
Biologic Functions of Hydroxychloroquine in Disease: From COVID-19 to Cancer

Abstract
:1. Introduction
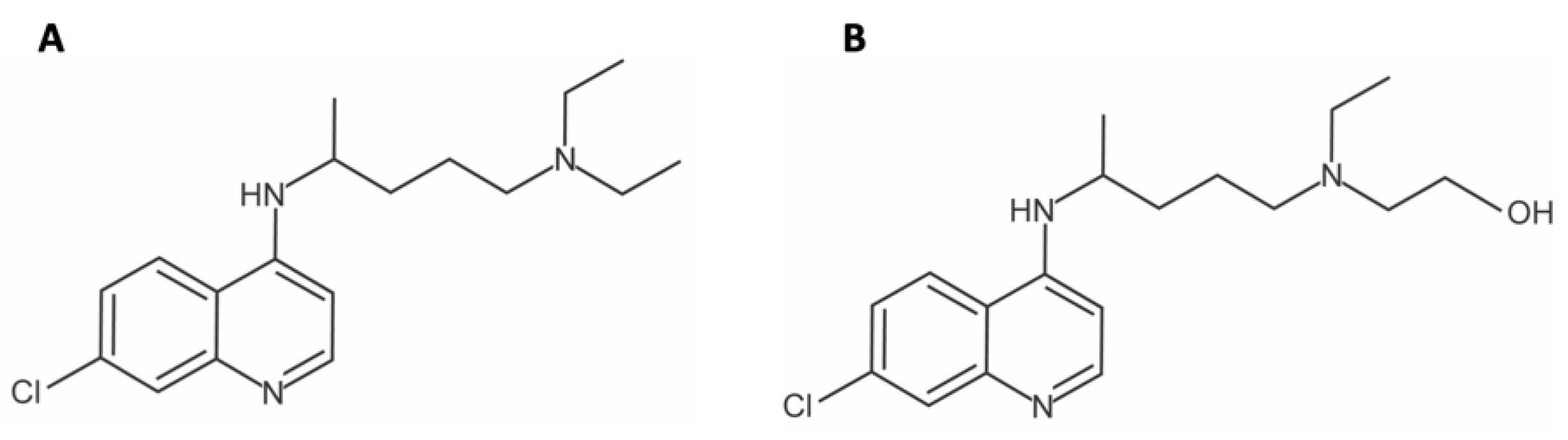
1.1. History of Chloroquine/Hydroxychloroquine
1.2. Repurposing
2. Biochemistry and Pharmacology
2.1. Side Effects
2.2. Contraindications
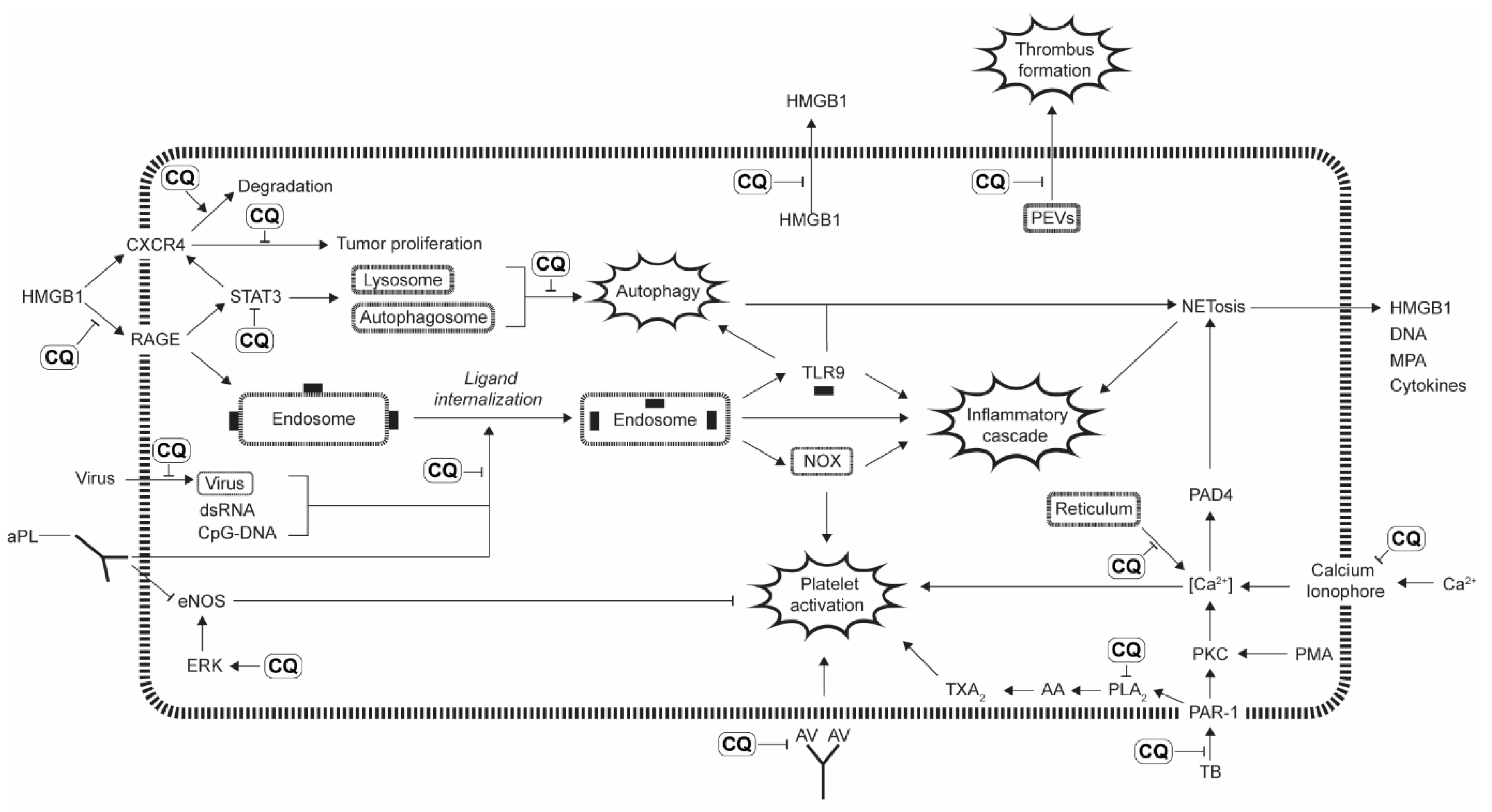
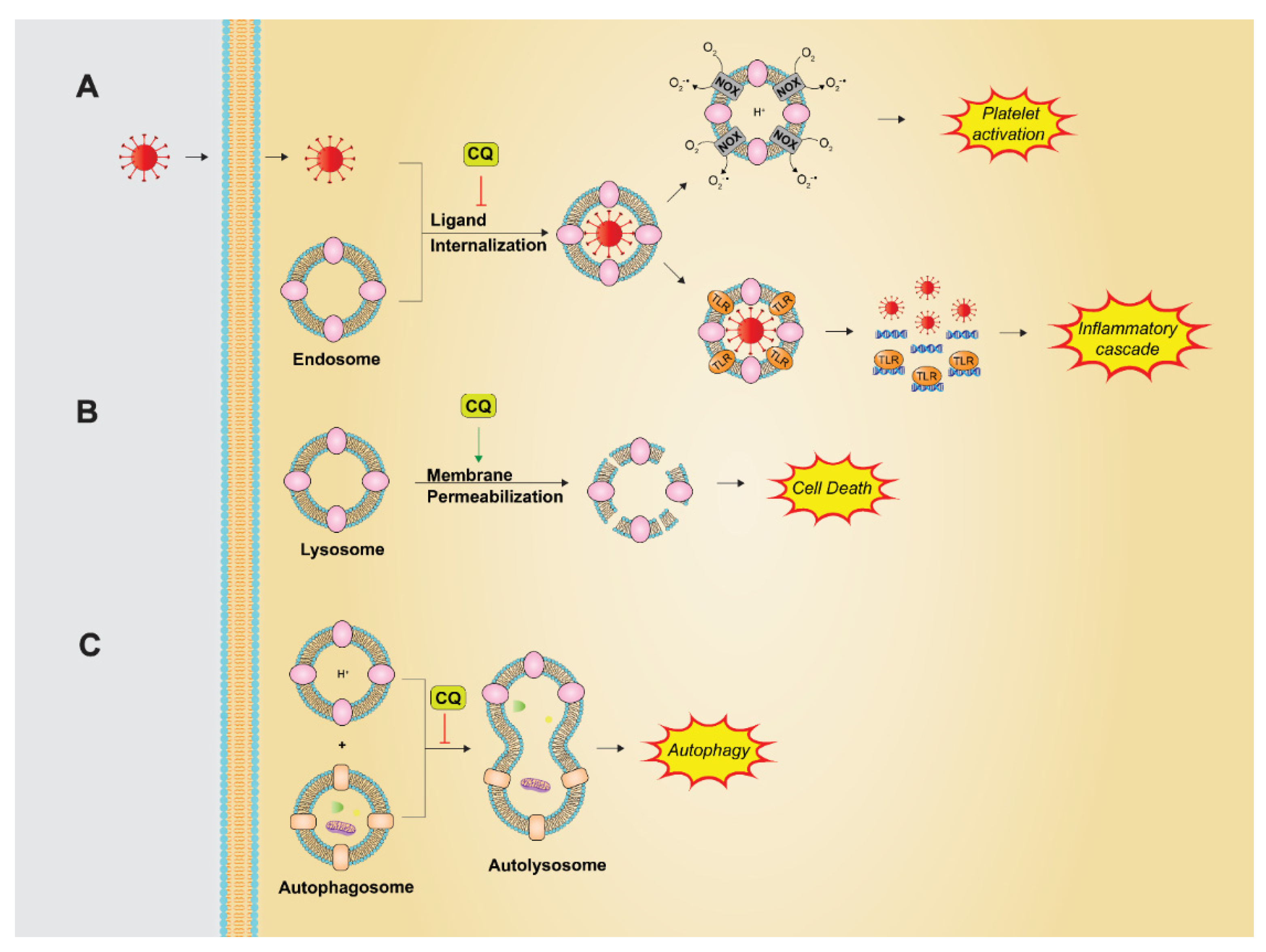
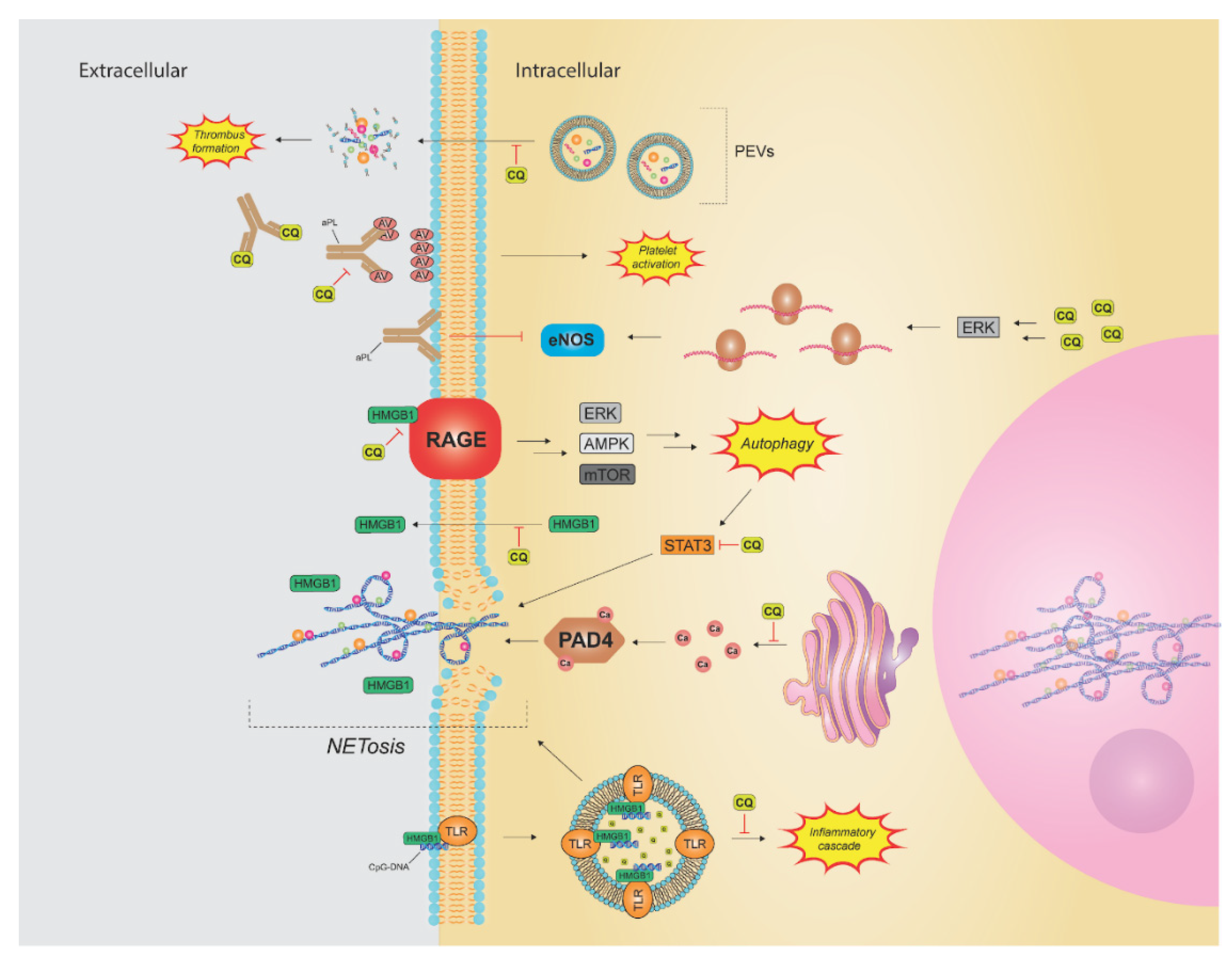
3. Mechanisms of Action
3.1. Alkalinization of Lysosomes and Endosomes
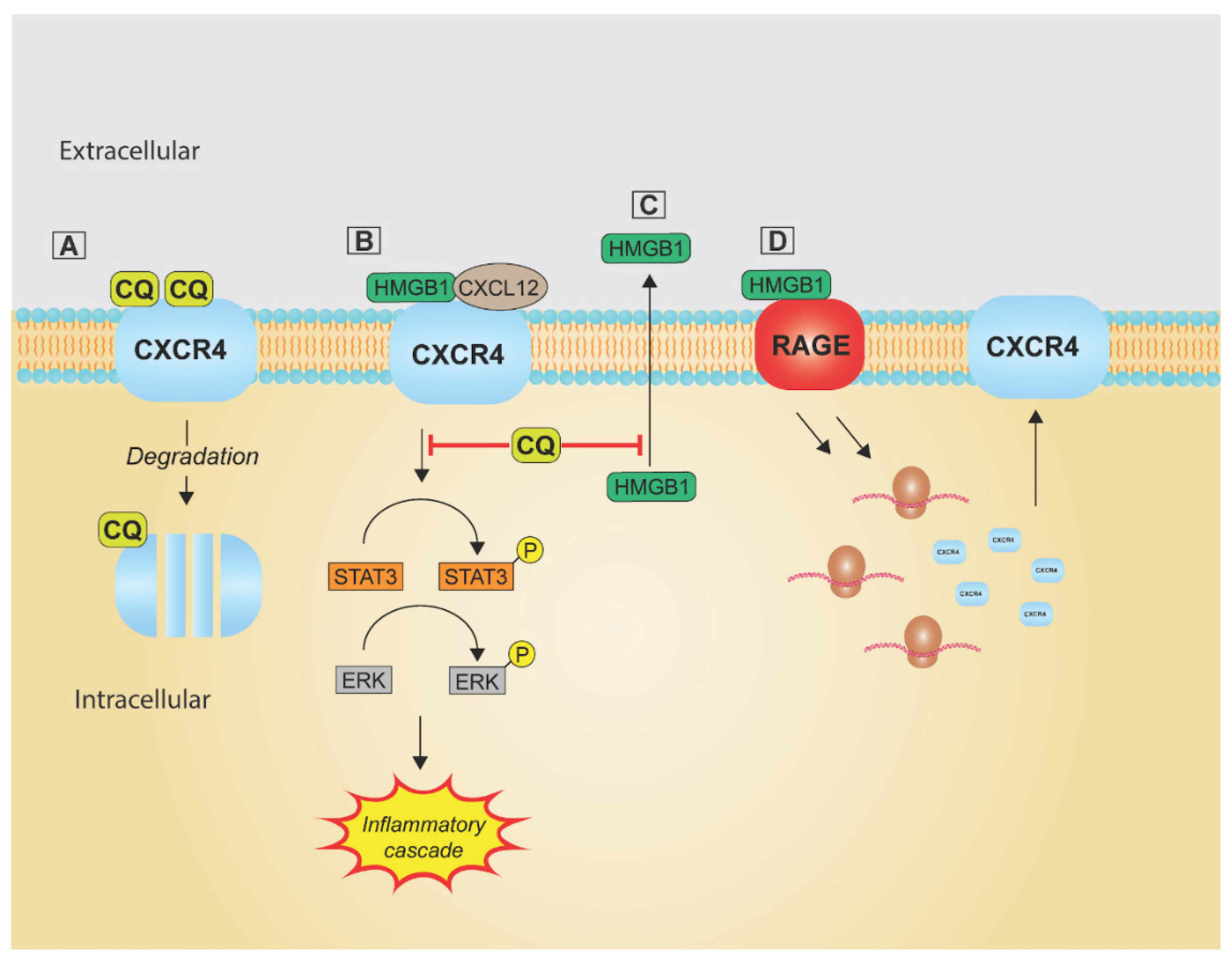
3.2. C-X-C Chemokine Receptor Type 4
3.3. High-Mobility Group Box 1 Protein
3.4. Alteration of Intracellular Calcium
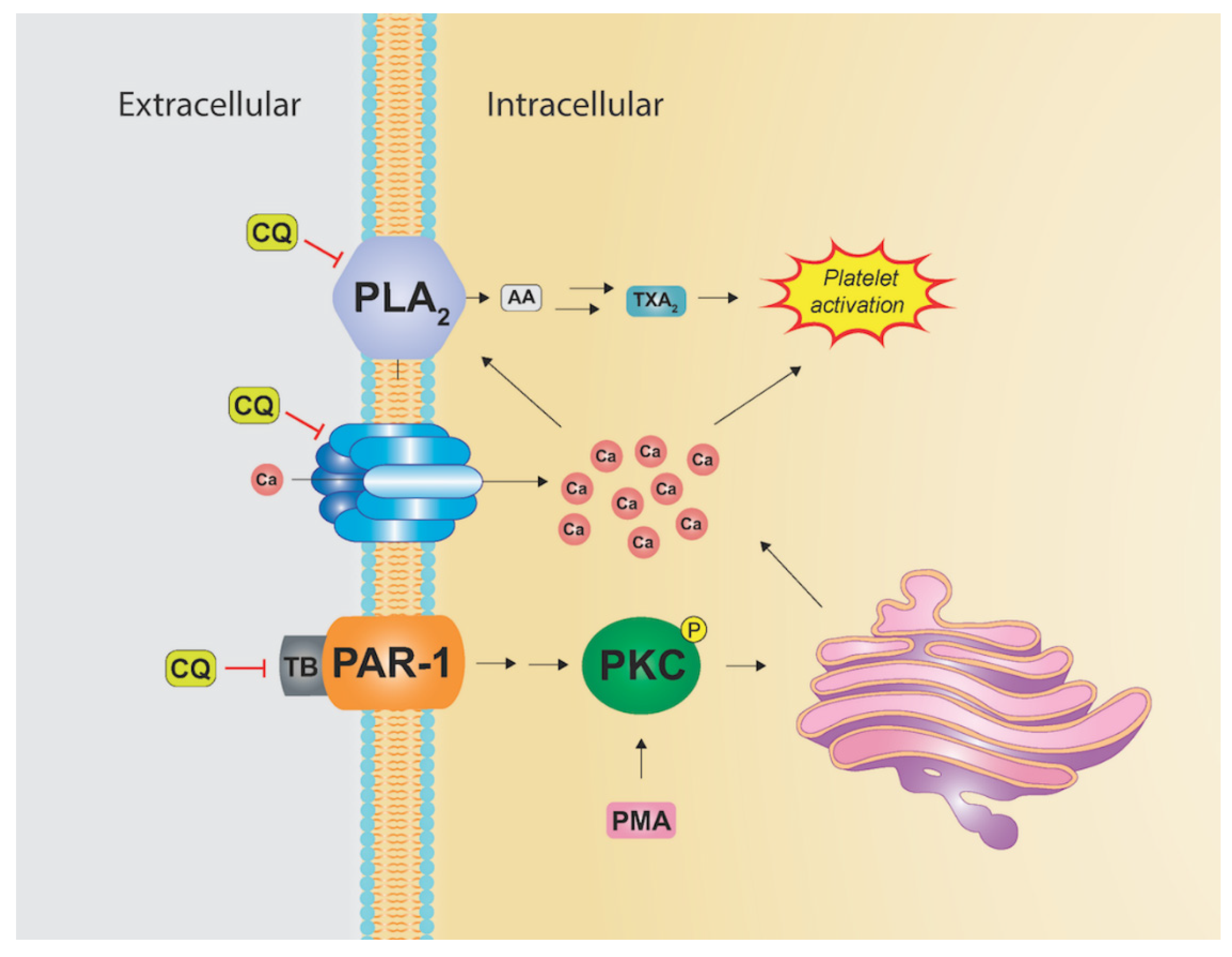
3.5. Prevention of Thrombosis
4. Clinical Trials
4.1. Autoimmune Disorders
4.1.1. Systemic Lupus Erythematosus
4.1.2. Rheumatoid Arthritis
4.1.3. Antiphospholipid Syndrome
4.2. Thrombus/DVT Prophylaxis
4.3. Cardiovascular Disease
4.4. Diabetes Mellitus
4.5. Cancer
4.5.1. Glioblastoma Multiforme
4.5.2. Pancreatic Ductal Adenocarcinoma
4.5.3. Other Malignancies
4.6. Viruses
4.6.1. COVID-19
4.6.2. HIV
4.6.3. Flaviviruses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) [Ref] | Design | Intervention | Outcome |
|---|---|---|---|
| Systemic Lupus Erythematous (SLE) | |||
| Fessler et al. (2005) [153] | Observational | HCQ | Lower disease activity and improved survival in patients receiving HCQ |
| Vilela et al. (2001) [238] | Phase II RCT | Prednisone and either HCQ or placebo | Lower disease activity and reduction in prednisone dose in HCQ group. No adverse side effects in infants of mothers receiving HCQ |
