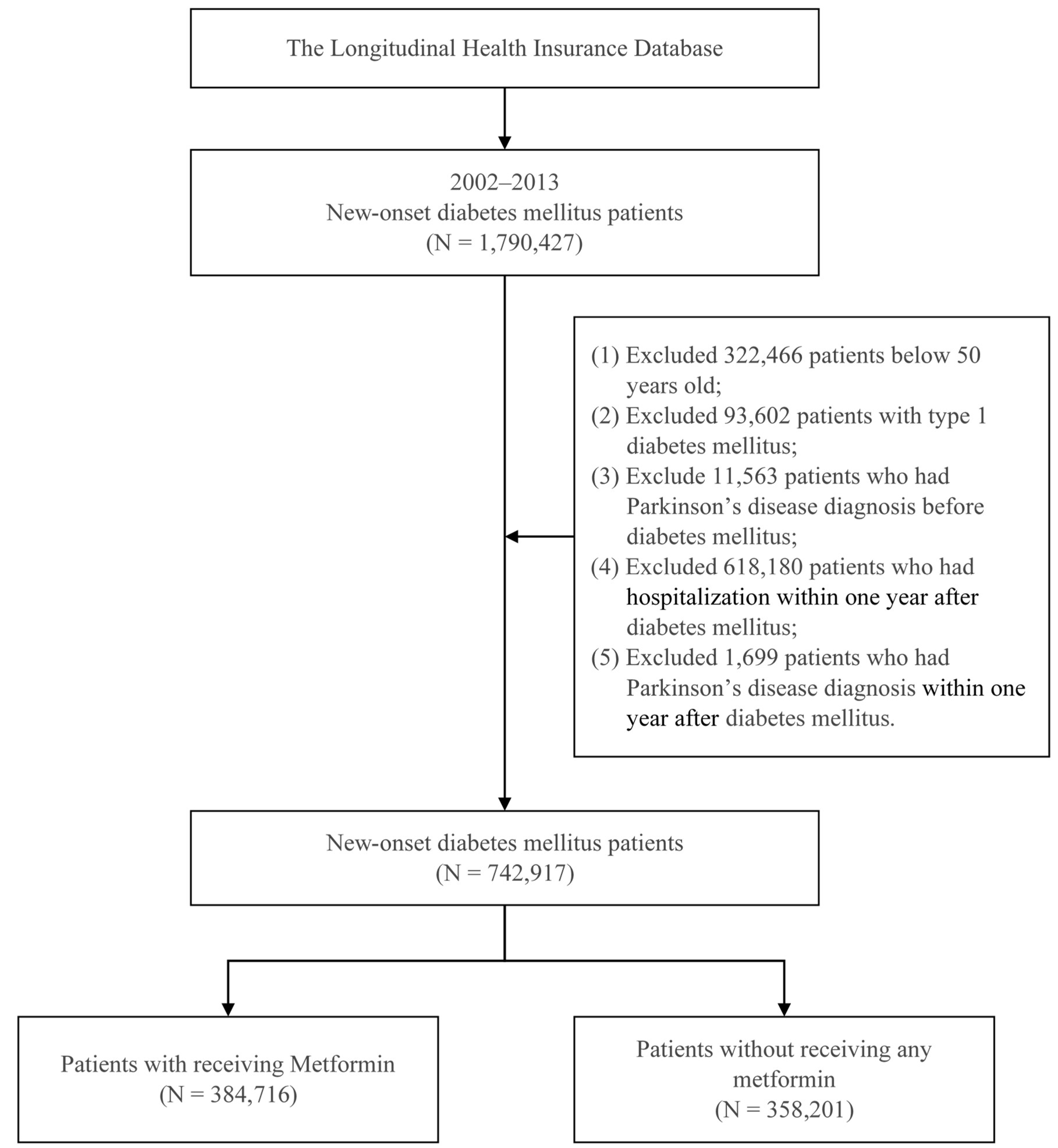
2.3. Study Sample
2.4. Study Design
2.5. Statistical Analyses
3. Results
3.1. Distribution of Patient Characteristics
3.2. Associations between PD and Metformin Use in Patients New-Onset T2DM—3-Year Follow-Up
3.3. Associations between PD and Metformin Use in Patients New-Onset T2DM—5-Year Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lima, M.M.; Targa, A.D.S.; Noseda, A.C.D.; Rodrigues, L.S.; Marcia Delattre, A.; dos Santos, F.V.; Fortes, M.H.; Maturana, M.J.; Ferraz, A.C. Does Parkinson’s disease and type-2 diabetes mellitus present common pathophysiological mechanisms and treatments? CNS Neurol. Disord. Drug Targets 2014, 13, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.A.; Obeso, J.A. Clinical and pathological features of Parkinson’s disease. Curr. Top. Behav. Neurosci. 2015, 22, 205–220. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H. Etiology and pathogenesis of Parkinson disease. Neurol. Clin. 2009, 27, 583–603. [Google Scholar] [CrossRef] [PubMed]
- Ping, F.; Jiang, N.; Li, Y. Association between metformin and neurodegenerative diseases of observational studies: Systematic review and meta-analysis. BMJ Open Diabetes Res. Care 2020, 8, e001370. [Google Scholar] [CrossRef]
- Cheong, J.L.Y.; de Pablo-Fernandez, E.; Foltynie, T.; Noyce, A.J. The Association between Type 2 Diabetes Mellitus and Parkinson’s Disease. J. Parkinsons Dis. 2020, 10, 775–789. [Google Scholar] [CrossRef] [Green Version]
- Hu, G.; Jousilahti, P.; Bidel, S.; Antikainen, R.; Tuomilehto, J. Type 2 diabetes and the risk of Parkinson’s disease. Diabetes Care 2007, 30, 842–847. [Google Scholar] [CrossRef] [Green Version]
- Soukas, A.A.; Hao, H.; Wu, L. Metformin as Anti-Aging Therapy: Is It for Everyone? Trends Endocrinol. Metab. 2019, 30, 745–755. [Google Scholar] [CrossRef]
- Han, J.; Li, Y.; Liu, X.; Zhou, T.; Sun, H.; Edwards, P.; Gao, H.; Yu, F.S.; Qiao, X. Metformin suppresses retinal angiogenesis and inflammation in vitro and in vivo. PLoS ONE 2018, 13, e0193031. [Google Scholar] [CrossRef] [Green Version]
- Ahuja, S.; Uniyal, A.; Akhtar, A.; Sah, S.P. Alpha lipoic acid and metformin alleviates experimentally induced insulin resistance and cognitive deficit by modulation of TLR2 signalling. Pharmacol. Rep. 2019, 71, 614–623. [Google Scholar] [CrossRef]
- Rotermund, C.; Machetanz, G.; Fitzgerald, J.C. The Therapeutic Potential of Metformin in Neurodegenerative Diseases. Front. Endocrinol. 2018, 9, 400. [Google Scholar] [CrossRef]
- Vicente Miranda, H.; El-Agnaf, O.M.; Outeiro, T.F. Glycation in Parkinson’s disease and Alzheimer’s disease. Mov. Disord. 2016, 31, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Koenig, A.M.; Mechanic-Hamilton, D.; Xie, S.X.; Combs, M.F.; Cappola, A.R.; Xie, L.; Detre, J.A.; Wolk, D.A.; Arnold, S.E. Effects of the Insulin Sensitizer Metformin in Alzheimer Disease: Pilot Data From a Randomized Placebo-controlled Crossover Study. Alzheimer Dis. Assoc. Disord. 2017, 31, 107–113. [Google Scholar] [CrossRef]
