
Effect of an Oxygen-Based Mechanical Drug Delivery System on Percutaneous Permeation of Various Substances In Vitro
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Buffers
2.3. Transdermal Formulations
2.4. Membranes
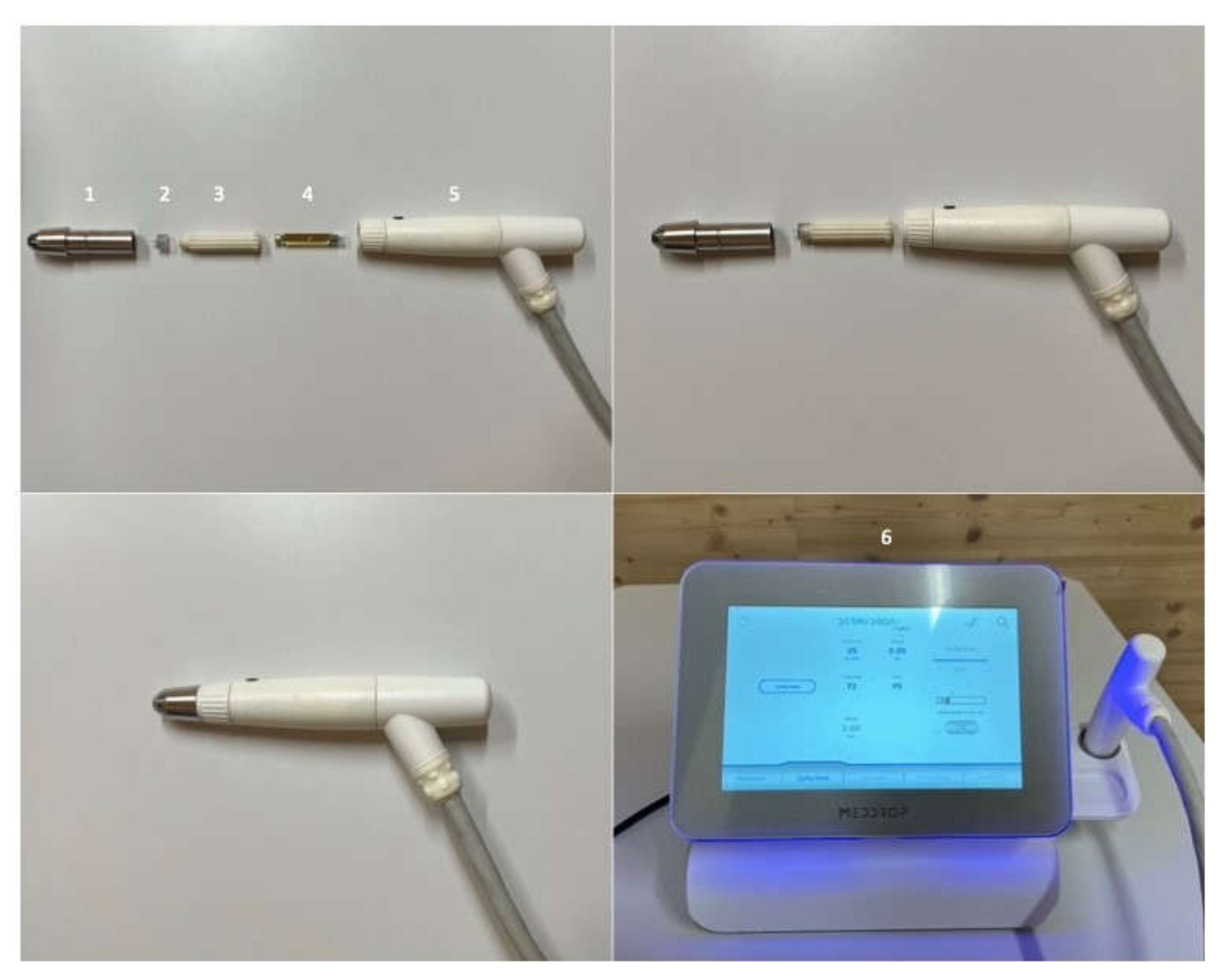
2.5. Medical Transdermal Application Device
2.6. Franz-Type Diffusion Cell Experiments
2.7. High-Performance Liquid Chromatography (HPLC)
2.8. Histological Examination
2.9. Data Analysis
3. Results
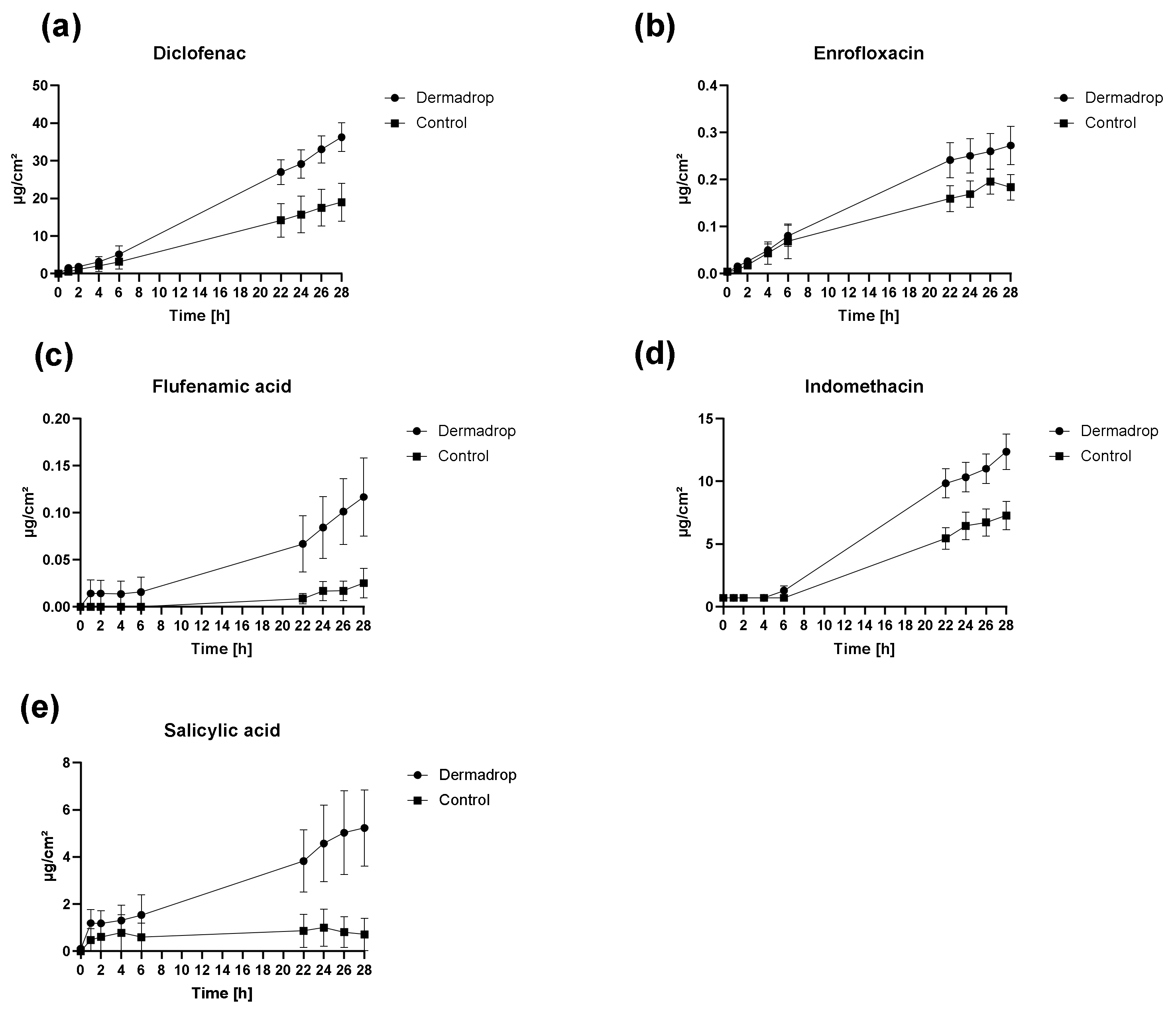
3.1. Skin Permeation
3.1.1. Permeation Rates
3.1.2. Permeation Parameters
3.1.3. Correlation between Permeation Parameters and Physicochemical Properties
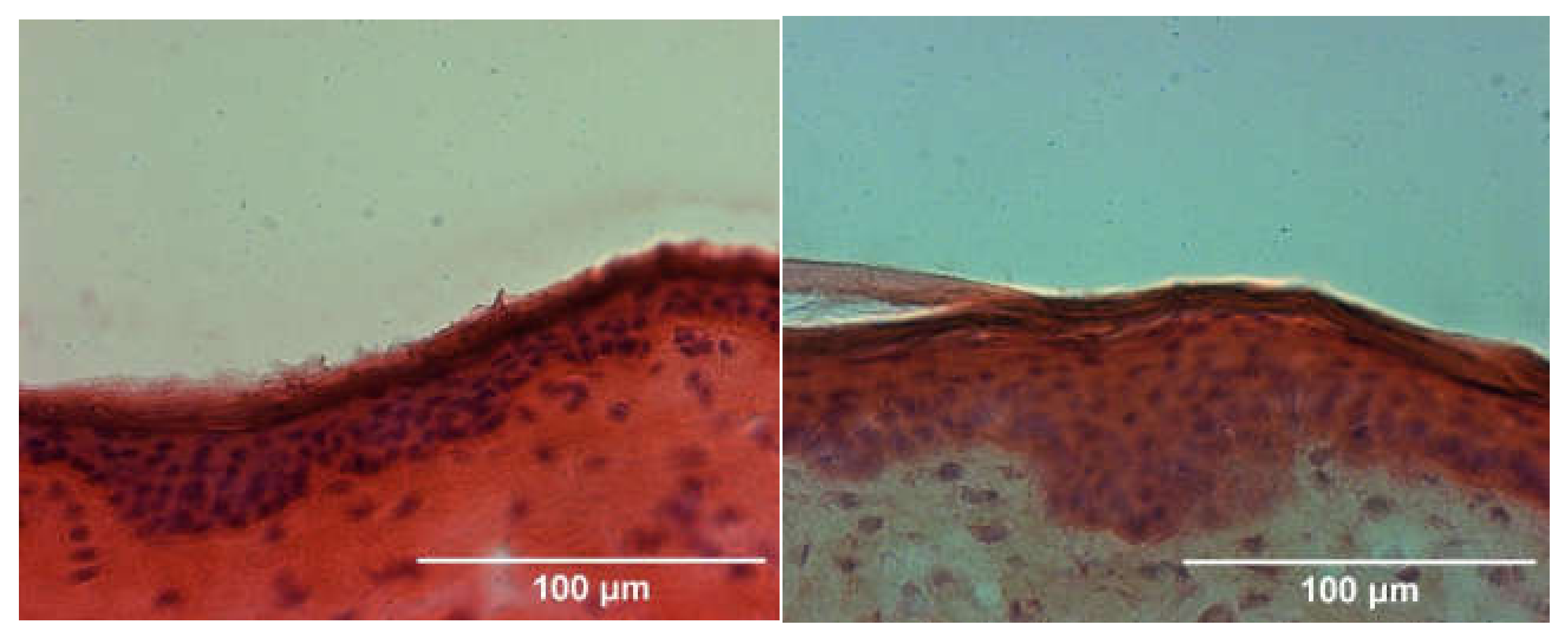
3.2. Histology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, A.C.; Barry, B.W. Penetration enhancers. Adv. Drug Deliv. Rev. 2004, 56, 603–618. [Google Scholar] [CrossRef]
- Mueller, J.; Trapp, M.; Neubert, R.H.H. The effect of hydrophilic penetration/diffusion enhancer on stratum corneum lipid models: Part II: DMSO. Chem. Phys. Lipids 2019, 225, 104816. [Google Scholar] [CrossRef]
- Newton, S.J. Chemical penetration enhancers. Int. J. Pharm. Compd. 2013, 17, 370–374. [Google Scholar]
- Raphael, A.P.; Wright, O.R.; Benson, H.A.; Prow, T.W. Recent advances in physical delivery enhancement of topical drugs. Curr. Pharm. Des. 2015, 21, 2830–2847. [Google Scholar] [CrossRef]
- Brown, M.B.; Martin, G.P.; Jones, S.A.; Akomeah, F.K. Dermal and transdermal drug delivery systems: Current and future prospects. Drug Deliv. 2006, 13, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Park, C.O.; Kim, H.L.; Park, J.W. Microneedle Transdermal Drug Delivery Systems for Allergen-Specific Immunotherapy, Skin Disease Treatment, and Vaccine Development. Yonsei Med. J. 2022, 63, 881–891. [Google Scholar] [CrossRef]
