
Two Innovative Approaches to Optimize Vancomycin Dosing Using Estimated AUC after First Dose: Validation Using Data Generated from Population PK Model Coupled with Monte-Carlo Simulation and Comparison with the First-Order PK Equation Approach

Abstract
:1. Introduction
2. Methods
2.1. Literature Review and Model Selection
2.2. Monte Carlo Simulation of PK Profile in Patients with Normal Renal Function
2.3. Estimation of AUC Using Four Serum Concentrations (Method 1)
2.4. Estimation of AUC Using Three Serum Concentrations (Method 2)
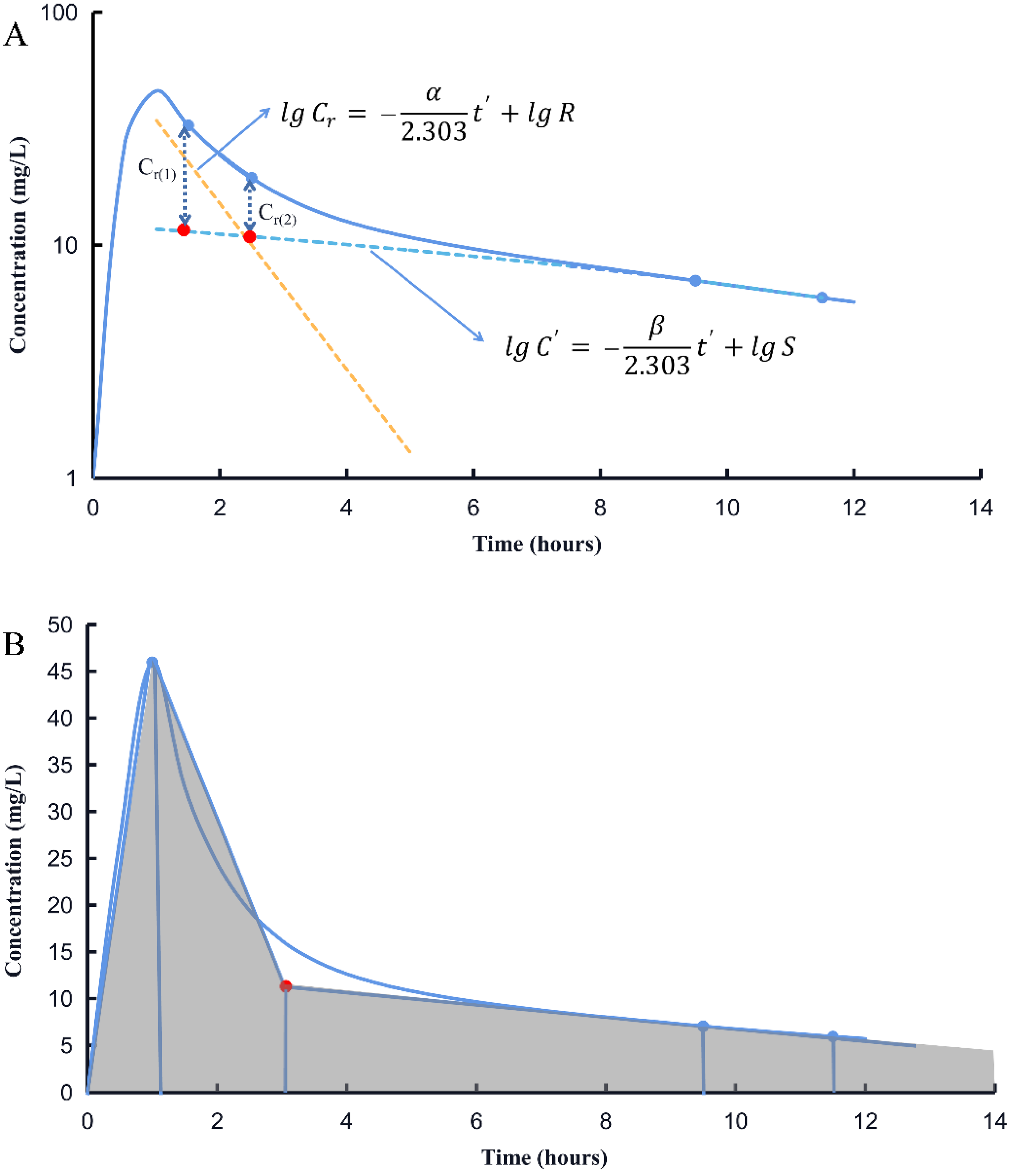
2.5. Estimation of AUC Using Two Serum Concentrations (Method 3)
- Step 1: Estimation of elimination rate constant (k)
- Step 2: Estimation of concentration at the end of infusion (Cmax)
- Step 3: Calculation of volume of distribution (Vd)
- Step 4: Calculation of clearance (CL)
- Step 5: Calculation of AUC0–∞
2.6. Method Evaluation
2.7. Extrapolation to Patients with Various Degrees of Renal Impairment and Method Evaluation
2.8. Sensitivity Analysis
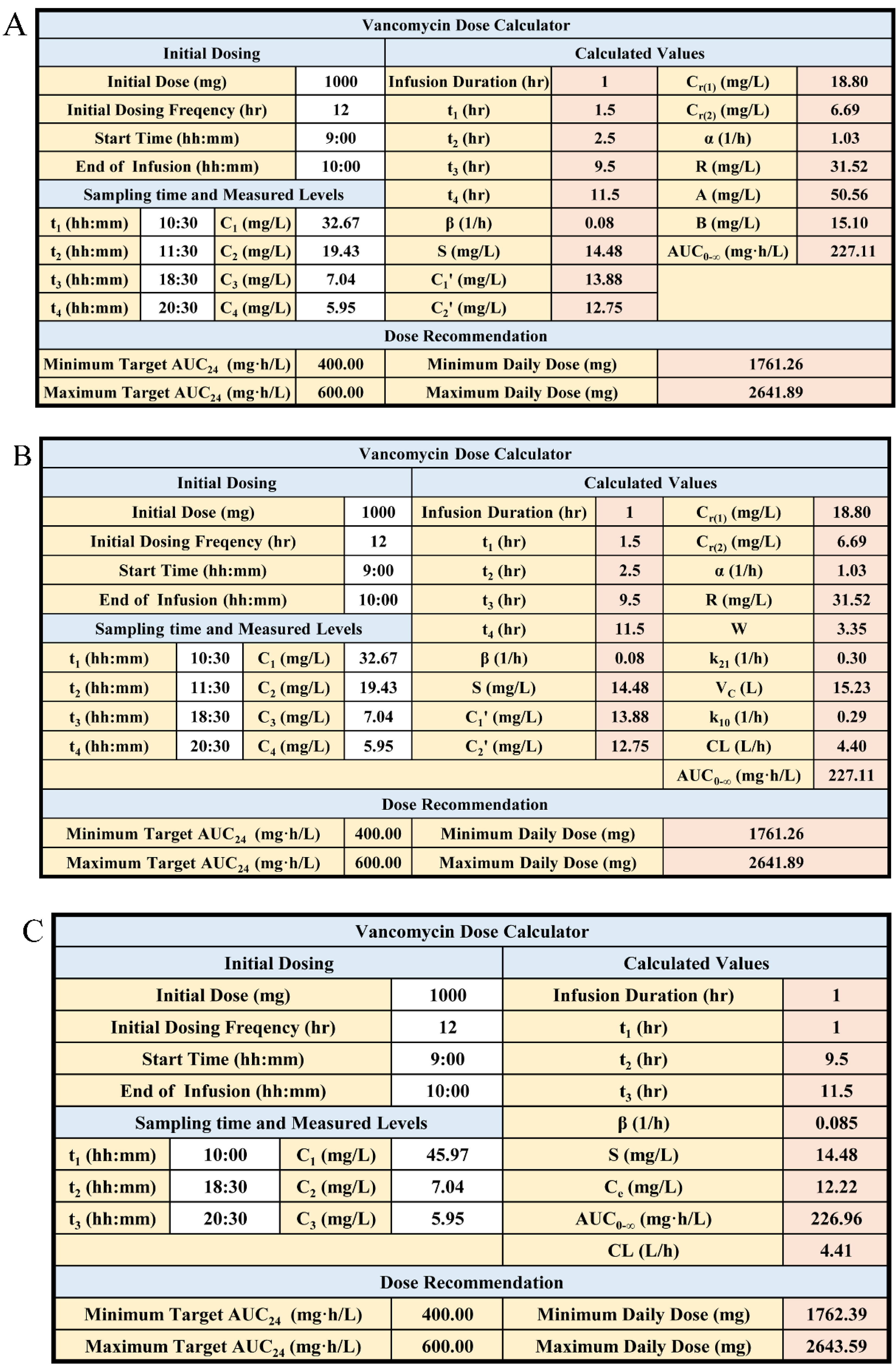
2.9. Development of the Dose Calculator Tool
3. Results
3.1. Literature Review and Model Selection
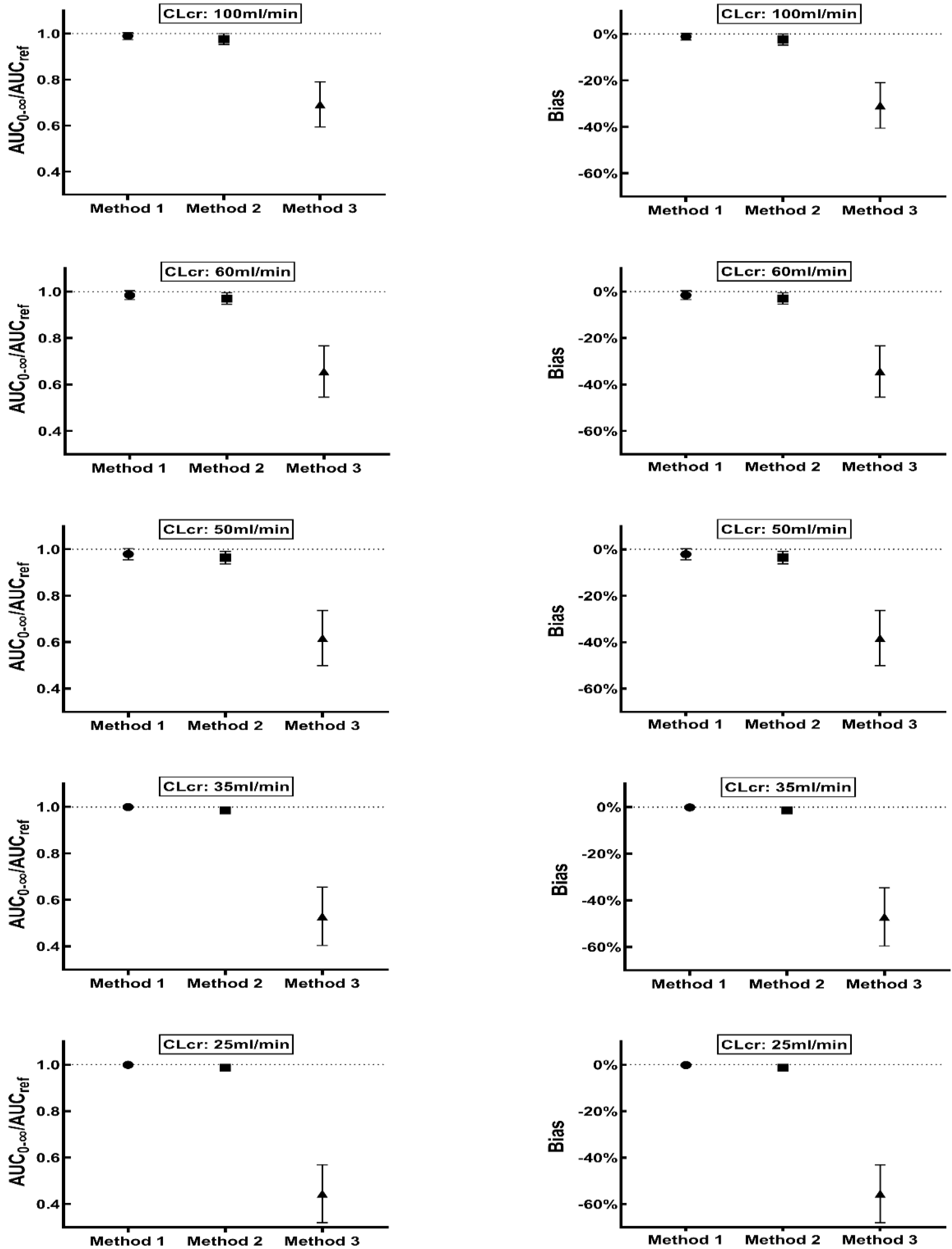
3.2. Monte Carlo Simulation and Method Evaluation
3.3. Method Evaluation in Patients with Various Degrees of Renal Impairment
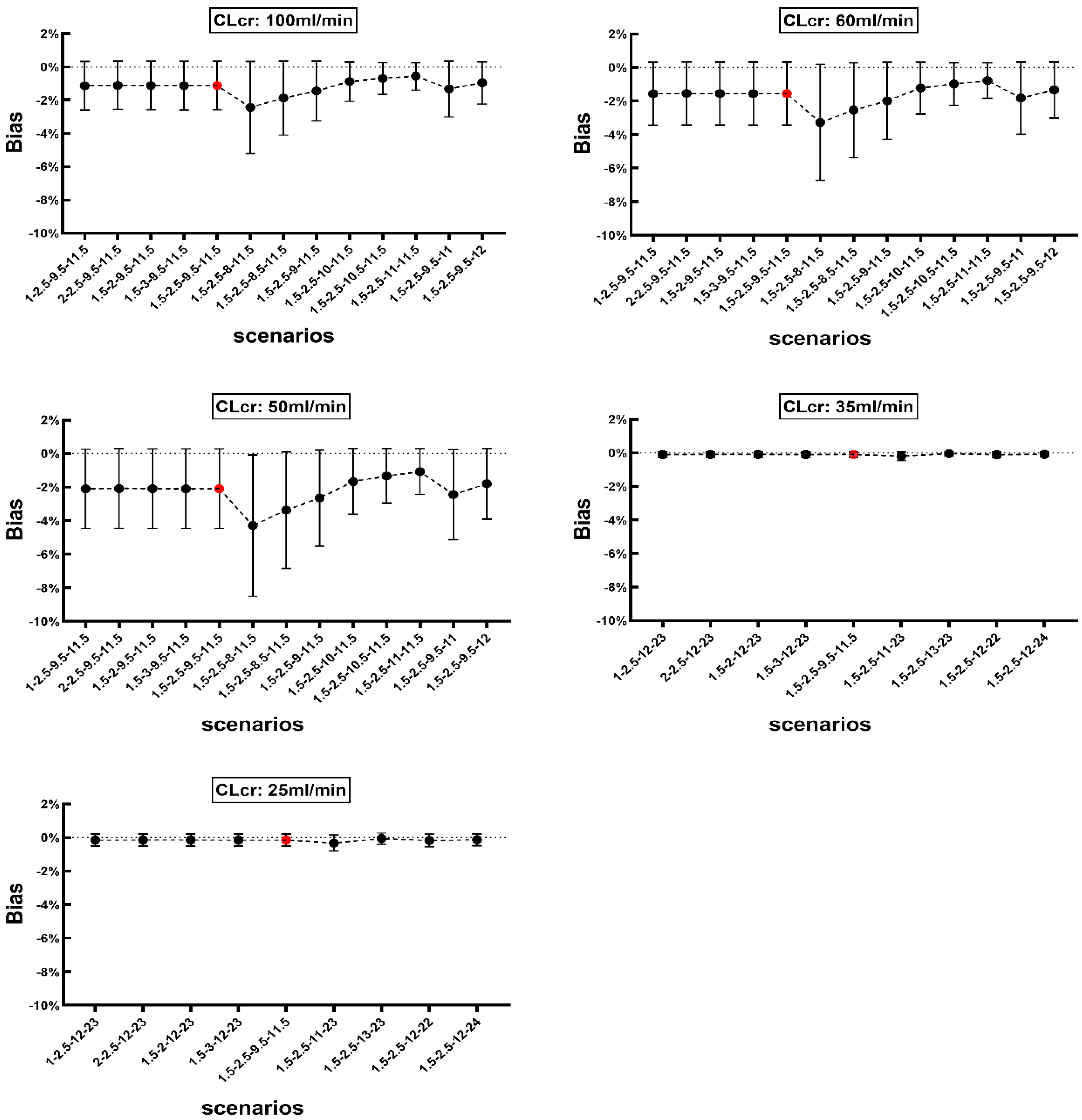
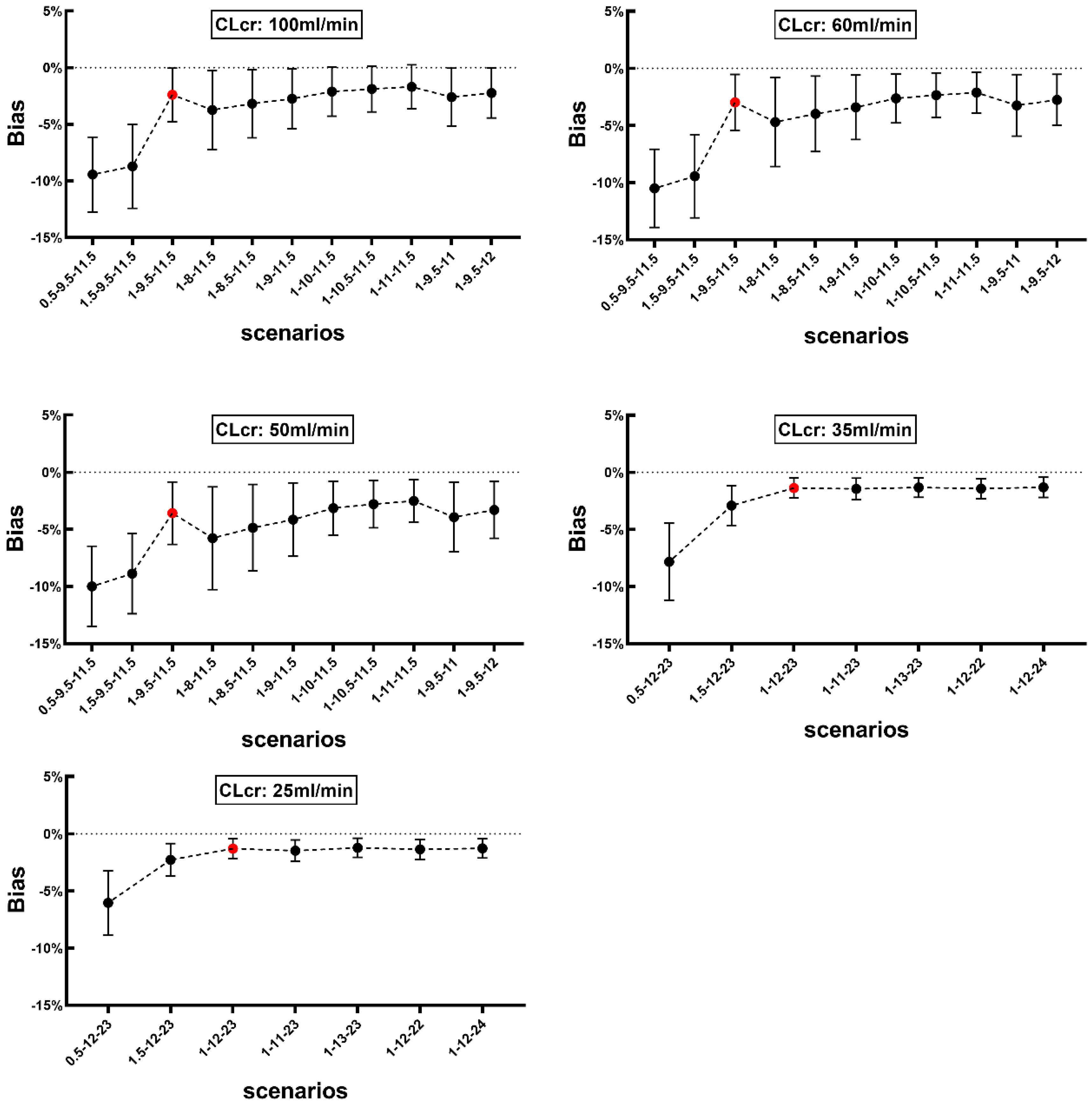
3.4. Sensitivity Analysis
3.5. Excel Calculator
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Filippone, E.J.; Kraft, W.K.; Farber, J.L. The Nephrotoxicity of Vancomycin. Clin. Pharmacol. Ther. 2017, 102, 459–469. [Google Scholar] [CrossRef]
- Heil, E.L.; Claeys, K.C.; Mynatt, R.P.; Hopkins, T.L.; Brade, K.; Watt, I.; Rybak, M.J.; Pogue, J.M. Making the change to area under the curve-based vancomycin dosing. Am. J. Health Syst. Pharm. 2018, 75, 1986–1995. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R., Jr.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef] [PubMed]
- Hermsen, E.D.; Hanson, M.; Sankaranarayanan, J.; Stoner, J.A.; Florescu, M.C.; Rupp, M.E. Clinical outcomes and nephrotoxicity associated with vancomycin trough concentrations during treatment of deep-seated infections. Expert Opin. Drug Saf. 2010, 9, 9–14. [Google Scholar] [CrossRef]
