
Potential of Nuclear Imaging Techniques to Study the Oral Delivery of Peptides
by
 ,
,
Tanya Saxena
1,
Claire Sie
1,
Kristine Lin
1,
Daisy Ye
1,
Katayoun Saatchi
1,* and
Urs O. Häfeli
1,2,* 1
Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC V6T1Z3, Canada
2
Department of Pharmacy, Faculty of Health and Medical Sciences, University of Copenhagen, 2100 Copenhagen, Denmark
*
Authors to whom correspondence should be addressed.
Pharmaceutics 2022, 14(12), 2809; https://doi.org/10.3390/pharmaceutics14122809
Submission received: 22 November 2022
/
Revised: 8 December 2022
/
Accepted: 12 December 2022
/
Published: 15 December 2022
(This article belongs to the Special Issue Molecular Imaging in Biopharmaceutical Research and Development)
Abstract
:Peptides are small biomolecules known to stimulate or inhibit important functions in the human body. The clinical use of peptides by oral delivery, however, is very limited due to their sensitive structure and physiological barriers present in the gastrointestinal tract. These barriers can be overcome with chemical and mechanical approaches protease inhibitors, permeation enhancers, and polymeric encapsulation. Studying the success of these approaches pre-clinically with imaging techniques such as fluorescence imaging (IVIS) and optical microscopy is difficult due to the lack of in-depth penetration. In comparison, nuclear imaging provides a better platform to observe the gastrointestinal transit and quantitative distribution of radiolabeled peptides. This review provides a brief background on the oral delivery of peptides and states examples from the literature on how nuclear imaging can help to observe and analyze the gastrointestinal transit of oral peptides. The review connects the fields of peptide delivery and nuclear medicine in an interdisciplinary way to potentially overcome the challenges faced during the study of oral peptide formulations.
1. Introduction
One of the most common routes of drug administration is oral delivery, 53% of FDA-approved drugs from 2015–2020 [1] since it provides better patient compliance and low manufacturing cost [2,3]. While parenteral drug delivery typically shows 80–100% bioavailability, rapid onset of drug effect, and most predictable pharmacokinetics, about 5% of the world’s population is still needle-phobic, and injections generally require medical training for administration [4]. Thus, oral drug delivery is by far the preferred route of administration by patients [5]. It plays a major role in the treatment of chronic disorders such as diabetes, gut infections, irritable bowel syndrome, and hypertension that require daily administration [6]. Despite many benefits, oral peptides comprise only 4% of protein and peptide FDA-approved formulations, primarily due to the challenges faced during the development of oral delivery systems [7]. The harsh environment of the gastrointestinal tract comprising acidic pH, enzymes, mucus lining, and gut microbiome prevents the delivery of sensitive drugs, e.g., peptides, into the systemic circulation, thereby reducing their oral bioavailability [8,9].
Peptides are polymeric biomolecules consisting of approximately 2–50 amino acids linked by peptide bonds [10]. One of the most commonly administered therapeutic peptides is insulin, a 51-amino acid long peptide hormone secreted by beta cells in the pancreas [11]. Insulin is used to treat diabetes which affected 537 million adults worldwide and caused 6.7 million deaths in 2021 [12]. In the past, insulin injections were given subcutaneously to treat diabetes due to low oral bioavailability in the gastrointestinal (GI) tract [13]. However, in 2019, a clinical Glucagon-like-peptide-1 (GLP-1) receptor agonist called Rybelsus® (Semaglutide) came into the market that treats Type 2 diabetes by stimulating the secretion of insulin from the pancreas [14]. It shows better efficacy compared to other GLP-1 agonists but has very low bioavailability (~1%) and can cause pancreatitis or thyroid cancer [15,16].
Peptides are very versatile biopharmaceuticals as they exhibit high specificity, bind to a variety of drug targets, and express low toxicity [17]. Nevertheless, their limitations exceed their benefits as they show low physiochemical stability, undergo proteolysis, and may induce immunogenicity [18]. Furthermore, high molecular weight, low lipophilicity, and the presence of charged functional groups make them poor permeators and reduce their bioavailability further [7,8,19,20,21,22].
The low oral bioavailability of peptides caused by these barriers has adversely affected the approval of oral peptide formulations, as seen in Figure 1 [7]. In July 2017, there were 380 drug variants (chemically modified analogs) of the total Federal Drug Administration (FDA) approved peptides in clinical use. Only 13 of these drug variants were delivered orally, while almost half (158) of them were administered intravenously, 116 were given subcutaneously, and 49 were intramuscularly [7]. Orally delivered peptides thus comprise only 4% of total peptide use (Figure 1) [7]. However, there has been a recent increase in the approval of oral peptide formulations due to innovative interdisciplinary drug delivery research. Currently, in 2021, there are 26 FDA-approved oral formulations of peptides, including the already mentioned 13 peptides plus octreotide and their drug variants (Table 1) [23]. Similarly, the European Medical Agency (EMA) approved 18 peptide drugs between 2010 and 2019, of which only four were administered orally, and two were retracted recently [23]. It is thus very apparent that oral delivery of peptides is still an uncommon method of clinical administration.
1.1. Barriers to Oral Delivery of Peptides
The first barrier for peptides (Figure 2) is potential degradation by gastric juices in the stomach, which is low in pH (~1 to 3) and high in proteases, e.g., pepsin [40]. As peptides leave the stomach, the pH gradually increases in the small intestine (5.5–7), large intestine (5.5–7.5), and colon (6.5–7.5) [3,41]. These changes in pH can chemically and functionally alter the 3D structure of peptides. The next barrier is enzymes such as trypsin and chymotrypsin present in the intestine, especially in the first segment of the small intestine (duodenum), that degrade peptides into small non-functional fragments. The thick mucus covering the intestinal wall acts as the third barrier and hinders the drug uptake process. Underlying the mucus is the last barrier made up of special epithelial cells called enterocytes that allow selective permeation of molecules into the systemic circulation but overall reduce drug penetration through the intestinal membrane [8].
Protease inhibitors, permeation enhancers, and polymeric encapsulation are some of the approaches that improve the pharmacological effect and oral bioavailability of peptides [25,42]. For example, Tarsa’s oral recombinant salmon calcitonin (TBRIATM) has shown encouraging safety and efficacy results in Phase 3 ORACAL trial for the treatment of postmenopausal osteoporosis by incorporating the approaches mentioned above. The tablet contains an outer layer of pH-lowering agent (citric acid) and an inner layer of peptide calcitonin along with the permeation enhancer lauroyl l-carnitine. An enteric coating of hydroxypropylmethylcellulose helps bypass the acidic stomach pH to achieve intestinal delivery. TBRIATM was less immunogenic but similarly effective and safe compared to commercially available nasal calcitonin sprays [43].
Nanoparticle and microsphere encapsulation is also effective in protecting peptides during oral delivery and increasing pharmacological effect [8]. For example, researchers have shown that the peptide insulin loaded in microspheres using a 1:1 ratio of poly(fumaric anhydride) and poly(lactide-co-glycolide) successfully penetrated the intestinal epithelium in rats and promoted the glucose uptake in cells, while the controls (saline or insulin solution given orally) increased blood glucose as expected to non-significantly different levels from each other [44].
1.2. Observing Oral Delivery of Peptides
Although oral delivery has been well studied clinically, scientists still struggle to accurately quantify drug uptake and distribution in the GI tract pre-clinically due to the smaller size and dimensions of the organs in animals [45,46]. In addition, physiological and anatomical barriers such as gastric juices, enzymes, and intestinal mucus membranes present in the GI tract reduce the bioavailability of drugs considerably [2,5]. Peptides, such as other biomolecular drugs, have sensitive 3D structures that get degraded easily in the GI tract and thus are not delivered orally (further discussed in the next section) [5,47,48]. Drug delivery systems (DDS) have been formulated to overcome this degradation by protecting/encapsulating peptides in excipients that improve the amount of intact functional peptides reaching the systemic circulation after oral administration [17,47,49,50].
The amount and rate of drug delivered from the oral DDS to the systemic circulation, i.e., the pharmacokinetic properties of the DDS, can be studied using different techniques such as traditional biodistribution studies, histological analyses, blood sampling techniques, and more recently, optical and fluorescent microscopy, and nuclear imaging techniques [51,52,53,54].
Over a period, new techniques have emerged, overcoming the limitations of earlier techniques, but each technique has its advantages and limitations. Biodistribution studies give an accurate quantitative analysis of drug distribution in the body but require a large number of animals for each time point to study drug uptake in different organs over time [55]. Whereas histology provides drug uptake at specific locations such as tissue layers at different time points after sacrificing the animals, thereby requiring discrete animals for each data point leading to large standard deviations [56,57,58]. Blood sampling overcomes this challenge since blood can be collected from the same animal at different time points, but it does not provide any data regarding drug uptake in tissues or organs. On the other hand, microscopy provides a good understanding of cellular uptake and reduces animal variability but lacks the depth of penetration [59]. Nuclear imaging overcomes all these challenges through real-time 3D images. It clearly shows the depth of penetration of drug uptake in the same animal since the drug is conjugated with a radioisotope that can be detected on a gamma camera while the drug is moving through the body [59,60,61]. However, nuclear imaging has its own drawbacks, such as low resolution at the cellular level (limitation of current gamma cameras) and the difficulty in observing the stability of radioisotope-bound peptides during GI transit and uptake into circulation [62].
This review, in addition to giving an update on the current clinically available oral peptide formulations and drug delivery systems, also discusses the potential of nuclear imaging techniques to study the oral biodistribution of biopharmaceutical peptide drugs with a special focus on Single Photon Emission Computed Tomography (SPECT) and Positron Emission Tomography (PET) imaging, as they are the most sensitive and quantitative in vivo nuclear imaging methods.
2. Existing Systems of Oral Delivery of Peptides
As mentioned briefly in the section above, to overcome physiological barriers present in the GI tract, components such as enzyme inhibitors, enteric coatings, and permeation enhancers are employed in DDSs such as liposomes, nanoparticles, micelles, and hydrogels (Figure 3) [47]. While microspheres and dendrimers are also being investigated pre-clinically as possible carriers for oral delivery of peptides [63,64,65,66,67], they are not discussed in this review.
2.1. Liposomes
First elucidated by Alec D Bangham in 1961, liposomes are the most common and well-studied type of nanocarrier used for drug delivery [68]. They are defined as vesicles composed of one or more phospholipid bilayers that self-assemble to enclose an aqueous interior space, typically between 50–150 nm in diameter (Figure 3A) [63]. Researchers’ fascination with the oral administration of therapeutic molecules via liposomes began in the 1970s incorporating insulin for managing blood glucose levels [57,69]. Patel and Ryman (1976) showed that liposomal formulations made up of lecithin, cholesterol, and diacetyl phosphate could successfully deliver insulin orally, reducing the blood glucose level of diabetic rats to approximately one-third of its initial value 3 h after administration [11]. They concluded that adopting a liposomal drug delivery system allowed insulin. A peptide previously believed to lose its therapeutic effects when orally administered to survive the harsh environments of the GI tract. Although the results were promising, it was later found that they were neither reproducible nor consistent, with only 54% of spontaneously diabetic rats and 67% of alloxan-induced diabetic rabbits responding to treatment [70]. These inconsistencies may have been in part due to the challenges faced by the early liposomal delivery systems that resulted in low circulation time due to uptake by the reticuloendothelial system and opsonization [71].
There are several advantages of using liposomes for the oral delivery of peptides. First, liposomes are biocompatible due to their lipid composition being similar to biological membranes [72]. Additionally, they are unparalleled among nanocarriers in their ability to encapsulate both hydrophobic and hydrophilic drugs, allowing for a diverse range of therapeutic molecules to be shielded from the external environment and successfully delivered [73]. Furthermore, they can be improved with a wide variety of physicochemical and biophysical functionalities, such as targeting ligand molecules, PEGylation, and polymeric coatings that might enhance peptide delivery and reduce the barriers faced by other oral DDS (Figure 3A) [74,75]. A pioneering liposomal polymerization technique introduced by Dr. Robert Langer’s lab composed of cross-linked 1,2-di (2,4-octadecadienoyl) phosphatidylcholine showed 50% more gastrointestinal stability than regular cholesterol-based liposomes and could deliver 75% of its contents intact to the intestine [76].
Overall, liposomal delivery systems are able to stabilize and protect therapeutic compounds from enzymatic degradation, prevent premature inactivation, and increase absorption through the GI tract [74].
2.2. Nanoparticles
Nanoparticles are particles typically sized from 1 to 100 nm and made from inorganic materials, such as silicates, carbon, silver, iron, titanium, and cerium, or organic materials, such as lipids, polymers, and proteins [77]. Nanoparticles have multiple benefits, such as efficient delivery of cargo to the blood circulation and the lymphatic system, thereby increasing the drug’s circulation time and concentration at the target site, for example, a. tumor (Figure 3B) [8]. Nanoparticles protect peptides during oral delivery by encapsulating biomolecules inside their core and preventing mechanical or physiological damage to the peptide [78]. Furthermore, bioadhesive nanoparticles assist in increasing the retention and residence time of peptides at target sites, such as under the tongue or in the gastrointestinal tract, increasing their uptake. In particular, mucoadhesive polymers such as chitosan, Carbopol, polymethacrylates, and carboxymethyl cellulose, mixed with or coated onto nanoparticles, promote strong adhesive interactions with mucus and increase the interaction with the intestinal epithelium [8,79]. This prolongs nanoparticles’ time in the intestinal lumen, increases a drug’s concentration in the systemic circulation, and reduces plasma fluctuations and side effects, thus overall improving drug bioavailability and efficacy [63].
As an example of nanoparticles used for oral peptide delivery, Zhang et al. in 2006 showed that insulin could be successfully delivered orally via solid lipid nanoparticles with a bioavailability of 4.99% to 7.11% in rats [80]. Another report by Sung et al. confirmed these findings and showed that nanoparticles sized between 110 nm to 250 nm and composed of chitosan and poly (γ-glutamic acid) incorporating 15% insulin resulted in an oral bioavailability of 15.1 ± 0.9% and a visible decrease in blood glucose levels of diabetic rats [81,82]. Mucoadhesive polymers such as chitosan contribute to the opening of tight junctions between the epithelial cells of the lining of the small intestine [82]. However, practical applications of chitosan are limited as it is poorly soluble in the intestine, and chemical modifications to its structure can affect the functionality of peptides being delivered [83]. Another type of polymeric nanoparticles composed of poly(-ε-caprolactone) and Eudragit® RS was found to be more biocompatible and effective but showed low oral bioavailability of 13% in diabetic rats after oral delivery [84].
2.3. Micelles
Polymeric micelles are spherical structures composed of amphiphilic copolymers which self-assemble in aqueous solutions (Figure 3C) [85]. They are typically under 100 nm in size and possess a hydrophobic core into which lipophilic therapeutic compounds may be loaded [85]. They protect incorporated drugs from degrading factors during circulation, and their altered physicochemical properties can increase membrane permeability [86]. In addition, micellar DDS avoid clearance by the reticuloendothelial system due to their small size and improve its systemic exposure [87].
Most successfully, micellar delivery systems were experimentally tested and revealed to be applicable for both ocular drug delivery [88] and delivery of anti-cancer drugs [89]. A wide variety of formulated copolymers have also been tested for use in oral drug delivery. For example, polyanionic copolymer mPEG-grafted-alginic acid (mPEG-g-AA)-based polyion complex (PIC) micelles were shown to increase the intestinal permeability of the 32-amino-acid peptide salmon calcitonin by 2.24-fold across a Caco-2 monolayer without affecting the cell integrity [90].
In 2020, for the first time, Han et al. developed zwitterionic micelles that can successfully deliver oral insulin in animals [91]. The micelles made up of DSPE-PCB (DSPE-1, 2-distearoyl-sn-glycero-3-phosphoethanolamine, PCB-poly(carboxybetaine) mimic the surface of capsid viruses, thereby penetrating the epithelial cell layer of GI tract by proton-assisted amino acid transporter 1 (PAT1) [92,93,94]. A key benefit of these micelles is their ultra-low critical micelle concentration (CMC) of ~10-6 mM that prevents the tight junctions from opening [95]. Thus, peptides delivered in DSPE-PCB micelles are only delivered by transcellular pathway and show a unique safety profile by maintaining gut health. The researchers also fabricated a prototype of oral insulin by encapsulating freeze-dried DSPE-PCB/insulin in an enteric-coated capsule and administering it in diabetic rats [91]. The formulation showed an oral bioavailability of 42.6% and a prolonged hypoglycemic effect of up to 6 h, depending on the loading ratio of DSPE-PCB and insulin [91].
2.4. Hydrogels
Another DDS under consideration for oral drug delivery of peptides is hydrogels. They are defined as polymers consisting of hydrophilic components cross-linked together, forming a 3D structure that can swell and hold a large amount of water [96]. In a comprehensive review by Sharpe et al., the authors noted that hydrogels are good candidates for oral drug delivery due to their biocompatibility, ability to be modified, and the wide range of materials, either synthetic or natural, that can be used in their fabrication [97]. A range of hydrophilic polymers is used to cross-link and form mesh-like structures that can be loaded with different drug moieties. An advancement in this field comes in the form of smart polymeric composite carriers such as carboxylated chitosan grafted nanoparticles (CCGN) combined with bilaminated films consisting of a hydrophilic alginate-Ca2+ mucoadhesive layer and a hydrophobic ethylcellulose backing layer [98]. Calcein was entrapped in the nanoparticles and loaded into the hydrogel alginate film. In vitro release studies showed no release in simulated gastric fluid at pH 1.2 (similar to humans) and 100% release within 30 min at intestinal pH due to the complete dissolution of the alginate layer [98].
