
Anti-Psoriasis Effect of Diclofenac and Celecoxib Using the Tail Model for Psoriasis


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Substances
2.3. Experimental Design
2.3.1. Animal Groups
- Group 1: negative control (untreated mice)
- Group 2: negative control (white soft paraffin)
- Group 3: positive control (tretinoin 0.05%)
- Group 4: test 1—diclofenac 1%
- Group 5: test 2—diclofenac 2%
- Group 6: test 3—celecoxib 1%
- Group 7: test 4—celecoxib 2%
2.3.2. Experimental Protocol
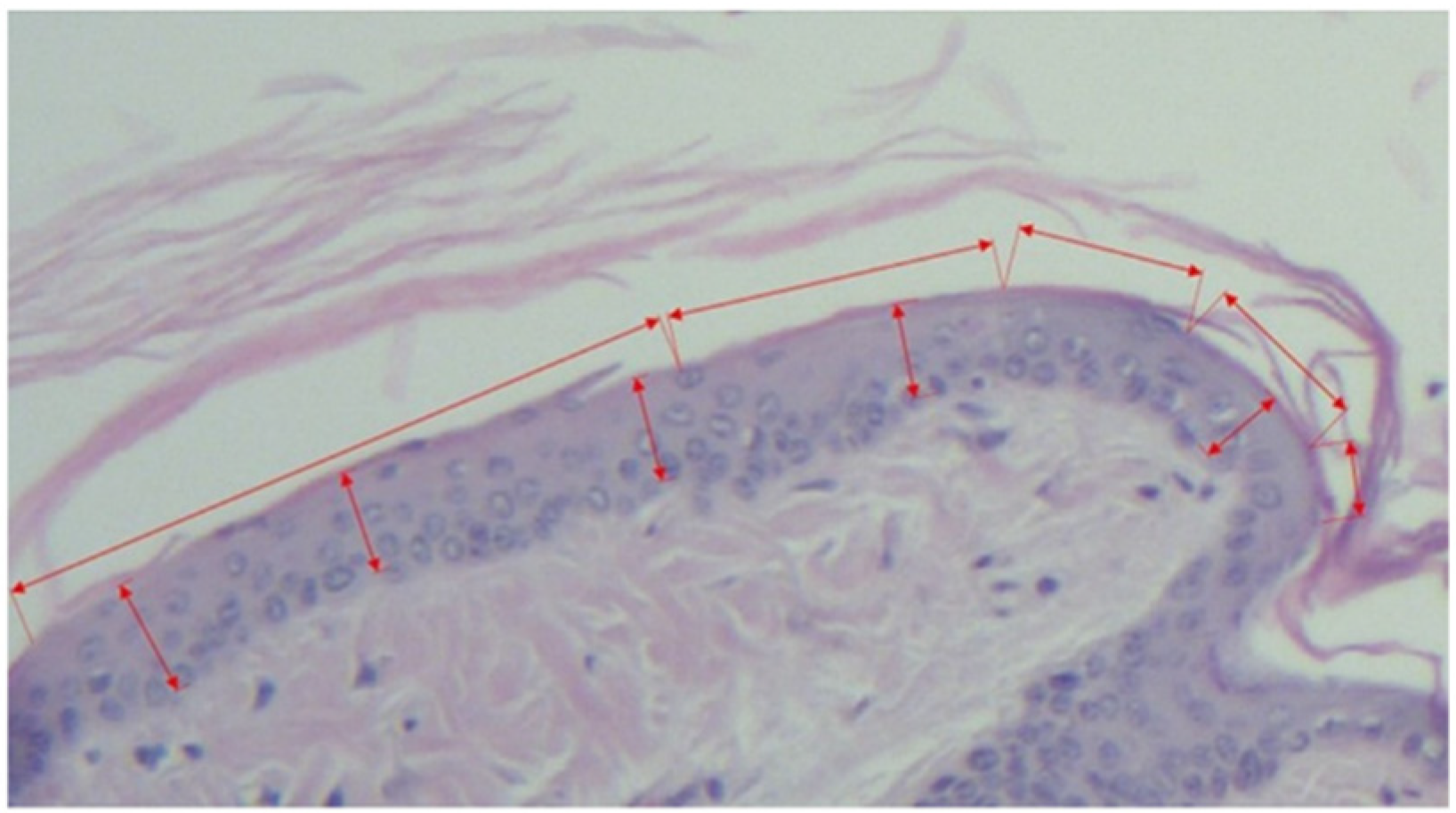
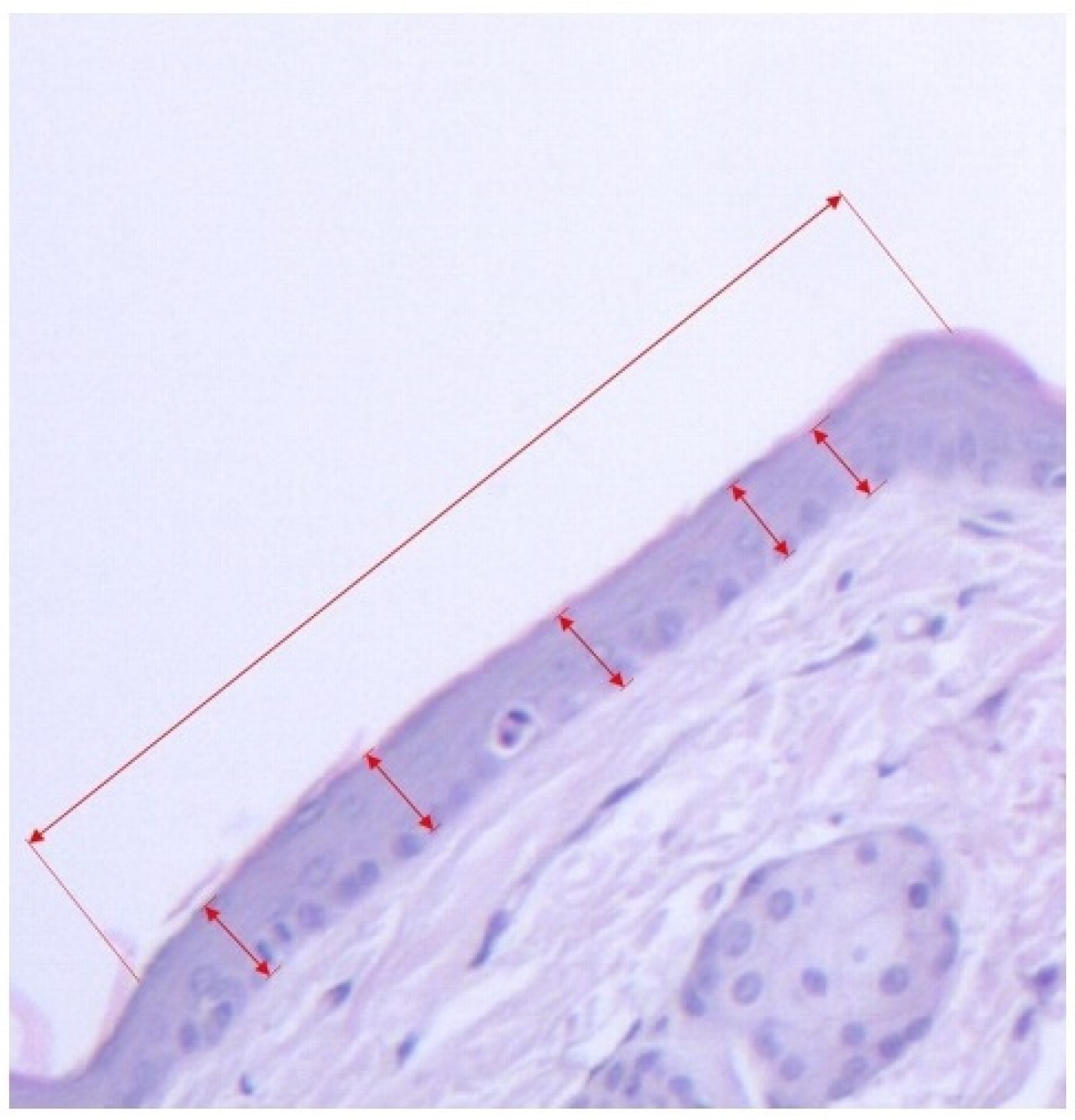
2.3.3. Morphometric Assessment
- A.
- B.
- Horizontal length of the scale, measured as the distance between two follicles including the sebaceous gland (see Figure 1 and Figure 3).From the values obtained at A-B the secondary parameters were obtained [4]:
- C.