- Jiang, P.; Gan, M.; Ebrahim, A.S.; Castanedes-Casey, M.; Dickson, D.W.; Yen, S.H. Adenosine monophosphate-activated protein kinase overactivation leads to accumulation of alpha-synuclein oligomers and decrease of neurites. Neurobiol. Aging 2013, 34, 1504–1515. [Google Scholar] [CrossRef] [Green Version]
- Stephenne, X.; Foretz, M.; Taleux, N.; van der Zon, G.C.; Sokal, E.; Hue, L.; Viollet, B.; Guigas, B. Metformin activates AMP-activated protein kinase in primary human hepatocytes by decreasing cellular energy status. Diabetologia 2011, 54, 3101–3110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picone, P.; Nuzzo, D.; Caruana, L.; Messina, E.; Barera, A.; Vasto, S.; Di Carlo, M. Metformin increases APP expression and processing via oxidative stress, mitochondrial dysfunction and NF-kappaB activation: Use of insulin to attenuate metformin’s effect. Biochim. Biophys. Acta 2015, 1853, 1046–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Zhou, K.; Wang, R.; Liu, Y.; Kwak, Y.D.; Ma, T.; Thompson, R.C.; Zhao, Y.; Smith, L.; Gasparini, L.; et al. Antidiabetic drug metformin (GlucophageR) increases biogenesis of Alzheimer’s amyloid peptides via up-regulating BACE1 transcription. Proc. Natl. Acad. Sci. USA 2009, 106, 3907–3912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sridhar, G.R.; Lakshmi, G.; Nagamani, G. Emerging links between type 2 diabetes and Alzheimer’s disease. World J. Diabetes 2015, 6, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Khattar, D.; Khaliq, F.; Vaney, N.; Madhu, S.V. Is Metformin-Induced Vitamin B12 Deficiency Responsible for Cognitive Decline in Type 2 Diabetes? Indian J. Psychol. Med. 2016, 38, 285–290. [Google Scholar] [CrossRef] [Green Version]
- Hashem, M.M.; Esmael, A.; Nassar, A.K.; El-Sherif, M. The relationship between exacerbated diabetic peripheral neuropathy and metformin treatment in type 2 diabetes mellitus. Sci. Rep. 2021, 11, 1940. [Google Scholar] [CrossRef]
- Grimmsmann, T.; Himmel, W. Discrepancies between prescribed and defined daily doses: A matter of patients or drug classes? Eur. J. Clin. Pharmacol. 2011, 67, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Wellington, K. Rosiglitazone/Metformin. Drugs 2005, 65, 1581–1592; discussion 1584–1593. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, C.; Sheng, X.; Zhang, X.; Wang, B.; Zhang, G. Peripheral expression of MAPK pathways in Alzheimer’s and Parkinson’s diseases. J. Clin. Neurosci. 2014, 21, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Khang, R.; Park, C.; Shin, J.H. Dysregulation of parkin in the substantia nigra of db/db and high-fat diet mice. Neuroscience 2015, 294, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Katila, N.; Bhurtel, S.; Shadfar, S.; Srivastav, S.; Neupane, S.; Ojha, U.; Jeong, G.S.; Choi, D.Y. Metformin lowers alpha-synuclein phosphorylation and upregulates neurotrophic factor in the MPTP mouse model of Parkinson’s disease. Neuropharmacology 2017, 125, 396–407. [Google Scholar] [CrossRef] [PubMed]
