
The Development of Innovative Dosage Forms of the Fixed-Dose Combination of Active Pharmaceutical Ingredients


Abstract
:1. Introduction
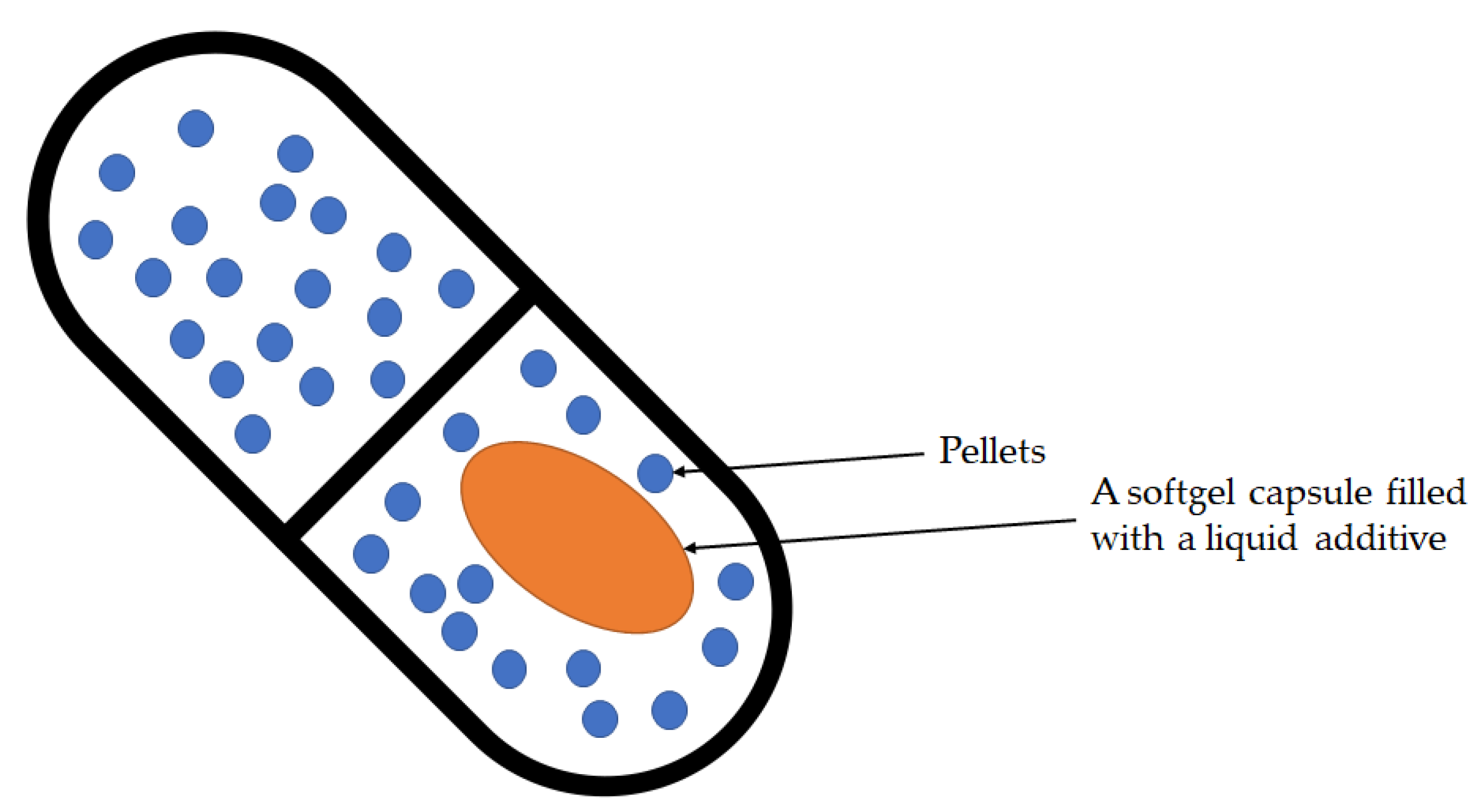
- Hard capsules containing pellets, mini-tablets, microcapsules, or the encapsulation of liquid combinations;
- Bilayer tablets;
- Multilayer tablets;
- Gastric retention of oral dosage forms (floating capsules, hydrodynamically balanced systems, raft-forming systems, expandable);
- Delivery systems by hot-melt extrusion, co-extrusion;
- Three-dimensional (3D) printing technology.
2. Advantages and Disadvantages of Using FDCs
3. Hard Capsules in Fixed-Dose Combinations
3.1. Encapsulation of Liquid Combination
3.2. Cardiovascular Polypill
3.3. Inhalation Combinations
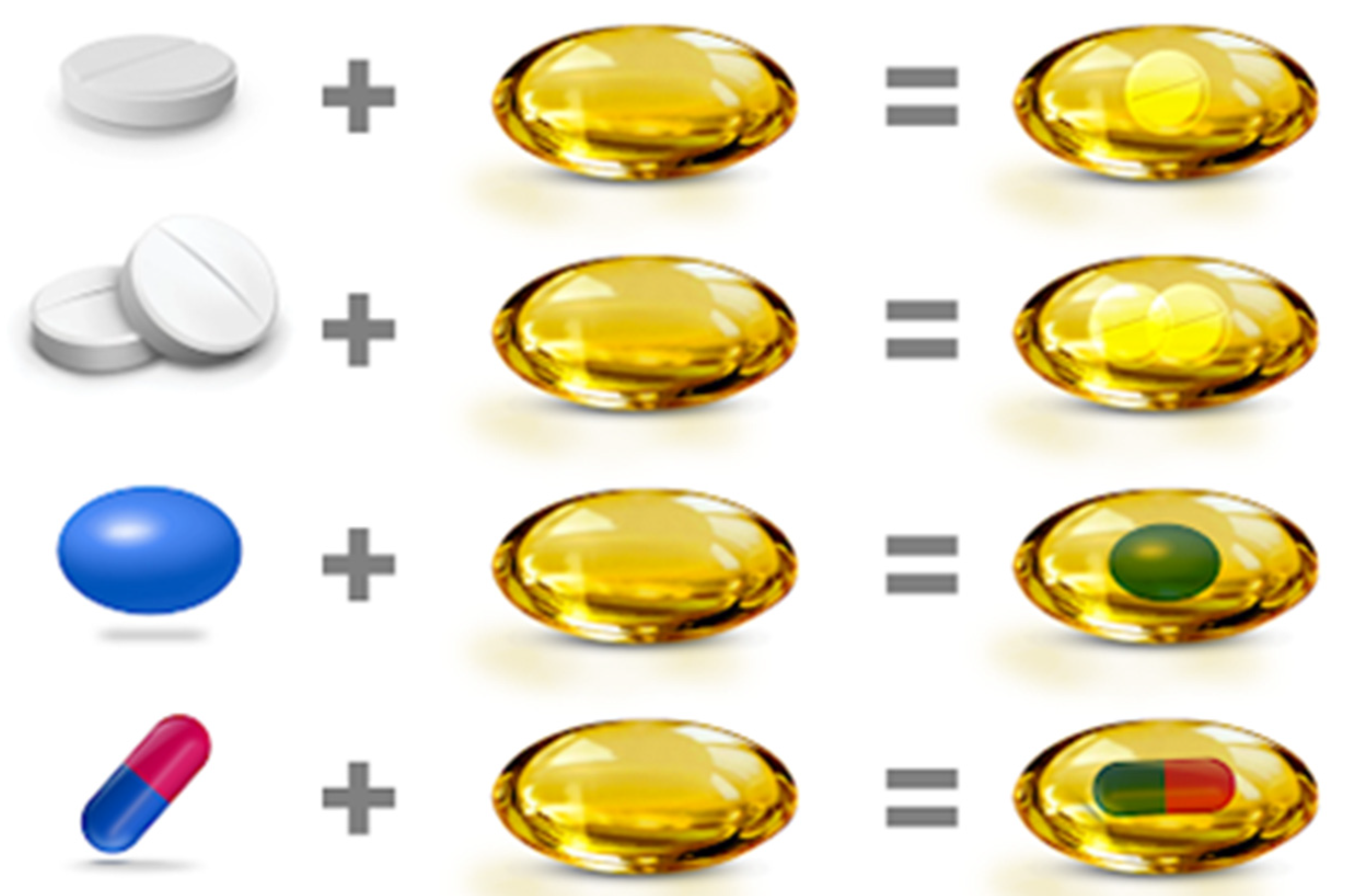
3.4. Fixed-Dose Combination Softgel
4. Bilayer Tablets
- These are unit dosage forms with the most remarkable capabilities of all oral dosage forms for dose precision.