| Canadian Hydroxychloroquine Study Group. (1991) [156] | Phase 3 RCT | Clinically stable SLE patients receiving HCQ for at least 6 months randomized to continue HCQ treatment or placebo | 2.5 × higher relative risk of clincal flare-up in placebo group |
| Ruiz-Irastorza et al. (2006) [162] | Observational prospective cohort study | CQ or HCQ treatment versus non-antimalarial treatment | Decreased thrombosis incidence and increased survival rate |
| An et al. (2019) [161] | Phase III RCT | Immunosuppressive treatment alone or in combination with HCQ for lupus nephritis | Higher rate of complete remission in combination group |
| Rheumatoid Arthritis | |||
| Das et al. (2007) [169] | Phase III RCT | Nimesulide 100 mg BID plus either 200 mg HCQ daily or placebo for 8 weeks | Symptomatic improvement with HCQ based on ACR 20 criteria |
| Gubar et al. (2008) [171] | Prospective randomized study | MTX (17.5 mg/week) alone versus in combination with SSZ (2.0 g/day) and HCQ (200 mg/day) for 1.5 years | Triple combination therapy with MTX, SSZ, and HCQ had improved symptomatic response (ACR > 50%) |
| O’Dell et al. (2013) [174] | Phase III RCT | Patients with active disease despite MTX randomized to either triple therapy (MTX, SSZ, HCQ) or Etanercept plus MTX | Significant improvement in disease activity score in both groups. Triple therapy was noninferior to Etanercept plus MTX |
| Antiphospholipid Syndrome | |||
| Kravvariti et al. (2020) [176] | Phase III RCT | HCQ plus standard anticoagulation and/or antiplatelet therapy versus standard care alone | Lower incidence of thrombosis with HCQ plus standard care than with standard care alone |
| Schmidt-Tanguy et al. (2013) [177] | Prospective non-randomized study | HCQ versus standard oral anticoagulants | No difference in thrombosis incidence |
