
Reparative Efficacy of Liposome-Encapsulated Oleanolic Acid against Liver Inflammation Induced by Fine Ambient Particulate Matter and Alcohol in Mice

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
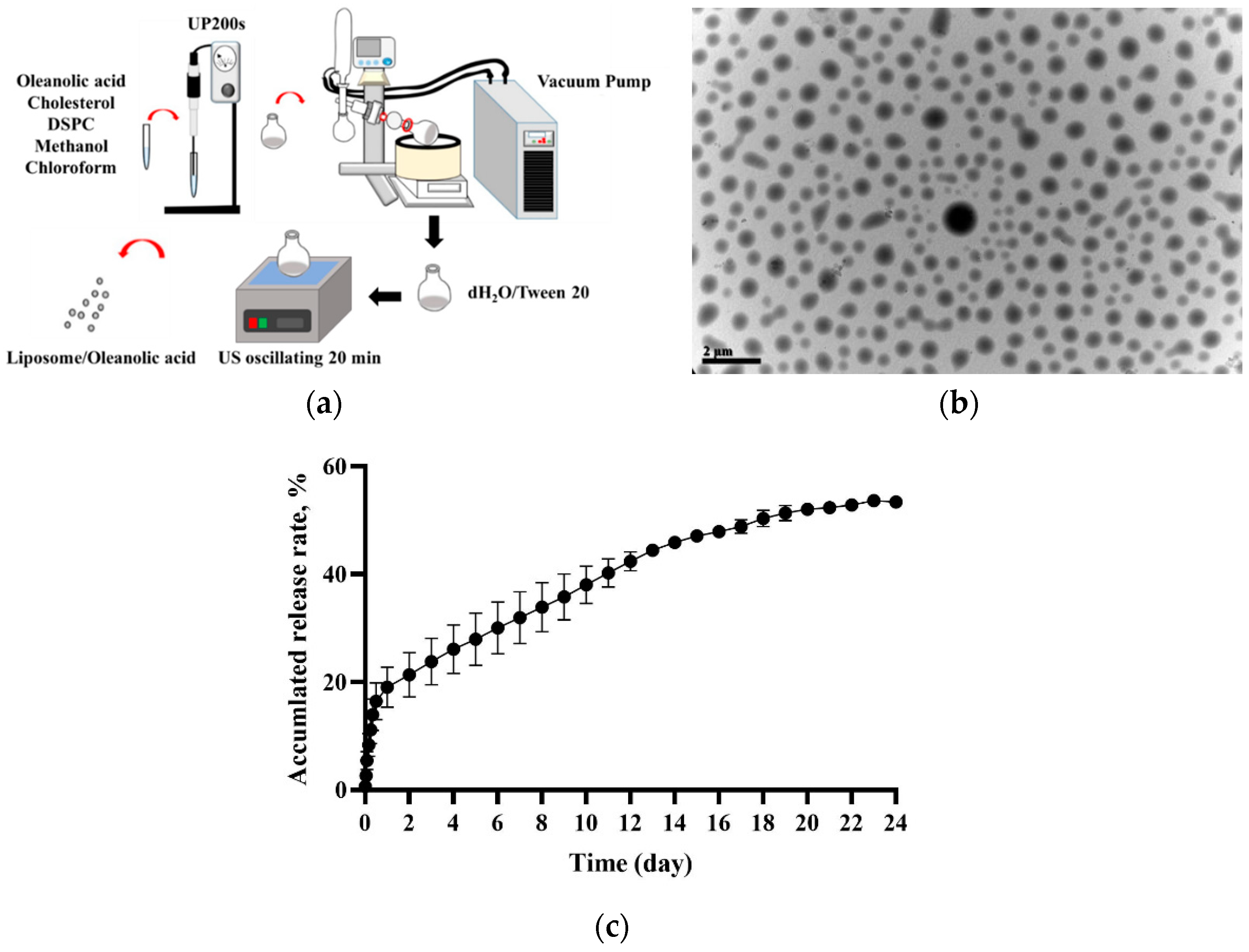
2.2. Lipo-OAs Production and Characterization
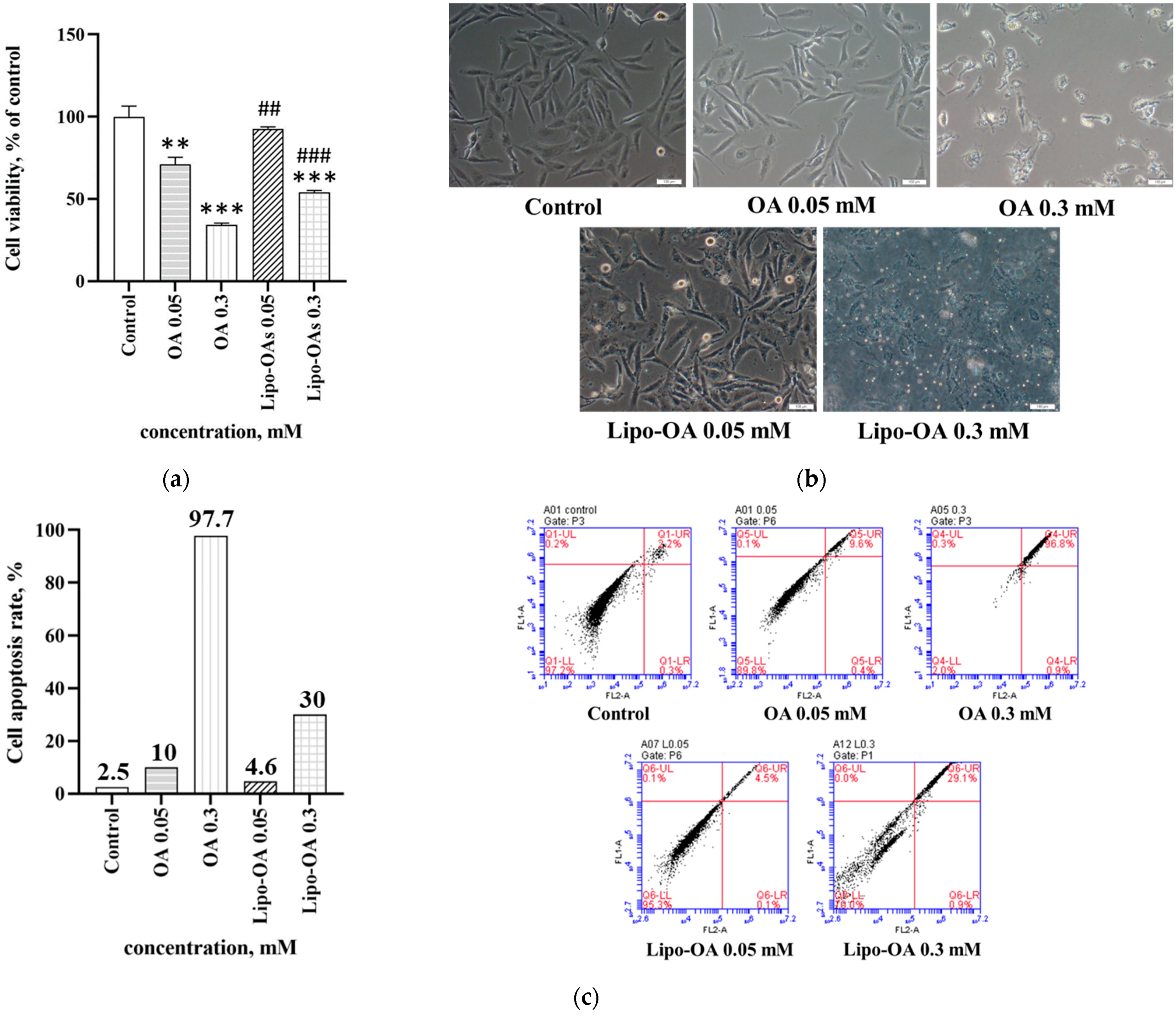
2.3. In Vitro Cell Viability Tests of OA and Lipo-OAs
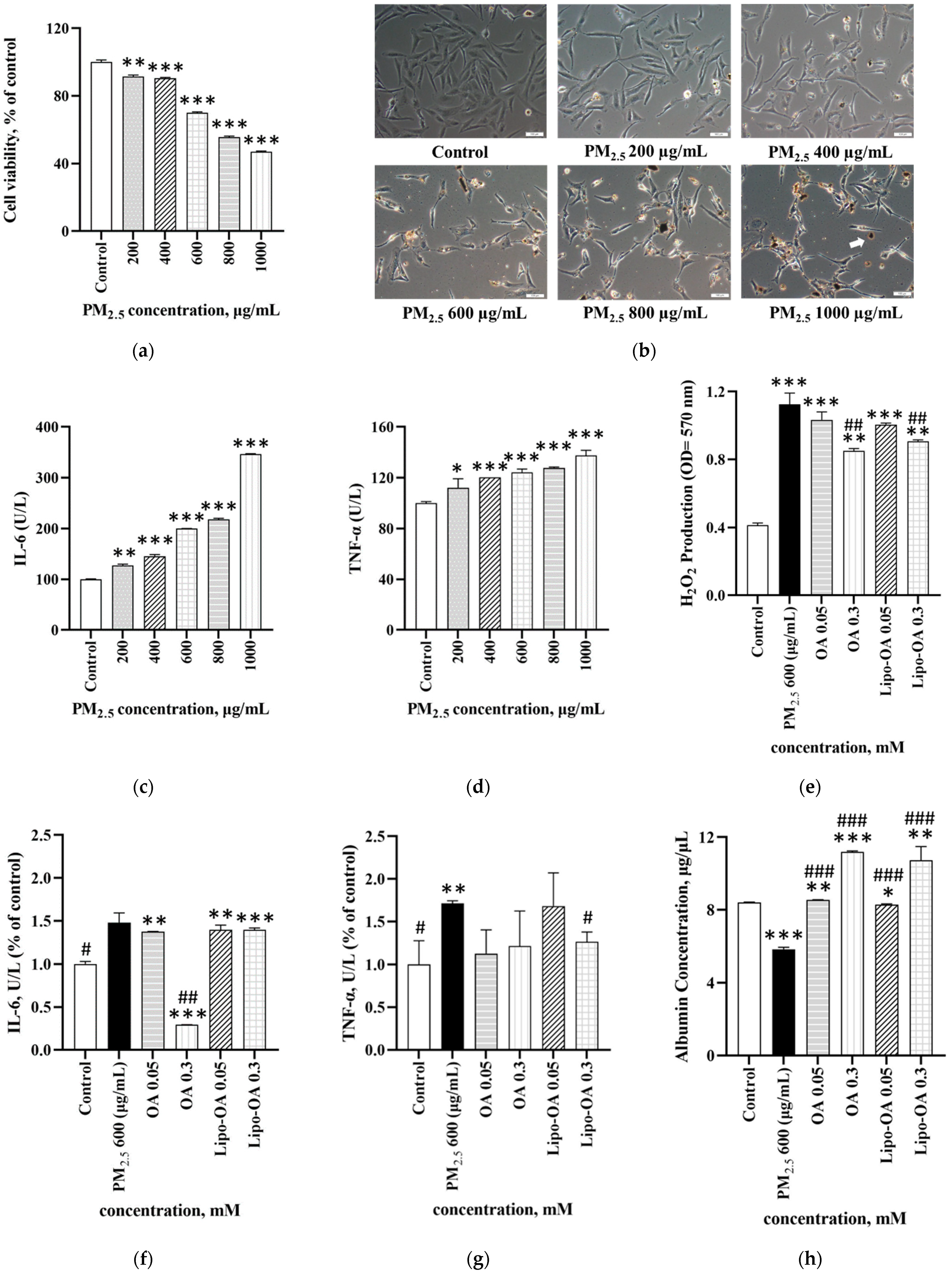
2.4. In Vitro Cell Viability and Inflammatory Response of LX-2 Cells Exposed to PM2.5
2.5. Antioxidant and Albumin Secretion by PM2.5-Induced Inflammatory LX-2 Cells Treated with OA and Lipo-OAs
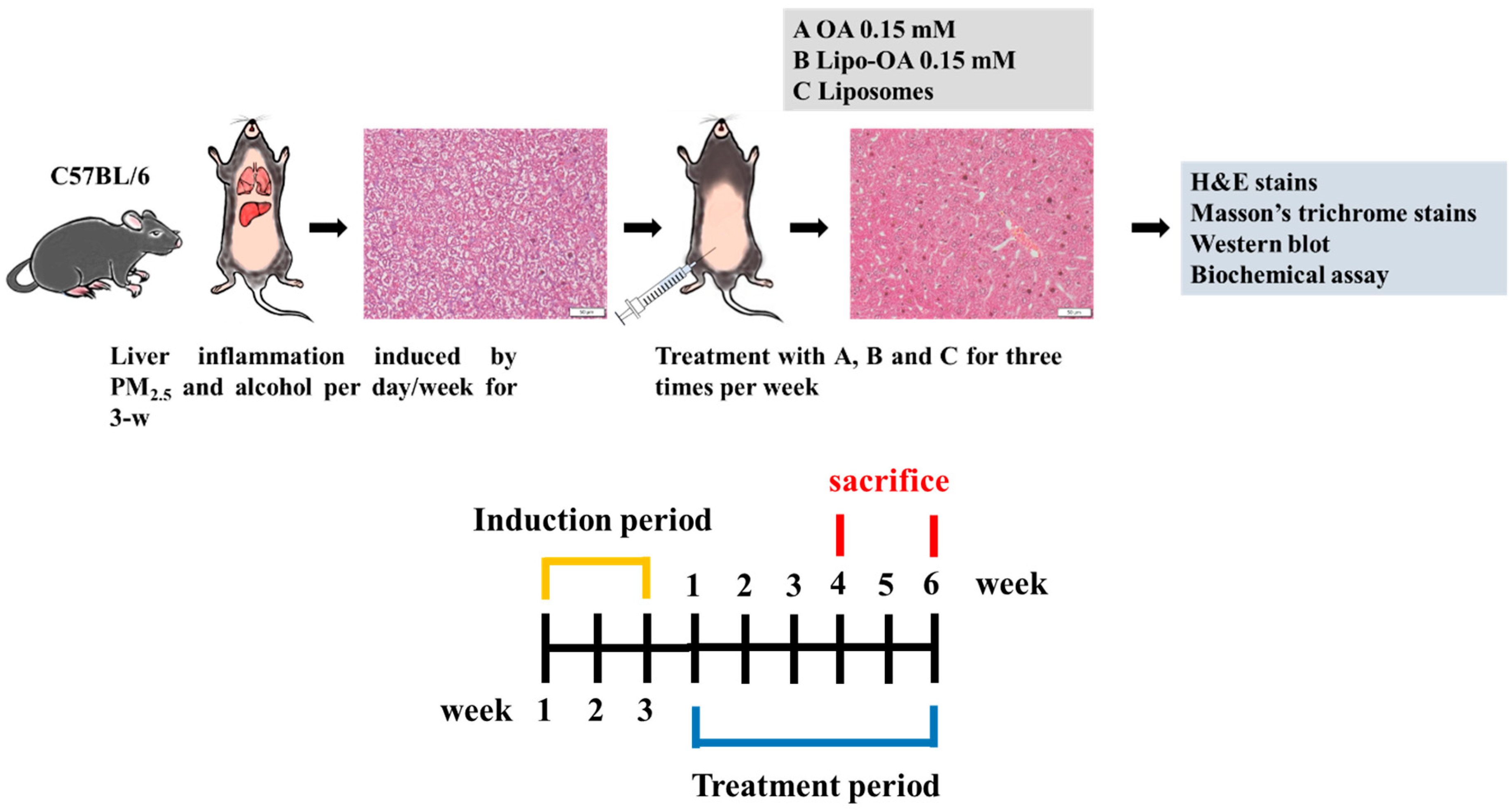
2.6. Animal Experiments
2.6.1. Establishment of PM2.5 and Alcohol-Induced Liver Inflammation Model in Mice
2.6.2. Histopathological Analysis
2.6.3. Ishak’s Modified HAI Score
- (1)
- Periportal or periseptal interface hepatitis score: 0 = absent; 1 = mild (focal, few portal areas); 2 = mild or moderate (focal, most portal areas); 3 = moderate (continuous around <50% of tracts or septa); and 4 = severe (continuous around >50% of tracts or septa);
- (2)
- Confluent necrosis score: 0 = absent; 1 = focal confluent necrosis; 2 = zone 3 necrosis in some areas; 3 = zone 3 necrosis in most areas; 4 = zone 3 necrosis + occasional portal–central (P–C) bridging; 5 = zone 3 necrosis + multiple P–C bridging; and 6 = pan-acinar or multiacinar necrosis;
- (3)
- Focal (or spotty) lytic necrosis or apoptosis and focal inflammation score: 0 = absent; 1 = ≤1 foci per 10× objective field; 2 = 2–4 foci per 10× objective field; 3 = 5–10 foci per 10× objective field; and 4 = >10 foci per 10× objective field;