3. Nuclear Imaging
To study the movement and ability of DDS to reach the target site, scientists have invented a variety of imaging techniques ranging from optical techniques to nuclear imaging. Optical techniques include light, electron, bioluminescence, and fluorescence microscopy for cells, in vivo imaging systems (IVIS) (includes fluorescence and bioluminescence imaging), and optical coherence tomography (OCT) for tissues/animals [99]. The optical techniques provide an easy, cost-effective in vitro quantification of the drug concentration within cells [100]. However, pre-clinical optical imaging is often challenging due to a lack of light absorption into the tissue/organ, making the imaging non-quantitative. The shortcomings of the optical techniques can be overcome by nuclear imaging, also known as radionuclide scanning, as it provides real-time analysis, high resolution, and fully quantitative results in 3D [59]. This section discusses the current applications and future potential of nuclear imaging in the field of oral peptide delivery for pre-clinical and clinical studies.
Nuclear medicine imaging, by the use of radiotracers and different radioisotopes, identifies abnormalities in the body at molecular levels, such as cancer, infectious and inflammatory disorders, neurodegenerative conditions, amongst others [59,101]. The tracers are administered intravenously or orally in millicurie (1 mCi = 37 MBq) doses. They accumulate in target organs over time, and through the emission of gamma, beta rays, or positrons, they can be detected by gamma camera systems or PET systems to display an image of the diseased site [102]. Nuclear imaging scans include gamma camera systems and PET systems. They provide a non-invasive, real-time imaging modality that can be validated with an ex vivo biodistribution study wherein the organs are harvested, and radioactivity is measured in each organ at different time points throughout the study or at the end of an experiment [103,104]. A recent advancement in the field of nuclear imaging is fusion imaging, consisting of PET/SPECT imaging combined with Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) which allows the concurrent assessment of both functional/physiological and morphological/anatomical conditions in a patient. Thus, a dual-modality imaging system such as PET/CT, PET/MRI, and SPECT/CT provides the radiation signal overlaid on an accurate visual background of a patient’s target organs and anatomy [60].
The steps toward the clinical development of a radiolabeled peptide for optimal targeting, as seen in Figure 4, include (1) Identification of the receptor or molecular target. Receptor homogeneity, density, and incidence play an important role in targeting receptors. (2) To improve the biological half-life of the peptides, occasionally, a more metabolically stable peptide analog is synthesized, which preserves the functionality and molecular structure of the natural peptide. (3) Radiolabeling process. The peptide is covalently coupled, with or without a spacer and/or chelator that can bind a radioisotope (e.g., 18F) or a radiometal (e.g., 111In) accordingly. For example, the peptide can be directly conjugated to radioiodine or 18F using a prosthetic group with a high labeling efficiency (>95%) and specific activity. (4) In vitro radiopeptide binding to study the affinity of the altered radiolabeled peptide to bind to cell receptors and produce the desired effect. (5) In vivo biodistribution and imaging to study the pharmacokinetic and pharmacodynamic properties of the radiopeptides in established animal models. (6) Testing of successful radiopeptide candidates for safety and efficacy in at least two animal models before going through clinical trials in humans [105,106].
One of the first radionuclide imaging studies on the (non-oral) delivery of peptides was carried out by Hassan et al. in 1999 [41] and showed the biodistribution of Iodine-131 (131I) radiolabeled Glucagon-like-Peptide-1 (GLP-1) (7–36) in rats after intravenous administration (Figure 5) using a gamma camera. It confirmed a very short half-life (~3.3 min), a high clearance rate (~117 mL/min) of GLP-1 and showed major accumulation in the kidneys after enzymatic degradation.
Clinically, radiolabeled somatostatin analogs are successfully used for cancer therapy after intravenous injection. For example, Somakit TOC is a diagnostic medicine approved by EMA, used to image gastroenteropancreatic neuroendocrine tumors (GEP-NETs). The kit contains the somatostatin analog, edotreotide, that binds to somatostatin receptors present in the GI tract and pancreas. The peptide is radiolabeled with the PET isotope gallium-68 before injection so that specific cancer cell receptor binding can be imaged. After confirming cancer diagnostically, Lutathera is used to treat GEP-NETs by irradiating the tumors with the beta-emitter lutetium-177. For this purpose, the somatostatin analog DOTA-TATE is radiolabeled with 177Lu to form a radiopeptide that specifically binds to the somatostatin receptors present in the tumor cells. While these radiolabeled peptides have been available commercially for a while now, no oral formulation has been reported.
3.1. Single Photon Emission Computed Tomography (SPECT) Imaging
Due to multiple barriers faced during the oral delivery of peptides, as stated in Section 1.1, the real-time imaging of peptides reaching the target site requires high sensitivity. SPECT imaging provides this high sensitivity and is additionally a great alternative to optical imaging, as it provides truly quantitative detection of radioactivity in comparison to the easily attenuated fluorescent or bioluminescent probes in live animals. For example, Niu et al. developed a nanocomplex between insulin as the model peptide and octaarginine as a cell-penetrating peptide, enveloped by the protecting polymer poly (glutamic acid)-poly (ethylene glycol) (PGA-PEG) that provided intestinal stability and much penetration [107]. Octaarginine was chemically conjugated with cholesterol or lauric acid to increase electrostatic/hydrophobic interaction with insulin. In vitro studies using a Caco-2 cell monolayer showed high cellular uptake of insulin (47.6 ± 5.8%) into epithelial cells. However, only 2.1% of the radioactive insulin went across the Caco-2 cell line monolayer [107].
Despite the low penetration, the researchers performed an in vivo pharmacokinetic study in Wistar rats using SPECT imaging (Figure 6). The authors radiolabeled the PGA-PEG-conjugated insulin nonspecifically with 99% labeling efficiency on the polymer end, using stannous chloride using pertechnetate (99mTcO4−). GI transit across the small intestine between 2 to 4 h and accumulation in the cecum for 11 h were observed [107]. Although the imaging method was not sensitive enough to measure the nanocomplex in the systemic circulation, the GI transit of the radiopharmaceutical could be studied properly over time, with the caveat that it likely formed 99mTc-oxides possibly not reflecting the fate of insulin. Furthermore, glucose levels in the blood did not change, pointing to minimal delivery of intact insulin into the systemic circulation.
More recently, the in vivo biodistribution of the peptide PYY3-36 radiolabeled with 111In (Table 2) was determined in mice after subcutaneous administration using non-invasive SPECT/CT imaging. The organ-specific uptake of acetylated PYY3-36 activity over 24 h was compared to PYY3-36 functionally modified with a bipyridine (bipy) group. The standardized uptake value (SUV) in the kidneys and injection site after 1 h was found to be double in the case of PYY3-36-bipy (23.4 ± 2.6%) compared to acetylated PYY3-36 (11.3 ± 2.5%) (Figure 7) [108].
In addition to real-time imaging, nuclear imaging also provides an opportunity for studying the pharmacokinetics of a peptide and its carrier at the same time, whereby one isotope (e.g., 67Ga) is conjugated to the peptide and a second isotope with a different energy peak (e.g., 111In) is conjugated to the carrier. This allows for a co-localization study of the entire drug delivery system and verifies the in vivo stability of both the peptide and the carrier. An example of this was illustrated by Sonaje et al. in 2010 with dual-isotope imaging, wherein the biodistribution of 99mTc-labeled chitosan as drug carrier and 123I-labeled as part-insulin as the drug was studied. The DDS was orally administered in rats as a nanoparticle formulation [55]. Using SPECT/CT imaging, the researchers observed the permeation of the radiolabeled aspart-insulin (analog of natural insulin) from the stomach into the systemic circulation, eventually leading to an accumulation in the kidneys and bladder 30 min after administration. However, the 99mTc-labeled chitosan (carrier) moved through the GI tract and remained in the intestinal lumen. The superimposition of both images shows the ability of SPECT/CT imaging to study the anatomical and functional properties of the DDS (Figure 8).
The same research group conducted another study in 2013 where they modified the previous nanoparticle formulation by conjugating chitosan to ethylene glycol tetraacetic acid (EGTA) [109] and encapsulated insulin within these nanoparticles to increase its oral bioavailability by 21% [110]. EGTA is known to chelate Ca2+ and provide protection to insulin from proteases such as trypsin and chymotrypsin, which are Ca2+ dependent enzymes and present inside the intestinal tract [111,112]. A decrease in Ca2+ also leads to a reversible opening of the apical junctional complex, thereby increasing the paracellular permeability of insulin through the Caco-2 cell monolayers [113]. The researchers showed that orally delivered 123I-labeled chitosan-EGTA nanoparticles circulated through the heart, renal cortex, renal pelvis, and liver leading to a prolonged hypoglycemic effect (~5 h) in diabetic rats (Figure 9) [110].
3.2. Positron Emission Tomography (PET) Imaging
For pre-clinical research, SPECT provides a slightly higher resolution (~1 mm) and more isotopes for radiotracer chemistries. However, for clinical imaging, PET scanners have a better spatial resolution (3–5 mm) compared to SPECT scanners (5–12 mm) [119]. Moreover, PET isotopes offer better image quality at lower injected radioactivity doses due to higher sensitivity and shorter half-lives of the radionuclides [120]. Thus, PET imaging is a commonly used clinical imaging technique to diagnose tumors, infections, and neurological function [121].
One of the most exploited PET radiopharmaceutical is glucose fluorinated with the PET-isotope Fluorine-18 (18F-FDG), which functions as a glucose analog and is used to diagnose cancer [122,123], inflammation and infection [124], and neurodegenerative diseases such as dementia [125]. 18F-FDG displays changes in glucose metabolism and tissue accumulation in both animals and humans. Chuang et al. have developed an oral combination therapy with nanoparticles loaded with insulin and exendin-4 (an analog of GLP-1) to treat type 2 diabetes in rats [126]. When released from the nanoparticles, the drugs stimulate the glucose transporter 4 to translocate from its intracellular location to the plasma membrane and facilitate glucose diffusion into the cells. The researchers used 18F-FDG to image and quantify the glucose uptake into the heart and muscle 2 h after oral ingestion of the combination nanoparticles. Dynamic PET scans (Figure 10) show high utilization of 18F-FDG in the nanoparticles containing insulin or a combination of insulin and exendin-4, validating the pharmacodynamic efficacy of these nanoparticle DDS [126].
18F-FDG PET imaging has also been used to study the effects of different small proteins after oral administration [127]. For example, chemotherapy-induced neutropenia can be reduced and recovery accelerated in cancer patients by orally administering granulocyte colony-stimulating factor (G-CSF) in chitosan nanoparticles. As an increased glucose uptake is often observed in the bone marrow during and after G-CSF therapy, Su et al. investigated this in rats after giving the drug subcutaneously, orally, and orally encapsulated in nanoparticles (Figure 11A) [128]. Packing G-CSF into nanoparticles and giving them orally increased the glucose metabolism in the bone marrow more than two-fold over the orally given free G-CSF (Figure 11B) [128]. However, a significantly larger (9-fold) dose had to be given orally to reach similar effects to the subcutaneous administration.
To investigate antimicrobial compounds in small animals, researchers from Stanford University labeled peptoids with 64Cu (Table 3) and determined the biodistribution of the peptoids by PET imaging [129]. Peptoids, or oligo-N-substituted glycines, are a novel class of polymers that mimic peptides and proteins but have a more stable molecular structure and higher bioavailability compared to natural peptides [130,131]. They also display increased cell permeability and can avoid immune recognition [132,133]. After developing three novel cationic amphipathic peptoids and studying their biodistribution after intravenous injection, the first peptoid termed 64Cu-1 was chosen for further study after oral and intraperitoneal administration in mice. It consisted of a cationic amphipathic peptoid conjugated with N-terminal 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA) and labeled with 64Cu. Peroral 64Cu-1 showed only gastrointestinal activity and eventual elimination after 24 h, with almost no systemic absorption (Figure 12) [129].
4. Conclusions and Future Developments
In this review, we established that studying the oral delivery of peptides in animals is difficult and should be conducted more often with nuclear imaging techniques which are highly sensitive at low therapeutic doses, quantifies organ activity (percentage of dose per organ) in real-time, provides early physiological information, allows for easy study of disease progression, and detects abnormalities during GI transit and/or circulation reliably [137]. Commonly used techniques such as biodistribution studies, microscopy, and MRI either do not allow for real-time analysis over extended time periods or do not provide accurate quantification of peptide uptake [138].
Additional benefits of nuclear imaging include the possibility of dual isotope imaging, theranostic applications, and obtaining immediate feedback on the success of the treatment (Figure 13). Dual isotope imaging helps to concurrently image the carrier as well as the peptide after radiolabeling them with radioisotopes of different gamma radiation energies. Subsequently, the peptide uptake mechanism and DDS clearance can be investigated in vivo fully quantitatively, leading to an improved understanding of peptide pharmacokinetics [55]. In theranostic applications, α- and β-emitting radioisotopes can be orally delivered to impart site-specific radiotherapy, in combination with γ-radioisotopes that provide diagnostic information about the molecular environment and report the success of the therapeutic intervention [139]. A milestone in nuclear imaging has been the development of fusion imaging, whereby SPECT and/or PET is superimposed with CT or MRI images to display anatomical and functional pharmacological properties of peptides concurrently in the same animal over time [139]. PET and SPECT imaging thus helps to translate work from pre-clinical to clinical research and speeds up getting to first human trials.
While nuclear imaging has many benefits, there are some limitations as well [140]. For instance, the spatial resolution of PET and SPECT imaging is lower than MRI and optical techniques; however, recent scanners are starting to bridge this gap [141]. Another drawback of nuclear imaging is the handling and exposure to ionizing radiation that requires radiation safety precautions [141]. Recent PET technology provides whole-body imaging at 40× lower radiation doses with shorter acquisition times, hence reducing potential tissue damage in humans significantly [142,143]. Furthermore, peptide pre-targeting followed by in vivo ‘click chemistry’ also reduces the radiation exposure as the peptide DDS is first delivered to the target site followed by the administration of a short half-life radioisotope which clicks covalently to the peptide in vivo, and can then be imaged or deliver treatment with minimal exposure [144].
In summary, oral delivery of peptides can be well studied and quantified with nuclear imaging and should be used more during early pilot studies and the development of novel peptide DDS. However, the literature review discussed in this review makes it evident that very limited nuclear imaging research has been performed until now. One major reason for this could be that the radiolabeling of drugs and DDS and its imaging in SPECT or PET cameras are rather specialized. While availability is limited, collaborating with experts in the field might yield excellent results [59]. Another reason for not using nuclear imaging to study oral peptide delivery could be that contrast of the gastrointestinal tract is low and prevents precise localization of the peptide in the different GI tract areas. The application of Artificial Intelligence (AI) is an ingenious way to solve this problem as the entire GI tract can be mapped, giving the exact location of peptide uptake, its quantification, and analysis within minutes. This is very similar to already existing techniques such as brain mapping of PET images [145]. Many recent examples from medical imaging support the notion that we are only at the beginning of gaining additional information from the use of AI, information that adds valuable data points to the trained eye of radiologists [146] and should be applied in the near future for gastrointestinal imaging.
When faced with a plethora of parameters and challenges during oral delivery, nuclear imaging can help to understand early on the in vivo path of a novel oral peptide DDS over time in groups of small numbers of animals. Nuclear imaging thus contributes an effective and fully quantitative tool to study the pharmacokinetic and pharmacodynamic profile of oral peptide formulations.
Author Contributions
Conceptualization, T.S. and U.O.H.; literature search T.S., C.S., K.L. and D.Y.; writing—original draft preparation T.S., C.S., K.L. and D.Y.; figures T.S.; editing and final version T.S., K.S. and U.O.H. All authors have read and agreed to the published version of the manuscript.
Funding
This review was made possible by funding from the Novo Nordisk Foundation for the Center for Biopharmaceuticals and Biobarriers in Drug Delivery (BioDelivery; Grand Challenge Program; NNF16OC0021948) and from the Lundbeck Foundation of Denmark (UBC-SUND Lundbeck Foundation Professorship to UOH; project number 2014-4176).
