
Development and Skin Penetration Pathway Evaluation Using Confocal Laser Scanning Microscopy of Microemulsions for Dermal Delivery Enhancement of Finasteride

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Solubility Study
2.3. Preparation of Microemulsions
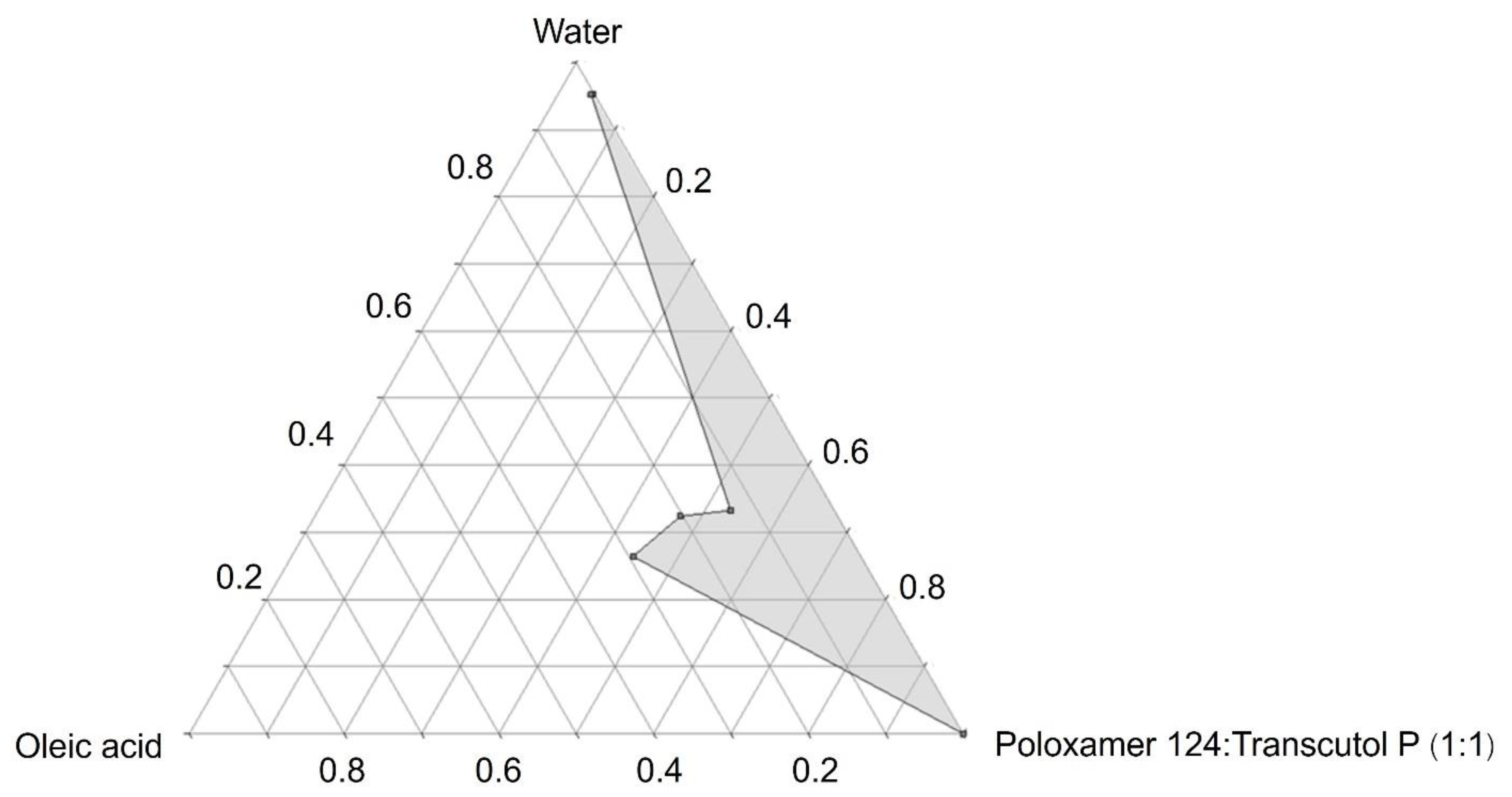
2.3.1. Construction of a Pseudoternary Phase Diagram of Microemulsions
2.3.2. Preparation of Finasteride-Loaded Microemulsions
2.4. Characterization of Microemulsions: Mean Particle Size, Surface Charge, Particle Size Distribution, and Electrical Conductivity
2.5. In Vitro Skin Penetration Study
2.5.1. Preparation of Skin
2.5.2. Skin Penetration Tests
2.6. Skin Penetration Pathway Evaluation
2.6.1. Preparation of Rhodamine B Base-Loaded NBD-PE Probed Microemulsions and Rhodamine B Base Solution
2.6.2. Skin Penetration Test
2.6.3. Preparation of Tissue Cross-Section Procedures
