
Sodium Valproate Incompatibility with Parenteral Nutrition Admixtures—A Risk to Patient Safety: An In Vitro Evaluation Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Visual Control
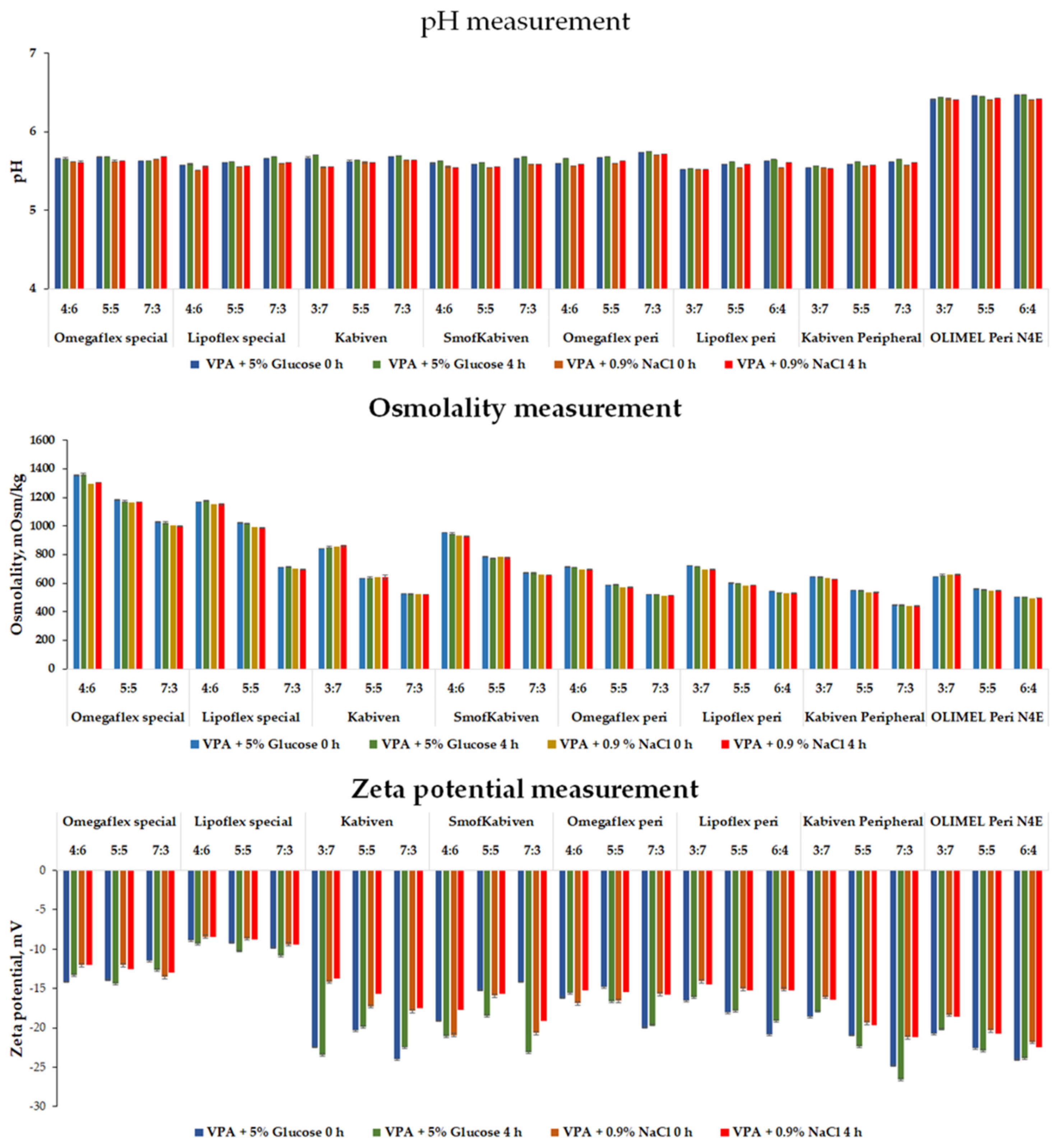
2.2.2. pH Measurement
2.2.3. Osmolality Measurement
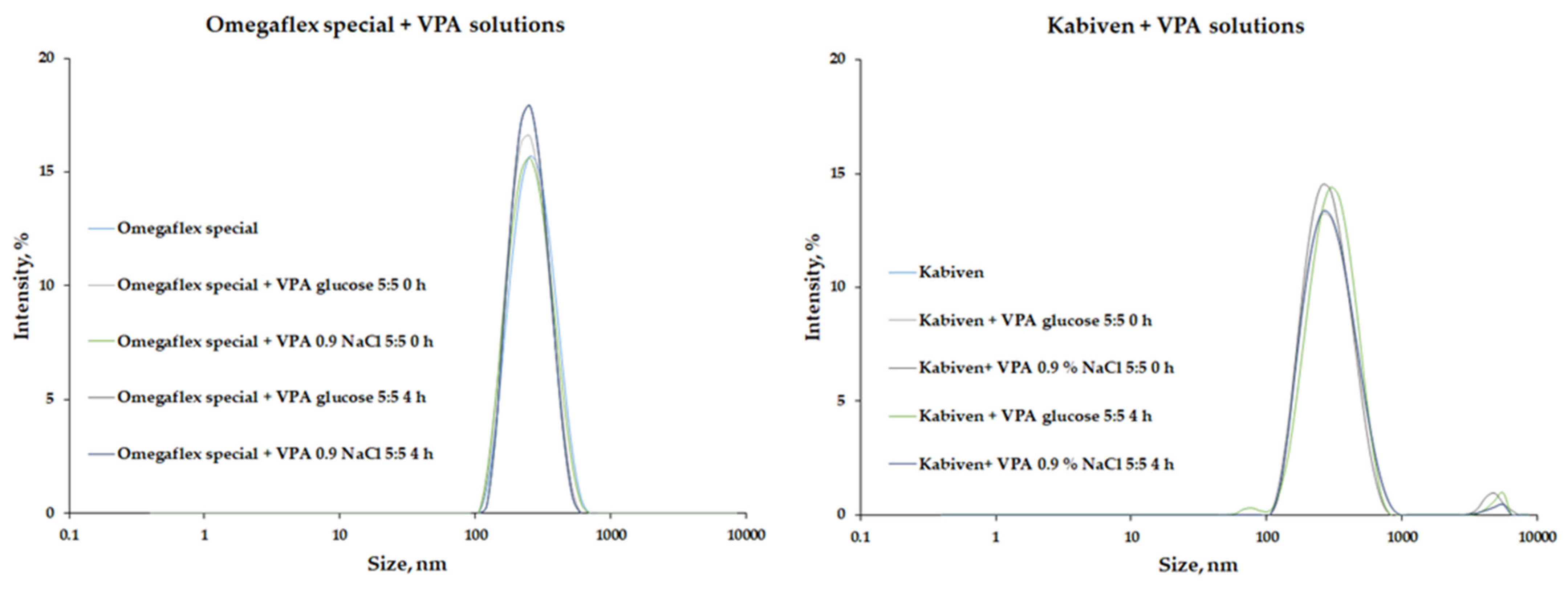
2.2.4. Polidispersity Index, MDD and Zeta Potential Measurements
2.2.5. Turbidity Measurement
2.2.6. Statistical Analysis
3. Results
3.1. Parenteral Nutrition Admixture without Drug Solutions—Reference Samples
3.2. Parenteral Nutrition Admixture with Drug Solutions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berg, A.T.; Berkovic, S.F.; Brodie, M.J.; Buchhalter, J.; Cross, J.H.; van Emde Boas, W.; Engel, J.; French, J.; Glauser, T.A.; Mathern, G.W.; et al. Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 2010, 51, 676–685. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Epilepsy. Available online: https://www.who.int/news-room/fact-sheets/detail/epilepsy (accessed on 20 December 2021).
