
Current Status of Therapeutic Drug Monitoring in Mental Health Treatment: A Review

Abstract
:1. Introduction
- 2.
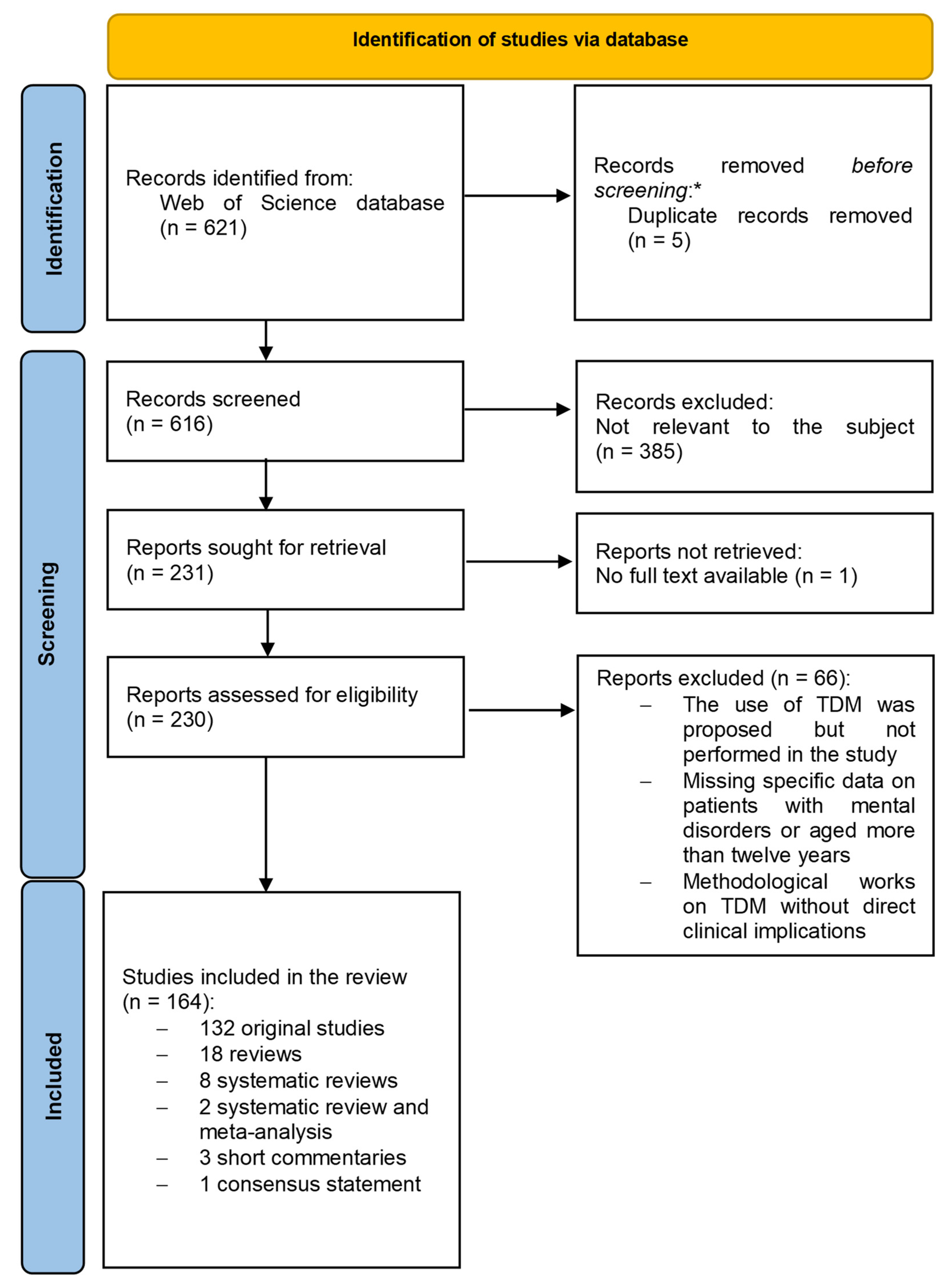
- Methods
- 3.
- Results and Discussion
- 3.1
- Individual Dose Finding
- 3.1.1
- Clinical Efficacy
- Schizophrenia Spectrum Disorders
- Bipolar Disorders
- Depressive Disorders
- 3.1.2
- Safety
- Clozapine
- Olanzapine, Other Antipsychotics, Antidepressants
- 3.2
- Adherence
- 3.3
- Special Populations
- 3.3.1
- Peripartum
- 3.3.2
- Adolescents
- 3.3.3
- Elderly Patients
- 3.3.4
- Extreme Body Weight
- Obesity
- Low Body Weight and Eating Disorders
- 3.3.5
- Other Medical and Surgical Conditions That Might Influence Pharmacokinetics
- 3.4
- Drug–Drug and Drug–Smoke Interactions
- 3.4.1
- Drug–Drug Interactions
- 3.4.2
- Drug–Smoke Interaction
- 3.4.3
- Other Interactions
- 3.5
- Pharmacogenetics and TDM
- 3.5.1
- Antipsychotics
- 3.5.2
- Antidepressants and Other Psychotropic Drugs
- 3.6
- Novel Approaches Toward Minimally Invasive TDM
- 3.6.1
- Dried Blood Spot Analysis (DBS)
- 3.6.2
- Volumetric Absorptive Microsampling (VAMS)
- 3.6.3
- Oral Fluid Analysis
- 3.6.4
- Other Non- or Mini-Invasive Procedures
- 3.7
- Towards Precision Pharmacotherapy in Psychiatry
- 4.
- Conclusions
2. Materials
3. Results and Discussion
3.1. Individual Dose Finding
3.1.1. Clinical Efficacy
Schizophrenia Spectrum Disorders
Bipolar Disorders
Depressive Disorders
3.1.2. Safety
Clozapine
Olanzapine, Other Antipsychotics, Antidepressants
3.2. Adherence
3.3. Special Populations
3.3.1. Peripartum
3.3.2. Adolescents
3.3.3. Elderly Patients
3.3.4. Extreme Body Weight
Obesity
Low Body Weight and Eating Disorders
3.3.5. Other Medical and Surgical Conditions That Might Influence Pharmacokinetics
3.4. Interactions with Psychotropic Drugs
3.4.1. Drug–Drug Interactions
3.4.2. Drug–Smoke Interaction
3.4.3. Other Interactions
3.5. Pharmacogenetics and TDM
3.5.1. Antipsychotics
3.5.2. Antidepressants and Other Psychotropic Drugs
3.6. Novel Approaches toward Minimally Invasive TDM
3.6.1. Dried Blood Spot Analysis (DBS)
3.6.2. Volumetric Absorptive Microsampling (VAMS)
3.6.3. Oral Fluid Analysis
3.6.4. Other Non- or Mini-Invasive Procedures
3.7. Towards Precision Pharmacotherapy in Psychiatry
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hiemke, C. Clinical Utility of Drug Measurement and Pharmacokinetics: Therapeutic Drug Monitoring in Psychiatry. Eur. J. Clin. Pharmacol. 2008, 64, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Hiemke, C.; Bergemann, N.; Clement, H.W.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, 9–62. [Google Scholar] [CrossRef] [Green Version]
- Herzog, D.P.; Wagner, S.; Ruckes, C.; Tadic, A.; Roll, S.C.; Härter, M.; Lieb, K. Guideline Adherence of Antidepressant Treatment in Outpatients with Major Depressive Disorder: A Naturalistic Study. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 267, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Conca, A.; Schmidt, E.; Pastore, M.; Hiemke, C.; Duffy, D.; Giupponi, G. Therapeutic Drug Monitoring in Italian Psychiatry. Pharmacopsychiatry 2011, 44, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Guo, G.-X.; Sun, C.; Zhang, J.; Rong, Z.; He, J.; Sun, Z.-L.; Yan, F.; Tang, Y.-L.; Wang, C.-Y.; et al. Therapeutic Drug Monitoring of Psychotropic Drugs in China: A Nationwide Survey. Ther. Drug Monit. 2013, 35, 816–822. [Google Scholar] [CrossRef]
- Okada, K.; Yamada, K.; Usui, K.; Ouchi, R.; Nibuya, M.; Takahashi, A.; Shito, Y.; Watanabe, Y.; Suzuki, E. Inadequate Therapeutic Drug Monitoring in Patients with Lithium Toxicity in Japan. Psychiatry Clin. Neurosci. 2020, 74, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Meehan, T.; Wang, H.; Drummond, A.; Lockman, H. Therapeutic Drug Monitoring (TDM) during Maintenance Phase Treatment at a Community Mental Health Centre. Australas. Psychiatry 2019, 27, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Nederlof, M.; Heerdink, E.R.; Egberts, A.C.G.; Wilting, I.; Stoker, L.J.; Hoekstra, R.; Kupka, R.W. Monitoring of Patients Treated with Lithium for Bipolar Disorder: An International Survey. Int. J. Bipolar Disord. 2018, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Ooba, N.; Tsutsumi, D.; Kobayashi, N.; Hidaka, S.; Hayashi, H.; Obara, T.; Satoh, M.; Kubota, K.; Fukuoka, N. Prevalence of Therapeutic Drug Monitoring for Lithium and the Impact of Regulatory Warnings: Analysis Using Japanese Claims Database. Ther. Drug Monit. 2018, 40, 252–256. [Google Scholar] [CrossRef] [Green Version]
- Ozunal, Z.G.; Ongen İpek, B. Therapeutic Drug Monitoring Characteristics in a Tertiary University Hospital in 2019. Cureus 2020, 12, e7612. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Baumann, P.; Conca, A.; Dietmaier, O.; Giupponi, G.; Gründer, G.; Hahn, M.; Hart, X.; Havemann-Reinecke, U.; Hefner, G.; et al. Therapeutic Drug Monitoring of Long-Acting Injectable Antipsychotic Drugs. Ther. Drug Monit. 2021, 43, 79–102. [Google Scholar] [CrossRef]
- Toja-Camba, F.J.; Gesto-Antelo, N.; Maroñas, O.; Echarri Arrieta, E.; Zarra-Ferro, I.; González-Barcia, M.; Bandín-Vilar, E.; Mangas Sanjuan, V.; Facal, F.; Arrojo Romero, M.; et al. Review of Pharmacokinetics and Pharmacogenetics in Atypical Long-Acting Injectable Antipsychotics. Pharmaceutics 2021, 13, 935. [Google Scholar] [CrossRef] [PubMed]
- Eap, C.B.; Gründer, G.; Baumann, P.; Ansermot, N.; Conca, A.; Corruble, E.; Crettol, S.; Dahl, M.L.; de Leon, J.; Greiner, C.; et al. Tools for Optimising Pharmacotherapy in Psychiatry (Therapeutic Drug Monitoring, Molecular Brain Imaging and Pharmacogenetic Tests): Focus on Antidepressants. World J. Biol. Psychiatry 2021, 22, 561–628. [Google Scholar] [CrossRef] [PubMed]
- Mandrioli, R.; Protti, M.; Mercolini, L. New-Generation, Non-SSRI Antidepressants: Therapeutic Drug Monitoring and Pharmacological Interactions. Part 1: SNRIs, SMSs, SARIs. Curr. Med. Chem. 2018, 25, 772–792. [Google Scholar] [CrossRef]
- Protti, M.; Mandrioli, R.; Marasca, C.; Cavalli, A.; Serretti, A.; Mercolini, L. New-Generation, Non-SSRI Antidepressants: Drug-Drug Interactions and Therapeutic Drug Monitoring. Part 2: NaSSAs, NRIs, SNDRIs, MASSAs, NDRIs, and Others. Med. Res. Rev. 2020, 40, 1794–1832. [Google Scholar] [CrossRef] [PubMed]
- Hiemke, C. Concentration-Effect Relationships of Psychoactive Drugs and the Problem to Calculate Therapeutic Reference Ranges. Ther. Drug Monit. 2019, 41, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Molden, E. Therapeutic Drug Monitoring of Clozapine in Adults with Schizophrenia: A Review of Challenges and Strategies. Expert Opin. Drug Metab. Toxicol. 2021, 17, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Arnaiz, J.A.; Rodrigues-Silva, C.; Mezquida, G.; Amoretti, S.; Cuesta, M.J.; Fraguas, D.; Lobo, A.; González-Pinto, A.; Díaz-Caneja, M.C.; Corripio, I.; et al. The Usefulness of Olanzapine Plasma Concentrations in Monitoring Treatment Efficacy and Metabolic Disturbances in First-Episode Psychosis. Psychopharmacology 2021, 238, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Nagai, G.; Mihara, K.; Nakamura, A.; Nemoto, K.; Kagawa, S.; Suzuki, T.; Kondo, T. Prediction of an Optimal Dose of Aripiprazole in the Treatment of Schizophrenia From Plasma Concentrations of Aripiprazole Plus Its Active Metabolite Dehydroaripiprazole at Week 1. Ther. Drug Monit. 2017, 39, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Tien, Y.; Huang, H.P.; Liao, D.L.; Huang, S.C. Dose-response analysis of aripiprazole in patients with schizophrenia in Taiwan. Ther. Adv. Psychopharmacol. 2022, 12, 20451253221113238. [Google Scholar] [CrossRef] [PubMed]
- Hart, X.M.; Hiemke, C.; Eichentopf, L.; Lense, X.M.; Clement, H.W.; Conca, A.; Faltraco, F.; Florio, V.; Grüner, J.; Havemann-Reinecke, U.; et al. Therapeutic Reference Range for Aripiprazole in Schizophrenia Revised: A Systematic Review and Metaanalysis. Psychopharmacology 2022, 239, 3377–3391. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, A.; Post, F.; Yalcin-Siedentopf, N.; Baumgartner, S.; Biedermann, F.; Edlinger, M.; Kemmler, G.; Rettenbacher, M.A.; Widschwendter, C.G.; Zernig, G.; et al. Corrigendum to “Changes in Psychopathology in Schizophrenia Patients Starting Treatment with New-Generation Antipsychotics: Therapeutic Drug Monitoring in a Naturalistic Treatment Setting”. Eur. Neuropsychopharmacol. 2020, 31, 162–163. [Google Scholar] [CrossRef] [PubMed]
- Paulzen, M.; Haen, E.; Stegmann, B.; Unterecker, S.; Hiemke, C.; Gründer, G.; Schoretsanitis, G. Clinical Response in a Risperidone-Medicated Naturalistic Sample: Patients’ Characteristics and Dose-Dependent Pharmacokinetic Patterns. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 267, 325–333. [Google Scholar] [CrossRef]
- Yada, Y.; Kitagawa, K.; Sakamoto, S.; Ozawa, A.; Nakada, A.; Kashiwagi, H.; Okahisa, Y.; Takao, S.; Takaki, M.; Kishi, Y.; et al. The Relationship between Plasma Clozapine Concentration and Clinical Outcome: A Cross-Sectional Study. Acta Psychiatr. Scand. 2021, 143, 227–237. [Google Scholar] [CrossRef]
- Kyllesø, L.; Smith, R.L.; Karlstad, Ø.; Andreassen, O.A.; Molden, E. Absolute and Dose-Adjusted Serum Concentrations of Clozapine in Patients Switching vs. Maintaining Treatment: An Observational Study of 1979 Patients. CNS Drugs 2021, 35, 999–1008. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Kane, J.M.; Ruan, C.-J.; Spina, E.; Hiemke, C.; de Leon, J. A Comprehensive Review of the Clinical Utility of and a Combined Analysis of the Clozapine/Norclozapine Ratio in Therapeutic Drug Monitoring for Adult Patients. Expert Rev. Clin. Pharmacol. 2019, 12, 603–621. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Kasudhan, K.S.; Murali, N.; Patil, A.N.; Pattanaik, S.; Chakrabarti, S.; Avasthi, A. Pharmacometabolomics-Guided Clozapine Therapy in Treatment Resistant Schizophrenia: Preliminary Exploration of Future Too Near. Asian J. Psychiatr. 2022, 67, 102939. [Google Scholar] [CrossRef]
- Whiskey, E.; Romano, G.; Elliott, M.; Campbell, M.; Anandarajah, C.; Taylor, D.; Valsraj, K. Possible Pharmacogenetic Factors in Clozapine Treatment Failure: A Case Report. Ther. Adv. Psychopharmacol. 2021, 11, 20451253211030844. [Google Scholar] [CrossRef] [PubMed]