- Marinangeli, C.; Didier, S.; Ahmed, T.; Caillerez, R.; Domise, M.; Laloux, C.; Begard, S.; Carrier, S.; Colin, M.; Marchetti, P.; et al. AMP-Activated Protein Kinase Is Essential for the Maintenance of Energy Levels during Synaptic Activation. iScience 2018, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Shi, Q.; Liu, S.; Fonseca, V.A.; Thethi, T.K.; Shi, L. Effect of metformin on neurodegenerative disease among elderly adult US veterans with type 2 diabetes mellitus. BMJ Open 2019, 9, e024954. [Google Scholar] [CrossRef] [Green Version]
- Mairet-Coello, G.; Courchet, J.; Pieraut, S.; Courchet, V.; Maximov, A.; Polleux, F. The CAMKK2-AMPK kinase pathway mediates the synaptotoxic effects of Abeta oligomers through Tau phosphorylation. Neuron 2013, 78, 94–108. [Google Scholar] [CrossRef] [Green Version]
- Hardie, D.G. Neither LKB1 nor AMPK are the direct targets of metformin. Gastroenterology 2006, 131, 973; author reply 974–975. [Google Scholar] [CrossRef]
- Wong, C.W.; Leung, C.S.; Leung, C.P.; Cheng, J.N. Association of metformin use with vitamin B12 deficiency in the institutionalized elderly. Arch Gerontol. Geriatr. 2018, 79, 57–62. [Google Scholar] [CrossRef]
- Chapman, L.E.; Darling, A.L.; Brown, J.E. Association between metformin and vitamin B12 deficiency in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2016, 42, 316–327. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, D.K.; Ismail, C.A.; Ghareeb, D.A. Differential metformin dose-dependent effects on cognition in rats: Role of Akt. Psychopharmacology 2016, 233, 2513–2524. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- Chang, H.Y.; Weiner, J.P.; Richards, T.M.; Bleich, S.N.; Segal, J.B. Validating the adapted Diabetes Complications Severity Index in claims data. Am. J. Manag. Care 2012, 18, 721–726. [Google Scholar]
- Chiu, W.C.; Ho, W.C.; Liao, D.L.; Lin, M.H.; Chiu, C.C.; Su, Y.P.; Chen, P.C. Health Data Analysis in Taiwan Research, G. Progress of Diabetic Severity and Risk of Dementia. J. Clin. Endocrinol. Metab. 2015, 100, 2899–2908. [Google Scholar] [CrossRef] [Green Version]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef]
- Collier, T.J.; Kanaan, N.M.; Kordower, J.H. Ageing as a primary risk factor for Parkinson’s disease: Evidence from studies of non-human primates. Nat. Rev. Neurosci. 2011, 12, 359–366. [Google Scholar] [CrossRef]