- Kaushik, V.; Keck, C.M. Influence of mechanical skin treatment (massage, ultrasound, microdermabrasion, tape stripping and microneedling) on dermal penetration efficacy of chemical compounds. Eur. J. Pharm. Biopharm. 2021, 169, 29–36. [Google Scholar] [CrossRef]
- Gill, H.S.; Andrews, S.N.; Sakthivel, S.K.; Fedanov, A.; Williams, I.R.; Garber, D.A.; Priddy, F.H.; Yellin, S.; Feinberg, M.B.; Staprans, S.I.; et al. Selective removal of stratum corneum by microdermabrasion to increase skin permeability. Eur. J. Pharm. Sci. 2009, 38, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidler, M.; Fouché, N.; Meth, I.; von Hahn, F.; von Rechenberg, B.; Kronen, P.W. Preliminary study on carprofen concentration measurements after transcutaneous treatment with Vetdrop® in a microfracture joint defect model in sheep. BMC Vet. Res. 2014, 10, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidler, M.; Fouché, N.; Meth, I.; von Hahn, F.; von Rechenberg, B.; Kronen, P. Transcutaneous treatment with vetdrop® sustains the adjacent cartilage in a microfracturing joint defect model in sheep. Open Orthop. J. 2013, 7, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Lebas, E.; Chapelier, C.; Quatresooz, P.; Seidel, L.; Nikkels, A.F. Exploratory Assessment of Oxygen Flow-Assisted Cutaneous Administration of Methotrexate for Superficial Basal Cell Carcinoma, Mycosis Fungoides, and Extramammary Paget Disease. J. Investig. Dermatol. 2020, 140, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Díaz, L.; Zambrano, E.; Flores, M.E.; Contreras, M.; Crispín, J.C.; Alemán, G.; Bravo, C.; Armenta, A.; Valdés, V.J.; Tovar, A.; et al. Ethical Considerations in Animal Research: The Principle of 3R’s. Rev. Investig. Clin. 2020, 73, 199–209. [Google Scholar] [CrossRef] [PubMed]