- Healthcare Cost and Utilization Project. Available online: https://hcupnet.ahrq.gov/#setup (accessed on 20 December 2021).
- Varelas, P.N.; Spanaki, M.V.; Mirski, M.A. Seizures and the neurosurgical intensive care unit. Neurosurg. Clin. N. Am. 2013, 24, 393–406. [Google Scholar] [CrossRef] [PubMed]
- Voils, S.A.; Human, T.; Brophy, G.M. Adverse neurologic effects of medications commonly used in the intensive care unit. Crit. Care Clin. 2014, 30, 795–811. [Google Scholar] [CrossRef] [PubMed]
- Farrokh, S.; Tahsili-Fahadan, P.; Ritzl, E.K.; Lewin, J.J.; Mirski, M.A. Antiepileptic drugs in critically ill patients. Crit. Care 2018, 22, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [Green Version]
- Mogensen, K.M.; Robinson, M.K.; Casey, J.D.; Gunasekera, N.S.; Moromizato, T.; Rawn, J.D.; Christopher, K.B. Nutritional Status and Mortality in the Critically ill. Crit. Care Med. 2015, 43, 2605–2615. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Granick, J.; Grutsch, J.F.; Vashi, P.G.; Lammersfeld, C.A. Malnutrition was associated with poor quality of life in colorectal cancer: A retrospective analysis. J. Clin. Epidemiol. 2006, 59, 704–709. [Google Scholar] [CrossRef]
- Anker, S.D.; Laviano, A.; Filippatos, G.; John, M.; Paccagnella, A.; Ponikowski, P.; Schols, A.M.W.J. ESPEN Guidelines on Parenteral Nutrition: On Cardiology and Pneumology. Clin. Nutr. 2009, 28, 455–460. [Google Scholar] [CrossRef]
- Kern, K.A.; Norton, J.A. Cancer cachexia. J. Parenter. Enter. Nutr. 1988, 12, 286–298. [Google Scholar] [CrossRef]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zurcher, G.; Muscaritoli, M.; ESPEN. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef]
- Braga, M.; Ljungqvist, O.; Soeters, P.; Fearon, K.; Weimann, A.; Bozzetti, F. ESPEN Guidelines on Parenteral Nutrition: Surgery. Clin. Nutr. 2009, 28, 378–386. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN Guideline ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Gostyńska, A.; Stawny, M.; Dettlaff, K.; Jelińska, A. The interactions between ciprofloxacin and parenteral nutrition admixtures. Pharmaceutics 2020, 12, 27. [Google Scholar] [CrossRef] [Green Version]
- Tomczak, S.; Gostyńska, A.; Nadolna, M.; Reisner, K.; Orlando, M.; Jelińska, A.; Stawny, M. Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins. Antibiotics 2021, 10, 549. [Google Scholar] [CrossRef]
- Stawny, M.; Nadolna, M.; Jelińska, A. In vitro compatibility studies of vancomycin with ready-to-use parenteral nutrition admixtures for safer clinical practice. Clin. Nutr. 2019, 39, 2539–2546. [Google Scholar] [CrossRef]
- Bouchoud, L.; Fonzo-Christe, C.; Klingmüller, M.; Bonnabry, P. Compatibility of intravenous medications with parenteral nutrition: In vitro evaluation. JPEN J. Parenter. Enter. Nutr. 2013, 37, 416–424. [Google Scholar] [CrossRef]
- Eckle, V.S.; Heim, E.; Hahn, M.; Grasshoff, C. Incompatibility of piritramide with cephalosporins. Ann. Pharmacother. 2013, 47, 426–427. [Google Scholar] [CrossRef]
- Pertkiewicz, M.; Cosslett, A.; Mühlebach, S.; Dudrick, S.J. Basics in clinical nutrition: Stability of parenteral nutrition admixtures. e-SPEN 2009, 4, e117–e119. [Google Scholar] [CrossRef] [Green Version]