2.6.4. CLSM Visualization
2.7. HPLC Analysis
2.8. Statistical Analysis
3. Results and Discussion
3.1. Solubility Study
3.2. Preparation of Microemulsions: Construction of a Pseudoternary Phase Diagram of Microemulsions and Preparation of Finasteride-Loaded Microemulsions
3.3. Characterization of Microemulsions: Mean Particle Size, Surface Charge, Particle Size Distribution, and Electrical Conductivity
3.4. In Vitro Skin Penetration Study
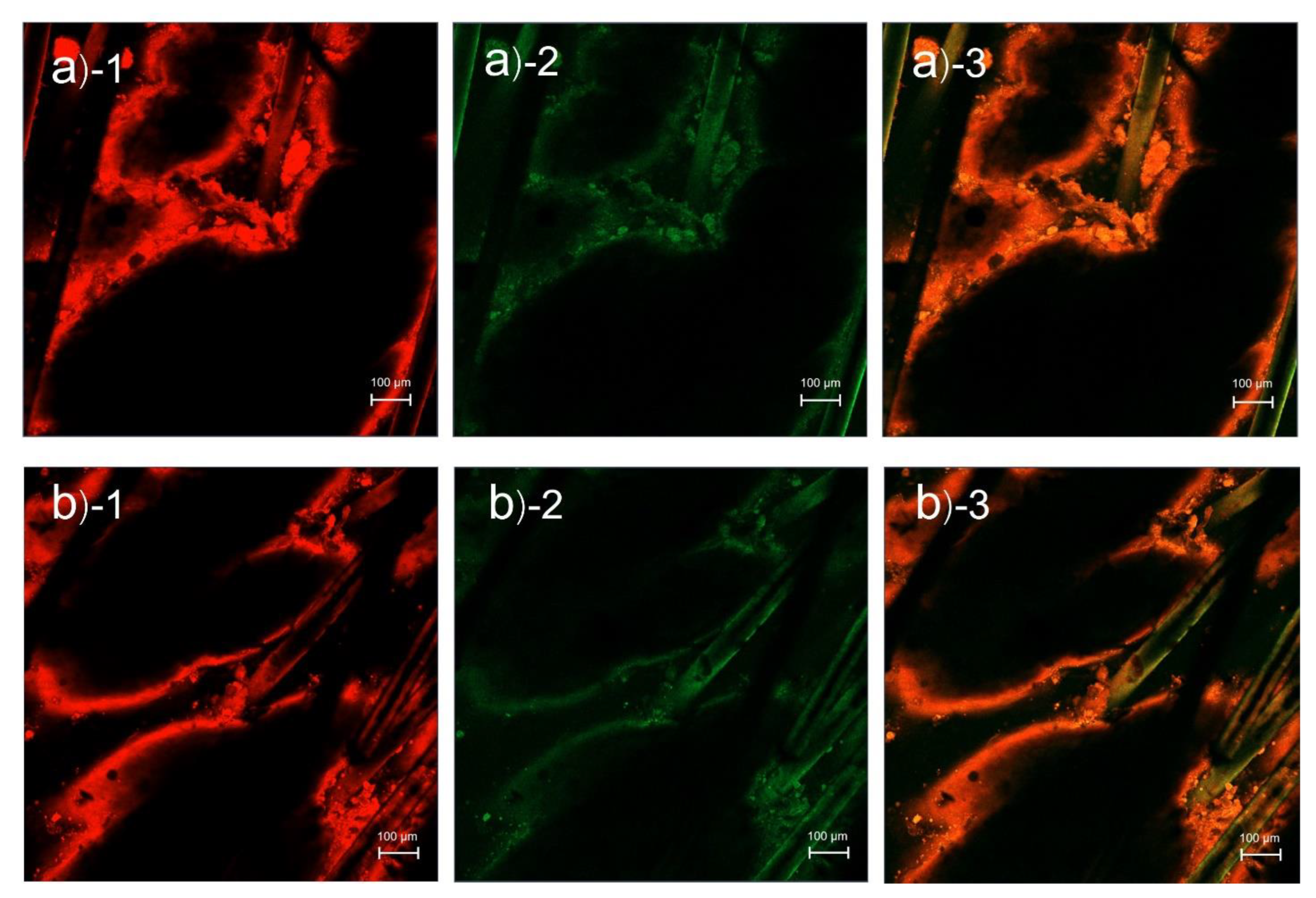
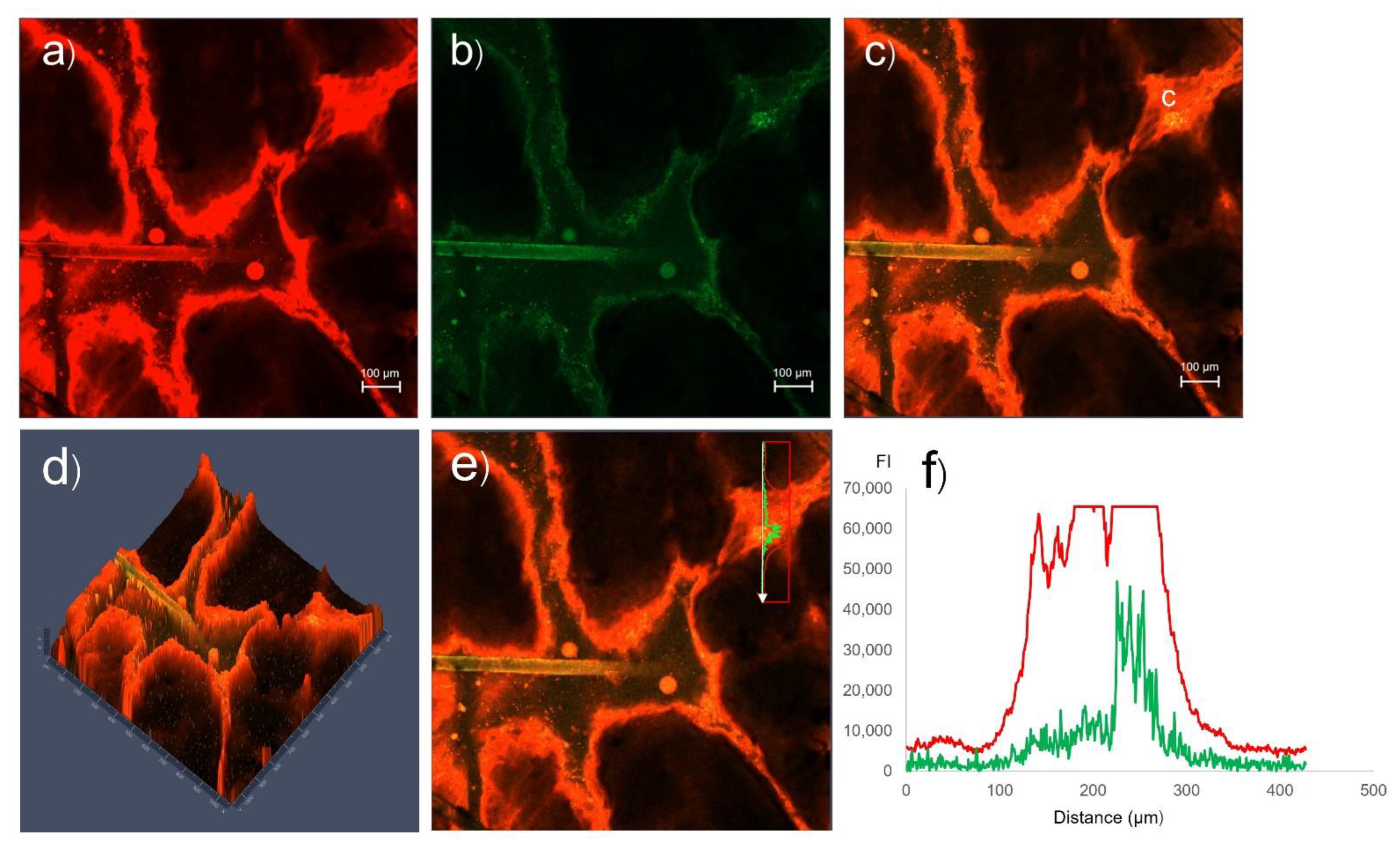
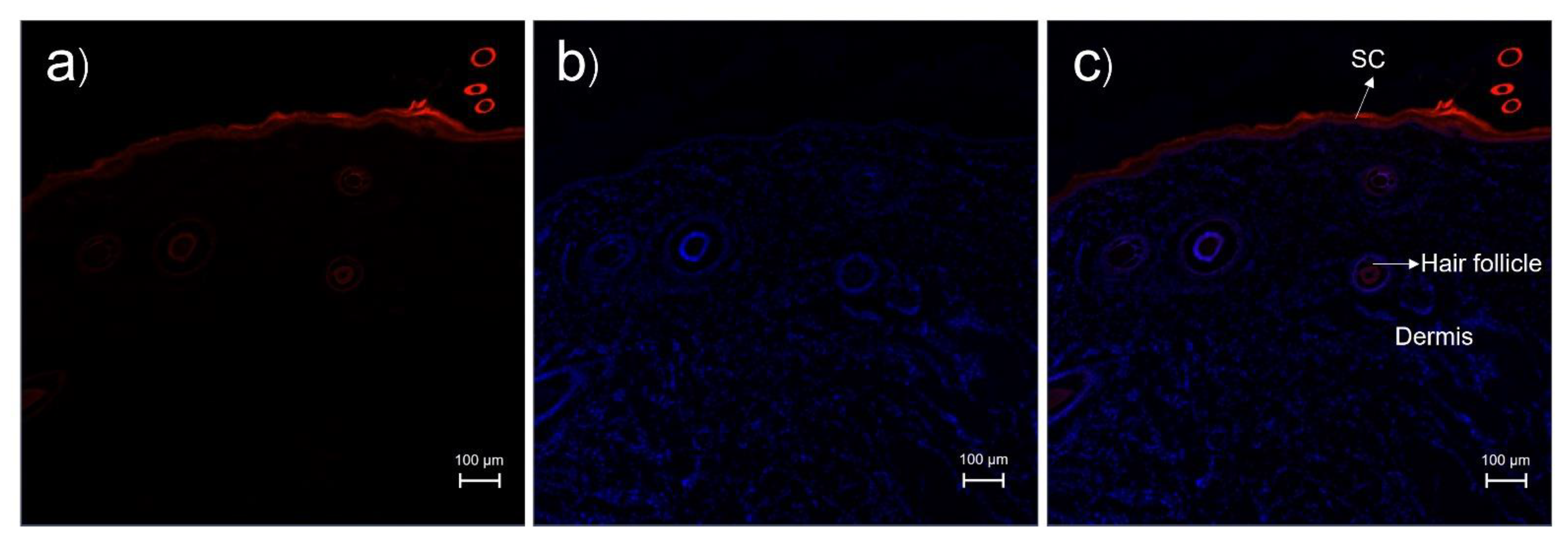
3.5. Skin Penetration Pathway Evaluation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nestor, M.S.; Ablon, G.; Gade, A.; Han, H.; Fischer, D.L. Treatment options for androgenetic alopecia: Efficacy, side effects, compliance, financial considerations, and ethics. J. Cosmet. Dermatol. 2021, 20, 3759–3781. [Google Scholar] [CrossRef] [PubMed]
