1. Introduction
Oral drug performance is dependent on oral drug bioavailability, the rate and extent of the drug reaching the systemic circulation unchanged. In addition to gut and hepatic metabolism, gastrointestinal (GI) absorption is a key factor influencing oral drug bioavailability. GI absorption is influenced by multiple factors, such as the extent and rate of drug dissolution, the formation of drug insoluble complexes, drug decomposition, and regional changes in drug permeability [
1]. Only the drug that is in solution will be absorbed, and thus the magnitude of dissolved drug concentrations in the lumen influences the rate and extent of drug absorption [
1]. Drug solubility in GI fluids dictates the upper concentration limit. Both intrinsic (e.g., anatomical, physiological) and extrinsic (e.g., nutritional) age-related changes affect the composition of GI fluids, which will ultimately impact drug solubility in the GI tract of pediatric patients [
2]. There is a high rate of change in these intrinsic and extrinsic factors in the youngest subpopulations, especially during the first months of life [
2].
The Biopharmaceutics Classification System (BCS) classifies drugs into four categories according to their solubility and permeability [
3]. Drugs are assigned to one of the following categories: BCS class I (high solubility, high permeability), BCS class II (low solubility, high permeability), BCS class III (high solubility, low permeability) and BCS class IV (low solubility, low permeability). Over the years, the BCS has proved useful in several stages of adult drug development. For BCS class II and IV compounds, oral drug absorption will be limited by drug solubility. Age-related differences in GI fluids of pediatric patients in comparison to adults can affect drug solubility, and thus, alterations in drug performance can occur [
4].
In the recent literature, the need for a Pediatric Biopharmaceutics Classification System (pBCS) has been highlighted [
2]; its development will allow for a more simplistic way of understanding possible changes in oral drug performance in pediatrics. However, due to insufficient knowledge concerning the influence of growth and maturation on the GI tract, the establishment of a pBCS has not been possible so far.
According to the adult BCS, drugs are classified as highly soluble if the highest dose strength is soluble in 250 mL (or less) of aqueous liquid at a relevant physiological pH range of 1.2–6.8 [
2,
5,
6]. Several issues arise concerning drug solubility classification within pediatrics, which include: (i) defining the highest single dose, (ii) Defining the initial gastric volume that is available upon drug arrival, and (iii) Establishing the luminal solubility of the drug; all of these factors vary amongst pediatric subpopulations, hindering the development of a pBCS [
2,
5,
6].
Concerning drug permeability classification, drugs are classified as highly permeable when the extent of oral absorption (i.e., the fraction of dose absorbed) is greater than 85% of the administered dose [
2,
5,
6]. If not available, correlations between in vivo and in vitro measurements of permeability are generally used, such as in vitro cell lines including Caco-2, or MDCK, as well as in silico models based on logP or logD data [
4]. Due to the controversial nature of using adult permeability data for pediatric subjects, and the scarcity of information on permeability in newborns and infants, establishing meaningful permeability criteria for these subpopulations has not yet been possible [
2,
5,
6].
The heterogeneity of the pediatric population poses another hurdle in the establishment of a pBCS, where balance is needed to develop a simple tool that discriminates the several pediatric subpopulations as much as possible. While such a tool remains to be developed, extrapolation of the adult BCS classification should be performed with care. The risk of using the BCS adult classification in pediatric drug development lies in possible shifts in the BCS classification of drugs due to alterations in the rate-limiting step of absorption resulting from growth and maturation [
7]. For example, BCS class I and III drugs are eligible for the submission of BCS-based biowaivers to regulatory agencies, such as the European Medicines Agency (EMA) and the United States Food and Drug Administration (FDA). Therefore, extrapolation of drug product bioequivalence, in specific cases, can be based on in vitro dissolution experiments [
4,
6]. If age-related physiological and/or anatomical changes are responsible for shifts in the BCS classification as a result of differences in drug solubility and/or permeability classification, the BCS biowaiver status of a certain compound can be impacted for pediatrics.
In the field of biopharmaceutics, biorelevant media that simulate the composition of GI contents in adults are commonly used. Recently, age-specific biorelevant media have been proposed for newborns (0–28 days) and infants (1–12 months) [
4]. The solubility of seven poorly water-soluble compounds was assessed in pediatric and adult biorelevant media to understand the impact of developmental differences in GI fluid composition on drug solubility.
This study aimed to understand drug solubilization as a function of age, and identify drugs at risk of altered drug solubility between newborns and young infants and adults. The solubility of seven drugs was assessed in adult and pediatric age-specific biorelevant media, in the fasted and fed state gastrointestinal (GI) simulated conditions. The characteristics of the investigated model drugs were restricted to include poorly water-soluble compounds, with a variety of physicochemical properties, and with documented usage in pediatrics and adults. Partial least squares regression (PLS-R) was used to evaluate the influence of drugs’ physicochemical properties and the composition of gastrointestinal fluids, as well as their interactions, on the pediatric-to-adult solubility ratio (Sp/Sa (%)).
