
Latest Trends in Surface Modification for Dental Implantology: Innovative Developments and Analytical Applications


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Historical Overview of Implantology
3. Engineering Strategies in Dental Implantology
3.1. Biomaterials Composition
3.2. Implant Geometry and Surface Features
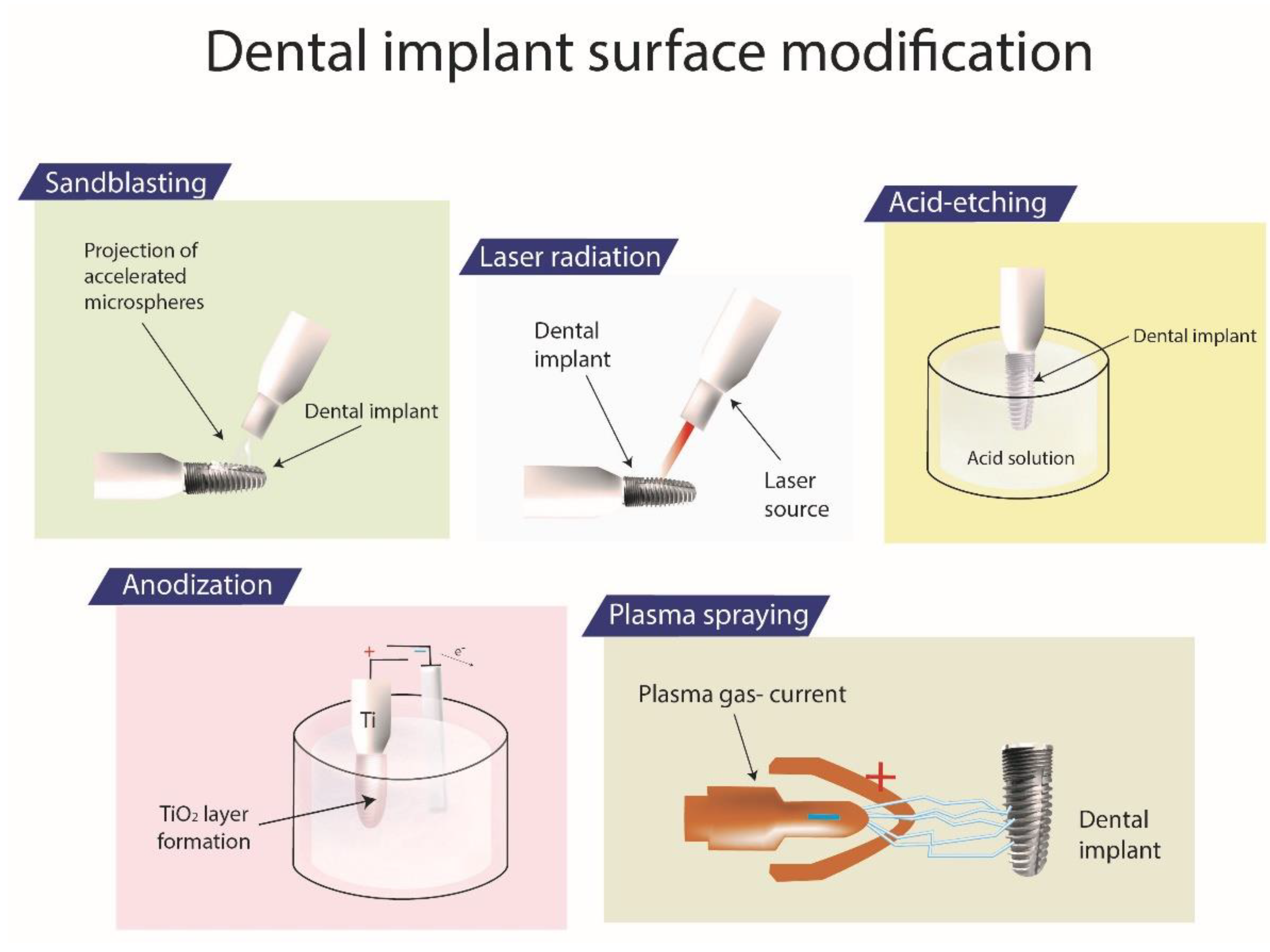
3.2.1. Sandblasting
3.2.2. Acid-Etching
3.2.3. Anodization
3.2.4. Plasma-Spraying
3.2.5. Laser Ablation
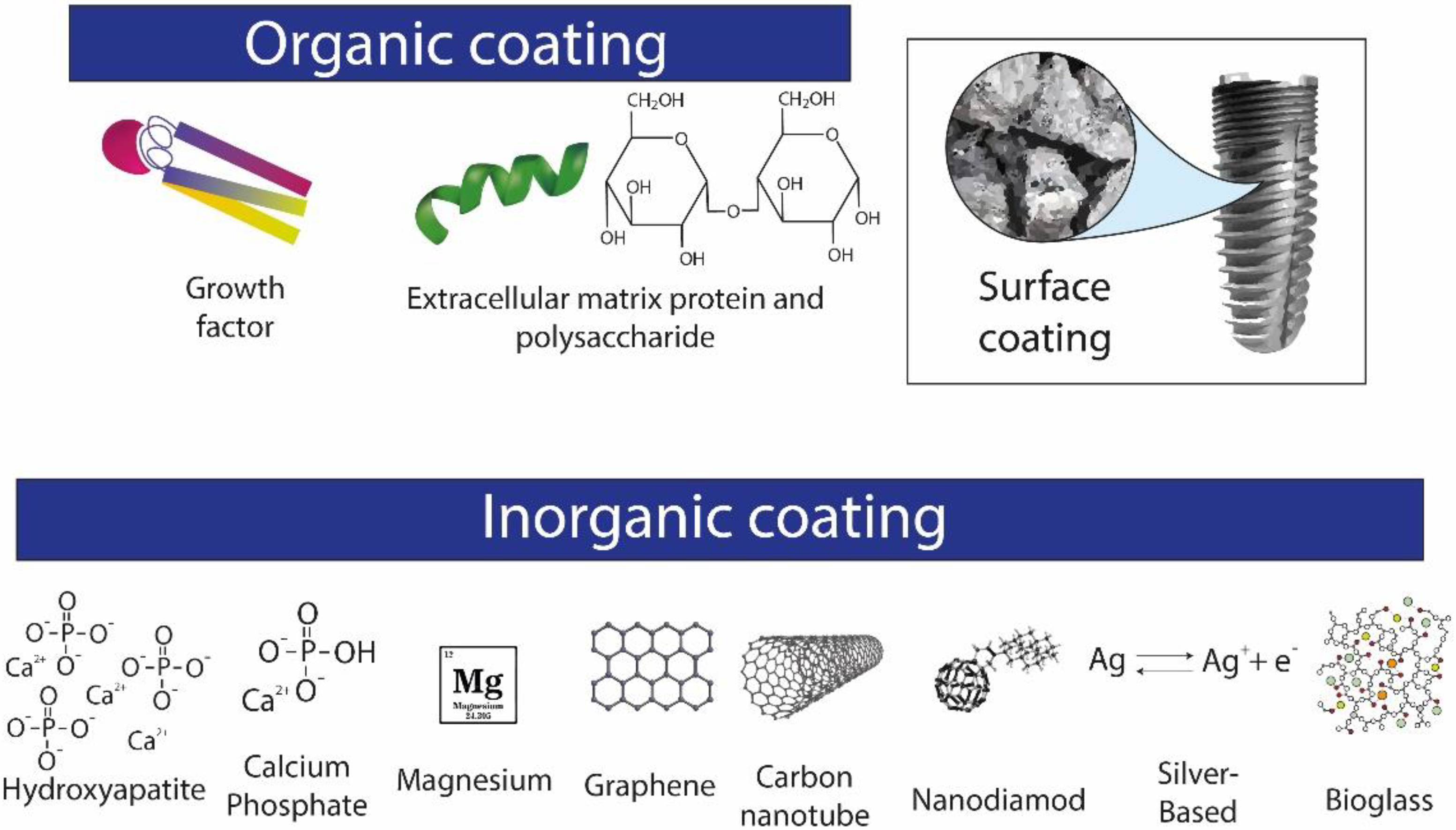
4. Coatings
4.1. Inorganic Coatings
4.1.1. Hydroxyapatite-Based Biomimetic Coatings
4.1.2. Calcium Phosphate-Based Biomimetic Coatings
4.1.3. Magnesium-Based Biomimetic Coatings
4.1.4. Graphene-Based Biomimetic Coatings
4.1.5. Carbon Nanotube-Based Coatings
4.1.6. Nanodiamond Coatings
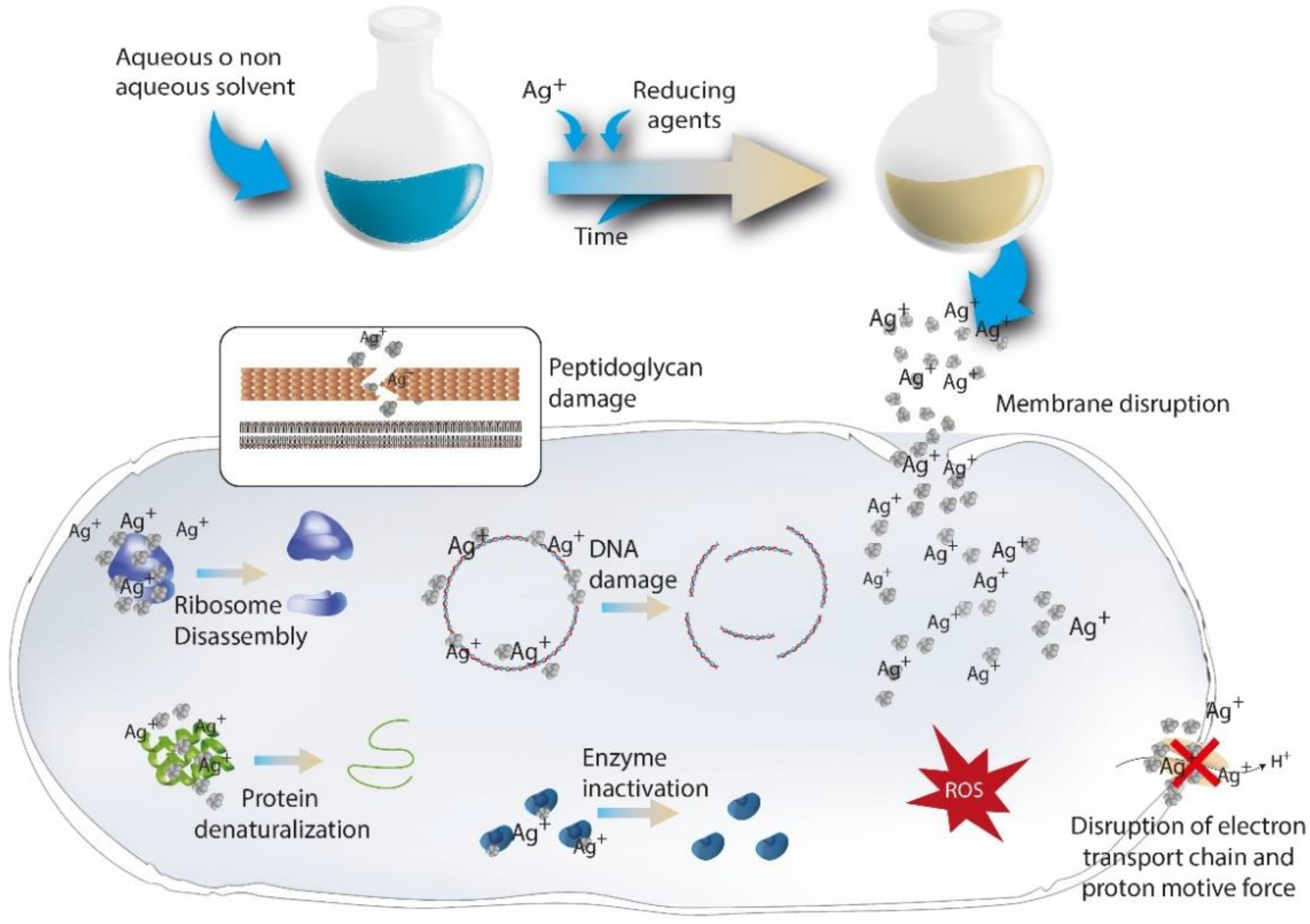
4.1.7. Silver-Based Coatings
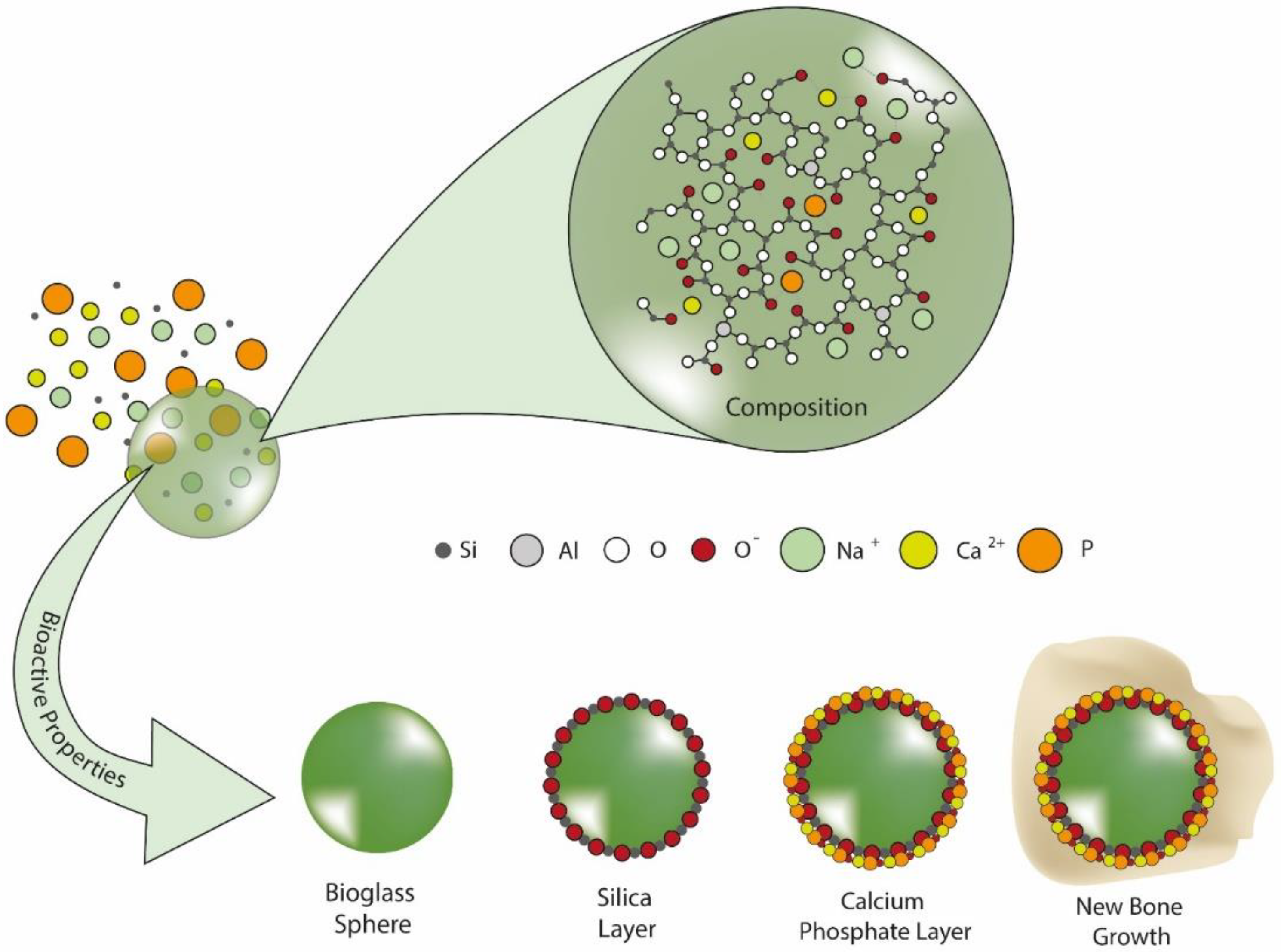
4.1.8. Bioactive Glasses
4.2. Organic Coatings
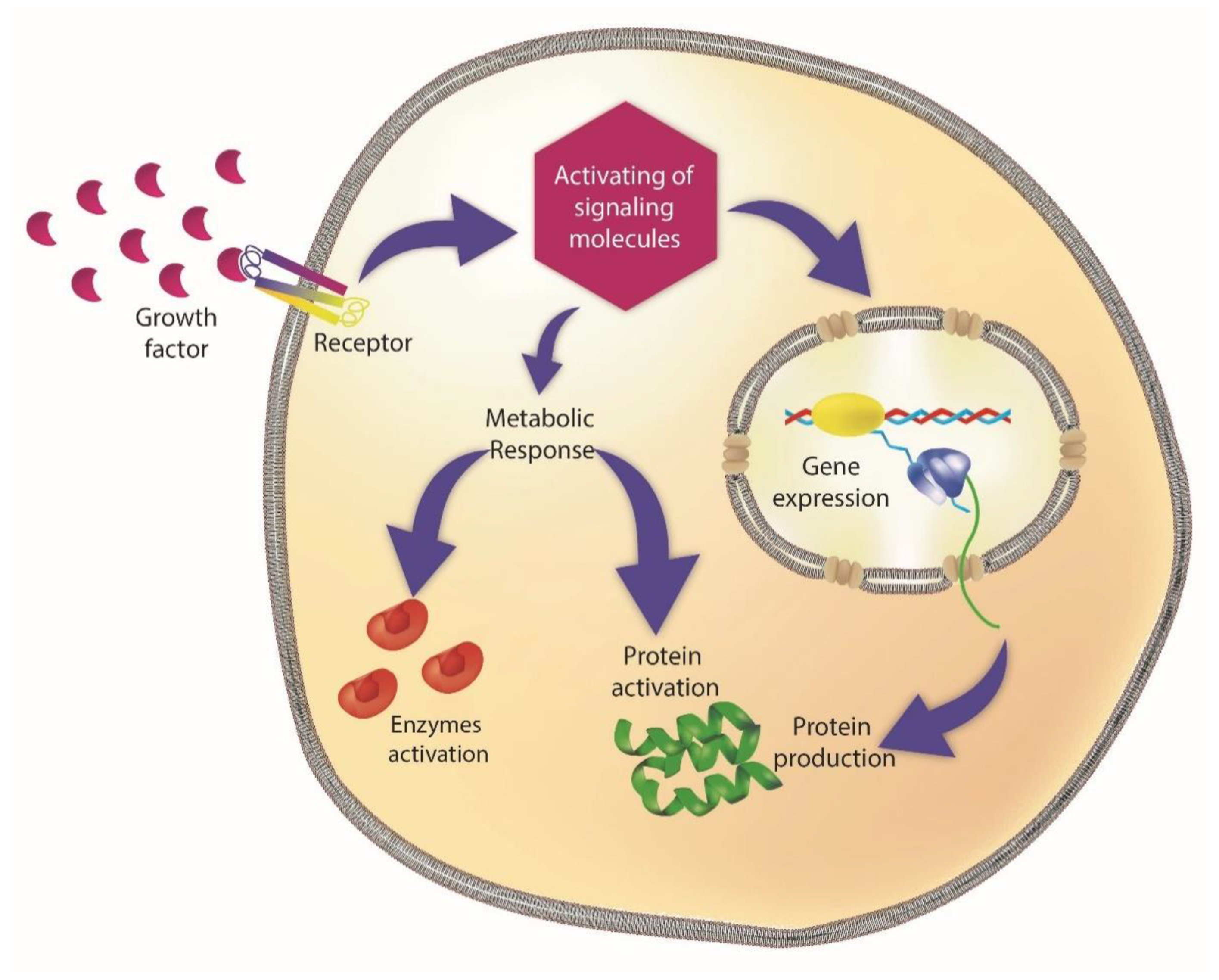
4.2.1. Growth Factors-Based Coatings
4.2.2. Extracellular Matrix Proteins and Polisaccarides
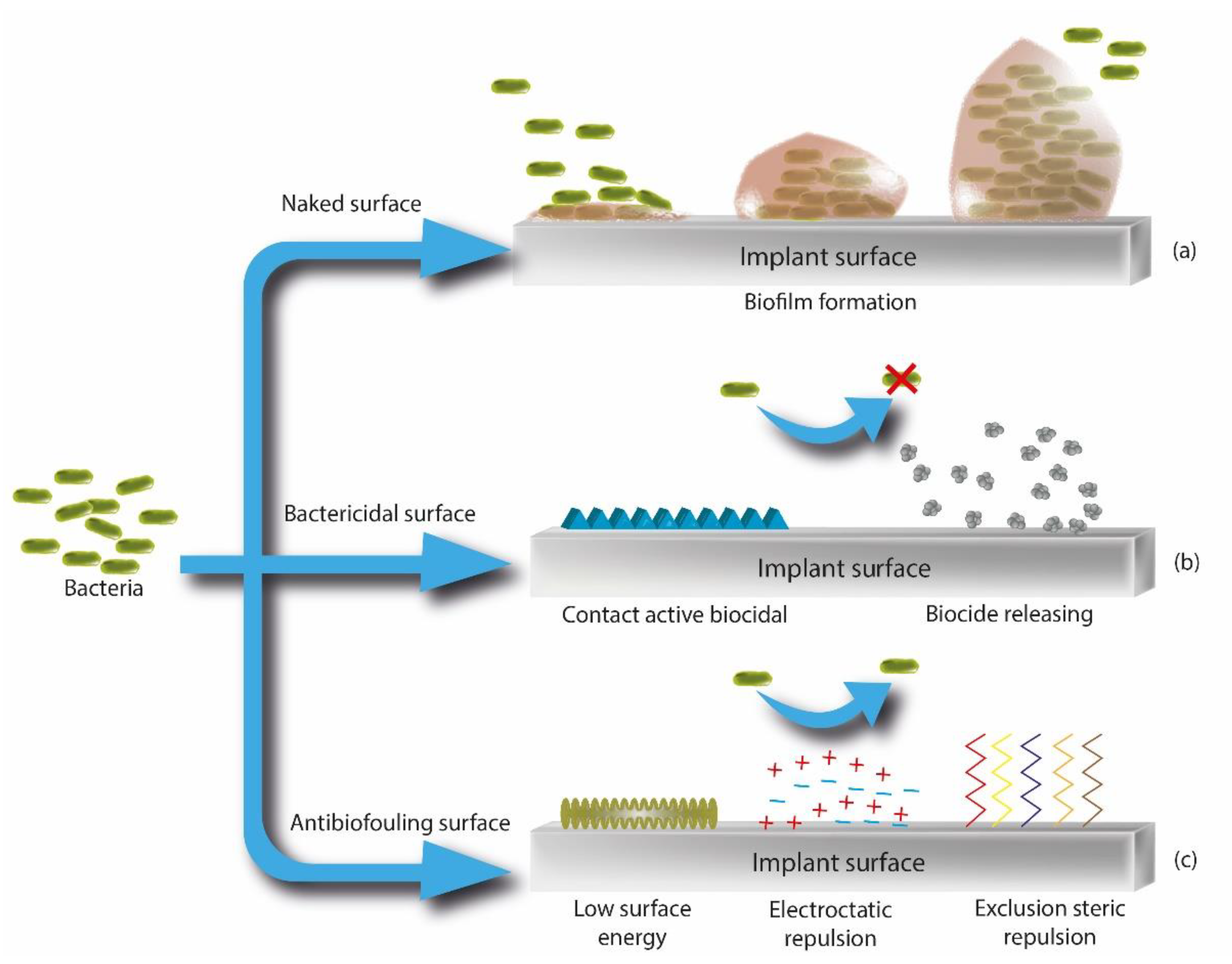
4.3. Antibacterial Strategies of Coatings
4.3.1. Drug-Releasing Coatings
4.3.2. “No-Releasing” Coatings
4.3.3. Antifouling Coatings
5. Latest Trends in Analytical Chemistry
5.1. OMICS in Dental Implantology
5.2. Detemination of Biomarkers for the Evaluation of Biomaterial Effect and Clinic Outcomes
5.3. Analytical Methods for the Characterization of Micro- and Nanosized Implant-Related Particles and Metals in Inflamed Peri-Implants Ttissues
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Orchestrating Soft Tissue Integration at the Transmucosal Region of Titanium Implants. Acta Biomater. 2021, 124, 33–49. [Google Scholar] [CrossRef]
- Asensio, G.; Vázquez-Lasa, B.; Rojo, L. Achievements in the Topographic Design of Commercial Titanium Dental Implants: Towards Anti-Peri-Implantitis Surfaces. J. Clin. Med. 2019, 8, 1982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Avila, E.D.; van Oirschot, B.A.; van den Beucken, J.J. Biomaterial-based Possibilities for Managing Peri-implantitis. J. Periodontal Res. 2020, 55, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, L.; Salcido, J.P.; Guda, T.; Ong, J.L. Current Trends in Dental Implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 50–60. [Google Scholar] [CrossRef]
- Snauwaert, K.; Duyck, J.; van Steenberghe, D.; Quirynen, M.; Naert, I. Time Dependent Failure Rate and Marginal Bone Loss of Implant Supported Prostheses: A 15-Year Follow-up Study. Clin. Oral Investig. 2000, 4, 13–20. [Google Scholar] [CrossRef]
- Bauer, S.; Schmuki, P.; Von Der Mark, K.; Park, J. Engineering Biocompatible Implant Surfaces: Part I: Materials and Surfaces. Prog. Mater. Sci. 2013, 58, 261–326. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J.; on behalf of Group D of the European Workshop on Periodontology. Peri-Implant Diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A New Classification Scheme for Periodontal and Peri-Implant Diseases and Conditions–Introduction and Key Changes from the 1999 Classification; Wiley Online Library: Hoboken, NJ, USA, 2018; ISBN 0022-3492. [Google Scholar]
- Mombelli, A.; Müller, N.; Cionca, N. The Epidemiology of Peri-implantitis. Clin. Oral Implant. Res. 2012, 23, 67–76. [Google Scholar] [CrossRef]
- Sumner, D.R.; Galante, J.O. Determinants of Stress Shielding: Design versus Materials versus Interface. Clin. Orthop. 1992, 274, 202–212. [Google Scholar] [CrossRef]
- Huiskes, R.; Weinans, H.; Van Rietbergen, B. The Relationship between Stress Shielding and Bone Resorption around Total Hip Stems and the Effects of Flexible Materials. Clin. Orthop. 1992, 274, 124–134. [Google Scholar] [CrossRef] [Green Version]
- Brunette, D.M.; Tengvall, P.; Textor, M.; Thomsen, P. Titanium in Medicine Material Science, Surface Science, Engineering, Biological Responses and Medical Applications; Springer: Berlin/Heidelberg, Germany, 2001; ISBN 978-3-642-63119-1. [Google Scholar]
- Torres, Y.; Trueba, P.; Pavón, J.; Montealegre, I.; Rodríguez-Ortiz, J.A. Designing, Processing and Characterisation of Titanium Cylinders with Graded Porosity: An Alternative to Stress-Shielding Solutions. Mater. Des. 2014, 63, 316–324. [Google Scholar] [CrossRef]
- Rompen, E.; Domken, O.; Degidi, M.; Farias Pontes, A.E.; Piattelli, A. The Effect of Material Characteristics, of Surface Topography and of Implant Components and Connections on Soft Tissue Integration: A Literature Review. Clin. Oral Implant. Res. 2006, 17, 55–67. [Google Scholar] [CrossRef]
- Yamano, S.; Al-Sowygh, Z.H.; Gallucci, G.O.; Wada, K.; Weber, H.-P.; Sukotjo, C. Early Peri-implant Tissue Reactions on Different Titanium Surface Topographies. Clin. Oral Implant. Res. 2011, 22, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Neuss, S.; Schneider, R.K.M.; Tietze, L.; Knüchel, R.; Jahnen-Dechent, W. Secretion of Fibrinolytic Enzymes Facilitates Human Mesenchymal Stem Cell Invasion into Fibrin Clots. Cells Tissues Organs 2010, 191, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E. Mechanisms of Endosseous Integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef]
- Khan, A.; Goyal, A.; Currell, S.D.; Sharma, D. Management of Peri-Implantitis Lesions without the Use of Systemic Antibiotics: A Systematic Review. Dent. J. 2020, 8, 106. [Google Scholar] [CrossRef]
- Mouhyi, J.; Dohan Ehrenfest, D.M.; Albrektsson, T. The Peri-Implantitis: Implant Surfaces, Microstructure, and Physicochemical Aspects: The Peri-Implantitis. Clin. Implant Dent. Relat. Res. 2012, 14, 170–183. [Google Scholar] [CrossRef]
- Toledano, M.; Osorio, M.T.; Vallecillo-Rivas, M.; Toledano-Osorio, M.; Rodríguez-Archilla, A.; Toledano, R.; Osorio, R. Efficacy of Local Antibiotic Therapy in the Treatment of Peri-Implantitis: A Systematic Review and Meta-Analysis. J. Dent. 2021, 113, 103790. [Google Scholar] [CrossRef]
- Moore, W.E.; Moore, L.V. The Bacteria of Periodontal Diseases. Periodontol. 2000 1994, 5, 66–77. [Google Scholar] [CrossRef]
- Gristina, A.G. Biomaterial-Centered Infection: Microbial Adhesion versus Tissue Integration. Science 1987, 237, 1588–1595. [Google Scholar] [CrossRef] [PubMed]
- Kolenbrander, P.E.; Andersen, R.N.; Blehert, D.S.; Egland, P.G.; Foster, J.S.; Palmer, R.J. Communication among Oral Bacteria. Microbiol. Mol. Biol. Rev. MMBR 2002, 66, 486–505, table of contents. [Google Scholar] [CrossRef] [Green Version]
- Morse, D.J.; Wilson, M.J.; Wei, X.; Lewis, M.A.O.; Bradshaw, D.J.; Murdoch, C.; Williams, D.W. Denture-Associated Biofilm Infection in Three-Dimensional Oral Mucosal Tissue Models. J. Med. Microbiol. 2018, 67, 364–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Belt, H.; Neut, D.; Schenk, W.; vanHorn, J.R.; van der Mei, H.C.; Busscher, H.J. Infection of Orthopedic Implants and the Use of Antibiotic-Loaded Bone Cements: A Review. Acta Orthop. Scand. 2001, 72, 557–571. [Google Scholar] [CrossRef]
- Hetrick, E.M.; Schoenfisch, M.H. Reducing Implant-Related Infections: Active Release Strategies. Chem. Soc. Rev. 2006, 35, 780–789. [Google Scholar] [CrossRef]
- Minkiewicz-Zochniak, A.; Jarzynka, S.; Iwańska, A.; Strom, K.; Iwańczyk, B.; Bartel, M.; Mazur, M.; Pietruczuk-Padzik, A.; Konieczna, M.; Augustynowicz-Kopeć, E.; et al. Biofilm Formation on Dental Implant Biomaterials by Staphylococcus Aureus Strains Isolated from Patients with Cystic Fibrosis. Materials 2021, 14, 2030. [Google Scholar] [CrossRef]
- Kassem, A.; Lindholm, C.; Lerner, U.H. Toll-Like Receptor 2 Stimulation of Osteoblasts Mediates Staphylococcus Aureus Induced Bone Resorption and Osteoclastogenesis through Enhanced RANKL. PLoS ONE 2016, 11, e0156708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, C.J.; Ward, C.L.; Romano, D.R.; Hurtgen, B.J.; Hardy, S.K.; Woodbury, R.L.; Trevino, A.V.; Rathbone, C.R.; Wenke, J.C. Staphylococcus Aureus Biofilms Decrease Osteoblast Viability, Inhibits Osteogenic Differentiation, and Increases Bone Resorption in Vitro. BMC Musculoskelet. Disord. 2013, 14, 187. [Google Scholar] [CrossRef] [Green Version]
- Trouillet-Assant, S.; Gallet, M.; Nauroy, P.; Rasigade, J.-P.; Flammier, S.; Parroche, P.; Marvel, J.; Ferry, T.; Vandenesch, F.; Jurdic, P.; et al. Dual Impact of Live Staphylococcus Aureus on the Osteoclast Lineage, Leading to Increased Bone Resorption. J. Infect. Dis. 2015, 211, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Abraham, C.M. A Brief Historical Perspective on Dental Implants, Their Surface Coatings and Treatments. Open Dent. J. 2014, 8, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Ring, M.E. Dentistry: An Illustrated History; Abrams: New York, NY, USA, 1985; ISBN 978-0-8109-1100-0. [Google Scholar]