- Hindle, J.V. Ageing, neurodegeneration and Parkinson’s disease. Age Ageing 2010, 39, 156–161. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes, A. Standards of medical care in diabetes–2010. Diabetes Care 2010, 33 (Suppl. 1), S11–S61. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Shafiq, I.; Hassan Shah, M. Prevalence of Vitamin B12 Deficiency in Patients with Type II Diabetes Mellitus on Metformin: A Study from Khyber Pakhtunkhwa. Cureus 2017, 9, e1577. [Google Scholar] [CrossRef] [Green Version]
- Collaborators, G.B.D.P.s.D. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Kummer, B.R.; Diaz, I.; Wu, X.; Aaroe, A.E.; Chen, M.L.; Iadecola, C.; Kamel, H.; Navi, B.B. Associations between cerebrovascular risk factors and parkinson disease. Ann Neurol. 2019, 86, 572–581. [Google Scholar] [CrossRef]
- Ishihara, L.; Brayne, C. A systematic review of depression and mental illness preceding Parkinson’s disease. Acta Neurol. Scand. 2006, 113, 211–220. [Google Scholar] [CrossRef]
- Braak, H.; Ghebremedhin, E.; Rub, U.; Bratzke, H.; Del Tredici, K. Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 2004, 318, 121–134. [Google Scholar] [CrossRef]
- Lin, C.H.; Lin, J.W.; Liu, Y.C.; Chang, C.H.; Wu, R.M. Risk of Parkinson’s disease following anxiety disorders: A nationwide population-based cohort study. Eur. J. Neurol. 2015, 22, 1280–1287. [Google Scholar] [CrossRef]
- Fang, F.; Xu, Q.; Park, Y.; Huang, X.; Hollenbeck, A.; Blair, A.; Schatzkin, A.; Kamel, F.; Chen, H. Depression and the subsequent risk of Parkinson’s disease in the NIH-AARP Diet and Health Study. Mov. Disord. 2010, 25, 1157–1162. [Google Scholar] [CrossRef] [Green Version]
- Wirdefeldt, K.; Adami, H.O.; Cole, P.; Trichopoulos, D.; Mandel, J. Epidemiology and etiology of Parkinson’s disease: A review of the evidence. Eur. J. Epidemiol. 2011, 26 (Suppl. 1), S1–S58. [Google Scholar] [CrossRef]
- Li, C.H.; Chen, W.C.; Liao, W.C.; Tu, C.Y.; Lin, C.L.; Sung, F.C.; Chen, C.H.; Hsu, W.H. The association between chronic obstructive pulmonary disease and Parkinson’s disease: A nationwide population-based retrospective cohort study. QJM 2015, 108, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total | Metformin | |||||
|---|---|---|---|---|---|---|---|
| Non-Users | Users | p-Value | |||||
| N | % | N | % | N | % | ||
| Total | 742,917 | 100.00 | 358,201 | 48.22 | 384,716 | 51.78 | |
| Gender | <0.001 | ||||||
| Female | 382,065 | 51.43 | 189,612 | 52.93 | 192,453 | 50.02 | |
| Male | 360,852 | 48.57 | 168,589 | 47.07 | 192,263 | 49.98 | |
| Age (year) (Mean ± SD) | 62.17 ± 8.86 | 63.08 ± 9.18 | 61.32 ± 8.47 | <0.001 | |||
| 50–64 | 475,631 | 64.02 | 215,040 | 60.03 | 260,591 | 67.74 | |
| 65–74 | 183,801 | 24.74 | 93,963 | 26.23 | 89,838 | 23.35 | |
| ≥75 | 83,485 | 11.24 | 49,198 | 13.73 | 34,287 | 8.91 | |
| Income level (NTD) a | <0.001 | ||||||
