
Fabrication and In Vitro/In Vivo Appraisal of Metronidazole Intra-Gastric Buoyant Sustained-Release Tablets in Healthy Volunteers



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Formulation of Metronidazole Floating Tablets
2.2.2. Effect of Hydrogel Composition on Buoyancy
2.2.3. Effect of Tablet Weight on Buoyancy
2.2.4. Effect of Hardness in Relation to Tablet Weight on Buoyancy
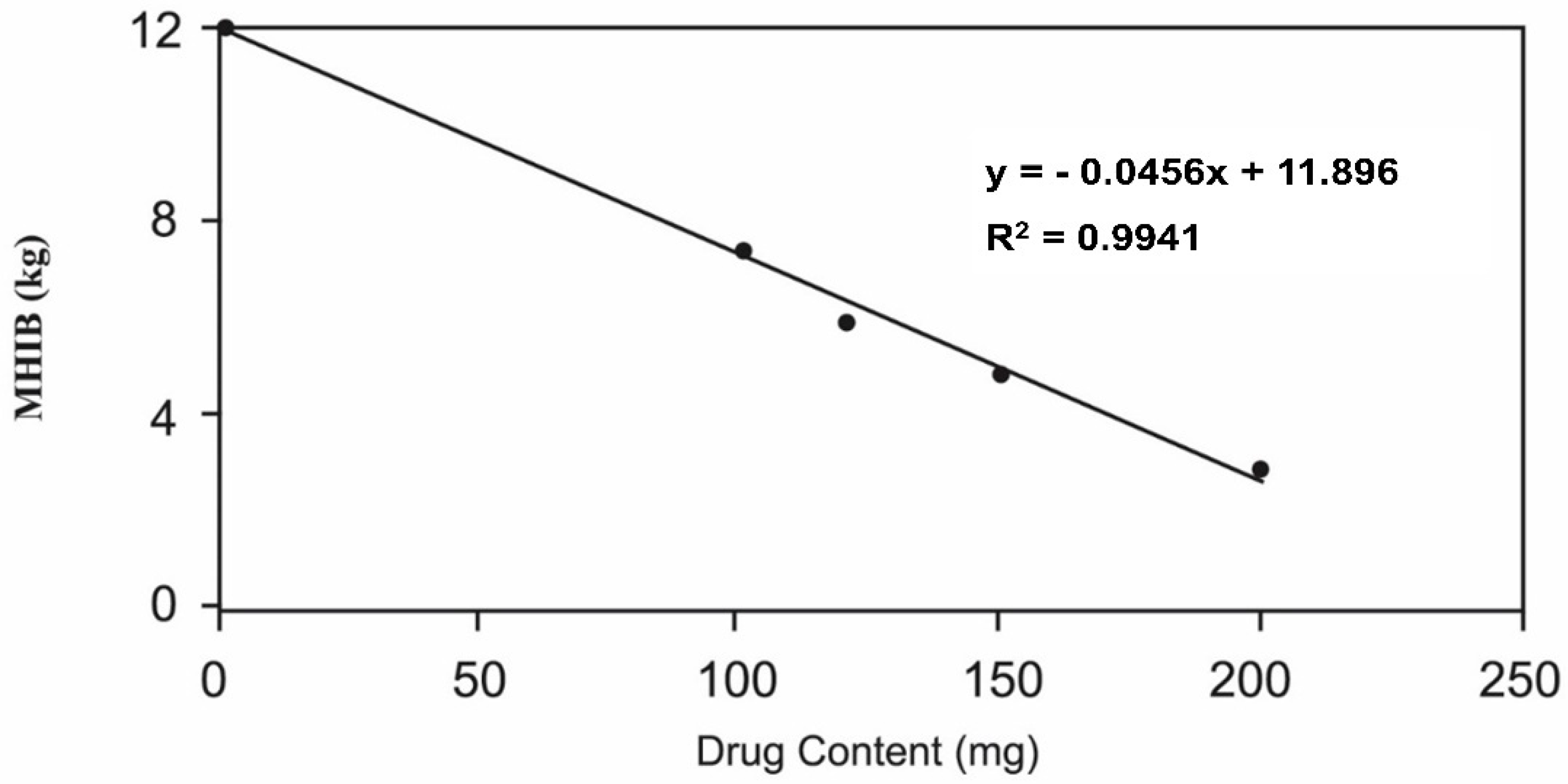
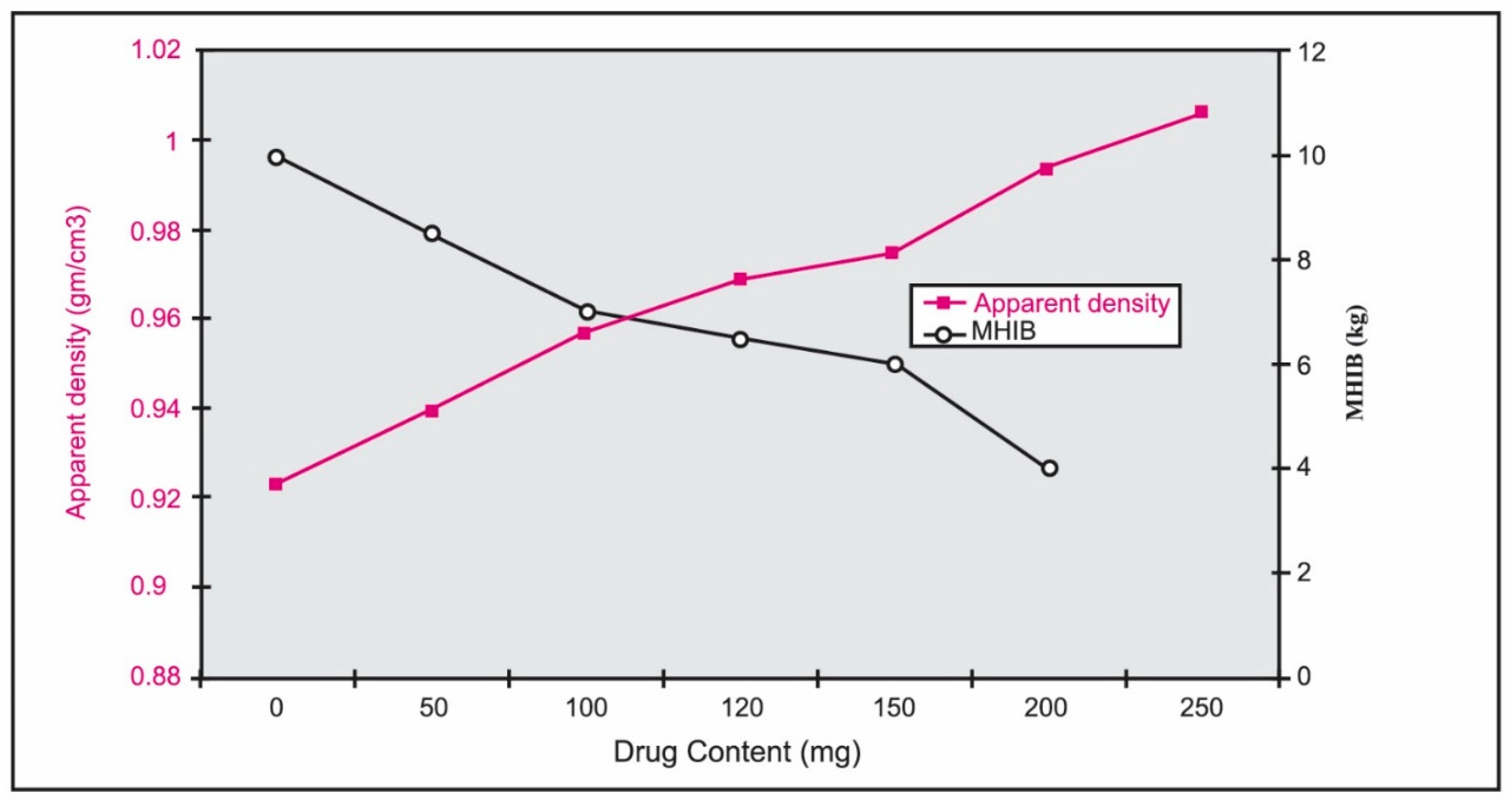
2.2.5. Effect of Drug Content on Buoyancy
2.2.6. Design of Metronidazole Tablets
2.2.7. In Vitro Evaluation of Proposed Tablets
2.2.8. Density Measurements
2.2.9. Buoyancy Study
2.2.10. In Vitro Release of Metronidazole Floating Tablets
3. Analysis of Metronidazole in Human Serum
3.1. HPLC of Metronidazole
3.2. HPLC Assay Validation Procedure
3.3. In Vivo Study
3.4. Volunteers
3.5. Experimental Design
3.6. Collection and Analysis of Blood Samples
3.7. Calculation of Pharmacokinetic Parameters
3.8. Statistical Analysis
4. Results and Discussion
4.1. Design and Optimization of Metronidazole Floating Tablets
4.1.1. Effect of Hydrogel Composition on Buoyancy
4.1.2. Effect of Tablet Weight and Hardness on Buoyancy
4.1.3. Effect of Drug Content on Buoyancy
4.2. In Vitro Evaluation of the Tablets
4.3. Density Measurements and Buoyancy Study
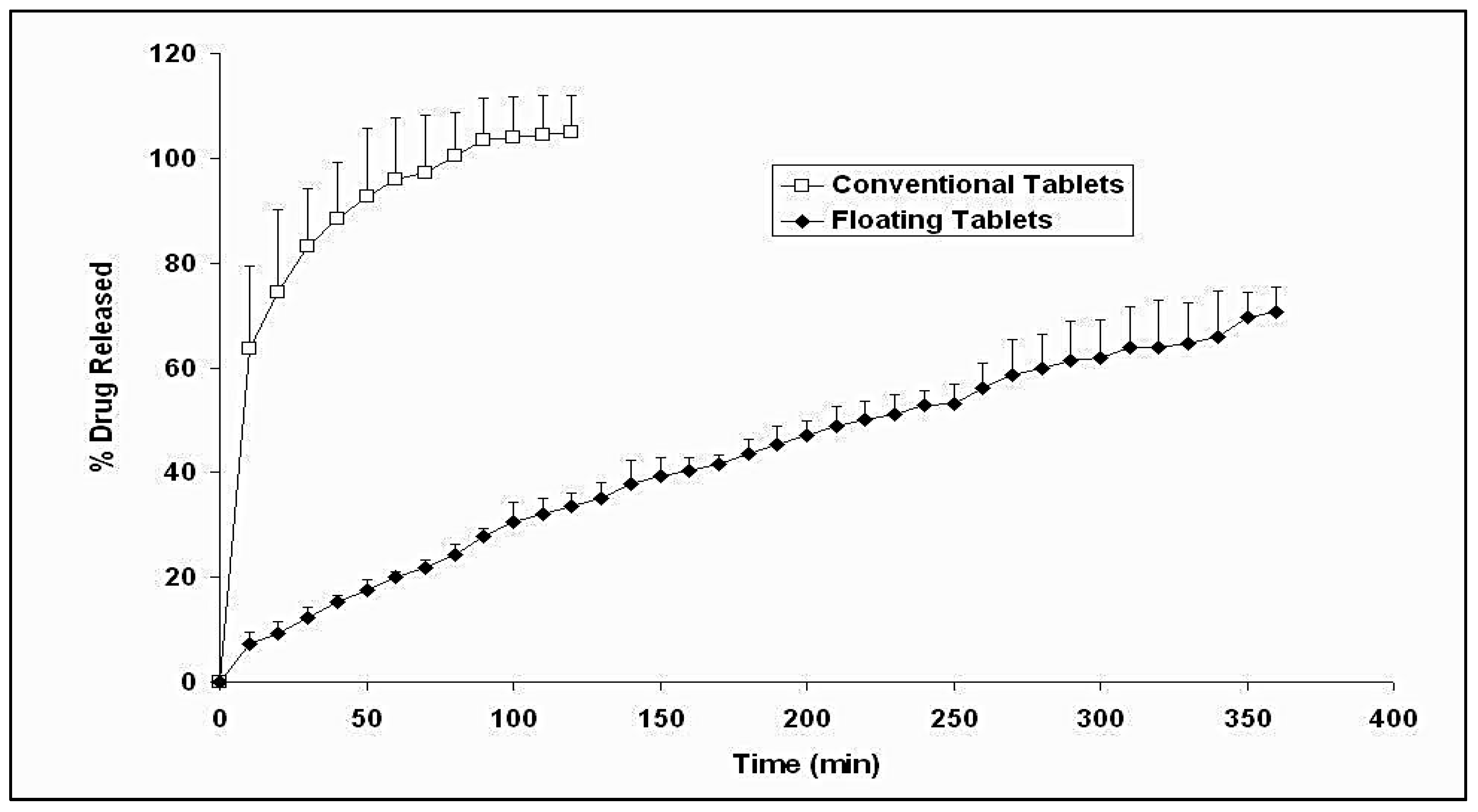
4.4. In Vitro Release of Buoyant and Conventional Metronidazole Tablets
4.5. Kinetic Analysis of Metronidazole Release Data
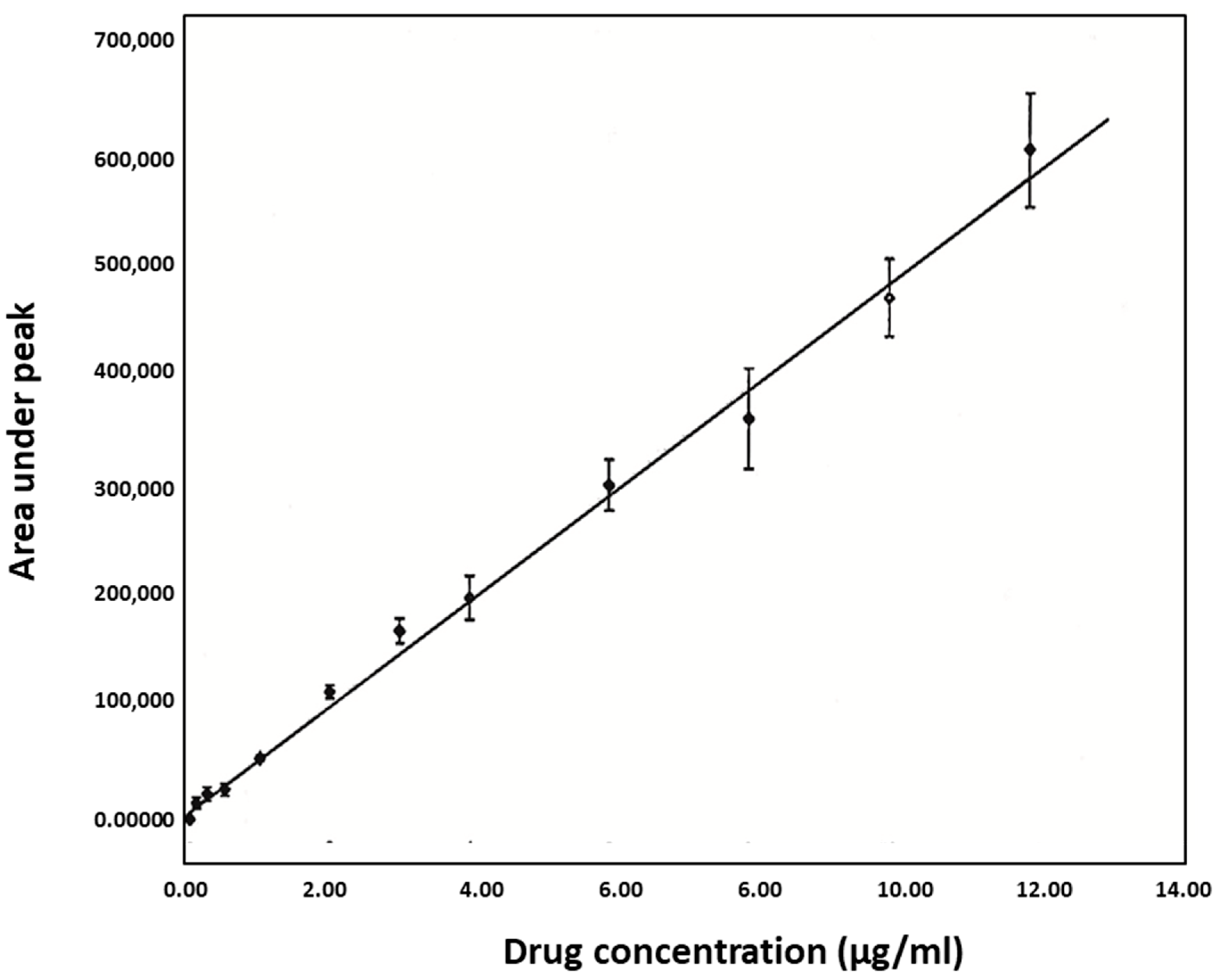
4.6. HPLC Assay Validation
