
Development of a Population Pharmacokinetic Model of Busulfan in Children and Evaluation of Different Sampling Schedules for Precision Dosing

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Blood Sampling
2.2. Population Pharmacokinetic Modeling
2.3. Model Selection Criteria
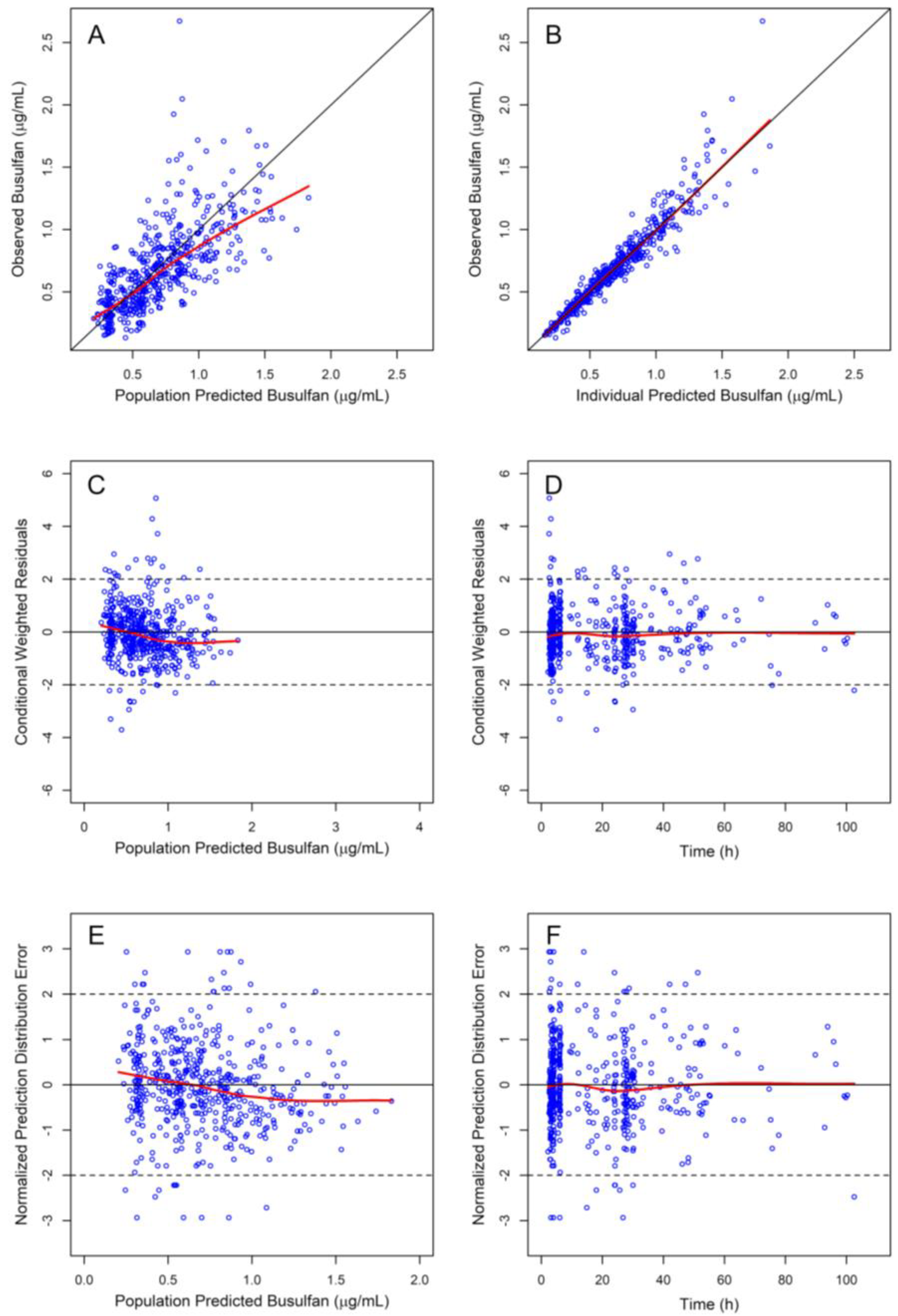
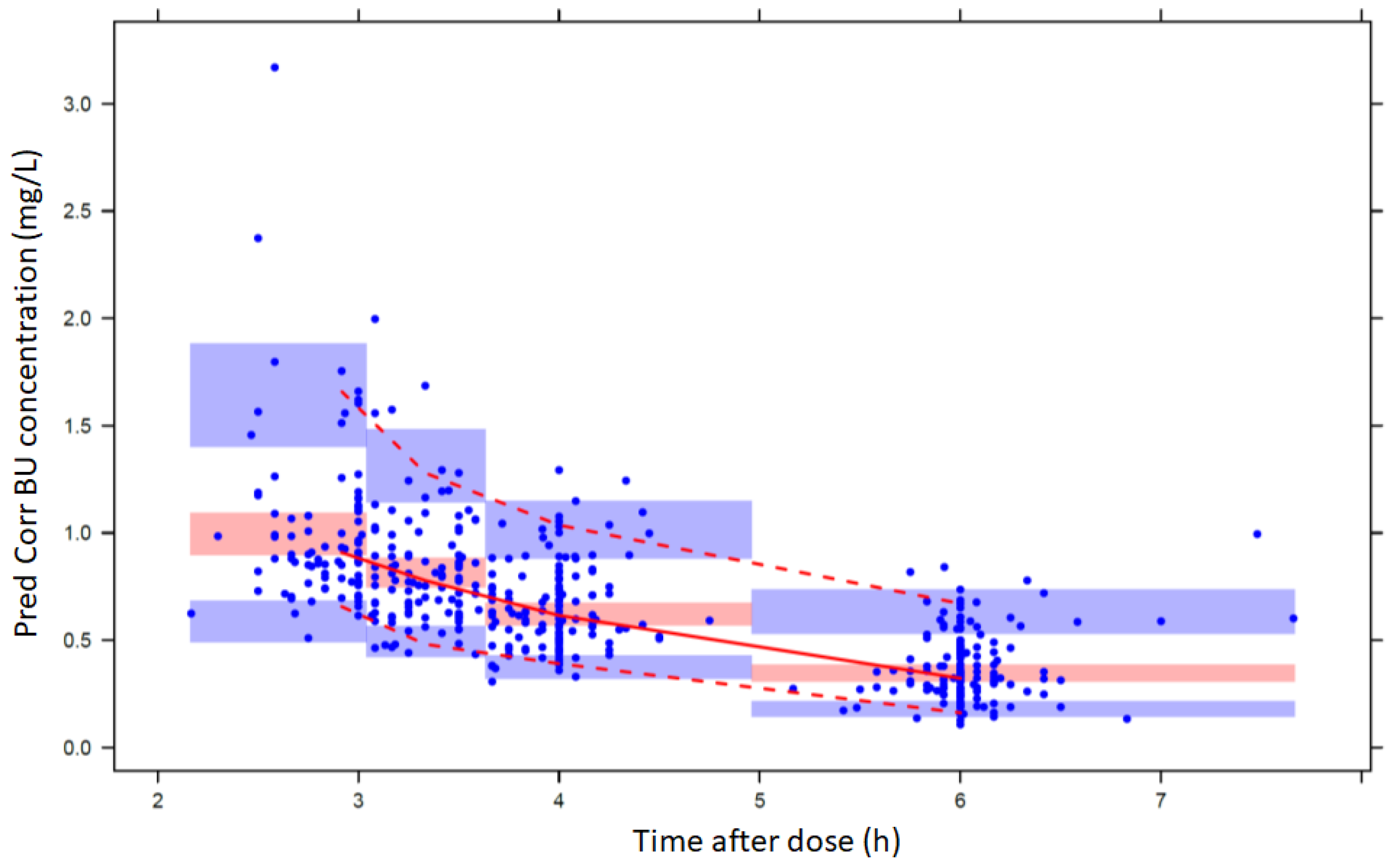
2.4. Pharmacokinetic Model Qualification
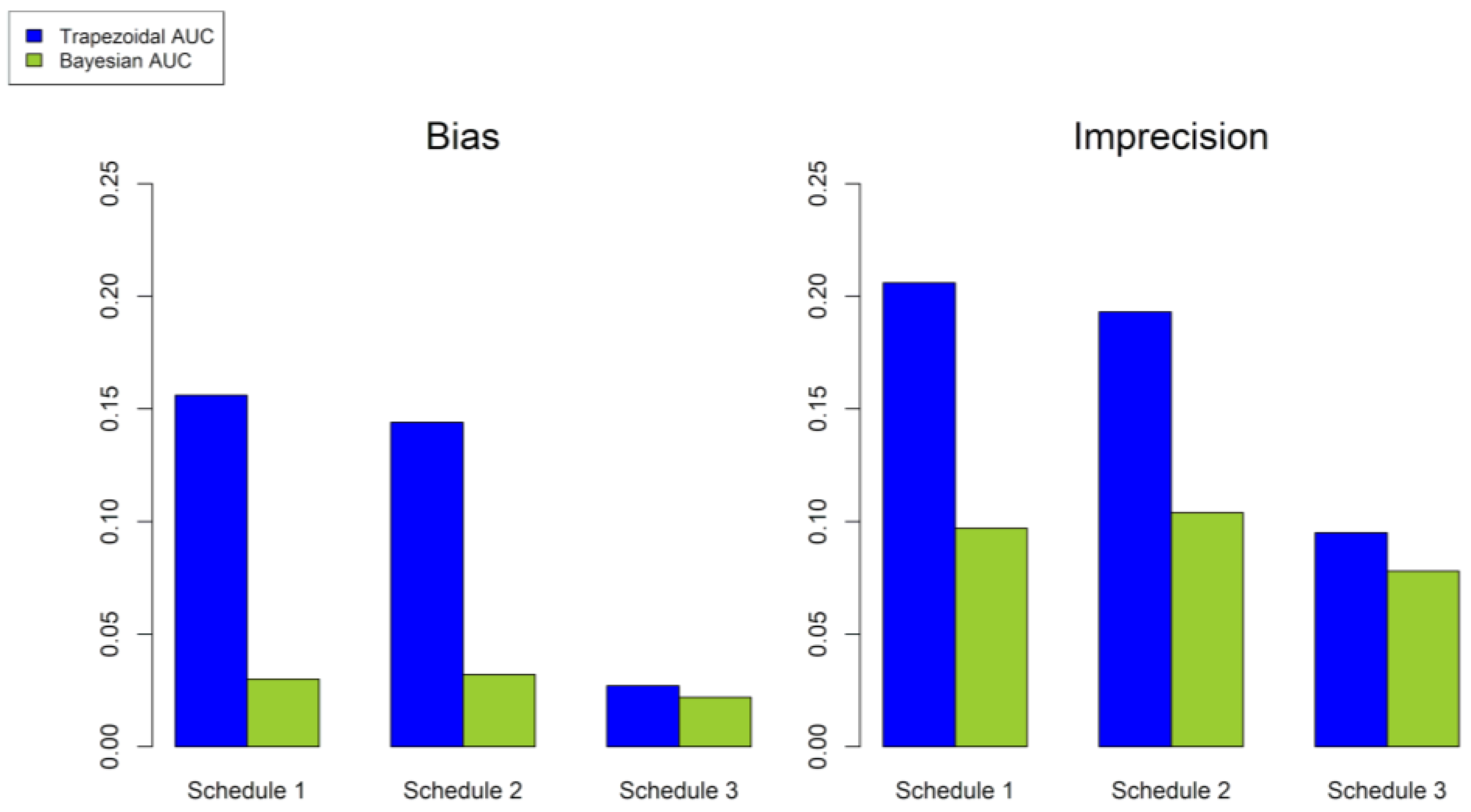
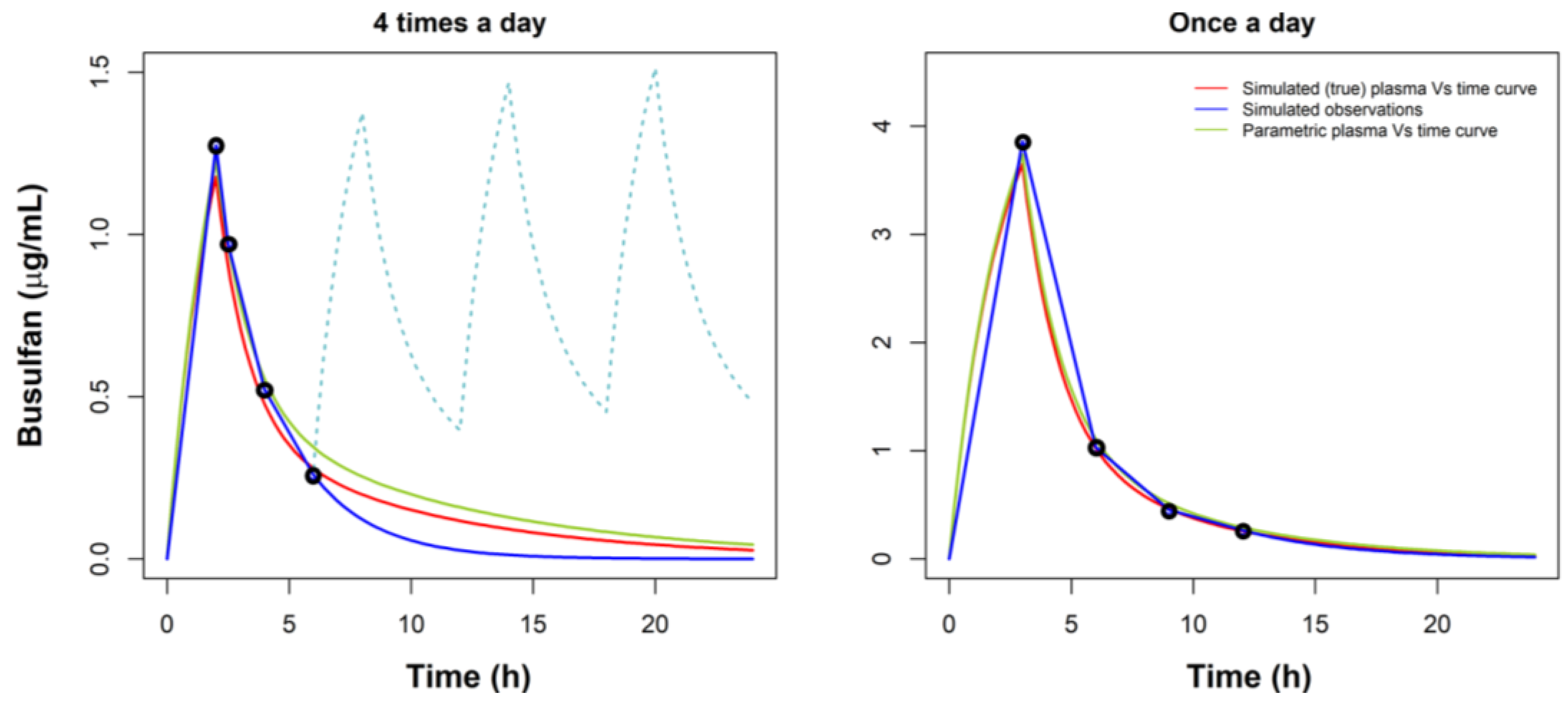
2.5. Evaluation of Model Performance for Dose Individualization
3. Results
3.1. Development of the Structural and Base PopPK Model
3.2. Development of the Final Covariate Model
3.3. BU Dose Individualization
3.4. Evaluation of Model Performance for Dose Individualization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galton, G.A. Myleran in Chronic Myeloid Leukemia: Results of Treatment. Lancet 1953, 31, 208–213. [Google Scholar] [CrossRef]
- Tutschka, P.J.; Santos, G.W. Bone marrow transplantation in the busulfan-treated rat. II. Effect of cyclophosphamide and antithymic serum on the presensitized state. Transplantation 1975, 20, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.W.; Tutschka, P.J.; Brookmeyer, R.; Saral, R.; Beschorner, W.E.; Bias, W.B.; Braine, H.G.; Burns, W.H.; Elfenbein, G.J.; Kaizer, H.; et al. Marrow transplantation for acute nonlymphocytic leukemia after treatment with busulfan and cyclophosphamide. N. Engl. J. Med. 1983, 309, 1347–1353. [Google Scholar] [CrossRef]