| ≤21,000 | 385,214 | 51.85 | 189,933 | 53.02 | 195,281 | 50.76 | |
| 21,001–33,000 | 176,301 | 23.73 | 79,224 | 22.12 | 97,077 | 25.23 | |
| ≥33,001 | 181,402 | 24.42 | 89,044 | 24.86 | 92,358 | 24.01 | |
| Urbanization b | <0.001 | ||||||
| Level 1 | 205,119 | 27.61 | 104,737 | 29.24 | 100,382 | 26.09 | |
| Level 2 | 240,126 | 32.32 | 115,045 | 32.12 | 125,081 | 32.51 | |
| Level 3 | 115,321 | 15.52 | 52,993 | 14.79 | 62,328 | 16.20 | |
| Level 4 | 104,346 | 14.05 | 49,332 | 13.77 | 55,014 | 14.30 | |
| Level 5 | 17,554 | 2.36 | 8569 | 2.39 | 8985 | 2.34 | |
| Level 6 | 31,709 | 4.27 | 14,535 | 4.06 | 17,174 | 4.46 | |
| Level 7 | 28,742 | 3.87 | 12,990 | 3.63 | 15,752 | 4.09 | |
| DCSI score c | <0.001 | ||||||
| 0 | 449,726 | 60.54 | 212,961 | 59.45 | 236,765 | 61.54 | |
| 1 | 158,619 | 21.35 | 76,184 | 21.27 | 82,435 | 21.43 | |
| ≥2 | 134,572 | 18.11 | 69,056 | 19.28 | 65,516 | 17.03 | |
| Hypertension | <0.001 | ||||||
| No | 407,559 | 54.86 | 191,320 | 53.41 | 216,239 | 56.21 | |
| Yes | 335,358 | 45.14 | 166,881 | 46.59 | 168,477 | 43.79 | |
| Hyperlipidemia | <0.001 | ||||||
| No | 584,466 | 78.67 | 269,156 | 75.14 | 315,310 | 81.96 | |
| Yes | 158,451 | 21.33 | 89,045 | 24.86 | 69,406 | 18.04 | |
| Hyperuricemia | <0.001 | ||||||
| No | 736,469 | 99.13 | 354,603 | 99.00 | 381,866 | 99.26 | |
| Yes | 6448 | 0.87 | 3598 | 1.00 | 2850 | 0.74 | |
| Cerebrovascular disease | <0.001 | ||||||
| No | 704,412 | 94.82 | 337,392 | 94.19 | 367,020 | 95.40 | |
| Yes | 38,505 | 5.18 | 20,809 | 5.81 | 17,696 | 4.60 | |
| Coronary artery disease | <0.001 | ||||||
| No | 678,208 | 91.29 | 323,771 | 90.39 | 354,437 | 92.13 | |
| Yes | 64,709 | 8.71 | 34,430 | 9.61 | 30,279 | 7.87 | |
| Arrhythmia | <0.001 | ||||||
| No | 711,085 | 95.72 | 340,798 | 95.14 | 370,287 | 96.25 | |
| Yes | 31,832 | 4.28 | 17,403 | 4.86 | 14,429 | 3.75 | |
| Heart failure | <0.001 | ||||||
| No | 728,751 | 98.09 | 350,928 | 97.97 | 377,823 | 98.21 | |
| Yes | 14,166 | 1.91 | 7273 | 2.03 | 6893 | 1.79 | |
| Anxiety | <0.001 | ||||||
| No | 669,132 | 90.07 | 318,432 | 88.90 | 350,700 | 91.16 | |
| Yes | 73,785 | 9.93 | 39,769 | 11.10 | 34,016 | 8.84 | |
| Depression | <0.001 | ||||||
| No | 739,016 | 99.47 | 356,096 | 99.41 | 382,920 | 99.53 | |
| Yes | 3901 | 0.53 | 2105 | 0.59 | 1796 | 0.47 | |
| COPD c | <0.001 | ||||||
| No | 697,869 | 93.94 | 333,813 | 93.19 | 364,056 | 94.63 | |
| Yes | 45,048 | 6.06 | 24,388 | 6.81 | 20,660 | 5.37 | |
| Chronic kidney disease | <0.001 | ||||||
| No | 736,925 | 99.19 | 353,755 | 98.76 | 383,170 | 99.60 | |
| Yes | 5992 | 0.81 | 4446 | 1.24 | 1546 | 0.40 | |
| Obesity | 0.008 | ||||||
| No | 739,680 | 99.56 | 356,716 | 99.59 | 382,964 | 99.54 | |
| Yes | 3237 | 0.44 | 1485 | 0.41 | 1752 | 0.46 | |
| Alcoholism | 0.824 | ||||||
| No | 742,478 | 99.94 | 357,987 | 99.94 | 384,491 | 99.94 | |