- Olmos, I.; Ibarra, M.; Vázquez, M.; Maldonado, C.; Fagiolino, P.; Giachetto, G. Population Pharmacokinetics of Clozapine and Norclozapine and Switchability Assessment between Brands in Uruguayan Patients with Schizophrenia. BioMed Res. Int. 2019, 2019, 3163502. [Google Scholar] [CrossRef]
- Oloyede, E.; Dzahini, O.; Whiskey, E.; Taylor, D. Clozapine and Norclozapine Plasma Levels in Patients Switched between Different Liquid Formulations. Ther. Drug Monit. 2020, 42, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Melkote, R.; Singh, A.; Vermeulen, A.; Remmerie, B.; Savitz, A. Relationship between Antipsychotic Blood Levels and Treatment Failure during the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Study. Schizophr. Res. 2018, 201, 324–328. [Google Scholar] [CrossRef]
- McCutcheon, R.; Beck, K.; D’Ambrosio, E.; Donocik, J.; Gobjila, C.; Jauhar, S.; Kaar, S.; Pillinger, T.; Reis Marques, T.; Rogdaki, M.; et al. Antipsychotic Plasma Levels in the Assessment of Poor Treatment Response in Schizophrenia. Acta Psychiatr. Scand. 2018, 137, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Kyllesø, L.; Smith, R.L.; Karlstad, Ø.; Andreassen, O.A.; Molden, E. Undetectable or Subtherapeutic Serum Levels of Antipsychotic Drugs Preceding Switch to Clozapine. NPJ Schizophr. 2020, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Javelot, H.; Rangoni, F.; Weiner, L.; Michel, B. High-Dose Quetiapine and Therapeutic Monitoring. Eur. J. Hosp. Pharm. 2019, 26, 285–287. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Spina, E.; Hiemke, C.; de Leon, J. A Systematic Review and Combined Analysis of Therapeutic Drug Monitoring Studies for Long-Acting Paliperidone. Expert Rev. Clin. Pharmacol. 2018, 11, 1237–1253. [Google Scholar] [CrossRef] [PubMed]
- Schoretsanitis, G.; Haen, E.; Piacentino, D.; Conca, A.; Endres, K.; Hiemke, C.; Gründer, G.; Paulzen, M. Clinical Response in Patients Treated with Once-Monthly Paliperidone Palmitate: Analysis of a Therapeutic Drug Monitoring (TDM) Database. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 1437–1443. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Haen, E.; Piacentino, D.; Conca, A.; Endres, K.; Hiemke, C.; Gründer, G.; Paulzen, M. Effects of Body Weight, Smoking Status, and Sex on Plasma Concentrations of Once-Monthly Paliperidone Palmitate. Expert Rev. Clin. Pharmacol. 2022, 15, 243–249. [Google Scholar] [CrossRef]
- Hýža, M.; Šilhán, P.; Češková, E.; Skřont, T.; Kacířová, I.; Uřinovská, R.; Grundmann, M. Plasma Levels of Long-Acting Injectable Antipsychotics in Outpatient Care: A Retrospective Analysis. Neuropsychiatr. Dis. Treat. 2021, 17, 1069–1075. [Google Scholar] [CrossRef]
- D’Anna, G.; Rotella, F.; Santarelli, G.; Scannerini, S.; Fanelli, A.; Ricca, V.; Ballerini, A. Therapeutic Drug Monitoring of Long-Acting Injectable Antipsychotics as a Predictor of Relapse in Schizophrenia Spectrum Disorders: A One-Year Pilot Study. Ther. Drug Monit. 2022, 43, 79–102. [Google Scholar] [CrossRef]
- Mauri, M.C.; Paletta, S.; Di Pace, C.; Reggiori, A.; Cirnigliaro, G.; Valli, I.; Altamura, A.C. Clinical Pharmacokinetics of Atypical Antipsychotics: An Update. EXCLI J. 2014, 13, 1163–1191. [Google Scholar] [CrossRef]
- Periclou, A.; Willavize, S.; Jaworowicz, D.; Passarell, J.; Carrothers, T.; Ghahramani, P.; Durgam, S.; Earley, W.; Kapás, M.; Khariton, T. Relationship Between Plasma Concentra-tions and Clinical Effects of Cariprazine in Patients With Schizophrenia or Bipolar Mania. Clin. Transl. Sci. 2020, 13, 362–371. [Google Scholar] [CrossRef] [Green Version]
- Malhi, G.S.; Gershon, S.; Outhred, T. Lithiumeter: Version 2.0. Bipolar Disord. 2016, 18, 631–641. [Google Scholar] [CrossRef]
- Mauri, M.C.; Reggiori, A.; Minutillo, A.; Franco, G.; Pace, C.D.; Paletta, S.; Cattaneo, D. Paliperidone LAI and Aripiprazole LAI Plasma Level Monitoring in the Prophylaxis of Bipolar Disorder Type I with Manic Predominance. Pharmacopsychiatry 2020, 53, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Funk, C.S.; Hart, X.M.; Gründer, G.; Hiemke, C.; Elsner, B.; Kreutz, R.; Riemer, T.G. Is Therapeutic Drug Monitoring Relevant for Antidepressant Drug Therapy? Implications from a Systematic Review and Meta-Analysis with Focus on Moderating Factors. Front. Psychiatry 2022, 13, 826138. [Google Scholar] [CrossRef]
- Tveit, K.; Hermann, M.; Waade, R.B.; Nilsen, R.M.; Wallerstedt, S.M.; Molden, E. Use of Antidepressants in Older People during a 10-Year Period: An Observational Study on Prescribed Doses and Serum Levels. Drugs Aging 2020, 37, 691–701. [Google Scholar] [CrossRef]
- Cellini, L.; De Donatis, D.; Zernig, G.; De Ronchi, D.; Giupponi, G.; Serretti, A.; Xenia, H.; Conca, A.; Florio, V. Antidepressant efficacy is correlated with plasma levels: Mega-analysis and further evidence. Int. Clin. Psychopharmacol. 2021, 37, 29–37. [Google Scholar] [CrossRef]
- De Donatis, D.; Porcelli, S.; Zernig, G.; Mercolini, L.; Giupponi, G.; Serretti, A.; Conca, A.; Florio, V. Venlafaxine and O-Desmethylvenlafaxine Serum Levels Are Positively Associated with Antidepressant Response in Elder Depressed out-Patients. World J. Biol. Psychiatry 2021, 23, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.R.; Kuhlmann, I.B.; Pottegård, A.; Damkier, P. Therapeutic Drug Monitoring of Venlafaxine in an Everyday Clinical Setting: Analysis of Age, Sex and Dose Concentration Relationships. Basic Clin. Pharmacol. Toxicol. 2017, 121, 298–302. [Google Scholar] [CrossRef] [Green Version]
- Bustillo, M.; Zabala, A.; Querejeta, I.; Carton, J.I.; Mentxaka, O.; González-Pinto, A.; García, S.; Meana, J.J.; Eguiluz, J.I.; Segarra, R. Therapeutic Drug Monitoring of Second-Generation Antipsychotics for the Estimation of Early Drug Effect in First-Episode Psychosis: A Cross-Sectional Assessment. Ther. Drug Monit. 2018, 40, 257–267. [Google Scholar] [CrossRef]
- Kitchen, D.; Till, A.; Xavier, P. Routine Clozapine Assay Monitoring to Improve the Management of Treatment-Resistant Schizophrenia. BJPsych Bull. 2021, 46, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Hart, X.M.; Konietzko, R.A.A.; Hirjak, D.; Gruender, G. Case Report: Therapeutic Drug Monitoring in a Female Schizophrenia Patient with Self-Induced Clozapine Intoxication Using Point-of-Care Testing. Eur. Neuropsychopharmacol. 2020, 40, S278. [Google Scholar] [CrossRef]
- Smith, R.L.; Haslemo, T.; Andreassen, O.A.; Eliasson, E.; Dahl, M.-L.; Spigset, O.; Molden, E. Correlation between Serum Concentrations of N-Desmethylclozapine and Granulocyte Levels in Patients with Schizophrenia: A Retrospective Observational Study. CNS Drugs 2017, 31, 991–997. [Google Scholar] [CrossRef]
- Diaz, F.J.; Josiassen, R.C.; de Leon, J. The Effect of Body Weight Changes on Total Plasma Clozapine Concentrations Determined by Applying a Statistical Model to the Data from a Double-Blind Trial. J. Clin. Psychopharmacol. 2018, 38, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Schoretsanitis, G.; Kuzin, M.; Kane, J.M.; Hiemke, C.; Paulzen, M.; Haen, E. Elevated Clozapine Concentrations in Clozapine-Treated Patients with Hypersalivation. Clin. Pharmacokinet. 2021, 60, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Skokou, M.; Karavia, E.A.; Drakou, Z.; Konstantinopoulou, V.; Kavakioti, C.A.; Gourzis, P.; Kavakioti, C.; Gourzis, P.; Kypreos, K.E.; Andreopoulou, O. Adverse Drug Reactions in Relation to Clozapine Plasma Levels: A Systematic Review. Pharmaceuticals 2022, 15, 817. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Lu, J.; Liu, W.; Shao, P.; Wu, R. Association between olanzapine concentration and metabolic dysfunction in drug-naive and chronic patients: Similarities and differences. Schizophr 2022, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Fan, H.; Yun, Y.; Chen, S.; Qi, S.; Ma, B.; Shi, J.; Wang, Z.; Yang, F. Relationship between Plasma Olanzapine and N-Desmethyl-Olanzapine Concentration and Metabolic Parameters in Patients with Schizophrenia. Front. Psychiatry 2022, 13, 930457. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.-L.; Chen, C.-H.; Kuo, P.-T.; Lin, C.-H.; Wu, T.-H. Application of Plasma Levels of Olanzapine and N-Desmethyl-Olanzapine to Monitor Metabolic Parameters in Patients with Schizophrenia. Schizophr Res. 2018, 193, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Carli, M.; Kolachalam, S.; Longoni, B.; Pintaudi, A.; Baldini, M.; Aringhieri, S.; Fasciani, I.; Annibale, P.; Maggio, R.; Scarselli, M. Atypical Antipsychotics and Metabolic Syndrome: From Molecular Mechanisms to Clinical Differences. Pharmaceuticals 2021, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, J.; Wagner, S.; Solheid, A.; Herzog, D.P.; Dreimüller, N.; Müller, M.B.; Tadić, A.; Hiemke, C.; Lieb, K. Tolerability of High-Dose Venlafaxine after Switch from Escitalopram in Nonresponding Patients with Major Depressive Disorder. J. Clin. Psychopharmacol. 2021, 41, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Schoretsanitis, G.; Haen, E.; Piacentino, D.; Conca, A.; Endres, K.; Carpi, F.; Hiemke, C.; Gründer, G.; Paulzen, M. Pharmacokinetic Correlates of Once-Monthly Paliperidone Palmitate-Related Adverse Drug Reactions. Clin. Pharmacokinet. 2021, 60, 1583–1589. [Google Scholar] [CrossRef] [PubMed]
- Veselinović, T.; Scharpenberg, M.; Heinze, M.; Cordes, J.; Mühlbauer, B.; Juckel, G.; Rüther, E.; Paulzen, M.; Haen, E.; Hiemke, C.; et al. Dopamine D2 Receptor Occupancy Estimated from Plasma Concentrations of Four Different Antipsychotics and the Subjective Experience of Physical and Mental Well-Being in Schizophrenia: Results from the Randomized NeSSy Trial. J. Clin. Psychopharmacol. 2019, 39, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Haddad, P.M.; Brain, C.; Scott, J. Nonadherence with Antipsychotic Medication in Schizophrenia: Challenges and Management Strategies. Patient Relat. Outcome Meas. 2014, 5, 43–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashi, K.; Medic, G.; Littlewood, K.J.; Diez, T.; Granström, O.; De Hert, M. Medication Adherence in Schizophrenia: Factors Influencing Adherence and Consequences of Nonadherence, a Systematic Literature Review. Ther. Adv. Psychopharmacol. 2013, 3, 200–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murru, A.; Pacchiarotti, I.; Amann, B.L.; Nivoli, A.M.A.; Vieta, E.; Colom, F. Treatment Adherence in Bipolar I and Schizoaffective Disorder, Bipolar Type. J. Affect. Disord. 2013, 151, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Emsley, R.; Chiliza, B.; Asmal, L.; Harvey, B.H. The Nature of Relapse in Schizophrenia. BMC Psychiatry 2013, 13, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geretsegger, C.; Pichler, E.-M.; Gimpl, K.; Aichhorn, W.; Stelzig, R.; Grabher-Stoeffler, G.; Hiemke, C.; Zernig, G. Non-Adherence to Psychotropic Medication Assessed by Plasma Level in Newly Admitted Psychiatric Patients: Prevalence before Acute Admission. Psychiatry Clin. Neurosci. 2019, 73, 175–178. [Google Scholar] [CrossRef]