- Salih, M.R.; Bahari, M.B.; Abd, A.Y. Selected pharmacokinetic issues of the use of antiepileptic drugs and parenteral nutrition in critically ill patients. Nutr. J. 2010, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.N. Redefining drug-nutrient interactions. Nutr. Clin. Pract. 2000, 15, 249–252. [Google Scholar] [CrossRef]
- Oberndorfer, S.; Grisold, W. Antiepileptic drugs in brain tumour patients. In Memo-Magazine of European Medical Oncology; Springer: New York City, NY, USA, 2008; Volume 1, pp. 28–30. [Google Scholar] [CrossRef]
- Dasgupta, A.; Crossey, M.J. Elevated free fatty acid concentrations in lipemic sera reduce protein binding of valproic acid significantly more than phenytoin. Am. J. Med. Sci. 1997, 313, 75–79. [Google Scholar] [CrossRef]
- Zimmerman, C.L.; Patel, I.H.; Levy, R.H.; Edwards, D.; Nelson, S.D.; Hutchinson, M. Protein binding of valproic acid in the presence of elevated free fatty acids in patient and normal human serum. Epilepsia 1981, 22, 11–17. [Google Scholar] [CrossRef]
- Dutkiewicz, G.; Wójcik, J.; Gawrońska-Szklarz, B. The effect of hyperlipidemia on pharmacokinetics of free phenytoin. Neurol. Neurochir. Pol. 1994, 28, 845–852. [Google Scholar]
- Bailey, D.N.; Briggs, J.R. The effect of parenteral nutrition fluids on the binding of therapeutic drugs to human serum in vitro. Ther. Drug Monit. 2004, 26, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Rashed, S.M.; Sweatman, T.W.; Thoma, L.; Hovinga, C.A.; Phelps, S.J. Chemical compatibility of depacon(®) with medications frequently administered by intravenous y-site delivery in patients with epilepsy or head trauma. J. Pediatr. Pharmacol. Ther. 2004, 9, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, M.I.; Boddu, S.H.S.; Mauro, V.F.; Churchwell, M.D. Physical compatibility of valproate sodium injection with dobutamine and dopamine. Am. J. Health-Syst. Pharm. 2017, 74, 280–281. [Google Scholar] [CrossRef] [PubMed]
- European Directorate for Quality in Medicines and Healthcare (EDQM). 2.9.20. Particulate contamination: Visible particles. In European Pharmacopeia; EDQM: Strasburg, France, 2017. [Google Scholar]
- Gostyńska, A.; Piwowarczyk, L.; Nadolna, M.; Jelińska, A.; Dettlaff, K.; Ogrodowczyk, M.; Popielarz-Brzezińska, M.; Stawny, M. Toward safe pharmacotherapy: The interplay between meropenem and parenteral nutrition admixtures. Antibiotics 2021, 10, 217. [Google Scholar] [CrossRef]
- Avery, L.M.; Chen, I.H.; Reyes, S.; Nicolau, D.P.; Kuti, J.L. Assessment of the Physical Compatibility of Eravacycline and Common Parenteral Drugs During Simulated Y-site Administration. Clin. Ther. 2019, 41, 2162–2170. [Google Scholar] [CrossRef]
- Monogue, M.L.; Almarzoky Abuhussain, S.S.; Kuti, J.L.; Nicolau, D.P. Physical compatibility of fosfomycin for injection with select i.v. drugs during simulated Y-site administration. Am. J. Health-Syst. Pharm. 2018, 75, e36–e44. [Google Scholar] [CrossRef]
- Trissel, L.A.; Bready, B.B. Turbidimetric assessment of the compatibility of taxol with selected other drugs during simulated Y-site injection. Am. J. Hosp. Pharm. 1992, 49, 1716–1719. [Google Scholar] [CrossRef]