| Yes | 439 | 0.06 | 214 | 0.06 | 225 | 0.06 | |
| Variables | Three-Year Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|
| Events | % | Adjusted Model 1 | Adjusted Model 2 | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Total | 3977 | 0.54 | ||||||
| cDDD of metformin use | ||||||||
| Non-users | 2223 | 0.62 | 1 | |||||
| <300 | 1728 | 0.46 | 0.88 | 0.83–0.94 | <0.001 | - | - | - |
| 300–500 | 23 | 0.45 | 1.09 | 0.72–1.65 | 0.676 | - | - | - |
| ≥500 | 3 | 1.27 | 2.59 | 0.83–8.03 | 0.100 | - | - | - |
| Intensity of metformin use | ||||||||
| Non-users | 2223 | 0.62 | 1 | |||||
| <10 | 1292 | 0.46 | - | - | - | 0.87 | 0.81–0.93 | <0.001 |
| 10–25 | 436 | 0.43 | - | - | - | 0.92 | 0.83–1.02 | 0.127 |
| ≥25 | 26 | 0.48 | - | - | - | 1.17 | 0.80–1.72 | 0.426 |
| Gender | ||||||||
| Female | 2078 | 0.54 | 1 | 1 | ||||
| Male | 1899 | 0.53 | 1.04 | 0.98–1.11 | 0.205 | 1.04 | 0.98–1.11 | 0.215 |
| Age (year) | ||||||||
| 50–64 | 940 | 0.20 | 1 | 1 | ||||
| 65–74 | 1617 | 0.88 | 3.95 | 3.64–4.29 | <0.001 | 3.96 | 3.64–4.30 | <0.001 |
| ≥75 | 1420 | 1.70 | 7.01 | 6.42–7.65 | <0.001 | 7.02 | 6.43–7.67 | <0.001 |
| Income level (NTD) a | ||||||||
| ≤21,000 | 2475 | 0.64 | 1 | 1 | ||||
| 21,001–33,000 | 803 | 0.46 | 0.96 | 0.88–1.04 | 0.272 | 0.96 | 0.88–1.04 | 0.274 |
| ≥33,001 | 699 | 0.39 | 0.91 | 0.83–0.99 | 0.033 | 0.91 | 0.83–0.99 | 0.033 |
| Urbanization b | ||||||||
| Level 1 | 919 | 0.45 | 1 | 1 | ||||
| Level 2 | 1167 | 0.49 | 1.09 | 1.00–1.18 | 0.066 | 1.09 | 1.00–1.18 | 0.066 |
| Level 3 | 599 | 0.52 | 1.09 | 0.98–1.21 | 0.098 | 1.09 | 0.98–1.21 | 0.098 |
| Level 4 | 712 | 0.68 | 1.25 | 1.13–1.38 | <0.001 | 1.25 | 1.13–1.38 | <0.001 |
| Level 5 | 169 | 0.96 | 1.47 | 1.25–1.74 | <0.001 | 1.47 | 1.25–1.74 | <0.001 |
| Level 6 | 230 | 0.73 | 1.20 | 1.04–1.39 | 0.014 | 1.20 | 1.04–1.39 | 0.013 |
| Level 7 | 181 | 0.63 | 1.10 | 0.94–1.29 | 0.239 | 1.10 | 0.94–1.30 | 0.236 |
| DCSI score c | ||||||||
| 0 | 1735 | 0.39 | 1 | 1 | ||||
| 1 | 890 | 0.56 | 1.16 | 1.06–1.26 | <0.001 | 1.16 | 1.06–1.26 | <0.001 |
| ≥2 | 1352 | 1.00 | 1.49 | 1.37–1.63 | <0.001 | 1.49 | 1.37–1.63 | <0.001 |
| Hypertension | ||||||||
| No | 1747 | 0.43 | 1 | 1 | ||||
| Yes | 2230 | 0.66 | 0.98 | 0.91–1.05 | 0.531 | 0.98 | 0.91–1.05 | 0.529 |
| Hyperlipidemia | ||||||||
| No | 3107 | 0.53 | 1 | 1 | ||||
| Yes | 870 | 0.55 | 0.90 | 0.83–0.98 | 0.010 | 0.90 | 0.83–0.98 | 0.010 |
| Hyperuricemia | ||||||||
| No | 3931 | 0.53 | 1 | 1 | ||||
| Yes | 46 | 0.71 | 1.12 | 0.84–1.50 | 0.436 | 1.12 | 0.84–1.50 | 0.435 |
| Cerebrovascular disease | ||||||||
| No | 3398 | 0.48 | 1 | 1 | ||||
| Yes | 579 | 1.50 | 1.55 | 1.41–1.71 | <0.001 | 1.55 | 1.41–1.71 | <0.001 |
| Coronary artery disease | ||||||||
| No | 3376 | 0.50 | 1 | 1 | ||||
| Yes | 601 | 0.93 | 1.05 | 0.95–1.15 | 0.351 | 1.05 | 0.95–1.15 | 0.351 |