- Lee, J.-H.; Frias, V.; Lee, K.-W.; Wright, R.F. Effect of Implant Size and Shape on Implant Success Rates: A Literature Review. J. Prosthet. Dent. 2005, 94, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I. Osseointegration and Its Experimental Background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Linkow, L.I.; Dorfman, J.D. Implantology in Dentistry. A Brief Historical Perspective. N. Y. State Dent. J. 1991, 57, 31–35. [Google Scholar]
- Goldberg, N.I.; Gershkoff, A. The Implant Lower Denture. Dent. Dig. 1949, 55, 490–494. [Google Scholar]
- Brånemark, P.-I. (Ed.) Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Books; 1. Reprinting; Quintessence: Chicago, IL, USA, 1986; ISBN 978-0-86715-129-9. [Google Scholar]
- Donati, M.; Ekestubbe, A.; Lindhe, J.; Wennström, J.L. Marginal Bone Loss at Implants with Different Surface Characteristics—A 20-Year Follow-up of a Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2018, 29, 480–487. [Google Scholar] [CrossRef]
- Shao, L.; Du, Y.; Dai, K.; Wu, H.; Wang, Q.; Liu, J.; Tang, Y.; Wang, L. β-Ti Alloys for Orthopedic and Dental Applications: A Review of Progress on Improvement of Properties through Surface Modification. Coatings 2021, 11, 1446. [Google Scholar] [CrossRef]
- Rahimi, S.; Tengku Mohd Ariff, T.; Affendi, N.; Ahmad, R. Surface Modifications of Dental Implant and Its Clinical Performance: A Review. Compend. Oral Sci. 2022, 9, 52. [Google Scholar] [CrossRef]
- Zhu, G.; Wang, G.; Li, J.J. Advances in Implant Surface Modifications to Improve Osseointegration. Mater. Adv. 2021, 2, 6901–6927. [Google Scholar] [CrossRef]
- Stich, T.; Alagboso, F.; Křenek, T.; Kovářík, T.; Alt, V.; Docheva, D. Implant-bone-interface: Reviewing the Impact of Titanium Surface Modifications on Osteogenic Processes in Vitro and in Vivo. Bioeng. Transl. Med. 2022, 7, e10239. [Google Scholar] [CrossRef]
- Kandavalli, S.R.; Wang, Q.; Ebrahimi, M.; Gode, C.; Djavanroodi, F.; Attarilar, S.; Liu, S. A Brief Review on the Evolution of Metallic Dental Implants: History, Design, and Application. Front. Mater. 2021, 8, 646383. [Google Scholar] [CrossRef]
- Kurup, A.; Dhatrak, P.; Khasnis, N. Surface Modification Techniques of Titanium and Titanium Alloys for Biomedical Dental Applications: A Review. Mater. Today Proc. 2021, 39, 84–90. [Google Scholar] [CrossRef]
- Nimbalkar, S.; Dhatrak, P.; Gherde, C.; Joshi, S. A Review Article on Factors Affecting Bone Loss in Dental Implants. Mater. Today Proc. 2021, 43, 970–976. [Google Scholar] [CrossRef]
- Ravald, N.; Dahlgren, S.; Teiwik, A.; Gröndahl, K. Long-Term Evaluation of Astra Tech and Brånemark Implants in Patients Treated with Full-Arch Bridges. Results after 12-15 Years. Clin. Oral Implant. Res. 2013, 24, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Barfeie, A.; Wilson, J.; Rees, J. Implant Surface Characteristics and Their Effect on Osseointegration. Br. Dent. J. 2015, 218, E9. [Google Scholar] [CrossRef]
- Shah, F.A.; Thomsen, P.; Palmquist, A. Osseointegration and Current Interpretations of the Bone-Implant Interface. Acta Biomater. 2019, 84, 1–15. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Sanjay, M.R.; Srisuk, R.; Parameswaranpillai, J.; Siengchin, S. A Comprehensive Review on Chemical Properties and Applications of Biopolymers and Their Composites. Int. J. Biol. Macromol. 2020, 154, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Triplett, R.G.; Frohberg, U.; Sykaras, N.; Woody, R.D. Implant Materials, Design, and Surface Topographies: Their Influence on Osseointegration of Dental Implants. J. Long. Term Eff. Med. Implant. 2003, 13, 18. [Google Scholar] [CrossRef]
- Hench, L.L. The Story of Bioglass®. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef]
- Trueba, P.; Navarro, C.; Rodríguez-Ortiz, J.A.; Beltrán, A.M.; García-García, F.J.; Torres, Y. Fabrication and Characterization of Superficially Modified Porous Dental Implants. Surf. Coat. Technol. 2021, 408, 126796. [Google Scholar] [CrossRef]
- Lascano, S.; Chávez-Vásconez, R.; Muñoz-Rojas, D.; Aristizabal, J.; Arce, B.; Parra, C.; Acevedo, C.; Orellana, N.; Reyes-Valenzuela, M.; Gotor, F.J.; et al. Graphene-Coated Ti-Nb-Ta-Mn Foams: A Promising Approach towards a Suitable Biomaterial for Bone Replacement. Surf. Coat. Technol. 2020, 401, 126250. [Google Scholar] [CrossRef]
- Toledano-Serrabona, J.; Sánchez-Garcés, M.Á.; Gay-Escoda, C.; Valmaseda-Castellón, E.; Camps-Font, O.; Verdeguer, P.; Molmeneu, M.; Gil, F.J. Mechanical Properties and Corrosion Behavior of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part II. Materials 2021, 14, 6519. [Google Scholar] [CrossRef] [PubMed]
- Bammidi, R.; Prasad, K.S. Ti-6AL-4V as Dental Implant. EAS J. Dent. Oral. Med. 2020, 2, 14–18. [Google Scholar]
- Toledano-Serrabona, J.; Gil, F.J.; Camps-Font, O.; Valmaseda-Castellón, E.; Gay-Escoda, C.; Sánchez-Garcés, M.Á. Physicochemical and Biological Characterization of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part I. Materials 2021, 14, 6507. [Google Scholar] [CrossRef] [PubMed]
- W Nicholson, J. Titanium Alloys for Dental Implants: A Review. Prosthesis 2020, 2, 100–116. [Google Scholar] [CrossRef]
- Cordeiro, J.M.; Barão, V.A.R. Is There Scientific Evidence Favoring the Substitution of Commercially Pure Titanium with Titanium Alloys for the Manufacture of Dental Implants? Mater. Sci. Eng. C 2017, 71, 1201–1215. [Google Scholar] [CrossRef]
- Oshida, Y.; Tominaga, T. Chapter 11. Properties in Biological Environment. In Nickel-Titanium Materials; De Gruyter: Berlin, Germany, 2020; pp. 480–572. ISBN 978-3-11-066611-3. [Google Scholar]
- Kassapidou, M.; Hjalmarsson, L.; Johansson, C.B.; Hammarström Johansson, P.; Morisbak, E.; Wennerberg, A.; Franke Stenport, V. Cobalt–Chromium Alloys Fabricated with Four Different Techniques: Ion Release, Toxicity of Released Elements and Surface Roughness. Dent. Mater. 2020, 36, e352–e363. [Google Scholar] [CrossRef]
- Fathi, M.H.; Salehi, M.; Saatchi, A.; Mortazavi, V.; Moosavi, S.B. In Vitro Corrosion Behavior of Bioceramic, Metallic, and Bioceramic–Metallic Coated Stainless Steel Dental Implants. Dent. Mater. 2003, 19, 188–198. [Google Scholar] [CrossRef]
- Saini, M. Implant Biomaterials: A Comprehensive Review. World J. Clin. Cases 2015, 3, 52. [Google Scholar] [CrossRef]
- Zhang, Y.; Gulati, K.; Li, Z.; Di, P.; Liu, Y. Dental Implant Nano-Engineering: Advances, Limitations and Future Directions. Nanomaterials 2021, 11, 2489. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Pedrosa, A.R.; Martins, M.D. Chemical and Topographic Analysis of Treated Surfaces of Five Different Commercial Dental Titanium Implants. Mater. Res. 2012, 15, 372–382. [Google Scholar] [CrossRef] [Green Version]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface Characteristics of Dental Implants: A Review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Gröbe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. BioMed Res. Int. 2016, 2016, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yurttutan, M.E.; Keskin, A. Evaluation of the Effects of Different Sand Particles That Used in Dental Implant Roughened for Osseointegration. BMC Oral Health 2018, 18, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonshor, A.; Goveia, G.; Sotirakis, E. A Prospective, Multicenter, 4-Year Study of the ACE Surgical Resorbable Blast Media Implant. J. Oral Implantol. 2003, 29, 174–180. [Google Scholar] [CrossRef]
- Gil, J.; Pérez, R.; Herrero-Climent, M.; Rizo-Gorrita, M.; Torres-Lagares, D.; Gutierrez, J.L. Benefits of Residual Aluminum Oxide for Sand Blasting Titanium Dental Implants: Osseointegration and Bactericidal Effects. Materials 2021, 15, 178. [Google Scholar] [CrossRef]
- Von Wilmowsky, C.; Moest, T.; Nkenke, E.; Stelzle, F.; Schlegel, K.A. Implants in Bone: Part I. A Current Overview about Tissue Response, Surface Modifications and Future Perspectives. Oral Maxillofac. Surg. 2014, 18, 243–257. [Google Scholar] [CrossRef]
- Chen, C.-J.; Ding, S.-J.; Chen, C.-C. Effects of Surface Conditions of Titanium Dental Implants on Bacterial Adhesion. Photomed. Laser Surg. 2016, 34, 379–388. [Google Scholar] [CrossRef]
- Sullivan, D.Y.; Sherwood, R.L.; Porter, S.S. Long-Term Performance of Osseotite Implants: A 6-Year Clinical Follow-Up. Compend. Contin. Educ. Dent. Jamesburg NJ 1995 2001, 22, 326–328, 330, 332–334. [Google Scholar]