2. Materials and Methods
2.1. Materials
Ultra-high-temperature-treated whole cow’s milk standardized to less than 4% of fat was acquired from Sainsbury’s, UK. The formula milk used in all experiments was First Infant Milk (cow’s milk-based formula) (Cow & Gate, Trowbridge, UK), and Wysoy (soy-based formula) (SMA-Nestlé, Gatwick, UK). Trifluoroacetic acid (TFA) (high-performance liquid chromatography (HPLC) grade), dimethyl sulfoxide (DMSO), sodium hydroxide, 37% hydrochloric acid, sodium chloride, sodium acetate trihydrate, ammonium acetate (HPLC grade), phosphate buffer salt, acetonitrile (I) (HPLC grade) and methanol (MeOH) (HPLC grade) were purchased from Fisher Scientific (UK). Montelukast sodium, mebendazole, mesalazine, sodium oleate, pepsin (from porcine), formic acid, maleic acid, dialysis tubing (12–14,000 Da molecular weight (MW) cut-off) and ammonium phosphate were obtained from Sigma-Aldrich Company Ltd., UK. Naproxen, amiodarone hydrochloride, nitrofurantoin and dipyridamole were obtained from VWR International, LLC. Water was ultra-pure (Milli-Q) laboratory grade. Sodium taurocholate (Prodotti Chimici Alimentari S.P.A., Basaluzzo, Italy), egg lecithin Lipoid EPCS (Lipoid GmbH, Ludwigshafen am Rhein, Germany) and glyceryl monooleate-Rylo Mg 19 (Danisco, Brabrand, Denmark) were obtained from the specified sources. Polytetrafluoroethylene (PTFE) filters (13 mm, 0.45 μm) were purchased from Fisher Scientific (Loughborough, UK).
2.2. Instrumentation
The equipment utilized in the investigation included a Buchi R114 Rotavapor (Switzerland), a Beckman Coulter J2-MC centrifuge (High Wycombe, UK), a pH meter (Mettler Toledo InLab Expert Pro-ISM, Schwerzenbach, Switzerland), a shaking water bath (model Grant SS40-2, Grant Instruments, UK), and a vortex mixer Rotamixer (East Grinstead, UK). HPLC analysis was performed using a Hewlett Packard Series 1100 system equipped with an autosampler, a temperature-regulated column compartment, a quaternary pump and a diode array detector (DAD) (Agilent Technologies, Santa Clara, CA, USA)
2.3. Drugs
The solubility of seven poorly water-soluble compounds (BCS class II and IV) was investigated, including three weak bases (dipyridamole, mebendazole and amiodarone), two amphoteric compounds (mesalazine and montelukast), and two weak acids (nitrofurantoin and naproxen). The physicochemical properties of the model drugs used are presented in
Table 1.
The obtained results were combined with values from a previous study, where solubility in pediatric and adult media was obtained for seven additional poorly water-soluble compounds (neutral: griseofulvin, spironolactone, carbamazepine, and fenofibrate; weak acids: phenytoin and indomethacin; weak base: dapsone) [
4].
2.4. Solubility Studies
Adult and pediatric biorelevant media were prepared according to Maharaj et al. [
4]. Solubility experiments were performed using the shake flask method, in a shaking water bath (37 °C, 200 strokes/min) [
4]. All solubility assessments were conducted in triplicate. An excess of the solid drug was used to saturate the volume of the medium used. In aqueous-based media (i.e., adult fasted state simulated gastric fluids (FaSSGF), adult fasted state simulated intestinal fluids (FaSSIF-V2) and adult fasted state simulated intestinal fluids (FeSSIF-V2)), experiments were conducted with 2 mL of medium in centrifuge tubes, and samples were collected at 24 h, media samples were filtered through 0.45 μm PTFE filters, diluted with fresh media and injected into the HPLC. For all the test drugs, filter adsorption studies were performed before the solubility measurements. Negligible drug adsorption to the filters used was observed (% drug adsorbed did not exceed 2%). In all media containing milk products (i.e., adult fed state simulated gastric fluids (FeSSGF)), the membrane dialysis technique was used to separate the undissolved drug. In this case, excess solid was added to the outside of the dialysis membrane. Experiments using milk-based media were conducted in 15 mL centrifuge tubes with 5 mL of the respective medium outside the membrane and 1 mL inside of the membrane. For sample collection, tubes were taken from the water bath, the dialysis membrane was removed, and its contents were collected at 48 h [
4]. A longer dwell period was used for milk-based samples to ensure that the solubility results were not limited by drug diffusion through the dialysis membrane. After collection, the milk-based media solubility samples (media within the membrane) were immediately centrifuged in 1500 µL plastic centrifugation tubes (8000 rpm for 15 min at 4 °C). In this process, 1000 µL of extraction solvent (methanol for all drugs, except for mebendazole and nitrofurantoin, for which DMSO was used, and mesalazine, for which 0.01 % TFA was used) was added to 500 µL of the supernatant. The mixture was vortexed for 1 min and centrifuged at 8000 rpm for 15 min at 4 °C. The supernatant was filtered through a 0.45 µm PTFE filter and injected into the HPLC.