- Finch, N.A.; Zasowski, E.J.; Murray, K.P.; Mynatt, R.P.; Zhao, J.J.; Yost, R.; Pogue, J.M.; Rybak, M.J. A Quasi-Experiment to Study the Impact of Vancomycin Area under the Concentration-Time Curve-Guided Dosing on Vancomycin-Associated Nephrotoxicity. Antimicrob. Agents Chemother. 2017, 61, e01293-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tkachuk, S.; Collins, K.; Ensom, M.H.H. The Relationship between Vancomycin Trough Concentrations and AUC/MIC Ratios in Pediatric Patients: A Qualitative Systematic Review. Paediatr. Drugs 2018, 20, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Bel Kamel, A.; Bourguignon, L.; Marcos, M.; Ducher, M.; Goutelle, S. Is Trough Concentration of Vancomycin Predictive of the Area Under the Curve? A Clinical Study in Elderly Patients. Ther. Drug Monit. 2017, 39, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [Green Version]
- Neely, M.N.; Youn, G.; Jones, B.; Jelliffe, R.W.; Drusano, G.L.; Rodvold, K.A.; Lodise, T.P. Are vancomycin trough concentrations adequate for optimal dosing? Antimicrob. Agents Chemother. 2014, 58, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai, M.P.; Neely, M.; Rodvold, K.A.; Lodise, T.P. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv. Drug Deliv. Rev. 2014, 77, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelliffe, R.W.; Schumitzky, A. Modeling, adaptive control, and optimal drug therapy. Med. Prog. Technol. 1990, 16, 95–110. [Google Scholar] [PubMed]
- Bayard, D.S.; Jelliffe, R.W. A Bayesian approach to tracking patients having changing pharmacokinetic parameters. J. Pharm. Pharm. 2004, 31, 75–107. [Google Scholar] [CrossRef] [PubMed]
- Shingde, R.V.; Graham, G.G.; Reuter, S.E.; Carland, J.E.; Day, R.O.; Stocker, S.L. Comparison of the Area Under the Curve for Vancomycin Estimated Using Compartmental and Noncompartmental Methods in Adult Patients With Normal Renal Function. Ther. Drug Monit. 