4.7. Linearity
4.8. Accuracy and Precision of the Assay
4.9. Selectivity
4.10. Precision of Retention Time
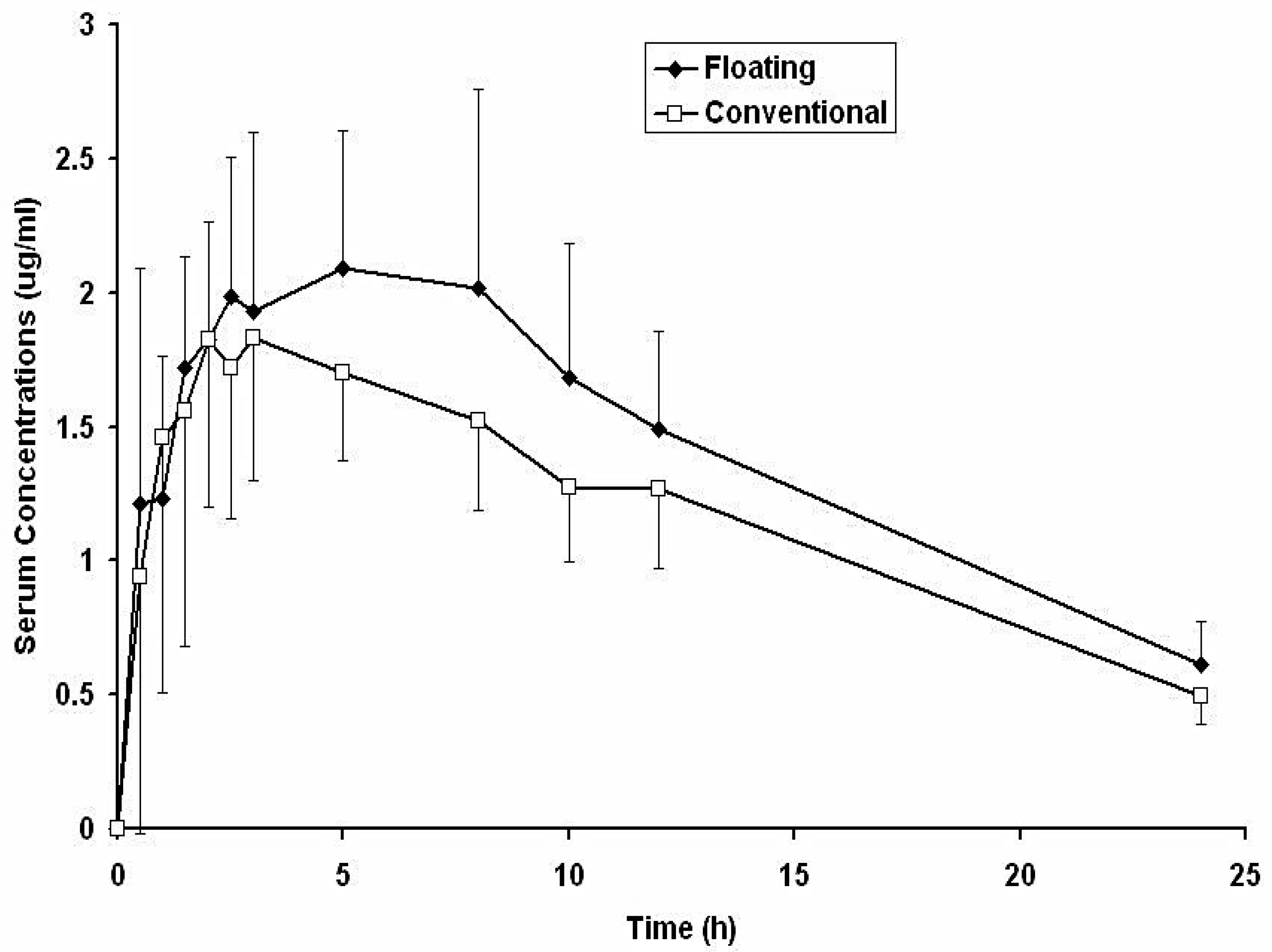
4.11. Bioavailability and Pharmacokinetics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alfarouk, K.O.; Bashir, A.H.H.; Aljarbou, A.N.; Ramadan, A.M.; Muddathir, A.K.; AlHoufie, S.T.S.; Hifny, A.; Elhassan, G.O.; Ibrahim, M.E.; Alqahtani, S.S.; et al. The Possible Role of Helicobacter pylori in Gastric Cancer and Its Management. Front. Oncol. 2019, 9, 75. [Google Scholar] [CrossRef]
- Naveed, S.; Qamar, F. Simple UV Spectrophotometric Assay of Metronidazole. Open Access Libr. J. 2014, 1, e615. [Google Scholar] [CrossRef]
- Chang, A.H.; Parsonnet, J. Role of Bacteria in Oncogenesis. Clin. Microbiol. Rev. 2010, 23, 837–857. [Google Scholar] [CrossRef] [Green Version]
- Kusters, J.G.; van Vliet, A.H.M.; Kuipers, E.J. Pathogenesis of Helicobacter pylori Infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef] [Green Version]
- Porro, G.B. Gastroenterology: An Illustrated Colour Text; Butcher, G.P., Ed.; Churchill Livingstone: Edinburgh, UK, 2003; p. 119. ISBN 0-443-06215-3. [Google Scholar]
- Ray, C.G.; Ryan, K.J. Sherris Medical Microbiology, 6th ed.; McGraw-Hill Education: New York, NY, USA, 2014. [Google Scholar]
- Suerbaum, S.; Michetti, P. Helicobacter pylori infection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.D.; Syn, N.L.; Moehler, M.; Grothe, W.; Yong, W.P.; Tai, B.C. Chemotherapy for advanced gastric cancer. Cochrane Database Syst. Rev. 2017, 8, CS004604. [Google Scholar] [CrossRef]