- (4)
- Portal inflammation score: 0 = none; 1 = mild (some or all portal areas); 2 = moderate (some or all portal areas); 3 = moderate or marked (all portal areas); and 4 = marked (all portal areas).
2.6.4. Western Blot Analysis
2.6.5. Blood Biochemical Assays
2.7. Statistical Analysis
3. Results
3.1. Lipo-OAs Characterization
3.2. Effects of OA and Lipo-OAs on Cell Viability
3.3. Effects of PM2.5 on Cell Viability and Inflammatory Response
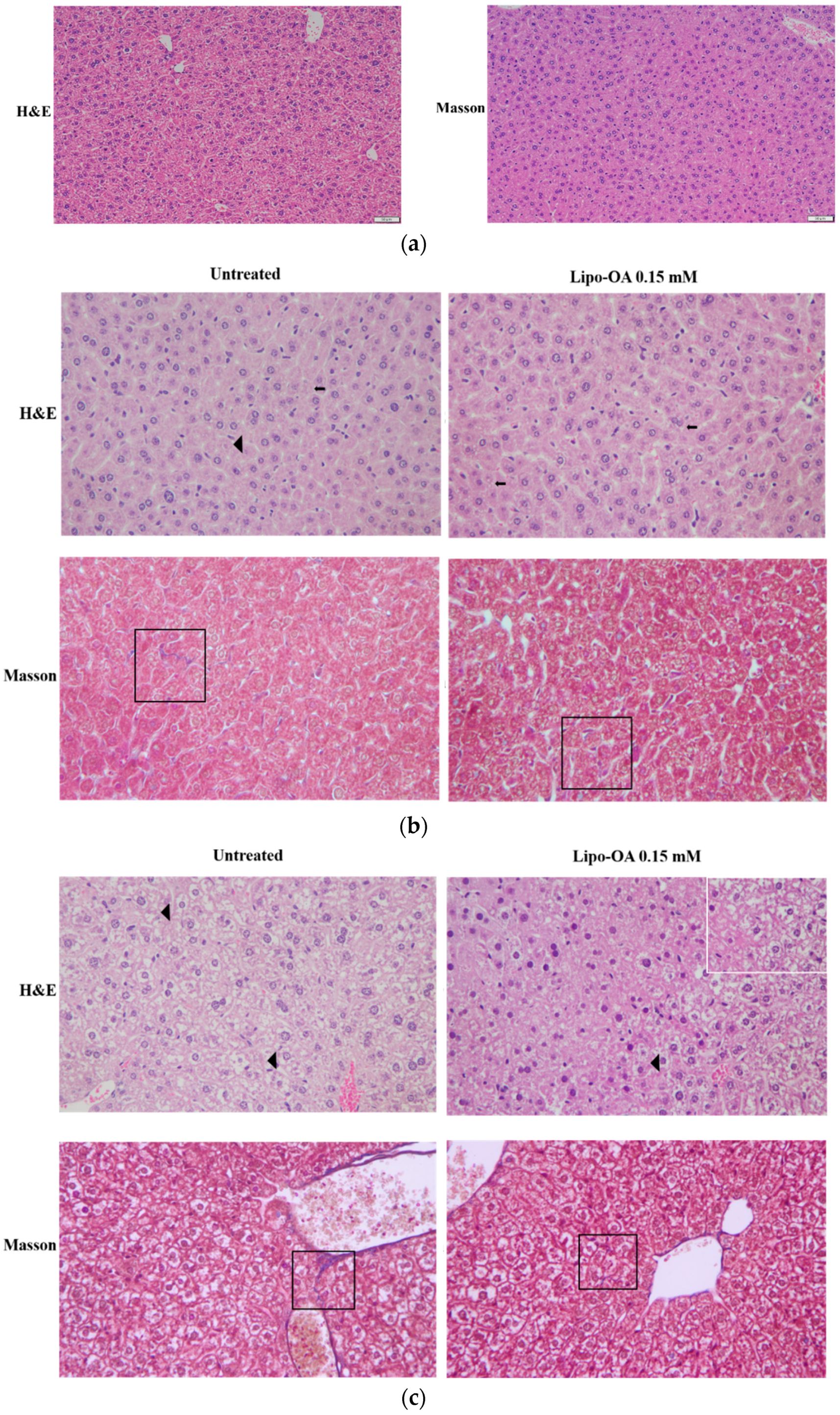
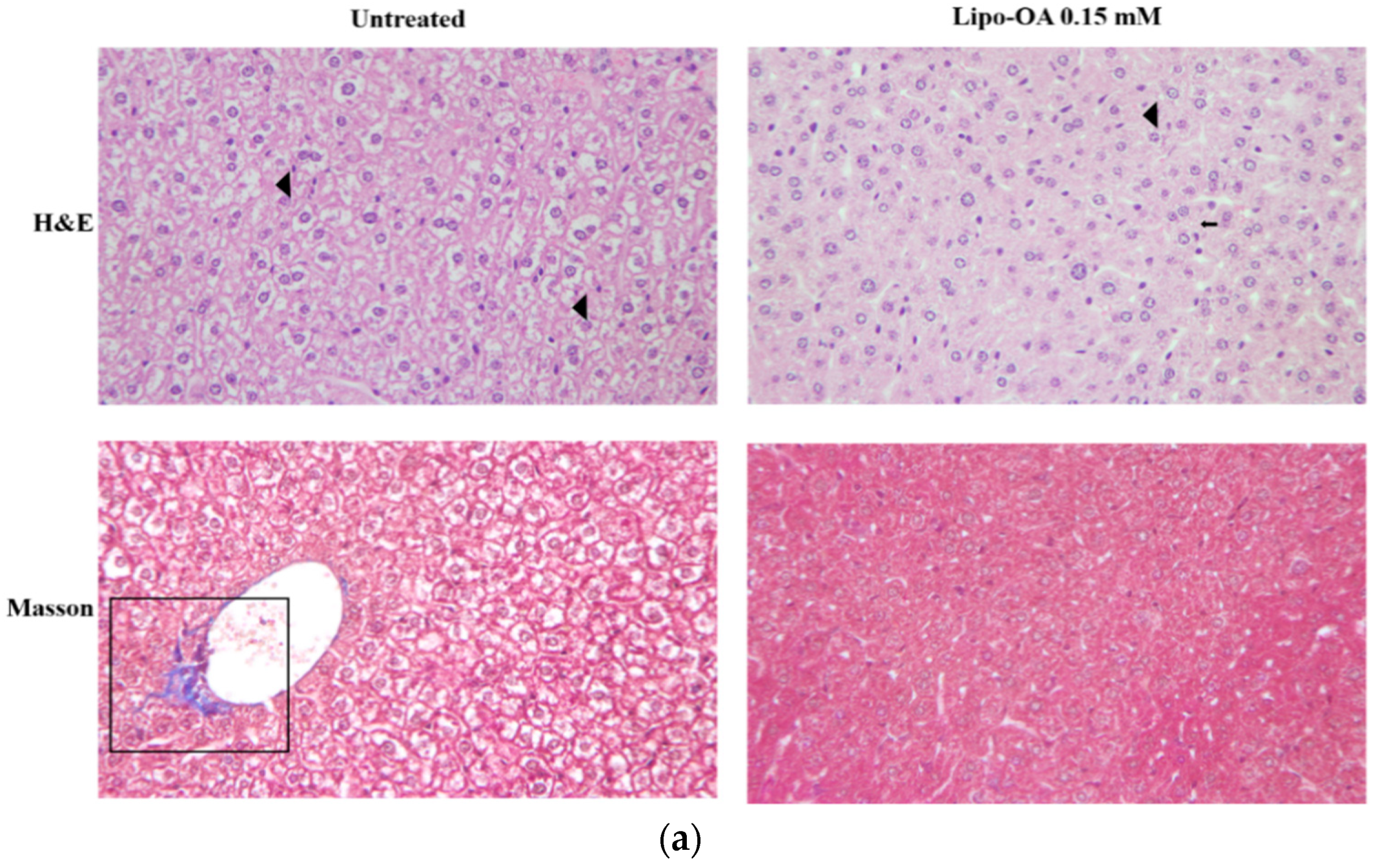
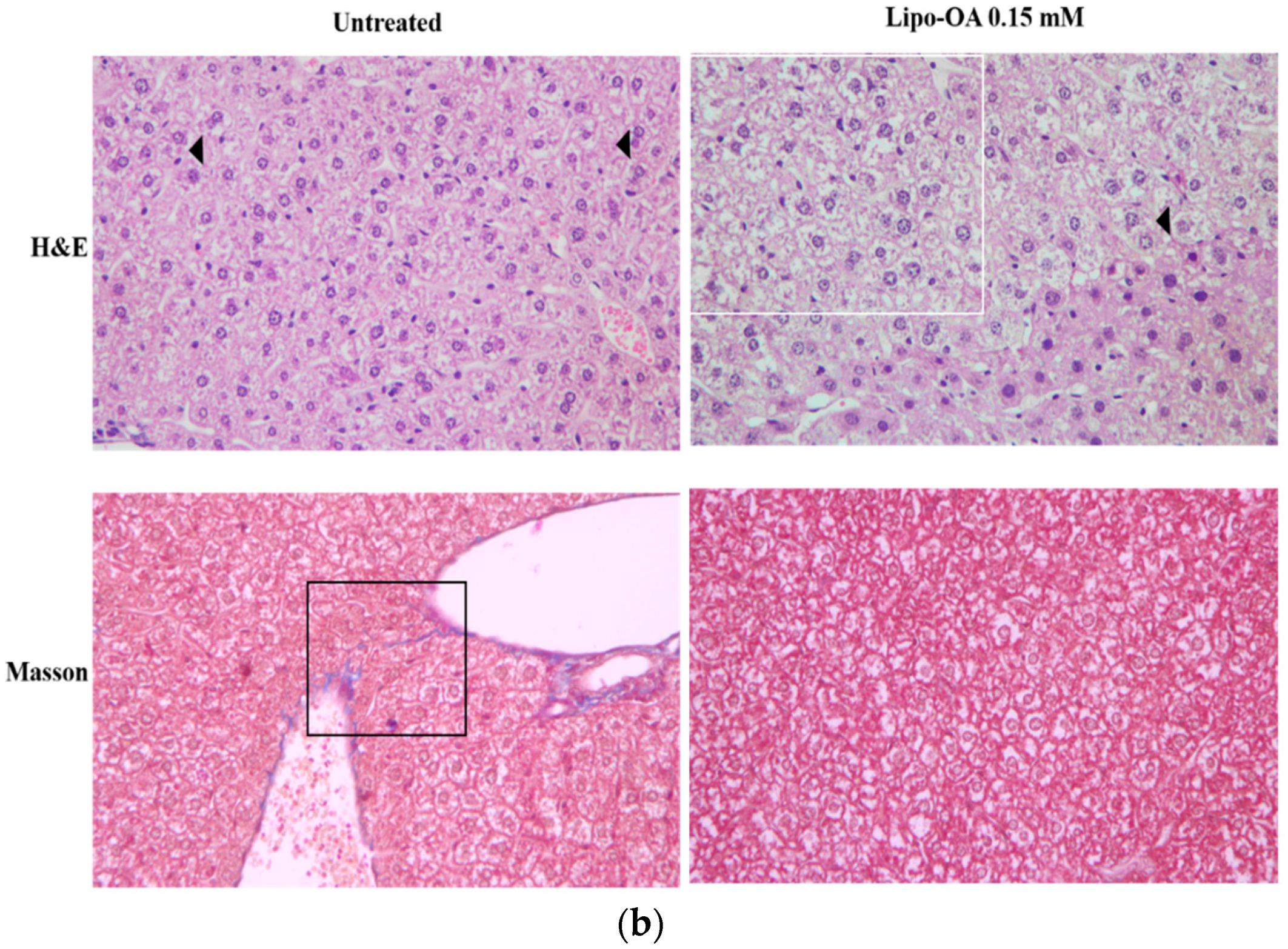
3.4. Histopathological Analysis of Mouse Liver
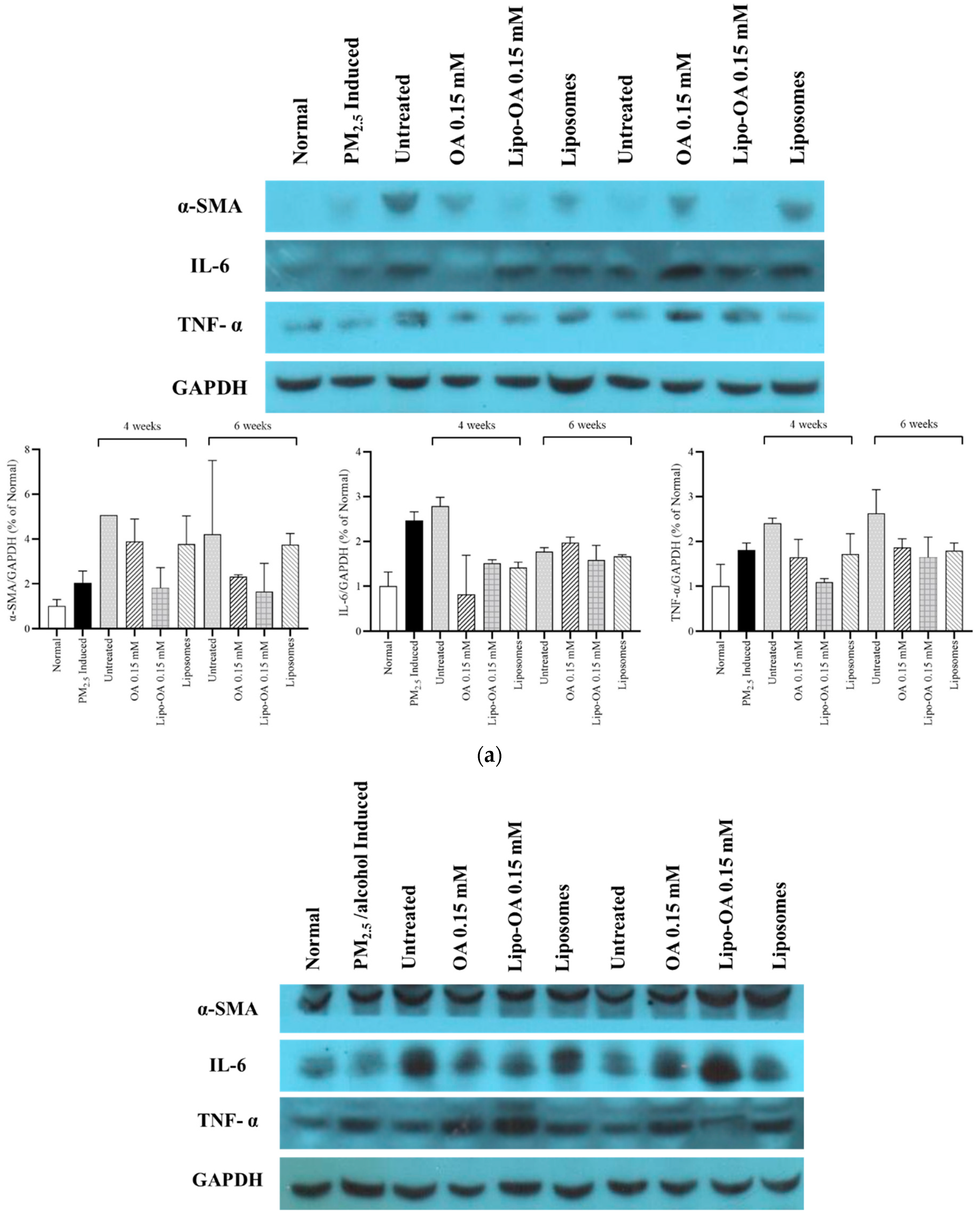
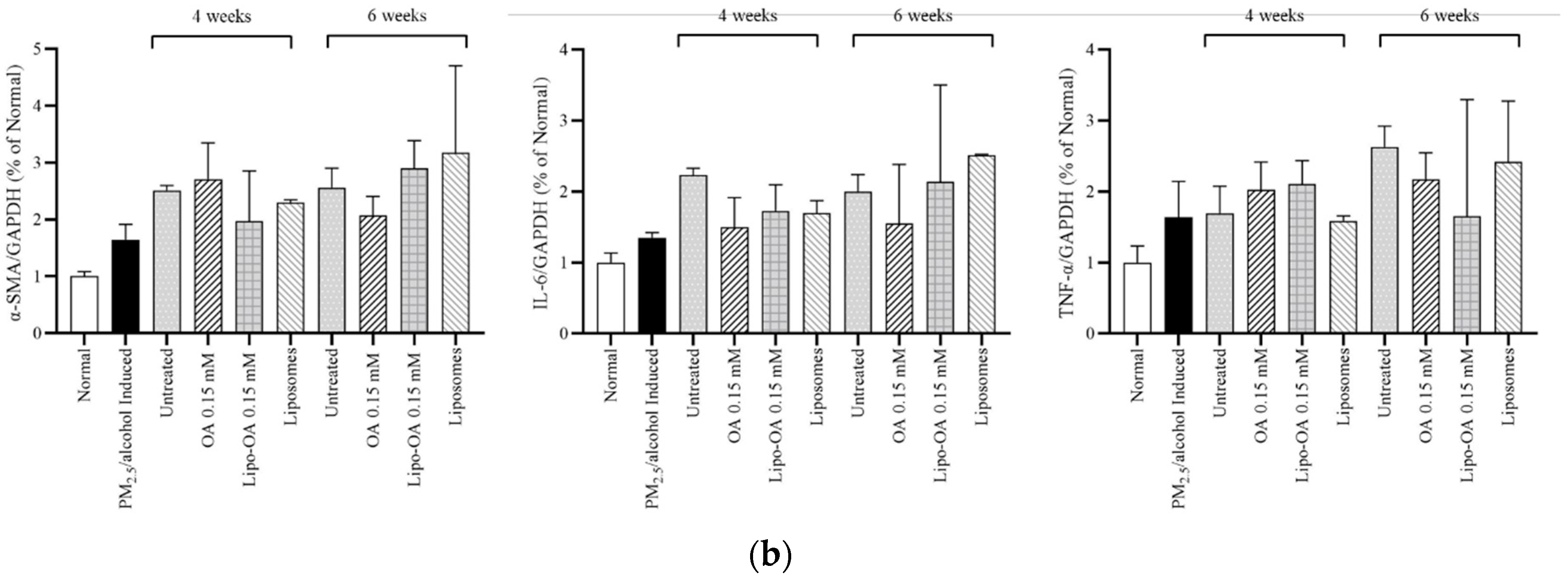
3.5. Western Blot Analysis
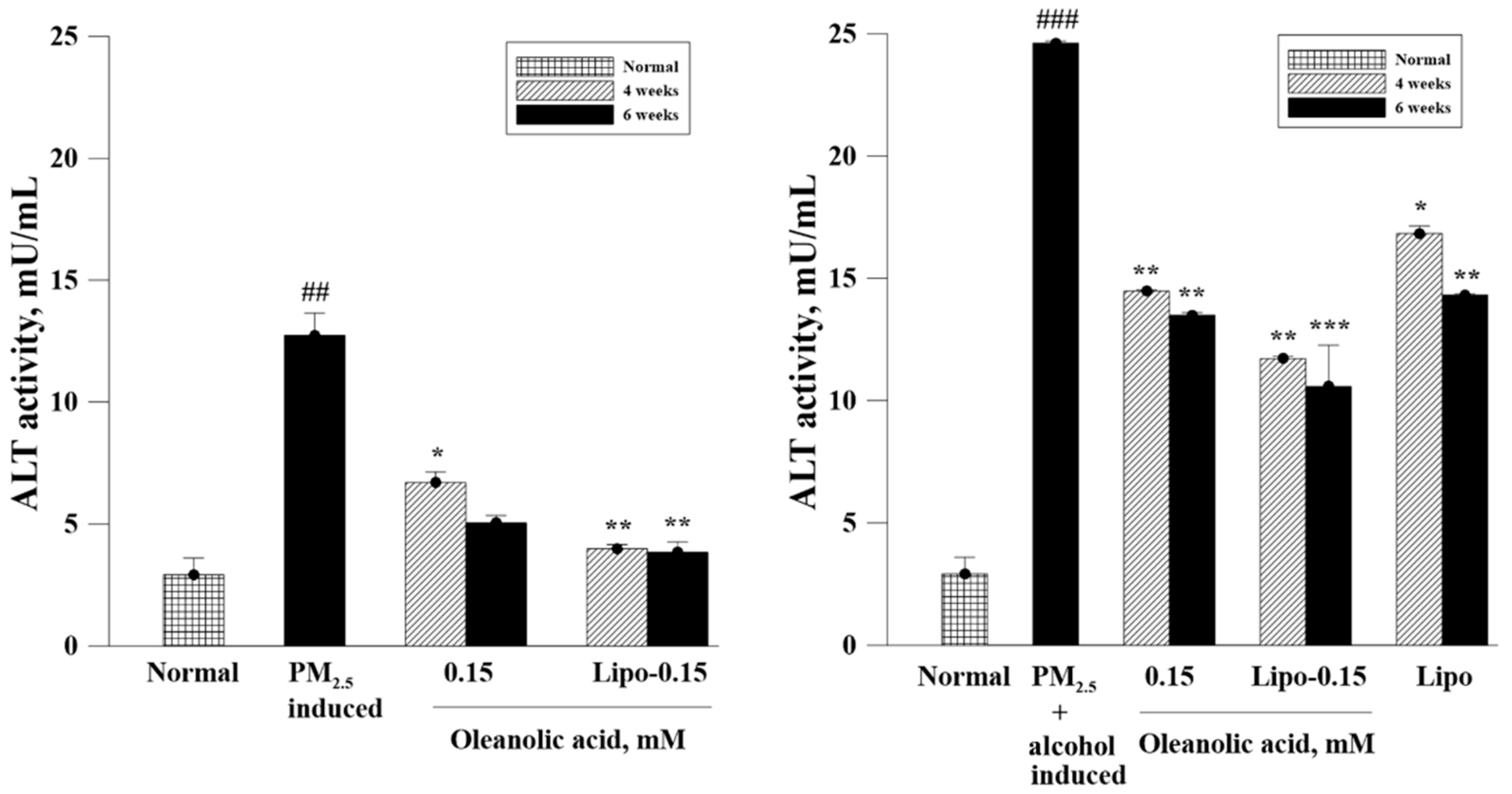
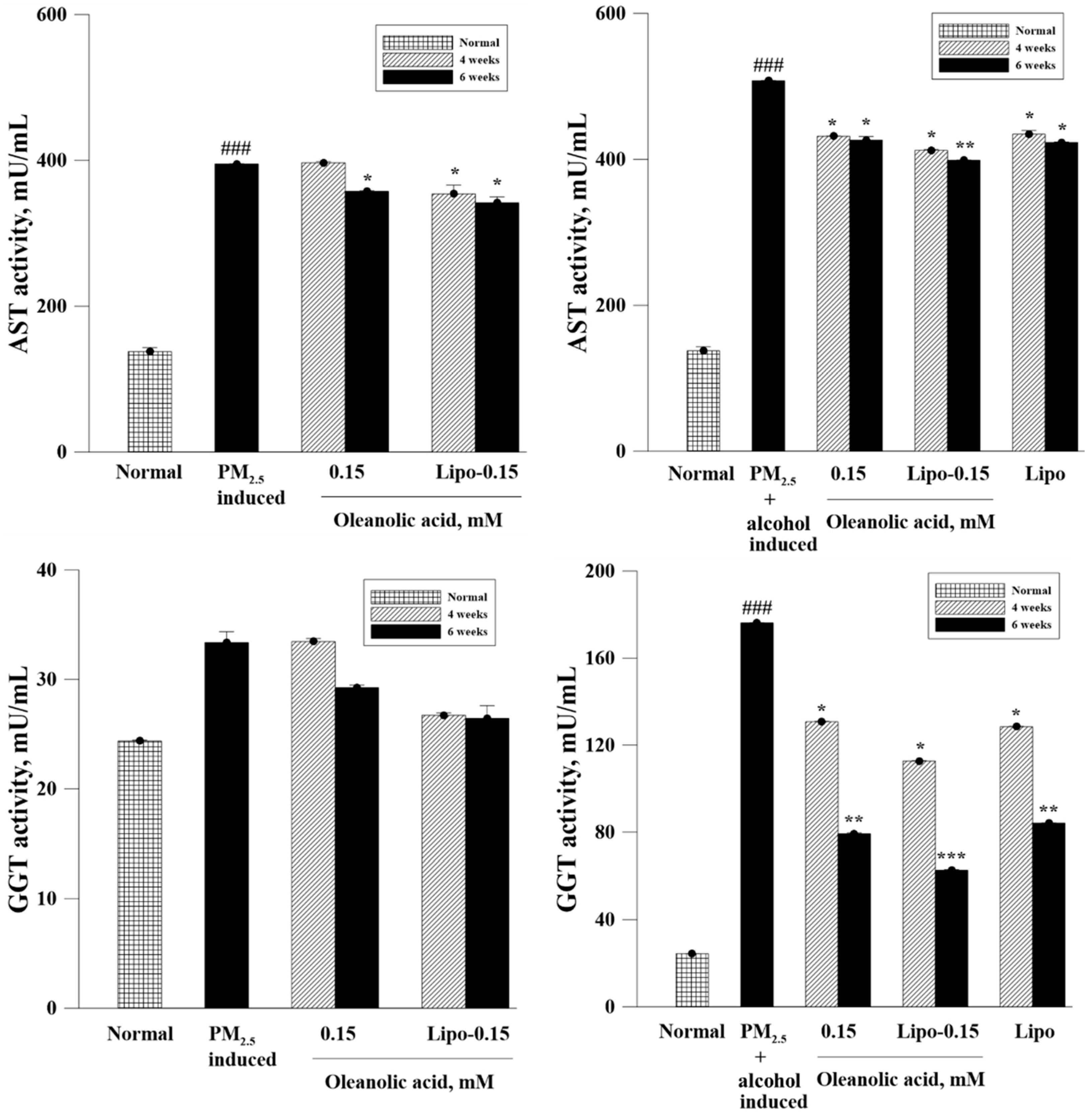
3.6. Biochemical Analysis of Serum ALT, AST, and GGT Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muriel, P.; Rivera-Espinoza, Y. Beneficial drugs for liver diseases. J. Appl. Toxicol. 2008, 28, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Ayeleso, T.B.; Matumba, M.G.; Mukwevho, E. Oleanolic Acid and Its Derivatives: Biological Activities and Therapeutic Potential in Chronic Diseases. Molecules 2017, 22, 1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.C.; Wu, G.X.; Huang, H.H.; Kuo, S.M. Liposome-encapsulated farnesol accelerated tissue repair in third-degree burns on a rat model. Burns 2019, 45, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Shiu, L.-Y.; Huang, H.H.; Chen, C.Y.; Cheng, H.