2019, 41, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Drennan, P.G.; Begg, E.J.; Gardiner, S.J.; Kirkpatrick, C.M.J.; Chambers, S.T. The dosing and monitoring of vancomycin: What is the best way forward? Int. J. Antimicrob. Agents 2019, 53, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Wong, T.; Huang, S.; Mui, E.; Nguyen, V.; Espinosa, G.; Desai, J.; Holubar, M.; Deresinski, S. Conversion from Vancomycin Trough Concentration-Guided Dosing to Area Under the Curve-Guided Dosing Using Two Sample Measurements in Adults: Implementation at an Academic Medical Center. Pharmacotherapy 2019, 39, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.N.; Goldman, J.L. A Moving Target-Vancomycin Therapeutic Monitoring. J. Pediatr. Infect. Dis. Soc. 2020, 9, 474–478. [Google Scholar] [CrossRef]
- Matzke, G.R.; Zhanel, G.G.; Guay, D.R. Clinical pharmacokinetics of vancomycin. Clin. Pharm. 1986, 11, 257–282. [Google Scholar] [CrossRef] [PubMed]
- Rotschafer, J.C.; Crossley, K.; Zaske, D.E.; Mead, K.; Sawchuk, R.J.; Solem, L.D. Pharmacokinetics of vancomycin: Observations in 28 patients and dosage recommendations. Antimicrob. Agents Chemother. 1982, 22, 391–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodvold, K.A.; Blum, R.A.; Fischer, J.H.; Zokufa, H.Z.; Rotschafer, J.C.; Crossley, K.B.; Riff, L.J. Vancomycin pharmacokinetics in patients with various degrees of renal function. Antimicrob. Agents Chemother. 1988, 32, 848–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.W.; Kim, D.J.; Zang, D.Y.; Lee, D.H. Effect of pharmacokinetic model misspecification on antibiotic probability of target attainment predicted by Monte Carlo simulation. Int. J. Clin. Pharmacol. Ther. 2019, 57, 362–374. [Google Scholar] [CrossRef]
- Flannery, A.H.; Delozier, N.L.; Effoe, S.A.; Wallace, K.L.; Cook, A.M.; Burgess, D.S. First-Dose Vancomycin Pharmacokinetics Versus Empiric Dosing on Area-Under-the-Curve Target Attainment in Critically Ill Patients. Pharmacotherapy 2020, 40, 1210–1218. [Google Scholar] [CrossRef]
- Smith, G.M.; Leyland, M.J.; Farrell, I.D.; Geddes, A.M. A clinical, microbiological and pharmacokinetic study of ciprofloxacin plus vancomycin as initial therapy of febrile episodes in neutropenic patients. J. Antimicrob. Chemother. 1988, 21, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, M.; Iga, T.; Zenda, H.; Okumura, K.; Oguma, T.; Yano, Y.; Hori, R. Population pharmacokinetics of vancomycin in Japanese adult patients. Ther. Drug Monit. 1998, 20, 139–148. [Google Scholar] [CrossRef]