- Wu, Q.; Yang, Z.P.; Xu, P.; Gao, L.C.; Fan, D.M. Association between H elicobacter pylori infection and the risk of colorectal neoplasia: A systematic review and meta-analysis. Colorectal Dis. 2013, 15, e352–e364. [Google Scholar] [CrossRef]
- Markowski, A.R.; Markowska, A.; Guzinska-Ustymowicz, K. Pathophysiological and clinical aspects of gastric hyperplastic polyps. World J. Gastroenterol. 2016, 22, 8883. [Google Scholar] [CrossRef]
- Soetikno, R.M. Prevalence of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Asymptomatic and Symptomatic Adults. JAMA 2008, 299, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Abbas, H.; Niazi, M.; Makker, J. Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma of the Colon: A Case Report and a Literature Review. Am. J. Case Rep. 2017, 18, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Wolkowiez, M.; Sampson, M.; Bloom, B.T.; Arrieta, A.; Wynn, J.; Martz, K.; Harper, B.; Kearns, G.L.; Capparelli, E.V.; Siegel, D.; et al. Determining Population and Developmental Pharmacokinetics of Metronidazole Using Plasma and Dried Blood Spot Samples From Premature Infants. Pediatr. Infect. Dis. J. 2013, 32, 956–961. [Google Scholar] [CrossRef] [Green Version]
- de Bergamaschi, C.C.; Berto, L.A.; Venâncio, P.C.; Cogo, K.; Franz-Montan, M.; Motta, R.H.; Santamaria, M.P.; Groppo, F.C. Concentrations of metronidazole in human plasma and saliva after tablet or gel administration. J. Pharm. Pharmacol. 2014, 66, 40–47. [Google Scholar] [CrossRef]