- The degree of orthokeratosis of the individual scale, measured as the percentual value of A divided by B. For orthokeratosis degree determination, 10 horizontal scales per animal were measured, 60 scales per group. The dimensions were calculated in micrometers.
- D.
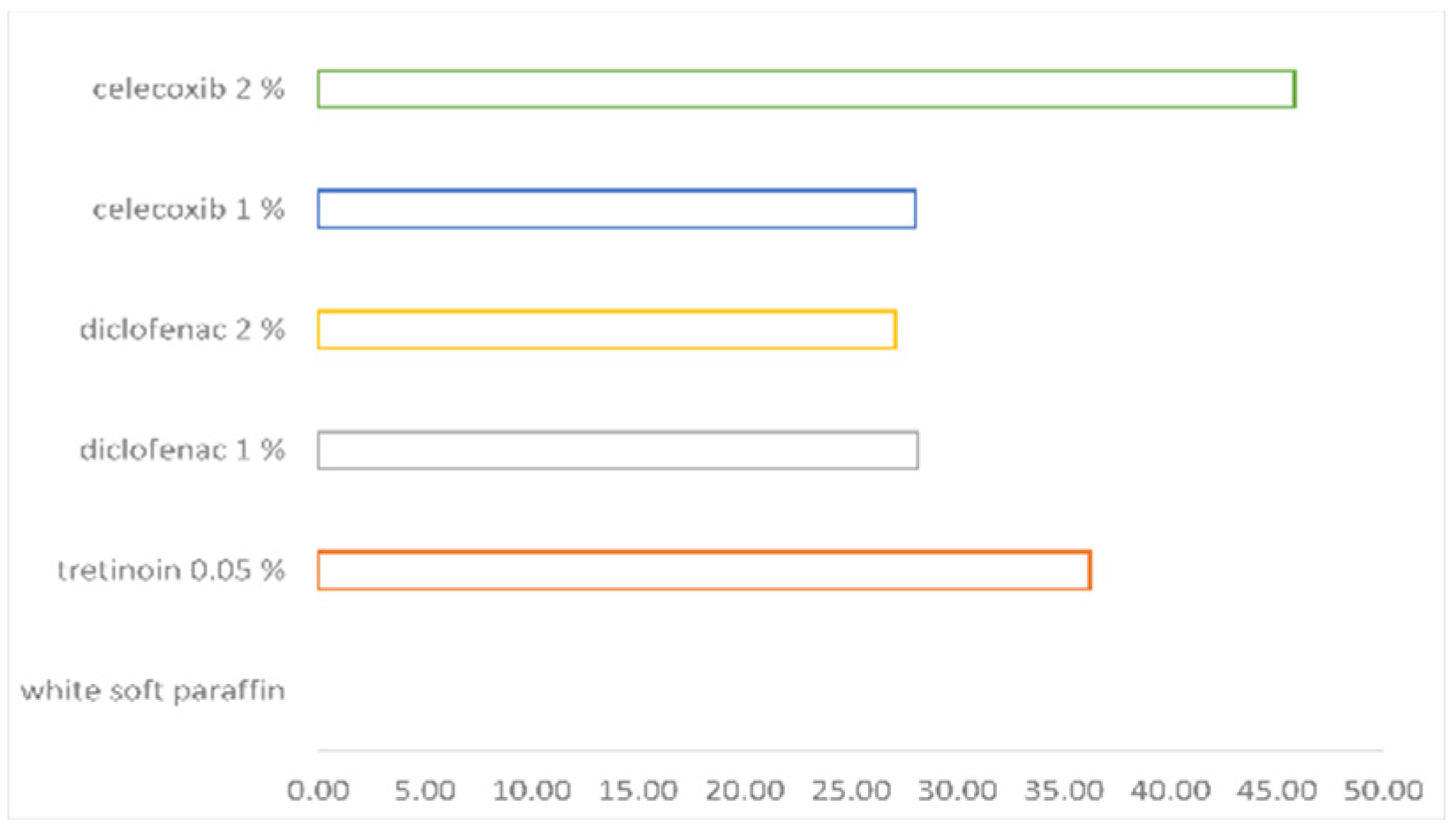
- The percentual drug activity was measured as (Oks − Okc)/(100 − Okc) × 100Oks = orthokeratosis as mean of the values obtained at D for the test substance (s)andOkc = orthokeratosis as mean of the values obtained at D for the negative control group 2 (c)—white soft paraffin
- E.