- Stockmann, C.; Roberts, J.K.; Yu, T.; Constance, J.E.; Knibbe, C.A.; Spigarelli, M.G.; Sherwin, C.M. Vancomycin pharmacokinetic models: Informing the clinical management of drug-resistant bacterial infections. Expert Rev. Anti-Infect. Ther. 2014, 12, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Schaible, D.H.; Rocci, M.L., Jr.; Alpert, G.A.; Campos, J.M.; Paul, M.H.; Polin, R.A.; Plotkin, S.A. Vancomycin pharmacokinetics in infants: Relationships to indices of maturation. Pediatr. Infect. Dis. 1986, 5, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Schaad, U.B.; McCracken, G.H., Jr.; Nelson, J.D. Clinical pharmacology and efficacy of vancomycin in pediatric patients. J. Pediatr. 1980, 96, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.; Ho, D.H.; Fong, K.L.; Bogerd, L.; Maksymiuk, A.; Bolivar, R.; Fainstein, V.; Bodey, G.P. Effects of hepatic function on vancomycin clinical pharmacology. Antimicrob. Agents Chemother. 1983, 23, 603–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Normand, Y.; Milpied, N.; Kergueris, M.F.; Harousseau, J.L. Pharmacokinetic parameters of vancomycin for therapeutic regimens in neutropenic adult patients. Int. J. Biomed. Comput. 1994, 36, 121–125. [Google Scholar] [CrossRef]
- Pleasants, R.A.; Michalets, E.L.; Williams, D.M.; Samuelson, W.M.; Rehm, J.R.; Knowles, M.R. Pharmacokinetics of vancomycin in adult cystic fibrosis patients. Antimicrob. Agents Chemother. 1996, 40, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blevins, R.D.; Halstenson, C.E.; Salem, N.G.; Matzke, G.R. Pharmacokinetics of vancomycin in patients undergoing continuous ambulatory peritoneal dialysis. Antimicrob. Agents Chemother. 1984, 25, 603–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decker, B.S.; Kays, M.B.; Chambers, M.; Kraus, M.A.; Moe, S.M.; Sowinski, K.M. Vancomycin pharmacokinetics and pharmacodynamics during short daily hemodialysis. Clin. J. Am. Soc. Nephrol. 2010, 5, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Harford, A.M.; Sica, D.A.; Tartaglione, T.; Polk, R.E.; Dalton, H.P.; Poynor, W. Vancomycin pharmacokinetics in continuous ambulatory peritoneal dialysis patients with peritonitis. Nephron 1986, 43, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Garaud, J.J.; Regnier, B.; Inglebert, F.; Faurisson, F.; Bauchet, J.; Vachon, F. Vancomycin pharmacokinetics in critically ill patients. J. Antimicrob. Chemother. 1984, 14 (Suppl. D), 53–57. [Google Scholar] [CrossRef]