- Hassan, M. The role of busulfan in bone marrow transplantation. Med. Oncol. 1999, 16, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; Hassan, M.; Bekassy, A.N. High busulfan concentrations are associated with increased transplant-related mortality in allogeneic bone marrow transplant patients. Bone Marrow Transplant. 1997, 20, 909–913. [Google Scholar] [CrossRef] [Green Version]
- Dix, S.P.; Wingard, J.R.; Mullins, R.E.; Jerkunica, I.; Davidson, T.G.; Gilmore, C.E.; York, R.C.; Lin, L.S.; Devine, S.M.; Geller, R.B.; et al. Association of busulfan area under the curve with veno-occlusive disease following BMT. Bone Marrow Transplant. 1996, 17, 225–230. [Google Scholar]
- Grochow, L.B.; Jones, R.J.; Brundrett, R.B.; Braine, H.G.; Chen, T.L.; Saral, R.; Santos, G.W.; Colvin, O.M. Pharmacokinetics of busulfan: Correlation with veno-occlusive disease in patients undergoing bone marrow transplantation. Cancer Chemother. Pharmacol. 1989, 25, 55–61. [Google Scholar] [CrossRef]
- McCune, J.S.; Gooley, T.; Gibbs, J.P.; Sanders, J.E.; Petersdorf, E.W.; Appelbaum, F.R.; Anasetti, C.; Risler, L.; Sultan, D.; Slattery, J.T. Busulfan concentration and graft rejection in pediatric patients undergoing hematopoietic stem cell transplantation. Bone Marrow Transplant. 2002, 30, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Slattery, J.T.; Clift, R.A.; Buckner, C.D.; Radich, J.; Storer, B.; Bensinger, W.I.; Soll, E.; Anasetti, C.; Bowden, R.; Bryant, E.; et al. Marrow transplantation for chronic myeloid leukemia: The influence of plasma busulfan levels on the outcome of transplantation. Blood 1997, 89, 3055–3060. [Google Scholar] [CrossRef]