| Cardiovascular Disease | |||
| Pareek et al. (2015) [193] | Phase III RCT | Atorvastatin alone versus in addition to HCQ in patients with primary dyslipidemia | Significant reduction in LDL in Atorvastatin/HCQ patients but no change in triglycerides or HDL. |
| Ulander et al. (2021) [196] | Phase II RCT | HCQ versus placebo after myocardial infarction | Lower IL-6 levels with HCQ treatment without higher adverse reactions |
| Cancer | |||
| Rosenfeld (2014) [204] | Phase I/II trial | HCQ with radiation and adjuvant temozolomide in glioblastoma multiforme patients. | Thrombocytopenia and Grade 3 and 4 neutropenia at 800 mg per day HCQ. Maximum tolerated dose was 600 mg per day with radiation and temozolomide. |
| Zeh et al. (2020) [207] | Phase II RCT | Two cycles of nab-paclitaxel and gemcitabine alone or with hydroxychloroquine in patients with potentially resectable pancreatic cancer | Improved histopathologic and CA 19-9 responses with addition of HCQ. No difference in severe adverse reactions. |
| Karasic et al. (2019) [208] | Phase II RCT | Nab-paclitaxel alone or with 600 mg HCQ BID in patients with previously untreated metastatic pancreatic cancer | No difference in overall survival at 12 months |
| Arnaout (2019) [210] | Phae II RCT | HCQ 500 mg daily versus placebo in newly diagnosed breast cancer patients | No change in cellular proliferation. Although all adverse effects were classified as grade 1, 15% of patients receiving HCQ withdrew from the study. |
| Viral | |||
| Cavalcanti et al. (2020) [216] | Phase III RCT | Standard care alone or in combination with HCQ +/− Azithromycin in patients with mild to moderate COVID-19 patients | No improvement in clinical status at 15 days as compared to standard care |