- Silhan, P.; Urinovska, R.; Kacirova, I.; Hyza, M.; Grundmann, M.; Ceskova, E. What Does Antidepressant Drug Level Monitoring Reveal about Outpatient Treatment and Patient Adherence? Pharmacopsychiatry 2019, 52, 78–83. [Google Scholar] [CrossRef]
- Baldelli, S.; Cheli, S.; Montrasio, C.; Cattaneo, D.; Clementi, E. Therapeutic Drug Monitoring and Pharmacogenetics of Antipsychotics and Antidepressants in Real Life Settings: A 5-Year Single Centre Experience. World J. Biol. Psychiatry 2021, 22, 34–45. [Google Scholar] [CrossRef]
- Lopez, L.V.; Shaikh, A.; Merson, J.; Greenberg, J.; Suckow, R.F.; Kane, J.M. Accuracy of Clinician Assessments of Medication Status in the Emergency Setting: A Comparison of Clinician Assessment of Antipsychotic Usage and Plasma Level Determination. J. Clin. Psychopharmacol. 2017, 37, 310–314. [Google Scholar] [CrossRef]
- Brasso, C.; Cisotto, M.; Ghirardini, C.; Pennazio, F.; Villari, V.; Rocca, P. Accuracy of Self-Reported Adherence and Therapeutic Drug Monitoring in a Psychiatric Emergency Ward. Psychiatry Res. 2021, 305, 114214. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Tveito, M.; Kyllesø, L.; Jukic, M.M.; Ingelman-Sundberg, M.; Andreassen, O.A.; Molden, E. Impact of Antipsychotic Polypharmacy on Nonadherence of Oral Antipsychotic Drugs—A Study Based on Blood Sample Analyses from 24,239 Patients. Eur. Neuropsychopharmacol. 2020, 37, 64–69. [Google Scholar] [CrossRef] [PubMed]
- El Abdellati, K.; De Picker, L.; Morrens, M. Antipsychotic Treatment Failure: A Systematic Review on Risk Factors and Interventions for Treatment Adherence in Psychosis. Front. Neurosci. 2020, 14, 531763. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Tveito, M.; Kyllesø, L.; Jukic, M.M.; Ingelman-Sundberg, M.; Andreassen, O.A.; Molden, E. Rates of Complete Nonadherence among Atypical Antipsychotic Drugs: A Study Using Blood Samples from 13,217 Outpatients with Psychotic Disorders. Schizophr Res. 2021, 228, 590–596. [Google Scholar] [CrossRef]
- Jones, I.; Chandra, P.S.; Dazzan, P.; Howard, L.M. Bipolar Disorder, Affective Psychosis, and Schizophrenia in Pregnancy and the Post-Partum Period. Lancet 2014, 384, 1789–1799. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Kane, J.M.; Correll, C.U.; Marder, S.R.; Citrome, L.; Newcomer, J.W.; Robinson, D.G.; Goff, D.C.; Kelly, D.L.; Freudenreich, O.; et al. Blood Levels to Optimize Antipsychotic Treatment in Clinical Practice: A Joint Consensus Statement of the American Society of Clinical Psychopharmacology and the Therapeutic Drug Monitoring Task Force of the Arbeitsgemeinschaft Für Neuropsychopharmakologie Und Pharmakopsychiatrie. J. Clin. Psychiatry 2020, 81, 19cs13169. [Google Scholar] [CrossRef]
- Leutritz, A.L.; van Braam, L.; Preis, K.; Gehrmann, A.; Scherf-Clavel, M.; Fiedler, K.; Unterecker, S.; Kittel-Schneider, S. Psychotropic medication in pregnancy and lactation and early development of exposed children. Br. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Huang, S.; Li, L.; Wang, Z.; Xiao, T.; Li, X.; Liu, S.; Zhang, M.; Lu, H.; Wen, Y.; Shang, D. Modeling and Simulation for Individualized Therapy of Amisulpride in Chinese Patients with Schizophrenia: Focus on Interindividual Variability, Therapeutic Reference Range and the Laboratory Alert Level. Drug Des. Dev. Ther. 2021, 15, 3903–3913. [Google Scholar] [CrossRef]
- Westin, A.A.; Brekke, M.; Molden, E.; Skogvoll, E.; Aadal, M.; Spigset, O. Changes in Drug Disposition of Lithium during Pregnancy: A Retrospective Observational Study of Patient Data from Two Routine Therapeutic Drug Monitoring Services in Norway. BMJ Open 2017, 7, e015738. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.T.; Newmark, R.L.; Wisner, K.L.; Stika, C.; Avram, M.J. Lithium Pharmacokinetics in the Perinatal Patient with Bipolar Disorder. J. Clin. Pharm. 2022, 62, 1385–1392. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Spigset, O.; Stingl, J.C.; Deligiannidis, K.M.; Paulzen, M.; Westin, A.A. The Impact of Pregnancy on the Pharmacokinetics of Antidepressants: A Systematic Critical Review and Meta-Analysis. Expert Opin. Drug Metab. Toxicol. 2020, 16, 431–440. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Augustin, M.; Saßmannshausen, H.; Franz, C.; Gründer, G.; Paulzen, M. Antidepressants in Breast Milk; Comparative Analysis of Excretion Ratios. Arch. Womens Ment. Health 2019, 22, 383–390. [Google Scholar] [CrossRef]
- Heinonen, E.; Blennow, M.; Blomdahl-Wetterholm, M.; Hovstadius, M.; Nasiell, J.; Pohanka, A.; Gustafsson, L.L.; Wide, K. Sertraline Concentrations in Pregnant Women Are Steady and the Drug Transfer to Their Infants Is Low. Eur. J. Clin. Pharmacol. 2021, 77, 1323–1331. [Google Scholar] [CrossRef]
- Westin, A.A.; Brekke, M.; Molden, E.; Skogvoll, E.; Castberg, I.; Spigset, O. Treatment with Antipsychotics in Pregnancy: Changes in Drug Disposition. Clin. Pharmacol. Ther. 2018, 103, 477–484. [Google Scholar] [CrossRef]
- Gogtay, N.; Vyas, N.S.; Testa, R.; Wood, S.J.; Pantelis, C. Age of Onset of Schizophrenia: Perspectives from Structural Neuroimaging Studies. Schizophr Bull. 2011, 37, 504–513. [Google Scholar] [CrossRef] [Green Version]
- Bolton, S.; Warner, J.; Harriss, E.; Geddes, J.; Saunders, K.E.A. Bipolar Disorder: Trimodal Age-at-Onset Distribution. Bipolar Disord. 2021, 23, 341–356. [Google Scholar] [CrossRef]
- Yee, C.S.; Hawken, E.R.; Baldessarini, R.J.; Vázquez, G.H. Maintenance Pharmacological Treatment of Juvenile Bipolar Disorder: Review and Meta-Analyses. Int. J. Neuropsychopharmacol. 2019, 22, 531–540. [Google Scholar] [CrossRef]
- Krause, M.; Zhu, Y.; Huhn, M.; Schneider-Thoma, J.; Bighelli, I.; Chaimani, A.; Leucht, S. Efficacy, Acceptability, and Tolerability of Antipsychotics in Children and Adolescents with Schizophrenia: A Network Meta-Analysis. Eur. Neuropsychopharmacol. 2018, 28, 659–674. [Google Scholar] [CrossRef]
- MacQueen, G.M.; Frey, B.N.; Ismail, Z.; Jaworska, N.; Steiner, M.; Lieshout, R.J.V.; Kennedy, S.H.; Lam, R.W.; Milev, R.V.; Parikh, S.V.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 6. Special Populations: Youth, Women, and the Elderly. Can. J. Psychiatry 2016, 61, 588–603. [Google Scholar] [CrossRef] [Green Version]
- Cipriani, A.; Zhou, X.; Del Giovane, C.; Hetrick, S.E.; Qin, B.; Whittington, C.; Coghill, D.; Zhang, Y.; Hazell, P.; Leucht, S.; et al. Comparative Efficacy and Tolerability of Antidepressants for Major Depressive Disorder in Children and Adolescents: A Network Meta-Analysis. Lancet 2016, 388, 881–890. [Google Scholar] [CrossRef]
- Tini, E.; Smigielski, L.; Romanos, M.; Wewetzer, C.; Karwautz, A.; Reitzle, K.; Correll, C.U.; Plener, P.L.; Malzahn, U.; Heuschmann, P. Therapeutic drug monitoring of sertraline in children and adolescents: A naturalistic study with insights into the clinical response and treatment of obsessive-compulsive disorder. Compr. Psychiatry 2022, 115, 152301. [Google Scholar] [CrossRef]
- Fekete, S.; Hiemke, C.; Gerlach, M. Dose-Related Concentrations of Neuroactive/Psychoactive Drugs Expected in Blood of Children and Adolescents. Ther. Drug Monit. 2020, 42, 315–324. [Google Scholar] [CrossRef]
- Kloosterboer, S.M.; Vierhout, D.; Stojanova, J.; Egberts, K.M.; Gerlach, M.; Dieleman, G.C.; Hillegers, M.H.J.; Passe, K.M.; van Gelder, T.; Dierckx, B.; et al. Psychotropic Drug Concentrations and Clinical Outcomes in Children and Adolescents: A Systematic Review. Expert Opin. Drug Saf. 2020, 19, 873–890. [Google Scholar] [CrossRef]
- Strawn, J.R.; Poweleit, E.A.; Uppugunduri, C.R.S.; Ramsey, L.B. Pediatric Therapeutic Drug Monitoring for Selective Serotonin Reuptake Inhibitors. Front. Pharmacol. 2021, 12, 749692. [Google Scholar] [CrossRef]
- Fekete, S.; Scherf-Clavel, M.; Gerlach, M.; Romanos, M.; Kittel-Schneider, S.; Unterecker, S.; Egberts, K. Dose-Corrected Serum Concentrations and Metabolite to Parent Compound Ratios of Venlafaxine and Risperidone from Childhood to Old Age. Pharmacopsychiatry 2021, 54, 117–125. [Google Scholar] [CrossRef]
- Piacentino, D.; Kotzalidis, G.D.; Schoretsanitis, G.; Paulzen, M.; Haen, E.; Cappelletti, S.; Giupponi, G.; Grözinger, M.; Conca, A. Plasma Risperidone-Related Measures in Children and Adolescents with Oppositional Defiant/Conduct Disorders. Clin. Psychopharmacol. Neurosci. 2020, 18, 41–48. [Google Scholar] [CrossRef]
- Egberts, K.; Reuter-Dang, S.-Y.; Fekete, S.; Kulpok, C.; Mehler-Wex, C.; Wewetzer, C.; Karwautz, A.; Mitterer, M.; Holtkamp, K.; Boege, I.; et al. Therapeutic Drug Monitoring of Children and Adolescents Treated with Aripiprazole: Observational Results from Routine Patient Care. J. Neural Transm. 2020, 127, 1663–1674. [Google Scholar] [CrossRef]
- Gehrmann, J.; Götz Lampe, P. Serum Level Measurements Optimize Aripriprazole Treatment in Adolescent Patients. Z. Kinder. Jugendpsychiatr. Psychother. 2019, 47, 261–264. [Google Scholar] [CrossRef]
- Castberg, I.; Westin, A.A.; Skogvoll, E.; Spigset, O. Effects of Age and Gender on the Serum Levels of Clozapine, Olanzapine, Risperidone, and Quetiapine. Acta Psychiatr. Scand. 2017, 136, 455–464. [Google Scholar] [CrossRef]
- Jönsson, A.K.; Spigset, O.; Reis, M. A Compilation of Serum Concentrations of 12 Antipsychotic Drugs in a Therapeutic Drug Monitoring Setting. Ther. Drug Monit. 2019, 41, 348–356. [Google Scholar] [CrossRef]
- Reeves, S.; Eggleston, K.; Cort, E.; McLachlan, E.; Brownings, S.; Nair, A.; Greaves, S.; Smith, A.; Dunn, J.; Marsden, P.; et al. Therapeutic D2/3 Receptor Occupancies and Response with Low Amisulpride Blood Concentrations in Very Late-Onset Schizophrenia-like Psychosis (VLOSLP). Int. J. Geriatr. Psychiatry 2018, 33, 396–404. [Google Scholar] [CrossRef] [Green Version]