- Andersson, B.S.; Kashyap, A.; Gian, V.; Wingard, J.R.; Fernandez, H.; Cagnoni, P.J.; Jones, R.B.; Tarantolo, S.; Hu, W.W.; Blume, K.G.; et al. Conditioning therapy with intravenous busulfan and cyclophosphamide (IV BuCy2) for hematologic malignancies prior to allogeneic stem cell transplantation: A phase II study. Biol. Blood Marrow Transplant. 2002, 8, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Russell, J.A.; Tran, H.T.; Quinlan, D.; Chaudhry, A.; Duggan, P.; Brown, C.; Stewart, D.; Ruether, J.D.; Morris, D.; Glück, S.; et al. Once-daily intravenous busulfan given with fludarabine as conditioning for allogeneic stem cell transplantation: Study of pharmacokinetics and early clinical outcomes. Biol. Blood Marrow Transplant. 2002, 8, 468–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelink, I.H.; Bredius, R.G.; Belitser, S.V.; Suttorp, M.M.; Bierings, M.; Knibbe, C.A.; Egeler, M.; Lankester, A.C.; Egberts, A.C.; Zwaveling, J.; et al. Association between busulfan exposure and outcome in children receiving intravenous busulfan before hematologic stem cell transplantation. Biol. Blood Marrow Transplant. 2009, 15, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güngör, T.; Teira, P.; Slatter, M.; Stussi, G.; Stepensky, P.; Moshous, D.; Vermont, C.; Ahmad, I.; Shaw, P.J.; da Cunha, J.M.T.; et al. Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients with chronic granulomatous disease: A prospective multicentre study. Lancet 2014, 383, 436–448. [Google Scholar] [CrossRef]