| Abella (2020) [222] | Phase II RCT | HCQ versus placebo as COVID-19 prophylaxis in healthcare workers | No difference in infection rates |
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldman, L.; Cole, D.P.; Preston, R.H. Chloroquine diphosphate in treatment of discoid lupus erythematosus. J. Am. Med. Assoc. 1953, 152, 1428–1429. [Google Scholar] [CrossRef] [PubMed]
- Pillsbury, D.M.; Jacobson, C. Treatment of chronic discoid lupus erythematosus with chloroquine (aralen). J. Am. Med. Assoc. 1954, 154, 1330–1333. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.G.; Magwere, T. Chloroquine: Novel uses & manifestations. Indian J. Med. Res. 2008, 127, 305–316. [Google Scholar] [PubMed]
- Manic, G.; Obrist, F.; Kroemer, G.; Vitale, I.; Galluzzi, L. Chloroquine and hydroxychloroquine for cancer therapy. Mol. Cell. Oncol. 2014, 1, e29911. [Google Scholar] [CrossRef]
- Coatney, G.R. Pitfalls in a Discovery: The Chronicle of Chloroquine. Am. J. Trop. Med. Hyg. 1963, 12, 121–128. [Google Scholar] [CrossRef]
- Most, H. Landmark article July 20, 1946: Chloroquine for treatment of acute attacks of vivax malaria. By Harry Most, Irving M. London, Charles A. Kane, Paul H. Lavietes, Edmund F. Schroeder and Joseph M. Hayman, Jr. JAMA 1984, 251, 2415–2419. [Google Scholar] [CrossRef]
- Sheehy, T.W.; Reba, R.C.; Neff, T.A.; Gaintner, J.R.; Tigertt, W.D. Supplemental sulfone (dapsone) therapy. Use in treatment of chloroquine-resistant falciparum malaria. Arch. Intern. Med. 1967, 119, 561–566. [Google Scholar] [CrossRef]
- Wyler, D.J. Landmark perspective: The ascent and decline of chloroquine. JAMA 1984, 251, 2420–2422. [Google Scholar] [CrossRef]