- Blouin, R.A.; Bauer, L.A.; Miller, D.D.; Record, K.E.; Griffen, W.O., Jr. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob. Agents Chemother. 1982, 21, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Lisby-Sutch, S.M.; Nahata, M.C. Dosage guidelines for the use of vancomycin based on its pharmacokinetics in infants. Eur. J. Clin. Pharmacol. 1988, 35, 637–642. [Google Scholar] [CrossRef]
- Healy, D.P.; Polk, R.E.; Garson, M.L.; Rock, D.T.; Comstock, T.J. Comparison of steady-state pharmacokinetics of two dosage regimens of vancomycin in normal volunteers. Antimicrob. Agents Chemother. 1987, 31, 393–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krogstad, D.J.; Moellering, R.C., Jr.; Greenblatt, D.J. Single-dose kinetics of intravenous vancomycin. J. Clin. Pharmacol. 1980, 20, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Cheung, R.P.; DiPiro, J.T. Vancomycin: An update. Pharmacotherapy 1986, 6, 153–169. [Google Scholar] [CrossRef]
- Levine, J.F. Vancomycin: A review. Med. Clin. N. Am. 1987, 71, 1135–1145. [Google Scholar] [CrossRef]
- Moffett, B.S.; Kim, S.; Edwards, M.S. Vancomycin dosing in obese pediatric patients. Clin. Pediatr. 2011, 50, 442–446. [Google Scholar] [CrossRef]
- Rybak, M.J.; Boike, S.C. Monitoring vancomycin therapy. Drug Intell. Clin. Pharm. 1986, 20, 757–761. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Gao, P.; Hu, J.; Chen, Y.; Zhang, L.; Shen, X.; Xu, H.; Xu, Q. Pharmacokinetic Characteristics and Clinical Outcomes of Vancomycin in Young Children With Various Degrees of Renal Function. J. Clin. Pharmacol. 2016, 56, 740–748. [Google Scholar] [CrossRef]
- Heffernan, A.J.; Germano, A.; Sime, F.B.; Roberts, J.A.; Kimura, E. Vancomycin population pharmacokinetics for adult patients with sepsis or septic shock: Are current dosing regimens sufficient? Eur. J. Clin. Pharmacol. 2019, 75, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Aiba, T.; Otsuka, T.; Suemaru, K.; Nishimiya, T.; Inoue, T.; Murase, M.; Kurosaki, Y.; Araki, H. Population pharmacokinetic analysis of vancomycin using serum cystatin C as a marker of renal function. Antimicrob. Agents Chemother. 2010, 54, 778–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.I. Design and power of a population pharmacokinetic study. Pharm. Res. 2001, 18, 75–82. [Google Scholar] [CrossRef]