- Romano, M.; Cuomo, A. Eradication of Helicobacter pylori: A clinical update. Medscape Gen. Med. 2004, 6, 19. [Google Scholar]
- Sahasathian, T.; Praphairaksit, N.; Muangsin, N. Mucoadhesive and floating chitosan-coated alginate beads for the controlled gastric release of amoxicillin. Arch. Pharmacal Res. 2010, 33, 889–899. [Google Scholar] [CrossRef]
- Chun, M.-K.; Sah, H.; Choi, H.-K. Preparation of mucoadhesive microspheres containing antimicrobial agents for eradication of H. pylori. Int. J. Pharm. 2005, 297, 172–179. [Google Scholar] [CrossRef]
- Rao, G.K.; Mandapalli, P.K.; Manthri, R.; Reddy, V.P. Development and in vivo evaluation of gastroretentive delivery systems for cefuroxime axetil. Saudi Pharm. J. 2012, 21, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Singh, B.N.; Kim, K.H. Floating drug delivery systems: An approach to oral controlled drug delivery via gastric retention. J. Control. Release 2000, 63, 235–259. [Google Scholar] [CrossRef]
- Higuchi, T. Mechanism of sustained-action medication. Theoretical analysis of rate of release of solid drugs dispersed in solid matrices. J. Pharm. Sci. 1963, 52, 1145–1149. [Google Scholar] [CrossRef]
- Ezzeldin, E.; El-Nahhas, T. New Analytical Method for the Determination of Metronidazole in Human Plasma: Application to Bioequivalence Study. Trop. J. Pharm. Res. 2013, 11, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Halabi, A.; Ferrayoli, C.; Palacio, M.; Dabbene, V.; Palacios, S. Validation of a chiral HPLC assay for (R)-salbutamol sulfate. J. Pharm. Biomed. Anal. 2004, 34, 45–51. [Google Scholar] [CrossRef]