- Tveito, M.; Smith, R.L.; Molden, E.; Høiseth, G. Impact of Age and CYP2D6 Genotype on Exposure of Zuclopenthixol in Patients Using Long-Acting Injectable versus Oral Formulation-an Observational Study Including 2044 Patients. Eur. J. Clin. Pharmacol. 2021, 77, 215–221. [Google Scholar] [CrossRef]
- Tveito, M.; Smith, R.L.; Molden, E.; Haslemo, T.; Refsum, H.; Hartberg, C.; Correll, C.U.; Høiseth, G. Age Impacts Olanzapine Exposure Differently during Use of Oral Versus Long-Acting Injectable Formulations: An Observational Study Including 8288 Patients. J. Clin. Psychopharmacol. 2018, 38, 570–576. [Google Scholar] [CrossRef]
- Deng, S.-H.; Wang, Z.-Z.; Lu, H.-Y.; Li, L.; Hu, J.-Q.; Zhu, X.-Q.; Xie, H.-S.; Chen, H.-Z.; Zhang, M.; Ni, X.-J.; et al. A Retrospective Analysis of Steady-State Olanzapine Concentrations in Chinese Patients Using Therapeutic Drug Monitoring: Effects of Valproate and Other Factors. Ther. Drug Monit. 2020, 42, 636–642. [Google Scholar] [CrossRef]
- An, H.; Fan, H.; Chen, S.; Qi, S.; Ma, B.; Shi, J.; Wang, Z.; Yang, F. Effects of Dose, Age, Sex, Body Weight, and Smoking on Plasma Concentrations of Olanzapine and N-Desmethyl Olanzapine in Inpatients With Schizophrenia. J. Clin. Psychopharmacol. 2021, 41, 255–259. [Google Scholar] [CrossRef]
- Tveito, M.; Høiseth, G.; Haslemo, T.; Molden, E.; Smith, R.L. Impact of Age and Gender on Paliperidone Exposure in Patients after Administration of Long-Acting Injectable Formulations-an Observational Study Using Blood Samples from 1223 Patients. Eur. J. Clin. Pharmacol. 2021, 77, 1201–1208. [Google Scholar] [CrossRef]
- Smith, R.L.; Haslemo, T.; Chan, H.F.; Refsum, H.; Molden, E. Clinically Relevant Effect of UGT1A4*3 on Lamotrigine Serum Concentration Is Restricted to Postmenopausal Women—A Study Matching Therapeutic Drug Monitoring and Genotype Data From 534 Patients. Ther. Drug Monit. 2018, 40, 567–571. [Google Scholar] [CrossRef]
- Hefner, G.; Hahn, M.; Hohner, M.; Roll, S.C.; Klimke, A.; Hiemke, C. QTc Time Correlates with Amitriptyline and Venlafaxine Serum Levels in Elderly Psychiatric Inpatients. Pharmacopsychiatry 2019, 52, 38–43. [Google Scholar] [CrossRef]
- Taurines, R.; Fekete, S.; Preuss-Wiedenhoff, A.; Warnke, A.; Wewetzer, C.; Plener, P.; Burger, R.; Gerlach, M.; Romanos, M.; Egberts, K.M. Therapeutic drug monitoring in children and adolescents with schizophrenia and other psychotic disorders using risperidone. J. Neural Transm. 2022, 129, 689–701. [Google Scholar] [CrossRef]
- Kuzin, M.; Haen, E.; Hiemke, C.; Bochon, B.; Bochon, K.; Gründer, G.; Paulzen, M.; Schoretsanitis, G. Body Mass Index as a Determinant of Clozapine Plasma Concentrations: A Pharmacokinetic-Based Hypothesis. J. Psychopharmacol. 2021, 35, 273–278. [Google Scholar] [CrossRef]
- Methaneethorn, J. Population Pharmacokinetics of Valproic Acid in Patients with Mania: Implication for Individualized Dosing Regimens. Clin. Ther. 2017, 39, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Schoretsanitis, G.; Haen, E.; Hiemke, C.; Fay, B.; Unholzer, S.; Correll, C.U.; Gründer, G.; Paulzen, M. Sex and Body Weight Are Major Determinants of Venlafaxine Pharmacokinetics. Int. Clin. Psychopharmacol. 2018, 33, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Warrings, B.; Samanski, L.; Deckert, J.; Unterecker, S.; Scherf-Clavel, M. Impact of Body Mass Index on Serum Concentrations of Antidepressants and Antipsychotics. Ther. Drug Monit. 2021, 43, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Maeda, H.; Oniki, K.; Yasui-Furukori, N.; Watanabe, H.; Saruwatari, J.; Kadowaki, D. New Insight Concerning Therapeutic Drug Monitoring-The Importance of the Concept of Psychonephrology. Biol. Pharm. Bull. 2022, 45, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Moschny, N.; Hefner, G.; Grohmann, R.; Eckermann, G.; Maier, H.B.; Seifert, J.; Heck, J.; Francis, F.; Bleich, S.; Toto, S.; et al. Therapeutic Drug Monitoring of Second- and Third-Generation Antipsychotic Drugs-Influence of Smoking Behavior and Inflammation on Pharmacokinetics. Pharmaceuticals 2021, 14, 514. [Google Scholar] [CrossRef]
- Zhang, Y.-Y.; Zhou, X.-H.; Shan, F.; Liang, J. Infection Is Associated with Elevated Serum Concentrations of Antipsychotic Drugs. Int. Clin. Psychopharmacol. 2021, 36, 264–267. [Google Scholar] [CrossRef]
- Scherf-Clavel, M.; Weidner, A.; Deckert, J.; Menke, A.; Unterecker, S. Pathological Concentration of C-Reactive Protein Is Correlated to Increased Concentrations of Quetiapine, but Not of Risperidone, Olanzapine and Aripiprazole in a Naturalistic Setting. Pharmacopsychiatry 2020, 53, 30–35. [Google Scholar] [CrossRef]
- Helland, A.; Habib, S.; Ulvestad, L.; Spigset, O. Systemic Inflammation Complicates the Interpretation of Therapeutic Drug Monitoring of Risperidone. J. Clin. Psychopharmacol. 2018, 38, 263–265. [Google Scholar] [CrossRef]
- Courlet, P.; Guidi, M.; Glatard, A.; Alves Saldanha, S.; Cavassini, M.; Buclin, T.; Marzolini, C.; Eap, C.B.; Decosterd, L.A.; Csajka, C.; et al. Escitalopram Population Pharmacokinetics in People Living with Human Immunodeficiency Virus and in the Psychiatric Population: Drug-Drug Interactions and Probability of Target Attainment. Br. J. Clin. Pharmacol. 2019, 85, 2022–2032. [Google Scholar] [CrossRef]
- Wallerstedt, S.M.; Nylén, K.; Axelsson, M.A.B. Serum Concentrations of Antidepressants, Antipsychotics, and Antiepileptics over the Bariatric Surgery Procedure. Eur. J. Clin. Pharmacol. 2021, 77, 1875–1885. [Google Scholar] [CrossRef]
- McGrane, I.R.; Salyers, L.A.; Molinaro, J.R.; Munjal, R.C. Roux-En-Y Gastric Bypass and Antipsychotic Therapeutic Drug Monitoring: Two Cases. J. Pharm. Pract. 2021, 34, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, J.J.; Daly, T.M.; Jacobs, K.; Khawam, E.A.; Pozuelo, L.; Morrison, R.D.; Milne, S.B.; Daniels, J.S.; Ryan, T.P. Medication Exposure in Highly Adherent Psychiatry Patients. ACS Chem. Neurosci. 2018, 9, 555–562. [Google Scholar] [CrossRef]
- Douglas-Hall, P.; Dzahini, O.; Gaughran, F.; Bile, A.; Taylor, D. Variation in Dose and Plasma Level of Lamotrigine in Patients Discharged from a Mental Health Trust. Ther. Adv. Psychopharmacol. 2017, 7, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Paulzen, M.; Haen, E.; Hiemke, C.; Stegmann, B.; Lammertz, S.E.; Gründer, G.; Schoretsanitis, G. Cytochrome P450-Mediated Interaction between Perazine and Risperidone: Implications for Antipsychotic Polypharmacy. Br. J. Clin. Pharmacol. 2017, 83, 1668–1675. [Google Scholar] [CrossRef]
- Paulzen, M.; Schoretsanitis, G.; Stegmann, B.; Hiemke, C.; Gründer, G.; Schruers, K.R.J.; Walther, S.; Lammertz, S.E.; Haen, E. Pharmacokinetic Considerations in Antipsychotic Augmentation Strategies: How to Combine Risperidone with Low-Potency Antipsychotics. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 76, 101–106. [Google Scholar] [CrossRef]
- Jiang, P.; Sun, X.; Ren, J.; Liu, H.; Lin, Z.; Liu, J.; Fang, X.; Zhang, C. Effects of the Combination of Second-Generation Antipsychotics on Serum Concentrations of Aripiprazole and Dehydroaripiprazole in Chinese Patients with Schizophrenia. Gen. Psychiatr. 2021, 34, e100423. [Google Scholar] [CrossRef]
- Hommers, L.; Scharl, M.; Hefner, G.; Hohner, M.; Fischer, M.; Pfuhlmann, B.; Deckert, J.; Unterecker, S. Comedication of Valproic Acid Is Associated with Increased Metabolism of Clozapine. J. Clin. Psychopharmacol. 2018, 38, 188–192. [Google Scholar] [CrossRef]
- Smith, R.L.; Wollmann, B.M.; Kyllesø, L.; Tran, T.T.A.; Tveito, M.; Molden, E. Effect of Valproic Acid on the Metabolic Spectrum of Clozapine in Patients with Schizophrenia. J. Clin. Psychopharmacol. 2022, 42, 43–50. [Google Scholar] [CrossRef]
- Gaebler, A.J.; Finner-Prével, M.; Lammertz, S.; Schaffrath, S.; Eisner, P.; Stöhr, F.; Röcher, E.; Winkler, L.; Kaleta, P.; Lenzen, L.; et al. The negative impact of vitamin D on antipsychotic drug exposure may counteract its potential benefits in schizophrenia. Br. J. Clin. Pharmacol. 2022, 88, 3193–3200. [Google Scholar] [CrossRef]
- Gaebler, A.J.; Schoretsanitis, G.; Ben Omar, N.; Haen, E.; Endres, K.; Hiemke, C.; Paulzen, M. Metamizole but Not Ibuprofen Reduces the Plasma Concentration of Sertraline: Implications for the Concurrent Treatment of Pain and Depression/Anxiety Disorders. Br. J. Clin. Pharmacol. 2021, 87, 1111–1119. [Google Scholar] [CrossRef]
- Paulzen, M.; Schoretsanitis, G.; Hiemke, C.; Gründer, G.; Haen, E.; Augustin, M. Reduced Clearance of Venlafaxine in a Combined Treatment with Quetiapine. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 85, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Kuzin, M.; Schoretsanitis, G.; Haen, E.; Stegmann, B.; Hiemke, C.; Gründer, G.; Paulzen, M. Effects of the Proton Pump Inhibitors Omeprazole and Pantoprazole on the Cytochrome P450-Mediated Metabolism of Venlafaxine. Clin. Pharmacokinet. 2018, 57, 729–737. [Google Scholar] [CrossRef]
- Magalhães, P.; Alves, G.; Fortuna, A.; Llerena, A.; Falcão, A. Clinical Collaborators of the GnG-PK/PD-AD Study Pharmacogenetics and Therapeutic Drug Monitoring of Fluoxetine in a Real-World Setting: A PK/PD Analysis of the Influence of (Non-)Genetic Factors. Exp. Clin. Psychopharmacol. 2020, 28, 589–600. [Google Scholar] [CrossRef]
- Kuzin, M.; Schoretsanitis, G.; Haen, E.; Ridders, F.; Hiemke, C.; Gründer, G.; Paulzen, M. Pharmacokinetic Interactions between Clozapine and Sertraline in Smokers and Non-Smokers. Basic Clin. Pharmacol. Toxicol. 2020, 127, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Kuzin, M.; Schoretsanitis, G.; Haen, E.; Dammann, G.; Hiemke, C.; Gründer, G.; Paulzen, M. The Effects of Co-Prescription of Pantoprazole on the Clozapine Metabolism. Pharmacopsychiatry 2020, 53, 65–70. [Google Scholar] [CrossRef]
- Depp, C.A.; Bowie, C.R.; Mausbach, B.T.; Wolyniec, P.; Thornquist, M.H.; Luke, J.R.; McGrath, J.A.; Pulver, A.E.; Patterson, T.L.; Harvey, P.D. Current Smoking Is Associated with Worse Cognitive and Adaptive Functioning in Serious Mental Illness. Acta Psychiatr. Scand. 2015, 131, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Firth, J.; Solmi, M.; Wootton, R.E.; Vancampfort, D.; Schuch, F.B.; Hoare, E.; Gilbody, S.; Torous, J.; Teasdale, S.B.; Jackson, S.E.; et al. A Meta-Review of “Lifestyle Psychiatry”: The Role of Exercise, Smoking, Diet and Sleep in the Prevention and Treatment of Mental Disorders. World Psychiatry 2020, 19, 360–380. [Google Scholar] [CrossRef]