-Y.; Chen, C.I.; Kuo, S.M. Reparative and toxicity-reducing effects of liposome-encapsulated saikosaponin in mice with liver fibrosis. Biosci. Rep. 2020, 40, BSR20201219. [Google Scholar] [CrossRef] [PubMed]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; Macsween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhang, X.; Wang, J.; Dandekar, A.; Kim, H.; Qiu, Y.; Xu, X.; Cui, Y.; Wang, A.; Chen, L.C.; et al. Exposure to fine airborne particulate matters induces hepatic fibrosis in murine models. J. Hepatol. 2015, 63, 1397–1404. [Google Scholar] [CrossRef] [Green Version]
- Mokdad, A.A.; Lopez, A.D.; Shahraz, S.; Lozano, R.; Stanaway, J.; Murray, C.J.L.; Naghavi, M. Liver cirrhosis mortality in 187 countries between 1980 and 2010: A systematic analysis. BMC Med. 2014, 12, 145. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.C.; Jiang, J.Y.; Goggins, W.B.; Liang, M.; Fang, Y.; Fung, F.D.; Leung, C.; Wang, H.H.; Wong, G.L.; Wong, V.W.; et al. International incidence and mortality trends of liver cancer: A global profile. Sci. Rep. 2017, 7, 45846. [Google Scholar] [CrossRef]
- Li, R.; Zhang, M.; Wang, Y.; Yung, K.K.L.; Su, R.; Li, Z.; Zhao, L.; Dong, C.; Cai, Z. Effects of sub-chronic exposure to atmospheric PM2.5 on fibrosis, inflammation, endoplasmic reticulum stress and apoptosis in the livers of rats. Toxicol. Res. 2018, 7, 271–282. [Google Scholar] [CrossRef] [Green Version]
- Im, P.K.; Millwood, I.Y.; Kartsonaki, C.; Guo, Y.; Chen, Y.; Turnbull, I.; Yu, C.; Du, H.; Pei, P.; Lv, J.; et al. Alcohol drinking and risks of liver cancer and non-neoplastic chronic liver diseases in China: A 10-year prospective study of 0.5 million adults. BMC Med. 2021, 19, 216. [Google Scholar] [CrossRef]