- Lambropoulos, J.; Spanos, G.A.; Lazaridis, N.V. Development and validation of an HPLC assay for fentanyl, alfentanil, and sufentanil in swab samples. J. Pharm. Biomed. Anal. 2000, 23, 421–428. [Google Scholar] [CrossRef]
- Elkomy, M.H. Changing the Drug Delivery System: Does it Add to Non-Compliance Ramifications Control? A Simulation Study on the Pharmacokinetics and Pharmacodynamics of Atypical Antipsychotic Drug. Pharmaceutics 2020, 12, 297. [Google Scholar] [CrossRef] [Green Version]
- Elkomy, M.H.; Alruwaili, N.; Elmowafy, M.; Shalaby, K.; Drover, D.R.; Ramamoorthy, C. Assessment of Ketamine Adult Anesthetic Doses in Pediatrics Using Pharmacokinetic Modeling and Simulations. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2019, 39, 454–462. [Google Scholar] [CrossRef]
- Sheth, P.R.; Tossounian, J. The Hydrodynamically Balanced System (Hbs™): A Novel Drug Delivery System for Oral Use. Drug Dev. Ind. Pharm. 1984, 10, 313–339. [Google Scholar] [CrossRef]
- Nur, A.O.; Zhang, J.S. Captopril Floating and/or Bioadhesive Tablets: Design and Release Kinetics. Drug Dev. Ind. Pharm. 2000, 26, 965–969. [Google Scholar] [CrossRef]
- Panda, D.; Eid, H.; Elkomy, M.; Khames, A.; Hassan, R.; El-Ela, F.A.; Yassin, H. Berberine Encapsulated Lecithin–Chitosan Nanoparticles as Innovative Wound Healing Agent in Type II Diabetes. Pharmaceutics 2021, 13, 1197. [Google Scholar] [CrossRef]