Acknowledgments
T.S. acknowledges the financial support by SERB (Science and Engineering Research Board), India. The authors acknowledge Lydia Cartar, Ben Last, Nojoud Al Fayez, and Nishith Saxena for proofreading and their feedback on the review. Figure 2, Figure 3, Figure 4 and Figure 5 and the graphical abstract were created with BioRender.com.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bhutani, P.; Joshi, G.; Raja, N.; Bachhav, N.; Rajanna, P.K.; Bhutani, H.; Paul, A.T.; Kumar, R.U.S. FDA Approved Drugs from June 2015–2020: A Perspective. J. Med. Chem. 2021, 64, 2339–2381. [Google Scholar] [CrossRef] [PubMed]
- Vllasaliu, D.; Thanou, M.; Stolnik, S.S.; Fowler, R. Recent advances in oral delivery of biologics: Nanomedicine and physical modes of delivery. Expert Opin. Drug Deliv. 2018, 15, 759–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duran-Lobato, M.; Niu, Z.; Alonso, M.J. Oral Delivery of Biologics for Precision Medicine. Adv. Mater. 2020, 32, e1901935. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, K., II. Needle phobia: A psychological perspective. Br. J. Anaesth. 2014, 113, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, M.; Gomez-Orellana, I. Challenges for the oral delivery of macromolecules. Nat. Rev. Drug Discov. 2003, 2, 289–295. [Google Scholar] [CrossRef]
- Innamudin; Asiri, A.; Mohammad, A. Applications of Nanocomposite Materials in Drug Delivery; Woodhead Publishing: Sawston, UK, 2018. [Google Scholar]
- Usmani, S.S.; Bedi, G.; Samuel, J.S.; Singh, S.; Kalra, S.; Kumar, P.; Ahuja, A.A.; Sharma, M.; Gautam, A.; Raghava, G.P.S. THPdb: Database of FDA-approved peptide and protein therapeutics. PLoS ONE 2017, 12, e0181748. [Google Scholar] [CrossRef] [Green Version]
- Bakhru, S.H.; Furtado, S.; Morello, A.P.; Mathiowitz, E. Oral delivery of proteins by biodegradable nanoparticles. Adv. Drug Deliv. Rev. 2013, 65, 811–821. [Google Scholar] [CrossRef]
- Thanki, K.; Gangwal, R.P.; Sangamwar, A.T.; Jain, S. Oral delivery of anticancer drugs: Challenges and opportunities. J. Control. Release 2013, 170, 15–40. [Google Scholar] [CrossRef]
- Rogers, K. What Is the Difference between a Peptide and a Protein? Available online: https://www.britannica.com/story/what-is-the-difference-between-a-peptide-and-a-protein (accessed on 1 December 2022).
- Patel, H.M.; Ryman, B.E. Oral administration of insulin by encapsulation within liposomes. FEBS Lett. 1976, 62, 60–63. [Google Scholar] [CrossRef] [Green Version]
- IDF Diabetes Atlas. Available online: https://www.diabetesatlas.org/ (accessed on 6 September 2022).
- Shah, R.B.; Shah, V.N.; Patel, M.; Maahs, D.M. Insulin delivery methods: Past, present and future. Int. J. Pharm. Investig. 2016, 6, 1–9. [Google Scholar] [CrossRef]
- Lewis, A.L.; McEntee, N.; Holland, J.; Patel, A. Development and approval of rybelsus (oral semaglutide): Ushering in a new era in peptide delivery. Drug Deliv. Transl. Res. 2022, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Meier, J.J. Efficacy of Semaglutide in a Subcutaneous and an Oral Formulation. Front. Endocrinol. 2021, 12, 645617. [Google Scholar] [CrossRef] [PubMed]
- Safety Data from RYBELSUS® (Semaglutide) Clinical Trials. Available online: https://www.novomedlink.com/diabetes/products/treatments/rybelsus/efficacy-safety/safety-data.html (accessed on 14 November 2022).
- des Rieux, A.; Fievez, V.; Garinot, M.; Schneider, Y.J.; Préat, V. Nanoparticles as potential oral delivery systems of proteins and vaccines: A mechanistic approach. J. Control. Release 2006, 116, 1–27. [Google Scholar] [CrossRef]
- Su, S.; Peter, M.K. Recent Advances in Nanocarrier-Assisted Therapeutics Delivery Systems. Pharmaceutics 2020, 12, 837. [Google Scholar] [CrossRef] [PubMed]
- Vila, A.; Sánchez, A.; Tobío, M.; Calvo, P.; Alonso, M. Design of biodegradable particles for protein delivery. J. Control. Release 2002, 78, 15–24. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Fact Sheet: FDA at a Glance, 2020 ed.; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2020.
- Kapoor, P.; Singh, H.; Gautam, A.; Chaudhary, K.; Kumar, R.; Raghava, G.P.S. TumorHoPe: A database of tumor homing peptides. PLoS ONE 2012, 7, e35187. [Google Scholar] [CrossRef] [Green Version]
- Gautam, A.; Singh, H.; Tyagi, A.; Chaudhary, K.; Kumar, R.; Kapoor, P.; Raghava, G.P.S. CPPsite: A curated database of cell penetrating peptides. Database 2012, 2012, bas015. [Google Scholar] [CrossRef] [Green Version]
- Tzotzos, S.J. Peptide Drugs of the Decade. The European Peptide Society. 2020. Available online: www.eurpepsoc.com (accessed on 10 July 2022).
- Aguirre, T.; Teijeiro-Osorio, D.; Rosa, M.; Coulter, I.; Alonso, M.; Brayden, D. Current status of selected oral peptide technologies in advanced preclinical development and in clinical trials. Adv. Drug Deliv. Rev. 2016, 106, 223–241. [Google Scholar] [CrossRef] [Green Version]
- Dubey, S.K.; Parab, S.; Dabholkar, N.; Agrawal, M.; Singhvi, G.; Alexander, A.; Bapat, R.A.; Kesharwani, P. Oral peptide delivery: Challenges and the way ahead. Drug Discov. Today 2021, 26, 931–950. [Google Scholar] [CrossRef]
- Houben, A.J.M.; Oostdijk, E.A.N.; van der Voort, P.H.J.; Monen, J.C.M.; Bonten, M.J.M.; Van der Bij, A.K.; Vlaspolder, F.; Stuart, J.W.T.C.; van Hees, B.C. Selective decontamination of the oropharynx and the digestive tract, and antimicrobial resistance: A 4 year ecological study in 38 intensive care units in the Netherlands. J. Antimicrob. Chemoth. 2014, 69, 797–804. [Google Scholar] [CrossRef]
- Park, K.; Koh, Y.B.; Kwak, J.Y.; Kim, S.J.; Yoon, Y.S.; Kang, C.M.; Kim, Y.S. An open randomized parallel group study to compare Sandimmune Neoral with Sandimmune soft gelatin capsule in stable renal transplant patients. Transpl. Proc. 1996, 28, 1202–1203. [Google Scholar]
- Weinberg, R.S.; Grecco, M.O.; Ferro, G.S.; Seigelshifer, D.J.; Perroni, N.V.; Terrier, F.J.; Sánchez-Luceros, A.; Maronna, E.; Sánchez-Marull, R.; Frahm, I.; et al. A phase II dose-escalation trial of perioperative desmopressin (1-desamino-8-d-arginine vasopressin) in breast cancer patients. SpringerPlus 2015, 4, 428. [Google Scholar] [CrossRef] [Green Version]
- Visca, A.; Bishop, C.T.; Hilton, S.; Hudson, V.M. Oral reduced L-glutathione improves growth in pediatric cystic fibrosis patients. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awasthi, S.; Pandya, U.; Singhal, S.S.; Lin, J.T.; Thiviyanathan, V.; Seifert, W.E.; Awasthi, Y.C.; Ansari, G. Curcumin-glutathione interactions and the role of human glutathione S-transferase P1-1. Chem. Biol. Interact. 2000, 128, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Lembo, A.J.; Lavins, B.J.; Shiff, S.J.; Kurtz, C.B.; Currie, M.G. Linaclotide for irritable bowel syndrome with constipation: A 26-week, randomized, double-blind, placebo-controlled trial to evaluate efficacy and safety. Am. J. Gastroenterol. 2012, 107, 1702–1712. [Google Scholar]
- Chey, W.D.; Lembo, A.J.; Lavins, B.J.; Shiff, S.J.; Kurtz, C.B.; Currie, M.G.; MacDougall, J.E.; Jia, X.D.; Shao, J.Z.; Fitch, D.A.; et al. Maintenance of Acromegaly Control in Patients Switching From Injectable Somatostatin Receptor Ligands to Oral Octreotide. J. Clin. Endocrinol. Metab. 2020, 107, 1702–1712. [Google Scholar]
- Welzel, T.M.; Hinrichsen, H.; Sarrazin, C.; Buggisch, P.; Baumgarten, A.; Christensen, S.; Berg, T.; Mauss, S.; Teuber, G.; Stein, K.; et al. Real-world experience with the all-oral, interferon-free regimen of ombitasvir/paritaprevir/ritonavir and dasabuvir for the treatment of chronic hepatitis C virus infection in the German Hepatitis C Registry. J. Viral Hepat. 2017, 24, 840–849. [Google Scholar] [CrossRef]
- Treem, W.R.; McAdams, L.; Stanford, L.; Kastoff, G.; Justinich, C.; Hyams, J. Sacrosidase therapy for congenital sucrase-isomaltase deficiency. J. Pediatr. Gastroenterol. Nutr. 1999, 28, 137–142. [Google Scholar] [CrossRef]
- Semenya, A.M.; Wilson, S.A. Oral Semaglutide (Rybelsus) for the Treatment of Type 2 Diabetes Mellitus. Am. Fam. Physician 2020, 102, 627–628. [Google Scholar]
- Aroda, V.R.; Rosenstock, J.; Terauchi, Y.; Altuntas, Y.; Lalic, N.M.; Villegas, E.C.M.; Jeppesen, O.K.; Christiansen, E.; Hertz, C.L.; Haluzík, M.; et al. PIONEER 1: Randomized Clinical Trial of the Efficacy and Safety of Oral Semaglutide Monotherapy in Comparison With Placebo in Patients With Type 2 Diabetes. Diabetes Care 2019, 42, 1724–1732. [Google Scholar] [CrossRef]
- Urayama, A.; Yamada, S.; Kimura, R.; Zhang, J.; Watanabe, Y. Neuroprotective effect and brain receptor binding of taltirelin, a novel thyrotropin-releasing hormone (TRH) analogue, in transient forebrain ischemia of C57BL/6J mice. Life Sci. 2002, 72, 601–607. [Google Scholar] [CrossRef]
- Stauss-Grabo, M.; Atiye, S.; Le, T.; Kretschmar, M. Decade-long use of the antimicrobial peptide combination tyrothricin does not pose a major risk of acquired resistance with gram-positive bacteria and Candida spp. Pharmazie 2014, 69, 838–841. [Google Scholar] [PubMed]
- Anderson, K.E.; Eliot, L.A.; Stevenson, B.R.; Rogers, J.A. Formulation and evaluation of a folic acid receptor-targeted oral vancomycin liposomal dosage form. Pharm. Res. 2001, 18, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Beasley, D.; Koltz, A.M.; Lambert, J.E.; Fierer, N.; Dunn, R. The Evolution of Stomach Acidity and Its Relevance to the Human Microbiome. PLoS ONE 2015, 10, e0134116. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Eskilsson, A.; Nilsson, C.; Jonsson, C.; Jacobsson, H.; Refai, E.; Larsson, S.; Efendic, S. In vivo dynamic distribution of 131I-glucagon-like peptide-1 (7-36) amide in the rat studied by gamma camera. Nucl. Med. Biol. 1999, 26, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Chen, Z.; Paul, P.K.; Lu, Y.; Wu, W.; Qi, J. Oral delivery of proteins and peptides: Challenges, status quo and future perspectives. Acta Pharm. Sin. B 2021, 11, 2416–2448. [Google Scholar] [CrossRef]
- Philomena, S. Study: Oral Calcitonin Tablet is Effective and Safe. Clinical Trials News, Medindia. 2011. Available online: https://www.medindia.net/news/study-oral-calcitonin-tablet-is-safe-and-effective-90770-1.htm (accessed on 1 December 2022).
- Mathiowitz, E.J.J.S.; Jong, Y.S.; Carino, G.P.; Chickering, D.E.; Chaturvedi, P.; Santos, C.A.; Vijayaraghavan, K.; Montgomery, S.; Bassett, M.; Morrel, C. Biologically erodible microspheres as potential oral drug delivery systems. Nature 1997, 386, 410–414. [Google Scholar] [CrossRef]
- Drakos, S.G.; Kfoury, A.G.; Stehlik, J.; Selzman, C.H.; Reid, B.B.; Terrovitis, J.V. Bridge to recovery: Understanding the disconnect between clinical and biological outcomes. Circulation 2012, 126, 230–241. [Google Scholar] [CrossRef] [Green Version]
- Gamboa, J.M.; Leong, K.W. In vitro and in vivo models for the study of oral delivery of nanoparticles. Adv. Drug Deliv. Rev. 2013, 65, 800–810. [Google Scholar] [CrossRef] [Green Version]
- Tyler, D.; Brown, K.A.W.S.M. Materials for oral delivery of proteins and peptides. Nat. Rev. Mater. 2019, 5, 127–148. [Google Scholar]
- Hamman, J.H.; Enslin, G.M.; Kotze, A.F. Oral delivery of peptide drugs: Barriers and developments. BioDrugs 2005, 19, 165–177. [Google Scholar] [CrossRef]
- Muheem, A.; Shakeel, F.; Jahangir, M.A.; Anwar, M.; Mallick, N.; Jain, G.K.; Warsi, M.H.; Ahmad, F.J. A review on the strategies for oral delivery of proteins and peptides and their clinical perspectives. Saudi. Pharm. J. 2016, 24, 413–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.H.; Han, H.K. Nanomedicines: Current status and future perspectives in aspect of drug delivery and pharmacokinetics. J. Pharm. Investig. 2018, 48, 43–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medarova, Z.; Evgenov, N.V.; Dai, G.; Bonner-Weir, S.; Moore, A. In vivo multimodal imaging of transplanted pancreatic islets. Nat. Protoc. 2006, 1, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Louchami, K.; Holvoet, B.; Verbeke, R.; Deroose, C.M.; Manshian, B.; Soenen, S.J.; Lentacker, I.; Himmelreich, U. Tri-modal In vivo Imaging of Pancreatic Islets Transplanted Subcutaneously in Mice. Mol. Imaging Biol. 2018, 20, 940–951. [Google Scholar] [CrossRef]
- Hofherr, S.E.; Adams, K.E.; Chen, C.Y.; May, S.; Weaver, E.A.; Barry, M.A. Real-time dynamic imaging of virus distribution in vivo. PLoS ONE 2011, 6, e17076. [Google Scholar] [CrossRef] [Green Version]
- Berroa, F.; Gastaminza, G.; Saiz, N.; Azofra, J.; Gamboa, P.M.; Vela, C.; García, B.E.; Lizarza, S.; Echenagusia, M.A.; Joral, A.; et al. In vivo and in vitro techniques in the diagnosis of lipid transfer protein sensitization. Ann. Allergy Asthma Immunol. 2013, 111, 571–573. [Google Scholar] [CrossRef]
- Sonaje, K.; Lin, K.J.; Wey, S.P.; Lin, C.K.; Yeh, T.H.; Nguyen, H.N. Biodistribution, pharmacodynamics and pharmacokinetics of insulin analogues in a rat model: Oral delivery using pH-responsive nanoparticles vs. subcutaneous injection. Biomaterials 2010, 31, 6849–6858. [Google Scholar] [CrossRef]
- Najafzadeh, H.; Kooshapur, H.; Kianidehkordi, F. Evaluation of an oral insulin formulation in normal and diabetic rats. Indian J. Pharmacol. 2012, 44, 103–105. [Google Scholar] [CrossRef] [Green Version]
- Dapergolas, G.; Gregoriadis, G. Hypoglycaemic effect of liposome-entrapped insulin administered intragastrically into rats. Lancet 1976, 2, 824–827. [Google Scholar] [CrossRef]
- Wright, E.E., Jr.; Aroda, V.R. Clinical review of the efficacy and safety of oral semaglutide in patients with type 2 diabetes considered for injectable GLP-1 receptor agonist therapy or currently on insulin therapy. Postgrad. Med. 2020, 132, 26–36. [Google Scholar] [CrossRef]
- Wallyn, J.; Anton, N.; Akram, S.; Vandamme, T.F. Biomedical Imaging: Principles, Technologies, Clinical Aspects, Contrast Agents, Limitations and Future Trends in Nanomedicines. Pharm. Res. 2019, 36, 78. [Google Scholar] [CrossRef] [PubMed]
- Schillaci, O. Hybrid SPECT/CT: A new era for SPECT imaging? Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Meester, E.J.; Krenning, B.J.; De Swart, J.; Segbers, M.; Barrett, H.E.; Bernsen, M.R.; Van Der Heiden, K.; De Jong, M. Perspectives on Small Animal Radionuclide Imaging; Considerations and Advances in Atherosclerosis. Front. Med. 2019, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Szymanski, C.; Wang, Z.; Zhou, Y.; Ma, X.; Yu, J.; Evans, J.; Orr, G.; Liu, S.; Zhu, Z.; et al. Chemical imaging of molecular changes in a hydrated single cell by dynamic secondary ion mass spectrometry and super-resolution microscopy. Integr. Biol. 2016, 8, 635–644. [Google Scholar] [CrossRef]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; del Pilar Rodriguez-Torres, M.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Ali, Y.; Lehmussaari, K. Industrial perspective in ocular drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1258–1268. [Google Scholar] [CrossRef]
- Freiberg, S.; Zhu, X.X. Polymer microspheres for controlled drug release. Int. J. Pharm. 2004, 282, 1–18. [Google Scholar] [CrossRef]
- Vasir, J.K.; Tambwekar, K.; Garg, S. Bioadhesive microspheres as a controlled drug delivery system. Int. J. Pharm. 2003, 255, 13–32. [Google Scholar] [CrossRef]
- Zhang, B.; He, D.; Fan, Y.; Liu, N.; Chen, Y. Oral delivery of exenatide via microspheres prepared by cross-linking of alginate and hyaluronate. PLoS ONE 2014, 9, e86064. [Google Scholar] [CrossRef] [Green Version]
- Deamer, D.W. From "banghasomes" to liposomes: A memoir of Alec Bangham, 1921–2010. FASEB J. 2010, 24, 1308–1310. [Google Scholar] [CrossRef]
- Hashimoto, A.; Kawada, J. Effects of oral administration of positively charged insulin liposomes on alloxan diabetic rats: Preliminary study. Endocrinol. Jpn. 1979, 26, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrieta-Molero, J.F.; Aleck, K.; Sinha, M.K.; Brownscheidle, C.M.; Shapiro, L.J.; Sperling, M.A. Orally administered liposome-entrapped insulin in diabetic animals. A critical assessment. Horm. Res. 1982, 16, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Willis, M.; Forssen, E. Ligand-targeted liposomes. Adv. Drug Deliv. Rev. 1998, 29, 249–271. [Google Scholar] [PubMed]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, preparation, and applications. Nanoscale Res. Lett. 2013, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Filipczak, N.; Pan, J.; Yalamarty, S.S.K.; Torchilin, V.P. Recent advancements in liposome technology. Adv. Drug Deliv. Rev. 2020, 156, 4–22. [Google Scholar] [CrossRef]