- Price, V.H. Androgenetic Alopecia in Women. J. Investig. Dermatol. Symp. Proc. 2003, 8, 24–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varothai, S.; Bergfeld, W.F. Androgenetic alopecia: An evidence-based treatment update. Am. J. Clin. Dermatol. 2014, 15, 217–230. [Google Scholar] [CrossRef]
- Han, S.-H.; Byun, J.-W.; Lee, W.-S.; Kang, H.; Kye, Y.-C.; Kim, K.-H.; Kim, D.-W.; Kim, M.-B.; Kim, S.-J.; Kim, H.-O.; et al. Quality of Life Assessment in Male Patients with Androgenetic Alopecia: Result of a Prospective, Multicenter Study. Ann. Dermatol. 2012, 24, 311–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lolli, F.; Pallotti, F.; Rossi, A.; Fortuna, M.C.; Caro, G.; Lenzi, A.; Sansone, A.; Lombardo, F. Androgenetic alopecia: A review. Endocrine 2017, 57, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Thiboutot, D.; Zouboulis, C.C. Cutaneous Androgen Metabolism: Basic Research and Clinical Perspectives. J. Investig. Dermatol. 2002, 119, 992–1007. [Google Scholar] [CrossRef] [Green Version]
- Fu, D.; Huang, J.; Li, K.; Chen, Y.; He, Y.; Sun, Y.; Guo, Y.; Du, L.; Qu, Q.; Miao, Y.; et al. Dihydrotestosterone-induced hair regrowth inhibition by activating androgen receptor in C57BL6 mice simulates androgenetic alopecia. Biomed. Pharmacother. 2021, 137, 111247. [Google Scholar] [CrossRef]
- Kwack, M.H.; Ahn, J.S.; Kim, M.K.; Kim, J.C.; Sung, Y.K. Dihydrotestosterone-Inducible IL-6 Inhibits Elongation of Human Hair Shafts by Suppressing Matrix Cell Proliferation and Promotes Regression of Hair Follicles in Mice. J. Investig. Dermatol. 2012, 132, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Kanti, V.; Messenger, A.; Dobos, G.; Reygagne, P.; Finner, A.; Blumeyer, A.; Trakatelli, M.; Tosti, A.; Del Marmol, V.; Piraccini, B.M.; et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men-short version. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 11–22. [Google Scholar] [CrossRef]
- Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Miller, G.J.; Ford, L.G.; Lieber, M.M.; Cespedes, R.D.; Atkins, J.N.; Lippman, S.M.; et al. The influence of finasteride on the development of prostate cancer. N. Engl. J. Med. 2003, 349, 215–224. [Google Scholar] [CrossRef]
- Naik, A.; Kalia, Y.N.; Guy, R.H. Transdermal drug delivery: Overcoming the skin’s barrier function. Pharm. Sci. Technol. Today 2000, 9, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Showing Compound Finasteride (FDB022782). Available online: https://foodb.ca/compounds/FDB022782 (accessed on 4 December 2022).