- Maximum prevention of cross-contamination between the two layers.
- Clear visual separation between the two layers.
- Low compression force to avoid capping and separating the two individual layers.
- Lowered cost compared to all other oral dosage forms.
- Easiest and cheapest to package and strip.
- Lighter and compact.
- Easy to swallow with the slightest tendency for hang-up.
- Product identification is easy and rapid, requiring no additional label when employing an embossed and/or monogrammed punch face.
- Suitable for large-scale production.
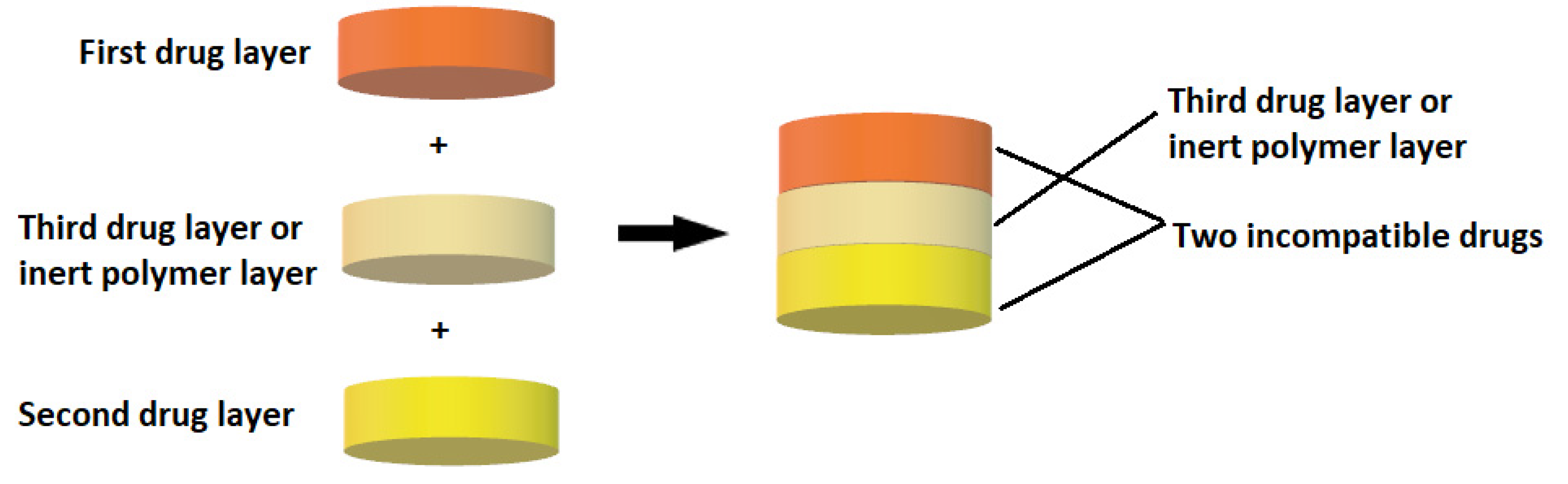
5. Multilayer Tablet
- Separation of incompatible active pharmaceutical ingredients (APIs).
- To control the rate of release of one or two different active pharmaceutical ingredients.
- Controlling the release of an API from one layer by taking advantage of the functional properties of the other layer (such as osmotic properties).
- To modify the total surface area of the API layer utilizing a spacer with one or two inactive layers to obtain swollen or erodible modified-release barriers.
- Possibility to implement fixed-dose combination drugs (FDCs), develop new drug delivery systems, and thus, extend the life cycle of a medicinal product (patent extension).
6. Oral Sustained Release Dosage Forms
7. Floating Capsules
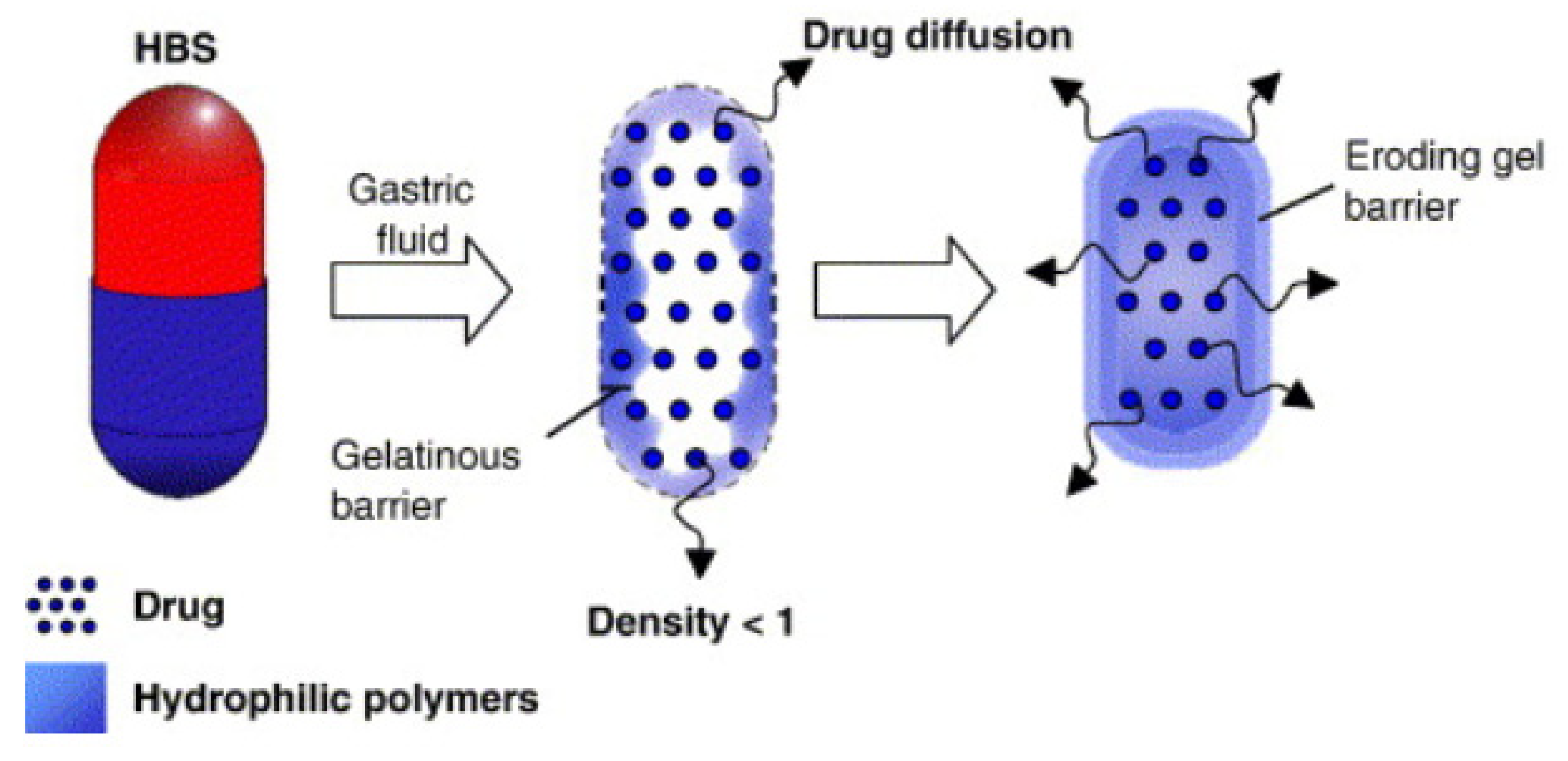
8. Hydrodynamically Balanced Systems (HBSs)
9. Raft-Forming Systems
10. Expandable
11. Long-Acting Oral (LAO) Gastro-Retentive Drug Delivery Systems
12. Hot-Melt Extrusion (HME) and Co-Extruded Solid Solutions
- It does not require the use of water or other solvents (the process is carried out in an anhydrous environment).
- It ensures the continuity of production and product homogeneity.
- A lower number of processing steps and a shorter time to obtain the product compared to traditional technologies.
- Maintains the process efficiency at a high level, compared to classical production methods.
- The possibility of obtaining molecular dispersions and solid dispersions.
- The possibility of producing drug forms containing thermolabile substances.
- The possibility of obtaining amorphous forms.
- Masking the taste and smell of medicinal substances.
- The possibility of shaping a mixture of substances that cannot be compressed and obtaining any shape.
13. Three-Dimensional (3D) Printing Technology
13.1. Fused Deposition Modeling (FDM)
13.2. Semi-Solid Extrusion (SSE)
13.3. Inkjet Printing
13.4. Powder Bed Technology
14. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Auwal, F.; Dahiru, M.; Abdu-Aguye, S. Availability and Rationality of Fixed Dose Combinations Available in Kaduna, Nigeria. Pharm. Pract. 2019, 17, 1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalal, K.; Ganguly, B.; Gor, A. Assessment of Rationality of Fixed Dose Combinations Approved in CDSCO List. J. Clin. Diagn. Res. 2016, 10, FC05–FC08. [Google Scholar] [CrossRef] [PubMed]
- Podczeck, F.; Jones, B.E. Pharmaceutical Capsules; Pharmaceutical Press: London, UK, 2004; ISBN 9780853695684. [Google Scholar]
- El-Malah, Y.; Nazzal, S.; Bottom, C.B. Hard Gelatin and Hypromellose (HPMC) Capsules: Estimation of Rupture Time by Real-Time Dissolution Spectroscopy. Drug Dev. Ind. Pharm. 2007, 33, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Combodart 0.5 Mg/0.4 Mg Hard Capsules—Summary of Product Characteristics (SmPC)—(Emc). Available online: https://www.medicines.org.uk/emc/product/507/smpc#gref (accessed on 18 March 2022).