- Wang, Y.-Y.; Wang, S.; Zheng, W.; Zhong, B.-L.; Ng, C.H.; Ungvari, G.S.; Wang, C.-X.; Xiang, Y.-T.; Li, X.-H. Cognitive Functions in Smoking and Non-Smoking Patients with Schizophrenia: A Systematic Review and Meta-Analysis of Comparative Studies. Psychiatry Res. 2019, 272, 155–163. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, Mental Illness, and Public Health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [Green Version]
- Augustin, M.; Schoretsanitis, G.; Hiemke, C.; Gründer, G.; Haen, E.; Paulzen, M. Differences in Duloxetine Dosing Strategies in Smoking and Nonsmoking Patients: Therapeutic Drug Monitoring Uncovers the Impact on Drug Metabolism. J. Clin. Psychiatry 2018, 79, 17m12086. [Google Scholar] [CrossRef]
- Schoretsanitis, G.; Haen, E.; Conca, A.; Piacentino, D.; Ridders, F.; Hiemke, C.; Gründer, G.; Paulzen, M. Lack of Smoking Effects on Pharmacokinetics of Oral Paliperidone-Analysis of a Naturalistic Therapeutic Drug Monitoring Sample. Pharmacopsychiatry 2021, 54, 31–35. [Google Scholar] [CrossRef]
- Augustin, M.; Schoretsanitis, G.; Pfeifer, P.; Gründer, G.; Liebe, C.; Paulzen, M. Effect of Fluvoxamine Augmentation and Smoking on Clozapine Serum Concentrations. Schizophr Res. 2019, 210, 143–148. [Google Scholar] [CrossRef]
- Scherf-Clavel, M.; Samanski, L.; Hommers, L.G.; Deckert, J.; Menke, A.; Unterecker, S. Analysis of Smoking Behavior on the Pharmacokinetics of Antidepressants and Antipsychotics: Evidence for the Role of Alternative Pathways Apart from CYP1A2. Int. Clin. Psychopharmacol. 2019, 34, 93–100. [Google Scholar] [CrossRef]
- Hart, X.M.; Heesen, S.; Schmitz, C.N.; Dörfler, S.; Wedekind, D.; Gründer, G.; Hiemke, C.; Havemann-Reinecke, U. Concentrations of escitalopram in blood of patients treated in a naturalistic setting: Focus on patients with alcohol and benzodiazepine use disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 1–9. [Google Scholar] [CrossRef]
- Jukic, M.M.; Smith, R.L.; Haslemo, T.; Molden, E.; Ingelman-Sundberg, M. Effect of CYP2D6 Genotype on Exposure and Efficacy of Risperidone and Aripiprazole: A Retrospective, Cohort Study. Lancet Psychiatry 2019, 6, 418–426. [Google Scholar] [CrossRef]
- Waade, R.B.; Solhaug, V.; Høiseth, G. Impact of CYP2D6 on Serum Concentrations of Flupentixol, Haloperidol, Perphenazine and Zuclopenthixol. Br. J. Clin. Pharmacol. 2021, 87, 2228–2235. [Google Scholar] [CrossRef]
- Jukić, M.M.; Smith, R.L.; Molden, E.; Ingelman-Sundberg, M. Evaluation of the CYP2D6 Haplotype Activity Scores Based on Metabolic Ratios of 4,700 Patients Treated with Three Different CYP2D6 Substrates. Clin. Pharmacol. Ther. 2021, 110, 750–758. [Google Scholar] [CrossRef]
- Miroshnichenko, I.I.; Pozhidaev, I.V.; Ivanova, S.A.; Baymeeva, N.V. Therapeutic Drug Monitoring of Olanzapine and Cytochrome P450 Genotyping in Nonsmoking Subjects. Ther. Drug Monit. 2020, 42, 325–329. [Google Scholar] [CrossRef]
- Ji, Y.; Skierka, J.M.; Blommel, J.H.; Moore, B.E.; VanCuyk, D.L.; Bruflat, J.K.; Peterson, L.M.; Veldhuizen, T.L.; Fadra, N.; Peterson, S.E.; et al. Preemptive pharmacogenomic testing for precision medicine: A comprehensive analysis of five actionable pharmacogenomic genes using next-generation DNA sequencing and a customized CYP2D6 genotyping cascade. J. Mol. Diagn. 2016, 18, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Kneller, L.A.; Zubiaur, P.; Koller, D.; Abad-Santos, F.; Hempel, G. Influence of CYP2D6 Phenotypes on the Pharmacokinetics of Aripiprazole and Dehydro-Aripiprazole Using a Physiologically Based Pharmacokinetic Approach. Clin. Pharmacokinet. 2021, 60, 1569–1582. [Google Scholar] [CrossRef]
- Smith, R.L.; O’Connell, K.; Athanasiu, L.; Djurovic, S.; Kringen, M.K.; Andreassen, O.A.; Molden, E. Correction: Identification of a Novel Polymorphism Associated with Reduced Clozapine Concentration in Schizophrenia Patients-a Genome-Wide Association Study Adjusting for Smoking Habits. Transl. Psychiatry 2020, 10, 366. [Google Scholar] [CrossRef]
- Sangüesa, E.; Cirujeda, C.; Concha, J.; Padilla, P.P.; Ribate, M.P.; García, C.B. Implementation of Pharmacogenetics in a Clozapine Treatment Resistant Patient: A Case Report. Pharmacogenomics 2019, 20, 871–877. [Google Scholar] [CrossRef]
- Hicks, J.K.; Sangkuhl, K.; Swen, J.J.; Ellingrod, V.L.; Müller, D.J.; Shimoda, K.; Bishop, J.R.; Kharasch, E.D.; Skaar, T.C.; Gaedigk, A.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2D6 and CYP2C19 Genotypes and Dosing of Tricyclic Antidepressants: 2016 Update. Clin. Pharmacol. Ther. 2017, 102, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Mifsud Buhagiar, L.; Casha, M.; Grech, A.; Serracino Inglott, A.; LaFerla, G. The interplay between pharmacogenetics, concomitant drugs and blood levels of amitriptyline and its main metabolites. Pers. Med. 2021, 19, 113–123. [Google Scholar] [CrossRef]
- Kringen, M.K.; Bråten, L.S.; Haslemo, T.; Molden, E. The Influence of Combined CYP2D6 and CYP2C19 Genotypes on Venlafaxine and O-Desmethylvenlafaxine Concentrations in a Large Patient Cohort. J. Clin. Psychopharmacol. 2020, 40, 137–144. [Google Scholar] [CrossRef]
- Haslemo, T.; Eliasson, E.; Jukić, M.M.; Ingelman-Sundberg, M.; Molden, E. Significantly Lower CYP2D6 Metabolism Measured as the O/N-Desmethylvenlafaxine Metabolic Ratio in Carriers of CYP2D6*41 versus CYP2D6*9 or CYP2D6*10: A Study on Therapeutic Drug Monitoring Data from 1003 Genotyped Scandinavian Patients. Br. J. Clin. Pharmacol. 2019, 85, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Scherf-Clavel, M.; Weber, H.; Wurst, C.; Stonawski, S.; Hommers, L.; Unterecker, S.; Wolf, C.; Domschke, K.; Rost, N.; Brückl, T.; et al. Effects of Pharmacokinetic Gene Variation on Therapeutic Drug Levels and Antidepressant Treatment Response. Pharmacopsychiatry 2022, 55, 246–254. [Google Scholar] [CrossRef]
- Zastrozhin, M.S.; Skryabin, V.; Rwere, F.; Petukhov, A.E.; Pankratenko, E.P.; Pozdniakov, S.A.; Ivanchenko, V.A.; Noskov, V.V.; Zaytsev, I.A.; Vinokurova, N.V.; et al. Influence of CYP2C19*17 Genetic Polymorphism on the Steady-State Concentration of Escitalopram in Patients with Recurrent Depressive Disorder. Psychopharmacol. Bull. 2022, 52, 8–19. [Google Scholar]
- Gaebler, A.J.; Schneider, K.L.; Stingl, J.C.; Paulzen, M. Subtherapeutic Bupropion and Hydroxybupropion Serum Concentrations in a Patient with CYP2C19*1/*17 Genotype Suggesting a Rapid Metabolizer Status. Pharm. J. 2020, 20, 840–844. [Google Scholar] [CrossRef]
- Suzuki, T.; Mihara, K.; Nagai, G.; Kagawa, S.; Nakamura, A.; Nemoto, K.; Kondo, T. Relationship Between UGT1A4 and UGT2B7 Polymorphisms and the Steady-State Plasma Concentrations of Lamotrigine in Patients With Treatment-Resistant Depressive Disorder Receiving Lamotrigine as Augmentation Therapy. Ther. Drug Monit. 2019, 41, 86–90. [Google Scholar] [CrossRef]
- Zastrozhin, M.S.; Skryabin, V.Y.; Smirnov, V.V.; Petukhov, A.E.; Pankratenko, E.P.; Zastrozhina, A.K.; Grishina, E.A.; Ryzhikova, K.A.; Bure, I.V.; Golovinskii, P.A.; et al. Effects of Plasma Concentration of Micro-RNA Mir-27b and CYP3A4*22 on Equilibrium Concentration of Alprazolam in Patients with Anxiety Disorders Comorbid with Alcohol Use Disorder. Gene 2020, 739, 144513. [Google Scholar] [CrossRef]
- Zijp, T.R.; Izzah, Z.; Åberg, C.; Gan, C.T.; Bakker, S.J.L.; Touw, D.J.; van Boven, J.F.M. Clinical Value of Emerging Bioanalytical Methods for Drug Measurements: A Scoping Review of Their Applicability for Medication Adherence and Therapeutic Drug Monitoring. Drugs 2021, 81, 1983–2002. [Google Scholar] [CrossRef]
- Martial, L.C.; Aarnoutse, R.E.; Mulder, M.; Schellekens, A.; Brüggemann, R.J.M.; Burger, D.M.; Schene, A.H.; Batalla, A. Dried Blood Spot Sampling in Psychiatry: Perspectives for Improving Therapeutic Drug Monitoring. Eur. Neuropsychopharmacol. 2017, 27, 205–216. [Google Scholar] [CrossRef]
- Geers, L.M.; Cohen, D.; Wehkamp, L.M.; van Hateren, K.; Koster, R.A.; Fedorenko, O.Y.; Semke, A.V.; Bokhan, N.; Ivanova, S.A.; Kosterink, J.G.W.; et al. Dried Blood Spot Analysis for Therapeutic Drug Monitoring of Clozapine. J. Clin. Psychiatry 2017, 78, e1211–e1218. [Google Scholar] [CrossRef]
- Marasca, C.; Protti, M.; Mandrioli, R.; Atti, A.R.; Armirotti, A.; Cavalli, A.; De Ronchi, D.; Mercolini, L. Whole Blood and Oral Fluid Microsampling for the Monitoring of Patients under Treatment with Antidepressant Drugs. J. Pharm. Biomed. Anal. 2020, 188, 113384. [Google Scholar] [CrossRef]
- Protti, M.; Marasca, C.; Cirrincione, M.; Cavalli, A.; Mandrioli, R.; Mercolini, L. Assessment of Capillary Volumetric Blood Microsampling for the Analysis of Central Nervous System Drugs and Metabolites. Analyst 2020, 145, 5744–5753. [Google Scholar] [CrossRef]
- Kloosterboer, S.M.; de Winter, B.C.M.; Bahmany, S.; Al-Hassany, L.; Dekker, A.; Dieleman, G.C.; van Gelder, T.; Dierckx, B.; Koch, B.C.P. Dried Blood Spot Analysis for Therapeutic Drug Monitoring of Antipsychotics: Drawbacks of Its Clinical Application. Ther. Drug Monit. 2018, 40, 344–350. [Google Scholar] [CrossRef]
- Londhe, V.; Rajadhyaksha, M. Opportunities and Obstacles for Microsampling Techniques in Bioanalysis: Special Focus on DBS and VAMS. J. Pharm. Biomed. Anal. 2020, 182, 113102. [Google Scholar] [CrossRef]
- Marasca, C.; Mandrioli, R.; Sardella, R.; Vovk, T.; Armirotti, A.; Cavalli, A.; Serretti, A.; Protti, M.; Mercolini, L. Dried volumetric microsampling approaches for the therapeutic drug monitoring of psychiatric patients undergoing clozapine treatment. Front. Psychiatry 2022, 13, 794609. [Google Scholar] [CrossRef]
- Stern, M.; Giebels, M.; Fey, T.; Lübking, M.; Alferink, J.; Hempel, G. Validation and Clinical Application of a Volumetric Absorptive Microsampling Method for 14 Psychiatric Drugs. Bioanalysis 2020, 12, 1129–1147. [Google Scholar] [CrossRef]
- Vincze, I.; Rudge, J.; Vásárhelyi, B.; Karvaly, G.B. Analysis of 14 Drugs in Dried Blood Mi-crosamples in a Single Workflow Using Whole Blood and Serum Calibrators. Bioanalysis 2020, 12, 1243–1261. [Google Scholar] [CrossRef]