- Testori, T.; Wiseman, L.; Woolfe, S.; Porter, S.S. A Prospective Multicenter Clinical Study of the Osseotite Implant: Four-Year Interim Report. Int. J. Oral Maxillofac. Implant. 2001, 16, 193–200. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for Replacing Missing Teeth: Different Times for Loading Dental Implants. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- Mandracci, P.; Mussano, F.; Rivolo, P.; Carossa, S. Surface Treatments and Functional Coatings for Biocompatibility Improvement and Bacterial Adhesion Reduction in Dental Implantology. Coatings 2016, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Anil, S.; Anand, P.S.; Alghamdi, H.; Janse, J.A. Dental Implant Surface Enhancement and Osseointegration. In Implant Dentistry—A Rapidly Evolving Practice; Turkyilmaz, I., Ed.; InTech: London, UK, 2011; ISBN 978-953-307-658-4. [Google Scholar]
- Gaviria, J.; Alcudia, A.; Begines, B.; Beltrán, A.M.; Villarraga, J.; Moriche, R.; Rodríguez-Ortiz, J.A.; Torres, Y. Synthesis and Deposition of Silver Nanoparticles on Porous Titanium Substrates for Biomedical Applications. Surf. Coat. Technol. 2021, 406, 126667. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Jimenez-Guerra, A.; Monsalve-Guil, L.; Ortiz-Garcia, I.; Nicolas-Silvente, A.I.; Segura-Egea, J.J.; Lopez-Lopez, J. Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface. Materials 2020, 13, 1553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasco-Ortega, E.; Alfonso-Rodríguez, C.A.; Monsalve-Guil, L.; España-López, A.; Jiménez-Guerra, A.; Garzón, I.; Alaminos, M.; Gil, F.J. Relevant Aspects in the Surface Properties in Titanium Dental Implants for the Cellular Viability. Mater. Sci. Eng. C 2016, 64, 1–10. [Google Scholar] [CrossRef]
- Ban, S.; Iwaya, Y.; Kono, H.; Sato, H. Surface Modification of Titanium by Etching in Concentrated Sulfuric Acid. Dent. Mater. 2006, 22, 1115–1120. [Google Scholar] [CrossRef]
- Blatt, S.; Pabst, A.M.; Schiegnitz, E.; Hosang, M.; Ziebart, T.; Walter, C.; Al-Nawas, B.; Klein, M.O. Early Cell Response of Osteogenic Cells on Differently Modified Implant Surfaces: Sequences of Cell Proliferation, Adherence and Differentiation. J. Cranio-Maxillofac. Surg. 2018, 46, 453–460. [Google Scholar] [CrossRef]
- Chauhan, P.; Koul, V.; Bhatnagar, N. Critical Role of Etching Parameters in the Evolution of Nano Micro SLA Surface on the Ti6Al4V Alloy Dental Implants. Materials 2021, 14, 6344. [Google Scholar] [CrossRef]
- Bourikas, K.; Kordulis, C.; Lycourghiotis, A. Titanium Dioxide (Anatase and Rutile): Surface Chemistry, Liquid–Solid Interface Chemistry, and Scientific Synthesis of Supported Catalysts. Chem. Rev. 2014, 114, 9754–9823. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. 10-Year Follow-Up of Immediately Loaded Implants with TiUnite Porous Anodized Surface: 10-Year Follow-Up of TiUnite Surface. Clin. Implant Dent. Relat. Res. 2012, 14, 828–838. [Google Scholar] [CrossRef]
- Traini, T.; Murmura, G.; Sinjari, B.; Perfetti, G.; Scarano, A.; D’Arcangelo, C.; Caputi, S. The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration. Coatings 2018, 8, 252. [Google Scholar] [CrossRef] [Green Version]
- Gong, Z.; Hu, Y.; Gao, F.; Quan, L.; Liu, T.; Gong, T.; Pan, C. Effects of Diameters and Crystals of Titanium Dioxide Nanotube Arrays on Blood Compatibility and Endothelial Cell Behaviors. Colloids Surf. B Biointerfaces 2019, 184, 110521. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Liu, T.; Zhang, Z.; Zhang, X.; Qiao, X.; Hu, Y.; Zhang, Q.; Yang, Z. Preparation of Chitosan-Zn2+ Complex Coating on Polydopamine-Modified TiO2 Nanotubes to Enhance Osteoblast Behaviors. Mater. Lett. 2021, 282, 128665. [Google Scholar] [CrossRef]
- Pan, C.; Liu, T.; Yang, Y.; Liu, T.; Gong, Z.; Wei, Y.; Quan, L.; Yang, Z.; Liu, S. Incorporation of Sr2+ and Ag Nanoparticles into TiO2 Nanotubes to Synergistically Enhance Osteogenic and Antibacterial Activities for Bone Repair. Mater. Des. 2020, 196, 109086. [Google Scholar] [CrossRef]
- Alipal, J.; Lee, T.C.; Koshy, P.; Abdullah, H.Z.; Idris, M.I. Evolution of Anodised Titanium for Implant Applications. Heliyon 2021, 7, e07408. [Google Scholar] [CrossRef]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface Treatments of Titanium Dental Implants for Rapid Osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef]
- Cochran, D.L. The Scientific Basis for and Clinical Experiences with Straumann Implants Including the ITI ® Dental Implant System: A Consensus Report. Clin. Oral Implant. Res. 2000, 11, 33–58. [Google Scholar] [CrossRef]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface Modifications and Their Effects on Titanium Dental Implants. BioMed Res. Int. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Simmons, C.A.; Valiquette, N.; Pilliar, R.M. Osseointegration of Sintered Porous-surfaced and Plasma Spray–Coated Implants: An Animal Model Study of Early Postimplantation Healing Response and Mechanical Stability. J. Biomed. Mater. Res. 1999, 47, 127–138. [Google Scholar] [CrossRef]
- Knabe, C.; Klar, F.; Fitzner, R.; Radlanski, R.J.; Gross, U. In Vitro Investigation of Titanium and Hydroxyapatite Dental Implant Surfaces Using a Rat Bone Marrow Stromal Cell Culture System. Biomaterials 2002, 23, 3235–3245. [Google Scholar] [CrossRef]
- Liu, X.; Poon, R.W.Y.; Kwok, S.C.H.; Chu, P.K.; Ding, C. Plasma Surface Modification of Titanium for Hard Tissue Replacements. Surf. Coat. Technol. 2004, 186, 227–233. [Google Scholar] [CrossRef]
- Abir, M.M.M.; Otsuka, Y.; Ohnuma, K.; Miyashita, Y. Effects of Composition of Hydroxyapatite/Gray Titania Coating Fabricated by Suspension Plasma Spraying on Mechanical and Antibacterial Properties. J. Mech. Behav. Biomed. Mater. 2022, 125, 104888. [Google Scholar] [CrossRef]
- Kurella, A.; Dahotre, N.B. Review Paper: Surface Modification for Bioimplants: The Role of Laser Surface Engineering. J. Biomater. Appl. 2005, 20, 5–50. [Google Scholar] [CrossRef] [PubMed]
- Pecora, G.E.; Ceccarelli, R.; Bonelli, M.; Alexander, H.; Ricci, J.L. Clinical Evaluation of Laser Microtexturing for Soft Tissue and Bone Attachment to Dental Implants. Implant Dent. 2009, 18, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevins, M.; Kim, D.M.; Jun, S.-H.; Guze, K.; Schupbach, P.; Nevins, M.L. Histologic Evidence of a Connective Tissue Attachment to Laser Microgrooved Abutments: A Canine Study. Int. J. Periodontics Restor. Dent. 2010, 30, 245–255. [Google Scholar]
- Al-Zubaidi, S.M.; Madfa, A.A.; Mufadhal, A.A.; Aldawla, M.A.; Hameed, O.S.; Yue, X.-G. Improvements in Clinical Durability From Functional Biomimetic Metallic Dental Implants. Front. Mater. 2020, 7, 106. [Google Scholar] [CrossRef]
- Farronato, D.; Mangano, F.; Briguglio, F.; Iorio-Siciliano, V.; Riccitiello, F.; Guarnieri, R. Influence of Laser-Lok Surface on Immediate Functional Loading of Implants in Single-Tooth Replacement: A 2-Year Prospective Clinical Study. Int. J. Periodontics Restor. Dent. 2014, 34, 79–89. [Google Scholar] [CrossRef]
- Rodríguez, Á.; Trueba, P.; Amado, J.M.; Tobar, M.J.; Giner, M.; Amigó, V.; Torres, Y. Surface Modification of Porous Titanium Discs Using Femtosecond Laser Structuring. Metals 2020, 10, 748. [Google Scholar] [CrossRef]
- Phillips, K.C.; Gandhi, H.H.; Mazur, E.; Sundaram, S.K. Ultrafast Laser Processing of Materials: A Review. Adv. Opt. Photonics 2015, 7, 684. [Google Scholar] [CrossRef]
- Mesa-Restrepo, A.; Civantos, A.; Allain, J.; Patiño, E.; Alzate, J.; Balcázar, N.; Montes, R.; Pavón, J.; Rodríguez-Ortiz, J.; Torres, Y. Synergistic Effect of RhBMP-2 Protein and Nanotextured Titanium Alloy Surface to Improve Osteogenic Implant Properties. Metals 2021, 11, 464. [Google Scholar] [CrossRef]
- Civantos, A.; Allain, J.P.; Pavón, J.J.; Shetty, A.; El-Atwani, O.; Walker, E.; Arias, S.L.; Gordon, E.; Rodríguez-Ortiz, J.A.; Chen, M.; et al. Directed Irradiation Synthesis as an Advanced Plasma Technology for Surface Modification to Activate Porous and “as-Received” Titanium Surfaces. Metals 2019, 9, 1349. [Google Scholar] [CrossRef] [Green Version]
- Boutinguiza, M.; Fernández-Arias, M.; del Val, J.; Buxadera-Palomero, J.; Rodríguez, D.; Lusquiños, F.; Gil, F.J.; Pou, J. Synthesis and Deposition of Silver Nanoparticles on Cp Ti by Laser Ablation in Open Air for Antibacterial Effect in Dental Implants. Mater. Lett. 2018, 231, 126–129. [Google Scholar] [CrossRef]
- Dong, H.; Liu, H.; Zhou, N.; Li, Q.; Yang, G.; Chen, L.; Mou, Y. Surface Modified Techniques and Emerging Functional Coating of Dental Implants. Coatings 2020, 10, 1012. [Google Scholar] [CrossRef]
- Zafar, M.S.; Fareed, M.A.; Riaz, S.; Latif, M.; Habib, S.R.; Khurshid, Z. Customized Therapeutic Surface Coatings for Dental Implants. Coatings 2020, 10, 568. [Google Scholar] [CrossRef]