- OECD/OCDE. Skin Absorption: In Vitro Method. In OECD Guideline for the Testing of Chemicals; OECD iLibrary News: Paris, France, 2004; pp. 1–8. Available online: https://www.oecd-ilibrary.org/environment/test-no-428-skin-absorption-in-vitro-method_9789264071087-en (accessed on 23 October 2022). [CrossRef]
- Stahl, J.; Niedorf, F.; Kietzmann, M. The correlation between epidermal lipid composition and morphologic skin characteristics with percutaneous permeation: An interspecies comparison of substances with different lipophilicity. J. Vet. Pharmacol. Ther. 2011, 34, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Scherz, G.; Stahl, J.; Glünder, G.; Kietzmann, M. Effects of carry-over of fluoroquinolones on the susceptibility of commensal Escherichia coli in the intestinal microbiota of poultry. Berl. Munch. Tierarztl. Wochenschr. 2014, 127, 478–485. [Google Scholar]
- McNally, M.E.; Usher, K.; Hansen, S.W.; Amoo, J.S.; Bernstein, A.P. Precision of Internal Standard and External Standard Methods in High Performance Liquid Chromatography; LCGC Supplements, Special Issues-04-01-2015; LCGC: Chester, UK, 2015; Volume 33, pp. 40–46. [Google Scholar]
- Stahl, J.; Niedorf, F.; Kietzmann, M. Characterisation of epidermal lipid composition and skin morphology of animal skin ex vivo. Eur. J. Pharm. Biopharm. 2009, 72, 310–316. [Google Scholar] [CrossRef]
- Wong, T.W. Electrical, magnetic, photomechanical and cavitational waves to overcome skin barrier for transdermal drug delivery. J. Control. Release 2014, 193, 257–269. [Google Scholar] [CrossRef]
- Nazary Abrbekoh, F.; Salimi, L.; Saghati, S.; Amini, H.; Fathi Karkan, S.; Moharamzadeh, K.; Sokullu, E.; Rahbarghazi, R. Application of microneedle patches for drug delivery; doorstep to novel therapies. J. Tissue Eng. 2022, 13, 20417314221085390. [Google Scholar] [CrossRef]