| Arrhythmia | ||||||||
| No | 3683 | 0.52 | 1 | 1 | ||||
| Yes | 294 | 0.92 | 1.01 | 0.89–1.14 | 0.909 | 1.01 | 0.89–1.14 | 0.905 |
| Heart failure | ||||||||
| No | 3831 | 0.53 | 1 | 1 | ||||
| Yes | 146 | 1.03 | 0.83 | 0.70–0.99 | 0.039 | 0.83 | 0.70–0.99 | 0.039 |
| Anxiety | ||||||||
| No | 3208 | 0.48 | 1 | 1 | ||||
| Yes | 769 | 1.04 | 1.79 | 1.65–1.94 | <0.001 | 1.79 | 1.65–1.94 | <0.001 |
| Depression | ||||||||
| No | 3914 | 0.53 | 1 | 1 | ||||
| Yes | 63 | 1.61 | 1.93 | 1.50–2.48 | <0.001 | 1.93 | 1.50–2.48 | <0.001 |
| COPD c | ||||||||
| No | 3527 | 0.51 | 1 | 1 | ||||
| Yes | 450 | 1.00 | 1.15 | 1.04–1.27 | 0.006 | 1.15 | 1.04–1.27 | 0.006 |
| Chronic kidney disease | ||||||||
| No | 3897 | 0.53 | 1 | 1 | ||||
| Yes | 80 | 1.34 | 1.19 | 0.95–1.49 | 0.142 | 1.19 | 0.95–1.49 | 0.140 |
| Obesity | ||||||||
| No | 3963 | 0.54 | 1 | 1 | ||||
| Yes | 14 | 0.43 | 1.09 | 0.64–1.84 | 0.761 | 1.09 | 0.64–1.84 | 0.759 |
| Alcoholism | ||||||||
| No | 3974 | 0.54 | 1 | 1 | ||||
| Yes | 3 | 0.68 | 1.51 | 0.49–4.69 | 0.475 | 1.51 | 0.49–4.69 | 0.476 |
| Variables | Five-Year Follow-Up of Incident Parkinson’s Disease | |||||||
|---|---|---|---|---|---|---|---|---|
| Events | % | Adjusted Model 1 | Adjusted Model 2 | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Total | 8488 | 1.14 | ||||||
| cDDD of metformin use | ||||||||
| Non-users | 4584 | 1.28 | 1 | |||||
| <300 | 3856 | 1.02 | 0.94 | 0.90–0.98 | 0.006 | - | - | - |
| 300–500 | 45 | 0.88 | 1.01 | 0.75–1.35 | 0.969 | - | - | - |
| ≥500 | 3 | 1.27 | 1.24 | 0.40–3.86 | 0.706 | - | - | - |
| Intensity of metformin use | ||||||||
| Non-users | 4584 | 1.28 | 1 | |||||
| <10 | 2890 | 1.04 | - | - | - | 0.93 | 0.89–0.98 | 0.003 |
| 10–25 | 966 | 0.96 | - | - | - | 0.97 | 0.90–1.04 | 0.365 |
| ≥25 | 48 | 0.90 | - | - | - | 1.02 | 0.77–1.35 | 0.900 |
| Gender | ||||||||
| Female | 4463 | 1.17 | 1 | 1 | ||||
| Male | 4025 | 1.12 | 1.03 | 0.99–1.08 | 0.138 | 1.03 | 0.99–1.08 | 0.144 |
| Age (year) | ||||||||
| 50–64 | 2161 | 0.45 | 1 | 1 | ||||
| 65–74 | 3560 | 1.94 | 3.88 | 3.67–4.10 | <0.001 | 3.88 | 3.67–4.10 | <0.001 |
| ≥75 | 2767 | 3.31 | 6.22 | 5.86–6.60 | <0.001 | 6.22 | 5.86–6.61 | <0.001 |
| Income level (NTD) a | ||||||||
| ≤21,000 | 5239 | 1.36 | 1 | 1 | ||||
| 21,001–33,000 | 1728 | 0.98 | 0.96 | 0.90–1.01 | 0.099 | 0.96 | 0.90–1.01 | 0.101 |
| ≥33,001 | 1521 | 0.84 | 0.90 | 0.84–0.95 | <0.001 | 0.90 | 0.84–0.95 | <0.001 |
| Urbanization b | ||||||||
| Level 1 | 2093 | 1.02 | 1 | 1 | ||||
| Level 2 | 2466 | 1.03 | 1.01 | 0.95–1.07 | 0.879 | 1.01 | 0.95–1.07 | 0.878 |
| Level 3 | 1297 | 1.12 | 1.04 | 0.97–1.11 | 0.323 | 1.04 | 0.97–1.11 | 0.322 |
| Level 4 | 1453 | 1.39 | 1.12 | 1.05–1.20 | <0.001 | 1.12 | 1.05–1.20 | <0.001 |
| Level 5 | 308 | 1.75 | 1.19 | 1.06–1.34 | 0.005 | 1.19 | 1.06–1.35 | 0.004 |