- Wald, N.J.; Wald, D.S. The Polypill Concept. Heart 2010, 86, 257–260. [Google Scholar] [CrossRef]
- Wald, N.J.; Law, M.R. A Strategy to Reduce Cardiovascular Disease by More than 80%. BMJ 2003, 326, 1419. [Google Scholar] [CrossRef] [Green Version]
- Polypill. The Free Dictionary. polypill. (n.d.) Abused, Confused, & Misused Words. (2007, 2013). Available online: https://www.thefreedictionary.com/polypill (accessed on 19 January 2022).
- Broncel, M.; Wójcik, K.; Jabłonowska, E. Expanding role of single tablets regimens in selected therapeutic areas. Med. Rodz. 2015, 2, 79–88. [Google Scholar]
- WHO. Secondary Prevention of Noncommunicable Diseases in Low- and Middle-Income Countries through Community-Based and Health Service Interventions. In Proceedings of the World Health Organization-Wellcome Trust Meeting of Experts; Cambridge, UK, 1–3 August 2001, World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- World Health Report: Reducing Risks, Promoting Healthy Life. 2002. Available online: https://www.who.int/publications-detail-redirect/9241562072 (accessed on 19 January 2022).
- Yusuf, S. Two Decades of Progress in Preventing Vascular Disease. Lancet 2002, 360, 2–3. [Google Scholar] [CrossRef]
- Tamargo, J.; Castellano, J.M.; Fuster, V. The Fuster-CNIC-Ferrer Cardiovascular Polypill: A Polypill for Secondary Cardiovascular Prevention. Int. J. Cardiol. 2015, 201 (Suppl. 1), S15–S22. [Google Scholar] [CrossRef] [Green Version]
- Sanz, G.; Fuster, V. Fixed-Dose Combination Therapy and Secondary Cardiovascular Prevention: Rationale, Selection of Drugs and Target Population. Nat. Rev. Cardiol. 2009, 6, 101–110. [Google Scholar] [CrossRef]
- Webster, R.; Patel, A.; Selak, V.; Billot, L.; Bots, M.L.; Brown, A.; Bullen, C.; Cass, A.; Crengle, S.; Raina Elley, C.; et al. Effectiveness of Fixed Dose Combination Medication (‘polypills’) Compared with Usual Care in Patients with Cardiovascular Disease or at High Risk: A Prospective, Individual Patient Data Meta-Analysis of 3140 Patients in Six Countries. Int. J. Cardiol. 2016, 205, 147–156. [Google Scholar] [CrossRef]
- Webster, R.; Castellano, J.M.; Onuma, O.K. Putting Polypills into Practice: Challenges and Lessons Learned. Lancet 2017, 389, 1066–1074. [Google Scholar] [CrossRef]
- Huffman, M.D. The Polypill: From Promise to Pragmatism. PLoS Med. 2015, 12, e1001862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amol Dattatreya, G.; Naveen Ahuja, K.; Srinivas, M. Pediatric Dosage Forms—Challenges and Recent Developments: A Critical Review. J. Appl. Pharm. Sci. 2020, 10, 155–166. [Google Scholar] [CrossRef]
- Ehrick, J.D.; Wylie, J.; Goodey, A.P.; Li, Y.; Liu, O.; Donovan, B. Orally Inhaled Fixed-Dose Combination Products for the Treatment of Asthma and Chronic Obstructive Pulmonary Disease: Not Simple Math. Ther. Deliv. 2014, 5, 297–317. [Google Scholar] [CrossRef]
- Stirbulov, R.; Fritscher, C.C.; Pizzichini, E.; Pizzichini, M.M.M. Evaluation of the Efficacy and Safety of a Fixed-Dose, Single-Capsule Budesonide-Formoterol Combination in Uncontrolled Asthma: A Randomized, Double-Blind, Multicenter, Controlled Clinical Trial. J. Bras. Pneumol. 2012, 38, 431–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Softigel—UnigelTM. Available online: https://www.softigel.com/softgel-technologies/unigel (accessed on 19 January 2022).