- F.
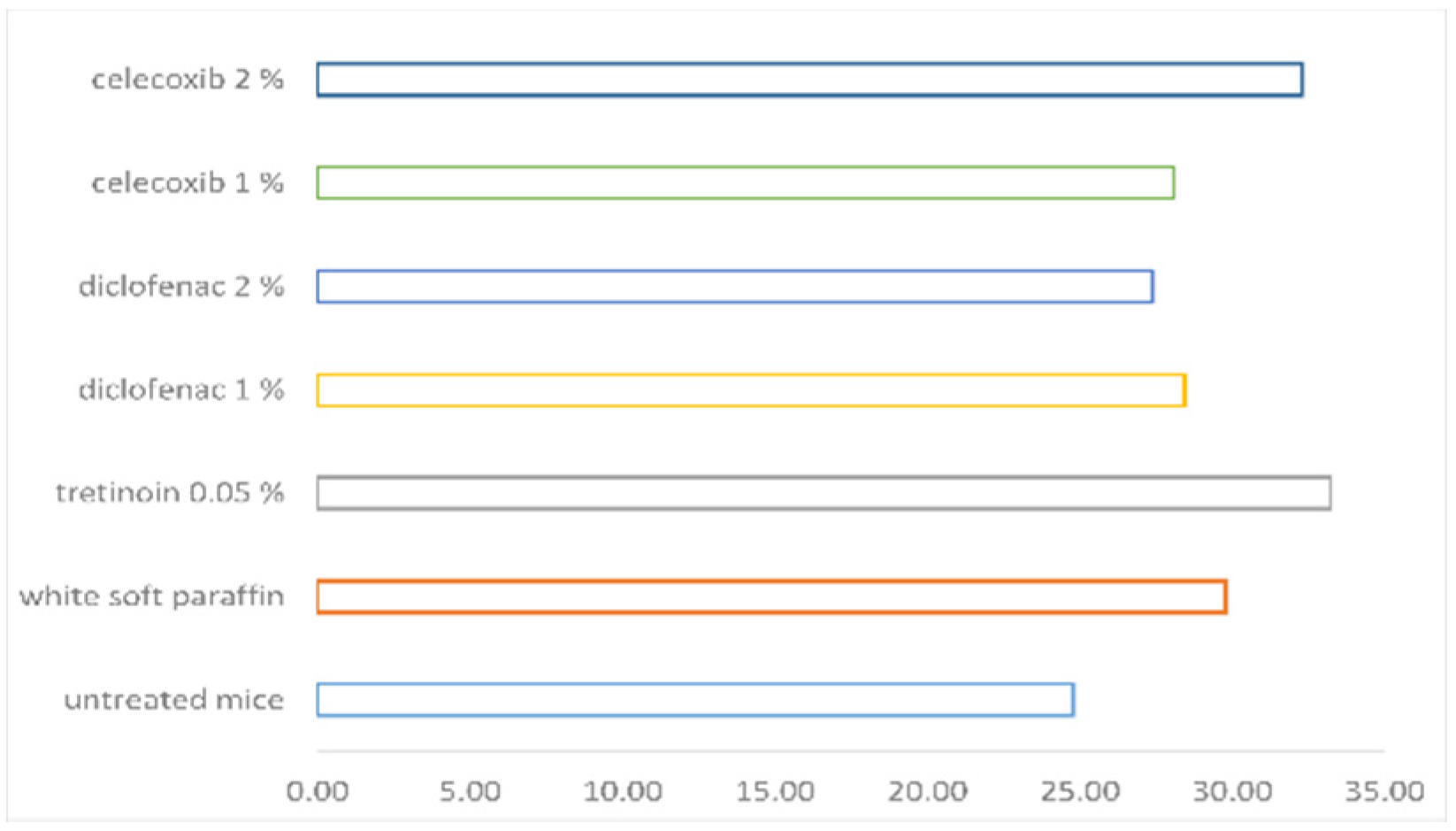
- Mean epidermal thickness of the individual scale (between two pilous follicles). For mean epidermal thickness, 5 measurements were made in each of the 10 scales, resulting in 300 measurements per group. The dimensions were calculated in micrometers.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amoruso, G.F.; Nisticò, S.P.; Iannone, L.; Russo, E.; Rago, G.; Patruno, C.; Bennardo, L. Ixekizumab May Improve Renal Function in Psoriasis. Healthcare 2021, 9, 543. [Google Scholar] [CrossRef] [PubMed]
- Dattola, A.; Silvestri, M.; Tamburi, F.; Amoruso, G.F.; Bennardo, L.; Nisticò, S.P. Emerging Role of anti-IL23 in the Treatment of Psoriasis: When Humanized Is Very Promising. Dermatol. Ther. 2020, 33, e14504. [Google Scholar] [CrossRef] [PubMed]
- Dastoli, S.; Nisticò, S.P.; Morrone, P.; Patruno, C.; Leo, A.; Citraro, R.; Gallelli, L.; Russo, E.; De Sarro, G.; Bennardo, L. Colchicine in Managing Skin Conditions: A Systematic Review. Pharmaceutics 2022, 14, 294. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhof, P.; Kragballe, K. Recommendations for the Topical Treatment of Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2005, 19, 495–499. [Google Scholar] [CrossRef]
- Nițescu, D.; Mușetescu, A.; Nițescu, M.; Costescu, M.; Coman, O. Experimental Research in Topical Psoriasis Therapy (Review). Exp. Ther. Med. 2021, 22, 971. [Google Scholar] [CrossRef]
- Basir, H.; Alirezaei, P.; Hamian, Z.; Khanlarzadeh, E. Are Quantitative Histopathologic Criteria Capable of Differentiating Psoriasis from Chronic Dermatitis? Clin. Cosmet. Investig. Dermatol. 2018, 11, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Cho, E.; Park, E.; Park, H.; Kim, K.; Kim, K. The Histopathological Differentiation between Palmar Psoriasis and Hand Eczema: A Retrospective Review of 96 Cases. J. Am. Acad. Dermatol. 2017, 77, 130–135. [Google Scholar] [CrossRef]
- Bakry, O.; Samaka, R.; Shoeib, M.; Abdel Aal, S. Nuclear Factor Kappa B and Cyclo-Oxygenase-2: Two Concordant Players in Psoriasis Pathogenesis. Ultrastruct. Pathol. 2015, 39, 49–61. [Google Scholar] [CrossRef]