2.5. Chromatographic Conditions for the Analysis of the Solubility Samples
Solubility samples were quantified using high-performance liquid chromatography with an ultraviolet detector (HPLC-UV). Analytical HPLC procedures were based on modifications of methods depicted in the literature and are denoted in
Table 1. All calibration curves for aqueous-based media (FaSSGF, FaSSIF-V2, and FeSSIF-V2) were prepared with five standard concentrations created as mobile phase dilutions of a concentrated stock solution of the drug dissolved in a compatible organic solvent. Milk-based media standards were prepared in the same conditions as samples (i.e., created by dilution of the drug stock solution with fresh medium and treated as previously described). Stock solutions were prepared in methanol, except for mebendazole and nitrofurantoin, which were prepared in DMSO, and mesalazine, which was prepared in a solution of methanol:water with 0.01% TFA (5:95).
2.6. Treatment of In Vitro Solubility Data
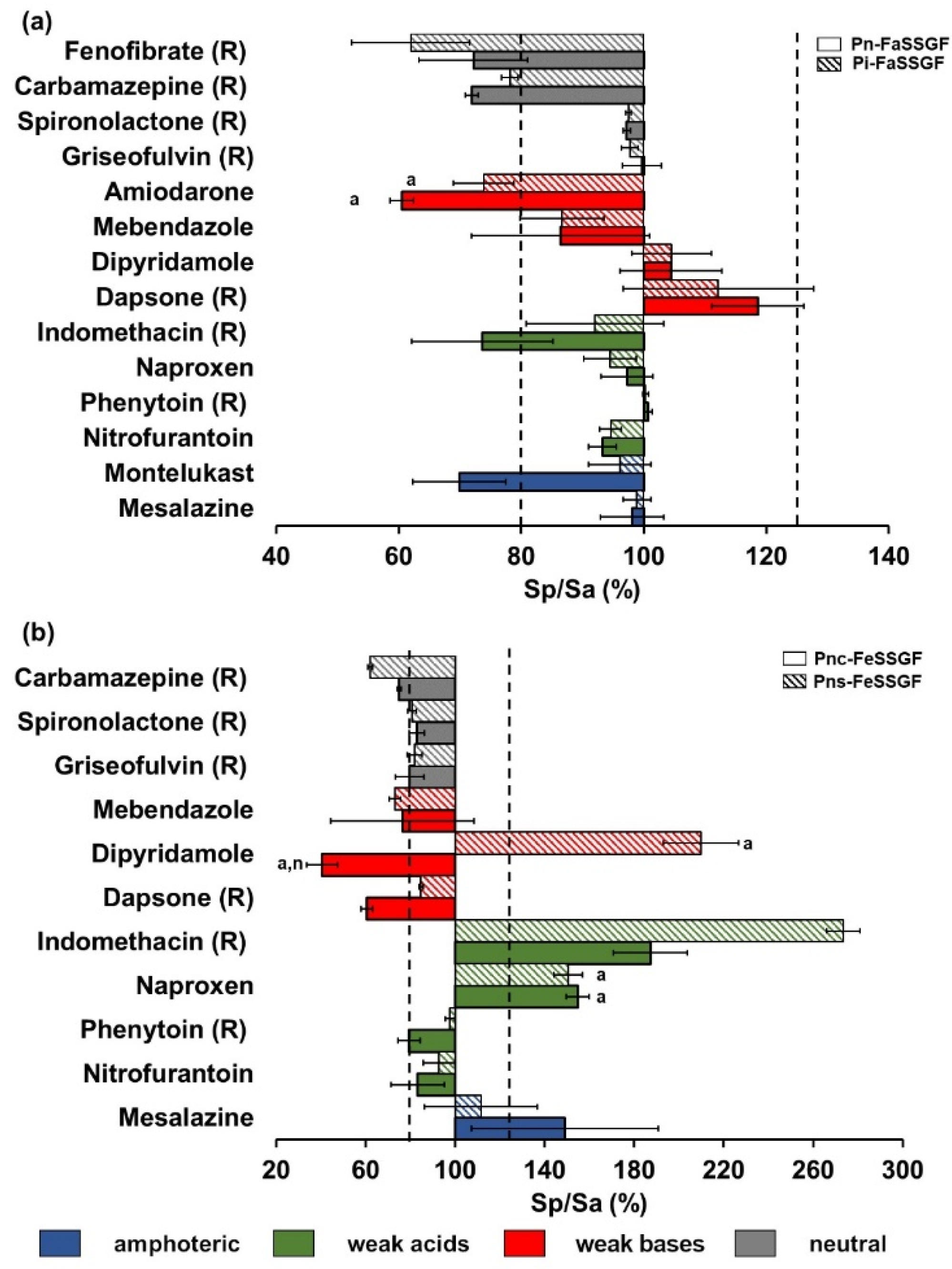
Drug solubility differences between using pediatric media and the corresponding reference adult media were expressed as a ratio % (Sp/Sa (%)), where Sp is the solubility in each pediatric medium and Sa is the solubility in respective adult medium. Sp/Sa (%) values lower than 100% represent lower drug solubility in pediatric media when compared to adult reference media, and Sp/Sa (%) values higher than 100% represent the opposite. To denote relevant discrepancies in solubility between adults and pediatrics, biopharmaceutic risk assessment limits corresponding to reference values of 80 and 125% were set. Sp/Sa (%) ratios outside these limits were considered at a higher risk of altered drug performance between pediatric and adult patients.