- Stahl, J.; Wohlert, M.; Kietzmann, M. Microneedle pretreatment enhances the percutaneous permeation of hydrophilic compounds with high melting points. BMC Pharmacol. Toxicol. 2012, 13, 5. [Google Scholar] [CrossRef] [Green Version]
- Sepassi, S.; Goodwin, D.J.; Drake, A.F.; Holland, S.; Leonard, G.; Martini, L.; Lawrence, M.J. Effect of polymer molecular weight on the production of drug nanoparticles. J. Pharm. Sci. 2007, 96, 2655–2666. [Google Scholar] [CrossRef]
- Davies, N.M.; Anderson, K.E. Clinical pharmacokinetics of diclofenac. Therapeutic insights and pitfalls. Clin. Pharmacokinet. 1997, 33, 184–213. [Google Scholar] [CrossRef]
- Vieno, N.; Sillanpää, M. Fate of diclofenac in municipal wastewater treatment plant—A review. Environ. Int. 2014, 69, 28–39. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Substance | Wavelength (nm) | Injection Volume (µL) | Flow-Rate (mL/min) | Mobile Phase (v/v) | Limit of Detection (ng/mL) | Limit of Quantification (ng/mL) | Molecular Weight [g/mol] | Octanol-Water-Coefficient (logKow) | Melting Point [°C] |
|---|---|---|---|---|---|---|---|---|---|
| Diclofenac | 238 | 30 | 1.5 | 80:20 MeOH:MICP | 5.5 | 20 | 296 | 4.51 | 289 |
| Enrofloxacin | excitation 280/emission 450 | 30 | 1.5 | 85:15 Citrate buffer:ACN | 0.2 | 0.6 | 359 | 0.70 | 220 |
| Flufenamic acid | 284 | 30 | 1.0 | 80:20 MeOH:MICP | 14.4 | 50 | 281 | 4.67 | 134 |
| Indomethacin | 237 | 100 | 1.5 | 70:30 ACN:MICP | 27.2 | 50 | 357 | 3.10 | 158 |
| Salicylic acid | 239 | 100 | 1.5 | 30:70 ACN:MICP | 54.2 | 200 | 138 | 2.06 | 158 |
| Papp Values (cm/s) | Lagtime (h) | |||
|---|---|---|---|---|
| DERMADROP TDA | Control | DERMADROP TDA | Control | |
| Diclofenac | 4.42 × 10−8 ± 1.54 × 10−8 * | 2.15 × 10−8 ± 1.24 × 10−8 | 2.58 ± 2.24 | 3.13 ± 1.89 |