- Thomas, G.; Herranz, P.; Balta Cruz, S.; Parodi, A. Treatment of Actinic Keratosis through Inhibition of Cyclooxygenase-2: Potential Mechanism of Action of Diclofenac Sodium 3% in Hyaluronic Acid 2.5%. Dermatol. Ther. 2019, 32, e12800. [Google Scholar] [CrossRef]
- Costescu, M.; Coman, O.; Tampa, M.; Tudose, I.; Coman, L.; Georgescu, S. Axillary Basal Cell Carcinoma—A Rare Form of a Frequent Kind of Carcinoma. Romanian J. Morphol. Embryol. 2013, 54, 851–856. [Google Scholar]
- Nelson, C.G. Diclofenac Gel in the Treatment of Actinic Keratoses. Ther. Clin. Risk Manag. 2011, 7, 207–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordero, J.A.; Camacho, M.; Obach, R.; Domenech, J.; Vila, L. In Vitro Based Index of Topical Anti-Inflammatory Activity to Compare a Series of NSAIDs. Eur. J. Pharm. Biopharm. 2001, 51, 135–142. [Google Scholar] [CrossRef]
- Chun, K.; Kim, S.; Song, Y.; Surh, Y. Celecoxib Inhibits Phorbol Ester-Induced Expression of COX-2 and Activation of AP-1 and P38 MAP Kinase in Mouse Skin. Carcinogenesis 2004, 25, 713–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Thorn, F.; Bertagnolli, M.; Grosser, T.; Altman, R.; Klein, T.; Li, G.; Thorn, F.C.; Bertagnolli, M.M. Celecoxib Pathways: Pharmacokinetics and Pharmacodynamics. Pharm. Genom. 2012, 22, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Bosman, B. Testing of Lipoxygenase Inhibitors, Cyclooxygenase Inhibitors, Drugs with Immunomodulating Properties and Some Reference Antipsoriatic Drugs in the Modified Mouse Tail Test, an Animal Model of Psoriasis. Skin Pharmacol. 1994, 7, 324–334. [Google Scholar] [CrossRef]
- Schön, P.; Manzke, V.; Erpenbeck, L. Animal Models of Psoriasis—Highlights and Drawbacks. J. Allergy Clin. Immunol. 2021, 147, 439–455. [Google Scholar] [CrossRef]
- Bosman, B.; Matthiesen, T.; Hess, V.; Friderichs, E. Quantitative Method for Measuring Antipsoriatic Activity of Drugs by the Mouse Tail Test. Skin Pharmacol. 1992, 5, 41–48. [Google Scholar] [CrossRef]