- Ansari, M.; Théoret, Y.; Rezgui, M.A.; Peters, C.; Mezziani, S.; Desjean, C.; Vachon, M.F.; Champagne, M.A.; Duval, M.; Krajinovic, M.; et al. Association between busulfan exposure and outcome in children receiving intravenous busulfan before hematopoietic stem cell transplantation. Ther. Drug Monit. 2014, 36, 93–99. [Google Scholar] [CrossRef]
- Ward, J.; Kletzel, M.; Duerst, R.; Fuleihan, R.; Chaudhury, S.; Schneiderman, J.; William, T.T. Single daily busulfan dosing for infants with nonmalignant diseases undergoing reduced-intensity conditioning for allogeneic hematopoietic progenitor cell transplantation. Biol. Blood Marrow Transplant. 2015, 21, 1612–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelink, I.H.; Lalmohamed, A.; van Reij, E.M.; Dvorak, C.C.; Savic, R.M.; Zwaveling, J.; Bredius, R.G.; Egberts, A.C.; Bierings, M.; Kletzel, M.; et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: A multicentre, retrospective cohort analysis. Lancet Haematol. 2016, 3, e526–e536. [Google Scholar] [CrossRef] [Green Version]
- Andersson, B.S.; Thall, P.F.; Madden, T.; Couriel, D.; Wang, X.; Tran, H.T.; Anderlini, P.; De Lima, M.; Gajewski, J.; Champlin, R.E. Busulfan systemic exposure relative to regimen-related toxicity and acute graft versus host disease: Defining a therapeutic window for i.v. BuCy2 in chronic myelogenous leukemia. Biol. Blood Marrow Transplant. 2002, 8, 477–485. [Google Scholar] [CrossRef] [Green Version]
- Busilvex®. Pierre Fabre Médicament Production (Site Aquitaine Pharm International, Avenue du Béarn –Idron, F-64320, France). Available online: https://www.ema.europa.eu/en/documents/product-information/busilvex-epar-product-information_en.pdf (accessed on 1 February 2022).