- Sürmelioğlu, N.; Nenni, M.; Fırat, A.; Demirkan, K.; Özcengiz, D. Evaluation of regular insulin adsorption to polypropylene bag and polyvinyl chloride infusion set. Int. J. Clin. Pract. 2021, 75, e13895. [Google Scholar] [CrossRef]
- Urien, S.; Albengres, E.; Tillement, J.P. Serum protein binding of valproic acid in healthy subjects and in patients with liver disease. Int. J. Clin. Pharm. Toxicol. 1981, 19, 319–325. [Google Scholar]
- Lenn, N.J.; Robertson, M. Clinical utility of unbound antiepileptic drug blood levels in the management of epilepsy. Neurology 1992, 42, 988–990. [Google Scholar] [CrossRef]
- VandenBerg, A.; Broadway, J. Enteral administration of protein supplement and valproate: A potential pharmacokinetic interaction. Ment. Health Clin. 2017, 7, 10. [Google Scholar] [CrossRef]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Development and evaluation of a test program for Y-site compatibility testing of total parenteral nutrition and intravenous drugs. Nutr. J. 2016, 15, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Stawny, M.; Gostyńska, A.; Dettlaff, K.; Jelińska, A.; Główka, E.; Ogrodowczyk, M. Effect of lipid emulsion on stability of ampicillin in total parenteral nutrition. Nutrients 2019, 11, 559. [Google Scholar] [CrossRef] [Green Version]
- Humbert-Delaloye, V.; Berger-Gryllaki, M.; Voirol, P.; Testa, B.; Pannatier, A. Screening for physicochemical incompatibilities of intravenous drugs in intensive care units: The case of monobasic potassium phosphate and furosemide. Eur. J. Hosp. Pharm. 2015, 22, 56–58. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.M.; Villareal, C.L.; Meyer, L.M. Y-Site Compatibility of Intravenous Levetiracetam with Commonly Used Critical Care Medications. Hosp. Pharm. 2019, 56, 282–286. [Google Scholar] [CrossRef]
- Staven, V.; Iqbal, H.; Wang, S.; Grønlie, I.; Tho, I. Physical compatibility of total parenteral nutrition and drugs in Y-site administration to children from neonates to adolescents. J. Pharm. Pharmacol. 2017, 69, 448–462. [Google Scholar] [CrossRef]
- Tomczak, S.; Stawny, M.; Jelińska, A. Co-Administration of Drugs and Parenteral Nutrition: In Vitro Compatibility Studies of Loop Diuretics for Safer Clinical Practice. Pharmaceutics 2020, 12, 1092. [Google Scholar] [CrossRef]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Physical stability of an all-in-one parenteral nutrition admixture for preterm infants upon mixing with micronutrients and drugs. Eur. J. Hosp. Pharm. 2020, 27, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Tomczak, S.; Stawny, M.; Dettlaff, K.; Kieliszek, M.; Słomińska, D.; Jelińska, A. Physicochemical Compatibility and Stability of Linezolid with Parenteral Nutrition. Molecules 2019, 24, 1242. [Google Scholar] [CrossRef] [Green Version]
- Wang, W. Tolerability of hypertonic injectables. Int. J. Pharm. 2015, 490, 308–315. [Google Scholar] [CrossRef]
- Washington, C. Stability of lipid emulsions for drug delivery. Adv. Drug Deliv. Rev. 1996, 20, 131–145. [Google Scholar] [CrossRef]
- FDA. Liposome Drug Products: Chemistry, Manufacturing, and Controls; Human Pharmacokinetics and Bioavailability; and Labeling Documentation; FDA-2016-D-2817; Center for Drug Evaluation and Research: Silver Spring, MD, USA, 2018.