- Centers for Disease Control (CDC). Chloroquine-resistant Plasmodium falciparum malaria in West Africa. MMWR. Morb. Mortal. Wkly. Rep. 1987, 36, 13–14. [Google Scholar]
- Augustijns, P.; Geusens, P.; Verbeke, N. Chloroquine levels in blood during chronic treatment of patients with rheumatoid arthritis. Eur. J. Clin. Pharmacol. 1992, 42, 429–433. [Google Scholar] [CrossRef]
- Savarino, A.; Gennero, L.; Chen, H.C.; Serrano, D.; Malavasi, F.; Boelaert, J.R.; Sperber, K. Anti-HIV effects of chloroquine: Mechanisms of inhibition and spectrum of activity. AIDS 2001, 15, 2221–2229. [Google Scholar] [CrossRef] [PubMed]
- Heimlich, H.J.; Chen, X.P.; Xiao, B.Q.; Liu, S.G.; Lu, Y.H.; Spletzer, E.G.; Yao, J.L. Malariotherapy for HIV patients. Mech. Ageing Dev. 1997, 93, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.J.; Bergeron, E.; Benjannet, S.; Erickson, B.R.; Rollin, P.E.; Ksiazek, T.G.; Seidah, N.G.; Nichol, S.T. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005, 2, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyall, J.; Coleman, C.M.; Hart, B.J.; Venkataraman, T.; Holbrook, M.R.; Kindrachuk, J.; Johnson, R.F.; Olinger, G.G., Jr.; Jahrling, P.B.; Laidlaw, M.; et al. Repurposing of Clinically Developed Drugs for Treatment of Middle East Respiratory Syndrome Coronavirus Infection. Antimicrob. Agents Chemother. 2014, 58, 4885–4893. [Google Scholar] [CrossRef] [Green Version]
- Dyall, J.; Gross, R.; Kindrachuk, J.; Johnson, R.F.; Olinger, G.G., Jr.; Hensley, L.E.; Frieman, M.B.; Jahrling, P.B. Middle East Respiratory Syndrome and Severe Acute Respiratory Syndrome: Current Therapeutic Options and Potential Targets for Novel Therapies. Drugs 2017, 77, 1935–1966. [Google Scholar] [CrossRef] [Green Version]