- He, H.; Lu, Y.; Qi, J.; Zhu, Q.; Chen, Z.; Wu, W. Adapting liposomes for oral drug delivery. Acta Pharm. Sin. B 2019, 9, 36–48. [Google Scholar] [CrossRef]
- Rogers, J.A.; Anderson, K.E. The potential of liposomes in oral drug delivery. Crit. Rev. Ther. Drug Carr. Syst. 1998, 15, 421–480. [Google Scholar] [CrossRef]
- Okada, J.; Cohen, S.; Langer, R. In vitro evaluation of polymerized liposomes as an oral drug delivery system. Pharm. Res. 1995, 12, 576–582. [Google Scholar] [CrossRef]
- Soares, A.F.; Carvalho Rde, A.; Veiga, F. Oral administration of peptides and proteins: Nanoparticles and cyclodextrins as biocompatible delivery systems. Nanomedicine 2007, 2, 183–202. [Google Scholar] [CrossRef]
- Benergossi, J.; Calixto, G.; Fonseca-Santos, B.; Aida, K.; Negrini, T.; Duque, C.; Gremião, M.; Chorilli, M. Highlights in peptide nanoparticle carriers intended to oral diseases. Curr. Top Med. Chem. 2015, 15, 345–355. [Google Scholar] [CrossRef]
- Khutoryanskiy, V.V. Advances in mucoadhesion and mucoadhesive polymers. Macromol. Biosci. 2011, 11, 748–764. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Ping, Q.; Huang, G.; Xu, W.; Cheng, Y.; Han, X. Lectin-modified solid lipid nanoparticles as carriers for oral administration of insulin. Int. J. Pharm. 2006, 327, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.W.; Sonaje, K.; Liao, Z.X.; Hsu, L.W.; Chuang, E.Y. pH-responsive nanoparticles shelled with chitosan for oral delivery of insulin: From mechanism to therapeutic applications. Acc. Chem. Res. 2012, 45, 619–629. [Google Scholar] [CrossRef]
- Matalqah, S.M.; Aiedeh, K.; Mhaidat, N.M.; Alzoubi, K.H.; Bustanji, Y.; Hamad, I. Chitosan Nanoparticles as a Novel Drug Delivery System: A Review Article. Curr. Drug Targets 2020, 21, 1613–1624. [Google Scholar] [CrossRef]
- Sultankulov, B.; Berillo, D.; Sultankulova, K.; Tokay, T.; Saparov, A. Progress in the Development of Chitosan-Based Biomaterials for Tissue Engineering and Regenerative Medicine. Biomolecules 2019, 9, 470. [Google Scholar] [CrossRef] [Green Version]
- Damge, C.; Maincent, P.; Ubrich, N. Oral delivery of insulin associated to polymeric nanoparticles in diabetic rats. J. Control. Release 2007, 117, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Yousefpour Marzbali, M.; Yari Khosroushahi, A. Polymeric micelles as mighty nanocarriers for cancer gene therapy: A review. Cancer Chemother. Pharmacol. 2017, 79, 637–649. [Google Scholar] [CrossRef]
- Onoue, S.; Yamada, S.; Chan, H.K. Nanodrugs: Pharmacokinetics and safety. Int. J. Nanomed. 2014, 9, 1025–1037. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Farrell, S.; Uhrich, K. Drug release characteristics of unimolecular polymeric micelles. J. Control. Release 2000, 68, 167–174. [Google Scholar] [CrossRef]
- Mandal, A.; Bisht, R.; Rupenthal, I.D.; Mitra, A.K. Polymeric micelles for ocular drug delivery: From structural frameworks to recent preclinical studies. J. Control. Release 2017, 248, 96–116. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Long, Y.; Guo, R.; Liu, X.; Tang, X.; Rao, J.; Yin, S.; Zhang, Z.; Li, M.; He, Q. Multifunctional polymeric micelle-based chemo-immunotherapy with immune checkpoint blockade for efficient treatment of orthotopic and metastatic breast cancer. Acta Pharm. Sin. B. 2019, 9, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Li, X.-R.; Zhou, Y.-X.; Li, W.-J.; Zhao, Y.; Ma, S.-J.; Li, J.-W.; Gao, Y.-J.; Liu, Y.; Wang, X.-L.; et al. The use of polyion complex micelles to enhance the oral delivery of salmon calcitonin and transport mechanism across the intestinal epithelial barrier. Biomaterials 2012, 33, 8881–8892. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Lu, Y.; Xie, J.; Zhang, E.; Zhu, H.; Du, H.; Wang, K.; Song, B.; Yang, C.; Shi, Y.; et al. Zwitterionic micelles efficiently deliver oral insulin without opening tight junctions. Nat. Nanotechnol. 2020, 15, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.K.; Wang, Y.Y.; Hanes, J. Mucus-penetrating nanoparticles for drug and gene delivery to mucosal tissues. Adv. Drug Deliv. Rev. 2009, 61, 158–171. [Google Scholar] [CrossRef]
- Cao, Z.; Zhang, L.; Jiang, S. Superhydrophilic zwitterionic polymers stabilize liposomes. Langmuir 2012, 28, 11625–11632. [Google Scholar] [CrossRef] [PubMed]
- Thwaites, D.T.; Anderson, C.M. The SLC36 family of proton-coupled amino acid transporters and their potential role in drug transport. Br. J. Pharmacol. 2011, 164, 1802–1816. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Yue, Z.; Xie, J.; Wang, W.; Zhu, H.; Zhang, E.; Cao, Z. Micelles with ultralow critical micelle concentration as carriers for drug delivery. Nat. Biomed. Eng. 2018, 2, 318–325. [Google Scholar] [CrossRef]
- Peppas, N.A.; Wood, K.M.; Blanchette, J.O. Hydrogels for oral delivery of therapeutic proteins. Expert Opin. Biol. Ther. 2004, 4, 881–887. [Google Scholar] [CrossRef]
- Sharpe, A.L.; Daily, A.M.; Horava, S.D.; Peppas, N.A. Therapeutic applications of hydrogels in oral drug delivery. Expert Opin. Drug Deliv. 2014, 11, 901–915. [Google Scholar] [CrossRef] [Green Version]
- He, C.; Cui, F.; Yin, L.; Qian, F.; Tang, C.; Yin, C. A polymeric composite carrier for oral delivery of peptide drugs: Bilaminated hydrogel film loaded with nanoparticles. Eur. Polym. J. 2009, 45, 368–376. [Google Scholar] [CrossRef]
- Lemon, W.C.; McDole, K. Live-cell imaging in the era of too many microscopes. Curr. Opin. Cell Biol. 2020, 66, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Shcherbakova, D.M.; Baloban, M.; Emelyanov, A.V.; Brenowitz, M.; Guo, P.; Verkhusha, V.V. Bright monomeric near-infrared fluorescent proteins as tags and biosensors for multiscale imaging. Nat. Commun. 2016, 7, 12405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, E.W.; Orvig, C. Matching chelators to radiometals for radiopharmaceuticals. Chem. Soc. Rev. 2014, 43, 260–290. [Google Scholar] [CrossRef] [PubMed]
- Radionuclide Scanning. Available online: https://www.drugs.com/health-guide/radionuclide-scanning.html (accessed on 1 December 2022).
- Bandara, N.; Zheleznyak, A.; Cherukuri, K.; Griffith, D.A.; Limberakis, C.; Tess, D.A. Evaluation of Cu-64 and Ga-68 Radiolabeled Glucagon-Like Peptide-1 Receptor Agonists as PET Tracers for Pancreatic beta cell Imaging. Mol. Imaging Biol. 2016, 18, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Cicone, F.; Malviya, G.; Sambuceti, G. Editorial: Perspectives in Small Animal Radionuclide Imaging. Front. Med. 2020, 7, 262. [Google Scholar] [CrossRef] [PubMed]
- Fani, M.; Maecke, H.R. Radiopharmaceutical development of radiolabelled peptides. Eur. J. Nucl. Med. Mol. Imaging 2012, 39 (Suppl. S1), S11–S30. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.T.; Guo, J.; Presas, E.; Donovan, M.D.; Alonso, M.J.; O’Driscoll, C.M. Pharmacokinetic, pharmacodynamic and biodistribution following oral administration of nanocarriers containing peptide and protein drugs. Adv. Drug Deliv. Rev. 2016, 106, 367–380. [Google Scholar] [CrossRef]
- Niu, Z.; Samaridou, E.; Jaumain, E.; Coëne, J.; Ullio, G.; Shrestha, N.; Garcia, J.; Durán-Lobato, M.; Tovar, S.; Santander-Ortega, M.J.; et al. PEG-PGA enveloped octaarginine-peptide nanocomplexes: An oral peptide delivery strategy. J. Control. Release 2018, 276, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Kalomoiri, P.; Rodríguez-Rodríguez, C.; Sørensen, K.K.; Bergamo, M.; Saatchi, K.; Häfeli, U.O.; Jensen, K.J. Bioimaging and Biodistribution of the Metal-Ion-Controlled Self-Assembly of PYY3-36 Studied by SPECT/CT. ChemBioChem 2020, 21, 3338–3348. [Google Scholar] [CrossRef]
- Kim, C.C.; Falkow, S. Delineation of upstream signaling events in the salmonella pathogenicity island 2 transcriptional activation pathway. J. Bacteriol. 2004, 186, 4694–4704. [Google Scholar] [CrossRef] [Green Version]
- Chuang, E.-Y.; Lin, K.-J.; Su, F.-Y.; Chen, H.-L.; Maiti, B.; Ho, Y.-C.; Yen, T.-C.; Panda, N.; Sung, H.-W. Calcium depletion-mediated protease inhibition and apical-junctional-complex disassembly via an EGTA-conjugated carrier for oral insulin delivery. J. Control. Release 2013, 169, 296–305. [Google Scholar] [CrossRef]
- Morishita, M.; Goto, T.; Peppas, N.A.; Joseph, J.I.; Torjman, M.C.; Munsick, C. Mucosal insulin delivery systems based on complexation polymer hydrogels: Effect of particle size on insulin enteral absorption. J. Control. Release 2004, 97, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.C.; Laskowski, M. The effect of calcium on chymotrypsins alpha and B. Biochim. Biophys. Acta 1956, 19, 110–115. [Google Scholar] [CrossRef]
- Shen, L.; Zhao, H.-Y.; Du, J.; Wang, F. Anti-tumor activities of four chelating agents against human neuroblastoma cells. In Vivo 2005, 19, 233–236. [Google Scholar] [PubMed]
- AL-N, A.; Fanti, S. Radiolabelled peptides in diagnosis and therapy: An introduction. Eur. J. Nucl. Med. Mol. Imaging 2012, 39 (Suppl. S1), S1–S3. [Google Scholar]
- Tamborino, G.; Nonnekens, J.; Struelens, L.; De Saint-Hubert, M.; Verburg, F.A.; Konijnenberg, M.W. Therapeutic efficacy of heterogeneously distributed radiolabelled peptides: Influence of radionuclide choice. Phys. Med. 2022, 96, 90–100. [Google Scholar] [CrossRef]
- Wadas, T.J.; Wong, E.H.; Weisman, G.R.; Anderson, C.J. Coordinating radiometals of copper, gallium, indium, yttrium, and zirconium for PET and SPECT imaging of disease. Chem. Rev. 2010, 110, 2858–2902. [Google Scholar] [CrossRef] [Green Version]
- Jamous, M.; Haberkorn, U.; Mier, W. Synthesis of peptide radiopharmaceuticals for the therapy and diagnosis of tumor diseases. Molecules 2013, 18, 3379–3409. [Google Scholar] [CrossRef] [Green Version]
- Rinne, S.S.; Leitao, C.D.; Mitran, B.; Bass, T.Z.; Andersson, K.G.; Tolmachev, V.; Ståhl, S.; Löfblom, J.; Orlova, A. Optimization of HER3 expression imaging using affibody molecules: Influence of chelator for labeling with indium-111. Sci. Rep. 2019, 9, 655. [Google Scholar] [CrossRef] [Green Version]
- Rahmim, A.; Zaidi, H. PET versus SPECT: Strengths, limitations and challenges. Nucl. Med. Commun. 2008, 29, 193–207. [Google Scholar] [CrossRef] [Green Version]
- James, M.L.; Gambhir, S.S. A molecular imaging primer: Modalities, imaging agents, and applications. Physiol. Rev. 2012, 92, 897–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jodal, L.; Le Loirec, C.; Champion, C. Positron range in PET imaging: An alternative approach for assessing and correcting the blurring. Phys. Med. Biol. 2012, 57, 3931–3943. [Google Scholar] [CrossRef] [Green Version]
- Shooli, H.; Assadi, M.; Aboian, M. [18F]-FDG PET/MR Neuroimaging: Focus on Neuro-Oncology Applications. In Hybrid PET/MR Neuroimaging: A Comprehensive Approach; Franceschi, A.M., Franceschi, D., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 89–98. [Google Scholar]
- Singnurkar, A.; Poon, R.; Metser, U. Comparison of 18F-FDG-PET/CT and 18F-FDG-PET/MR imaging in oncology: A systematic review. Ann. Nucl. Med. 2017, 31, 366–378. [Google Scholar] [CrossRef]
- Casali, M.; Lauri, C.; Altini, C.; Bertagna, F.; Cassarino, G.; Cistaro, A.; Erba, A.P.; Ferrari, C.; Mainolfi, C.G.; Palucci, A.; et al. State of the art of (18)F-FDG PET/CT application in inflammation and infection: A guide for image acquisition and interpretation. Clin. Transl. Imaging 2021, 9, 299–339. [Google Scholar] [CrossRef] [PubMed]
- Calabria, F.; Cimini, A. 18F-FDG. In Radiopharmaceuticals: A Guide to PET/CT and PET/MRI; Calabria, F., Schillaci, O., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–36. [Google Scholar]
- Chuang, E.-Y.; Nguyen, G.T.H.; Su, F.-Y.; Lin, K.-J.; Chen, C.-T.; Mi, F.-L.; Yen, T.-C.; Juang, J.-H.; Sung, H.-W. Combination therapy via oral co-administration of insulin- and exendin-4-loaded nanoparticles to treat type 2 diabetic rats undergoing OGTT. Biomaterials 2013, 34, 7994–8001. [Google Scholar] [CrossRef]
- Rangger, C.; Haubner, R. Radiolabelled Peptides for Positron Emission Tomography and Endoradiotherapy in Oncology. Pharmaceuticals 2020, 13, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.-Y.; Chuang, E.-Y.; Lin, P.-Y.; Chou, Y.-C.; Chen, C.-T.; Mi, F.-L.; Wey, S.-P.; Yen, T.-C.; Lin, K.-J.; Sung, H.-W. Treatment of chemotherapy-induced neutropenia in a rat model by using multiple daily doses of oral administration of G-CSF-containing nanoparticles. Biomaterials 2014, 35, 3641–3649. [Google Scholar] [CrossRef]
- Seo, J.; Ren, G.; Liu, H.; Miao, Z.; Park, M.; Wang, Y. In vivo biodistribution and small animal PET of (64)Cu-labeled antimicrobial peptoids. Bioconju. Chem. 2012, 23, 1069–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, R.J.; Kania, R.S.; Zuckermann, R.N.; Huebner, V.D.; Jewell, D.A.; Banville, S.; Ng, S.; Wang, L.; Rosenberg, S.; Marlowe, C.K. Peptoids: A modular approach to drug discovery. Proc. Natl. Acad Sci. USA 1992, 89, 9367–9371. [Google Scholar] [CrossRef] [Green Version]
- Gobbo, M.; Benincasa, M.; Bertoloni, G.; Biondi, B.; Dosselli, R.; Papini, E.; Reddi, E.; Rocchi, R.; Tavano, R.; Gennaro, R. Substitution of the arginine/leucine residues in apidaecin Ib with peptoid residues: Effect on antimicrobial activity, cellular uptake, and proteolytic degradation. J. Med. Chem. 2009, 52, 5197–5206. [Google Scholar] [CrossRef]
- Kwon, Y.U.; Kodadek, T. Quantitative evaluation of the relative cell permeability of peptoids and peptides. J. Am. Chem. Soc. 2007, 129, 1508–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udugamasooriya, D.G.; Dineen, S.P.; Brekken, R.A.; Kodadek, T. A peptoid "antibody surrogate" that antagonizes VEGF receptor 2 activity. J. Am. Chem. Soc. 2008, 130, 5744–5752. [Google Scholar] [CrossRef] [PubMed]
- Koopmans, K.P.; Glaudemans, A.W. Rationale for the use of radiolabelled peptides in diagnosis and therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39 (Suppl. S1), S4–S10. [Google Scholar] [CrossRef] [PubMed]
- de Jong, M.; Visser, T.J.; de Blois, E.; Breeman, W.A.P.; Kwekkeboom, D.J.; Krenning, E.P. Radiolabelled regulatory peptides for imaging and therapy. Anticancer Agents Med.Chem. 2007, 7, 345–357. [Google Scholar] [CrossRef]
- Gaertner, F.C.; Kessler, H.; Wester, H.-J.; Schwaiger, M.; Beer, A.J. Radiolabelled RGD peptides for imaging and therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39 (Suppl. S1), S126–S138. [Google Scholar] [CrossRef] [PubMed]
- Soni, V.; Kohli, D.V.; Jain, S.K. Transferrin-conjugated liposomal system for improved delivery of 5-fluorouracil to brain. J. Drug Target 2008, 16, 73–78. [Google Scholar] [CrossRef]
- Man, F.; Gawne, P.J. RTMd. Nuclear imaging of liposomal drug delivery systems: A critical review of radiolabelling methods and applications in nanomedicine. Adv. Drug Deliv. Rev. 2019, 143, 134–160. [Google Scholar] [CrossRef]
- Stéen, E.J.L.; Edem, P.E.; Nørregaard, K.; Jørgensen, J.T.; Shalgunov, V.; Kjaer, A.; Herth, M.M. Pretargeting in nuclear imaging and radionuclide therapy: Improving efficacy of theranostics and nanomedicines. Biomaterials 2018, 179, 209–245. [Google Scholar] [CrossRef]
- Mather, S.J. Radiolabelled peptides--promises and pitfalls. Nucl. Med. Commun. 2000, 21, 507–509. [Google Scholar] [CrossRef]
- Southworth, R.; de Rosales, R.T.M.; Meszaros, L.K.; Ma, M.T.; Mullen, G.E.; Fruhwirth, G. Opportunities and challenges for metal chemistry in molecular imaging: From gamma camera imaging to PET and multimodality imaging. Adv. Inorg. Chem. 2016, 68, 1–41. [Google Scholar]
- Cherry, S.R.; Jones, T.; Karp, J.S.; Qi, J.; Moses, W.W.; Badawi, R.D. Total-Body PET: Maximizing Sensitivity to Create New Opportunities for Clinical Research and Patient Care. J. Nucl. Med. 2018, 59, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badawi, R.D.; Shi, H.; Hu, P.; Chen, S.; Xu, T.; Price, P.M.; Ding, Y.; Spencer, B.A.; Nardo, L.; Liu, W.; et al. First Human Imaging Studies with the EXPLORER Total-Body PET Scanner. J. Nucl. Med. 2019, 60, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Rossin, R.; Läppchen, T.; Bosch, S.M.V.D.; Laforest, R.; Robillard, M.S. Diels-Alder reaction for tumor pretargeting: In vivo chemistry can boost tumor radiation dose compared with directly labeled antibody. J. Nucl. Med. 2013, 54, 1989–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, D.; Egan, G.; O’Keefe, G.; Abbott, D. Characterization of dynamic 3-D PET imaging for functional brain mapping. IEEE Trans. Med. Imaging 1997, 16, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pie charts display the current distribution of FDA-approved peptide drugs based on their route of administration [7].
