
Practical Recommendations for the Manipulation of Kinase Inhibitor Formulations to Age-Appropriate Dosage Forms
 ,
, 
Abstract
:1. Introduction
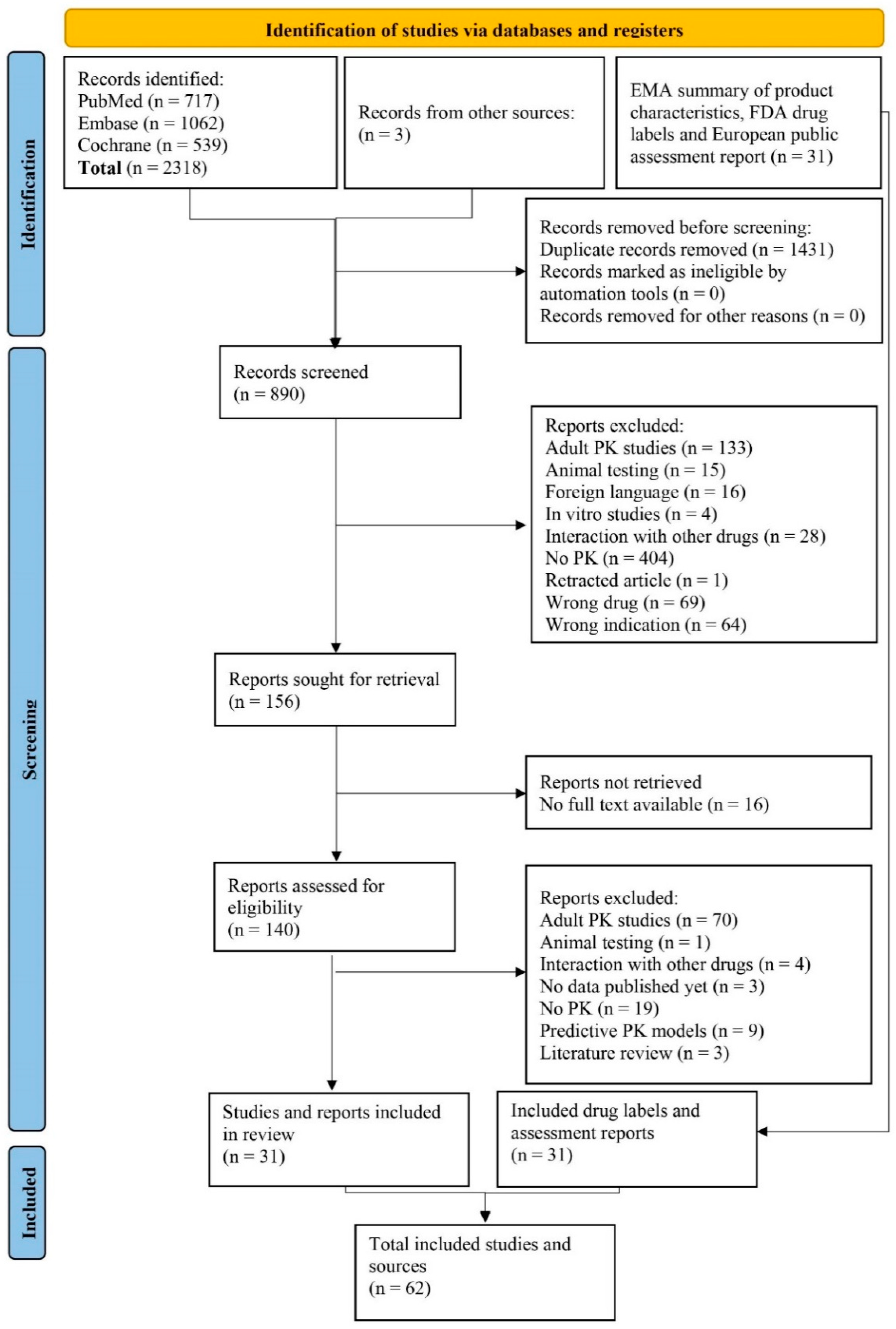
2. Methods
2.1. Literature Analysis
2.2. Providing Practical Recommendations
3. Results
3.1. Phase I/II Study Results
3.2. LoE 1 Recommendation (Larotrectinib, Dasatinib, Imatinib, Ruxolitnib)
3.3. LoE 2 Recommendation (Sunitinib)
3.4. LoE 3 Recommendation
3.5. LoE 4 Recommendation (Dabrafenib, Bosutinib, Crizotinib, Trametinib)
3.5.1. Dabrafenib and Trametinib
3.5.2. Bosutinib
3.5.3. Crizotinib
3.6. LoE 5 Recommendations (Cobimetinib, Ruxolitinib, Cabozantinib, Dabrafenib, Imatinib, Ponatinib, Bosutinib, Crizotinib, Entrectinib, Nilotinib, Selumetinib, Trametinib)
3.7. BCS Class I: Cobimetinib and Ruxolitinib
3.7.1. Cobimetinib
3.7.2. Ruxolitinib
3.8. BCS Class II and IV
3.8.1. Trametinib
3.8.2. Ponatinib and Imatinib
4. Relevant Additional Recommendations
4.1. Therapeutic Drug Monitoring
4.2. Administration Via Enteral Feeding Tube
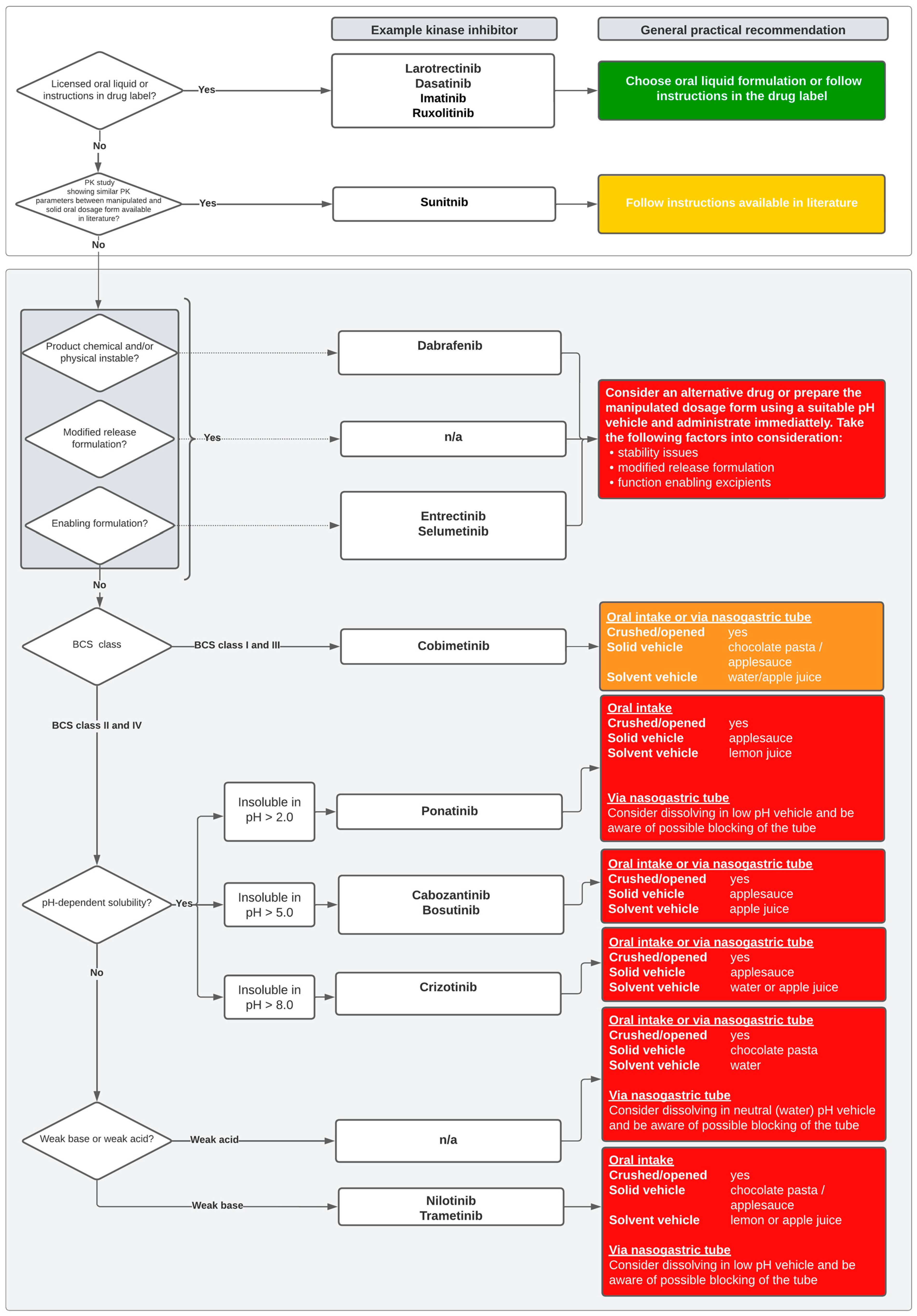
5. The Decision Tool
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Terms and Definitions
| Term | Definition |
| Oral liquid formulation | A pediatric oral liquid formulation available on the drug market, provided by the pharmaceutical company |
| Formulation manipulation | Change in (oral) drug formulation (e.g., crushing of tablets, opening of capsules, dissolving content in a vehicle) that is needed in clinical practice but is not described in the drug label |
| BCS class | System to categorize drugs according to their permeability and solubility [95] BCS class I: high solubility, high permeability BCS class II: low solubility, high permeability BCS class III: high solubility, low permeability BCS class IV: low solubility, low permeability |
| Solubility | The minimum solubility of the drug across a pH range from 1 to 8 and at a temperature of 37 ± 0.5 °C. High-solubility drugs are those with a ratio of dose to solubility volume that is less than or equal to 250 mL [95] |
| Permeability | The effective human jejunal wall permeability of a drug. High-permeability drugs are generally those with an extent of absorption greater than or equal to 90% and are not associated with any documented instability in the gastrointestinal tract [95] |
| Bioavailability | The extent and rate at which an active pharmaceutical ingredient (API) is absorbed in the systemic circulation and available at the site of drug action [95]. This is dependent upon the AUC, Cmax and Tmax of a medicinal product |
| Bioequivalence | The term bioequivalence was introduced to ensure safety and efficacy and comparable in vivo performance of two medicinal products containing the same active substance. Bioequivalence between two medicinal products is assumed when the bioavailability (determined by a plasma concentration curve from which AUC, Cmax and Tmax can be calculated) is between 80% and 125% of the reference medicinal product. This is investigated in a bioequivalence or bioavailability study that meet the requirements of the study design described in the EMA or FDA bioequivalence guidelines and, as a main goal, investigates bioequivalence between two medicinal products containing the same active substance [9,10] |
| Similar PK parameters | Similar PK parameters (i.e., AUC and Cmax) of the manipulated oral dosage form that are within 80–125% of the solid oral dosage form. This is typically shown in a PK study that as a main outcome calculated PK parameters and investigated treatment outcomes (such as toxicity and response) of an solid oral dosage form and as a secondary outcome included PK parameter calculations of manipulated oral dosage forms but do not meet the requirements of EMA or FDA bioequivalence guidelines [9,10] |
| BCS = Biopharmaceutics Classification System; AUC = area under the curve; Cmax = maximum plasma concentration; EMA = European Medical Agency; FDA = U.S. Food and Drug Administration; PK = pharmacokinetics. | |
Appendix A
Appendix A.1. General Search
Appendix A.2. Drug Formulation Search
Appendix B

Appendix C

{kind=link}
{kind=link}
{kind=link}
| TKI | Tradename | Dosage Form | Excipients 1 (Function) | |
|---|---|---|---|---|
| Tablet Core or Capsule Content | Tablet Film Coating or Capsule Shell | |||
| BCS class I | ||||
| Cobimetinib | Cotellic® (Roche) | Immediate release film-coated tablet 20 mg | Lactose monohydrate (diluent, compression) Microcrystalline cellulose (E460) (diluent) Croscarmellose sodium (E468) (binder, disintegrant) Magnesium stearate (E470b) (lubricant) | Polyvinyl alcohol Titanium dioxide (E171) Macrogol 3350 Talc (E553b) |
| Ruxolitinib | Jakavi® (Novartis Pharma) | Immediate release film-coated tablet 5, 10, 15, 20 mg | Microcrystalline cellulose (diluent) Magnesium stearate (lubricant) Silica, colloidal anhydrous (glidant) Sodium starch glycolate (Type A) (disintegrant) Povidone K30 (binder) Hydroxypropylcellulose 300 to 600 cps (binder) Lactose monohydrate(diluent, direct compression excipient) | na |