- Akpovwa, H. Chloroquine could be used for the treatment of filoviral infections and other viral infections that emerge or emerged from viruses requiring an acidic pH for infectivity. Cell Biochem. Funct. 2016, 34, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Smit, C.; Peeters, M.Y.M.; Anker, J.N.V.D.; Knibbe, C.A.J. Chloroquine for SARS-CoV-2: Implications of Its Unique Pharmacokinetic and Safety Properties. Clin. Pharmacokinet. 2020, 59, 659–669. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Agrawal, S.; Ish, P. Chloroquine in COVID-19: The evidence. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Management Sciences for Health (MSH). International Medical Products Price Guide; Management Sciences for Health: Medford, MA, USA, 2016. [Google Scholar]
- Njaria, P.M.; Okombo, J.; Njuguna, N.M.; Chibale, K. Chloroquine-containing compounds: A patent review (2010–2014). Expert Opin. Ther. Patents 2015, 25, 1003–1024. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, L.L.; Walker, O.; Alvan, G.; Beermann, B.; Estevez, F.; Gleisner, L.; Lindstrom, B.; Sjoqvist, F. Disposition of chloroquine in man after single intravenous and oral doses. Br. J. Clin. Pharmacol. 1983, 15, 471–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frisk-Holmberg, M.; Bergqvist, Y.; Termond, E.; Domeij-Nyberg, B. The single dose kinetics of chloroquine and its major metabolite desethylchloroquine in healthy subjects. Eur. J. Clin. Pharmacol. 1984, 26, 521–530. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, A.C.; Cutler, D.J. The potential role of lysosomes in tissue distribution of weak bases. Biopharm. Drug Dispos. 1988, 9, 513–526. [Google Scholar] [CrossRef] [PubMed]