Figure 1.
Pie charts display the current distribution of FDA-approved peptide drugs based on their route of administration [7].

Figure 2.
Barriers to oral delivery of peptides.

Figure 3.
Schematic diagram of currently used drug delivery systems for oral delivery of peptides. (A). Liposome with possible physicochemical modifications: (i) Lipid composition of liposomes can be modified to include varying ratios of positive, negative, and neutral phospholipids, (ii) PEGylated phospholipids increase steric stability, (iii) Ligands such as antibodies, carbohydrates, and proteins can be added to the surface of liposomes for stability or specific targeting of a delivery system; (B). Self-assembled and solid lipid nanoparticles; (C). Micelle and polymeric micelle.
Figure 3.
Schematic diagram of currently used drug delivery systems for oral delivery of peptides. (A). Liposome with possible physicochemical modifications: (i) Lipid composition of liposomes can be modified to include varying ratios of positive, negative, and neutral phospholipids, (ii) PEGylated phospholipids increase steric stability, (iii) Ligands such as antibodies, carbohydrates, and proteins can be added to the surface of liposomes for stability or specific targeting of a delivery system; (B). Self-assembled and solid lipid nanoparticles; (C). Micelle and polymeric micelle.

Figure 4.
Conjugation of the drug molecule, e.g., an antibody, to a radioisotope using a chelator followed by oral gavage of the radiopharmaceuticals and biodistribution study in mice using SPECT/CT imaging in a preclinical scanner.
Figure 4.
Conjugation of the drug molecule, e.g., an antibody, to a radioisotope using a chelator followed by oral gavage of the radiopharmaceuticals and biodistribution study in mice using SPECT/CT imaging in a preclinical scanner.

Figure 5.
In vivo distribution of 131I-GLP-1 in a rat shortly after intravenous administration. Reprinted with permission from Hassan et al. (1999) [41].
Figure 5.
In vivo distribution of 131I-GLP-1 in a rat shortly after intravenous administration. Reprinted with permission from Hassan et al. (1999) [41].

Figure 6.
Oral biodistribution of 99mTc-enveloped nanocomplexes (ENCPs) and 99mTc pertechnetate (control) at 1, 2, 4, 8, 11, and 26 h using SPECT/CT imaging (A,B) and gamma counting (C,D) in Wistar rats (s = stomach, i = intestine, c = cecum, cl = colon, r = rectum, b = bladder). Reprinted with permission from Niu et al. (2018) [107].
Figure 6.
Oral biodistribution of 99mTc-enveloped nanocomplexes (ENCPs) and 99mTc pertechnetate (control) at 1, 2, 4, 8, 11, and 26 h using SPECT/CT imaging (A,B) and gamma counting (C,D) in Wistar rats (s = stomach, i = intestine, c = cecum, cl = colon, r = rectum, b = bladder). Reprinted with permission from Niu et al. (2018) [107].

Figure 7.
Coronal view of SPECT/CT scans after subcutaneous administration of (A) 111In-DTPA-PYY3–36-bipy and (B) 111In-DTPA-PYY3–36-Ac in mice (n = 3). (C) Biodistribution (%ID/g) of radioconjugates 24 h post-injection. Reprinted with permission from Kalomoiri et al. (2020) [108].
Figure 7.
Coronal view of SPECT/CT scans after subcutaneous administration of (A) 111In-DTPA-PYY3–36-bipy and (B) 111In-DTPA-PYY3–36-Ac in mice (n = 3). (C) Biodistribution (%ID/g) of radioconjugates 24 h post-injection. Reprinted with permission from Kalomoiri et al. (2020) [108].

Figure 8.