- Wilkinson, L.; Jones, R.V.; Paton, W.D.M. William Brockedon, FRS (1787–1854). Notes Rec. R. Soc. Lond. 1971, 26, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Douglas, S.; John, S. Pharmaceutical Formulations and Their Manufacture. U.S. Patent US3146169A, 25 May 1964. [Google Scholar]
- Wu, C.-Y.; Seville, J.P.K. A Comparative Study of Compaction Properties of Binary and Bilayer Tablets. Powder Technol. 2009, 2, 285–294. [Google Scholar] [CrossRef]
- Won, D.H.; Park, H.; Ha, E.-S.; Kim, H.-H.; Jang, S.W.; Kim, M.-S. Optimization of Bilayer Tablet Manufacturing Process for Fixed Dose Combination of Sustained Release High-Dose Drug and Immediate Release Low-Dose Drug Based on Quality by Design (QbD). Int. J. Pharm. 2021, 605, 120838. [Google Scholar] [CrossRef]
- Dinakaran, S.K.; Kumar, S.; Banji, D.; Avasarala, H.; Rao, V. Formulation and Evaluation of Bi-Layer Floating Tablets of Ziprasidone HCl and Trihexyphenidyl HCl. Braz. J. Pharm. Sci. 2011, 47, 545–553. [Google Scholar] [CrossRef] [Green Version]
- Chun, M.-H.; Kim, J.Y.; Park, E.-S.; Choi, D.H. Development of a Robust Control Strategy for Fixed-Dose Combination Bilayer Tablets with Integrated Quality by Design, Statistical, and Process Analytical Technology Approach. Pharmaceutics 2021, 13, 1443. [Google Scholar] [CrossRef]
- Saif, A.A.; Alburyhi, M.M.; Noman, M.A.; Almaktari, A. Formulation and Evaluation of Trimetazidine Hydrochloride and Clopidogrel Bisulphate Multi-Unit Solid Dosage Forms. Available online: https://www.semanticscholar.org/paper/Formulation-and-evaluation-of-trimetazidine-and-Saif-Alburyhi/b26a294974e3c83beda79b9ccc11fb8a0cc95b6f (accessed on 19 January 2022).
- Pattanayak, D.P. Bilayer Tablet Formulation of Metformin Hydrochloride and Glimepiride: A Novel Approach to Improve Therapeutic Efficacy. Int. J. Drug Discov. Herb. Res. 2011, 1, 1–4. [Google Scholar]
- Mohideen, S.; Jyothi, B.; Pavani, S.; Satyanarayana, T.; Kumar, P.S.; Krishnan, S.N. Formulation and Evaluation of Bilayered Tablets of Metformin Hydrochloride and Atorvastatin Calcium. Int. J. Pharm. Sci. Rev. Res. 2011, 10, 5. [Google Scholar]
- Jadhav, R.T.; Patil, P.H.; Patil, P.R. Formulation and Evaluation of Bilayered Tablet of Piracetam and Vinpocetine. J. Chem. Pharm. Res. 2011, 3, 423–431. [Google Scholar]
- Kumar, G.V. Formulation and Evaluation of Bilayered Tablets of Cefixime Trihydrate and Dicloxacillin Sodium. Int. J. PharmTech Res. 2011, 3, 613–618. [Google Scholar]
- Jayaprakash, S.; Halith, M.; Kumaraswamy Pillai, K.; Balasubramaniyam, P.; Firthouse, U.M.; Boopathi, M. Formulation and Evaluation of Bilayer Tablets of Amlodipine Besilate and Metprolol Succinate. Pharm. Lett. 2011, 3, 143–154. [Google Scholar]
- Atram, S.C.; Udavant, Y.K.; Salunke, R.J.; Neb, G.B.; Shahi, S.; Gulecha, B.; Padalkar, A. Formulation of Bilayer Tablet Containing Metoprolol Succinate and Amlodipine Besylate as a Model Drug for Antihypertensive Therapy. J. Pharm. Res. 2009, 2, 1335–1347. [Google Scholar]
- Gohel, M.C.; Parikh, R.K.; Nagori, S.A.; Jethwa, B.A. Fabrication and Evaluation of Bi-Layer Tablet Containing Conventional Paracetamol and Modified Release Diclofenac Sodium. Indian J. Pharm. Sci. 2010, 72, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, A.; Bhatia, M. Development and Evaluation of Regioselective Bilayer Floating Tablets of Atenolol and Lovastatin for Biphasic Release Profile. Iran. J. Pharm. Res. 2010, 8, 15–25. [Google Scholar] [CrossRef]
- Rathod, R.T.; Misra, D. FDC of Montelukast with Levocetirizine: Focus on Bilayer Technology. J. Indian Med. Assoc. 2009, 107, 562–564. [Google Scholar]
- Nagaraju, R.; Kaza, R. Formulation and Evaluation of Bilayer Sustained Release Tablets of Salbutamol and Theophylline. Int. J. Pharm. Sci. Nanotechnol. 2009, 2, 638–646. [Google Scholar] [CrossRef]
- Gohel, M.C.; Sarvaiya, K.G. A Novel Solid Dosage Form of Rifampicin and Isoniazid with Improved Functionality. AAPS PharmSciTech 2007, 8, E68. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, M.F.G.W.S.A.; Sanz, E.G.G.W.S.A. Pharmaceutical Formulation. French Patent WO/2003/030942, 17 April 2003. [Google Scholar]
- Ouali, A.; Azad, A. Composition Pharmaceutique Stabilisee a Base D’agent Anti-Inflammatoire Non Steroidien et de Prostaglandine. French Patent WO/2000/056339, 28 September 2000. [Google Scholar]
- Dhumal, R.S.; Rajmane, S.T.; Dhumal, S.T.; Pawar, A.P. Design and Evaluation of Bilayer Floating Tablets of Cefuroxime Axetil for Bimodal Release. J. Sci. Ind. Res. 2006, 65, 5. [Google Scholar]
- Ozdemir, N.; Ordu, S.; Ozkan, Y. Studies of Floating Dosage Forms of Furosemide: In Vitro and in Vivo Evaluations of Bilayer Tablet Formulations. Drug Dev. Ind. Pharm. 2000, 26, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Alprax Plus Tablet SR: View Uses, Side Effects, Price and Substitutes. Available online: https://www.1mg.com/drugs/alprax-plus-tablet-sr-167243 (accessed on 17 March 2022).