| Larotrectinib | Vitrakvi® (Bayer) | Immediate release hard capsule 25, 100 mg | na | Gelatin (shell) Titanium dioxide (E 171) (colourant) |
| Oral solution 20 mg/mL | Purified water (solution base) Sucrose (suspending, sweetening agent) Hydroxypropylbetadex (?) Glycerol (E 422) (sweetening, antimicrobial preservative, solvent) Sorbitol (E 420) (sweetening agent) Sodium citrate (E 331) (emulsyfing agent) Sodium dihydrogen phosphate dihydrate (E 339) (buffer?) Citric acid (E 330) (buffer agent. antioxidant) Propylene glycol (E 1520) (solvent) Potassium sorbate (E 202) (solvent) Methyl parahydroxybenzoate (E 218) (antimicrobial preservative) Citrus fruit flavor (flavor) Natural flavor (flavor) | na | ||
| BCS class II | ||||
| Cabozantinib | CabometyxTM (Ipsen Farmaceutica) | Immediate release film-coated tablet 20, 40, 60 mg | Microcrystalline cellulose (diluent) Anhydrous lactose (diluent, compression excipient) Hydroxypropyl cellulose (disintegrant, binder) Croscarmellose sodium (disintegrant) Colloidal anhydrous silica (disintegrant) Magnesium stearate (lubricant) | Hypromellose 2910 Titanium dioxide (E171) Triacetin Iron oxide yellow (E172) |
| Cometriq® (Ipsen Farmaceutica) | Immediate release hard capsule 20, 80 mg | Microcrystalline cellulose (diluent) Croscarmellose sodium (disintegrant) Sodium starch glycolate (disintegrant) Silica colloidal anhydrous (glidant) Stearic acid (lubricant) | Gelatin Black iron oxide (E172) (20 mg capsules only) Red iron oxide (E172) (80 mg capsules only) Titanium dioxide (E171) | |
| Dabrafenib | Tafinlar® (Novartis Pharma) | Immediate release capsule 50, 75 mg | Microcrystalline cellulose (diluent) Magnesium stearate (lubricant) Colloidal silicone dioxide (glidant) | Hypromellose (E464) Red iron oxide (E172) Titanium dioxide (E171) |
| Dasatinib | Sprycel® (Bristol-Meyers Squibb)2 | Immediate release film-coated tablet 20, 50, 70, 80, 100, 140 mg | Lactose monohydrate (diluent) Microcrystalline cellulose (diluent) Croscarmellose sodium (disintegrant) Hydroxypropylcellulose (disintegrant, binder) Magnesium stearate (lubricant) | Hypromellose Titanium dioxide (E171) Macrogol 400 |
| Powder for suspension 10 mg/mL | Sucrose (suspending agent, sweetening, viscosity increasing agent) Carmellose sodium (viscosity increasing agent, adsorbent, emulsifying agent, suspending agent) Simethicone emulsion consisting of: simeticone, polyethylene glycol sorbitan tristearate, polyethoxylate stearate, glycerides, methylcellulose, xanthan gum, benzoic acid, sorbic acid, sulfuric acid. Tartaric acid Trisodium citrate anhydrous Sodium benzoate (E211) Silica hydrophobic colloidal Mixed berry flavour [containing benzyl alcohol, sulphur dioxide (E220)] | na | ||
| Imatinib | Glivec® (Novartis Pharma)2 | Immediate release hard capsule 100 mg | Cellulose microcrystalline (diluent, compression agent) Crospovidone (lubricant, dispersing, solubilizing agent) Magnesium stearate (lubricant) Silica colloidal, anhydrous (disintegrant) | Gelatin Iron oxide, red (E172) Iron oxide, yellow (E172) Titanium dioxide (E171) |
| Immediate release film-coated tablets 100, 400 mg | Cellulose microcrystalline (diluent) Crospovidone (disintegrating, solubilizing) Hypromellose (binder, solubilizing) Magnesium stearate (lubricant) Silica, colloidal anhydrous(disintegrant) | Iron oxide, red (E172) Iron oxide, yellow (E172) Macrogol Talc Hypromellose | ||
| Ponatinib | Iclusig® (Incyte Biosciences) | Immediate release film-coated tablet 15, 30, 45 mg | Lactose monohydrate (diluent, compression excipient) Microcrystalline cellulose (diluent) Sodium starch glycolate (disintegrant) Colloidal anhydrous silica (disintegrant) Magnesium stearate (lubricant) | Talc Macrogol 4000 Poly(vinyl alcohol) Titanium dioxide (E171) |
| BCS class IV | ||||
| Bosutinib | Bosulif® (Pfizer) | Immediate release film-coated tablet 100, 400, 500 mg | Microcrystalline cellulose (E460) (diluent, compression agent) Croscarmellose sodium (E468) (disintegrant) Poloxamer 188 (binder, solubilizing agent) Povidone (E1201) (binder) Magnesium stearate (E470b) (lubricant) | Polyvinyl alcohol Titanium dioxide (E171) Macrogol 3350 Talc (E553b) Iron oxide yellow (E172) (100 and 400 mg only) Iron oxide red (E172) (400 and 500 mg tablet only) |
| Crizotinib | Xalkori® (Pfizer) | Immediate release hard capsule 200, 250 mg | Colloidal anhydrous silica (disintegrant) Microcrystalline cellulose (diluent) Anhydrous calcium hydrogen phosphate (lubricant) Sodium starch glycolate (Type A) (disintegrant) Magnesium stearate (lubricant) | Gelatin Titanium dioxide (E171) Red iron oxide (E172) |
| Entrectinib | Rozlytrek® (Roche) | Immediate release hard capsule 100, 200 mg | Tartaric acid (acidulant) Lactose (Diluent, compression agent) Hypromellose (binder, dispersing agent, solubilizing agent) Crospovidone (disintegrant, solubilizing agent) Microcrystalline cellulose (diluent) Colloidal anhydrous silica (disintegrant) Magnesium stearate (lubricant) | Hypromellose Titanium dioxide (E171) Yellow iron oxide (E172—100 mg hard capsule) Sunset yellow FCF (E110—200 mg hard capsule) |