(A) Oral biodistribution of 99mTc-labeled-chitosan nanoparticles (green) containing 123I-labeled aspart-insulin (red) using SPECT/CT imaging in a rat model. Percentage dose of aspart-insulin observed over time in the urinary bladder, injection site/GI tract, and peripheral tissue/plasma after (B) subcutaneous injection and (C) oral gavage in rats. Reprinted with permission from Sonaje et al. (2010) [55].
Figure 8.
(A) Oral biodistribution of 99mTc-labeled-chitosan nanoparticles (green) containing 123I-labeled aspart-insulin (red) using SPECT/CT imaging in a rat model. Percentage dose of aspart-insulin observed over time in the urinary bladder, injection site/GI tract, and peripheral tissue/plasma after (B) subcutaneous injection and (C) oral gavage in rats. Reprinted with permission from Sonaje et al. (2010) [55].

Figure 9.
(A) Organ activities and (B) SPECT images of orally ingested 123I-labeled insulin loaded in nanoparticles, superimposed with soft-tissue contrast CT images at different time points; (C) Blood glucose change vs. time profiles of diabetic rats treated with different formulations of insulin. Oral gavaged 123I-labeled insulin loaded in nanoparticles are in red. Reprinted with permission from Chuang et al. (2013) [110].
Figure 9.
(A) Organ activities and (B) SPECT images of orally ingested 123I-labeled insulin loaded in nanoparticles, superimposed with soft-tissue contrast CT images at different time points; (C) Blood glucose change vs. time profiles of diabetic rats treated with different formulations of insulin. Oral gavaged 123I-labeled insulin loaded in nanoparticles are in red. Reprinted with permission from Chuang et al. (2013) [110].

Figure 10.
Oral biodistribution and utilization of 18F-FDG was studied in type 2 diabetic rats using (A) PET/CT imaging and (B) standard uptake value (SUV) measurements in the heart and skeletal muscles. 2-API NPs are the combination nanoparticles of insulin and exendin-4. Reprinted with permission from Chuang et al. (2013) [126].
Figure 10.
Oral biodistribution and utilization of 18F-FDG was studied in type 2 diabetic rats using (A) PET/CT imaging and (B) standard uptake value (SUV) measurements in the heart and skeletal muscles. 2-API NPs are the combination nanoparticles of insulin and exendin-4. Reprinted with permission from Chuang et al. (2013) [126].

Figure 11.
(A) PET/CT images show 18F-FDG accumulation in rats following G-CSF treatment given subcutaneously (SC), orally, or orally within nanoparticles (NPs). (B) Radioactive 18F-FDG concentrations are graphed over 2 h in the bone marrow for the different application modalities. Reprinted with permission from Su et al. (2014) [107,128].
Figure 11.
(A) PET/CT images show 18F-FDG accumulation in rats following G-CSF treatment given subcutaneously (SC), orally, or orally within nanoparticles (NPs). (B) Radioactive 18F-FDG concentrations are graphed over 2 h in the bone marrow for the different application modalities. Reprinted with permission from Su et al. (2014) [107,128].

Figure 12.
Coronal PET images of the antimicrobial peptoid 64Cu-1 after (A) intra-peritoneal (IP), (B) oral (PO), and (C) intravenous (IV) administration in Balb/C mice at different time points (n = 4). Reprinted with permission from Seo et al. (2012) [129].
Figure 12.
Coronal PET images of the antimicrobial peptoid 64Cu-1 after (A) intra-peritoneal (IP), (B) oral (PO), and (C) intravenous (IV) administration in Balb/C mice at different time points (n = 4). Reprinted with permission from Seo et al. (2012) [129].

Figure 13.
Advantages of nuclear imaging to study oral delivery of peptides.


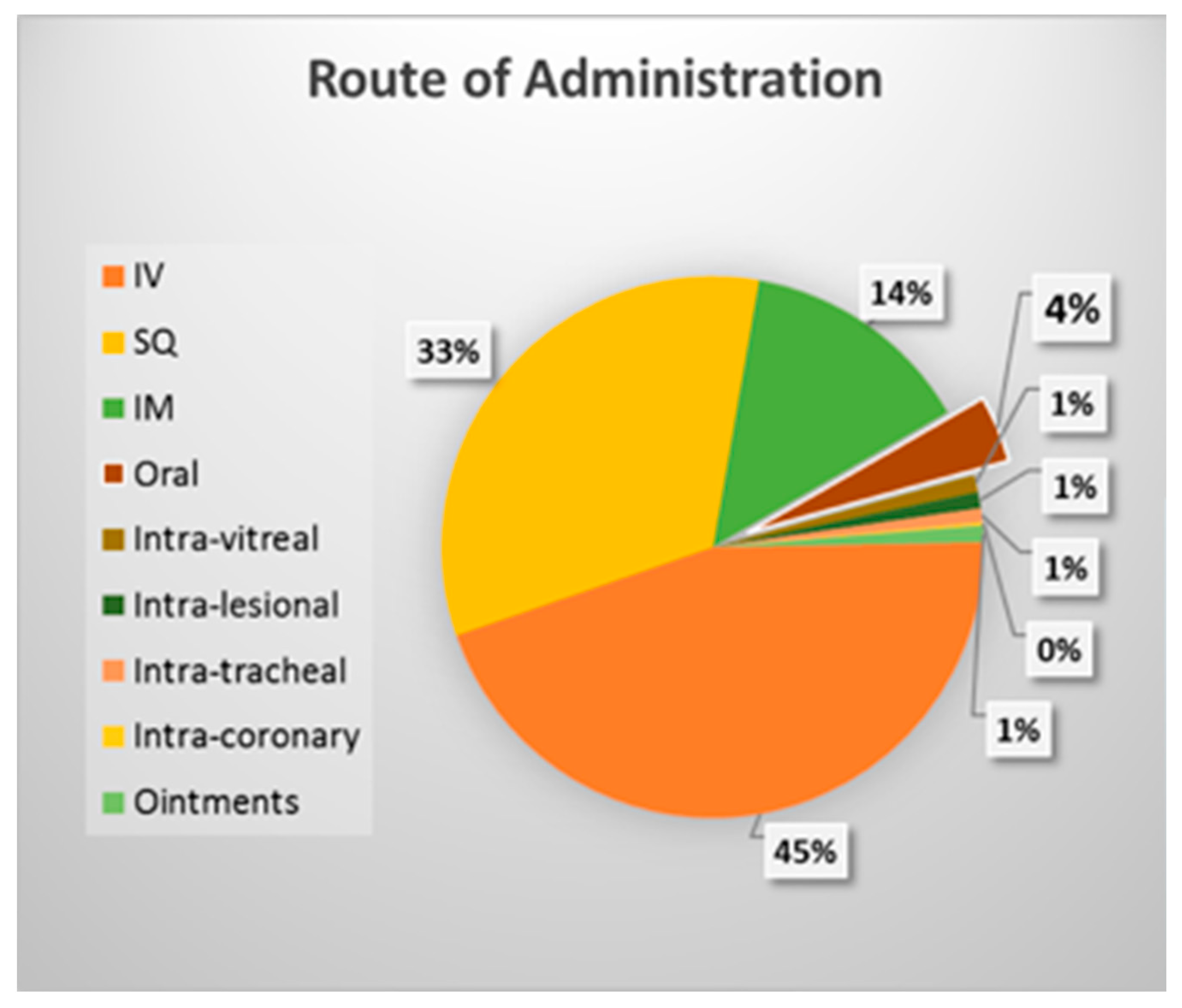{kind=link}
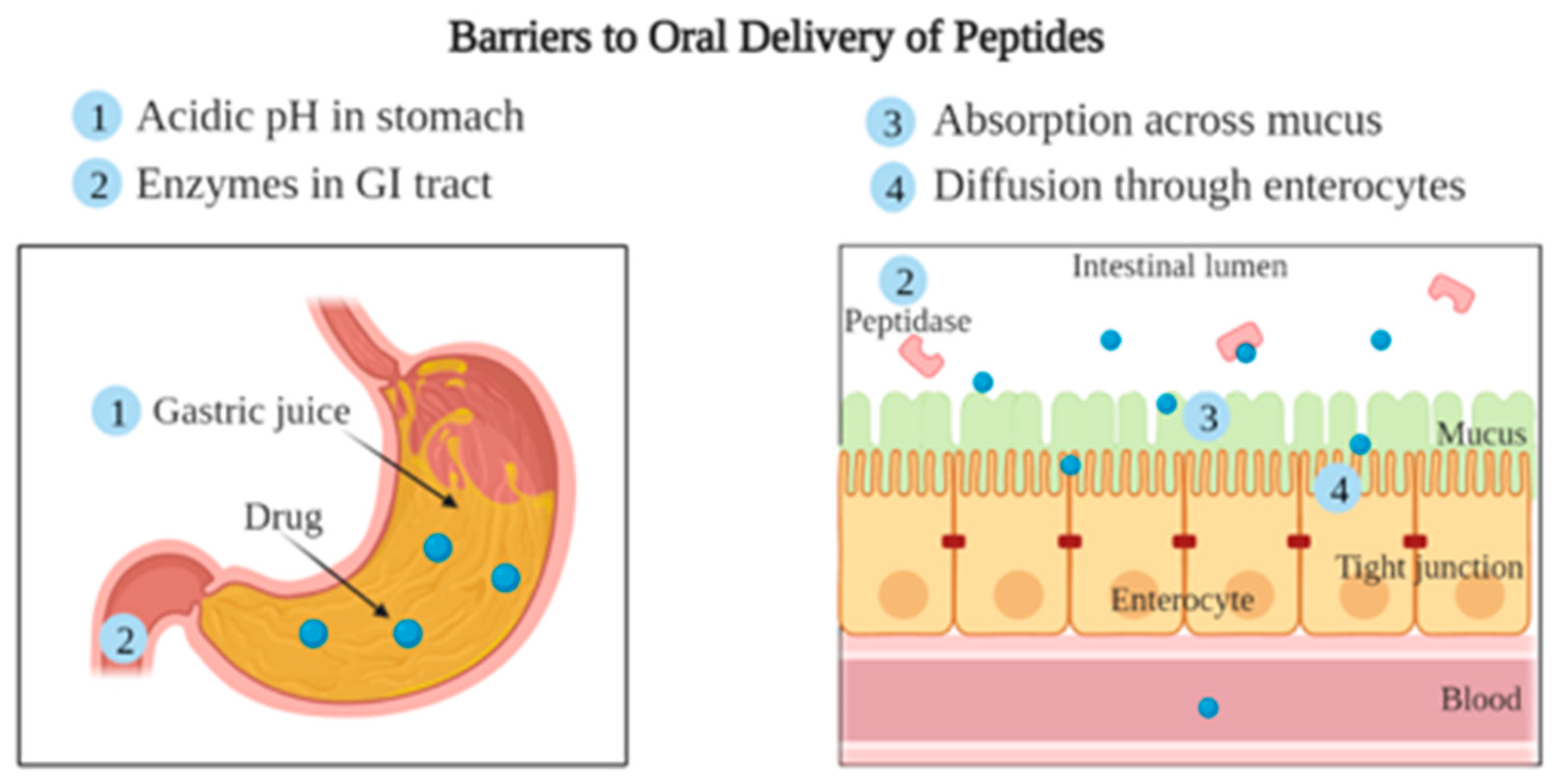{kind=link}