- Parthasarathy, G.; Revelo, X.; Malhi, H. Pathogenesis of Nonalcoholic Steatohepatitis: An Overview. Hepatol. Commun. 2020, 4, 478–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, K.A.; McGee, J.O. Alcohol induced liver disease. J. Clin. Pathol. 1984, 37, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Liu, J. Oleanolic acid and ursolic acid: Research perspectives. J. Ethnopharmacol. 2005, 100, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Bi, S.; Chu, F.; Wang, M.; Li, B.; Mao, P.; Zhang, H.; Wang, P.; Guo, W.; Xu, L.; Ren, L.; et al. Ligustrazine-Oleanolic Acid Glycine Derivative, G-TOA, Selectively Inhibited the Proliferation and Induced Apoptosis of Activated HSC-T6 Cells. Molecules 2016, 21, 1599. [Google Scholar] [CrossRef] [Green Version]
- Feng, A.; Yang, S.; Sun, Y.; Zhang, L.; Bo, F.; Li, L. Development and Evaluation of Oleanolic Acid Dosage Forms and Its Derivatives. Biomed. Res. Int. 2020, 2020, 1308749. [Google Scholar] [CrossRef]
- Wu, Y.C.; Huang, H.H.; Wu, Y.J.; Manousakas, I.; Yang, C.C.; Kuo, S.M. Therapeutic and Protective Effects of Liposomal Encapsulation of Astaxanthin in Mice with Alcoholic Liver Fibrosis. Int. J. Mol. Sci. 2019, 20, 4057. [Google Scholar] [CrossRef] [Green Version]
- Cadinoiu, A.N.; Rata, D.M.; Atanase, L.I.; Daraba, O.M.; Gherghel, D.; Vochita, G.; Popa, M. Aptamer-Functionalized Liposomes as a Potential Treatment for Basal Cell Carcinoma. Polymers 2019, 11, 1515. [Google Scholar] [CrossRef] [Green Version]
- Cadinoiu, A.; Rata, D.; Atanase, L.; Mihai, C.; Bacaita, S.; Popa, M. Formulations Based on Drug Loaded Aptamer-Conjugated Liposomes as a Viable Strategy for the Topical Treatment of Basal Cell Carcinoma-In Vitro Tests. Pharmaceutics 2021, 13, 866. [Google Scholar] [CrossRef]