- Ingerman, M.J.; Santoro, J. Vancomycin. A new old agent. Infect. Dis. Clin. N. Am. 1989, 3, 641–651. [Google Scholar] [CrossRef]
- Purwonugroho, T.A.; Chulavatnatol, S.; Preechagoon, Y.; Chindavijak, B.; Malathum, K.; Bunuparadah, P. Population pharmacokinetics of vancomycin in Thai patients. Sci. World J. 2012, 2012, 762649. [Google Scholar] [CrossRef] [PubMed]
- Oda, K.; Katanoda, T.; Hashiguchi, Y.; Kondo, S.; Narita, Y.; Iwamura, K.; Nosaka, K.; Jono, H.; Saito, H. Development and evaluation of a vancomycin dosing nomogram to achieve the target area under the concentration-time curve. A retrospective study. J. Infect. Chemother. 2020, 26, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Lee, D.H.; Ahn, S.; Jung, J.; Kiem, S.; Kim, S.W.; Shin, J.G. A new population pharmacokinetic model for vancomycin in patients with variable renal function: Therapeutic drug monitoring based on extended covariate model using CKD-EPI estimation. J. Clin. Pharm. Ther. 2019, 44, 750–759. [Google Scholar] [CrossRef]
- Ji, X.W.; Ji, S.M.; He, X.R.; Zhu, X.; Chen, R.; Lu, W. Influences of renal function descriptors on population pharmacokinetic modeling of vancomycin in Chinese adult patients. Acta Pharmacol. Sin. 2018, 39, 286–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, I.; Duan, J. Population pharmacokinetics with a very small sample size. Drug Metabol. Drug Interact. 2009, 24, 259–274. [Google Scholar] [CrossRef] [PubMed]
- Frymoyer, A.; Hersh, A.L.; Coralic, Z.; Benet, L.Z.; Joseph Guglielmo, B. Prediction of vancomycin pharmacodynamics in children with invasive methicillin-resistant Staphylococcus aureus infections: A Monte Carlo simulation. Clin. Ther. 2010, 32, 534–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodise, T.P., Jr.; Lomaestro, B.; Rodvold, K.A.; Danziger, L.H.; Drusano, G.L. Pharmacodynamic profiling of piperacillin in the presence of tazobactam in patients through the use of population pharmacokinetic models and Monte Carlo simulation. Antimicrob. Agents Chemother. 2004, 48, 4718–4724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef] [Green Version]