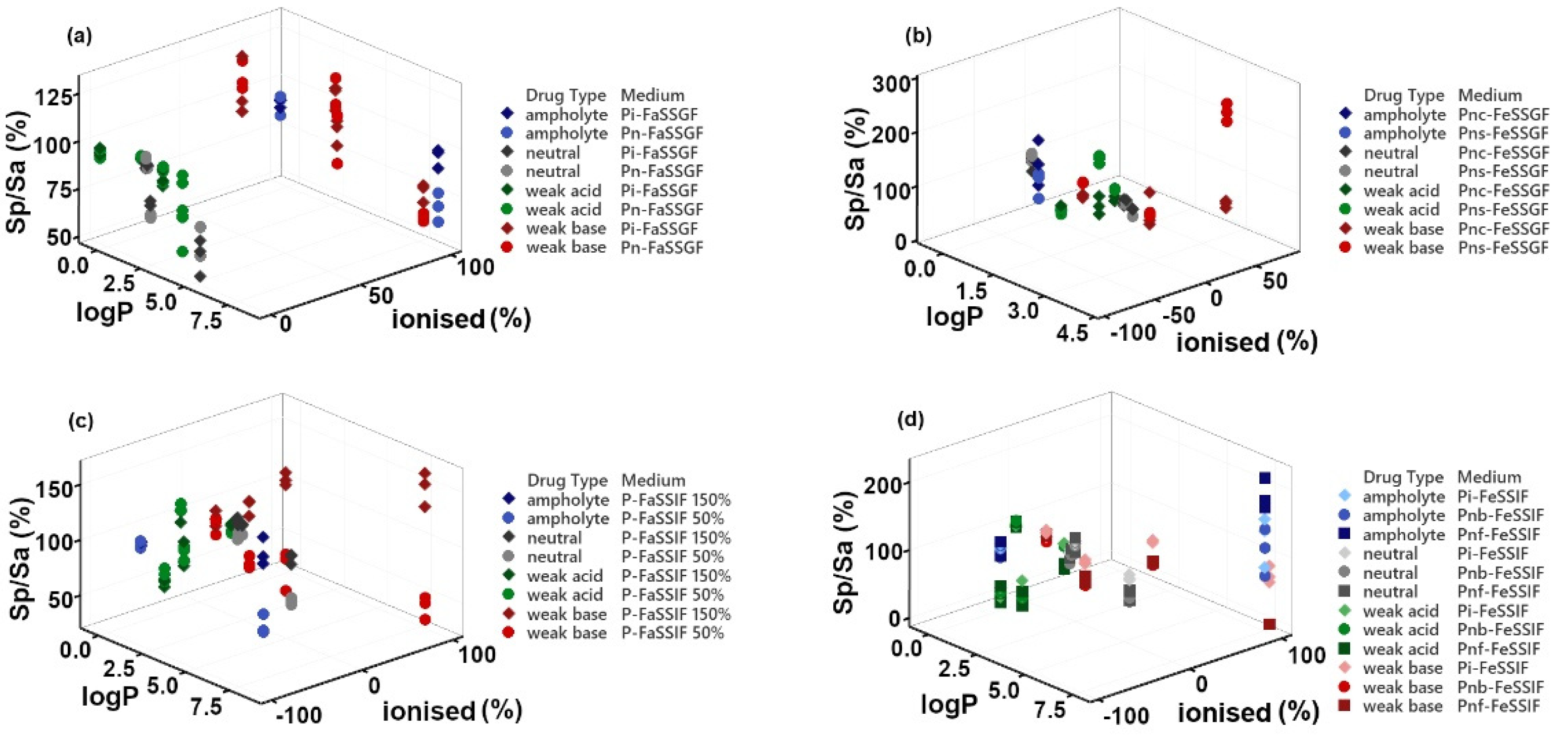
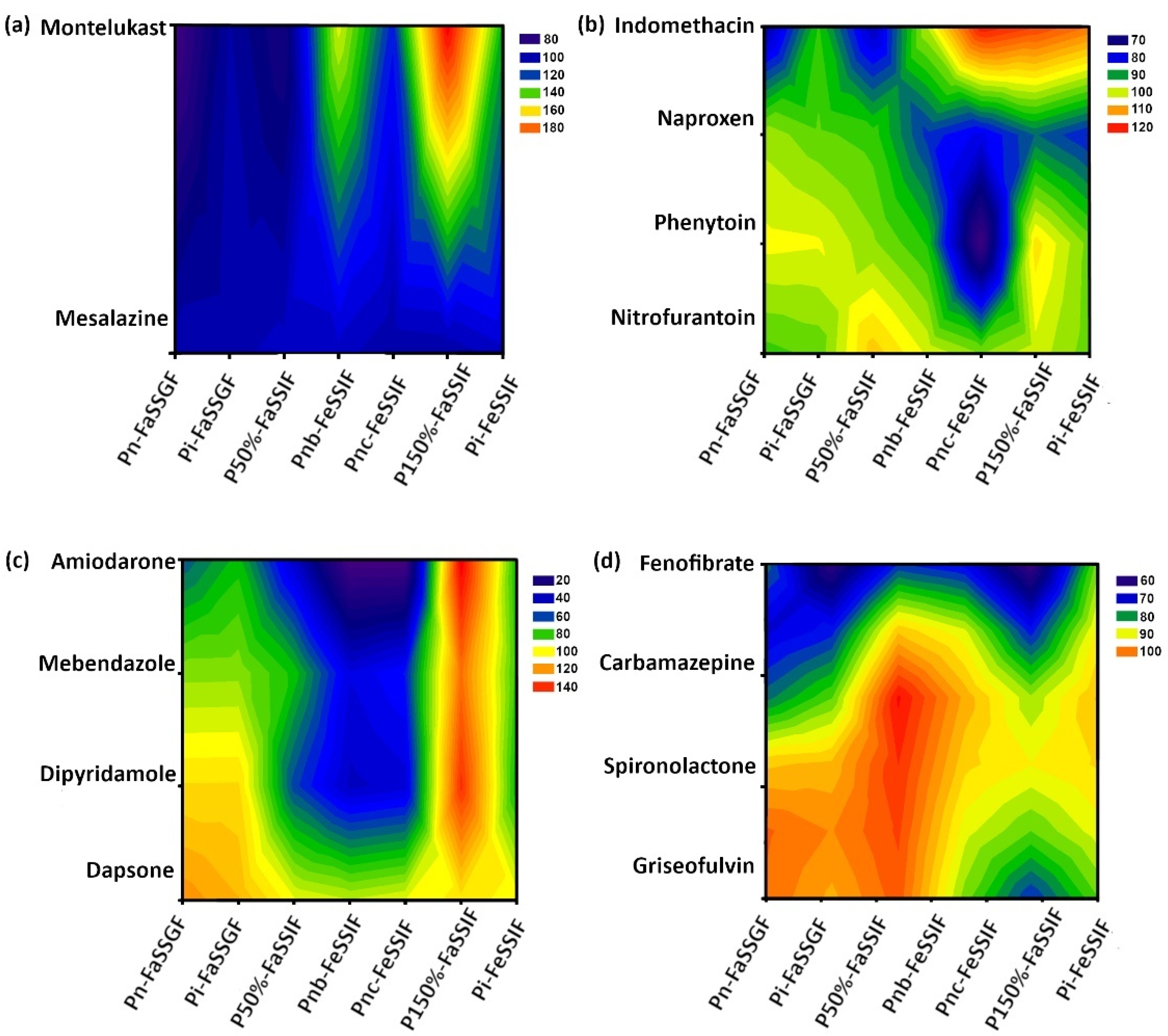
Graphs comparing the pediatric-to-adult drug solubility ratio in biorelevant media (Sp/Sa (%)) ± SD were constructed in Microsoft Excel 2016, Office 365® (Microsoft, London, UK). For the correlation of drugs’ physicochemical properties and solubility ratio (Sp/Sa (%)), 3D scatter plots and contour plots were generated. The 3D scatter plots conveyed Sp/Sa (%) as a function of logP and ionized (%), and were constructed using Minitab® 19.2020.1 (©2020 Minitab, LLC, Coventry, UK). The contour plots portraying drug Sp/Sa (%) as a function of drugs logP and medium bile salts concentrations were generated using SigmaPlot 13.0 (SystatSoftware Inc., Slough, UK).
2.7. Statistical Analysis
All statistical evaluations were performed with XLSTAT® add-in (Addinsoft, New York, USA) for Microsoft Excel 2016, Office 365® (Microsoft, London, UK).
One-way analysis of variance (ANOVA) with a post hoc Tukey’s multiple comparisons test was performed to assess statistical significance between drug solubility in each set of simulated fluids (i.e., neonate, infant and adult FaSSGF, etc.) using a significance level of p ≤ 0.05.