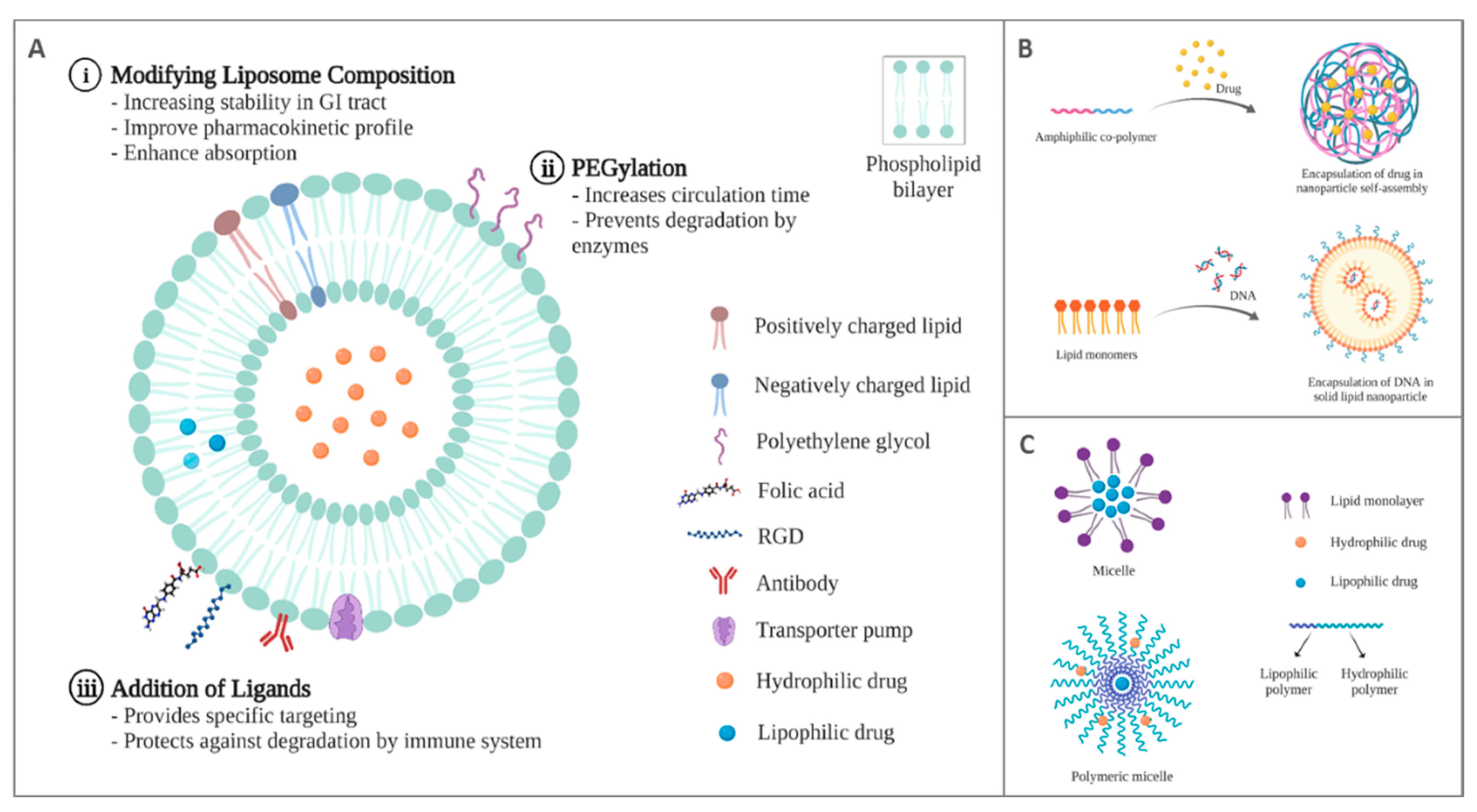{kind=link}
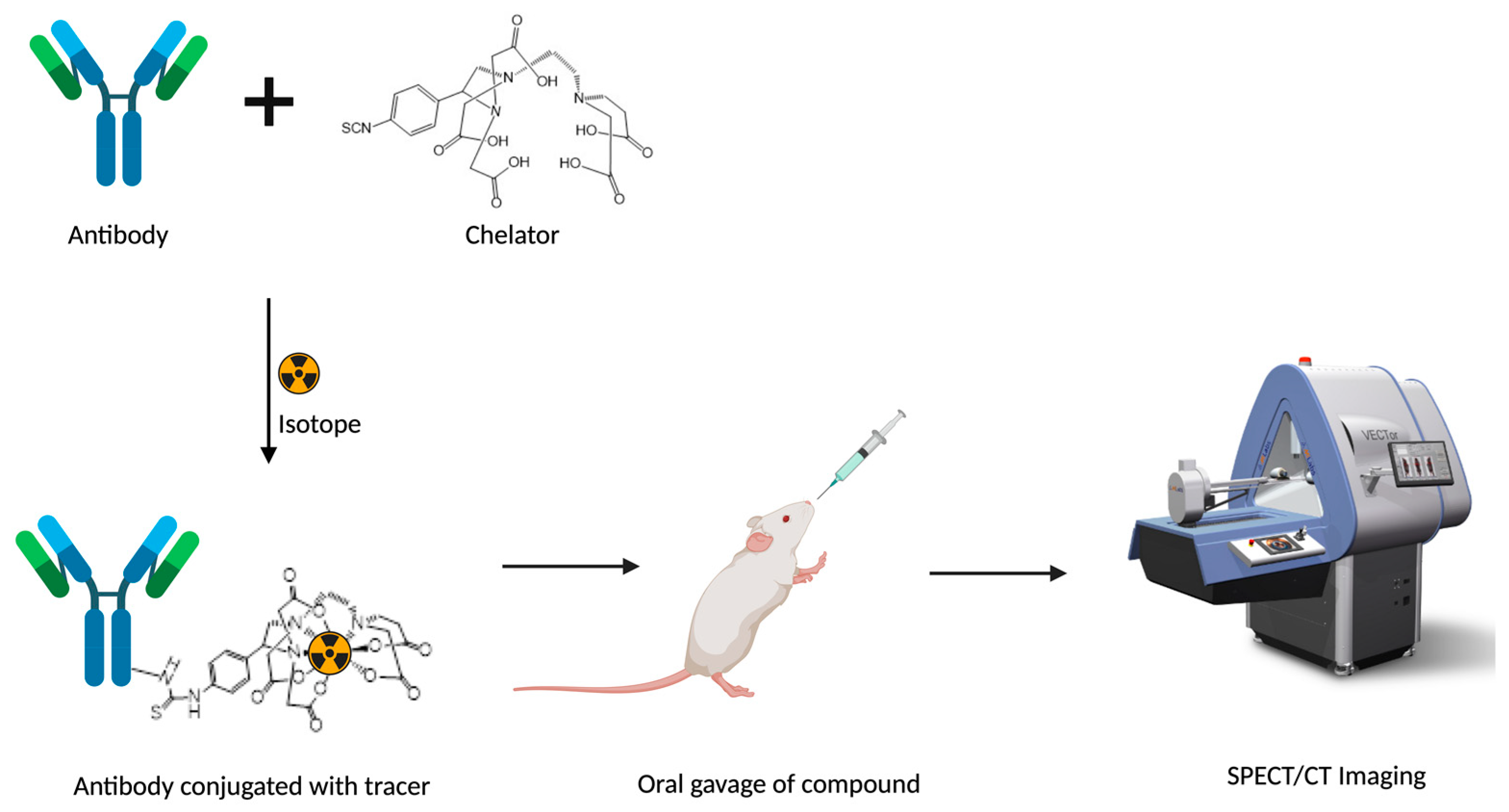{kind=link}
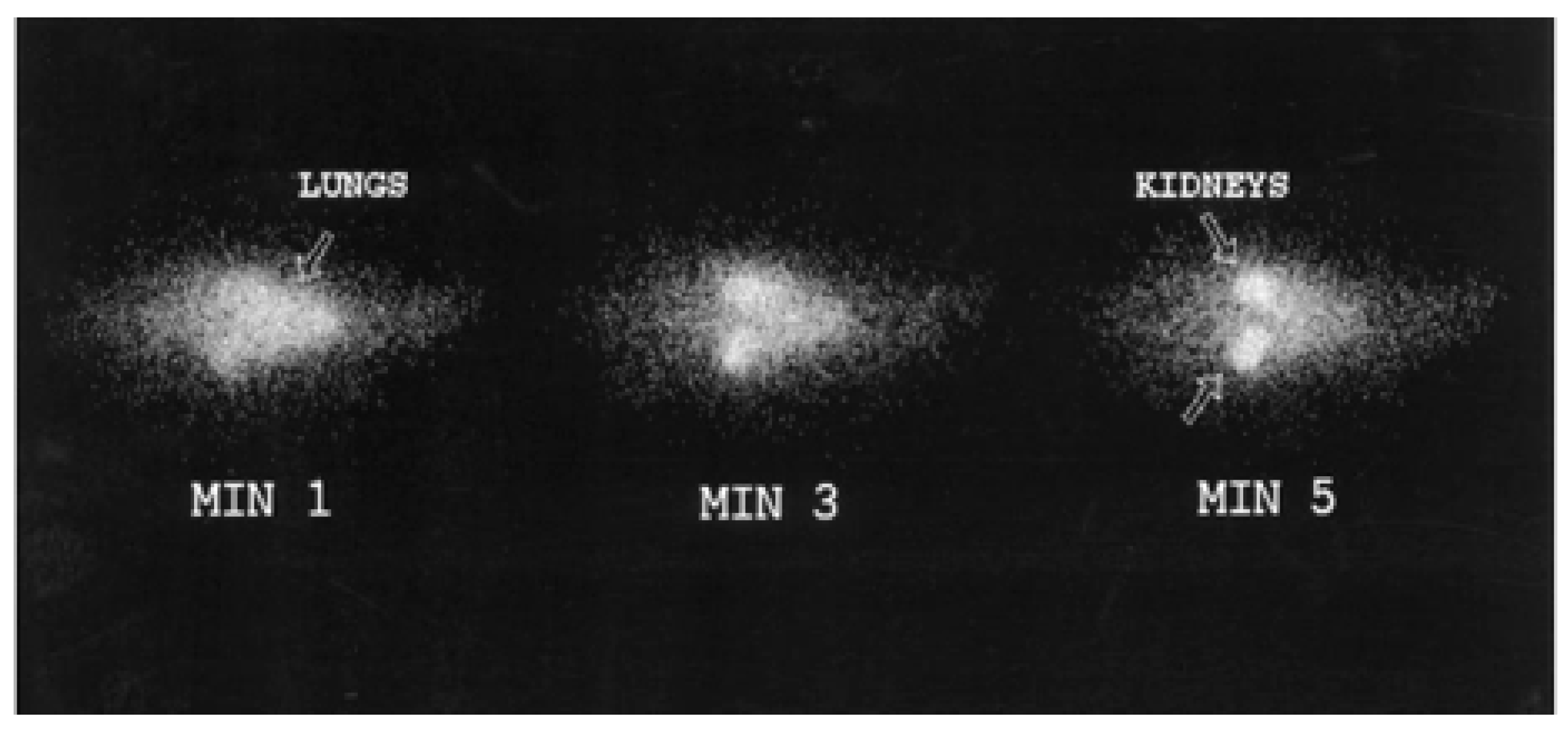{kind=link}
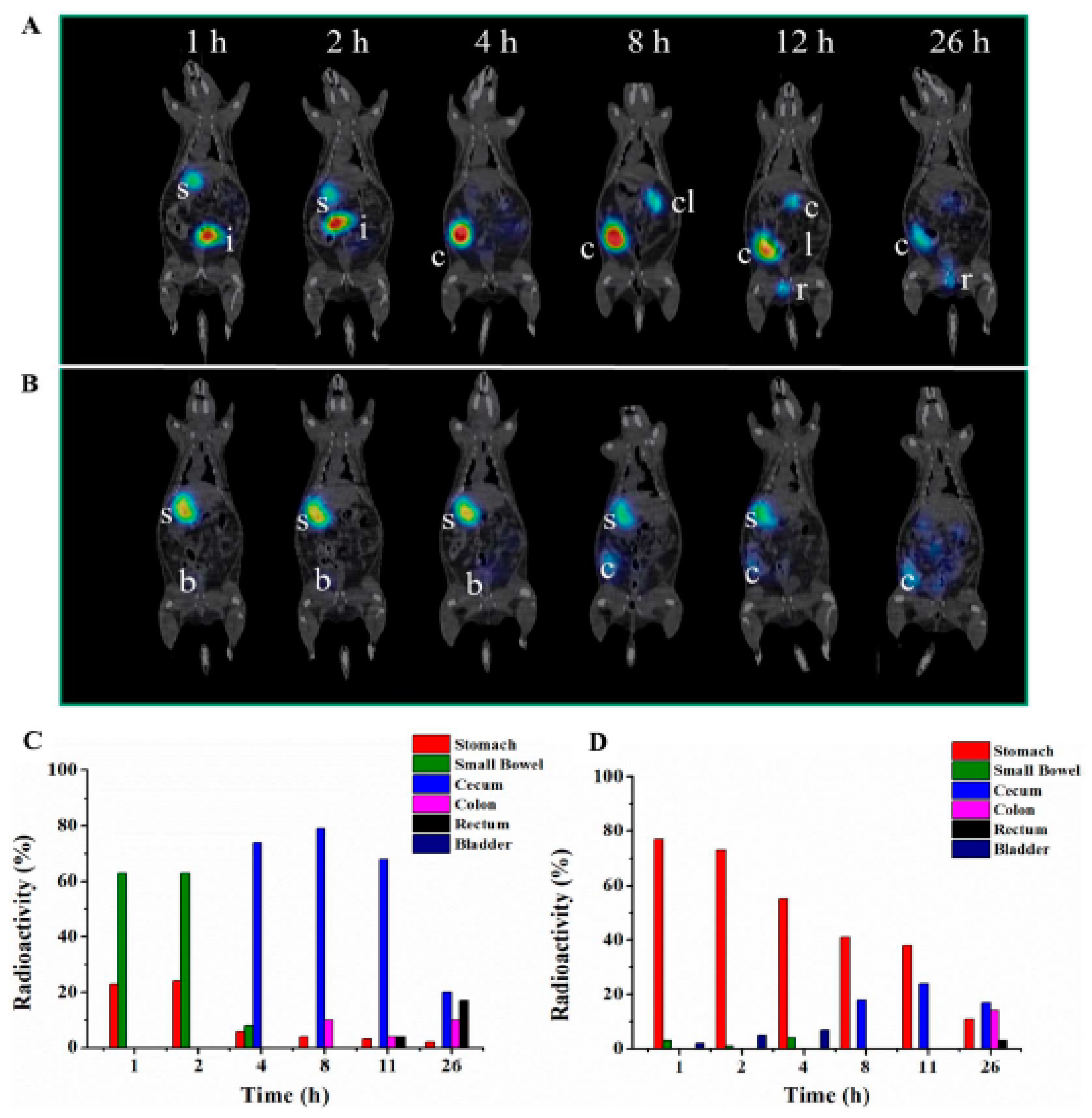{kind=link}
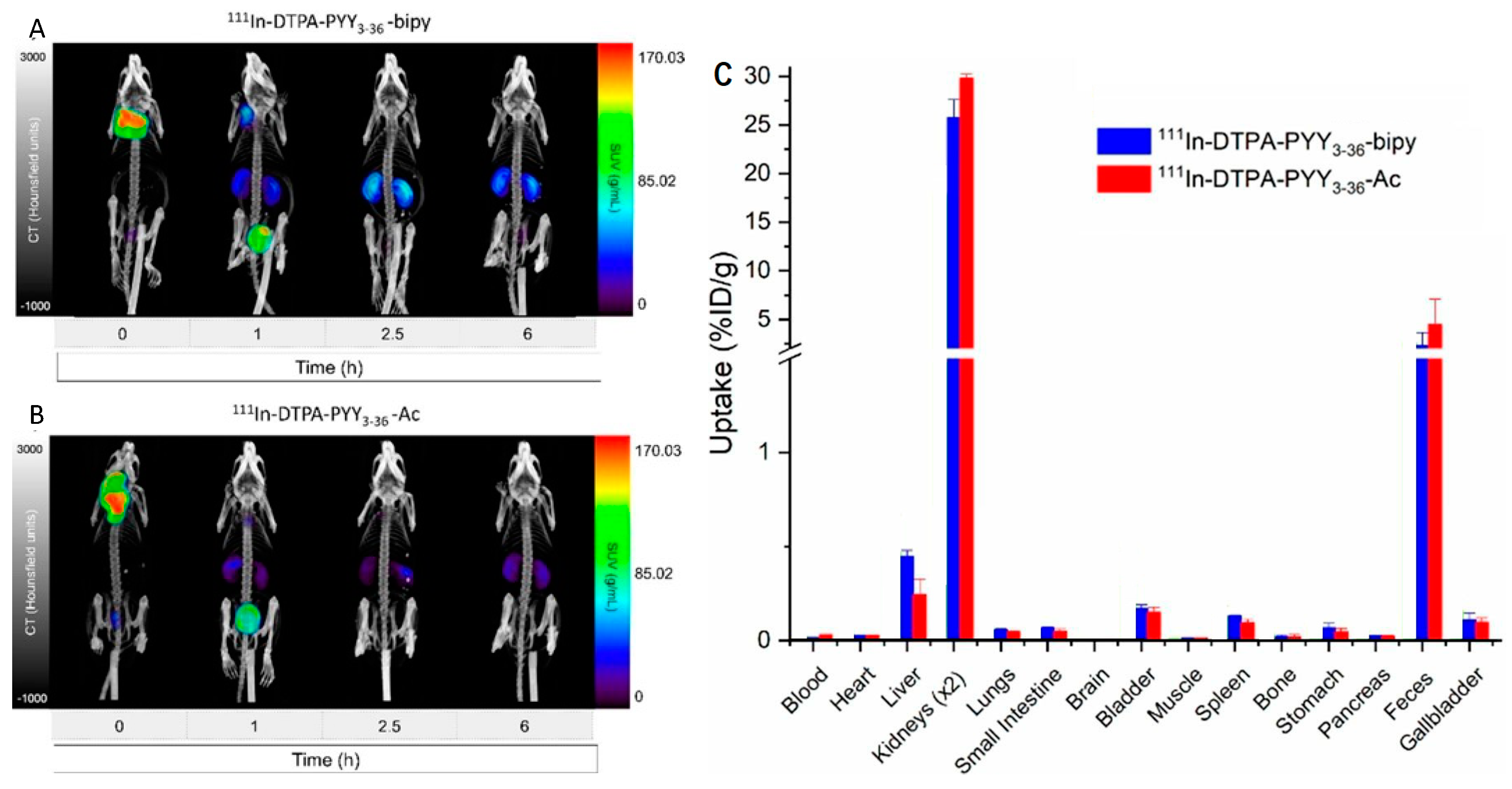{kind=link}
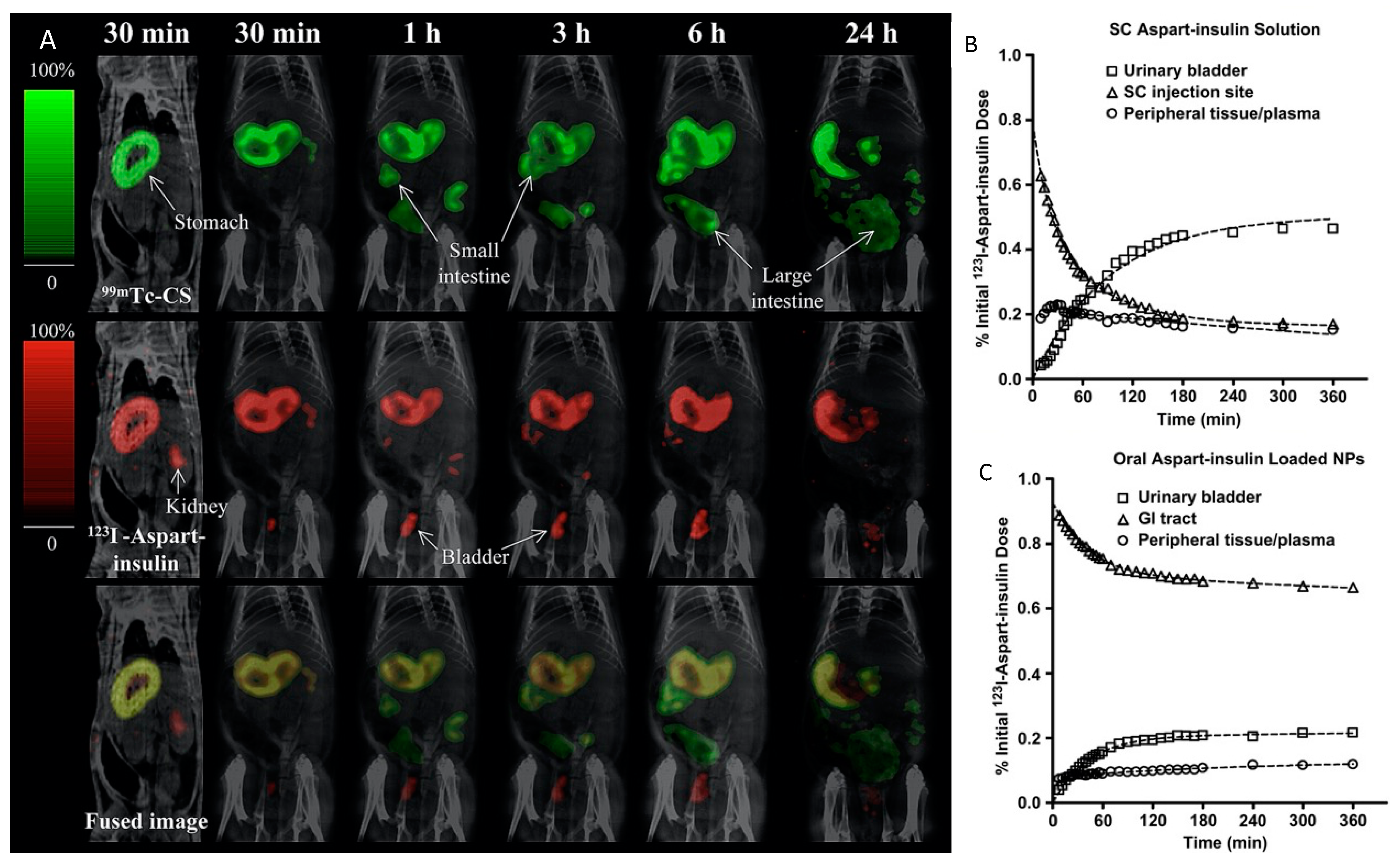{kind=link}
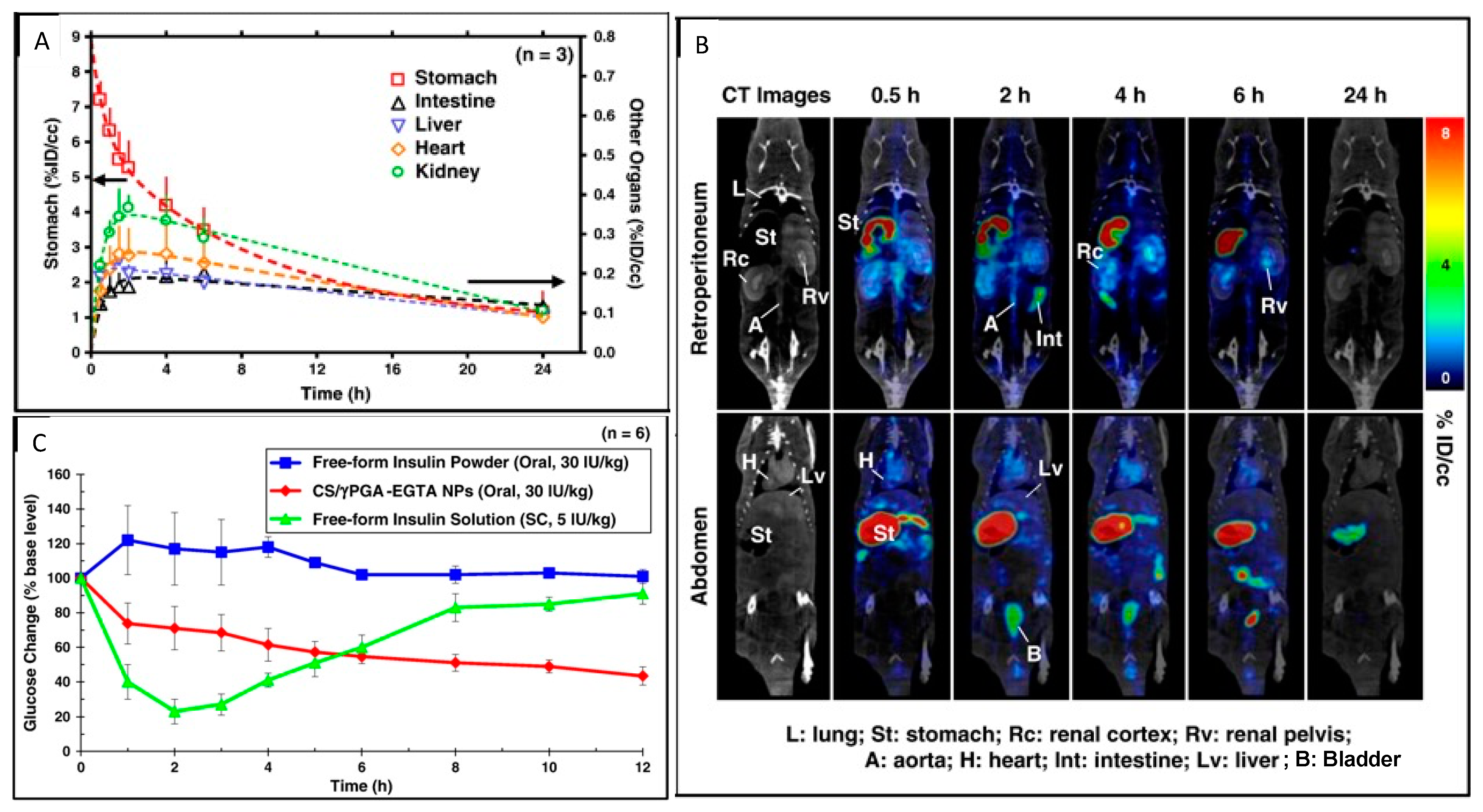{kind=link}
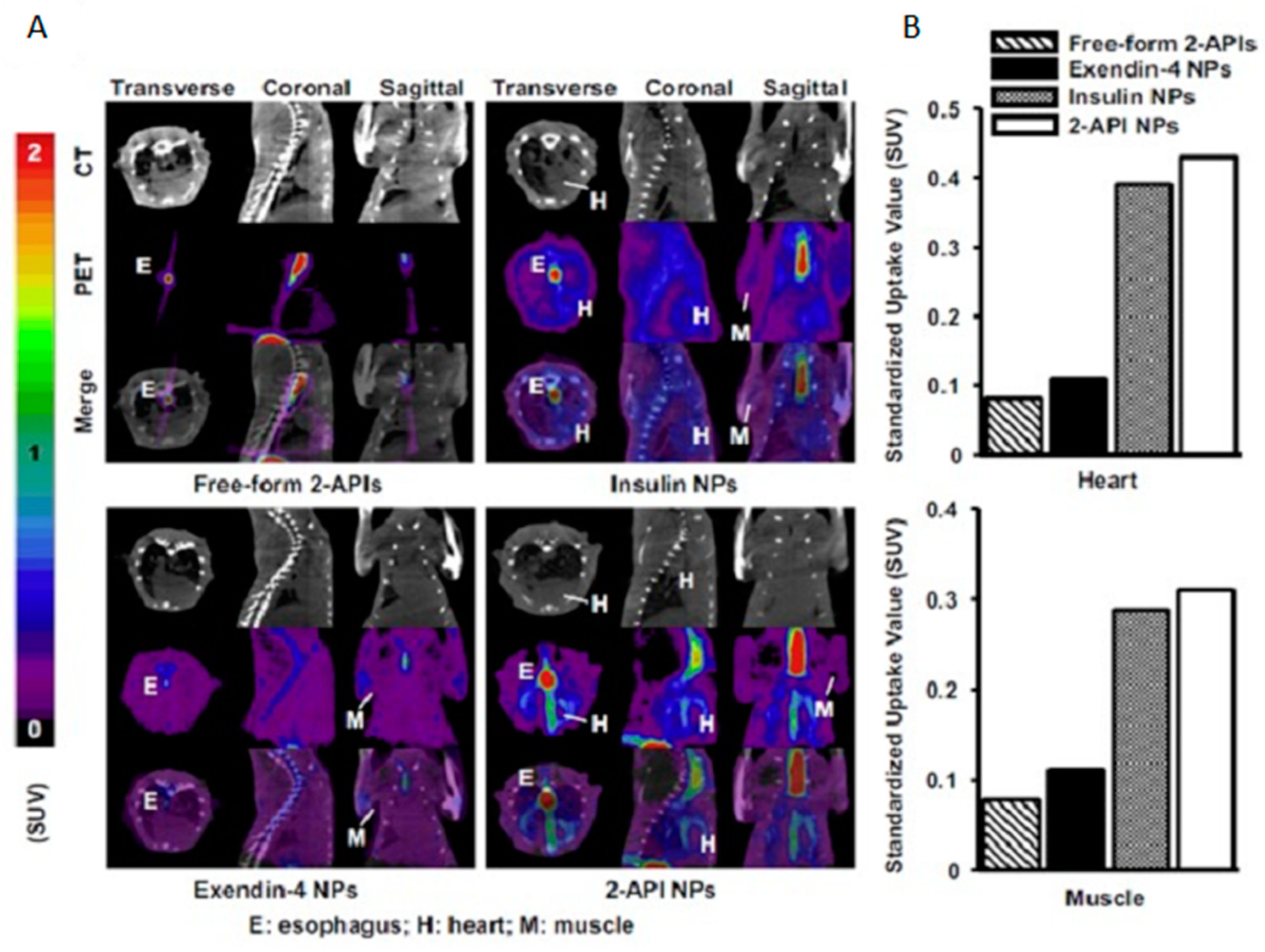{kind=link}
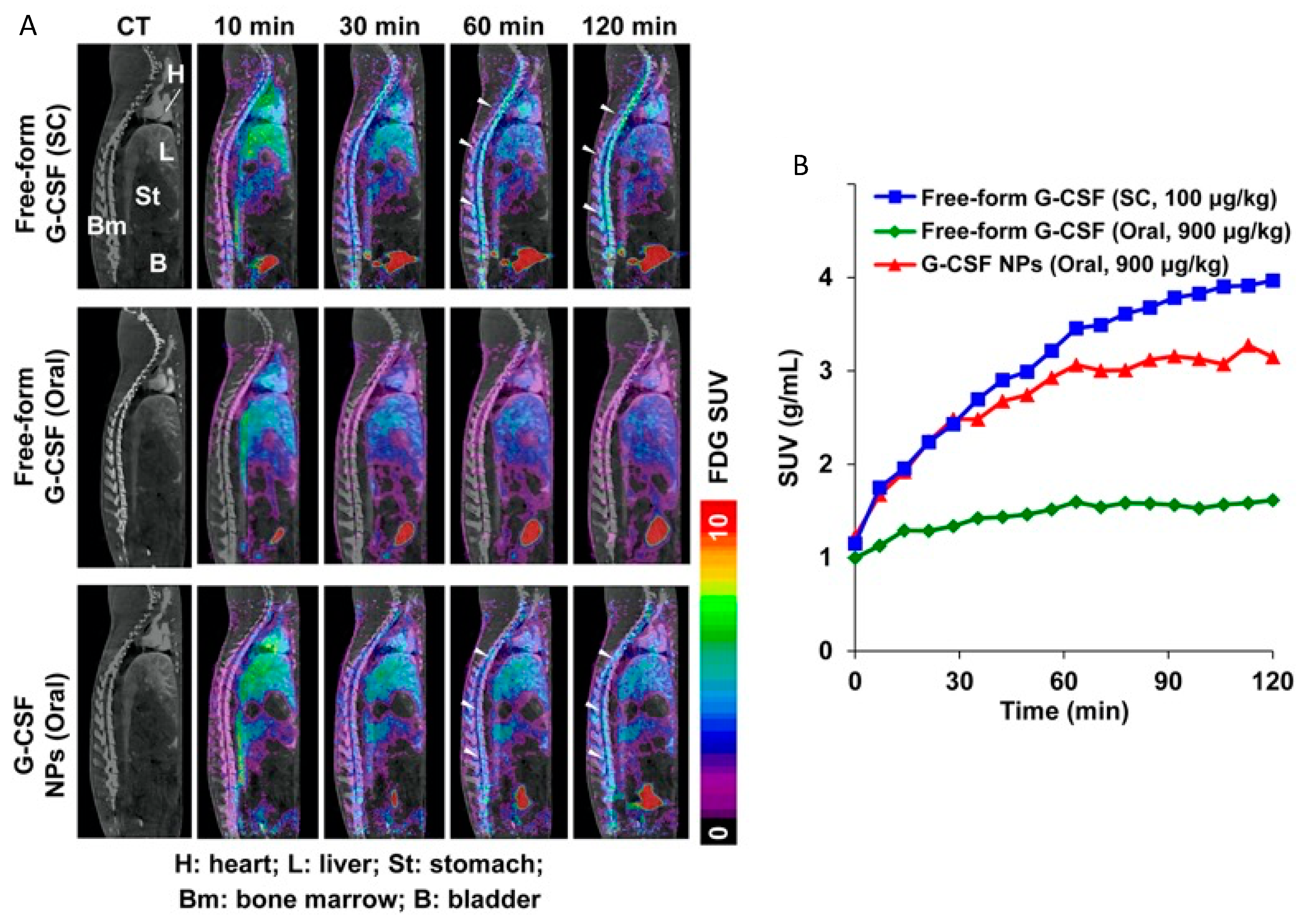{kind=link}
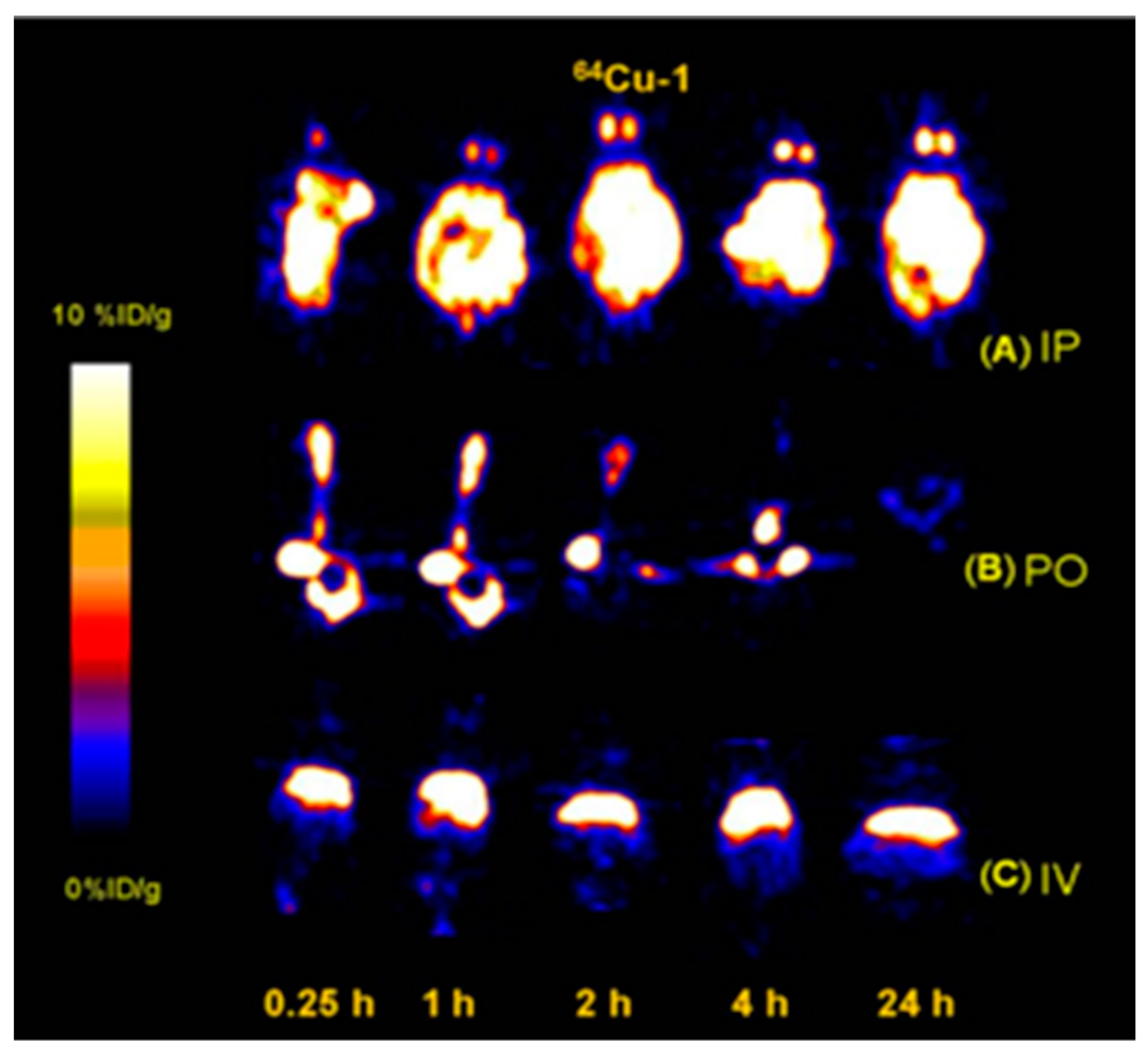{kind=link}
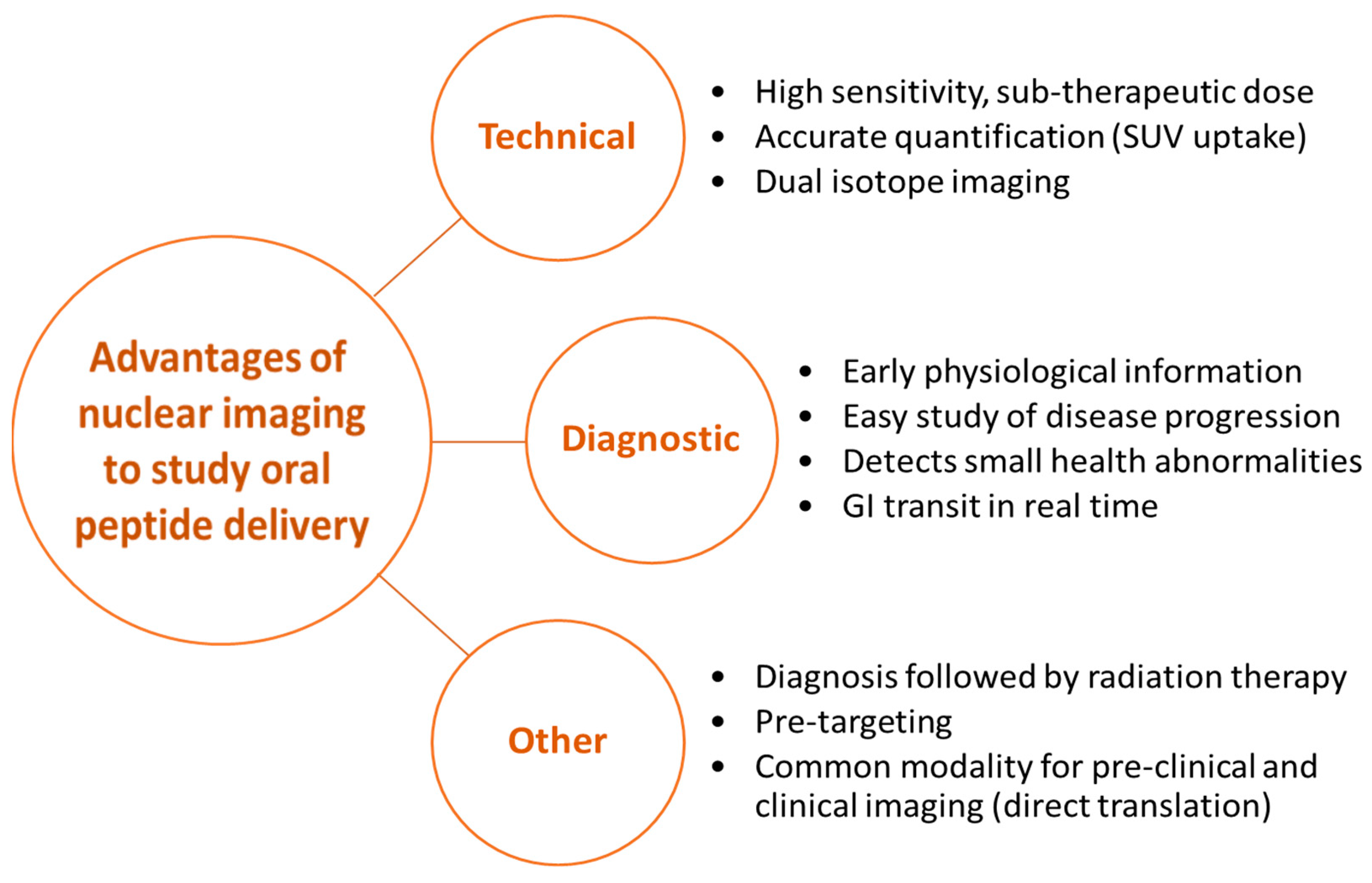{kind=link}
Table 1.
Commercially available FDA-approved oral peptide formulations [24,25] (* discontinued after 2017, # also approved by EMA). ^ Sodium N-[8-(2-hydroxybenzoyl) amino caprylate.
| Therapeutic Peptide | Brand | Application | Additional Components | Bioavailability |
|---|---|---|---|---|
| Aliskiren * | Tekturna®, Tekamlo®, Amturnide® | Treat hypertension | ||
| Boceprevir # [24] | Victrelis® | Treat chronic hepatitis C | Protease inhibitor | Up to 65% |
| Colistin [26] | Koolistin® | Treat multi-drug resistant bacterial infections | Local | |
| Cyclosporine [27] | Neoral®/Sandimmune® | Suppress immune system | Non-ionic surfactant | 25–30% |
| Desmopressin [28] | DDAVP® tablets, DDAVP® Melt, Minrin® | Treat central diabetes insipidus, primary nocturnal enuresis, blood disorders | Desmopressin acetate hydrate or Arginine Vasopressin | 0.08–0.16% |
| Glutathione | Reduced L-Glutathione | Reduce gut inflammation in cystic fibrosis patients [29] | Curcumin, no excipients [30] | Not documented |
| Linaclotide # | Linzess®, Constella® | Treat irritable bowel syndrome [31] | Microcrystalline cellulose spheres, enteric coating, hard gelatin capsules | Local |
| Octreotide [32] | Mycapssa® | Treat acromegaly | Polyvinylpyrrolidone (PVP-12), polysorbate 80, co-emulsifiers (glyceryl caprylates), gelatin capsules, and Acryl-EZE® (methacrylate) | 53–88% |
| Ombitasvir [33] | Viekirax® | Treat Chronic hepatitis C | Combination of dasabuvir, ombitasvir, paritaprevir, and ritonavir | 48–53% |
| Pancrelipase [24] | Pancrecarb®, Viokace®, ULTRESA®, PERTZYE®, ULTRASE®, ZENPEP® | Improve food digestion | Pancreatic amylase, pancreatic lipase, and chymotrypsin | 27–29% |
| Ragweed [24] | Ragwitek® | Treat ragweed allergy | Pollen extract | Not documented |
| Sacrosidase | Sucraid® | Hydrolyze sucrose | Sucrase [34] | Local |
| Semaglutide [35,36] | Rybelsus® | Induce insulin secretion | Enzyme inhibitor, enteric coating, Absorption enhancer (SNAC) ^ | ~1% |
| Taltirelin [37] | Ceredist® Ceredist OD® | Protect thyrotropin releasing hormone from enzyme hydrolysis | 75% | |
| Tyrothricin [38] | Several brands | Treat infected skin and oro-pharyngeal mucus membranes | Local | |
| Vancomycin [39] | Vancocin® | Treat pseudomembranous colitis | Local |
Table 2.
Summary of SPECT radionuclides and reaction parameters used in the preparation of radiolabeled peptides for pre-clinical and clinical imaging [105,114,115,116,117]. a Hydrazinonicotinic acid; b diethylenetriaminepentaacetic acid; c 1,4,7-triazacyclononane-1,4,7-triacetic acid; d 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid; e glucagon-like-phosphate-1 peptide. RT = room temperature.
Table 2.
Summary of SPECT radionuclides and reaction parameters used in the preparation of radiolabeled peptides for pre-clinical and clinical imaging [105,114,115,116,117]. a Hydrazinonicotinic acid; b diethylenetriaminepentaacetic acid; c 1,4,7-triazacyclononane-1,4,7-triacetic acid; d 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid; e glucagon-like-phosphate-1 peptide. RT = room temperature.