- Gao, D.; Tang, S.; Tong, Q. Oleanolic acid liposomes with polyethylene glycol modification: Promising antitumor drug delivery. Int. J. Nanomed. 2012, 7, 3517–3526. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.; Gao, D.; Zhao, T.; Zhou, J.; Zhao, X. An evaluation of the anti-tumor efficacy of oleanolic acid-loaded PEGylated liposomes. Nanotechnology 2013, 24, 235102. [Google Scholar] [CrossRef]
- Sarfraz, M.; Afzal, A.; Raza, S.M.; Bashir, S.; Madni, A.; Khan, M.W.; Xiang, G. Liposomal co-delivered oleanolic acid attenuates doxorubicin-induced multi-organ tox-icity in hepatocellular carcinoma. Oncotarget 2017, 8, 47136–47153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buyl, K.; De Kock, J.; Bolleyn, J.; Rogiers, V.; Vanhaecke, T. Measurement of Albumin Secretion as Functionality Test in Primary Hepatocyte Cultures. Methods Mol. Biol. 2015, 1250, 303–308. [Google Scholar] [PubMed]
- Shiha, G.; Zalata, K. Ishak versus METAVIR: Terminology, Convertibility and Correlation with Laboratory Changes in Chronic Hepatitis C. Liver Biopsy; Takahashi, H., Ed.; IntechOpen: London, UK, 2011. [Google Scholar] [CrossRef] [Green Version]
- Lee-Montiel, F.T.; George, S.; Gough, A.H.; Sharma, A.D.; Wu, J.; DeBiasio, R.; Vernetti, L.; Taylor, D.L. Control of oxygen tension recapitulates zone-specific functions in human liver microphysiology systems. Exp. Biol. Med. 2017, 242, 1617–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatta, A.; Verardo, A.; Bolognesi, M. Hypoalbuminemia. Intern. Emerg. Med. 2012, 7 (Suppl. S3), S193–S199. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Hu, S.; Fan, P.; Li, L.; Feng, S.; Xiao, H.; Zhu, L. The Roles of Liver Inflammation and the Insulin Signaling Pathway in PM2.5 Instillation-Induced Insulin Resistance in Wistar Rats. Dis. Markers 2021, 2021, 2821673. [Google Scholar] [CrossRef]
- Domenicali, M.; Caraceni, P.; Giannone, F.; Baldassarre, M.; Lucchetti, G.; Quarta, C.; Patti, C.; Catani, L.; Nanni, C.; Lemoli, R.M.; et al. A novel model of CCl4-induced cirrhosis with ascites in the mouse. J. Hepatol. 2009, 51, 991–999. [Google Scholar] [CrossRef]
- Cobbina, E.; Akhlaghi, F. Non-alcoholic fatty liver disease (NAFLD)—Pathogenesis, classification, and effect on drug metabolizing enzymes and transporters. Drug Metab. Rev. 2017, 49, 197–211. [Google Scholar] [CrossRef]
- Singer, C.; Stancu, P.; Coşoveanu, S.; Botu, A. Non-alcoholic Fatty liver disease in children. Curr. Health Sci. J. 2014, 40, 170–176. [Google Scholar]
- Denk, H.; Stumptner, C.; Zatloukal, K. Mallory bodies revisited. J. Hepatol. 2000, 32, 689–702. [Google Scholar] [CrossRef]
- Wang, Y.; Zhong, Y.; Liao, J.; Wang, G. PM2.5-related cell death patterns. Int. J. Med. Sci. 2021, 18, 1024–1029. [Google Scholar] [CrossRef]
- Jeong, S.; Park, S.A.; Park, I.; Kim, P.; Cho, N.H.; Hyun, J.W.; Hyun, Y.-M. PM2.5 Exposure in the Respiratory System Induces Distinct Inflammatory Signaling in the Lung and the Liver of Mice. J. Immunol. Res. 2019, 2019, 3486841. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Yuan, C.; Si, B.; Wang, M.; Da, S.; Bai, L.; Wu, W. Combined effects of ambient particulate matter exposure and a high-fat diet on oxidative stress and steatohepatitis in mice. PLoS ONE 2019, 14, e0214680. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Zhang, C.; Li, B.; Xu, X.; Liang, M.; Gu, S.; Chu, F.; Xu, B.; Ren, J.; Wang, P.; et al. A Series of Oleanolic Acid Derivatives as Anti-Hepatitis B Virus Agents: Design, Synthesis, and in Vitro and in Vivo Biological Evaluation. Molecules 2016, 21, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapper, E.B.; Saini, S.D.; Sengupta, N. Extensive testing or focused testing of patients with elevated liver enzymes. J. Hepatol. 2017, 66, 313–319. [Google Scholar] [CrossRef]
- Roehlen, N.; Crouchet, E.; Baumert, T.F. Liver Fibrosis: Mechanistic Concepts and Therapeutic Perspectives. Cells 2020, 9, 875. [Google Scholar] [CrossRef] [Green Version]
- Federico, A.; Dallio, M.; Loguercio, C. Silymarin/Silybin and Chronic Liver Disease: A Marriage of Many Years. Molecules 2017, 22, 191. [Google Scholar] [CrossRef] [Green Version]
- Song, Z.; Deaciuc, I.; Song, M. Silymarin protects against acute ethanol-induced hepatotoxicity in mice. Alcohol. Clin. Exp. Res. 2006, 30, 407–413. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Steatosis | Mallory Body and Ballooning Cells | Ishak Modified HAI Score | Pericellular Fibrosis |
|---|---|---|---|---|
| untreated | + | ++ | 1 | ++ |
| OA | + | ++ | 0 | +~++ |
| Liposome | ++ | ++ | 2 | ++ |
| Lipo-OAs | + | + | 0 | + |
| Group | Steatosis | Mallory Body and Ballooning Cells | Necrosis | Ishak Modified HAI Score | Pericellular Fibrosis |
|---|---|---|---|---|---|
| untreated | +++ | +++ | − | 1 | −/+ |