- Campione, E.; Paternò, E.; Candi, E.; Falconi, M.; Constanza, G.; Diluvio, L.; Terrinoni, A.; Bianchi, L.; Orlandi, A. The Relevance of Piroxicam for the Prevention and Treatment of Nonmelanoma Skin Cancer and Its Precursors. Drug Des. Dev. Ther. 2015, 9, 5843–5850. [Google Scholar] [CrossRef] [Green Version]
- Hagen, M.; Baker, M. Skin Penetration and Tissue Permeation after Topical Administration of Diclofenac. Curr. Med. Res. Opin. 2017, 33, 1623–1634. [Google Scholar] [CrossRef] [Green Version]
- Szymański, Ł.; Skopek, R.; Palusińska, M.; Schenk, T.; Stengel, S.; Lewicki, S.; Kraj, L.; Kamiński, P.; Zelent, A. Retinoic Acid and Its Derivatives in Skin. Cells 2020, 9, 2660. [Google Scholar] [CrossRef]
- Chen, J.; Ma, Y.; Tao, Y.; Zhao, X.; Xiong, Y.; Chen, Z.; Tian, Y. Formulation and Evaluation of a Topical Liposomal Gel Containing a Combination of Zedoary Turmeric Oil and Tretinoin for Psoriasis Activity. J. Liposome Res. 2021, 31, 130–144. [Google Scholar] [CrossRef] [PubMed]
- Kang, S. The Mechanism of Action of Topical Retinoids. Cutis 2005, 75 (Suppl. 2), 10–13. [Google Scholar] [PubMed]
- Huang, P.; Chandra, V.; Rastinejad, F. Retinoic Acid Actions Through Mammalian Nuclear Receptors. Chem. Rev. 2014, 114, 233–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, K.M.; Rundhaug, E.; Fischer, S. Multiple Signaling Pathways Are Responsible for Prostaglandin E2–Induced Murine Keratinocyte Proliferation. Mol. Cancer Res. 2008, 6, 1003–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolae, I.; Nicolae, C.; Coman, O.; Stefanescu, M.; Coman, L.; Ardeleanu, C. Serum Total Gangliosides Level: Clinical Prognostic Implication. Romanian J. Morphol. Embryol. 2011, 52, 1277–1281. [Google Scholar]
- Maldve, R.; Kim, Y.; Muga, S.; Fischer, S. Prostaglandin E2 Regulation of Cyclooxygenase Expression in Keratinocytes Is Mediated via Cyclic Nucleotide-Linked Prostaglandin Receptors. J. Lipid Res. 2000, 41, 873–881. [Google Scholar] [CrossRef]