Partial least squares regression (PLS-R) analysis was performed due to its ability to deal with collinearity between independent variables [
24]. Sp/Sa (%) was set as the response variable for the PLS-R analysis. Explanatory variables were set as drugs’ physicochemical properties (i.e., logP, ionized (%) (positive value for compounds with a basic pKa, and a negative value for compounds with an acidic pKa, obtained from ACD/Labs
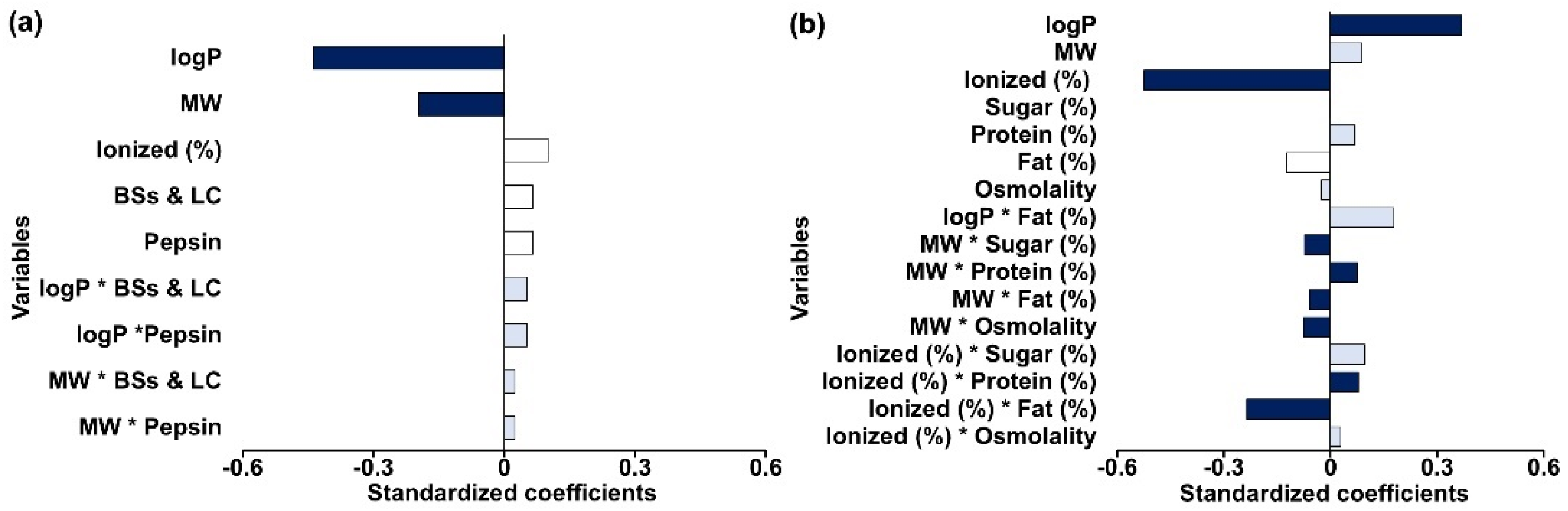
© 2022–2018), and MW), changes in media components when comparing between pediatric and adult biorelevant media (i.e., pepsin, bile salts, lecithin, sodium oleate, glyceryl monooleate, fat (%), sugar (%), protein (%), etc.), and interactions between the medium and drug individual variables. A schematic of the independent variables and interaction terms used for each model is presented in
Figure 1.
Composite variables (combination of two or more individual variables) were used when the ratio of the individual components for each of the composite variables was maintained throughout each pediatric medium. The influence of “bile salts and lecithin (BSs and LC)” was evaluated as a composite variable comprised of sodium taurocholate (NaTC) and lecithin concentrations, and the variable “fat products” was set to represent concentrations of sodium oleate and glyceryl monooleate. The PLS-R analysis was conducted for the seven compounds investigated in this study and for an additional seven compounds investigated in a previous study [
4]. The PLS-R regression generates components based on the defined independent variables to explain the response [
25]. The number of components will be lower than the initial independent variables selected for the PLS-R models. The PLS-R components are built iteratively so that they explain as well as possible the variability of Y (also known as the response and dependent variable). The model quality was evaluated based on the square of the coefficient of determination (R
2) and goodness of prediction (Q
2), where R
2 and Q
2 close to 1 represent good model fit and high predictive power, respectively [
26]. The number of principal components for each model was selected based on the model’s optimum Q
2 value and predicted residual error sum of squares (PRESS) [
24,
25,
27]. A Q
2 value higher than 0.5 is considered acceptable for good model predictability [
26]. The PLS-R was built and evaluated based on full cross-validation (leave-one-out procedure). Independent variables were considered to have an impact on the response if variable importance in projection (VIP) values were higher than 1.0, whereas 0.7–1.0 values were regarded as important (i.e., moderate impact), and values lower than 0.7 were generally regarded as insignificant [
24,
25,
27]. Standardized coefficients were generated for each independent variable and selected interactions. These coefficients were related to the independent variables and the response variance and were normalised for the variation of Y. The normalisation of the coefficients was accomplished by dividing the non-standardized coefficient value obtained for each independent variable by its respective standard deviation (SD) [
25]. In the PLS-R analysis, the generation of standardized coefficients allowed the comparison between variables within a model but not between different models [
25]. Outliers in the analyses were identified by means of the comparison of the distance of each observation to the model in the Y-plane (DModY) with their calculated critical value (DCrit(Y)); an outlier was present if the standardized DCritY for an observation was greater than DCritY [
28,
29,
30]. Outliers were only excluded if (i) the PLS model improved significantly after exclusion and (ii) there was a clear scientific rational on why the data should be excluded (i.e., why the current models would not be able to explain the results).