- Dziurkowska, E.; Wesołowski, M. Effects of Age, Drug Dose, and Sampling Time on Salivary Levels of Olanzapine, Quetiapine, and Their Metabolites. J. Clin. Med. 2020, 9, 3288. [Google Scholar] [CrossRef]
- Parkin, G.M.; McCarthy, M.J.; Thein, S.H.; Piccerillo, H.L.; Warikoo, N.; Granger, D.A.; Thomas, E.A. Saliva Testing as a Means to Monitor Therapeutic Lithium Levels in Patients with Psychiatric Disorders: Identification of Clinical and Environmental Covariates, and Their Incorporation into a Prediction Model. Bipolar Disord. 2021, 23, 679–688. [Google Scholar] [CrossRef]
- Ebert, K.; Maurice, E.; Lukačin, R.; Fleischhaker, C.; Schulz, E.; Ebert, D.; Clement, H.-W. Serum and Saliva Concentrations of Venlafaxine, O-Desmethylvenlafaxine, Quetiapine, and Citalopram in Psychiatric Patients. Ther. Drug Monit. 2018, 40, 351–355. [Google Scholar] [CrossRef]
- Wohkittel, C.; Högger, P.; Fekete, S.; Romanos, M.; Gerlach, M. Relationship between Amphetamine Concentrations in Saliva and Serum in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Ther. Drug Monit. 2021, 43, 564–569. [Google Scholar] [CrossRef]
- Neumann, J.; Beck, O.; Dahmen, N.; Böttcher, M. Potential of Oral Fluid as a Clinical Specimen for Compliance Monitoring of Psychopharmacotherapy. Ther. Drug Monit. 2018, 40, 245–251. [Google Scholar] [CrossRef]
- Criscuolo, F.; Cantu, F.; Taurino, I.; Carrara, S.; De Micheli, G. A Wearable Electrochemical Sensing System for Non-Invasive Monitoring of Lithium Drug in Bipolar Disorder. IEEE Sens. J. 2021, 21, 9649–9656. [Google Scholar] [CrossRef]
- Sweilam, M.N.; Cordery, S.F.; Totti, S.; Velliou, E.G.; Campagnolo, P.; Varcoe, J.R.; Delgado-Charro, M.B.; Crean, C. Textile-Based Non-Invasive Lithium Drug Monitoring: A Proof-of-Concept Study for Wearable Sensing. Biosens. Bioelectron. 2020, 150, 111897. [Google Scholar] [CrossRef]
- Mobed, A.; Ahmadalipour, A.; Fakhari, A.; Kazem, S.S.; Saadi, G.K. Bioassay: A Novel Approach in Antipsychotic Pharmacology. Clin. Chim. Acta 2020, 509, 30–35. [Google Scholar] [CrossRef]
- Roda, A.; Zangheri, M.; Calabria, D.; Mirasoli, M.; Caliceti, C.; Quintavalla, A.; Lombardo, M.; Trombini, C.; Simoni, P. A Simple Smartphone-Based Thermochemiluminescent Immunosensor for Valproic Acid Detection Using 1,2-Dioxetane Analogue-Doped Nanoparticles as a Label. Sens. Actuators B Chem. 2019, 279, 327–333. [Google Scholar] [CrossRef]
- Mazzilli, R.; Curto, M.; De Bernardini, D.; Olana, S.; Capi, M.; Salerno, G.; Cipolla, F.; Zamponi, V.; Santi, D.; Mazzilli, F.; et al. Psychotropic Drugs Levels in Seminal Fluid: A New Therapeutic Drug Monitoring Analysis? Front. Endocrinol. 2021, 12, 620936. [Google Scholar] [CrossRef]
- Enders, J.R.; Reddy, S.G.; Strickland, E.C.; McIntire, G.L. Identification of Metabolites of Brexpiprazole in Human Urine for Use in Monitoring Patient Compliance. Clin. Mass. Spectrom. 2017, 6, 21–24. [Google Scholar] [CrossRef]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; Sanislow, C.; Wang, P. Research Domain Criteria (RDoC): Toward a New Classification Framework for Research on Mental Disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar] [CrossRef] [Green Version]
- Tandon, R.; Nasrallah, H.A.; Keshavan, M.S. Schizophrenia, “Just the Facts” 4. Clinical Features and Conceptualization. Schizophr Res. 2009, 110, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Kupka, R.; Duffy, A.; Scott, J.; Almeida, J.; Balanzá-Martínez, V.; Birmaher, B.; Bond, D.J.; Brietzke, E.; Chendo, I.; Frey, B.N.; et al. Consensus on Nomenclature for Clinical Staging Models in Bipolar Disorder: A Narrative Review from the International Society for Bipolar Disorders (ISBD) Staging Task Force. Bipolar Disord. 2021, 23, 659–678. [Google Scholar] [CrossRef]
- Horwitz, T.; Lam, K.; Chen, Y.; Xia, Y.; Liu, C. A Decade in Psychiatric GWAS Research. Mol. Psychiatry 2019, 24, 378–389. [Google Scholar] [CrossRef]
- Witt, S.H.; Streit, F.; Jungkunz, M.; Frank, J.; Awasthi, S.; Reinbold, C.S.; Treutlein, J.; Degenhardt, F.; Forstner, A.J.; Heilmann-Heimbach, S.; et al. Genome-Wide Association Study of Borderline Personality Disorder Reveals Genetic Overlap with Bipolar Disorder, Major Depression and Schizophrenia. Transl. Psychiatry 2017, 7, e1155. [Google Scholar] [CrossRef] [Green Version]
- Etkin, A. A Reckoning and Research Agenda for Neuroimaging in Psychiatry. Am. J. Psychiatry 2019, 176, 507–511. [Google Scholar] [CrossRef]
- McLoughlin, G.; Makeig, S.; Tsuang, M.T. In Search of Biomarkers in Psychiatry: EEG-Based Measures of Brain Function. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2014, 165B, 111–121. [Google Scholar] [CrossRef]
- Kam, H.; Jeong, H. Pharmacogenomic Biomarkers and Their Applications in Psychiatry. Genes 2020, 11, 1445. [Google Scholar] [CrossRef]
- Stern, S.; Linker, S.; Vadodaria, K.C.; Marchetto, M.C.; Gage, F.H. Prediction of Response to Drug Therapy in Psychiatric Disorders. Open Biol. 2018, 8, 180031. [Google Scholar] [CrossRef] [PubMed]
- Ziani, P.R.; Feiten, J.G.; Goularte, J.F.; Colombo, R.; Antqueviezc, B.; Géa, L.P.; Rosa, A.R. Potential Candidates for Biomarkers in Bipolar Disorder: A Proteomic Approach through Systems Biology. Clin. Psychopharmacol. Neurosci. 2022, 20, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.M.; Reilly, J.L.; Harris, M.S.H.; Patel, S.R.; Weiden, P.J.; Prasad, K.M.; Badner, J.A.; Nimgaonkar, V.L.; Keshavan, M.S.; Sweeney, J.A.; et al. Antipsychotic Pharmacogenomics in First Episode Psychosis: A Role for Glutamate Genes. Transl. Psychiatry 2016, 6, e739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lydiard, J.; Nemeroff, C.B. Biomarker-Guided Tailored Therapy. Front. Psychiatry 2019, 1192, 199–224. [Google Scholar] [CrossRef]


{kind=link}
| Obligatory TDM |
|---|
| Dose optimization after initial prescription or after dose change for drugs with a high level of recommendation to use TDM |
| Drugs for which TDM is mandatory for safety reasons (e.g., lithium or carbamazepine) |
| Specific indications for TDM |
| Uncertain adherence to medication |
| Relapse prevention because of uncertain adherence to medication |
| Lack of clinical improvement under recommended doses |
| Relapse under maintenance treatment |
| Determination of optimal individual drug concentration when the patient has attained the desired clinical outcome |
| Recurrence of symptoms under adequate doses |
| Clinical improvement and adverse effects under recommended doses |
| Combination treatment with a drug known for its interaction potential or suspected drug interaction |
| Use of counterfeit medications by the patient |
| Presence of a genetic peculiarity concerning drug metabolism (genetic deficiency, gene multiplication) |
| Patients with differential ethnicity |
| Patients with abnormally high or low body weight |
| Pregnant or breastfeeding patient |
| Children or adolescent patient |
| Elderly patient (>65 y) |
| Patients with intellectual disability |
| Patients with pharmacokinetically relevant comorbidity (hepatic or renal insufficiency, cardiovascular disease) |
| Patients with acute or chronic inflammations or infections |
| Patients with restrictive gastrointestinal resection or bariatric surgery |
| Problems occurring after switching from an original preparation to a generic form (and vice versa) |
| Use of over-the-counter (OTC) drugs by the patient |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| Arnaiz et al., 2021 [18] | Prospective multicentric | Olanzapine | 47 | 26.2 ± 5.1 (mean ± SD) | Patients with FEP; ethnicity: Caucasian, other | Affective and non-affective first psychotic symptoms of at least 1-week duration | Positive association between drug C/D ratio and clinical response |
| Bustillo et al., 2018 [49] | Prospective multicentric | SGA | 64 | 28.7 ± 7.3 (mean ± SD), 18–49 (range) | Patients with FEP; ethnicity: Caucasian, Hispanic | SSD and BD | Drug SC is not associated with early clinical response |
| Cellini et al., 2022 [46] | Prospective | Escitalopram, Duloxetine, Venlafaxine, Mirtazapine | 206 | 58.11 ± 16.85 (mean ± SD) | Patients with current major depressive episode (HAMD-21 ≥ 14) treated with first-line AD ethnicity: Caucasian, other | MDD | Concentration-dependent clinical efficacy of first-line ADs with a bell-shaped quadratic function indicating a progressive increase in AD efficacy up to around the upper normalized limit of the TRR with a decrease in the AD response at higher SC. |
| D’Anna et al., 2022 [39] | Prospective | LAI SGA | 48 | 44.33 ± 12.63 (mean ± SD) | Clinically stable outpatients | SSD | Under-range LAI levels predicted relapse in SSDs |
| Grover et al., 2022 [27] | Cross-sectional | Clozapine | 50 | 35.7, 19–62 (mean, range) | Clozapine responders and non-responders, Asian ethnicity | Treatment-resistant schizophrenia | Association between a higher clozapine/norclozapine ratio and clinical non-response |
| Hyza et al., 2021 [38] | Retrospective | LAI FGA and SGA | 40 | 45 ± 13 (mean± SD) | At least 3-month LAI treatment, ethnicity not stated | Schizophrenia and related disorders | High prevalence of subtherapeutic drug SC |
| Kauffmann et al., 2016 (corrigendum 2020) [22] | Prospective | SGA | 87 | 34.7 ± 79.9 (mean ± SD), 18–58 (range) | In- and outpatients starting SGA monotherapy; ethnicity not stated | SSD | No correlation between clinical response and observed drug SC |
| Kylleso et al., 2021 [25] | Retrospective | Clozapine | 190 | Switchers: 39 ± 2 (mean ± SD); non-switchers: 43 ± 1 (mean ± SD) | Patients switching from clozapine to other AP | Schizophrenia | Association between clozapine discontinuation and low SC |
| Mauri et al., 2020 [43] | Prospective | LAI aripiprazole and LAI paliperidone | 56 | Aripiprazole: 41.92 ± 13.28 (mean ± SD); paliperidone: 40.83 ± 13.32 (mean ± SD) | Patients clinically stabilized with oral treatment¸ ethnicity not stated | BD with manic predominance | Lower paliperidone SC may have positive effect on depressive symptoms |