- Glycomet-GP 2 Forte from USV, Glimepiride + Metformin—3D-Oha to Betagrim-M|DrugsUpdate India. Available online: http://www.drugsupdate.com/brand/generic/Glimepiride%20+%20Metformin/5313 (accessed on 17 March 2022).
- Generic Lopressor HCT Availability. Available online: https://www.drugs.com/availability/generic-lopressor-hct.html (accessed on 17 March 2022).
- Diovan HCT (Valsartan and Hydrochlorothiazide): Uses, Dosage, Side Effects, Interactions, Warning. Available online: https://www.rxlist.com/diovan-hct-drug.htm (accessed on 17 March 2022).
- Lotensin Hct (Benazepril HCl and HCTZ): Uses, Dosage, Side Effects, Interactions, Warning. Available online: https://www.rxlist.com/lotensin-hct-drug.htm (accessed on 17 March 2022).
- Clarinex-D 12hr (Desloratadine and Pseudoephedrine Sulfate): Uses, Dosage, Side Effects, Interactions, Warning. Available online: https://www.rxlist.com/clarinex-d-12hr-drug.htm (accessed on 17 March 2022).
- Treximet (Sumatriptan and Naproxen Sodium Tablets): Uses, Dosage, Side Effects, Interactions, Warning. Available online: https://www.rxlist.com/treximet-drug.htm (accessed on 17 March 2022).
- Atripla Oral: Uses, Side Effects, Interactions, Pictures, Warnings & Dosing—WebMD. Available online: https://www.webmd.com/drugs/2/drug-144753/atripla-oral/details (accessed on 17 March 2022).
- Clinical Trial on Healthy: Flurbiprofen 100 Mg Famotidine 20 Mg Multi-Layer Tablet, Antadys® 100 Mg, Pepcid® 20 Mg—Clinical Trials Registry—ICH GCP. Available online: https://ichgcp.net/clinical-trials-registry/NCT01910090 (accessed on 17 March 2022).
- Goyal, S.; Agarwal, G.; Agarwal, S.; Karar, P.K. Oral Sustained Release Tablets: An Overview with a Special Emphasis on Matrix Tablet. Am. J. Adv. Drug Deliv. 2017, 5, 64–76. [Google Scholar] [CrossRef] [Green Version]
- Ankit, B. Oral Sustained Release Dosage Form: An Opportunity to Prolong the Release of Drug. Res. Pharm. Bio. Sci. 2013, 8, 7–14. [Google Scholar]
- Cargill, R.; Caldwell, L.J.; Engle, K.; Fix, J.A.; Porter, P.A.; Gardner, C.R. Controlled Gastric Emptying. 1. Effects of Physical Properties on Gastric Residence Times of Nondisintegrating Geometric Shapes in Beagle Dogs. Pharm. Res. 1988, 5, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Zubedi, S.S.; Mohammed, S. Floating Tablets and Its Polymers. J. Drug Deliv. Ther. 2018, 8, 16–24. [Google Scholar] [CrossRef]
- Singh, B.N.; Kim, K.H. Floating Drug Delivery Systems: An Approach to Oral Controlled Drug Delivery via Gastric Retention. J. Control. Release 2000, 63, 235–259. [Google Scholar] [CrossRef]
- Müller, R.H.; Hildebrand, G.E. Technologia Nowoczesnych Postaci Leków; Wydawnictwo Lekarskie PZWL: Stryków, Poland, 1998; ISBN 9788320022063. [Google Scholar]
- Adibkia, K.; Ghanbarzadeh, S.; Mohammadi, G.; Atashgah, R.B.; Sabzevari, A. Gastro Retentive Drug Delivery Systems: A Review. J. Rep. Pharm. Sci. 2013, 2, 190. [Google Scholar]
- Crevoisier, C.; Hoevels, B.; Zürcher, G.; Da Prada, M. Bioavailability of L-Dopa after Madopar HBS Administration in Healthy Volunteers. Eur. Neurol. 1987, 27 (Suppl. 1), 36–46. [Google Scholar] [CrossRef]
- Oth, M.; Franz, M.; Timmermans, J.; Möes, A. The Bilayer Floating Capsule: A Stomach-Directed Drug Delivery System for Misoprostol. Pharm. Res. 1992, 9, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Yu, Z.; Bi, D. Design and Evaluation of a Two-Layer Floating Tablet for Gastric Retention Using Cisapride as a Model Drug. Drug Dev. Ind. Pharm. 2001, 27, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Rouge, N.; Cole, E.T.; Doelker, E.; Buri, P. Buoyancy and Drug Release Patterns of Floating Minitablets Containing Piretanide and Atenolol as Model Drugs. Pharm. Dev. Technol. 1998, 3, 73–84. [Google Scholar] [CrossRef]
- Johnson, F.A.; Craig, D.Q.M.; Mercer, A.D.; Chauhan, S. The Effects of Alginate Molecular Structure and Formulation Variables on the Physical Characteristics of Alginate Raft Systems. Int. J. Pharm. 1997, 1, 35–42. [Google Scholar] [CrossRef]
- Vrettos, N.-N.; Roberts, C.J.; Zhu, Z. Gastroretentive Technologies in Tandem with Controlled-Release Strategies: A Potent Answer to Oral Drug Bioavailability and Patient Compliance Implications. Pharmaceutics 2021, 13, 1591. [Google Scholar] [CrossRef] [PubMed]
- Sabale, V.; Sakarkar, S.N.; Pund, S.; Sabale, P.M. Formulation and Evaluation of Floating Dosage Forms: An Overview. Syst. Rev. Pharm. 2010, 1, 33–39. [Google Scholar] [CrossRef]
- Altreuter, D.H.; Kirtane, A.R.; Grant, T.; Kruger, C.; Traverso, G.; Bellinger, A.M. Changing the Pill: Developments toward the Promise of an Ultra-Long-Acting Gastroretentive Dosage Form. Expert Opin. Drug Deliv. 2018, 15, 1189–1198. [Google Scholar] [CrossRef]
- Pereira, G.G.; Figueiredo, S.; Fernandes, A.I.; Pinto, J.F. Polymer Selection for Hot-Melt Extrusion Coupled to Fused Deposition Modelling in Pharmaceutics. Pharmaceutics 2020, 12, 795. [Google Scholar] [CrossRef]