| Nilotinib | Tasigna® (Novartis Pharma) | Immediate release hard capsule 50, 150, 200 mg | Lactose monohydrate (diluent, compression agent) Crospovidone Type A (disintegrant, solubilizing agent) Poloxamer 188 (lubricant, solubilizing agent) Colloidal anhydrous silica (disintegrant) Magnesium stearate(lubricant) | Gelatin Titanium dioxide (E171) Red iron oxide (E172) (50 mg capsule only) Yellow iron oxide (E172) |
| Selumetinib | Koselugo® (AstraZeneca) | Immediate release hard capsule 10, 25 mg | Vitamin E polyethylene glycol succinate (D α-tocopheryl polyethylene glycol succinate) (solubilizing agent, binder) | Hypromellose (E464) Carrageenan (E407) Potassium chloride (E508) Titanium dioxide (E171) Carnauba wax (E903)Indigo carmine aluminium lake (E132) (25 mg capsule only) Iron oxide yellow (E172) (25 mg capsule only) |
| Sunitinib | Sutent® (Pfizer) 2 | Immediate release hard capsule 12.5, 25, 37.5, 50 mg | Mannitol (E421) (diluent) Croscarmellose sodium (binder, disintegrant) Povidone (K-25) (solubilizing agent, disintegrant) Magnesium stearate (lubricant) | Gelatin Red iron oxide (E172) Titanium dioxide (E171) Yellow iron oxide (E172) (25, 37.5, 50 mg capsule only) Black iron oxide (E172) (25, 50 mg capsule only) |
| Trametinib | Mekinist® (Novartis Pharma) | Immediate release film-coated tablet 0.5, 2 mg | Mannitol (E421) (diluent) Microcrystalline cellulose (E460) (diluent) Hypromellose (E464) (binder, solubilizing agent) Croscarmellose sodium (E468) (binder, disintegrant) Magnesium stearate (E470b) (lubricant) Sodium laurilsulfate (lubricant, solubilizing agent) Colloidal silicon dioxide(E551) (disintegrant) | Hypromellose (E464) Titanium dioxide (E171) Polyethylene glycol Iron oxide yellow(E172) (0.5 mg tablet only) Polysorbate 80 (E433) (2 mg tablet only) Iron oxide red (E172) (2 mg tablet only) |
Appendix D
| TKI | Study Design 1 | No. of Patients | Age Range (Years) | Tested Drug Formulations | Similar PK Parameters Demonstrated? | Refs |
|---|---|---|---|---|---|---|
| BCS class I | ||||||
| Cobimetinib | - | - | - | - | - | - |
| Larotrectinib | Phase 1 PK study | 24 | 0–18 | Capsules and oral liquid formulation 2 | Yes, between capsule and oral liquid 2 | [63] |
| Ruxolitinib | Phase 1 PK study | 49 | 2–21 | Tablets and m.d.f 3 (i.e., crushed tablets or added to apple sauce or OraPlus) | No | [69] |
| BCS class II | ||||||
| Cabozantinib | Phase 1 PK study | 41 | 4–18 | Tablets | - | [70] |
| Dabrafenib | Phase 1 PK study | 27 | 0–17 | Capsules and oral liquid formulation 2 (i.e., oral suspension) | No | [71] |
| Dasatinib | Phase 1 PK study | 39 | 2–20 | Tablet, capsules and m.d.f 3 (i.e., crushed/dissolved in lemonade, apple or orange juice) | No | [72,73,74] |
| Phase 1 PK study | 25 | 2–17 | ||||
| Phase 1 PK study | 58 | 0–21 | ||||
| Imatinib | Phase 1 PK study | 31 | 3–20 | Tablets, capsules and m.d.f 3 (i.e., opened or dissolved in water or apple juice) | No | [53,54,55,56,57,75] |
| Phase I PK study | 24 | 3–21 | ||||
| Phase II PK study | 24 | 2–18 | ||||
| Phase II PK study | 71 | 3–29 | ||||
| Phase II PK study | 19 | 2–18 | ||||
| PK study | 36 | 2–22 | ||||
| Ponatinib | - | - | - | - | - | - |
| BCS class IV | ||||||
| Bosutinib | - | - | - | - | - | - |
| Crizotinib | Phase 1 PK study | 79 | 1–20 | Capsules and oral liquid formulation 2 (i.e., powder in a bottle, powder in capsule or oral liquid) | No | [58,59,60] |
| Phase 1 PK study | 75 | 2–22 | ||||
| Phase 1 PK study | 25 | 2–21 | ||||
| Entrectinib | - | - | - | - | - | - |
| Nilotinib | PK study | 15 | 5–17 | Capsules or sprinkled over apple sauce | No | [61] |
| Selumetinib | Phase 1 PK study | 24 | 3–18 | Capsules, tablets | No | [62,64,65] |
| Phase 1 PK study | 38 | 5–20 | ||||
| Phase II PK study | 50 | 3–20 | ||||
| Sunitinib | Phase 1 PK study | 23 | 3–20 | Capsule or m.d.f 3 (i.e., opened and sprinkled over yoghurt or applesauce) | Yes, between capsule and manipulated oral dosage form | [39,66,67,68] |
| Phase 1 PK study | 12 | 4–21 | ||||
| Phase II PK study | 30 | 3–20 | ||||
| Phase I/II PK study | 6 | 13–16 | ||||
| Trametinib | - | - | - | - | - | - |
References
- Juárez-Hernández, J.E.; Carleton, B.C. Paediatric oral formulations: Why don’t our kids have the medicines they need? Br. J. Clin. Pharmacol. 2022, 88, 4337–4348. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.; Cross, D.; Jänne, P.A. Kinase drug discovery 20 years after imatinib: Progress and future directions. Nat. Rev. Drug Discov. 2021, 20, 551–569. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.; Adams, V.; Overley, C. Alternate dosage formulations of oral targeted anticancer agents. J. Oncol. Pharm. Pract. 2021, 27, 1963–1981. [Google Scholar] [CrossRef] [PubMed]
- Bellantoni, A.J.; Wagner, L.M. Pursuing precision: Receptor tyrosine kinase inhibitors for treatment of pediatric solid tumors. Cancers 2021, 13, 3531. [Google Scholar] [CrossRef] [PubMed]