- Suchonwanit, P.; Iamsumang, W.; Leerunyakul, K. Topical finasteride for the treatment of male androgenetic alopecia and female pattern hair loss: A review of the current literature. J. Dermatol. Treat. 2022, 33, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Tabbakhian, M.; Tavakoli, N.; Jaafari, M.R.; Daneshamouz, S. Enhancement of follicular delivery of finasteride by liposomes and niosomes: 1. In vitro permeation and in vivo deposition studies using hamster flank and ear models. Int. J. Pharm. 2006, 323, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Singh, B.; Bakshi, G.; Katare, O.P. Development of Liposomal Systems of Finasteride for Topical Applications: Design, Characterization, and In Vitro Evaluation. Pharm. Dev. Technol. 2007, 12, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cao, S.; Yu, K.; Yang, F.; Yu, X.; Zhai, Y.; Wu, C.; Xu, Y. Integrating tacrolimus into eutectic oil-based microemulsion for atopic dermatitis: Simultaneously enhancing percutaneous delivery and treatment efficacy with relieving side effects. Int. J. Nanomed. 2019, 14, 5849–5863. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, S.; Pani, N.R.; Sahoo, S.K. Microemulsion based topical hydrogel of sertaconazole: Formulation, characterization and evaluation. Colloids Surf. B Biointerfaces 2014, 120, 193–199. [Google Scholar] [CrossRef]
- Ma, H.; Yu, M.; Lei, M.; Tan, F.; Li, N. A Novel Topical Targeting System of Caffeine Microemulsion for Inhibiting UVB-Induced Skin Tumor: Characterization, Optimization, and Evaluation. AAPS PharmSciTech 2015, 16, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Subongkot, T.; Sirirak, T. Development and skin penetration pathway evaluation of microemulsions for enhancing the dermal delivery of celecoxib. Colloids Surf. B Biointerfaces 2020, 193, 111103. [Google Scholar] [CrossRef]
- Sakr, F.M.; Gado, A.M.; Mohammed, H.R.; Adam, A.N. Preparation and evaluation of a multimodal minoxidil microemulsion versus minoxidil alone in the treatment of androgenic alopecia of mixed etiology: A pilot study. Drug Des. Dev. Ther. 2013, 7, 413–423. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Magri, F.; D’Arino, A.; Pigliacelli, F.; Muscianese, M.; Leoncini, P.; Caro, G.; Federico, A.; Fortuna, M.C.; Carlesimo, M. Efficacy of Topical Finasteride 0.5% vs 17α-Estradiol 0.05% in the Treatment of Postmenopausal Female Pattern Hair Loss: A Retrospective, Single-Blind Study of 119 Patients. Dermatol. Pract. Concept. 2020, 10, e2020039. [Google Scholar] [CrossRef]
- Adiraj Iyer, M.; Eddington, D.T. Storing and releasing rhodamine as a model hydrophobic compound in polydimethylsiloxane microfluidic devices. Lab Chip. 2019, 19, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Duangjit, S.; Rattanachithawat, N.; Opanasopit, P.; Ngawhirunpat, T. Development and optimization of finasteride-cinnamon oil-loaded ethanol-free microemulsions for transdermal delivery. J. Drug Deliv. Sci. Technol. 2022, 69, 103107. [Google Scholar] [CrossRef]