| Enrofloxacin | 6.59 × 10−8 ± 2.03 × 10−8 * | 3.98 × 10−8 ± 1.29 × 10−8 | 0.68 ± 1.16 | 1.32 ± 1.55 |
| Flufenamic acid | 7.45 × 10−9 ± 4.05 × 10−9 | 1.73 × 10−9 ± 2.49 × 10−9 | 12.23 ± 8.47 | 9.28 ± 10.90 |
| Indomethacin | 9.60 × 10−8 ± 3.40 × 10−8 * | 5.42 × 10−8 ± 2.59 × 10−8 | 2.09 ± 2.17 | 1.14 ± 1.78 |
| Salicylic acid | 6.96 × 10−8 ± 1.16 × 10−7 * | 9.25 × 10−9 ± 5.12 × 10−9 | 1.97 ± 0.97 | 2.42 ± 0.13 |
| Recovery (%) | Recovery DERMADROP TDA/ | ||
|---|---|---|---|
| DERMADROP TDA | Control | Recovery Control | |
| Diclofenac | 42.58 ± 14.40 * | 22.26 ± 14.14 | 2 |
| Enrofloxacin | 62.08 ± 18.54 | 40.43 ± 14.66 | 2 |
| Flufenamic acid | 3.06 ± 3.01 | 0.79 ± 1.20 | 4 |
| Indomethacin | 89.13 ± 14.52 * | 57.21 ± 21.68 | 2 |
| Salicylic acid | 39.15 ± 29.79 * | 5.30 ± 12.64 | 7 |
| Thickness of the Stratum Corneum [µm] | |
|---|---|
| DERMADROP TDA | Control |
| 13.96 ± 2.55 | 13.17 ± 2.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elksnat, A.-L.; Zscherpe, P.; Klein, K.; Cavalleri, J.M.; Meißner, J. Effect of an Oxygen-Based Mechanical Drug Delivery System on Percutaneous Permeation of Various Substances In Vitro. Pharmaceutics 2022, 14, 2722. https://doi.org/10.3390/pharmaceutics14122722
Elksnat A-L, Zscherpe P, Klein K, Cavalleri JM, Meißner J. Effect of an Oxygen-Based Mechanical Drug Delivery System on Percutaneous Permeation of Various Substances In Vitro. Pharmaceutics. 2022; 14(12):2722. https://doi.org/10.3390/pharmaceutics14122722
Chicago/Turabian StyleElksnat, Anna-Lena, Paula Zscherpe, Karina Klein, Jessika Maximiliane Cavalleri, and Jessica Meißner. 2022. "Effect of an Oxygen-Based Mechanical Drug Delivery System on Percutaneous Permeation of Various Substances In Vitro" Pharmaceutics 14, no. 12: 2722. https://doi.org/10.3390/pharmaceutics14122722