- Lejman, M.; Kusmierczuk, K.; Bednarz, K.; Ostapińska, K.; Zawitkowska, J. Targeted Therapy in the Treatment of Pediatric Acute Lymphoblastic Leukemia—Therapy and Toxicity Mechanisms. Int. J. Mol. Sci. 2021, 22, 9827. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, H.K.; Marriott, J.F. Formulations for children: Problems and solutions. Br. J. Clin. Pharmacol. 2015, 79, 405–418. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.S.H. Extemporaneous compounding of oral liquid dosage formulations and alternative drug delivery methods for anticancer drugs. Pharmacotherapy 2011, 31, 164–192. [Google Scholar] [CrossRef]
- Herbrink, M.; Nuijen, B.; Schellens, J.H.M.; Beijnen, J.H. Variability in bioavailability of small molecular tyrosine kinase inhibitors. Cancer Treat. Rev. 2015, 41, 412–422. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline on the Investigation of Bioequivalence. 2010. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-bioequivalence-rev1_en.pdf (accessed on 13 October 2022).
- FDA. Guidance for Industry: Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs—General Considerations. Center for Drug Evaluation and Research: Silver Spring, MD, USA, 2014; p. 24. [Google Scholar]
- Martir, J.; Flanagan, T.; Mann, J.; Fotaki, N. Recommended strategies for the oral administration of paediatric medicines with food and drinks in the context of their biopharmaceutical properties: A review. J. Pharm. Pharmacol. 2017, 69, 384–397. [Google Scholar] [CrossRef] [Green Version]
- Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 1 January 2022).
- EMA. Assessment Report Cotellic. 2015. Available online: https://www.ema.europa.eu/en/documents/assessment-report/cotellic-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Imatinib. 2012. Available online: https://www.ema.europa.eu/en/documents/assessment-report/imatinib-teva-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Iclusig. 2013. Available online: https://www.ema.europa.eu/en/documents/assessment-report/iclusig-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Koselugo. 2021. Available online: https://www.ema.europa.eu/en/documents/assessment-report/koselugo-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Cabometyx. 2016. Available online: https://www.ema.europa.eu/en/documents/assessment-report/cabometyx-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Cometriq. 2013. Available online: https://www.ema.europa.eu/en/documents/assessment-report/cometriq-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. SmPC Ponatinib. Available online: https://www.ema.europa.eu/en/documents/product-information/iclusig-epar-product-information_en.pdf (accessed on 7 July 2022).
- EMA. Assessment Report Jakavi. 2012. Available online: https://www.ema.europa.eu/en/documents/assessment-report/jakavi-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Mekinist. 2014. Available online: https://www.ema.europa.eu/en/documents/assessment-report/mekinist-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Xalkori. 2012. Available online: https://www.ema.europa.eu/en/documents/assessment-report/xalkori-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. SmPC Nilotinib. Available online: https://www.ema.europa.eu/en/documents/product-information/tasigna-epar-product-information_nl.pdf (accessed on 28 October 2022).
- EMA. SmPC Ruxolitinib. Available online: https://www.ema.europa.eu/en/documents/product-information/jakavi-epar-product-information_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Tasigna. 2017. Available online: https://www.ema.europa.eu/en/documents/variation-report/tasigna-h-c-798-x-0088-g-epar-assessment-report-variation_en.pdf (accessed on 1 January 2022).
- EMA. SmPC Sunitinib. Available online: https://www.ema.europa.eu/en/documents/product-information/sutent-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMA. SmPC Trametinib. Available online: https://www.ema.europa.eu/en/documents/product-information/mekinist-epar-product-information_nl.pdf (accessed on 28 October 2022).
- EMA. SmPC Crizotinib. Available online: https://www.ema.europa.eu/en/documents/product-information/xalkori-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMA. SmPC Entrectinib. Available online: https://www.ema.europa.eu/en/documents/product-information/rozlytrek-epar-product-information_en.pdf (accessed on 7 July 2022).
- EMA. SmPC Dabrafenib. Available online: https://www.ema.europa.eu/en/documents/product-information/tafinlar-epar-product-information_en.pdf (accessed on 7 July 2022).
- EMA. SmPC Imatinib. Available online: https://www.ema.europa.eu/en/documents/product-information/glivec-epar-product-information_en.pdf (accessed on 7 July 2022).
- EMA. SmPC Cobimetinib. Available online: https://www.ema.europa.eu/en/documents/product-information/cotellic-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMA. SmPC Bosutinib. Available online: https://www.ema.europa.eu/en/documents/product-information/bosulif-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMA. SmPC Cabozantinib. Available online: https://www.ema.europa.eu/en/documents/product-information/cabometyx-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMC. SmPC Sprycel 10 mg/ml. Available online: https://www.medicines.org.uk/emc/product/10228/smpc#gref (accessed on 1 February 2022).