- Peterfreund, R.A.; Philip, J.H. Critical parameters in drug delivery by intravenous infusion. Expert. Opin. Drug Deliv. 2013, 10, 1095–1108. [Google Scholar] [CrossRef]
- Lovich, M.A.; Doles, J.; Peterfreund, R.A. The impact of carrier flow rate and infusion set dead volume on the dynamics of intravenous drug delivery. Anesth. Analg. 2005, 100, 1048–1055. [Google Scholar] [CrossRef]
- Bartels, K.; Moss, D.R.; Peterfreund, R.A. An analysis of drug delivery dynamics via a pediatric central venous infusion system: Quantification of delays in achieving intended doses. Anesth. Analg. 2009, 109, 1156–1161. [Google Scholar] [CrossRef]
- Neff, S.B.; Neff, T.A.; Gerber, S.; Weiss, M.M. Flow rate, syringe size and architecture are critical to start-up performance of syringe pumps. Eur. J. Anaesthesiol. 2007, 24, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Lovich, M.A.; Kinnealley, M.E.; Sims, N.M.; Peterfreund, R.A. The delivery of drugs to patients by continuous intravenous infusion: Modeling predicts potential dose fluctuations depending on flow rates and infusion system dead volume. Anesth. Analg. 2006, 102, 1147–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neroutsos, E.; Athanasiadou, I.; Paisiou, A.; Zisaki, K.; Goussetis, E.; Archontaki, H.; Tsirigotis, P.; Kitra, M.; Grafakos, S.; Spyridonidis, A.; et al. Dose individualization of intravenous busulfan in pediatric patients undergoing bone marrow transplantation: Impact and in vitro evaluation of infusion lag-time. J. Pharm. Pharmacol. 2021, 73, 1340–1350. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Lindbom, L.; Pihlgren, P.; Jonsson, E.N. PsN-Toolkit—a collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Holford, N.H.G. Mechanistic Basis of Using Body Size and Maturation to Predict Clearance in Humans. Drug Metab. Pharmacokinet. 2009, 24, 25–36. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean/Number | SD | Range |
|---|---|---|---|
| Number of patients | 76 | ||
| Male patients | 49 | ||
| Age (years) | 7.6 | 5.1 | 0.5–19 |
| Body Weight (kg) | 30.6 | 21.6 | 7.38–104 |
| Height (cm) | 121.8 | 35.2 | 0.71–207 |
| BSA (m2) | 0.99 | 0.49 | 0.09–2.44 |
| Sr Cr (mg/dL) | 0.36 | 0.15 | 0.10–0.90 |
| CKPD-EPI (mL/min/1.73 m2) | 197 | 41 | 107–346 |
| BW Category (kg) | Dose (mg/kg) | Lag-Time (min) | Number of Patients (Ν) | Median BW, kg (Range) | Median Age, Years (Range) |
|---|---|---|---|---|---|
| <9 | 1 | 40 | 4 | 8.02 (7.4–8.7) | 0.7 (0.58–0.75) |
| 9–16 | 1.2 | 40 | 20 | 12.31 (9.2–15.0) | 3.1 (0.5–7.0) |
| 16–23 | 1.1 | 35/25 | 13 | 19.35 (16.0–66.7) | 5.23 (3.0–7.0) |
| 23–34 | 0.95 | 20 | 16 | 28.7 (25.0–34.0) | 7.9 (5.0–12.0) |
| >34 | 0.8 | 10/5 | 23 | 58.1 (34.5–104.0) | 13.9 (6.0–19.0) |
| Parameter | ΝOΝΜΕΜ Estimation | Bootstrap Analysis | |||||
|---|---|---|---|---|---|---|---|
| Estimate | SE | RSE% | Mean | SD | CV% | CI (2.5–97.5%) | |
| CL (L/h) | 10.7 | 0.431 | 4.05% | 10.7 | 0.430 | 4.04% | 9.79–1.47 |
| V1 (L) | 39.5 | 2.70 | 6.84% | 39.1 | 2.66 | 6.79% | 34.0–44.3 |
| Q (L/h) | 4.68 | 0.712 | 15.2% | 4.78 | 0.701 | 14.7% | 3.65–6.30 |
| V2 (L) | 17.5 | 3.00 | 17.2% | 17.5 | 3.06 | 17.5% | 12.4–24.4 |