| Radionuclide | Half-Life (h) | Chelator/Prosthetic Group | Reaction Temperature | Reaction pH | Associated Preclinical/Clinical Peptide |
|---|---|---|---|---|---|
| 99mTc | 6.01 | Amidethiols, tetraamines (N4) or HYNIC a | RT for N4 80–100 °C for HYNIC | Octreotide, demobesin, sulfated cholecystokinin, demogastrin, exendin | |
| 111In | 67.31 | DTPA b, NOTA c | RT for DTPA, 60–65 °C for NOTA [118] | 4–5 | Octreotide, bombesin, neuropeptide Y, AMBA, minigastrin, GLP-1 e |
| 67Ga | 78.28 | DTPA b, NOTA c, DOTA d | RT for DTPA, NOTA 85–100 °C for DOTA | 2–11 | PESIN |
| 123I | 13.22 | Bolton-Hunter reagent | RT | 7–8 | GLP-1 |
Table 3.
Summary of PET radionuclides and reaction parameters used in the preparation of radiolabeled peptides for pre-clinical and clinical imaging [105,114,116,117,134,135,136]. a N-succinimidyl 4-[18F]fluorobenzoate; b 4-[18F]fluorobenzaldehyde; c 2-[18F]fluoro-2-deoxyglucose; d diethylenetriaminepentaacetic acid; e 1,4,7-triazacyclononane-1,4,7-triacetic acid; f 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid; g 1,4,8,11-tetraazacyclotetradecane, 1,4,8,11-tetraacetic acid; h cross-bridged-cyclam with TETA; i 3,6,10,13,16,19-hexaazabicyclo [6.6.6]icosane; j N-succinimidyl-5-[*I]iodo-3-pyridine carboxylate; k N-succinimidyl-3-[*I]iodobenzoate; l Arginine-Glycine-Aspartate probe.
Table 3.
Summary of PET radionuclides and reaction parameters used in the preparation of radiolabeled peptides for pre-clinical and clinical imaging [105,114,116,117,134,135,136]. a N-succinimidyl 4-[18F]fluorobenzoate; b 4-[18F]fluorobenzaldehyde; c 2-[18F]fluoro-2-deoxyglucose; d diethylenetriaminepentaacetic acid; e 1,4,7-triazacyclononane-1,4,7-triacetic acid; f 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid; g 1,4,8,11-tetraazacyclotetradecane, 1,4,8,11-tetraacetic acid; h cross-bridged-cyclam with TETA; i 3,6,10,13,16,19-hexaazabicyclo [6.6.6]icosane; j N-succinimidyl-5-[*I]iodo-3-pyridine carboxylate; k N-succinimidyl-3-[*I]iodobenzoate; l Arginine-Glycine-Aspartate probe.
| Radionuclide | Half-Life (h) | Chelator/Prosthetic Group | Reaction Temperature | Reaction pH | Associated Preclinical/Clinical Peptide |
|---|---|---|---|---|---|
| 18F | 1.83 | FSB a, FBA b, FDG c | RT | ~7 | Octreotate, bombesin analog BAY, GLP-1, RGD l |
| 68Ga | 1.13 | DTPA d, NOTA e, DOTA f | 85–100 °C for DOTA | 2–4, 7–11 | Somatostatin, exendin, RGD l |
| 64Cu | 12.70 | NOTA e, TETA g, CB-TE2A h, Sar i | RT for NOTA, TE2A 25–37 °C for Sar | 5–8 | Octreotide, bombesin, exendin, RGD l |
| 124I | 100.22 | Bolton-Hunter reagent, SIPC j or SIB k | RT | 7–8 | GLP-1 |
| 86/90Y | 14.74 | DOTA f | 80–85 °C | 4–5 | Somatostatin, RGD l |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Saxena, T.; Sie, C.; Lin, K.; Ye, D.; Saatchi, K.; Häfeli, U.O. Potential of Nuclear Imaging Techniques to Study the Oral Delivery of Peptides. Pharmaceutics 2022, 14, 2809. https://doi.org/10.3390/pharmaceutics14122809
AMA Style
Saxena T, Sie C, Lin K, Ye D, Saatchi K, Häfeli UO. Potential of Nuclear Imaging Techniques to Study the Oral Delivery of Peptides. Pharmaceutics. 2022; 14(12):2809. https://doi.org/10.3390/pharmaceutics14122809
Chicago/Turabian StyleSaxena, Tanya, Claire Sie, Kristine Lin, Daisy Ye, Katayoun Saatchi, and Urs O. Häfeli. 2022. "Potential of Nuclear Imaging Techniques to Study the Oral Delivery of Peptides" Pharmaceutics 14, no. 12: 2809. https://doi.org/10.3390/pharmaceutics14122809
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.