- EMA. Assessment Report Sprycel. 2018. Available online: https://www.ema.europa.eu/en/documents/variation-report/sprycel-h-c-000709-x-0056-g-epar-assessment-report-variation_en.pdf (accessed on 1 February 2022).
- EMC. SmPC Vitrakvi 20 mg/mL. Available online: https://www.medicines.org.uk/emc/product/10766/smpc#gref (accessed on 7 July 2022).
- FDA. Drug Label Ruxolitinib. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/202192s023lbl.pdf (accessed on 20 February 2022).
- Dubois, S.G.; Shusterman, S.; Reid, J.M.; Ingle, A.M.; Ahern, C.H.; Baruchel, S.; Glade-Bender, J.; Ivy, P.; Adamson, P.C.; Blaney, S.M. Tolerability and pharmacokinetic profile of a sunitinib powder formulation in pediatric patients with refractory solid tumors: A Children’s Oncology Group study. Cancer Chemother. Pharmacol. 2012, 69, 1021–1027. [Google Scholar] [CrossRef]
- Sistla, A.; Sunga, A.; Phung, K.; Koparkar, A.; Shenoy, N. Powder-in-Bottle Formulation of SU011248. Enabling Rapid Progression into Human Clinical Trials. Drug Dev. Ind. Pharm. 2004, 30, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Tamai, K.; Nagata, K.; Otsuka, K.; Nakagawa, A.; Tachikawa, R.; Otsuka, K.; Katakami, N.; Tomii, K. Crizotinib administered via nasogastric and percutaneous endoscopic gastrostomy tubes for the successful treatment of ALK-rearranged lung cancer in a patient with poor performance status. Respir. Investig. 2013, 51, 46–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, D.S.; Allred, A.; Zhou, Y.; Infante, J.R.; Gordon, M.S.; Bendell, J.; Jones, S.; Burris, H.; Orford, K. Relative bioavailability of pediatric oral solution and tablet formulations of trametinib in adult patients with solid tumors. Clin. Pharmacol. Drug Dev. 2015, 4, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Mamdouhi, T.; Vagrecha, A.; Johnson, A.A.; Levy, C.F.; Atlas, M.; Krystal, J.I. Successful use of crushed formulation of dabrafenib and trametinib in a pediatric glioneural tumor. Pediatr. Blood Cancer 2021, 68, 28–29. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Imamura, C.K.; Shimada, H.; Katayama, D.; Urabe, K.; Suzuki, R.; Takitani, K.; Ashida, A. Pharmacokinetics, efficacy and safety of bosutinib in a pediatric patient with chronic myeloid leukemia. J. Pediatr. Pharmacol. Ther. 2020, 25, 742–745. [Google Scholar] [CrossRef]
- Marangon, E.; Citterio, M.; Sala, F.; Barisone, E.; Lippi, A.A.; Rizzari, C.; Biondi, A.; D’Incalci, M.; Zucchetti, M. Pharmacokinetic profile of imatinib mesylate and N-desmethyl-imatinib (CGP 74588) in children with newly diagnosed Ph+ acute leukemias. Cancer Chemother. Pharmacol. 2009, 63, 563–566. [Google Scholar] [CrossRef]
- Tanimura, K.; Yamasaki, K.; Okuhiro, Y.; Hira, K.; Nitani, C.; Okada, K.; Fujisaki, H.; Matsumoto, K.; Hara, J. Monitoring Ponatinib in a Child with Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia. Case Rep. Oncol. 2021, 14, 24–28. [Google Scholar] [CrossRef]
- EMA. Assessment Report Rozlytrek. 2020. Available online: https://www.ema.europa.eu/en/documents/assessment-report/rozlytrek-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Vitrakvi. 2019. Available online: https://www.ema.europa.eu/en/documents/assessment-report/vitrakvi-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. SmPC Selumetinib. Available online: https://www.ema.europa.eu/en/documents/product-information/koselugo-epar-product-information_en.pdf (accessed on 28 October 2022).
- EMA. Assessment Report Bosulif. 2013. Available online: https://www.ema.europa.eu/en/documents/assessment-report/bosulif-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Sunitinib. 2020. Available online: https://www.ema.europa.eu/en/documents/assessment-report/sunitinib-accord-epar-public-assessment-report_en.pdf (accessed on 1 January 2022).
- EMA. Assessment Report Tafinlar. 2013. Available online: https://www.ema.europa.eu/en/documents/assessment-report/tafinlar-epar-public-assessment-report_en.pdf (accessed on 1 February 2022).
- Calafiore, L.; Amoroso, L.; Della Casa alberighi, O.; Luksch, R.; Zanazzo, G.; Castellano, A.; Podda, M.; Dominici, C.; Haupt, R.; Corrias, M.V.; et al. Two-stage phase II study of imatinib mesylate in subjects with refractory or relapsing neuroblastoma. Ann. Oncol. 2013, 24, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Pollack, I.F.; Jakacki, R.I.; Blaney, S.M.; Hancock, M.L.; Kieran, M.W.; Phillips, P.; Kun, L.E.; Friedman, H.; Packer, R.; Banerjee, A.; et al. Phase I trial of imatinib in children with newly diagnosed brainstem and recurrent malignant gliomas: A Pediatric Brain Tumor Consortium report. Neuro. Oncol. 2007, 9, 145–160. [Google Scholar] [CrossRef] [Green Version]
- Champagne, M.A.; Capdeville, R.; Krailo, M.; Qu, W.; Peng, B.; Rosamilia, M.; Therrien, M.; Zoellner, U.; Blaney, S.M.; Bernstein, M. Imatinib mesylate (STI571) for treatment of children with Philadelphia chromosome-positive leukemia: Results from a Children’s Oncology Group phase 1 study. Blood 2004, 104, 2655–2660. [Google Scholar] [CrossRef]
- Bond, M.; Bernstein, M.L.; Pappo, A.; Schultz, K.R.; Krailo, M.; Blaney, S.M.; Adamson, P.C. A Phase II Study of Imatinib Mesylate in Children With Refractory or Relapsed Solid Tumors: A Children’s Oncology Group Study. Pediatr. Blood Cancer 2008, 50, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Baruchel, S.; Sharp, J.R.; Bartels, U.; Hukin, J.; Odame, I.; Portwine, C.; Strother, D.; Fryer, C.; Halton, J.; Egorin, M.J.; et al. A Canadian paediatric brain tumour consortium (CPBTC) phase II molecularly targeted study of imatinib in recurrent and refractory paediatric central nervous system tumours. Eur. J. Cancer 2009, 45, 2352–2359. [Google Scholar] [CrossRef]
- Broniscer, A.; Jia, S.; Mandrell, B.; Hamideh, D.; Huang, J.; Onar-Thomas, A.; Gajjar, A.; Raimondi, S.C.; Tatevossian, R.G.; Stewart, C.F. Phase 1 trial, pharmacokinetics, and pharmacodynamics of dasatinib combined with crizotinib in children with recurrent or progressive high-grade and diffuse intrinsic pontine glioma. Pediatr. Blood Cancer 2018, 65, e27035. [Google Scholar] [CrossRef] [PubMed]