- Choi, A.H.; Ben-Nissan, B.; Matinlinna, J.P.; Conway, R.C. Current Perspectives: Calcium Phosphate Nanocoatings and Nanocomposite Coatings in Dentistry. J. Dent. Res. 2013, 92, 853–859. [Google Scholar] [CrossRef]
- Bonsor, S.J. Are Dentine Pins Obsolete? Dent. Update 2013, 40, 253–258. [Google Scholar] [CrossRef]
- Sörensen, J.H.; Lilja, M.; Sörensen, T.C.; Åstrand, M.; Procter, P.; Fuchs, S.; Strømme, M.; Steckel, H. Biomechanical and Antibacterial Properties of Tobramycin Loaded Hydroxyapatite Coated Fixation Pins: Functional Ha Coatings as Local Drug Delivery Vehicles. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- García-Cabezón, C.; Godinho, V.; Salvo-Comino, C.; Torres, Y.; Martín-Pedrosa, F. Improved Corrosion Behavior and Biocompatibility of Porous Titanium Samples Coated with Bioactive Chitosan-Based Nanocomposites. Materials 2021, 14, 6322. [Google Scholar] [CrossRef] [PubMed]
- Kay, J.F. Calcium Phosphate Coatings for Dental Implants. Current Status and Future Potential. Dent. Clin. N. Am. 1992, 36, 1–18. [Google Scholar]
- Habibovic, P.; Li, J.; van der Valk, C.M.; Meijer, G.; Layrolle, P.; van Blitterswijk, C.A.; de Groot, K. Biological Performance of Uncoated and Octacalcium Phosphate-Coated Ti6Al4V. Biomaterials 2005, 26, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Barrère, F.; van der Valk, C.M.; Meijer, G.; Dalmeijer, R.A.J.; de Groot, K.; Layrolle, P. Osteointegration of Biomimetic Apatite Coating Applied onto Dense and Porous Metal Implants in Femurs of Goats: Osteointegration of Biomimetic Apatite Coating. J. Biomed. Mater. Res. B Appl. Biomater. 2003, 67B, 655–665. [Google Scholar] [CrossRef]
- Coelho, P.G.; Takayama, T.; Yoo, D.; Jimbo, R.; Karunagaran, S.; Tovar, N.; Janal, M.N.; Yamano, S. Nanometer-Scale Features on Micrometer-Scale Surface Texturing: A Bone Histological, Gene Expression, and Nanomechanical Study. Bone 2014, 65, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Bucci-Sabattini, V.; Cassinelli, C.; Coelho, P.G.; Minnici, A.; Trani, A.; Ehrenfest, D.M.D. Effect of Titanium Implant Surface Nanoroughness and Calcium Phosphate Low Impregnation on Bone Cell Activity in Vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Mendes, V.C.; Moineddin, R.; Davies, J.E. The Effect of Discrete Calcium Phosphate Nanocrystals on Bone-Bonding to Titanium Surfaces. Biomaterials 2007, 28, 4748–4755. [Google Scholar] [CrossRef] [PubMed]
- Goené, R.J.; Testori, T.; Trisi, P. Influence of a Nanometer-Scale Surface Enhancement on de Novo Bone Formation on Titanium Implants: A Histomorphometric Study in Human Maxillae. Int. J. Periodontics Restor. Dent. 2007, 27, 211–219. [Google Scholar]
- Mendes, V.C.; Moineddin, R.; Davies, J.E. Discrete Calcium Phosphate Nanocrystalline Deposition Enhances Osteoconduction on Titanium-Based Implant Surfaces. J. Biomed. Mater. Res. A 2009, 90A, 577–585. [Google Scholar] [CrossRef]
- Telleman, G.; Meijer, H.J.A.; Vissink, A.; Raghoebar, G.M. Short Implants with a Nanometer-Sized CaP Surface Provided with Either a Platform-Switched or Platform-Matched Abutment Connection in the Posterior Region: A Randomized Clinical Trial. Clin. Oral Implant. Res. 2013, 24, 1316–1324. [Google Scholar] [CrossRef] [Green Version]
- Bonfante, E.A.; Granato, R.; Marin, C.; Jimbo, R.; Giro, G.; Suzuki, M.; Coelho, P.G. Biomechanical Testing of Microblasted, Acid-Etched/Microblasted, Anodized, and Discrete Crystalline Deposition Surfaces: An Experimental Study in Beagle Dogs. Int. J. Oral Maxillofac. Implant 2013, 28, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Ewald, A.; Kreczy, D.; Brückner, T.; Gbureck, U.; Bengel, M.; Hoess, A.; Nies, B.; Bator, J.; Klammert, U.; Fuchs, A. Development and Bone Regeneration Capacity of Premixed Magnesium Phosphate Cement Pastes. Materials 2019, 12, 2119. [Google Scholar] [CrossRef] [Green Version]
- Nabiyouni, M.; Ren, Y.; Bhaduri, S.B. Magnesium Substitution in the Structure of Orthopedic Nanoparticles: A Comparison between Amorphous Magnesium Phosphates, Calcium Magnesium Phosphates, and Hydroxyapatites. Mater. Sci. Eng. C 2015, 52, 11–17. [Google Scholar] [CrossRef]
- Pardun, K.; Treccani, L.; Volkmann, E.; Streckbein, P.; Heiss, C.; Gerlach, J.W.; Maendl, S.; Rezwan, K. Magnesium-Containing Mixed Coatings on Zirconia for Dental Implants: Mechanical Characterization and in Vitro Behavior. J. Biomater. Appl. 2015, 30, 104–118. [Google Scholar] [CrossRef] [Green Version]
- Sikder, P.; Bhaduri, S.B. Microwave Assisted Synthesis and Characterization of Single-phase Tabular Hexagonal Newberyite, an Important Bioceramic. J. Am. Ceram. Soc. 2018, 101, 2537–2544. [Google Scholar] [CrossRef]
- Lee, S.; Chang, Y.-Y.; Lee, J.; Madhurakkat Perikamana, S.K.; Kim, E.M.; Jung, Y.-H.; Yun, J.-H.; Shin, H. Surface Engineering of Titanium Alloy Using Metal-Polyphenol Network Coating with Magnesium Ions for Improved Osseointegration. Biomater. Sci. 2020, 8, 3404–3417. [Google Scholar] [CrossRef]
- Mróz, W.; Budner, B.; Syroka, R.; Niedzielski, K.; Golański, G.; Slósarczyk, A.; Schwarze, D.; Douglas, T.E.L. In Vivo Implantation of Porous Titanium Alloy Implants Coated with Magnesium-Doped Octacalcium Phosphate and Hydroxyapatite Thin Films Using Pulsed Laser Depostion: Pulsed Laser Deposition of Mg-Enriched Ceramic Layers on Porous Ti6Al4V. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 103, 151–158. [Google Scholar] [CrossRef]
- Arciola, C.R.; Campoccia, D.; Speziale, P.; Montanaro, L.; Costerton, J.W. Biofilm Formation in Staphylococcus Implant Infections. A Review of Molecular Mechanisms and Implications for Biofilm-Resistant Materials. Biomaterials 2012, 33, 5967–5982. [Google Scholar] [CrossRef]
- Novoselov, K.S.; Geim, A.K.; Morozov, S.V.; Jiang, D.; Zhang, Y.; Dubonos, S.V.; Grigorieva, I.V.; Firsov, A.A. Electric Field Effect in Atomically Thin Carbon Films. Science 2004, 306, 666–669. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, R.; Han, Y.M.; Morin, J.L.P.; Luong-Van, E.K.; Chew, R.J.J.; Castro Neto, A.H.; Nijhuis, C.A.; Rosa, V. Inhibiting Corrosion of Biomedical-Grade Ti-6Al-4V Alloys with Graphene Nanocoating. J. Dent. Res. 2020, 99, 285–292. [Google Scholar] [CrossRef]
- Shin, S.R.; Li, Y.-C.; Jang, H.L.; Khoshakhlagh, P.; Akbari, M.; Nasajpour, A.; Zhang, Y.S.; Tamayol, A.; Khademhosseini, A. Graphene-Based Materials for Tissue Engineering. Adv. Drug Deliv. Rev. 2016, 105, 255–274. [Google Scholar] [CrossRef] [Green Version]
- Guang, M.; Huang, B.; Yao, Y.; Zhang, L.; Yang, B.; Gong, P. Effects of Vascular Endothelial Growth Factor on Osteoblasts around Dental Implants In Vitro and In Vivo. J. Oral Sci. 2017, 59, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Y.; Pei, X.; Yang, S.; Qin, H.; Cai, H.; Hu, S.; Sui, L.; Wan, Q.; Wang, J. Graphene Oxide/Hydroxyapatite Composite Coatings Fabricated by Electrochemical Deposition. Surf. Coat. Technol. 2016, 286, 72–79. [Google Scholar] [CrossRef]
- Chen, J.; Peng, H.; Wang, X.; Shao, F.; Yuan, Z.; Han, H. Graphene Oxide Exhibits Broad-Spectrum Antimicrobial Activity against Bacterial Phytopathogens and Fungal Conidia by Intertwining and Membrane Perturbation. Nanoscale 2014, 6, 1879–1889. [Google Scholar] [CrossRef]
- Dubey, N.; Ellepola, K.; Decroix, F.E.D.; Morin, J.L.P.; Castro Neto, A.; Seneviratne, C.J.; Rosa, V. Graphene onto Medical Grade Titanium: An Atom-Thick Multimodal Coating That Promotes Osteoblast Maturation and Inhibits Biofilm Formation from Distinct Species. Nanotoxicology 2018, 12, 274–289. [Google Scholar] [CrossRef]
- Qiu, J.; Geng, H.; Wang, D.; Qian, S.; Zhu, H.; Qiao, Y.; Qian, W.; Liu, X. Layer-Number Dependent Antibacterial and Osteogenic Behaviors of Graphene Oxide Electrophoretic Deposited on Titanium. ACS Appl. Mater. Interfaces 2017, 9, 12253–12263. [Google Scholar] [CrossRef]
- Qian, W.; Qiu, J.; Su, J.; Liu, X. Minocycline Hydrochloride Loaded on Titanium by Graphene Oxide: An Excellent Antibacterial Platform with the Synergistic Effect of Contact-Killing and Release-Killing. Biomater. Sci. 2018, 6, 304–313. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.; Choi, K.S.; Ji, M.-K.; Kim, S.; Gwon, Y.; Park, C.; Kim, J.; Lim, H.-P. Graphene–Chitosan Hybrid Dental Implants with Enhanced Antibacterial and Cell-Proliferation Properties. Appl. Sci. 2020, 10, 4888. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, F.; Jiang, Z.; Lan, J.; Zhao, L.; Si, P. Effect of Graphene Oxide on the Mechanical, Tribological, and Biological Properties of Sintered 3Y–ZrO2/GO Composite Ceramics for Dental Implants. Ceram. Int. 2021, 47, 6940–6946. [Google Scholar] [CrossRef]