- Elkomy, M.H.; Elmowafy, M.; Shalaby, K.; Azmy, A.F.; Ahmad, N.; Zafar, A.; Eid, H.M. Development and machine-learning optimization of mucoadhesive nanostructured lipid carriers loaded with fluconazole for treatment of oral candidiasis. Drug Dev. Ind. Pharm. 2021, 47, 246–258. [Google Scholar] [CrossRef]
- El Menshawe, S.F.; Aboud, H.M.; Elkomy, M.H.; Kharshoum, R.M.; Abdeltwab, A.M. A novel nanogel loaded with chitosan decorated bilosomes for transdermal delivery of terbutaline sulfate: Artificial neural network optimization, in vitro characterization and in vivo evaluation. Drug Deliv. Transl. Res. 2019, 10, 471–485. [Google Scholar] [CrossRef]
- Eid, H.M.; Elkomy, M.H.; El Menshawe, S.F.; Salem, H.F. Development, Optimization, and In Vitro/In Vivo Characterization of Enhanced Lipid Nanoparticles for Ocular Delivery of Ofloxacin: The Influence of Pegylation and Chitosan Coating. AAPS PharmSciTech 2019, 20, 183. [Google Scholar] [CrossRef]
- Elkomy, M.H.; El-Menshawe, S.F.; Ali, A.A.; Halawa, A.A.; El-Din, A.S.S. Betahistine dihydrochloride transdermal delivery via optimized thermosensitive gels: Percutaneous absorption evaluation using rat growth as a biomarker. Drug Deliv. Transl. Res. 2017, 8, 165–177. [Google Scholar] [CrossRef]
- Elkomy, M.H.; El Gazayerly, O.; Abdelrahman, A.A. The Influence of Solid/Solvent Interfacial Interactions on Physicochemical and Mechanical Properties of Ofloxacin. J. Pharm. Innov. 2020, 16, 170–180. [Google Scholar] [CrossRef]
- European Medicines Agency. ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology; European Medicines Agency: Amsterdam, The Netherlands, 2005; p. 5.