- Veignie, E.; Moreau, S. The mode of action of chloroquine. Non-weak base properties of 4-aminoquinolines and antimalarial effects on strains ofPlasmodium. Ann. Trop. Med. Parasitol. 1991, 85, 229–237. [Google Scholar] [CrossRef]
- Tett, S.; Cutler, D.; Day, R.; Brown, K. Bioavailability of hydroxychloroquine tablets in healthy volunteers. Br. J. Clin. Pharmacol. 1989, 27, 771–779. [Google Scholar] [CrossRef] [Green Version]
- White, N.J.; Miller, K.D.; Churchill, F.C.; Berry, C.; Brown, J.; Williams, S.B.; Greenwood, B.M. Chloroqine Treatment of Severe Malaria in Children. Pharmacokinetics, toxicity, and new dosage recommendations. N. Engl. J. Med. 1988, 319, 1493–1500. [Google Scholar] [CrossRef]
- Karunajeewa, H.A.; Salman, S.; Mueller, I.; Baiwog, F.; Gomorrai, S.; Law, I.; Page-Sharp, M.; Rogerson, S.; Siba, P.; Ilett, K.F.; et al. Pharmacokinetics of Chloroquine and Monodesethylchloroquine in Pregnancy. Antimicrob. Agents Chemother. 2010, 54, 1186–1192. [Google Scholar] [CrossRef] [Green Version]
- Ofori-Adjei, D.; Ericsson, O.; Lindstrom, B.; Sjöqvist, F. Protein binding of chloroquine enantiomers and desethylchloroquine. Br. J. Clin. Pharmacol. 1986, 22, 356–358. [Google Scholar] [CrossRef] [Green Version]
- Walker, O.; Birkett, D.; Alvan, G.; Gustafsson, L.; Sjoqvist, F. Characterization of chloroquine plasma protein binding in man. Br. J. Clin. Pharmacol. 1983, 15, 375–377. [Google Scholar] [CrossRef] [Green Version]
- Augustijns, P.; Verbeke, N. Stereoselective Pharmacokinetic Properties of Chloroquine and De-Ethyl-Chloroquine in Humans. Clin. Pharmacokinet. 1993, 24, 259–269. [Google Scholar] [CrossRef]