- Terada, M.; Abe, S.; Akasaka, T.; Uo, M.; Kitagawa, Y.; Watari, F. Multiwalled Carbon Nanotube Coating on Titanium. Biomed. Mater. Eng. 2009, 19, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Hirata, E.; Uo, M.; Takita, H.; Akasaka, T.; Watari, F.; Yokoyama, A. Multiwalled Carbon Nanotube-Coating of 3D Collagen Scaffolds for Bone Tissue Engineering. Carbon 2011, 49, 3284–3291. [Google Scholar] [CrossRef]
- Borges, A.L.S.; Tribst, J.P.M.; Dal Piva, A.M.O.; Souza, A.C.O. In Vitro Evaluation of Multi-Walled Carbon Nanotube Reinforced Nanofibers Composites for Dental Application. Int. J. Polym. Mater. Polym. Biomater. 2020, 69, 1015–1022. [Google Scholar] [CrossRef]
- Hahn, B.-D.; Lee, J.-M.; Park, D.-S.; Choi, J.-J.; Ryu, J.; Yoon, W.-H.; Lee, B.-K.; Shin, D.-S.; Kim, H.-E. Mechanical and in Vitro Biological Performances of Hydroxyapatite–Carbon Nanotube Composite Coatings Deposited on Ti by Aerosol Deposition. Acta Biomater. 2009, 5, 3205–3214. [Google Scholar] [CrossRef]
- Kim, K.-I.; Kim, D.-A.; Patel, K.D.; Shin, U.S.; Kim, H.-W.; Lee, J.-H.; Lee, H.-H. Carbon Nanotube Incorporation in PMMA to Prevent Microbial Adhesion. Sci. Rep. 2019, 9, 4921. [Google Scholar] [CrossRef]
- Munir, K.S.; Wen, C.; Li, Y. Carbon Nanotubes and Graphene as Nanoreinforcements in Metallic Biomaterials: A Review. Adv. Biosyst. 2019, 3, 1800212. [Google Scholar] [CrossRef]
- Vaitkuviene, A.; McDonald, M.; Vahidpour, F.; Noben, J.-P.; Sanen, K.; Ameloot, M.; Ratautaite, V.; Kaseta, V.; Biziuleviciene, G.; Ramanaviciene, A.; et al. Impact of Differently Modified Nanocrystalline Diamond on the Growth of Neuroblastoma Cells. New Biotechnol. 2015, 32, 7–12. [Google Scholar] [CrossRef]
- Chouirfa, H.; Bouloussa, H.; Migonney, V.; Falentin-Daudré, C. Review of Titanium Surface Modification Techniques and Coatings for Antibacterial Applications. Acta Biomater. 2019, 83, 37–54. [Google Scholar] [CrossRef]
- Qin, H.; Cao, H.; Zhao, Y.; Jin, G.; Cheng, M.; Wang, J.; Jiang, Y.; An, Z.; Zhang, X.; Liu, X. Antimicrobial and Osteogenic Properties of Silver-Ion-Implanted Stainless Steel. ACS Appl. Mater. Interfaces 2015, 7, 10785–10794. [Google Scholar] [CrossRef]
- Wang, L.; Hu, C.; Shao, L. The Antimicrobial Activity of Nanoparticles: Present Situation and Prospects for the Future. Int. J. Nanomed. 2017, 12, 1227–1249. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Wang, H.; Huo, K.; Cui, L.; Zhang, W.; Ni, H.; Zhang, Y.; Wu, Z.; Chu, P.K. Antibacterial Nano-Structured Titania Coating Incorporated with Silver Nanoparticles. Biomaterials 2011, 32, 5706–5716. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, J.; Alcudia, A.; Begines, B.; Beltrán, A.M.; Rodríguez-Ortiz, J.A.; Trueba, P.; Villarraga, J.; Torres, Y. Biofunctionalization of Porous Ti Substrates Coated with Ag Nanoparticles for Potential Antibacterial Behavior. Metals 2021, 11, 692. [Google Scholar] [CrossRef]
- Flores, C.Y.; Diaz, C.; Rubert, A.; Benítez, G.A.; Moreno, M.S.; Fernández Lorenzo de Mele, M.A.; Salvarezza, R.C.; Schilardi, P.L.; Vericat, C. Spontaneous Adsorption of Silver Nanoparticles on Ti/TiO2 Surfaces. Antibacterial Effect on Pseudomonas Aeruginosa. J. Colloid Interface Sci. 2010, 350, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Beltrán, A.M.; Begines, B.; Alcudia, A.; Rodríguez-Ortiz, J.A.; Torres, Y. Biofunctional and Tribomechanical Behavior of Porous Titanium Substrates Coated with a Bioactive Glass Bilayer (45S5–1393). ACS Appl. Mater. Interfaces 2020, 12, 30170–30180. [Google Scholar] [CrossRef]
- Maximov, M.; Maximov, O.-C.; Craciun, L.; Ficai, D.; Ficai, A.; Andronescu, E. Bioactive Glass—An Extensive Study of the Preparation and Coating Methods. Coatings 2021, 11, 1386. [Google Scholar] [CrossRef]
- Rahaman, M.N.; Day, D.E.; Sonny Bal, B.; Fu, Q.; Jung, S.B.; Bonewald, L.F.; Tomsia, A.P. Bioactive Glass in Tissue Engineering. Acta Biomater. 2011, 7, 2355–2373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrán, A.M.; Alcudia, A.; Begines, B.; Rodríguez-Ortiz, J.A.; Torres, Y. Porous Titanium Substrates Coated with a Bilayer of Bioactive Glasses. J. Non-Cryst. Solids 2020, 544, 120206. [Google Scholar] [CrossRef]
- Torres, Y.; Begines, B.; Beltrán, A.M.; Boccaccini, A.R. Deposition of Bioactive Gelatin Coatings on Porous Titanium: Influence of Processing Parameters, Size and Pore Morphology. Surf. Coat. Technol. 2021, 421, 127366. [Google Scholar] [CrossRef]
- Park, S.-Y.; Kim, K.-H.; Kim, S.; Lee, Y.-M.; Seol, Y.-J. BMP-2 Gene Delivery-Based Bone Regeneration in Dentistry. Pharmaceutics 2019, 11, 393. [Google Scholar] [CrossRef] [Green Version]
- Al-Jarsha, M.; Moulisova, V.; Leal-Egana, A.; Connell, A.; Naudi, K.B.; Ayoub, A.; Dalby, M.J.; Salmerón-Sánchez, M. Engineered Coatings for Titanium Implants to Present Ultra-Low Doses of BMP-7. ACS Biomater. Sci. Eng. 2018, 5, 1812–1819. [Google Scholar] [CrossRef]
- Kim, J.-E.; Kang, S.-S.; Choi, K.-H.; Shim, J.-S.; Jeong, C.-M.; Shin, S.-W.; Huh, J.-B. The Effect of Anodized Implants Coated with Combined RhBMP-2 and Recombinant Human Vascular Endothelial Growth Factors on Vertical Bone Regeneration in the Marginal Portion of the Peri-Implant. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, e24–e31. [Google Scholar] [CrossRef]
- Kellesarian, S.V.; Malignaggi, V.R.; Kellesarian, T.V.; Bashir Ahmed, H.; Javed, F. Does Incorporating Collagen and Chondroitin Sulfate Matrix in Implant Surfaces Enhance Osseointegration? A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 241–251. [Google Scholar] [CrossRef]
- Yin, D.; Komasa, S.; Yoshimine, S.; Sekino, T.; Okazaki, J. Effect of Mussel Adhesive Protein Coating on Osteogenesis in Vitro and Osteointegration in Vivo to Alkali-Treated Titanium with Nanonetwork Structures. Int. J. Nanomed. 2019, 14, 3831–3843. [Google Scholar] [CrossRef] [Green Version]
- Raphel, J.; Karlsson, J.; Galli, S.; Wennerberg, A.; Lindsay, C.; Haugh, M.G.; Pajarinen, J.; Goodman, S.B.; Jimbo, R.; Andersson, M.; et al. Engineered Protein Coatings to Improve the Osseointegration of Dental and Orthopaedic Implants. Biomaterials 2016, 83, 269–282. [Google Scholar] [CrossRef] [Green Version]
- Sabino, R.M.; Mondini, G.; Kipper, M.J.; Martins, A.F.; Popat, K.C. Tanfloc/Heparin Polyelectrolyte Multilayers Improve Osteogenic Differentiation of Adipose-Derived Stem Cells on Titania Nanotube Surfaces. Carbohydr. Polym. 2021, 251, 117079. [Google Scholar] [CrossRef]
- Shahi, R.G.; Albuquerque, M.T.P.; Münchow, E.A.; Blanchard, S.B.; Gregory, R.L.; Bottino, M.C. Novel Bioactive Tetracycline-Containing Electrospun Polymer Fibers as a Potential Antibacterial Dental Implant Coating. Odontology 2017, 105, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Gonzalez, Z.; Utomo, E.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Poly(Caprolactone)-Based Coatings on 3D-Printed Biodegradable Implants: A Novel Strategy to Prolong Delivery of Hydrophilic Drugs. Mol. Pharm. 2020, 17, 3487–3500. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Ivanovski, S. Dental Implants Modified with Drug Releasing Titania Nanotubes: Therapeutic Potential and Developmental Challenges. Expert Opin. Drug Deliv. 2017, 14, 1009–1024. [Google Scholar] [CrossRef]
- Langer, R. New Methods of Drug Delivery. Science 1990, 249, 1527–1533. [Google Scholar] [CrossRef]
- Gultepe, E.; Nagesha, D.; Sridhar, S.; Amiji, M. Nanoporous Inorganic Membranes or Coatings for Sustained Drug Delivery in Implantable Devices. Adv. Drug Deliv. Rev. 2010, 62, 305–315. [Google Scholar] [CrossRef]
- Siepmann, J.; Peppas, N.A. Modeling of Drug Release from Delivery Systems Based on Hydroxypropyl Methylcellulose (HPMC). Adv. Drug Deliv. Rev. 2012, 64, 163–174. [Google Scholar] [CrossRef]
- Korsmeyer, R.W.; Gurny, R.; Doelker, E.; Buri, P.; Peppas, N.A. Mechanisms of Solute Release from Porous Hydrophilic Polymers. Int. J. Pharm. 1983, 15, 25–35. [Google Scholar] [CrossRef]
- Siepmann, J.; Siepmann, F. Modeling of Diffusion Controlled Drug Delivery. J. Control. Release 2012, 161, 351–362. [Google Scholar] [CrossRef]
- Ibekwe, V.C.; Fadda, H.M.; Parsons, G.E.; Basit, A.W. A Comparative in Vitro Assessment of the Drug Release Performance of PH-Responsive Polymers for Ileo-Colonic Delivery. Int. J. Pharm. 2006, 308, 52–60. [Google Scholar] [CrossRef]
- Pan, C.; Zhou, Z.; Yu, X. Coatings as the Useful Drug Delivery System for the Prevention of Implant-Related Infections. J. Orthop. Surg. 2018, 13, 220. [Google Scholar] [CrossRef] [Green Version]
- Stewart, S.; Domínguez-Robles, J.; Donnelly, R.; Larrañeta, E. Implantable Polymeric Drug Delivery Devices: Classification, Manufacture, Materials, and Clinical Applications. Polymers 2018, 10, 1379. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, C.L.; Santini, J.T.; Langer, R. Reservoir-Based Drug Delivery Systems Utilizing Microtechnology. Adv. Drug Deliv. Rev. 2012, 64, 1590–1602. [Google Scholar] [CrossRef] [Green Version]