| CL IIV | 0.284 | 0.0147 | 5.18% | 0.282 | 0.0259 | 9.16% | 0.231–0.335 |
| V1 IIV | 0.409 | 0.058 | 14.2% | 0.412 | 0.0728 | 17.7% | 0.267–0.554 |
| Cor. CL-V1 | 0.679 | 0.025 | 3.68% | 0.680 | 0.0807 | 11.9% | 0.495–0.813 |
| CL IOV | 0.105 | 0.00259 | 2.47% | 0.103 | 0.0125 | 12.1% | 0.078–0.127 |
| Prop. RE * | 0.126 | 0.00208 | 1.65% | 0.125 | 0.0082 | 6.56% | 0.109–0.141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neroutsos, E.; Nalda-Molina, R.; Paisiou, A.; Zisaki, K.; Goussetis, E.; Spyridonidis, A.; Kitra, V.; Grafakos, S.; Valsami, G.; Dokoumetzidis, A. Development of a Population Pharmacokinetic Model of Busulfan in Children and Evaluation of Different Sampling Schedules for Precision Dosing. Pharmaceutics 2022, 14, 647. https://doi.org/10.3390/pharmaceutics14030647
Neroutsos E, Nalda-Molina R, Paisiou A, Zisaki K, Goussetis E, Spyridonidis A, Kitra V, Grafakos S, Valsami G, Dokoumetzidis A. Development of a Population Pharmacokinetic Model of Busulfan in Children and Evaluation of Different Sampling Schedules for Precision Dosing. Pharmaceutics. 2022; 14(3):647. https://doi.org/10.3390/pharmaceutics14030647
Chicago/Turabian StyleNeroutsos, Efthymios, Ricardo Nalda-Molina, Anna Paisiou, Kalliopi Zisaki, Evgenios Goussetis, Alexandros Spyridonidis, Vasiliki Kitra, Stelios Grafakos, Georgia Valsami, and Aristides Dokoumetzidis. 2022. "Development of a Population Pharmacokinetic Model of Busulfan in Children and Evaluation of Different Sampling Schedules for Precision Dosing" Pharmaceutics 14, no. 3: 647. https://doi.org/10.3390/pharmaceutics14030647