- Acharya, D.P.; Hartley, P.G. Progress in microemulsion characterization. Curr. Opin. Colloid Interface Sci. 2012, 17, 274–280. [Google Scholar] [CrossRef]
- Azeem, A.; Khan, Z.I.; Aqil, M.; Ahmad, F.J.; Khar, R.K.; Talegaonkar, S. Microemulsions as a Surrogate Carrier for Dermal Drug Delivery. Drug Dev. Ind. Pharm. 2009, 35, 525–547. [Google Scholar] [CrossRef] [PubMed]
- Krauel, K.; Davies, N.; Hook, S.; Rades, T. Using different structure types of microemulsions for the preparation of poly(alkylcyanoacrylate) nanoparticles by interfacial polymerization. J. Control. Release 2005, 106, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Menon, G.K.; Cleary, G.W.; Lane, M.E. The structure and function of the stratum corneum. Int. J. Pharm. 2012, 435, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Francoeur, M.L.; Golden, G.M.; Potts, R.O. Oleic Acid: Its Effects on Stratum Corneum in Relation to (Trans)Dermal Drug Delivery. Pharm. Res. 1990, 7, 621–627. [Google Scholar] [CrossRef]
- Rowat, A.C.; Kitson, N.; Thewalt, J.L. Interactions of oleic acid and model stratum corneum membranes as seen by 2H NMR. Int. J. Pharm. 2006, 307, 225–231. [Google Scholar] [CrossRef]
- Ayala-Bravo, H.A.; Quintanar-Guerrero, D.; Naik, A.; Kalia, Y.; Cornejo-Bravo, J.; Ganem-Quintanar, A. Effects of Sucrose Oleate and Sucrose Laureate on in Vivo Human Stratum Corneum Permeability. Pharm. Res. 2003, 20, 1267–1273. [Google Scholar] [CrossRef]
- Strati, F.; Neubert, R.H.; Opálka, L.; Kerth, A.; Brezesinski, G. Non-ionic surfactants as innovative skin penetration enhancers: Insight in the mechanism of interaction with simple 2D stratum corneum model system. Eur. J. Pharm. Sci. 2021, 157, 105620. [Google Scholar] [CrossRef]
- Su, R.; Fan, W.; Yu, Q.; Dong, X.; Qi, J.; Zhu, Q.; Zhao, W.; Wu, W.; Chen, Z.; Li, Y.; et al. Size-dependent penetration of nanoemulsions into epidermis and hair follicles: Implications for transdermal delivery and immunization. Oncotarget 2017, 8, 38214–38226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.; Bian, Q.; Zhou, Y.; Huang, Q.; Gao, J. Hair follicle-targeting drug delivery strategies for the management of hair follicle-associated disorders. Asian J. Pharm. Sci. 2022, 17, 333–352. [Google Scholar] [CrossRef] [PubMed]
- Schätzlein, A.; Cevc, G. Non-uniform cellular packing of the stratum corneum and permeability barrier function of intact skin: A high-resolution confocal laser scanning microscopy study using highly deformable vesicles (Transfersomes). Br. J. Dermatol. 1998, 138, 583–592. [Google Scholar] [CrossRef]
- Carrer, D.C.; Vermehren, C.; Bagatolli, L.A. Pig skin structure and transdermal delivery of liposomes: A two photon microscopy study. J. Control. Release 2008, 132, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Harding, C.R.; Watkinson, A.; Rawlings, A.V.; Scott, I.R. Dry skin, moisturization and corneodesmolysis. Int. J. Cosmet. Sci. 2000, 22, 21–52. [Google Scholar] [CrossRef]