- Sticozzi, C.; Belmonte, B.; Cervellati, F.; Di Capua, A.; Valacchi, G. Antiproliferative Effect of Two Novel COX-2 Inhibitors on Human Keratinocytes. Eur. J. Pharm. Sci. 2013, 49, 133–141. [Google Scholar] [CrossRef]
- Nicolae, I.; Caragheorgheopol, A.; Schipor, S.; Nicolae, C.; Paun, D.; Coman, O.; Benea, V. Gangliosides and Sex Hormones in Human Melanoma. Acta Endocrinol. 2011, 7, 337–344. [Google Scholar]
- Chang, S.; Ai, Y.; Breyer, R.; Lane, T.; Hla, T. The Prostaglandin E2 Receptor EP2 Is Required for Cyclooxygenase 2-Mediated Mammary Hyperplasia. Cancer Res. 2005, 65, 4496–4499. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; Kim, T.H.; Kim, H.I.; Shin, Y.K.; Lee, C.S.; Park, M.; Song, J.-H. Celecoxib Inhibits Na+ Currents in Rat Dorsal Root Ganglion Neurons. Brain Res. 2007, 1148, 53–61. [Google Scholar] [CrossRef]
- Frolov, R.V.; Singh, S. Evidence of More Ion Channels Inhibited by Celecoxib: KV1.3 and L-Type Ca2+ Channels. BMC Res. Notes 2015, 8, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ORTHOKERATOSIS DEGREE | MEAN EPIDERMAL THICKNESS | PERCENTUAL DRUG ACTIVITY | |
|---|---|---|---|
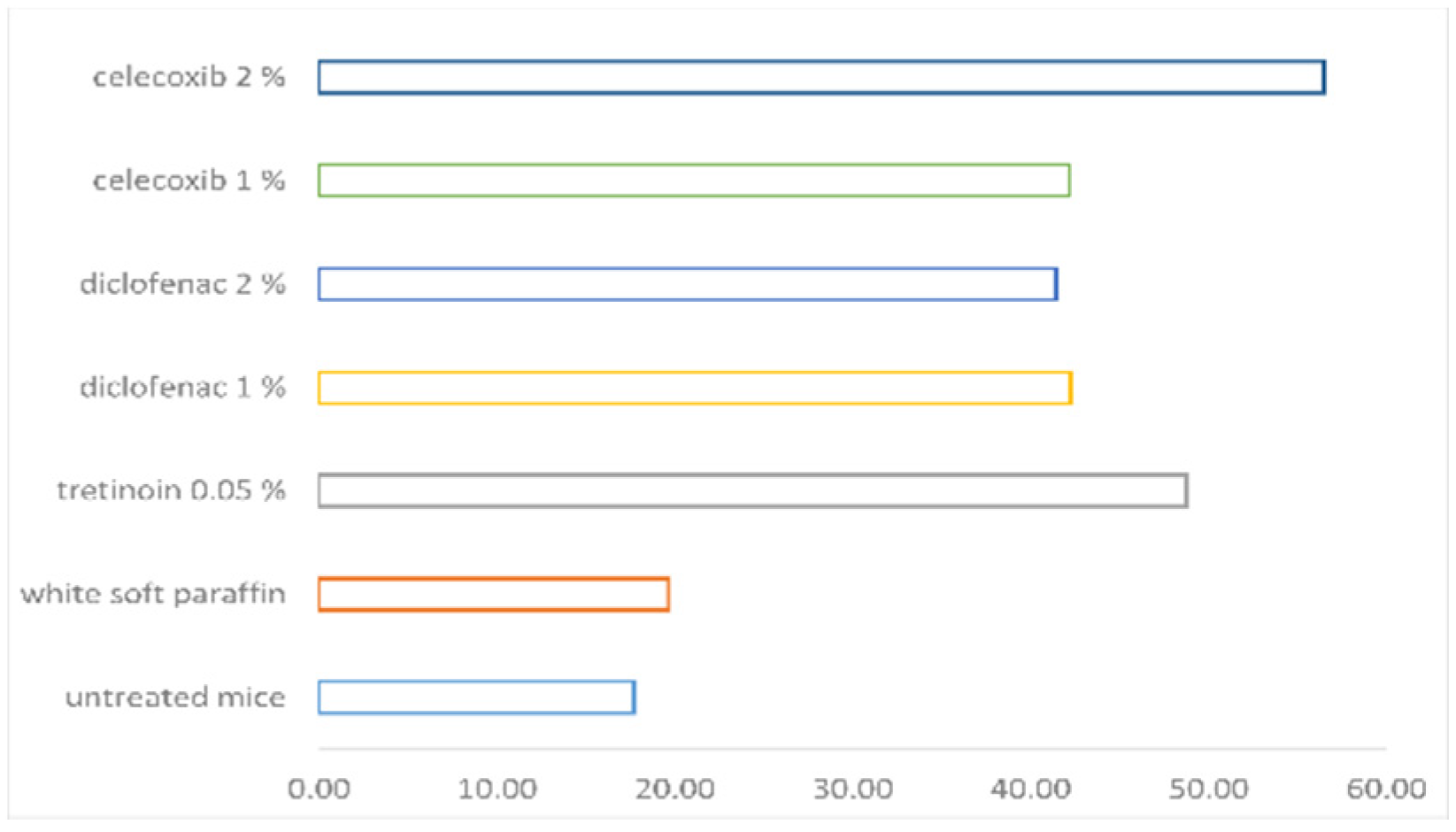
| UNTREATED MICE | 17.7 ± 1.81 | 24.77 ± 2.43 | |
| WHITE SOFT PARAFFIN | 19.64 ± 3.2 | 29.76 ± 2.02 | 0 |
| TRETINOIN 0.05% | 48.72 ± 6.09 | 33.22 ± 2.61 | 36.19 |
| DICLOFENAC 1% | 42.24 ± 13.73 | 28.42 ± 2.62 | 28.12 |
| DICLOFENAC 2% | 41.42 ± 8.17 | 27.38 ± 2.75 | 27.10 |
| CELECOXIB 1% | 42.15 ± 7.28 | 28.07 ± 2.37 | 28.01 |
| CELECOXIB 2% | 56.48 ± 11.33 | 32.28 ± 6.18 | 45.84 |
| Gropus | Untreated Mice | White Soft Paraffin | Tretinoin 0.05% | Diclofenac 1% | Diclofenac 2% | Celecoxib 1% | Celecoxib 2% |
|---|---|---|---|---|---|---|---|
| Untreated mice | N (0.361) | S (0.006) | S (0.006) | S (0.006) | S (0.006) | S (0.006) | |
| White soft paraffin | N (0.361) | S (0.004) | S (0.004) | S (0.004) | S (0.004) | S (0.004) | |
| Tretinoin 0.05% | S (0.006) | S (0.004) | N (0.109) | N (0.262) | N (0.337) | N (0.337) | |
| Diclofenac 1% | S (0.006) | S (0.004) | N (0.109) | N (0.837) | N (0.423) | N (0.055) | |