4. Discussion
Differences in drug solubilization between pediatric and adult biorelevant media were observed in the fasted and fed state gastrointestinal conditions. Of the compounds investigated in this study (n = 7), nitrofurantoin (weak acid, logP −0.47) was the only one for which solubility differences between pediatric and adult biorelevant media were within the 80–125% risk assessment limits for all pediatric media tested. Additionally, no significant solubility differences were found between adults and pediatrics. These results are probably related to nitrofurantoin’s low lipophilicity (logP = −0.47) and its acidic pKa of 7.2, meaning that it is primarily non-ionized in all the biorelevant media tested.
For the fasted gastric state, a trend was identified for solubility ratios (Sp/Sa (%)) lower than 100%, which is in accordance with what was previously found [
4]. The solubility differences in the fasted state gastric media seemed to be related to compound lipophilicity, as three of the compounds that show the highest differences have a logP > 5 (fenofibrate, montelukast and amiodarone). These observations are further confirmed by the PLS-R analysis which showed that logP and MW were the most important factors responsible for solubility differences between pediatric and adult media (
Figure 6). The fact that these variables display a negative effect on Sp/Sa (%) indicates that there is a potential risk for reduced drug solubility of high lipophilic/high MW compounds in the younger pediatric patients. Note that the fasted gastric model accounted for a low degree of variability of the response (R
2 = 0.37) and showed limited predictive power (Q
2 = 0.25), therefore, caution is granted for interpretation of the results.
For the fed gastric state, drug lipophilicity and ionization were shown to have a significant effect on the solubility differences between pediatric and adult fluids (
Figure 6b) (7). Drug lipophilicity has previously been shown to play a role in the prominence of the impact of pH changes on drug solubility [
32,
33,
34]. Taking into account that solubility is highly driven by pH changes and that the pediatric fed gastric media is the only set of media with differences in pH when compared to the respective adult medium, changes in drug solubility in these media are expected to be more significant for ionized compounds. In the PLS-R analysis, a significant effect of ionized (%) on the Sp/Sa (%) (positive or negative) is related to the ionization properties of the compound (weak acidic/weak basic pKa). For example, in the fed gastric state, higher differences between solubility in adults and pediatrics were observed for weak acids (specifically naproxen and indomethacin). For the majority of the weak bases, the opposite trend was observed; however, for dipyridamole (logP 2.74), a significantly higher solubility in Pns-FeSSGF (medium containing soy formula) and a significantly lower solubility in Pnc-FeSSGF (medium containing cow’s milk formula) were observed when compared to adult solubility in FeSSGF. Dipyridamole solubility in fed gastric pediatric media suggests that drugs might exhibit distinct affinities for infant cow’s milk or soy formula due to small differences in their composition, such as protein type, protein content, sugar content, and fat content. This observation is supported by the PLS-R results, which show for example that the interaction of drug ionized (%) and the protein and fat medium composition is a significant factor affecting Sp/Sa (%). The results from the statistical analysis show that differences in the composition between different types of milk products (e.g., formula, cow’s milk) can affect the solubility of drugs in GI fluids. Infant formula is developed to closely represent breast milk concerning the proportions of energy provided by macronutrients (proteins, fats and carbohydrates); however, differences with regard to fat (e.g., individual components of the lipid system such as triglycerides and phospholipids), protein type (whey and casein protein from milk vs. protein concentrate from soy), and whey to casein ratios of protein can be observed [
4]. In this study, Wysoy
® by SMA
® and First Infant Milk by Cow & Gate
® were used as soy-based formula and cow’s milk-based formula, respectively, although protein content is similar for both formulas (1.8 g and 1.3 g per 100 mL of prepared formula, respectively), the type of protein is different. While the soy-based formula is composed of soy protein isolate, in cow’s milk-based formula, whey (0.8 g) and casein proteins (0.5 g) are present. Furthermore, while total carbohydrate content is similar (6.9 g in soy-based formula and 7.2 g in the cow-based formula), only 2.5 g of sugar is present in Wysoy
® compared to 7.2 g of sugar in First Infant Milk
®, of which 7.0 g is lactose. It should be noted that lactose is not present in Wysoy
®.