| McCutcheon et al., 2018 [32] | Retrospective | FGA and SGA | 99 | Patient with SC in therapeutic range: 44.4 (median); patient with low SC: 35.7 (median) | Patients with treatment-resistant schizophrenia; ethnicity: White British, Black | Schizophrenia, schizoaffective disorder, other | Association between resistance to treatment and subtherapeutic drug SC |
| Melkote et al., 2018 [31] | Retrospective analysis of data from prospective RCT | Olanzapine, risperidone | 316 | 40.9 (mean), 43 (median), 18–67(range) | Patient included in CATIE study undergoing treatment failure; ethnicity: Caucasian, African American, other | Schizophrenia | Correlation between treatment failure and antipsychotics SC below TRR |
| Nagai et al., 2017 [19] | Prospective | Aripiprazole | 26 | 37.7 ± 12.8 (mean ± SD) | Japanese inpatients, early treatment phase | Schizophrenia | Optimal dose predictable through aripiprazole + dehydroaripiprazole TDM at week 1 |
| Olmos et al., 2019 [29] | Prospective | Clozapine | 98 | 39 (median), 20–67 (range) | Caucasian | Schizophrenia | Bioequivalence of two clozapine brands |
| Oloyede et al., 2020 [30] | Prospective | Clozapine | 28 | 47 ± 11.59 (mean ± SD) | In- and outpatients; ethnicity: Asian, Black, Caucasian | Schizophrenia | Bioequivalence of two clozapine formulations |
| Paulzen et al., 2017 [23] | Retrospective | Risperidone | 590 | Responders: 46.1, 18–82 (mean, range); Non-responders: 40.9, 18–87 (mean, range) | Ethnicity not stated | Not stated | Positive association between risperidone active moiety and clinical response |
| Schoretsanitis et al., 2021 [36] | Retrospective | PP1M | 173 | Responders: 44.0, 32.0–59.0 (median, IQR); non-responders: 47.5, 39.8–58.5 (median, IQR) | Ethnicity not stated | SSD, BD, other | Possible specific patterns of clinical response according to diagnosis and SC |
| Schoretsanitis et al., 2022 [37] | Retrospective | PP1M | 183 | Control: 43.0, 33.0– 62.5 (median, IQR); Overweight: 47.0, 34.2–59.7 (median, IQR); Obese: 49.0, 39.2–57.7 (median, IQR) | Adults, elderly, normal and overweight patients | SSD, BD, other | High interindividual variability of SC, no influence of age, sex, smoking, or body weight on SC |
| Tien et al., 2022 [20] | Prospective | Aripiprazole | 64 | Aripiprazole SC: ≤300 ng/mL: 35.2 ± 14.9; >300 ng/mL: 34.3 ± 11.3 (mean ± SD) | Ethnicity; Asian—Taiwan | Schizophrenia | Higher response in terms of Clinical Global Impressions (CGI) scores with aripiprazole SC > 300 ng/mL (higher than the western population-based TRR). |
| Yada et al., 2021 [24] | Cross-sectional multicentric | Clozapine | 131 | 40.1 ± 12.0 (mean ± SD), 16–72 (range) | Japanese patients | Treatment-resistant schizophrenia | Confirmed validity of AGNP clozapine TRR; doses above 1000 ng/mL are more effective but have higher toxicity risk |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| An et al., 2022 [57] | Cross-sectional | Olanzapine | 352 | 56.6 ± 14.2 (mean ± SD) | Inpatients | Schizophrenia | Negative association between plasma DMO concentrations and glucose, insulin, and triglycerides SC Positive association between plasma olanzapine concentrations and C-reactive protein and homocysteine SC |
| Arnaiz et al., 2021 [18] | Prospective multicentric | Olanzapine | 47 | 26.2 ± 5.1 (mean ± SD) | Patients with FEP; ethnicity: Caucasian (94.2%), other | Affective and non-affective first psychotic symptoms of at least 1-week duration | Positive correlation between drug SC and weight gain |
| Diaz et al., 2017 [53] | Retrospective analysis of data from RCT | Clozapine | 47 | 45 ± 10 (mean ± SD), 28–62 (range) | Patients included in RCT; ethnicity: African Americans, Caucasians | Schizophrenia | Association between weight gain and higher SC |
| Engelmann et al., 2021 [60] | RCT | Venlafaxine | 234 | 39.9 ± 12.2 (mean ± SD) | Non-responders to first-line treatment with escitalopram, ethnicity not stated | MDD | No significant correlation between venlafaxine SC and ADRs |
| Kang et al., 2022 [56] | Prospective | Olanzapine | 117 | Drug-naïve: 27.50 (24.83–30.17) Chronic: 38.82 (36.19–41.45) (Interquartile range) | First episode drug-naïf and patients with a duration of illness > 5 years ethnicity not stated | Schizophrenia | Metabolic dysfunction is more severe and dose-dependent in drug-naive patients but independent in patients with chronic schizophrenia |
| Kitchen et al., 2021 [50] | Retrospective | Clozapine | 874 | - | Patients undergoing routine TDM; ethnicity not stated | Schizophrenia, schizoaffective disorder | Reduction of patients with high-risk clozapine SC through routinary TDM implementation |
| Lu et al., 2018 [58] | Prospective | Olanzapine | 151 | 41.3 ± 12.1 (mean ± SD) | In- and outpatients | Schizophrenia | Negative correlation between DMO C/D ratio and presence of metabolic syndrome. Positive correlation between olanzapine SC/DMO SC ratio and presence of metabolic syndrome. Proposal of a range for olanzapine SC/DMO SC (3–6) to maximize efficacy and reduce metabolic side effects |
| Schoretsanitis et al., 2021 [61] | Retrospective | PP1M | 172 | Patients with ADR: 50.5 (25.0) (median, IQR); patients without ADR: 47.0 (23.2) (median, IQR) | In- and outpatients, ethnicity not stated | Not stated | Paliperidone C/D ratio over 7.7 (ng/mL)/(mg/day) associated with higher ADRs risk |
| Schoretsanitis et al., 2021 [54] | Retrospective | Clozapine | 395 | Patients with hypersalivation: 41.5 (21.0) (median, IQR); patients without hypersalivation: 41.0 (22.0) (median, IQR) | In- and outpatients, ethnicity not stated | Not stated | Correlation between high clozapine SC and C/D ratio and hypersalivation |
| Smith et al., 2017 [52] | Retrospective | Clozapine | 129 | 34, 20–84 (median, range) | Ethnicity not stated | Schizophrenia | Correlation between norclozapine SC and granulocyte count |
| Veselinović et al., 2019 [62] | Retrospective analysis of data from RCT | Aripiprazole, flupentixol, haloperidol, olanzapine, quetiapine, | 69 | 34.8 ± 10.9 (mean ± SD) | Patients included in RCT; ethnicity not stated | Schizophrenia | Association between high SC, high D2 receptors occupancy, and low subjective well-being |
| Yada et al., 2021 [24] | Cross-sectional multicentric | Clozapine | 131 | 40.1 ± 12.0 (mean ± SD), 16–72 (range) | Japanese patients | Treatment-resistant schizophrenia | Confirmed validity of AGNP clozapine TRR; doses above 1000 ng/mL are more effective but have higher toxicity risk |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| Baldelli et al., 2020 [69] | Retrospective | AP, AD | 1197 | Not stated | Italian database; ethnicity not stated | Not stated | 45% of patients with SC below TRR |
| Brasso et al., 2021 [71] | Prospective | AP, mood stabilizers | 133 | Patients with SSD: 43.1 ± 13.5 (mean ± SD); patients with BD: 51.9 ± 14.4 (mean ± SD) | Inpatients in a psychiatric emergency service; ethnicity: Caucasian, other | SSD, BD, and related disorders | 50% of patients with SC out of TRR; no correlation between TDM and self-assessment of adherence |
| Geretsegger et al., 2019 [67] | Prospective | AP, AD | 161 | 40.4 (mean) | Inpatients newly admitted to a psychiatric emergency service; ethnicity not stated | Psychotic disorders, mood disorders, other disorders | 52% of patients with SC below TRR, patients with psychotic disorder are less adherent compared to patients with mood disorders |
| Lopez et al., 2017 [70] | Prospective | Aripiprazole, risperidone, olanzapine, paliperidone, quetiapine | 97 | 39, 18–74 (mean, range) | Patients acceding to a psychiatric emergency service; ethnicity: African American, Asian, White, Hispanic, other | Schizophrenia, schizoaffective disorder, BD, psychotic disorder not otherwise specified | 66% of patients with SC out of TRR; no correlation between TDM and clinician assessment of adherence |
| Silhan et al., 2018 [68] | Prospective | Citalopram, escitalopram, paroxetine, sertraline, venlafaxine | 83 | 40.3 ± 12.2 (mean ± SD) | In- and outpatients; ethnicity not stated | Depressive disorders, anxiety disorders | 37.3% of non-adherent patients in the whole sample; 56.8% of the outpatient subgroup with SC below TRR |
| Smith et al., 2020 [72] | Retrospective | AP | 24,239 | 44 (median), 15–106 (range) | Norwegian database; ethnicity not specified | Not stated | AP polypharmacy is associated with non-adherence |
| Smith et al., 2021 [74] | Retrospective | Aripiprazole, clozapine, olanzapine, quetiapine, risperidone | 13,217 | 44.3 ± 16.0 (mean ± SD) | Norwegian database, outpatients; ethnicity not specified | Schizophrenia, other | Complete non-adherence in less than 5% of patients with psychotic symptoms; higher non-adherence in patients receiving olanzapine compared to other drugs |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| Clark et al., 2022 [80] | Prospective | Lithium | 3 | 22–39 (range) | Women during pregnancy and post-partum; 1 Caucasian, 1 Hispanic, 1 Afro-American | BD, type I | Lithium elimination clearance increase of 63.5% by the third trimester; lithium elimination clearance was inversely related to SC; mood symptoms worsened with declines in SC; lithium elimination clearance returned to baseline at 4 to 9 weeks postpartum |
| Heinonen et al., 2021 [83] | RCT | Sertraline | 9 | 24–39 (range) | Women during pregnancy and post-partum, infants; ethnicity not stated | Depression | High interindividual maternal serum concentration, low infant exposition |
| Leutritz et al., 2022 [77] | Retrospective and Prospective | Amitriptyline, Aripiprazole, Bupropion, Citalopram Clomipramine, Duloxetine, Escitalopram, Lamotrigine, Mirtazapine Paroxetine, Quetiapine, Sertraline, Venlafaxine | 60 | 33.26 ± 2.45 (mean ± SD) | Outpatients during pregnancy and post-partum infants; ethnicity not stated | Major depressive disorder, Anxiety disorders, Obsessive–compulsive disorder, Bipolar disorders, Schizoaffective disorder, Adjustment disorder, Substance use disorders | ↓ SC from the I to the II trimester of amitriptyline, duloxetine, escitalopram, quetiapine, and sertraline; citalopram stayed stable during pregnancy, ↑ sertraline SC from the II to the III trimester; high concentration-by-dose ratios in breastmilk for venlafaxine and lamotrigine, low for quetiapine and clomipramine |