- Kanasty, R.; Low, S.; Bhise, N.; Yang, J.; Peeke, E.; Schwarz, M.; Wright, J.; Carter, B.; Moorthy, S.; Grant, T.; et al. A Pharmaceutical Answer to Nonadherence: Once Weekly Oral Memantine for Alzheimer’s Disease. J. Control. Release 2019, 303, 34–41. [Google Scholar] [CrossRef]
- Bellinger, A.M.; Jafari, M.; Grant, T.M.; Zhang, S.; Slater, H.C.; Wenger, E.A.; Mo, S.; Lee, Y.-A.L.; Mazdiyasni, H.; Kogan, L.; et al. Oral, Ultra-Long-Lasting Drug Delivery: Application toward Malaria Elimination Goals. Sci. Transl. Med. 2016, 8, 365ra157. [Google Scholar] [CrossRef] [Green Version]
- Maniruzzaman, M.; Boateng, J.S.; Snowden, M.J.; Douroumis, D. A Review of Hot-Melt Extrusion: Process Technology to Pharmaceutical Products. ISRN Pharm. 2012, 2012, 436763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palem, C.R.; Kumar Battu, S.; Maddineni, S.; Gannu, R.; Repka, M.A.; Yamsani, M.R. Oral Transmucosal Delivery of Domperidone from Immediate Release Films Produced via Hot-Melt Extrusion Technology. Pharm. Dev. Technol. 2013, 18, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Breitenbach, J. Melt Extrusion Can Bring New Benefits to HIV Therapy: The Example of Kaletra® Tablets. Am. J. Drug Deliv. 2006, 4, 61–64. [Google Scholar] [CrossRef]
- Crowley, M.M.; Zhang, F.; Repka, M.A.; Thumma, S.; Upadhye, S.B.; Battu, S.K.; McGinity, J.W.; Martin, C. Pharmaceutical Applications of Hot-Melt Extrusion: Part I. Drug Dev. Ind. Pharm. 2007, 33, 909–926. [Google Scholar] [CrossRef] [PubMed]
- Jagtap, P.; Jain, S.S.; Dand, N.; Jadhav, K.; Kadam, V.J. Hot Melt Extrusion Technology, Approach of Solubility Enhancement: A Brief Review. Pharm. Lett. 2012, 4, 42–53. [Google Scholar]
- Zhang, F.; McGinity, J.W. Properties of Sustained-Release Tablets Prepared by Hot-Melt Extrusion. Pharm. Dev. Technol. 1999, 4, 241–250. [Google Scholar] [CrossRef]
- Dierickx, L.; Van Snick, B.; Monteyne, T.; De Beer, T.; Remon, J.P.; Vervaet, C. Co-Extruded Solid Solutions as Immediate Release Fixed-Dose Combinations. Eur. J. Pharm. Biopharm. 2014, 88, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Abdelquader, M.M.; Essa, E.A.; El Maghraby, G.M. Inhibition of Co-Crystallization of Olmesartan Medoxomil and Hydrochlorothiazide for Enhanced Dissolution Rate in Their Fixed Dose Combination. AAPS PharmSciTech 2018, 20, 3. [Google Scholar] [CrossRef]
- Fischer, M.A. Implanon: A New Contraceptive Implant. J. Obstet. Gynecol. Neonatal. Nurs. 2008, 37, 361–368. [Google Scholar] [CrossRef]
- Prasad, L.K.; Smyth, H. 3D Printing Technologies for Drug Delivery: A Review. Drug Dev. Ind. Pharm. 2016, 42, 1019–1031. [Google Scholar] [CrossRef]
- Pravin, S.; Sudhir, A. Integration of 3D Printing with Dosage Forms: A New Perspective for Modern Healthcare. Biomed. Pharmacother. 2018, 107, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Norman, J.; Madurawe, R.D.; Moore, C.M.V.; Khan, M.A.; Khairuzzaman, A. A New Chapter in Pharmaceutical Manufacturing: 3D-Printed Drug Products. Adv. Drug Deliv. Rev. 2017, 108, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. Medical Applications for 3D Printing: Current and Projected Uses. Pharm. Ther. 2014, 39, 704–711. [Google Scholar]
- Masood, S. Application of Fused Deposition Modelling in Controlled Drug Delivery Devices. Assem. Autom. 2007, 27, 215–221. [Google Scholar] [CrossRef]
- Gioumouxouzis, C.I.; Baklavaridis, A.; Katsamenis, O.L.; Markopoulou, C.K.; Bouropoulos, N.; Tzetzis, D.; Fatouros, D.G. A 3D Printed Bilayer Oral Solid Dosage Form Combining Metformin for Prolonged and Glimepiride for Immediate Drug Delivery. Eur. J. Pharm. Sci. 2018, 120, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keikhosravi, N.; Mirdamadian, S.Z.; Varshosaz, J.; Taheri, A. Preparation and Characterization of Polypills Containing Aspirin and Simvastatin Using 3D Printing Technology for the Prevention of Cardiovascular Diseases. Drug Dev. Ind. Pharm. 2020, 46, 1665–1675. [Google Scholar] [CrossRef]
- Seoane-Viaño, I.; Januskaite, P.; Alvarez-Lorenzo, C.; Basit, A.W.; Goyanes, A. Semi-Solid Extrusion 3D Printing in Drug Delivery and Biomedicine: Personalised Solutions for Healthcare Challenges. J. Control. Release 2021, 332, 367–389. [Google Scholar] [CrossRef]
- Khaled, S.A.; Burley, J.C.; Alexander, M.R.; Yang, J.; Roberts, C.J. 3D Printing of Five-in-One Dose Combination Polypill with Defined Immediate and Sustained Release Profiles. J. Control. Release 2015, 217, 308–314. [Google Scholar] [CrossRef]
- Gu, Y.; Chen, X.; Lee, J.-H.; Monteiro, D.A.; Wang, H.; Lee, W.Y. Inkjet Printed Antibiotic- and Calcium-Eluting Bioresorbable Nanocomposite Micropatterns for Orthopedic Implants. Acta Biomater. 2012, 8, 424–431. [Google Scholar] [CrossRef]
- Rowe, C.W.; Katstra, W.E.; Palazzolo, R.D.; Giritlioglu, B.; Teung, P.; Cima, M.J. Multimechanism Oral Dosage Forms Fabricated by Three Dimensional Printing. J. Control. Release 2000, 66, 11–17. [Google Scholar] [CrossRef]
- ZipDose Technology | Spritam | Aprecia. Available online: https://www.aprecia.com/technology/zipdose (accessed on 19 January 2022).