- Mossé, Y.P.; Lim, M.S.; Voss, S.D.; Wilner, K.; Ruffner, K.; Laliberte, J.; Rolland, D.; Balis, F.M.; Maris, J.M.; Weigel, B.J.; et al. Safety and activity of crizotinib for paediatric patients with refractory solid tumours or anaplastic large-cell lymphoma. Lancet Oncol. 2013, 14, 472–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balis, F.M.; Thompson, P.A.; Mosse, Y.P.; Blaney, S.M.; Minard, C.G.; Weigel, B.J.; Fox, E. First-dose and steady-state pharmacokinetics of orally administered crizotinib in children with solid tumors: A report on ADVL0912 from the Children’s Oncology Group Phase 1/Pilot Consortium. Cancer Chemother. Pharmacol. 2017, 79, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hijiya, N.; Michel Zwaan, C.; Rizzari, C.; Foà, R.; Abbink, F.; Lancaster, D.; Landman-Parker, J.; Millot, F.; Moppett, J.; Nelken, B.; et al. Pharmacokinetics of nilotinib in pediatric patients with Philadelphia chromosome–positive chronic myeloid leukemia or acute lymphoblastic leukemia. Clin. Cancer Res. 2020, 26, 812–820. [Google Scholar] [CrossRef]
- Fangusaro, J.; Onar-Thomas, A.; Young Poussaint, T.; Wu, S.; Ligon, A.H.; Lindeman, N.; Banerjee, A.; Packer, R.J.; Kilburn, L.B.; Goldman, S.; et al. Selumetinib in paediatric patients with BRAF-aberrant or neurofibromatosis type 1-associated recurrent, refractory, or progressive low-grade glioma: A multicentre, phase 2 trial. Lancet Oncol. 2019, 20, 1011–1022. [Google Scholar] [CrossRef]
- Laetsch, T.W.; DuBois, S.G.; Mascarenhas, L.; Turpin, B.; Federman, N.; Albert, C.M.; Nagasubramanian, R.; Davis, J.L.; Rudzinski, E.; Feraco, A.M.; et al. Larotrectinib for paediatric solid tumors harbouring NTKR gene fusions: A multicentre, open-label, phase 1 study. Lancet Oncol. 2018, 19, 705–714. [Google Scholar] [CrossRef]
- Banerjee, A.; Jakacki, R.I.; Onar-Thomas, A.; Wu, S.; Nicolaides, T.; Young Poussaint, T.; Fangusaro, J.; Phillips, J.; Perry, A.; Turner, D.; et al. A phase i trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: A Pediatric Brain Tumor Consortium (PBTC) study. Neuro Oncol. 2017, 19, 1135–1144. [Google Scholar] [CrossRef] [Green Version]
- Dombi, E.; Baldwin, A.; Marcus, L.J.; Fisher, M.J.; Weiss, B.; Kim, A.; Whitcomb, P.; Martin, S.; Aschbacher-Smith, L.E.; Rizvi, T.A.; et al. Activity of Selumetinib in Neurofibromatosis Type 1–Related Plexiform Neurofibromas. N. Engl. J. Med. 2016, 375, 2550–2560. [Google Scholar] [CrossRef]
- Verschuur, A.C.; Bajčiová, V.; Mascarenhas, L.; Khosravan, R.; Lin, X.; Ingrosso, A.; Janeway, K.A. Sunitinib in pediatric patients with advanced gastrointestinal stromal tumor: Results from a phase I/II trial. Cancer Chemother. Pharmacol. 2019, 84, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, S.G.; Shusterman, S.; Ingle, A.M.; Ahern, C.H.; Joel, M.; Wu, B.; Baruchel, S.; Glade-bender, J.; Ivy, P.; Grier, H.E. Phase I and Pharmacokinetic Study of Sunitinib in Pediatric Patients with Refractory Solid Tumors: A Children’s Oncology Group Study. Clin. Cancer Res. 2011, 17, 5113–5122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetmore, C.; Daryani, V.M.; Billups, C.A.; Boyett, J.M.; Leary, S.; Tanos, R.; Goldsmith, K.C.; Stewart, C.F.; Blaney, S.M.; Gajjar, A. Phase II evaluation of sunitinib in the treatment of recurrent or refractory high-grade glioma or ependymoma in children: A children’s Oncology Group Study ACNS1021. Cancer Med. 2016, 5, 1416–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loh, M.L.; Tasian, S.K.; Rabin, K.R.; Brown, P.; Magoon, D.; Reid, J.; Chen, X.; Ahern, C.H.; Weigel, B.J.; Blaney, S.M. A Phase 1 Dosing Study of Ruxolitinib in Children with Relapsed or Refractory Solid tumors, Leukemias, or Myeloproliferative Neoplasms: A Children’s Oncology Group Phase 1 Consortium Study (ADVL1011). Pediatr. Blood Cancer 2015, 62, 1717–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuk, M.K.; Widemann, B.C.; Minard, C.G.; Liu, X.; Kim, A.R.; Bernhardt, M.B.; Kudgus, R.A.; Reid, J.M.; Voss, S.D.; Blaney, S.; et al. A phase 1 study of cabozantinib in children and adolescents with recurrent or refractory solid tumors, including CNS tumors: Trial ADVL1211, a report from the Children’s Oncology Group. Pediatr. Blood Cancer 2018, 65, e27077. [Google Scholar] [CrossRef] [PubMed]
- Kieran, M.W.; Geoerger, B.; Dunkel, I.J.; Broniscer, A.; Hargrave, D.; Hingorani, P.; Aerts, I.; Bertozzi, A.I.; Cohen, K.J.; Hummel, T.R.; et al. A phase I and pharmacokinetic study of oral dabrafenib in children and adolescent patients with recurrent or refractory BRAF V600 mutation–positive solid tumors. Clin. Cancer Res. 2019, 25, 7294–7302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwaan, C.M.; Rizzari, C.; Mechinaud, F.; Lancaster, D.L.; Lehrnbecher, T.; Van Der Velden, V.H.J.; Beverloo, B.B.; Den Boer, M.L.; Pieters, R.; Reinhardt, D.; et al. Dasatinib in children and adolescents with relapsed or refractory leukemia: Results of the CA180-018 phase I dose-escalation study of the Innovative Therapies for Children with Cancer Consortium. J. Clin. Oncol. 2013, 31, 2460–2468. [Google Scholar] [CrossRef] [PubMed]
- Broniscer, A.; Baker, S.D.; Wetmore, C.; Pai Panandiker, A.S.; Huang, J.; Davidoff, A.M.; Onar-Thomas, A.; Panetta, J.C.; Chin, T.K.; Merchant, T.E.; et al. Phase I Trial, Pharmacokinetics, and Pharmacodynamics of Vandetanib and Dasatinib in Children with Newly Diagnosed Diffuse Intrinsic Pontine Glioma. Bone 2013, 19, 3050–3058. [Google Scholar] [CrossRef] [Green Version]
- Aplenc, R.; Blaney, S.M.; Strauss, L.C.; Balis, F.M.; Shusterman, S.; Ingle, A.M.; Agrawal, S.; Sun, J.; Wright, J.J.; Adamson, P.C. Pediatric phase I trial and pharmacokinetic study of dasatinib: A report from the children’s oncology group phase I consortium. J. Clin. Oncol. 2011, 29, 839–844. [Google Scholar] [CrossRef]
- Geoerger, B.; Morland, B.; Ndiaye, A.; Doz, F.; Kalifa, G.; Geoffray, A.; Pichon, F.; Frappaz, D.; Chatelut, E.; Opolon, P.; et al. Target-driven exploratory study of imatinib mesylate in children with solid malignancies by the Innovative Therapies for Children with Cancer (ITCC) European Consortium. Eur. J. Cancer 2009, 45, 2342–2351. [Google Scholar] [CrossRef]
- PubChem Cobimetinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/16222096 (accessed on 1 January 2022).