- US Pharmacopeia. Globule Size Distribution in Lipid Injectable Emulsions; US Pharmacopeia: Rockville, MD, USA, 2011; Volume 1, pp. 297–299. [Google Scholar]
- Gilbert, R.G.; Hess, M.; Jenkins, A.D.; Jones, R.G.; Kratochvíl, P.; Stepto, R.F.T. Dispersity in polymer science (IUPAC Recommendations 2009). Pure Appl. Chem. 2009, 81, 351–353. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Dong, W.-J.; Li, L.; Xu, J.-M.; Jin, D.-J.; Xia, X.-J.; Liu, Y.-L. Effect of high-pressure homogenization preparation on mean globule size and large-diameter tail of oil-in-water injectable emulsions. J. Food Drug Anal. 2015, 23, 828–835. [Google Scholar] [CrossRef]
- Markoutsa, E.; Papadia, K.; Clemente, C.; Flores, O.; Antimisiaris, S.G. Anti-AÎ2-MAb and dually decorated nanoliposomes: Effect of AÎ21-42 peptides on interaction with hCMEC/D3 cells. Eur. J. Pharm. Biopharm. 2012, 81, 49–56. [Google Scholar] [CrossRef]
- Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R.; Dokhani, A.; Khorasani, S.; Mozafari, M.R. Impact of Particle Size and Polydispersity Index on the Clinical Applications of Lipidic Nanocarrier Systems. Pharmaceutics 2018, 10, 57. [Google Scholar] [CrossRef] [Green Version]
- Putri, D.C.A.; Dwiastuti, R.; Marchaban, M.; Nugroho, A.K. Optimization of mixing temperatur and sonication duration in liposome preparation. J. Pharm. Sci. Community 2017, 14, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Badran, M. Formulation and in vitro evaluation of flufenamic acid loaded deformable liposomes for improved skin delivery. Dig. J. Nanomater. Biostructures 2014, 9, 83–91. [Google Scholar]
- Harun, S.N.; Nordin, S.A.; Gani, S.S.A.; Shamsuddin, A.F.; Basri, M.; Basri, H. Bin Development of nanoemulsion for efficient brain parenteral delivery of cefuroxime: Designs, characterizations, and pharmacokinetics. Int. J. Nanomed. 2018, 13, 2571–2584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stawny, M.; Gostyńska, A.; Nadolna, M.; Jelińska, A. Safe practice of Y-site drug administration: The case of colistin and parenteral nutrition. Pharmaceutics 2020, 12, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| PNA | Total Energy (kcal) | Glucose (g) | Lipid (g) | MCT 1 (g) | Soya-Bean Oil (g) | Fish Oil (g) | Olive Oil (g) | Acids Ω-3 (g) | Amino Acids (g) | Nitrogen (g) | Vitamin Source | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Central access | Omegaflex special | 1184.0 | 144.0 | 40.0 | 20.0 | 16.0 | - | - | 4.0 | 56.0 | 8.0 | Viantan |
| Lipoflex special | 1184.0 | 144.0 | 40.0 | 20.0 | 20.0 | - | - | - | 56.0 | 8.0 | Viantan | |