| Schoretsanitis et al., 2019 [82] | Prospective | Citalopram, sertraline, venlafaxine | 17 | 23–40 (range) | Breast-feeding women; ethnicity not stated | Depressive episode | Higher breastfed children exposure to venlafaxine |
| Westin et al., 2017 [79] | Retrospective | Lithium | 13 | 32.9 ± 3.8 (mean ± SD) | Pregnant women, assessment at baseline, during pregnancy, and after delivery; ethnicity not stated | BD | ↓ lithium SC during III trimester |
| Westin et al., 2018 [84] | Retrospective | AP | 103 | 29 (mean) | Pregnant women, assessment at baseline and during pregnancy; ethnicity not stated | Not stated | ↓quetiapine and aripiprazole SC during III trimester |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome | |
|---|---|---|---|---|---|---|---|---|
| Adolescents | Egberts et al., 2020 [97] | Retrospective | Aripiprazole | 130 | 15.0 ± 2.6 (mean ± SD), 7.6–19.0 (range) | 65% of the patients treated with polytherapy; ethnicity not stated | SSD, mood disorders, other | Aripiprazole TRR for adolescents similar to adults; positive correlation between weight and aripiprazole SC |
| Fekete et al., 2021 [95] | Retrospective | Risperidone, venlafaxine | Total sample: 1555; patients < 18: 100 | Patients < 18 treated with risperidone: 14.0; 4.0 (mean; IQR), 7–17 (range); patients < 18 treated with venlafaxine: 16.0; 2.0 (mean; IQR), 12–17 (range) | German database; ethnicity not stated | Not stated | Risperidone and venlafaxine dose-adjusted SC lower in adolescents than adults | |
| Piacentino et al., 2020 [96] | Retrospective | Aripiprazole, risperidone | 140 | 14.2 ± 3.1 (mean ± SD), 5−18 (range) | Ethnicity not stated | Oppositional Defiant/Conduct Disorders | Higher aripiprazole and risperidone dose-adjusted SC in girls; lower risperidone active moiety SC in lower-weight patients | |
| Taurines et al., 2022 [109] | Prospective | Risperidone | 64 | 15.6 ± 1.7 (mean ± SD), 11–18 (range) | Inpatients and outpatients; Ethnicity not stated | SSD | Higher SC associated with a higher risk of EPS. Preliminary indications for a lower TRR in this population | |
| Tini et al., 2022 [91] | Prospective | Sertraline | 78 | 14.2 ± 2.4 (mean ± SD), 7–18 (range) | Ethnicity not stated | Obsessive–compulsive and Major Depressive Disorders | Strong linear positive dose–serum concentration relationship; significant effects of weight and co-medication; no association between dose or SC and side effects; higher doses and SCs are more effective in the treatment of the OCD | |
| Elderly | An et al., 2021 [105] | Retrospective | Olanzapine | 185 | 18–87 (range), 67.6% of the sample aged ≥56 | Chinese population | Schizophrenia | Age-related ↓ N-desmethyl olanzapine SC |
| Castberg et al., 2017 [99] | Retrospective | Clozapine, olanzapine, quetiapine, risperidone | 11,968 | 18–100 (range) | Data from Norwegian database; ethnicity not stated | Not stated | Age-related ↑ dose-adjusted SC of clozapine, olanzapine, quetiapine, risperidone, particularly in women | |
| Deng et al., 2020 [104] | Retrospective | Olanzapine | 884 | 38 ± 16 (mean ± SD), 13–90 (range) | Chinese population | SSD, BD | Age-related ↑ olanzapine SC and dose-adjusted SC | |
| Fekete et al., 2020 [95] | Retrospective | Risperidone, venlafaxine | Total sample: 1555, patients > 60 years: 428 | Patients > 60 treated with risperidone: 73.0; 11.0 (mean; IQR), 61–92 (range); Patients > 60 treated with venlafaxine: 71.0; 13.0 (mean; IQR), 60–93 (range) | German database, ethnicity not stated | Not stated | Age-related ↑ risperidone dose adjusted SC | |
| Hansen et al., 2017 [48] | Retrospective | Venlafaxine | 1177 | 45 (median), 34–59 (IQR range) | Danish database, ethnicity not stated | Not stated | ↑ dose-adjusted venlafaxine SC in patients over 64 | |
| Hefner et al., 2019 [108] | Retrospective | Amitriptyline, venlafaxine | 34 | 69.7 ± 3.5 (mean ± SD), 65–78 (range) (data referred to the whole database from which data on the 34 patients included in the study are taken from) | Ethnicity not stated | Not stated | Correlation between amitriptyline and venlafaxine SC and QT prolongation in the elderly | |
| Huang et al., 2021 [78] | Retrospective | Amisulpride | 121 | 35.83 ± 13.50 (mean ± SD) | Inpatients Chinese population | Schizophrenia | Age-related ↑ dose-adjusted SC of amisulpride; proposal of 600 mg/day as the maximum dosage of amisulpride in patients over 60 | |
| Jönsson et al., 2019 [100] | Retrospective | Amisulpride, aripiprazole, clozapine, flupenthixol, haloperidol, olanzapine, perphenazine, quetiapine, risperidone, sertindole, zuclopenthixol, ziprasidone | Different n° of patients for each drug, ranging from 11,272 (olanzapine) to 225 (sertindole) | Different ages for each drug ranging from 31 (median, sertindole) to 50 (median, haloperidol) | Data from Norwegian database; ethnicity not stated | Not stated | Age-related ↑ dose-adjusted SC of amisulpride, aripiprazole, clozapine, haloperidol, olanzapine, perphenazine, quetiapine, risperidone, sertindole, zuclopenthixol, particularly in women | |
| Reeves et al., 2018 [101] | Prospective | Amisulpride | 8 | 76 ± 6 (mean ± SD) | Outpatients; Caucasian, African, Asian | Very late-onset schizophrenia-like psychosis | D2 receptor occupancy over 40% and good clinical efficacy with an amisulpride dose of 50 mg/day | |
| Smith et al., 2018 [107] | Retrospective | Lamotrigine | 534 | 40 (median), 18–95 (range) | Norwegian database, ethnicity not stated | Not stated | Age-related ↑ lamotrigine dose-adjusted SC, particularly in women carrying the UGT1A4*3 allele | |
| Tveit et al., 2020 [45] | retrospective | Citalopram, escitalopram, mirtazapine, sertraline, venlafaxine | 806 (2007 cohort); 1932 (2017 cohort) | 2007 cohort, age < 65: 41, 19 (median, IQR); age ≥ 65: 76, 13 (median, IQR); 2017 cohort, age < 65: 41, 22 (median, IQR); age ≥ 65: 79, 15 (median, IQR) | Norwegian database, ethnicity not stated | Not stated | Age-related ↑ citalopram, escitalopram, mirtazapine, sertraline, venlafaxine SC, especially in women. Relevant percentage of the sample exposed to concentrations above TRR | |
| Tveito et al. 2021 [106] | Retrospective | Paliperidone LAI | 1223 | PP1M: 41.1 (mean) PP3M: 44.3 years (mean) | Norwegian database, one-third of the sample aged > 50; ethnicity not stated | Not stated | Age-related ↑ paliperidone dose-adjusted SC for paliperidone LAI users, especially in women | |
| Tveito et al., 2018 [103] | Retrospective | Olanzapine oral and LAI | 8288 | 45, 18–102 (median, range) | Data from Norwegian database; ethnicity not stated | Not stated | Age-related ↑ olanzapine dose adjusted SC for oral formulation but not LAI users | |
| Tveito et al., 2021 [102] | Retrospective | Zuclopenthixol oral and LAI | 2044 | Oral subgroup: 52.3 ± 17.5 (mean ± SD); LAI subgroup: 47.3 ± 15.4 (mean ± SD) | Data from Norwegian database; ethnicity not stated | Not stated | Age-related ↑ dose-adjusted SC of zuclopenthixol for both oral and LAI formulation; LAI users over 65 and with low CYP2D6 function at risk of high SC exposure |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| An et al., 2021 [105] | Retrospective | Olanzapine | 185 | 18–87 (range) | Chinese population | Schizophrenia | High body weight associated with ↓ olanzapine and n-desmethylolanzapine SC |
| Diaz et al., 2017 [53] | Retrospective analysis of data from RCT | Clozapine | 47 | 45 ± 10 (mean ± SD), 28–62 (range) | Patients included in RCT; ethnicity: African Americans, Caucasians | Schizophrenia | Association between weight gain and ↑ SC |
| Kuzin et al., 2021 [110] | Retrospective | Clozapine | 455 | 19–88 (range) | German database, in- and outpatients, ethnicity not stated | Not stated | High BMI associated with ↑ clozapine SC and C/D ratio |
| Methaneethorn et al., 2017 [111] | Retrospective | Valproic acid | 206 | 39.3 ± 13.1 (mean ± SD) | Asian ethnicity | BD, manic episode | Reduced clearance in overweight patients |
| Schoretsanitis et al., 2018 [112] | Retrospective | Venlafaxine | 737 | 45.4 ± 14.6 (mean ± SD) | German database, in- and outpatients, ethnicity not stated | SSD, mood disorders, other | Negative correlation between BMI and venlafaxine active moiety SC, O-desmethylvenlafaxine SC, and venlafaxine C/D ratio |
| Warrings et al., 2021 [113] | Retrospective | Amitriptyline, clozapine, doxepin, escitalopram, mirtazapine, quetiapine, risperidone, venlafaxine | 1657 (whole sample) | 18–92 (range) | In- and outpatients, ethnicity not stated | Not stated | Negative correlation between BMI and venlafaxine active moiety SC, O-desmethylvenlafaxine SC |
| Study | Study Design | Drugs | n | Age | Sample Characteristics | Diagnosis | Outcome |
|---|---|---|---|---|---|---|---|
| Courlet et al., 2019 [119] | Retrospective | Escitalopram | 110 | 48, 36–56 (median, IQR) | Patients living with HIV, control group of patients not affected by HIV | Not stated | Escitalopram SC below TRR in 56% of HIV + patients; no significant DDI with antiretroviral drug identified |
| Scherf-Clavel et al., 2020 [117] | Retrospective | Aripiprazole, olanzapine, quetiapine, risperidone | Aripiprazole: 30, olanzapine: 24, quetiapine: 166, risperidone: 45 | 18–85 (range) | In- and outpatients with CRP concentration ≥ 0.5 mg/dL | Not stated | Positive correlation between elevated CRP and quetiapine C/D |
| Zhang et al., 2021 [116] | Retrospective | Aripiprazole, clozapine, quetiapine, risperidone | Aripiprazole: 13, clozapine: 42, quetiapine: 21, risperidone: 36 | 16–76 (range) | Inpatients with respiratory tract infections | Not stated | Higher C/D ratios during infection for all drugs considered |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pennazio, F.; Brasso, C.; Villari, V.; Rocca, P. Current Status of Therapeutic Drug Monitoring in Mental Health Treatment: A Review. Pharmaceutics 2022, 14, 2674. https://doi.org/10.3390/pharmaceutics14122674
Pennazio F, Brasso C, Villari V, Rocca P. Current Status of Therapeutic Drug Monitoring in Mental Health Treatment: A Review. Pharmaceutics. 2022; 14(12):2674. https://doi.org/10.3390/pharmaceutics14122674
Chicago/Turabian StylePennazio, Filippo, Claudio Brasso, Vincenzo Villari, and Paola Rocca. 2022. "Current Status of Therapeutic Drug Monitoring in Mental Health Treatment: A Review" Pharmaceutics 14, no. 12: 2674. https://doi.org/10.3390/pharmaceutics14122674