In this study, the use of equilibrium dialysis for amiodarone (logP = 7.90) and montelukast (logP = 8.79) was challenging, and the results are not presented. Amiodarone and montelukast are extremely lipophilic (logP 7.6 and 8.8, respectively), with high MW (645 and 586, respectively), and also show high binding to plasma proteins (~97% and ~99%, respectively, according to ACD/I-Lab©, 2010–2018 ACD/Labs). Drug separation by equilibrium dialysis was also found to be ineffective in the previous study by Maharaj et al. [
4]. For fenofibrate, a compound with very similar characteristics, and for which hemodialysis is considered inefficacious [
4], if the drug is highly bound to the milk proteins and fat globules, this could limit the diffusion of the solubilized drug through the membrane. Limitations of equilibrium dialysis have previously been reported during drug release studies [
35,
36]. Drug adsorption to the dialysis membrane has also been reported as a limiting factor of this technique [
37]. Most of these issues could be potentially resolved if enough time is given for diffusion to occur; however, because this study aimed to compare results between drugs, it was key that the dwell period was the same for all drugs.
In the fasted intestinal state, higher differences were found between pediatric media and the corresponding adult medium for the most lipophilic of the investigated compounds (montelukast, amiodarone and fenofibrate, for which logP is between 5 and 8). Sp/Sa (%) for 5 out of the 14 investigated compounds were outside the biopharmaceutical risk assessment limits. It appears that weak bases were the compounds most prone to be affected by changes in the concentrations of BSs and LC. The statistical analysis confirmed this interpretation and showed that BSs and LC is the only individual variable influencing solubility differences (positive impact). Additionally, interactions between BSs and LC and drug properties contribute towards defining the extent and magnitude of observed drug solubility changes. Drug lipophilicity, MW and ionization showed a positive impact on Sp/Sa (%), and therefore with higher BSs and LC concentrations and ionizable drugs with high logP or high MW, higher solubility ratios are expected (i.e., increased drug solubility in pediatric media in comparison to drug solubility in adult media).
Sp/Sa (%) in fed state intestinal fluids showed values lower than 100% for all drugs, except montelukast. For this drug, a trend for higher Sp/Sa (%) was observed in all pediatric FeSSIF, although only the solubility in Pnc-FeSSIF was significantly different from adults (
p ≤ 0.05). This is probably related to the fact that pediatric media contain a smaller amount of sodium chloride, and therefore the solubility results are probably related to a common-ion effect, since montelukast sodium was used in the experiments [
38]. Pnc-FeSSIF medium simulates newborns intestinal conditions following feeding with cow’s milk formula, which contains the highest content of fat digestion products (sodium oleate and glyceryl monooleate); this can most likely explain the higher solubility of montelukast (logP = 8.8) in comparison to the remaining fed state intestinal media.
The results of this study suggest that weak bases are at a higher risk of altered drug solubility in fasted and fed intestinal fluids, as shown by the impact of ionization as a single variable and/or the interaction of ionized drugs with BSs and LC. Additionally, logP and MW were also critical in modulating pediatric solubility either as individual variables or as interactions with BSs and LC. The results observed in the fasted and fed intestinal PLS-R analyses (positive effect of BSs and LC on drug solubility changes between adults and pediatrics) are in agreement with previous literature reports where the concentration of physiologically relevant surfactants (i.e., sodium oleate, bile salt and lecithin) were revealed to be more important than other components of biorelevant media, such as salt, buffer, and pancreatin, in modulating solubility in both fasted and fed intestinal fluids [
32,
33,
34]. In accordance with this, Mithani et al. previously showed that the solubilization effect of bile salts (NaTC) increases with increasing drug lipophilicity, and that logP and MW can be used as a surrogate for predicting solubility as a function of bile salts concentrations [
39]. Drug MW was selected as an independent variable in the models (
Figure 7) for the investigation of drugs’ physicochemical properties, due to its relationship with the volume/space that the drug occupies, which can influence the way it will solubilize into micelles [
40]. Even though drug logP and MW often display collinearity, they represent different properties of a molecule. For example, during dissolution studies, drug diffusion through a medium containing micelles will be influenced by the molecular weight of the drug, where larger drug-micelle complexes will migrate slower [
41].
Due to the nature of the compounds selected for this study (poorly water-soluble, BCS class II and IV), age-related changes in drug solubility are more likely to play a role in influencing drug absorption. For BCS class II compounds, absorption is highly influenced by the solubility and the rate of drug dissolution in the GI fluids. While drug solubility will define the upper limit of absorption, it can also affect the drug dissolution rate. A decrease in drug solubility in pediatric GI fluids can result in a lower amount of drug available for absorption, which might result in differences in oral bioavailability. To conclude on the therapeutic impact of these results, changes in drug solubility should be considered alongside the remaining factors that have the potential to affect absorption, including drug substance and formulation properties (i.e., dose administered, type of formulation, excipients present, and others), as well as physiological factors (i.e., gastric emptying, small intestinal transit times, intestinal surface area, and others). Age-appropriate in vitro drug dissolution studies with an appropriate pediatric dose and age-appropriate biorelevant dissolution conditions should also be performed in the future to further understand the impact of age-related factors not only on drug solubilization, but also on drug dissolution rate and extent. The incorporation of pediatric simulated GI fluid solubility and dissolution into physiologically based pharmacokinetic (PBPK) models offers the opportunity to mechanistically understand drug product behavior in vivo.


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}