| Diclofenac 2% | S (0.006) | S (0.004) | N (0.262) | N (0.837) | N (1) | N (0.055) | |
| Celecoxib 1% | S (0.006) | S (0.004) | N (0.337) | N (0.423) | N (1) | N (0.055) | |
| Celecoxib 2% | S (0.006) | S (0.004) | N (0.337) | N (0.055) | N (0.055) | N (0.055) |
| Gropus | Untreated Mice | White Soft Paraffin | Tretinoin 0.05% | Diclofenac 1% | Diclofenac 2% | Celecoxib 1% | Celecoxib 2% |
|---|---|---|---|---|---|---|---|
| Untreated mice | S (0.018) | S (0.006) | N (0.1) | N (0.201) | S (0.045) | S (0.028) | |
| White soft paraffin | S (0.018) | N (0.078) | N (0.423) | N (0.055) | N (0.262) | N (1) | |
| Tretinoin 0.05% | S (0.006) | N (0.078) | S (0.037) | S (0.016) | S (0.025) | N (0.337) | |
| Diclofenac 1% | N (0.1) | N (0.423) | S (0.037) | N (0.631) | N (0.749) | N (0.337) | |
| Diclofenac 2% | N (0.201) | N (0.055) | S (0.016) | N (0.631) | N (0.631) | N (0.078) | |
| Celecoxib 1% | S (0.045) | N (0.262) | S (0.025) | N (0.749) | N (0.631) | N (0.262) | |
| Celecoxib 2% | S (0.028) | N (1) | N (0.337) | N (0.337) | N (0.078) | N (0.262) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nițescu, D.A.-M.; Păunescu, H.; Ștefan, A.E.; Coman, L.; Georgescu, C.C.; Stoian, A.C.; Gologan, D.; Fulga, I.; Coman, O.A. Anti-Psoriasis Effect of Diclofenac and Celecoxib Using the Tail Model for Psoriasis. Pharmaceutics 2022, 14, 885. https://doi.org/10.3390/pharmaceutics14040885
Nițescu DA-M, Păunescu H, Ștefan AE, Coman L, Georgescu CC, Stoian AC, Gologan D, Fulga I, Coman OA. Anti-Psoriasis Effect of Diclofenac and Celecoxib Using the Tail Model for Psoriasis. Pharmaceutics. 2022; 14(4):885. https://doi.org/10.3390/pharmaceutics14040885
Chicago/Turabian StyleNițescu, Diana Ana-Maria, Horia Păunescu, Alina Elena Ștefan, Laurențiu Coman, Corneliu Cristian Georgescu, Andrei Constantin Stoian, Daniela Gologan, Ion Fulga, and Oana Andreia Coman. 2022. "Anti-Psoriasis Effect of Diclofenac and Celecoxib Using the Tail Model for Psoriasis" Pharmaceutics 14, no. 4: 885. https://doi.org/10.3390/pharmaceutics14040885