| Level 6 | 482 | 1.52 | 1.11 | 1.01–1.23 | 0.040 | 1.11 | 1.01–1.23 | 0.039 |
| Level 7 | 389 | 1.35 | 1.04 | 0.94–1.16 | 0.456 | 1.04 | 0.94–1.16 | 0.452 |
| DCSI score c | ||||||||
| 0 | 3889 | 0.86 | 1 | 1 | ||||
| 1 | 1970 | 1.24 | 1.16 | 1.09–1.22 | <0.001 | 1.16 | 1.09–1.22 | <0.001 |
| ≥2 | 2629 | 1.95 | 1.35 | 1.27–1.43 | <0.001 | 1.35 | 1.27–1.43 | <0.001 |
| Hypertension | ||||||||
| No | 3785 | 0.93 | 1 | 1 | ||||
| Yes | 4703 | 1.40 | 1.00 | 0.95–1.04 | 0.818 | 1.00 | 0.95–1.04 | 0.816 |
| Hyperlipidemia | ||||||||
| No | 6633 | 1.13 | 1 | 1 | ||||
| Yes | 1855 | 1.17 | 0.91 | 0.86–0.96 | <0.001 | 0.91 | 0.86–0.96 | <0.001 |
| Hyperuricemia | ||||||||
| No | 8402 | 1.14 | 1 | 1 | ||||
| Yes | 86 | 1.33 | 1.01 | 0.81–1.25 | 0.944 | 1.01 | 0.81–1.25 | 0.941 |
| Cerebrovascular disease | ||||||||
| No | 7375 | 1.05 | 1 | 1 | ||||
| Yes | 1113 | 2.89 | 1.50 | 1.40–1.61 | <0.001 | 1.50 | 1.40–1.61 | <0.001 |
| Coronary artery disease | ||||||||
| No | 7259 | 1.07 | 1 | 1 | ||||
| Yes | 1229 | 1.90 | 1.04 | 0.97–1.11 | 0.249 | 1.04 | 0.97–1.11 | 0.250 |
| Arrhythmia | ||||||||
| No | 7856 | 1.10 | 1 | 1 | ||||
| Yes | 632 | 1.99 | 1.08 | 0.99–1.17 | 0.073 | 1.08 | 0.99–1.17 | 0.073 |
| Heart failure | ||||||||
| No | 8193 | 1.12 | 1 | 1 | ||||
| Yes | 295 | 2.08 | 0.87 | 0.77–0.98 | 0.027 | 0.87 | 0.77–0.98 | 0.026 |
| Anxiety | ||||||||
| No | 6917 | 1.03 | 1 | 1 | ||||
| Yes | 1571 | 2.13 | 1.74 | 1.64–1.84 | <0.001 | 1.74 | 1.64–1.84 | <0.001 |
| Depression | ||||||||
| No | 8376 | 1.13 | 1 | 1 | ||||
| Yes | 112 | 2.87 | 1.67 | 1.38–2.01 | <0.001 | 1.67 | 1.38–2.01 | <0.001 |
| COPD c | ||||||||
| No | 7583 | 1.09 | 1 | 1 | ||||
| Yes | 905 | 2.01 | 1.13 | 1.05–1.21 | <0.001 | 1.13 | 1.05–1.21 | <0.001 |
| Chronic kidney disease | ||||||||
| No | 8351 | 1.13 | 1 | 1 | ||||
| Yes | 137 | 2.29 | 1.06 | 0.89–1.26 | 0.502 | 1.06 | 0.89–1.26 | 0.499 |
| Obesity | ||||||||
| No | 8465 | 1.14 | 1 | 1 | ||||
| Yes | 23 | 0.71 | 0.81 | 0.54–1.22 | 0.314 | 0.81 | 0.54–1.22 | 0.313 |
| Alcoholism | ||||||||
| No | 8483 | 1.14 | 1 | 1 | ||||
| Yes | 5 | 1.14 | 1.18 | 0.49–2.83 | 0.718 | 1.18 | 0.49–2.83 | 0.717 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, K.-H.; Chang, Y.-L.; Gau, S.-Y.; Tsai, T.-H.; Lee, C.-Y. Dose–Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus. Pharmaceutics 2022, 14, 946. https://doi.org/10.3390/pharmaceutics14050946
Huang K-H, Chang Y-L, Gau S-Y, Tsai T-H, Lee C-Y. Dose–Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus. Pharmaceutics. 2022; 14(5):946. https://doi.org/10.3390/pharmaceutics14050946
Chicago/Turabian StyleHuang, Kuang-Hua, Ya-Lan Chang, Shuo-Yan Gau, Tung-Han Tsai, and Chien-Ying Lee. 2022. "Dose–Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus" Pharmaceutics 14, no. 5: 946. https://doi.org/10.3390/pharmaceutics14050946