- He, N.; Su, S.; Ye, Z.; Du, G.; He, B.; Li, D.; Liu, Y.; Yang, K.; Zhang, X.; Zhang, Y.; et al. Evidence-based Guideline for Therapeutic Drug Monitoring of Vancomycin: 2020 Update by the Division of Therapeutic Drug Monitoring, Chinese Pharmacological Society. Clin. Infect. Dis. 2020, 71, S363–S371. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.; Almatrafi, A.; Bin Aydan, N.; Alqahtani, M.; Alzamil, F.; Alsultan, A.; Asiri, Y. Optimization of Vancomycin Dosing Regimen in Cancer Patients using Pharmacokinetic/Pharmacodynamic Modeling. Pharmacotherapy 2020, 40, 1192–1200. [Google Scholar] [CrossRef]
- Hamada, Y.; Kuti, J.L.; Nicolau, D.P. Vancomycin serum concentrations do not adequately predict tissue exposure in diabetic patients with mild to moderate limb infections. J. Antimicrob. Chemother. 2015, 70, 2064–2067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, Q.; Ye, Y.; Zhu, Y.L.; Cheng, J.; Yang, H.F.; Liu, Y.Y.; Li, H.R.; Li, J.B. Use of Monte Carlo simulation to evaluate the development of vancomycin resistance in meticillin-resistant Staphylococcus aureus. Int. J. Antimicrob. Agents 2015, 45, 652–656. [Google Scholar] [CrossRef]
- Tsai, D.; Stewart, P.C.; Hewagama, S.; Krishnaswamy, S.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Optimised dosing of vancomycin in critically ill Indigenous Australian patients with severe sepsis. Anaesth. Intensiv. Care 2018, 46, 374–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prybylski, J.P. A Strategy for Dosing Vancomycin to Therapeutic Targets Using Only Trough Concentrations. Clin. Pharm. 2017, 56, 263–272. [Google Scholar] [CrossRef]
- Wrishko, R.E.; Levine, M.; Khoo, D.; Abbott, P.; Hamilton, D. Vancomycin pharmacokinetics and Bayesian estimation in pediatric patients. Ther. Drug Monit. 2000, 22, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, B.H.; Olsen, K.M.; Padilla, C.B. Errors in assuming a one-compartment model for vancomycin. Ther. Drug Monit. 1990, 12, 304–305. [Google Scholar] [PubMed]