- Warner, R.R.; Boissy, Y.L.; Lilly, N.A.; Spears, M.J.; McKillop, K.; Marshall, J.L.; Stone, K.J. Water disrupts stratum corneum lipid lamellae: Damage is similar to surfactants. J. Investig. Dermatol. 1999, 113, 960–966. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Oils/Surfactants | Solubility (mg/mL) |
|---|---|
| Medium-chain triglycerides | 2.31 ± 0.03 |
| Isopropyl myristate | 3.24 ± 0.61 |
| Oleic acid | 42.63 ± 0.04 |
| Transcutol P | 68.05 ± 0.07 |
| Tween 20 | 17.59 ± 0.51 |
| PEG-80 sorbitan laurate | 18.48 ± 0.35 |
| PEG-6 Caprylic/Capric Glycerides | 12.25 ± 0.14 |
| Kolliphor EL | 15.59 ± 0.39 |
| PEG-12 | 7.31 ± 0.04 |
| Poloxamer 124 | 4.11 ± 0.16 |
| Formulations | Ratio | Finasteride-Loaded Microemulsion (% w/v) | ||
|---|---|---|---|---|
| Oleic Acid | Mixtures of Surfactants (Poloxamer 124:Transcutol P) | Water | ||
| P1 | 15 | 60 | 25 | 0.5 |
| P2 | 20 | 55 | 25 | 0.5 |
| P3 | 10 | 70 | 20 | 0.5 |
| Formulations | Particle Size (nm) | Polydispersity Index (PDI) | Zeta Potential (mV) | Electrical Conductivity (µS/cm) | ||||
|---|---|---|---|---|---|---|---|---|
| Blank MEs | Finasteride-Loaded MEs | Blank MEs | Finasteride-Loaded MEs | Blank MEs | Finasteride-Loaded MEs | Blank MEs | Finasteride-Loaded MEs | |
| P1 | 51.18 ± 6.49 | 115.63 ± 24.52 | 0.39 ± 0.07 | 0.21 ± 0.01 | −0.2 ± 0.1 | −0.47 ± 0.11 | 77.23 ± 0.21 | 72.97 ± 2.71 |
| P2 | 66.12 ± 1.79 | 80.09 ± 16.67 | 0.31 ± 0.05 | 0.37 ± 0.03 | −0.24 ± 0.08 | −0.37 ± 0.21 | 57.83 ± 0.15 | 59.8 ± 3.6 |
| P3 | 57.66 ± 12.61 | 136.97 ± 27.94 | 0.15 ± 0.02 | 0.29 ± 0.03 | −0.34 ± 0.29 | −0.11 ± 0.02 | 55.93 ± 0.41 | 57.97 ± 0.41 |
| Formulations | Stratum Corneum (µg/cm2) | Viable Epidermis, Dermis, and Subcutaneous Tissue (µg/cm2) | Receiver Medium (µg/mL) | Enhancement Ratio |
|---|---|---|---|---|
| Solution | 6.77 ± 5.38 | 1.88 ± 0.76 | ND | - |
| P1 | 23.84 ± 15.75 | 5.17 ± 0.44 | ND | 2.75 |
| P2 | 45.52 ± 25.29 | 10.55 ± 1.14 * | ND | 5.61 |
| P3 | 21.46 ± 1.56 | 4.03 ± 0.71 | ND | 2.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subongkot, T.; Charernsriwilaiwat, N.; Chanasongkram, R.; Rittem, K.; Ngawhirunpat, T.; Opanasopit, P. Development and Skin Penetration Pathway Evaluation Using Confocal Laser Scanning Microscopy of Microemulsions for Dermal Delivery Enhancement of Finasteride. Pharmaceutics 2022, 14, 2784. https://doi.org/10.3390/pharmaceutics14122784
Subongkot T, Charernsriwilaiwat N, Chanasongkram R, Rittem K, Ngawhirunpat T, Opanasopit P. Development and Skin Penetration Pathway Evaluation Using Confocal Laser Scanning Microscopy of Microemulsions for Dermal Delivery Enhancement of Finasteride. Pharmaceutics. 2022; 14(12):2784. https://doi.org/10.3390/pharmaceutics14122784
Chicago/Turabian StyleSubongkot, Thirapit, Natthan Charernsriwilaiwat, Rattathammanoon Chanasongkram, Kantawat Rittem, Tanasait Ngawhirunpat, and Praneet Opanasopit. 2022. "Development and Skin Penetration Pathway Evaluation Using Confocal Laser Scanning Microscopy of Microemulsions for Dermal Delivery Enhancement of Finasteride" Pharmaceutics 14, no. 12: 2784. https://doi.org/10.3390/pharmaceutics14122784