- Khaled, S.A.; Burley, J.C.; Alexander, M.R.; Yang, J.; Roberts, C.J. 3D Printing of Tablets Containing Multiple Drugs with Defined Release Profiles. Int. J. Pharm. 2015, 494, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Goyanes, A.; Det-Amornrat, U.; Wang, J.; Basit, A.W.; Gaisford, S. 3D Scanning and 3D Printing as Innovative Technologies for Fabricating Personalized Topical Drug Delivery Systems. J. Control. Release 2016, 234, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Goyanes, A.; Kobayashi, M.; Martínez-Pacheco, R.; Gaisford, S.; Basit, A.W. Fused-Filament 3D Printing of Drug Products: Microstructure Analysis and Drug Release Characteristics of PVA-Based Caplets. Int. J. Pharm. 2016, 514, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.; Müller, L.; Sarwinska, D.; Seidlitz, A.; Sznitowska, M.; Weitschies, W. 3D Printing of Mini Tablets for Pediatric Use. Pharmaceuticals 2021, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Okwuosa, T.C.; Pereira, B.C.; Arafat, B.; Cieszynska, M.; Isreb, A.; Alhnan, M.A. Fabricating a Shell-Core Delayed Release Tablet Using Dual FDM 3D Printing for Patient-Centred Therapy. Pharm. Res. 2017, 34, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Sadia, M.; Isreb, A.; Abbadi, I.; Isreb, M.; Aziz, D.; Selo, A.; Timmins, P.; Alhnan, M.A. From “fixed Dose Combinations” to “a Dynamic Dose Combiner”: 3D Printed Bi-Layer Antihypertensive Tablets. Eur. J. Pharm. Sci. 2018, 123, 484–494. [Google Scholar] [CrossRef]
- Wu, W.; Zheng, Q.; Guo, X.; Sun, J.; Liu, Y. A Programmed Release Multi-Drug Implant Fabricated by Three-Dimensional Printing Technology for Bone Tuberculosis Therapy. Biomed. Mater. 2009, 4, 065005. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Advantages | Limitations |
|---|---|
| Complimentary mechanism of action and synergistic effects. Lower doses of individual drugs reduce the frequency of side effects and improve tolerance to treatment. | Less dosage flexibility (it is not possible to change individual doses for each ingredient/Difficulty in dose adjustment. |
| Fewer tablets and simplification of the dosing schedule (preferably once a day in the morning) | It is best to start and stabilize patients on individual tablets in some situations before starting the corresponding FDC product. |
| Lower medical costs/Reduced cost. The price of an FDC formulation is usually comparable to, or less than, the total price of the individual components. | Difficulties in identifying the source of possible undesirable actions/Misidentifying the causative medicine when the patient experiences side effects/Some adverse effects are common to many active ingredients, so it may be challenging to identify which medicine is responsible. |
| Faster achievement of blood pressure control/Glycemic goals (improved glycemic control)/Pain reduction, etc., and treatment targets. | Over- or underdosing. Inadvertent duplication of FDC and single-agent prescriptions occurring. |
| Convenience/Ease in dispensing. Improves adherence and lowers default rate. Several logistical advantages, such as ordering, planning and drug management. | One of the significant issues with FDCs is the issue of rationality—Several studies from parts of Asia, India, and Latin America have shown that many FDCs are not rational. Furthermore, the government of some countries has banned several FDCs. |
| Reduction in pill burden/ Simple treatment plan. | The use of one or more broad-spectrum antibiotics in combination (FDC) can also cause serious problems for patients’, e.g., antibiotic-associated diarrhea and increased risk of developing resistance to one or more antibiotics. |
| All of the above elements improve cooperation between the patient and doctor, which in turn improves effective treatment. | Formulation scientists experience challenges in the development stages of multi-drug formulations, such as compatibility issues among active ingredients and excipients affecting solubility and dissolution. |
| Trade Name | Components | Company | Geography | Approval Year |
|---|---|---|---|---|
| Polypills with marketing approval | ||||
| Atamra CV Kit | Atorvastatin, Ramipril, Clopidogrel | Amra Remedies | India | 2015 |
| CV-Pill Kit | Ramipril, Metoprolol, Atorvastatin, Aspirin | Torrent Pharmaceuticals | India | 2013 |
| Heart Pill | Ramipril, Atorvastatin, Aspirin | Excella Pharma | India | 2015 |
| Imprida HCT | Amlodipine, Valsartan Hydrochlorothiazid | Novartis | Austria, Belgium, Bulgaria, Croatia, Czech Republic, Cyprus, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia | 2009 |
| Polycap | Aspirin, Ramipril, Hydrohlortiazyd, Atenolol, Simvastatin | Cadila Pharmaceuticals | India and Zambia | 2009 |
| Polypill—E | Aspirin, Atorvastatin, Hydrohlortiazyd, Enalapril | Alborz Darou Pharmaceuticals | Iran | 2015 |
| Polypill—V | Aspirin, Atorvastatin, Hydrohlortiazyd, Valsartan | Alborz Darou Pharmaceuticals | Iran | 2015 |
| Ramitorva | Aspirin, Ramipril, Atorvastatin | Zydus Cadila Healthcare | India | 2014/2015 |
| RIL-AA | Ramipril, Atorvastatin, Aspirin | East-West Pharma | India | 2014/2015 |
| Starpill | Aspirin, Losartan, Atenolol, Atorvastatin | Cipla | India | 2014/2015 |
| Polytorva | Aspirin, Ramipril, Atorvastatin | USV | India | 2015 |
| Trinomia Sincronium Iltria | Aspirin, Ramipril, Atorvastatin or Simvastatin | Ferrer | Latin America: Guatemala, Honduras, Dominican Republic, El Salvador, Nicaragua, Argentina, Chile, Paraguay, Ecuador, Mexico; Europe: Belgium, Bulgaria, Germany, Finland, France, Greece, Ireland, Italy, Austria, Poland, Portugal, Romania, Spain, Sweden, Czech Republic. | 2014/2015 |
| Triveram | Perindopril, Amlodipine, Atorvastatin | Servier | Austria, Belgium, Bulgaria, Croatia, Czech Republic, Cyprus, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia | 2015 |
| Triplixam | Amlodipine, Perindopril Indapamide | Servier | Austria, Belgium, Bulgaria, Croatia, Czech Republic, Cyprus, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia | 2014 |
| ZYCAD-4 kit | Ramipril, Metoprolol, Atorvastatin, Aspirin | Zydus Cadila Healthcare | India | 2015 |
| Polypills in development | ||||
| GSK3074477 | Amlodipine, Rosuvastatin | GlaxoSmithKline | - | - |
| Livalo | Pitavastatin, Valsartan | JW Pharmaceutical | - | - |
| Unnamed | Valsartan, Rosuvastatin | EMS | - | - |
| Drugs | Dosage Form | Form Rational | Year | Ref. No |
|---|---|---|---|---|
| Metformin HCl Evogliptin tartrate | Bilayer tablets | Synergistic effect in diabetes | 2021 | [25] |
| Metformin HCl Dapagliflozin l-proline | Bilayer tablets | Synergistic effect in diabetes | 2021 | [27] |
| Trimetazidine HCl, Clopidogrel bisulphate | Bilayer tablets | Cytoprotective anti-ischemic, platelet inhibitor in acute coronary syndromes | 2014 | [28] |
| Metformin HCl, Glimipiride | Bilayer tablets | Synergistic effect in diabetes | 2011 | [29] |