| OA | +++ | +++ | + | 3 | + |
| Liposome | +++ | +++ | + | 2 | + |
| Lipo-OAs | ++ | +~++ | − | 0 | −/+ |
| Group | Steatosis | Mallory Body and Ballooning Cells | Ishak Modified HAI Score | Pericellular Fibrosis |
|---|---|---|---|---|
| Untreated | +++ | +++ | 2 | −/+ |
| OA | +++ | +++ | 1 | −/+ |
| Liposome | +++ | +++ | 2 | −/+ |
| Lipo-OAs | + | + | 0 | −/+ |
| Garoup | Steatosis | Mallory Body and Ballooning Cells | Ishak Modified HAI score | Pericellular Fibrosis |
|---|---|---|---|---|
| Untreated | +++ | +++ | 2 | −/+ |
| OA | +++ | +++ | 1 | −/+~+ |
| Liposome | +++ | +++ | 2 | −/+ |
| Lipo-OAs | +++ | ++ | 0 | −/+ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, C.-T.; Wang, Y.-W.; Wu, Y.-C.; Lin, L.-W.; Chen, C.-C.; Chen, C.-Y.; Kuo, S.-M. Reparative Efficacy of Liposome-Encapsulated Oleanolic Acid against Liver Inflammation Induced by Fine Ambient Particulate Matter and Alcohol in Mice. Pharmaceutics 2022, 14, 1108. https://doi.org/10.3390/pharmaceutics14051108
Wei C-T, Wang Y-W, Wu Y-C, Lin L-W, Chen C-C, Chen C-Y, Kuo S-M. Reparative Efficacy of Liposome-Encapsulated Oleanolic Acid against Liver Inflammation Induced by Fine Ambient Particulate Matter and Alcohol in Mice. Pharmaceutics. 2022; 14(5):1108. https://doi.org/10.3390/pharmaceutics14051108
Chicago/Turabian StyleWei, Ching-Ting, Yu-Wen Wang, Yu-Chiuan Wu, Li-Wei Lin, Chia-Chi Chen, Chun-Yin Chen, and Shyh-Ming Kuo. 2022. "Reparative Efficacy of Liposome-Encapsulated Oleanolic Acid against Liver Inflammation Induced by Fine Ambient Particulate Matter and Alcohol in Mice" Pharmaceutics 14, no. 5: 1108. https://doi.org/10.3390/pharmaceutics14051108