- Wolinsky, J.B.; Colson, Y.L.; Grinstaff, M.W. Local Drug Delivery Strategies for Cancer Treatment: Gels, Nanoparticles, Polymeric Films, Rods, and Wafers. J. Control. Release 2012, 159, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Mauri, E.; Rossi, F.; Sacchetti, A. Tunable Drug Delivery Using Chemoselective Functionalization of Hydrogels. Mater. Sci. Eng. C 2016, 61, 851–857. [Google Scholar] [CrossRef]
- Exner, A.A.; Saidel, G.M. Drug-Eluting Polymer Implants in Cancer Therapy. Expert Opin. Drug Deliv. 2008, 5, 775–788. [Google Scholar] [CrossRef]
- Rossi, F.; Castiglione, F.; Ferro, M.; Moioli, M.; Mele, A.; Masi, M. The Role of Drug-Drug Interactions in Hydrogel Delivery Systems: Experimental and Model Study. ChemPhysChem 2016, 17, 1615–1622. [Google Scholar] [CrossRef]
- reza Saboktakin, M.; Tabatabaei, R.M. Supramolecular Hydrogels as Drug Delivery Systems. Int. J. Biol. Macromol. 2015, 75, 426–436. [Google Scholar] [CrossRef]
- Aw, M.S.; Gulati, K.; Losic, D. Controlling Drug Release from Titania Nanotube Arrays Using Polymer Nanocarriers and Biopolymer Coating. J. Biomater. Nanobiotechnol. 2011, 02, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Han, C.-M.; Jang, T.-S.; Kim, H.-E.; Koh, Y.-H. Creation of Nanoporous TiO2 Surface onto Polyetheretherketone for Effective Immobilization and Delivery of Bone Morphogenetic Protein: Creation of Nanoporous TiO2 Surface onto Peek. J. Biomed. Mater. Res. A 2014, 102, 793–800. [Google Scholar] [CrossRef]
- Liang, J.; Peng, X.; Zhou, X.; Zou, J.; Cheng, L. Emerging Applications of Drug Delivery Systems in Oral Infectious Diseases Prevention and Treatment. Molecules 2020, 25, 516. [Google Scholar] [CrossRef] [Green Version]
- Vallet-Regí, M.; Colilla, M.; Manzano, M. Recent Advances in Ceramic Implants as Drug Delivery Systems for Biomedical Applications. Int. J. Nanomed. 2008, 403. [Google Scholar] [CrossRef] [Green Version]
- Shirzaei Sani, E.; Portillo Lara, R.; Aldawood, Z.; Bassir, S.H.; Nguyen, D.; Kantarci, A.; Intini, G.; Annabi, N. An Antimicrobial Dental Light Curable Bioadhesive Hydrogel for Treatment of Peri-Implant Diseases. Matter 2019, 1, 926–944. [Google Scholar] [CrossRef] [Green Version]
- Water, J.J.; Bohr, A.; Boetker, J.; Aho, J.; Sandler, N.; Nielsen, H.M.; Rantanen, J. Three-Dimensional Printing of Drug-Eluting Implants: Preparation of an Antimicrobial Polylactide Feedstock Material. J. Pharm. Sci. 2015, 104, 1099–1107. [Google Scholar] [CrossRef]
- Centre of Microbial and Plant Genetics (CMPG) KU Leuven, Kasteelpark Arenberg 20 box 2460, 3001 Leuven, Belgium; De Cremer, K.; Braem, A.; Gerits, E.; De Brucker, K.; Vandamme, K.; Martens, J.; Michiels, J.; Vleugels, J.; Cammue, B.; et al. Controlled Release of Chlorhexidine from a Mesoporous Silica-Containing Macroporous Titanium Dental Implant Prevents Microbial Biofilm Formation. Eur. Cell. Mater. 2017, 33, 13–27. [Google Scholar] [CrossRef]
- Baghdan, E.; Raschpichler, M.; Lutfi, W.; Pinnapireddy, S.R.; Pourasghar, M.; Schäfer, J.; Schneider, M.; Bakowsky, U. Nano Spray Dried Antibacterial Coatings for Dental Implants. Eur. J. Pharm. Biopharm. 2019, 139, 59–67. [Google Scholar] [CrossRef]
- Karacan, I.; Ben-Nissan, B.; Wang, H.A.; Juritza, A.; Swain, M.V.; Müller, W.H.; Chou, J.; Stamboulis, A.; Macha, I.J.; Taraschi, V. Mechanical Testing of Antimicrobial Biocomposite Coating on Metallic Medical Implants as Drug Delivery System. Mater. Sci. Eng. C 2019, 104, 109757. [Google Scholar] [CrossRef]
- De Avila, E.D.; Castro, A.G.B.; Tagit, O.; Krom, B.P.; Löwik, D.; van Well, A.A.; Bannenberg, L.J.; Vergani, C.E.; van den Beucken, J.J.J.P. Anti-Bacterial Efficacy via Drug-Delivery System from Layer-by-Layer Coating for Percutaneous Dental Implant Components. Appl. Surf. Sci. 2019, 488, 194–204. [Google Scholar] [CrossRef]
- Lucke, M.; Schmidmaier, G.; Sadoni, S.; Wildemann, B.; Schiller, R.; Haas, N.P.; Raschke, M. Gentamicin Coating of Metallic Implants Reduces Implant-Related Osteomyelitis in Rats. Bone 2003, 32, 521–531. [Google Scholar] [CrossRef]
- Popat, K.C.; Eltgroth, M.; LaTempa, T.J.; Grimes, C.A.; Desai, T.A. Decreased Staphylococcus Epidermis Adhesion and Increased Osteoblast Functionality on Antibiotic-Loaded Titania Nanotubes. Biomaterials 2007, 28, 4880–4888. [Google Scholar] [CrossRef]
- Norowski, P.A.; Courtney, H.S.; Babu, J.; Haggard, W.O.; Bumgardner, J.D. Chitosan Coatings Deliver Antimicrobials from Titanium Implants: A Preliminary Study. Implant Dent. 2011, 20, 56–67. [Google Scholar] [CrossRef]
- Bottino, M.C.; Münchow, E.A.; Albuquerque, M.T.P.; Kamocki, K.; Shahi, R.; Gregory, R.L.; Chu, T.-M.G.; Pankajakshan, D. Tetracycline-Incorporated Polymer Nanofibers as a Potential Dental Implant Surface Modifier: TETRACYCLINE-INCORPORATED POLYMER NANOFIBERS. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 2085–2092. [Google Scholar] [CrossRef] [PubMed]
- Francolini, I.; Vuotto, C.; Piozzi, A.; Donelli, G. Antifouling and Antimicrobial Biomaterials: An Overview. APMIS 2017, 125, 392–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radin, S.; Ducheyne, P. Controlled Release of Vancomycin from Thin Sol–Gel Films on Titanium Alloy Fracture Plate Material. Biomaterials 2007, 28, 1721–1729. [Google Scholar] [CrossRef] [PubMed]
- Swanson, T.E.; Cheng, X.; Friedrich, C. Development of Chitosan-Vancomycin Antimicrobial Coatings on Titanium Implants. J. Biomed. Mater. Res. A 2011, 97A, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Zhang, P.; Wang, X.; Kasugai, S. A Doxycycline-Treated Hydroxyapatite Implant Surface Attenuates the Progression of Peri-Implantitis: A Radiographic and Histological Study in Mice. Clin. Implant Dent. Relat. Res. 2019, 21, 154–159. [Google Scholar] [CrossRef]
- Alécio, A.B.W.; Ferreira, C.F.; Babu, J.; Shokuhfar, T.; Jo, S.; Magini, R.; Garcia-Godoy, F. Doxycycline Release of Dental Implants with Nanotube Surface, Coated with Poly Lactic-Co-Glycolic Acid for Extended PH-Controlled Drug Delivery. J. Oral Implantol. 2019, 45, 267–273. [Google Scholar] [CrossRef]
- Ferreira, C.; Babu, J.; Hamlekhan, A.; Patel, S.; Shokuhfar, T. Efficiency of Nanotube Surface–Treated Dental Implants Loaded with Doxycycline on Growth Reduction of Porphyromonas Gingivalis. Int. J. Oral Maxillofac. Implant. 2017, 32, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Xing, R.; Witsø, I.L.; Jugowiec, D.; Tiainen, H.; Shabestari, M.; Lyngstadaas, S.P.; Lönn-Stensrud, J.; Haugen, H.J. Antibacterial Effect of Doxycycline-Coated Dental Abutment Surfaces. Biomed. Mater. 2015, 10, 055003. [Google Scholar] [CrossRef]
- Nie, B.; Ao, H.; Zhou, J.; Tang, T.; Yue, B. Biofunctionalization of Titanium with Bacitracin Immobilization Shows Potential for Anti-Bacteria, Osteogenesis and Reduction of Macrophage Inflammation. Colloids Surf. B Biointerfaces 2016, 145, 728–739. [Google Scholar] [CrossRef]
- Gómez-Florit, M.; Monjo, M.; Ramis, J.M. Quercitrin for Periodontal Regeneration: Effects on Human Gingival Fibroblasts and Mesenchymal Stem Cells. Sci. Rep. 2015, 5, 16593. [Google Scholar] [CrossRef] [Green Version]
- Somsanith, N.; Kim, Y.-K.; Jang, Y.-S.; Lee, Y.-H.; Yi, H.-K.; Jang, J.-H.; Kim, K.-A.; Bae, T.-S.; Lee, M.-H. Enhancing of Osseointegration with Propolis-Loaded TiO2 Nanotubes in Rat Mandible for Dental Implants. Materials 2018, 11, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Gao, B.; Liu, X.; Zhao, X.; Sun, W.; Ren, H.; Wu, J. In Vivo Evaluation of an Antibacterial Coating Containing Halogenated Furanone Compound-Loaded Poly(l-Lactic Acid) Nanoparticles on Microarc-Oxidized Titanium Implants. Int. J. Nanomed. 2016, 11, 1337–1347. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.-W.; Kim, M.-J.; Paeng, K.-W.; Yu, K.; Lee, C.-K.; Song, Y.W.; Cha, J.-K.; Sanz, M.; Jung, U.-W. Locally Applied Slow-Release of Minocycline Microspheres in the Treatment of Peri-Implant Mucositis: An Experimental In Vivo Study. Pharmaceutics 2020, 12, 668. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Bonilla, A.; Fernández-García, M. Polymeric Materials with Antimicrobial Activity. Prog. Polym. Sci. 2012, 37, 281–339. [Google Scholar] [CrossRef]
- Lawson, M.C.; Shoemaker, R.; Hoth, K.B.; Bowman, C.N.; Anseth, K.S. Polymerizable Vancomycin Derivatives for Bactericidal Biomaterial Surface Modification: Structure−Function Evaluation. Biomacromolecules 2009, 10, 2221–2234. [Google Scholar] [CrossRef] [Green Version]