- PubChem Cabozantinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/25102847 (accessed on 1 January 2022).
- PubChem Dabrafenib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/44462760 (accessed on 1 February 2022).
- Janssen, J.M.; Dorlo, T.P.C.; Steeghs, N.; Beijnen, J.H.; Hanff, L.M.; van Eijkelenburg, N.K.A.; van der Lugt, J.; Zwaan, C.M.; HuitEMA, A.D.R. Pharmacokinetic Targets for Therapeutic Drug Monitoring of Small Molecule Kinase Inhibitors in Pediatric Oncology. Clin. Pharmacol. Ther. 2020, 108, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Celano, P.; Fausel, C.A.; Kennedy, E.B.; Miller, T.M.; Oliver, T.K.; Page, R.; Ward, J.C.; Zon, R.T. Safe handling of hazardous drugs: ASCO standards. J. Clin. Oncol. 2019, 37, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.T. Medication administration through enteral feeding tubes. Am. J. Health Pharm. 2008, 65, 2347–2357. [Google Scholar] [CrossRef]
- PubChem Larotrectinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/46188928 (accessed on 1 January 2022).
- PubChem Ruxolitinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/25126798 (accessed on 1 January 2022).
- PubChem Dasatinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/3062316 (accessed on 1 February 2022).
- PubChem Imatinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/5291 (accessed on 1 February 2022).
- PubChem Ponatinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/24826799 (accessed on 1 February 2022).
- PubChem Bosutinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/5328940 (accessed on 1 January 2022).
- Drugbank Bosutinib. Available online: https://go.drugbank.com/drugs/DB06616 (accessed on 1 January 2022).
- PubChem Crizotinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/11626560 (accessed on 1 January 2022).
- PubChem Entrectinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/25141092 (accessed on 1 January 2022).
- PubChem Nilotinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/644241 (accessed on 1 January 2022).
- PubChem Selumetinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/10127622 (accessed on 1 January 2022).
- PubChem Sunitinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/5329102 (accessed on 1 January 2022).
- PubChem Trametinib. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/11707110 (accessed on 1 January 2022).
- Martinez, M.N.; Amidon, G.L. A mechanistic approach to understanding the factors affecting drug absorption: A review of fundamentals. J. Clin. Pharmacol. 2002, 42, 620–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Riet-Nales, D.A.; Ferreira, J.A.; Schobben, A.F.A.M.; De Neef, B.J.; Egberts, T.C.G.; Rademaker, C.M.A. Methods of administering oral formulations and child acceptability. Int. J. Pharm. 2015, 491, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Spencer, S.H.; Menard, S.M.; Labedz, M.Z.; Krueger, C.D.; Sarna, K.V. Enteral tube administration of oral chemotherapy drugs. J. Oncol. Pharm. Pract. 2020, 26, 703–717. [Google Scholar] [CrossRef]
- EMA. Requirements to the Chemical and Pharmaceutical Quality Documentation Concerning Investigational Medicinal Products in Clinical Trials. Available online: https://www.ema.europa.eu/en/requirements-chemical-pharmaceutical-quality-documentation-concerning-investigational-medicinal (accessed on 1 September 2022).
- Phase II Pediatric Study with Dabrafenib in Combination with Trametinib in Patients with HGG and LGG. 2016. Available online: https://www.clinicaltrials.gov/ct2/show/study/NCT02684058?titles=BRAF+V600+mutation+positive+Low+Grade+Glioma+%28LGG%29+or+relapsed+or+refractory+High+Grade+Glioma+%28HGG%29&draw=2 (accessed on 1 March 2022).
- A Phase I/II, Multicenter, Open-Label, Dose-Escalation Study of the Safety and Pharmacokinetics of Cobimetinib in Pediatric and Young Adult Patients with Previously Treated Solid Tumors. 2015. Available online: https://www.clinicaltrials.gov/ct2/show/NCT02639546?titles=A+PHASE+I%2FII%2C+MULTICENTER%2C+OPEN-LABEL%2C+DOSE-ESCALATION+STUDY+OF+THE+SAFETY+AND+PHARMACOKINETICS+OF+COBIMETINIB+IN+PEDIATRIC+AND+YOUNG+ADULT+PATIENTS+WITH+PREVIOUSLY+TREATED+SOLID+TUMORS&dr (accessed on 1 February 2022).
- Drumond, N.; van Riet-Nales, D.A.; Karapinar-Çarkit, F.; Stegemann, S. Patients’ appropriateness, acceptability, usability and preferences for pharmaceutical preparations: Results from a literature review on clinical evidence. Int. J. Pharm. 2017, 521, 294–305. [Google Scholar] [CrossRef]
- Pawar, G.; Wu, F.; Zhao, L.; Fang, L.; Burckart, G.J.; Feng, K.; Mousa, Y.M.; Naumann, F.; Batchelor, H.K. Development of a Pediatric Relative Bioavailability/Bioequivalence Database and Identification of Putative Risk Factors Associated with Evaluation of Pediatric Oral Products. AAPS J. 2021, 23, s12248-s021. [Google Scholar] [CrossRef]
- Kaczmarska, A.; Śliwa, P.; Lejman, M.; Zawitkowska, J. The use of inhibitors of tyrosine kinase in paediatric haemato-oncology—When and why? Int. J. Mol. Sci. 2021, 22, 2089. [Google Scholar] [CrossRef]
- Evans, W.E.; Pui, C.H.; Yang, J.J. The Promise and the Reality of Genomics to Guide Precision Medicine. Clin. Pharmacol. Ther. 2020, 107, 176–180. [Google Scholar] [CrossRef]
- Martir, J.; Flanagan, T.; Mann, J.; Fotaki, N. BCS-based biowaivers: Extension to paediatrics. Eur. J. Pharm. Sci. 2020, 155, 105549. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, I. Naive pooled-data approach for pharmacokinetic studies in pediatrics with a very small sample size. Am. J. Ther. 2014, 21, 269–274. [Google Scholar] [CrossRef] [PubMed]


| Crushed/Opened (Solid) Oral Administration (A) | LoE A | Oral Liquid (i.a. Nasogastric Tube Administration 1) (B) | LoE B | Refs | |
|---|---|---|---|---|---|
| BCS class I | |||||
| Cobimetinib | Crush the tablet and administrate with a small amount of apple sauce or chocolate pasta | 5 | Dissolve the tablet in water and carefully stir/shake until the suspension is formed. Administrate the suspension immediately | 5 | [13,32,76] |
| Larotrectinib | Use available oral solution | 1 | Use available oral solution | 1 | [37] |
| Ruxolitinib | Crush the tablet and administrate with a small amount of apple sauce | 5 | Dissolve tablet in 40 mL of water and carefully stir/shake for 10 min. Administrate the suspension immediately | 1 | [24,38] |
| BCS class II | |||||