- Sobiak, J.; Resztak, M.; Chrzanowska, M.; Zachwieja, J.; Ostalska-Nowicka, D. The Evaluation of Multiple Linear Regression-Based Limited Sampling Strategies for Mycophenolic Acid in Children with Nephrotic Syndrome. Molecules 2021, 26, 3723. [Google Scholar] [CrossRef]
- Dadkhah, A.; Alihodzic, D.; Broeker, A.; Kroger, N.; Langebrake, C.; Wicha, S.G. Evaluation of the Robustness of Therapeutic Drug Monitoring Coupled with Bayesian Forecasting of Busulfan with Regard to Inaccurate Documentation. Pharm. Res. 2021, 38, 1721–1729. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CLcr (mL/min) | Time Reaching SS (day) | Dosage (mg) | Dosing Interval (h) | Infusion Rate (mg/h) | Sampling Time (h) | |
|---|---|---|---|---|---|---|
| Method 1 | Method 2 | |||||
| 100 | 15 | 1000 | 12 | 1000 | 1.5, 2.5, 9.5, 11.5 | 1, 9.5, 11.5 |
| 60 | 30 | 750 | 12 | 750 | 1.5, 2.5, 9.5, 11.5 | 1, 9.5, 11.5 |
| 50 | 30 | 500 | 12 | 500 | 1.5, 2.5, 9.5, 11.5 | 1, 9.5, 11.5 |
| 35 | 30 | 750 | 24 | 750 | 1.5, 2.5, 12, 23 | 1, 12, 23 |
| 25 | 30 | 500 | 24 | 500 | 1.5, 2.5, 12, 23 | 1, 12, 23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Q.; Huang, H.; Xu, B.; Li, D.; Liu, M.; Shaik, I.H.; Wu, X. Two Innovative Approaches to Optimize Vancomycin Dosing Using Estimated AUC after First Dose: Validation Using Data Generated from Population PK Model Coupled with Monte-Carlo Simulation and Comparison with the First-Order PK Equation Approach. Pharmaceutics 2022, 14, 1004. https://doi.org/10.3390/pharmaceutics14051004
Liu Q, Huang H, Xu B, Li D, Liu M, Shaik IH, Wu X. Two Innovative Approaches to Optimize Vancomycin Dosing Using Estimated AUC after First Dose: Validation Using Data Generated from Population PK Model Coupled with Monte-Carlo Simulation and Comparison with the First-Order PK Equation Approach. Pharmaceutics. 2022; 14(5):1004. https://doi.org/10.3390/pharmaceutics14051004
Chicago/Turabian StyleLiu, Qingxia, Huiping Huang, Baohua Xu, Dandan Li, Maobai Liu, Imam H. Shaik, and Xuemei Wu. 2022. "Two Innovative Approaches to Optimize Vancomycin Dosing Using Estimated AUC after First Dose: Validation Using Data Generated from Population PK Model Coupled with Monte-Carlo Simulation and Comparison with the First-Order PK Equation Approach" Pharmaceutics 14, no. 5: 1004. https://doi.org/10.3390/pharmaceutics14051004