- Kenawy, E.-R.; Abdel-Hay, F.I.; El-Magd, A.A.; Mahmoud, Y. Biologically Active Polymers: Modification and Anti-Microbial Activity of Chitosan Derivatives. J. Bioact. Compat. Polym. 2005, 20, 95–111. [Google Scholar] [CrossRef]
- Denyer, S.P. Mechanisms of Action of Antibacterial Biocides. Int. Biodeterior. Biodegrad. 1995, 36, 227–245. [Google Scholar] [CrossRef]
- Cheung, R.C.F.; Ng, T.B.; Wong, J.H.; Chan, W.Y. Chitosan: An Update on Potential Biomedical and Pharmaceutical Applications. Mar. Drugs 2015, 13, 5156–5186. [Google Scholar] [CrossRef]
- Yang, M.; Jiang, P.; Ge, Y.; Lan, F.; Zhou, X.; He, J.; Wu, Y. Dopamine Self-Polymerized along with Hydroxyapatite onto the Preactivated Titanium Percutaneous Implants Surface to Promote Human Gingival Fibroblast Behavior and Antimicrobial Activity for Biological Sealing. J. Biomater. Appl. 2018, 32, 1071–1082. [Google Scholar] [CrossRef]
- Shi, Z.; Neoh, K.G.; Kang, E.T.; Poh, C.K.; Wang, W. Surface Functionalization of Titanium with Carboxymethyl Chitosan and Immobilized Bone Morphogenetic Protein-2 for Enhanced Osseointegration. Biomacromolecules 2009, 10, 1603–1611. [Google Scholar] [CrossRef]
- Zheng, D.; Neoh, K.G.; Kang, E.-T. Bifunctional Coating Based on Carboxymethyl Chitosan with Stable Conjugated Alkaline Phosphatase for Inhibiting Bacterial Adhesion and Promoting Osteogenic Differentiation on Titanium. Appl. Surf. Sci. 2016, 360, 86–97. [Google Scholar] [CrossRef]
- Palla-Rubio, B.; Araújo-Gomes, N.; Fernández-Gutiérrez, M.; Rojo, L.; Suay, J.; Gurruchaga, M.; Goñi, I. Synthesis and Characterization of Silica-Chitosan Hybrid Materials as Antibacterial Coatings for Titanium Implants. Carbohydr. Polym. 2019, 203, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, H.; Ghasemi, Z.; Kharaziha, M.; Karimzadeh, F.; Alihosseini, F. Chitosan-58S Bioactive Glass Nanocomposite Coatings on TiO2 Nanotube: Structural and Biological Properties. Appl. Surf. Sci. 2018, 441, 138–149. [Google Scholar] [CrossRef]
- Fei Liu, X.; Lin Guan, Y.; Zhi Yang, D.; Li, Z.; De Yao, K. Antibacterial Action of Chitosan and Carboxymethylated Chitosan. J. Appl. Polym. Sci. 2001, 79, 1324–1335. [Google Scholar] [CrossRef]
- Tan, Y.; Han, F.; Ma, S.; Yu, W. Carboxymethyl Chitosan Prevents Formation of Broad-Spectrum Biofilm. Carbohydr. Polym. 2011, 84, 1365–1370. [Google Scholar] [CrossRef]
- Zafar, M.S.; Al-Samadani, K.H. Potential Use of Natural Silk for Bio-Dental Applications. J. Taibah Univ. Med. Sci. 2014, 9, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.; Jung, R.; Kim, H.-S.; Youk, J.H.; Jin, H.-J. Silver Nanoparticles Incorporated Electrospun Silk Fibers. J. Nanosci. Nanotechnol. 2007, 7, 3888–3891. [Google Scholar] [CrossRef]
- Xia, Y.; Gao, G.; Li, Y. Preparation and Properties of Nanometer Titanium Dioxide/Silk Fibroin Blend Membrane. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90B, 653–658. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, W.; Niu, J.; Chen, Y. Mechanism of Photogenerated Reactive Oxygen Species and Correlation with the Antibacterial Properties of Engineered Metal-Oxide Nanoparticles. ACS Nano 2012, 6, 5164–5173. [Google Scholar] [CrossRef]
- Rossi, M.C.; Bezerra, F.J.B.; Silva, R.A.; Crulhas, B.P.; Fernandes, C.J.C.; Nascimento, A.S.; Pedrosa, V.A.; Padilha, P.; Zambuzzi, W.F. Titanium-Released from Dental Implant Enhances Pre-Osteoblast Adhesion by ROS Modulating Crucial Intracellular Pathways: Dental Implants on Osteoblast Behavior. J. Biomed. Mater. Res. A 2017, 105, 2968–2976. [Google Scholar] [CrossRef]
- Chun, M.-J.; Shim, E.; Kho, E.-H.; Park, K.-J.; Jung, J.; Kim, J.-M.; Kim, B.; Lee, K.-H.; Cho, D.-L.; Bai, D.-H.; et al. Surface Modification of Orthodontic Wires with Photocatalytic Titanium Oxide for Its Antiadherent and Antibacterial Properties. Angle Orthod. 2007, 77, 483–488. [Google Scholar] [CrossRef]
- Buxadera-Palomero, J.; Canal, C.; Torrent-Camarero, S.; Garrido, B.; Javier Gil, F.; Rodríguez, D. Antifouling Coatings for Dental Implants: Polyethylene Glycol-like Coatings on Titanium by Plasma Polymerization. Biointerphases 2015, 10, 029505. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.I.; Lee, J.H.; Andrade, J.D.; De Gennes, P.G. Protein—Surface Interactions in the Presence of Polyethylene Oxide. J. Colloid Interface Sci. 1991, 142, 149–158. [Google Scholar] [CrossRef]
- Buxadera-Palomero, J.; Albó, K.; Gil, F.J.; Mas-Moruno, C.; Rodríguez, D. Polyethylene Glycol Pulsed Electrodeposition for the Development of Antifouling Coatings on Titanium. Coatings 2020, 10, 456. [Google Scholar] [CrossRef]
- Accioni, F.; García-Gómez, D.; Girela, E.; Rubio, S. SUPRAS Extraction Approach for Matrix-Independent Determination of Amphetamine-Type Stimulants by LC-MS/MS. Talanta 2018, 182, 574–582. [Google Scholar] [CrossRef]
- Accioni, F.; García-Gómez, D.; Rubio, S. Exploring Polar Hydrophobicity in Organized Media for Extracting Oligopeptides: Application to the Extraction of Opiorphin in Human Saliva. J. Chromatogr. A 2021, 1635, 461777. [Google Scholar] [CrossRef]
- Prime, K.L.; Whitesides, G.M. Self-Assembled Organic Monolayers: Model Systems for Studying Adsorption of Proteins at Aurfaces. Science 1991, 252, 1164–1167. [Google Scholar] [CrossRef] [Green Version]
- Freitas, S.C.; Correa-Uribe, A.; Martins, M.C.L.; Pelaez-Vargas, A. Self-Assembled Monolayers for Dental Implants. Int. J. Dent. 2018, 2018, 4395460. [Google Scholar] [CrossRef]
- Francolini, I.; Hall-Stoodley, L.; Stoodley, P. Biofilms, Biomaterials, and Device-Related Infections. In Biomaterials Science; Elsevier: Amsterdam, The Netherlands, 2020; pp. 823–840. ISBN 978-0-12-816137-1. [Google Scholar]
- Roosjen, A.; de Vries, J.; van der Mei, H.C.; Norde, W.; Busscher, H.J. Stability and Effectiveness against Bacterial Adhesion of Poly(Ethylene Oxide) Coatings in Biological Fluids. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 73B, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Chen, C.; Melo, M.A.; Bai, Y.-X.; Cheng, L.; Xu, H.H. A Novel Protein-Repellent Dental Composite Containing 2-Methacryloyloxyethyl Phosphorylcholine. Int. J. Oral Sci. 2015, 7, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Kwon, J.-S.; Kim, J.-Y.; Mangal, U.; Seo, J.-Y.; Lee, M.-J.; Jin, J.; Yu, J.-H.; Choi, S.-H. Durable Oral Biofilm Resistance of 3D-Printed Dental Base Polymers Containing Zwitterionic Materials. Int. J. Mol. Sci. 2021, 22, 417. [Google Scholar] [CrossRef] [PubMed]
- Ramburrun, P.; Pringle, N.A.; Dube, A.; Adam, R.Z.; D’Souza, S.; Aucamp, M. Recent Advances in the Development of Antimicrobial and Antifouling Biocompatible Materials for Dental Applications. Materials 2021, 14, 3167. [Google Scholar] [CrossRef] [PubMed]
- Hirota, K.; Murakami, K.; Nemoto, K.; Miyake, Y. Coating of a Surface with 2-Methacryloyloxyethyl Phosphorylcholine (MPC) Co-Polymer Significantly Reduces Retention of Human Pathogenic Microorganisms. FEMS Microbiol. Lett. 2005, 248, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyama, J.; Fukazawa, K.; Ishihara, K.; Mori, Y. In Situ Surface Modification on Dental Composite Resin Using 2-Methacryloyloxyethyl Phosphorylcholine Polymer for Controlling Plaque Formation. Mater. Sci. Eng. C 2019, 104, 109916. [Google Scholar] [CrossRef] [PubMed]
- Ikeya, K.; Iwasa, F.; Inoue, Y.; Fukunishi, M.; Takahashi, N.; Ishihara, K.; Baba, K. Inhibition of Denture Plaque Deposition on Complete Dentures by 2-Methacryloyloxyethyl Phosphorylcholine Polymer Coating: A Clinical Study. J. Prosthet. Dent. 2018, 119, 67–74. [Google Scholar] [CrossRef]
- Falde, E.J.; Yohe, S.T.; Colson, Y.L.; Grinstaff, M.W. Superhydrophobic Materials for Biomedical Applications. Biomaterials 2016, 104, 87–103. [Google Scholar] [CrossRef] [Green Version]
- Bartlet, K.; Movafaghi, S.; Dasi, L.P.; Kota, A.K.; Popat, K.C. Antibacterial Activity on Superhydrophobic Titania Nanotube Arrays. Colloids Surf. B Biointerfaces 2018, 166, 179–186. [Google Scholar] [CrossRef]
- Souza, J.G.S.; Bertolini, M.; Costa, R.C.; Cordeiro, J.M.; Nagay, B.E.; de Almeida, A.B.; Retamal-Valdes, B.; Nociti, F.H.; Feres, M.; Rangel, E.C.; et al. Targeting Pathogenic Biofilms: Newly Developed Superhydrophobic Coating Favors a Host-Compatible Microbial Profile on the Titanium Surface. ACS Appl. Mater. Interfaces 2020, 12, 10118–10129. [Google Scholar] [CrossRef]
- Singh, R.; Kumar, S. Applications of Graphene-Based Sensors for Biomedical Industries. In Comprehensive Analytical Chemistry; Elsevier: Amsterdam, The Netherlands, 2020; Volume 91, pp. 201–233. ISBN 978-0-323-85371-2. [Google Scholar]