| Metformin HCl Atorvastatin Calcium | Bilayer tablets | To develop polytherapy for the treatment of NIDDS and hyperlipidemia | 2011 | [30] |
| Piracetam Vinpocetine | Bilayer tablets | Synergistic effect in Alzheimer disease | 2011 | [31] |
| Trihexyphenidyl HCl Ziprasidone HCl. | Bilayer floating tablets | For extending the metabolism and improving the bioavailability of both APIs; simultaneous administration of antipsychotics and anticholinergics to prevent or treat extrapyramidal syndrome (EPS) | 2011 | [26] |
| Cefixime Trihydrate, Dicloxacillin Sodium | Bilayer tablets | Synergistic effect in bacterial infections | 2011 | [32] |
| Amlodipine besylate, Metoprolol Succinate | Bilayer tablets | Synergistic effect in hypertension | 2009, 2011 | [33,34] |
| Diclofenac Sodium, Paracetamol | Bilayer tablets | Synergistic effect in pain | 2010 | [35] |
| Atenolol, Lovastatin | Bilayer floating tablets | Synergistic effect in hypertension and biphasic release profile | 2009 | [36] |
| Montelukast, Levocetrizine | Bilayer tablets | Improvement of the stability of drugs in combination | 2009 | [37] |
| Salbutamol Theophylline | Bilayer tablets | Synergistic effect of drugs in asthma | 2009 | [38] |
| Rifampicin, Isoniazid | Capsule and tablet in capsule | To avoid interaction b/w incompatible drugs | 2007 | [39] |
| Ranitidine, Aspirin | Single-layer coated tablets | Minimizing the contact of two incompatible drugs | 2003 | [40] |
| Misoprostol, Diclofenac | Bilayer tablets | To minimize contact b/w drugs | 2007 | [41] |
| Product Name | Chemical Name | Dosage Form | Therapeutic | Manufacturer/ Developer | Ref |
|---|---|---|---|---|---|
| Alprax Plus | Sertraline/ Alprazolam | Bilayer tablets | Anti-depressant | Torrent Pharmaceuticals Ltd. | [44] |
| Glycomet-GP2Forte | Metformin hydrochloride/Glimepiride | Bilayer tablets | Anti-diabetic | USV Limited | [45] |
| Lopressor HCT | Metoprolol/Hydrochlorothiazide | Bilayer tablets | Antihypertensive | Novartis Pharmaceuticals Corporation | [46] |
| Diovan HCT | Valsartan/ Hydrochlorothiazide | Bilayer tablets | Antihypertensive | Novartis Pharmaceuticals Corporation | [47] |
| Lotensin HCT | Benazepril/Hydrochlorothiazide | Bilayer tablets | Antihypertensive | Novartis Pharmaceuticals Corporation | [48] |
| Clarinex-D | Desloratadine/Pseudoephedrine sulphate | Bilayer tablets | Allergic rhinitis | MSD | [49] |
| Treximet | Sumatriptan/Naproxen sodium | Bilayer tablets | Migraine | Pernix Therapeutics | [50] |
| Atripla | Efavirenz/Emtricitabine/Tenofovir disoproxil fumarate | Multilayer tablets | HIV/AIDS | Gilead Sciences | [51] |
| Under development -In clinical trials/Patent EP 2 682 112 A1 | Flurbiprofen 100 mg Famotidine 20 mg | Multilayer tablet | An NSAID with anti-inflammatory, analgesic and antipyretic activities, an H2 receptor antagonist used for preventing or minimizing gastroin-testinal side effects caused by NSAIDs | Pharmaceutical Research Unit, Jordan | [52] |
| Delivery System | Brand Name | Active Pharmaceutical Ingredient | Manufacturing Company |
|---|---|---|---|
| Hydrodynamically Balanced | Madopar® | Levodopa and Benserazide | Intec Pharma (Israel) |
| Raft-forming | Gaviscon® Tablets | Sodium bicarbonate and Calcium carbonate | Reckitt Benckiser Healthcare (UK) Ltd. |
| Topalkan® | Aluminum and magnesium | Pierre Fabre Medicament (France) | |
| Expandable | Accordion Pill® | Levodopa and Carbidopa | Intec Pharma (Israel) |
| Janumet® XR | Sitagliptin and Metformin | Merck Sharp & Dohme (USA) |
| Product | Company | HME Purpose | Indication | Approval Year |
|---|---|---|---|---|
| Kaletra (Ritonavir, Lopinavir) | AbbVie | Amorphous dispersion | Anti-viral (HIV) | 2000 |
| Viekira Pak (Ombitasvir, Paritaprevir, Ritonavir, dasabuvir) | AbbVie | Amorphous dispersion | Anti-viral (HCV) | 2014 |
| Zok-Zid tablet (Metoprolol tartrate, hydrochlorothiazide) | Pfizer | Hot-melt co-extrusion | Hypertension | 2012 |
| NuvaRing (Etonogestrel, Ethinyl Estradiol) | Merck | Shaped system | Contraceptive | 2001 |
| Eucreas (Vildagliptin, Metformin HCl) | Novartis | Melt granulation | Diabetes | 2008 |
| Dapivirine, Maraviroc, BMS793, CMPD 167 | Particle sciences | Shaped system | Anti-viral (HIV) | Under development |
| 3D Printing Technology Used | Formulations | API(s) | Excipient(s) | Year | Ref. No |
|---|---|---|---|---|---|
| Extrusion | Immediate/sustained polypill | Aspirin, hydrochlorothiazide, ramipril, pravastatin sodium, atenolol | Cellulose acetate, D-mannitol, polyethylene glycol (PEG 6000) sodium starch glycolate, polyvinylpyrrolidone (Povidon K30), hydroxypropyl methylcellulose (Methocel™ K100MCR), lactose | 2015 | [88] |
| Semi-solid extrusion (SSE) | Multiactive tablets (polypill) | Nifedipine, Glipizide, Captopril | Hydroxypropyl methylcellulose (HPMC 2208), polyethylene glycol (PEG 6000), tromethamine, lactose, sodium chloride, D-mannitol, croscarmellose sodium, microcrystalline cellulose, sodium starch glycolate, hydroxypropyl methylcellulose (Methocel™), cellulose acetate | 2015 | [92] |
| Stereolithography (SLA) | Modified tablets | 4-Aminosalicylic acid and paracetamol | Polyethylene glycol diacrylate, diphenyl (2,4,6-trimethylbenzoyl) phosphine oxide, and (PEG 300) | 2016 | [93] |
| Fused deposition modeling (FDM) | Caplets | Paracetamol and caffeine | Polyvinyl alcohol | 2016 | [94] |
| Mini-tablets (for pediatric use) | Caffeine and propranolol | Hyprolose and Hypromellose | 2021 | [95] | |
| Bilayer dosage form | Metformin and Glimepiride | Eudragit® RL, polyvinyl alcohol (PVA) | 2018 | [85] | |
| Shell-core tablets | Theophylline, budesonide, and diclofenac sodium | Core: Polyvinylpyrrolidone, triethyl citrate, talc or tribasic phosphate sodium, and APIShell: Eudragit® L 100–55, triethyl citrate, and talc | 2017 | [96] | |
| Bilayer tablet | Enalapril maleate, and hydrochlorothiazide | Methacrylate polymer | 2018 | [97] | |
| Inkjet 3D printing | Multidrug implant | Rifampicin and isoniazid | Polyethylene oxide, polylactic acid (PLA), polyvinyl alcohol (PVA) | 2009 | [98] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janczura, M.; Sip, S.; Cielecka-Piontek, J. The Development of Innovative Dosage Forms of the Fixed-Dose Combination of Active Pharmaceutical Ingredients. Pharmaceutics 2022, 14, 834. https://doi.org/10.3390/pharmaceutics14040834
Janczura M, Sip S, Cielecka-Piontek J. The Development of Innovative Dosage Forms of the Fixed-Dose Combination of Active Pharmaceutical Ingredients. Pharmaceutics. 2022; 14(4):834. https://doi.org/10.3390/pharmaceutics14040834
Chicago/Turabian StyleJanczura, Magdalena, Szymon Sip, and Judyta Cielecka-Piontek. 2022. "The Development of Innovative Dosage Forms of the Fixed-Dose Combination of Active Pharmaceutical Ingredients" Pharmaceutics 14, no. 4: 834. https://doi.org/10.3390/pharmaceutics14040834