| Cabozantinib | Open capsule or crush the tablet and sprinkle content over a spoon of apple sauce | 5 | Dissolve tablet or content of capsule in apple juice and carefully stir/shake. Administrate the suspension immediately | 5 | [17,34,77] |
| Cave: food interaction (higher AUC, Cmax and risk of toxicity) | |||||
| Dabrafenib | Open the capsule and sprinkle content over a spoon of applesauce. Administrate the prepared suspension immediately | 5 | Dissolve capsule content in 5 mL water or apple juice and carefully stir/shake. Administrate the suspension immediately | 4 | [30,43,52,78] |
| Cave: food interaction and chemical instable | |||||
| Dasatinib | Use available oral suspension | 1 | Use available oral suspension | 1 | [35] |
| Cave: antacid interaction, no bioequivalence between tablets and oral suspension | |||||
| Imatinib | Open capsule or crush the tablet and sprinkle content over a spoon of applesauce | 5 | Dissolve 100 mg imatinib (capsule content or tablet) with 10 mL water. Administrate the suspension immediately | 1 | [31,45] |
| Cave: do not mix imatinib with orange juice, milk or cola | |||||
| Ponatinib | Crush the tablet and administrate with a small amount of applesauce | 5 | Dissolve tablet in lemon juice and carefully stir/shake. Administrate the suspension immediately | 5 | [15,19,46] |
| Cave: only soluble in pH ≤ 2.0 | |||||
| BCS class IV | |||||
| Bosutinib | Crush tablet in a small amount of chocolate pasta | 4 | Dissolve tablet in apple juice and carefully stir/shake. Administrate the suspension immediately | 5 | [33,44,50] |
| Cave: antacid interaction | |||||
| Crizotinib | Open the capsule and sprinkle the content over a small amount of applce sauce | 5 | Dissolve capsule (with shell) in warm water (50 °C) and carefully stir/shake. Administrate the suspension immediately | 4 | [28,41] |
| Entrectinib | Open the capsule and sprinkle the content over small amount of applesauce | 5 | Consider dissolving the capsule content in a low pH vehicle (e.g., lemon juice) | 5 | [29,47] |
| Cave: not soluble and has non-standardized excipient (acidulant) in the formulation. Be aware of possible blocking of the feeding tube | |||||
| Nilotinib | Open the capsule and sprinkle content over a spoon of apple sauce or chocolate pasta | 5 | Consider dissolving the capsule content in a low pH vehicle (e.g., lemon juice) due to insolubility of nilotinib | 5 | [23,25] |
| Cave: food interaction and insolubility of nilotinib. Be aware of possible blocking of feeding tube | |||||
| Selumetinib | Open the capsule and sprinkle the content over a small amount of applesauce | 5 | Consider dissolving the capsule content in a low pH vehicle (e.g., lemon juice) | 5 | [16,49] |
| Cave: food interaction, low absorption in suspension formulation, use of non-standardized excipient (solubilizing agent) and insolubility of selumetinib. Be aware of possible blocking of feeding tube | |||||
| Sunitinib | Open the capsule and sprinkle the content over applesauce (or yoghurt) | 2 | Dissolve capsule content in apple juice and carefully stir/shake. Administrate the suspension immediately | 2 | [26,39,40] |
| Cave: sunitinib is light sensitive and will form (impure) isomers within two hours after dissolving in a glass of apple juice | |||||
| Trametinib | Crush tablet and add content to a spoon of apple sauce | 5 | Dissolve tablet in 5 mL water or consider dissolving the tablet in a low pH vehicle (e.g., lemon or apple juice) and carefully stir. Administrate the suspension immediately | 4 | [21,27,42,43] |
| Cave: food interaction and insolubility of trametinib. Be aware of possible blocking of feeding tube | |||||
| General recommendations Always perform therapeutic drug monitoring (TDM) after manipulating the solid dosage form (see TDM recommendations in study of Janssen et al., 2020 [79]). Always use gloves and a mouth cap before manipulating the solid dosage form of anticancer drugs [80]. | |||||
| Off-Label Indication | Ligand | Log p | Solubility Range (pH) | pKa | Salt Form | Refs | |
|---|---|---|---|---|---|---|---|
| BCS Class I | |||||||
| Cobimetinib | Solid tumors | MEK | 3.9 | 1.0–7.5 | - | Hemifumarate | [13,76] |
| Larotrectinib | Solid tumors, Primary CNS tumors | TRK | 1.7 | 1.0–8.0 | - | Sulfate | [48,82] |
| Ruxolitinib | Relapsed or refractory solid tumors, leukemia or myeloproliferative neoplasms | JAK | 2.1 | 1.0–8.0 | 0.91, 5.51, 13.89 | Phosphate | [20,83] |
| BCS Class II | |||||||
| Cabozantinib | HB, HCC | VEGF | 5.4 | 1.0–4.0 (capsules) 1.0–3.0 (tablets) | - | Malate | [17,18,77] |
| Dabrafenib | LGG, HGG | B-RAF | 4.8 | 1.0–4.0 | −1.5 | Mesylate (and micronized, pharmaceutical development) | [52,78] |
| Dasatinib | CML | BCR-ABL | 3.6 | - | - | Monohydrate | [36,84] |
| Imatinib | CML, ALL | BCR-ABL | 3.5 | Soluble in water | - | Mesilate | [14,85] |
| Ponatinib | CML, Ph+ ALL | BCR-ABL | 4.1 | 1.0–2.0 | 2.77, 7.8 | HCL | [15,86] |
| BCS Class IV | |||||||
| Bosutinib | CML | BCR-ABL | 5.4 | 1.0–5.0 | - | Monohydrate | [50,87,88] |
| Crizotinib | ALCL | ALK | 1.65 | 1.6–8.2 | - | na | [22,89] |
| Entrectinib | Solid tumors | ROS 1 and NTRK | 5.7 | Not soluble | - | na | [47,90] |
| Nilotinib | Relapsed or refractory malignancies | BCR-ABL | 4.9 | - | 2.1, 5.4 | Monohydrate | [25,91] |
| Selumetinib | Relapsed or refractory tumors | MEK | 3.6 | Not soluble | - | Hydrogen sulfate | [16,92] |
| Sunitinib | Renal tumors | VEGF | 5.2 | 1.0–5.0 | 8.95 | Maleate | [51,93] |
| Trametinib | LGG, HGG | MEK | 3.4 | Not soluble | - | Dimethyl sulfoxide | [21,94] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernsen, E.C.; Hogenes, V.J.; Nuijen, B.; Hanff, L.M.; Huitema, A.D.R.; Diekstra, M.H.M. Practical Recommendations for the Manipulation of Kinase Inhibitor Formulations to Age-Appropriate Dosage Forms. Pharmaceutics 2022, 14, 2834. https://doi.org/10.3390/pharmaceutics14122834
Bernsen EC, Hogenes VJ, Nuijen B, Hanff LM, Huitema ADR, Diekstra MHM. Practical Recommendations for the Manipulation of Kinase Inhibitor Formulations to Age-Appropriate Dosage Forms. Pharmaceutics. 2022; 14(12):2834. https://doi.org/10.3390/pharmaceutics14122834
Chicago/Turabian StyleBernsen, Emma C., Valery J. Hogenes, Bastiaan Nuijen, Lidwien M. Hanff, Alwin D. R. Huitema, and Meta H. M. Diekstra. 2022. "Practical Recommendations for the Manipulation of Kinase Inhibitor Formulations to Age-Appropriate Dosage Forms" Pharmaceutics 14, no. 12: 2834. https://doi.org/10.3390/pharmaceutics14122834