- Gul, S.S.; Abdulkareem, A.A.; Sha, A.M.; Rawlinson, A. Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases. Diagnostics 2020, 10, 838. [Google Scholar] [CrossRef]
- Souza, J.G.S.; Bertolini, M.M.; Costa, R.C.; Nagay, B.E.; Dongari-Bagtzoglou, A.; Barão, V.A.R. Targeting Implant-Associated Infections: Titanium Surface Loaded with Antimicrobial. iScience 2021, 24, 102008. [Google Scholar] [CrossRef]
- Catauro, M.; Papale, F.; Bollino, F.; Piccolella, S.; Marciano, S.; Nocera, P.; Pacifico, S. Silica/Quercetin Sol–Gel Hybrids as Antioxidant Dental Implant Materials. Sci. Technol. Adv. Mater. 2015, 16, 035001. [Google Scholar] [CrossRef] [Green Version]
- Reise, M.; Wyrwa, R.; Müller, U.; Zylinski, M.; Völpel, A.; Schnabelrauch, M.; Berg, A.; Jandt, K.D.; Watts, D.C.; Sigusch, B.W. Release of Metronidazole from Electrospun Poly(l-Lactide-Co-d/l-Lactide) Fibers for Local Periodontitis Treatment. Dent. Mater. 2012, 28, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Nikolin, B.; Imamović, B.; Medanhodžić-Vuk, S.; Sober, M. High Performance Liquid Chromatography in Pharmaceutical Analyses. Bosn. J. Basic Med. Sci. 2004, 4, 5–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapter, G. 621> Chromatography. U. S. Pharmacop. 2012, 40, 508–520. [Google Scholar]
- Stevanović, M.; Djošić, M.; Janković, A.; Kojić, V.; Stojanović, J.; Grujić, S.; Bujagić, I.M.; Rhee, K.Y.; Mišković-Stanković, V. The Chitosan-Based Bioactive Composite Coating on Titanium. J. Mater. Res. Technol. 2021, 15, 4461–4474. [Google Scholar] [CrossRef]
- Guo, M.X.; Wrisley, L.; Maygoo, E. Measurement of Tobramycin by Reversed-Phase High-Performance Liquid Chromatography with Mass Spectrometry Detection. Anal. Chim. Acta 2006, 571, 12–16. [Google Scholar] [CrossRef]
- Fabre, H.; Sekkat, M.; Blanchin, M.D.; Mandrou, B. Determination of Aminoglycosides in Pharmaceutical Formulations—II. High-Performance Liquid Chromatography. J. Pharm. Biomed. Anal. 1989, 7, 1711–1718. [Google Scholar] [CrossRef]
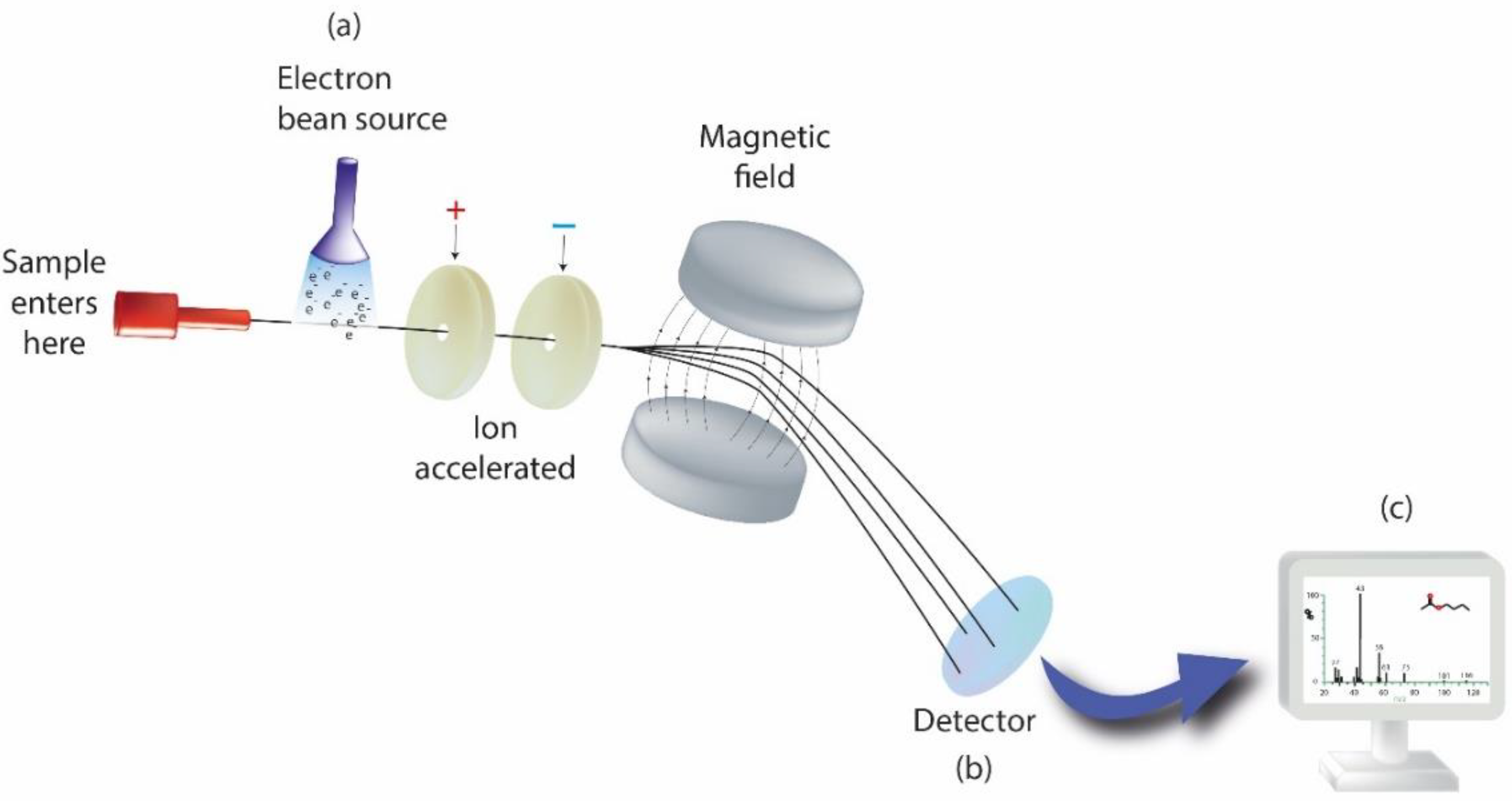
- Altuntaş, E.; Schubert, U.S. “Polymeromics”: Mass Spectrometry Based Strategies in Polymer Science toward Complete Sequencing Approaches: A Review. Anal. Chim. Acta 2014, 808, 56–69. [Google Scholar] [CrossRef]
- Vailati-Riboni, M.; Palombo, V.; Loor, J.J. What Are Omics Sciences? In Periparturient Diseases of Dairy Cows; Springer: Cham, Switzerland, 2017; pp. 1–7. [Google Scholar]
- Calciolari, E.; Donos, N. The Use of Omics Profiling to Improve Outcomes of Bone Regeneration and Osseointegration. How Far Are We from Personalized Medicine in Dentistry? J. Proteom. 2018, 188, 85–96. [Google Scholar] [CrossRef]
- Alalwiat, A.; Tang, W.; Gerişlioğlu, S.; Becker, M.L.; Wesdemiotis, C. Mass Spectrometry and Ion Mobility Characterization of Bioactive Peptide–Synthetic Polymer Conjugates. Anal. Chem. 2017, 89, 1170–1177. [Google Scholar] [CrossRef]
- Biomarkers and Surrogate Endpoints: Preferred Definitions and Conceptual Framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [CrossRef] [PubMed]
- Albeshri, S.; Alblaihess, A.; Niazy, A.A.; Ramalingam, S.; Sundar, C.; Alghamdi, H.S. Biomarkers as Independent Predictors of Bone Regeneration around Biomaterials: A Systematic Review of Literature. J. Contemp. Dent. Pract. 2018, 19, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Colombo, J.S.; Balani, D.; Sloan, A.J.; Crean, S.J.; Okazaki, J.; Waddington, R.J. Delayed Osteoblast Differentiation and Altered Inflammatory Response around Implants Placed in Incisor Sockets of Type 2 Diabetic Rats: Delayed Osteoblast Differentiation in Diabetic Bone Healing. Clin. Oral Implant. Res. 2011, 22, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Monjo, M.; Ramis, J.M.; Rønold, H.J.; Taxt-Lamolle, S.F.; Ellingsen, J.E.; Lyngstadaas, S.P. Correlation between Molecular Signals and Bone Bonding to Titanium Implants. Clin. Oral Implant. Res. 2012, 24. [Google Scholar] [CrossRef]
- Song, C. Single-Dose Local Simvastatin Injection Improves Implant Fixation via Increased Angiogenesis and Bone Formation in an Ovariectomized Rat Model. Med. Sci. Monit. 2015, 21, 1428–1439. [Google Scholar] [CrossRef] [Green Version]
- Monjo, M.; Lamolle, S.F.; Lyngstadaas, S.P.; Rønold, H.J.; Ellingsen, J.E. In Vivo Expression of Osteogenic Markers and Bone Mineral Density at the Surface of Fluoride-Modified Titanium Implants. Biomaterials 2008, 29, 3771–3780. [Google Scholar] [CrossRef]
- Kumar, Y.; Jain, V.; Chauhan, S.S.; Bharate, V.; Koli, D.; Kumar, M. Influence of Different Forms and Materials (Zirconia or Titanium) of Abutments in Peri-Implant Soft-Tissue Healing Using Matrix Metalloproteinase-8: A Randomized Pilot Study. J. Prosthet. Dent. 2017, 118, 475–480. [Google Scholar] [CrossRef]
- Nelson, K.; Hesse, B.; Addison, O.; Morrell, A.P.; Gross, C.; Lagrange, A.; Suárez, V.I.; Kohal, R.; Fretwurst, T. Distribution and Chemical Speciation of Exogenous Micro- and Nanoparticles in Inflamed Soft Tissue Adjacent to Titanium and Ceramic Dental Implants. Anal. Chem. 2020, 92, 14432–14443. [Google Scholar] [CrossRef]
- Schoon, J.; Hesse, B.; Rakow, A.; Ort, M.J.; Lagrange, A.; Jacobi, D.; Winter, A.; Huesker, K.; Reinke, S.; Cotte, M.; et al. Metal-Specific Biomaterial Accumulation in Human Peri-Implant Bone and Bone Marrow. Adv. Sci. 2020, 7, 2000412. [Google Scholar] [CrossRef]
- Delgado-Ruiz, R.; Romanos, G. Potential Causes of Titanium Particle and Ion Release in Implant Dentistry: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef] [Green Version]
- Carcuac, O.; Berglundh, T. Composition of Human Peri-Implantitis and Periodontitis Lesions. J. Dent. Res. 2014, 93, 1083–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garaicoa-Pazmino, C.; Fretwurst, T.; Squarize, C.H.; Berglundh, T.; Giannobile, W.V.; Larsson, L.; Castilho, R.M. Characterization of Macrophage Polarization in Periodontal Disease. J. Clin. Periodontol. 2019, 46, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Müller, J.; Larsson, L.; Bronsert, P.; Hazard, D.; Castilho, R.M.; Kohal, R.; Nelson, K.; Iglhaut, G. Immunohistological Composition of Peri-implantitis Affected Tissue around Ceramic Implants—A Pilot Study. J. Periodontol. 2021, 92, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Addison, O.; Davenport, A.J.; Newport, R.J.; Kalra, S.; Monir, M.; Mosselmans, J.F.W.; Proops, D.; Martin, R.A. Do ‘Passive’ Medical Titanium Surfaces Deteriorate in Service in the Absence of Wear? J. R. Soc. Interface 2012, 9, 3161–3164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Reichl, F.-X.; Milz, S.; Michalke, B.; Wu, X.; Sprecher, C.M.; Yang, Y.; Gahlert, M.; Röhling, S.; Kniha, H.; et al. Titanium and Zirconium Release from Titanium- and Zirconia Implants in Mini Pig Maxillae and Their Toxicity In Vitro. Dent. Mater. 2020, 36, 402–412. [Google Scholar] [CrossRef] [PubMed]
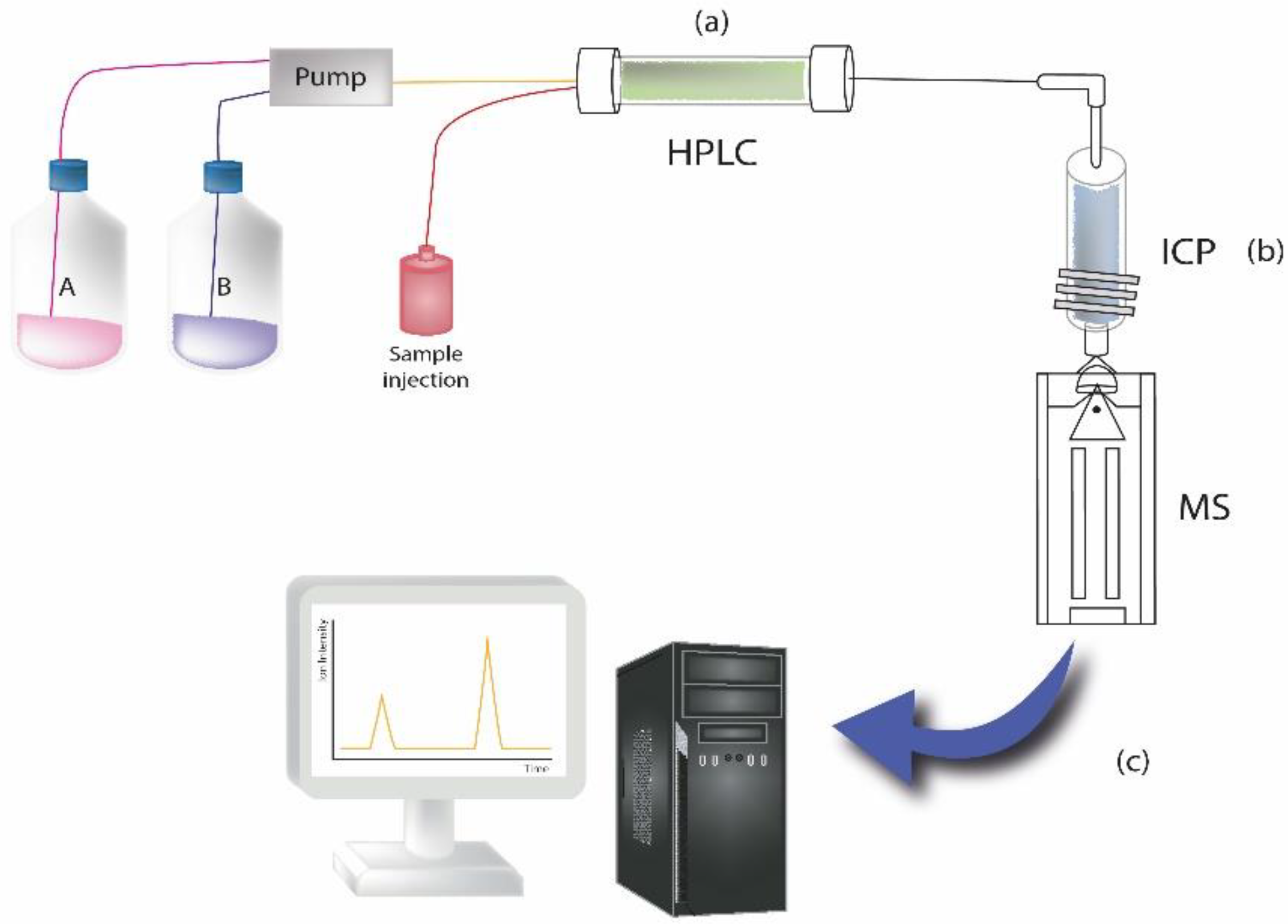
- Pechancová, R.; Pluháček, T.; Gallo, J.; Milde, D. Study of Chromium Species Release from Metal Implants in Blood and Joint Effusion: Utilization of HPLC-ICP-MS. Talanta 2018, 185, 370–377. [Google Scholar] [CrossRef]
- Balcaen, L.; Bolea-Fernandez, E.; Resano, M.; Vanhaecke, F. Accurate Determination of Ultra-Trace Levels of Ti in Blood Serum Using ICP-MS/MS. Anal. Chim. Acta 2014, 809, 1–8. [Google Scholar] [CrossRef]
- Sarmiento-González, A.; Encinar, J.R.; Marchante-Gayón, J.M.; Sanz-Medel, A. Titanium Levels in the Organs and Blood of Rats with a Titanium Implant, in the Absence of Wear, as Determined by Double-Focusing ICP-MS. Anal. Bioanal. Chem. 2009, 393, 335–343. [Google Scholar] [CrossRef]
- Sajnóg, A.; Hanć, A.; Koczorowski, R.; Barałkiewicz, D. New Procedure of Quantitative Mapping of Ti and Al Released from Dental Implant and Mg, Ca, Fe, Zn, Cu, Mn as Physiological Elements in Oral Mucosa by LA-ICP-MS. Talanta 2017, 175, 370–381. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Accioni, F.; Vázquez, J.; Merinero, M.; Begines, B.; Alcudia, A. Latest Trends in Surface Modification for Dental Implantology: Innovative Developments and Analytical Applications. Pharmaceutics 2022, 14, 455. https://doi.org/10.3390/pharmaceutics14020455
Accioni F, Vázquez J, Merinero M, Begines B, Alcudia A. Latest Trends in Surface Modification for Dental Implantology: Innovative Developments and Analytical Applications. Pharmaceutics. 2022; 14(2):455. https://doi.org/10.3390/pharmaceutics14020455
Chicago/Turabian StyleAccioni, Francesca, Juan Vázquez, Manuel Merinero, Belén Begines, and Ana Alcudia. 2022. "Latest Trends in Surface Modification for Dental Implantology: Innovative Developments and Analytical Applications" Pharmaceutics 14, no. 2: 455. https://doi.org/10.3390/pharmaceutics14020455