- Ibrahim, M.; Naguib, Y.W.; Sarhan, H.A.; Abdelkader, H. Gastro-retentive oral drug delivery systems: A promising approach for narrow absorption window drugs. J. Adv. Biomed. Pharm. Sci. 2019, 2, 98–110. [Google Scholar] [CrossRef]
- Wen, H.; Jung, H.; Li, X. Drug Delivery Approaches in Addressing Clinical Pharmacology-Related Issues: Opportunities and Challenges. AAPS J. 2015, 17, 1327–1340. [Google Scholar] [CrossRef]
- Vasvári, G.; Haimhoffer, Á.; Horváth, L.; Budai, I.; Trencsényi, G.; Béresová, M.; Dobó-Nagy, C.; Váradi, J.; Bácskay, I.; Ujhelyi, Z.; et al. Development and Characterisation of Gastroretentive Solid Dosage Form Based on Melt Foaming. AAPS PharmSciTech 2019, 20, 290. [Google Scholar] [CrossRef]
- Farooq, U.; Khan, S.; Nawaz, S.; Ranjha, N.M.; Haider, M.S.; Khan, M.M.; Dar, E.; Nawaz, A. Enhanced gastric retention and drug release via development of novel floating microspheres based on Eudragit E100 and polycaprolactone: Synthesis and in vitro evaluation. Des. Monomers Polym. 2017, 20, 419–433. [Google Scholar] [CrossRef] [Green Version]
- Huanbutta, K.; Nernplod, T.; Akkaramongkolporn, P.; Sriamornsak, P. Design of porous Eudragit ® L beads for floating drug delivery by wax removal technique. Asian J. Pharm. Sci. 2016, 12, 227–234. [Google Scholar] [CrossRef]
- El-Mahrouk, M.G.; Aboul-Einien, M.H.; Makhlouf, A.I. Design, optimization, and evaluation of a novel metronidazole-loaded gastro-retentive pH-sensitive hydrogel. AAPS PharmSciTech 2016, 17, 1285–1297. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation No. | Drug (mg) | Hydrogel (mg) | Avicel (mg) | Tablet Weight (mg) | Floating Status a | ||
|---|---|---|---|---|---|---|---|
| HPC | HMC | HPMC | |||||
| A1 | --- | 600 | --- | --- | --- | 600 | S |
| A2 | --- | --- | 600 | --- | --- | 600 | F |
| A3 | --- | --- | --- | 600 | --- | 600 | F |
| A4 | --- | --- | 540 | --- | 60 | 600 | S |
| A5 | --- | --- | --- | 300 | 300 | 600 | F |
| A6 | --- | --- | --- | 270 | 330 | 600 | S |
| Subject No. | Age (Year) | Weight (kgs) |
|---|---|---|
| 1 | 30 | 60 |
| 2 | 34 | 72 |
| 3 | 29 | 66 |
| 4 | 30 | 62 |
| 5 | 32 | 67 |
| 6 | 31 | 69 |
| Average (±SD) | 31 ± 1.788 | 66 ± 4.427 |
| Tablet Weight | Hardness Range (kg) | Floating Aspects a | MHIB b (kg) |
|---|---|---|---|
| 400 mg | 3–5 | F | 8 |
| 5–7 | F | ||
| 8–9 | F | ||
| 9–10 | S | ||
| 500 mg | 9–10 | F | 9 |
| 10–14 | S | ||
| 600 mg | 13–14 | F | 13 |
| 14–15 | S | ||
| 700 mg | 13–14 | F | 13 |
| 14–15 | S | ||
| 800 mg | >15 | F | 15 |
| Formulation | Drug (mg) | Hardness (kg) | Friability (%) | Thickness (cm) | Apparent Density (gm/cm3) | Lag Time (min) | MHIB a (kg) |
|---|---|---|---|---|---|---|---|
| F1 | 0.0 | 5.2 ± 0.2 | 0.324 ± 0.01 | 0.563 ± 0.001 | 0.923 ± 0.009 | 0.0 | 10.0 |
| F2 | 50 | 5.4 ± 0.2 | 0.411 ± 0.04 | 0.553 ± 0.004 | 0.939 ± 0.009 | 0.0 | 8.5 |
| F3 | 100 | 5.3 ± 0.1 | 0.495 ± 0.07 | 0.543 ± 0.003 | 0.957 ± 0.010 | 0.0 | 7.0 |