| Kabiven | 909.1 | 97.4 | 39.0 | - | 39.0 | - | - | - | 33.1 | 5.3 | V + S 2 | |
| SmofKabiven | 1083.3 | 126.6 | 37.9 | 11.4 | 11.4 | 5.7 | 9.6 | - | 50.8 | 8.1 | V + S 2 | |
| Peripheral access | Omegaflex peri | 764.0 | 64.0 | 40.0 | 20.0 | 16.0 | - | - | 4.0 | 32.0 | 4.6 | Viantan |
| Lipoflex peri | 764.0 | 64.0 | 40.0 | 20.0 | 20.0 | - | - | - | 32.0 | 4.6 | Viantan | |
| Kabiven Peripheral | 694.4 | 67.4 | 35.4 | - | 35.4 | - | - | - | 23.6 | 3.8 | V + S 2 | |
| Olimel Peri N4E | 700.0 | 75.0 | 30.0 | - | 24.0 | - | 6.0 | - | 25.3 | 4.0 | Cernevit | |
| Parenteral Fluids | Infusion Rate, mL/h | Calculated Ratio VPA:PNA | ||||
|---|---|---|---|---|---|---|
| Minimum | Maximum | |||||
| Omegaflex special | 79 | 119 | 5:5 | 7:3 | 4:6 | 6:4 |
| Lipoflex special | 79 | 119 | 5:5 | 7:3 | 4:6 | 6:4 |
| Kabiven | 75 | 182 | 5:5 | 7:3 | 3:7 | 5:5 |
| SmofKabiven | 82 | 140 | 5:5 | 7:3 | 4:6 | 6:4 |
| Omegaflex peri | 78 | 175 | 5:5 | 6:4 | 3:7 | 5:5 |
| Kabiven Peripheral | 80 | 259 | 5:5 | 7:3 | 3:7 | 4:6 |
| Lipoflex peri | 78 | 175 | 5:5 | 7:3 | 3:7 | 5:5 |
| Olimel Peri N4E | 104 | 224 | 5:5 | 6:4 | 3:7 | 4:6 |
| Sodium valproate solutions | 88.2 | 176.4 | - - - | |||
| PNA | pH ± SD | Turbidity ± SD (NTU) | Osmolality ± SD (mOsm/kgH2O) | Zeta Potential ± SD (mV) | MDD ± SD (nm) | PDI ± SD |
|---|---|---|---|---|---|---|
| Omegaflex special | 5.58 ± 0.01 | 0.328 ± 0.025 | 1925.00 ± 0.00 | −11.70 ± 0.53 | 249.27 ± 3.25 | 0.096 ± 0.009 |
| Lipoflex special | 5.51 ± 0.01 | 0.133 ± 0.004 | 1972.00 ± 0.00 | −8.35 ± 0.55 | 267.27 ± 3.76 | 0.102 ± 0.024 |
| Kabiven | 5.57 ± 0.01 | 0.169 ± 0.009 | 1044.00 ± 0.00 | −10.60 ± 0.46 | 277.67 ± 1.96 | 0.116 ± 0.008 |
| SmofKabiven | 5.53 ± 0.01 | 0.169 ± 0.009 | 1596.00 ± 0.00 | −12.00 ± 0.44 | 240.37 ± 2.73 | 0.106 ± 0.011 |
| Omegaflex peri | 5.48 ± 0.01 | 0.118 ± 0.001 | 903.00 ± 0.00 | −15.07 ± 0.61 | 244.80 ± 2.91 | 0.112 ± 0.008 |
| Lipoflex peri | 5.74 ± 0.01 | 0.091 ± 0.001 | 938.15 ± 6.36 | −14.47 ± 0.59 | 257.40 ± 0.70 | 0.092 ± 0.017 |
| Kabiven Peripheral | 5.63 ± 0.01 | 0.180 ± 0.025 | 808.00 ± 0.00 | −15.03 ± 0.51 | 267.50 ± 0.95 | 0.120 ± 0.018 |
| Olimel Peri N4E | 6.45 ± 0.01 | 0.140 ± 0.002 | 846.00 ± 0.00 | −17.20 ± 0.17 | 257.33 ± 1.45 | 0.111 ± 0.019 |
| PNA | VPA Solution in 5% Glucose | VPA Solution in 0.9% NaCl | |||||||
|---|---|---|---|---|---|---|---|---|---|
| t1 = 0 h | t2 = 4 h | t1 = 0 h | t2 = 4 h | ||||||
| Omegaflex special | 4:6 | 241.2 ± 4.6 | 243.5 ± 3.2 | 239.9 ± 2.6 | 243.0 ± 2.6 | ||||
| 5:5 | 239.7 ± 3.6 | 241.3 ± 1.4 | 242.2 ± 1.6 | 241.9 ± 1.0 | |||||
| 7:3 | 241.8 ± 8.9 | 247.4 ± 1.3 | 238.3 ± 4.8 | 240.3 ± 0.4 | |||||
| Lipoflex special | 4:6 | 264.0 ± 7.8 | + | 257.8 ± 1.0 | 259.5 ± 1.4 | 258.1 ± 1.8 | |||
| 5:5 | 262.1 ± 4.8 | + | 261.0 ± 1.0 | 262.6 ± 2.7 | 259.0 ± 2.7 | ||||
| 7:3 | 255.3 ± 6.9 | + | 258.4 ± 3.1 | 256.7 ± 3.8 | 254.0 ± 2.9 | + | |||
| Kabiven | 3:7 | 277.1 ± 2.8 | + | 279.8 ± 3.8 | + | 277.8 ± 4.3 | 276.4 ± 3.9 | ||
| 5:5 | 275.0 ± 1.8 | + | 276.6 ± 5.1 | + | 274.6 ± 5.3 | + | 273.9 ± 2.7 | + | |
| 7:3 | 274.5 ± 2.5 | + | 277.6 ± 4.0 | + | 276.6 ± 6.1 | + | 277.0 ± 3.9 | + | |
| SmofKabiven | 4:6 | 231.5 ± 2.4 | 236.2 ± 6.0 | 236.3 ± 3.6 | 243.8 ± 2.9 | + | |||
| 5:5 | 235.5 ± 3.2 | 237.6 ± 6.2 | 234.9 ± 4.5 | + | 234.3 ± 2.9 | + | |||
| 7:3 | 242.8 ± 8.1 | 234.6 ± 1.6 | 232.2 ± 1.8 | 234.8 ± 5.2 | |||||
| Omegaflex peri | 4:6 | 246.2 ± 3.8 | 249.2 ± 2.4 | 248.2 ± 4.4 | 248.2 ± 0.8 | ||||
| 5:5 | 249.4 ± 1.9 | 241.5 ± 2.4 | 249.4 ± 4.9 | 246.5 ± 3.0 | |||||
| 7:3 | 242.5 ± 1.8 | 247.8 ± 0.7 | 242.5 ± 3.9 | 243.7 ± 5.1 | |||||
| Lipoflex peri | 3:7 | 261.4 ± 2.5 | 257.1 ± 3.6 | 259.3 ± 3.4 | 254.4 ± 1.6 | ||||
| 5:5 | 257.6 ± 2.6 | 257.0 ± 2.4 | + | 256.3 ± 2.1 | 252.8 ± 2.8 | ||||
| 6:4 | 258.5 ± 1.3 | 256.0 ± 1.2 | + | 256.5 ± 1.2 | 255.2 ± 2.1 | ||||
| Kabiven Peripheral | 3:7 | 269.0 ± 5.0 | + | 269.3 ± 1.9 | 268.1 ± 2.9 | 267.5 ± 0.7 | |||
| 5:5 | 266.9 ± 1.6 | + | 272.0 ± 3.4 | 270.6 ± 5.2 | + | 267.9 ± 1.6 | + | ||
| 7:3 | 272.0 ± 2.1 | + | 274.1 ± 2.2 | + | 263.4 ± 2.0 | + | 274.5 ± 2.0 | + | |
| Olimel Peri N4E | 3:7 | 263.0 ± 5.0 | 257.4 ± 1.7 | 258.3 ± 5.1 | 257.1 ± 4.7 | ||||
| 5:5 | 256.1 ± 3.3 | + | 254.9 ± 3.9 | 261.1 ± 6.1 | + | 258.4 ± 5.4 | + | ||
| 6:4 | 266.9 ± 4.9 | + | 258.9 ± 3.1 | + | 257.2 ± 3.4 | 255.3 ± 4.7 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piwowarczyk, L.; Tomczak, S.; Antkowiak, P.; Jelińska, A.; Stawny, M. Sodium Valproate Incompatibility with Parenteral Nutrition Admixtures—A Risk to Patient Safety: An In Vitro Evaluation Study. Pharmaceutics 2022, 14, 371. https://doi.org/10.3390/pharmaceutics14020371
Piwowarczyk L, Tomczak S, Antkowiak P, Jelińska A, Stawny M. Sodium Valproate Incompatibility with Parenteral Nutrition Admixtures—A Risk to Patient Safety: An In Vitro Evaluation Study. Pharmaceutics. 2022; 14(2):371. https://doi.org/10.3390/pharmaceutics14020371
Chicago/Turabian StylePiwowarczyk, Ludwika, Szymon Tomczak, Patryk Antkowiak, Anna Jelińska, and Maciej Stawny. 2022. "Sodium Valproate Incompatibility with Parenteral Nutrition Admixtures—A Risk to Patient Safety: An In Vitro Evaluation Study" Pharmaceutics 14, no. 2: 371. https://doi.org/10.3390/pharmaceutics14020371