| F4 | 120 | 5.6 ± 0.3 | 0.573 ± 0.04 | 0.536 ± 0.003 | 0.968 ± 0.010 | 0.0 | 6.5 |
| F5 | 150 | 5.3 ± 0.2 | 0.686 ± 0.06 | 0.533 ± 0.002 | 0.974 ± 0.010 | 0.0 | 6.0 |
| F6 | 200 | 5.7 ± 0.3 | 0.833 ± 0.04 | 0.516 ± 0.005 | 0.994 ± 0.010 | 35.0 ± 5.0 | 4.0 |
| F7 | 250 | 5.7 ± 0.2 | 0.864 ± 0.03 | 0.513 ± 0.004 | 1.01 ± 0.011 | 42.7 ± 2.52 | - |
| Formulation | Initial % Release (after 10 min) | Release Rate Constant (K) (mg min−1/2) | Release Half-Life (T1/2) (min) |
|---|---|---|---|
| Buoyant | 7.293 (±2.137) b | 6.278 (±0.853) b | 181.341 (±37.905) b |
| Conventional | 63.626 (±15.802) | 10.666 (±1.621) | 16.321 (±5.936) |
| Nominal Concentration (µg/mL) | Found Concentration (µg/mL) | % CV | % of Nominal Concentration |
|---|---|---|---|
| Intra-day | |||
| 8 | 7.90 ± 0.19 | 2.41 | 98.78 |
| 10 | 10.35 ± 0.28 | 2.76 | 103.59 |
| 12 | 11.91 ± 0.32 | 2.72 | 99.29 |
| 14 | 13.87 ± 0.27 | 1.96 | 99.07 |
| 16 | 16.08 ± 0.34 | 2.13 | 100.50 |
| 18 | 17.36 ± 0.13 | 0.785 | 96.47 |
| 20 | 20.51 ± 0.15 | 0.741 | 102.55 |
| Inter-day | |||
| 8 | 7.97 ± 0.81 | 10.19 | 99.64 |
| 10 | 10.55 ± 1.36 | 12.89 | 105.59 |
| 12 | 12.07 ± 1.23 | 10.21 | 100.63 |
| 14 | 14.15 ± 1.31 | 9.27 | 101.09 |
| 16 | 16.08 ± 1.12 | 6.99 | 100.53 |
| 18 | 17.69 ± 1.59 | 8.99 | 98.32 |
| 20 | 20.96 ± 1.85 | 8.86 | 104.82 |
| Parameter | Validation Data |
|---|---|
| Retention time range | 3.1–3.3 min |
| Linearity range | 0.1–12 µg/mL |
| Intra-day accuracy | 96.47–103.59% |
| Inter-day accuracy | 98.32–105.59% |
| Intra-day precision | 0.741–2.76% |
| Inter-day precision | 6.99–12.89% |
| Parameters | Floating Tablets | Conventional Tablets |
|---|---|---|
| Cmax (µg/mL) | 2.490 ± 0.653 | 2.060 ± 0.473 |
| Tmax (h) | 5.66 ± 2.804 b | 2.5 ± 2.756 |
| Ka (h−1) | 0.78 ± 0.319 b | 1.336 ± 0.273 |
| K (h−1) | 0.03 ± 0.003 | 0.070 ± 0.005 |
| T1/2 (h) | 9.52 ± 0.510 | 9.837 ± 0.787 |
| AUC0–24 (µg·h·mL−1) | 34.155 ± 7.099 b | 28.478 ± 6.394 |
| AUC0–∞ (µg·h·mL−1) | 42.658 ± 8.952 b | 35.535 ± 7.664 |
| MRT (h) | 15.917 ± 0.876 b | 14.342 ± 0.541 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkomy, M.H.; Abou-Taleb, H.A.; Eid, H.M.; Yassin, H.A. Fabrication and In Vitro/In Vivo Appraisal of Metronidazole Intra-Gastric Buoyant Sustained-Release Tablets in Healthy Volunteers. Pharmaceutics 2022, 14, 863. https://doi.org/10.3390/pharmaceutics14040863
Elkomy MH, Abou-Taleb HA, Eid HM, Yassin HA. Fabrication and In Vitro/In Vivo Appraisal of Metronidazole Intra-Gastric Buoyant Sustained-Release Tablets in Healthy Volunteers. Pharmaceutics. 2022; 14(4):863. https://doi.org/10.3390/pharmaceutics14040863
Chicago/Turabian StyleElkomy, Mohammed H., Heba A. Abou-Taleb, Hussein M. Eid, and Heba A. Yassin. 2022. "Fabrication and In Vitro/In Vivo Appraisal of Metronidazole Intra-Gastric Buoyant Sustained-Release Tablets in Healthy Volunteers" Pharmaceutics 14, no. 4: 863. https://doi.org/10.3390/pharmaceutics14040863