- Aderounmu, A.F.; Salako, L.A.; Lindstrom, B.; Walker, O.; Ekman, L. Comparison of the pharmacokinetics of chloroquine after single intravenous and intramuscular administration in healthy Africans. Br. J. Clin. Pharmacol. 1986, 22, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducharme, J.; Farinotti, R. Clinical Pharmacokinetics and Metabolism of Chloroquine. Focus on recent advancements. Clin. Pharmacokinet. 1996, 31, 257–274. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, L.L.; Rombo, L.; Alván, G.; Björkman, A.; Lind, M.; Walker, O. On the question of dose-dependent chloroquine elimination of a single oral dose. Clin. Pharmacol. Ther. 1983, 34, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Frisk-Holmberg, M.; Bergqvist, Y.; Englund, U. Chloroquine intoxication. Br. J. Clin. Pharmacol. 1983, 15, 502–503. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Marmor, M.F. The Risk of Toxic Retinopathy in Patients on Long-term Hydroxychloroquine Therapy. JAMA Ophthalmol. 2014, 132, 1453–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Marmor, M.F. Rates and predictors of hydroxychloroquine retinal toxicity in patients with rheumatoid arthritis and systemic lupus erythematosus. Arthritis Care Res. 2010, 62, 775–784. [Google Scholar] [CrossRef]
- Costedoat-Chalumeau, N.; Dunogué, B.; Leroux, G.; Morel, N.; Jallouli, M.; Le Guern, V.; Piette, J.-C.; Brézin, A.P.; Melles, R.B.; Marmor, M.F. A Critical Review of the Effects of Hydroxychloroquine and Chloroquine on the Eye. Clin. Rev. Allergy Immunol. 2015, 49, 317–326. [Google Scholar] [CrossRef]
- Yusuf, I.; Latheef, F.; Ardern-Jones, M.; Lotery, A. New recommendations for retinal monitoring in hydroxychloroquine users: Baseline testing is no longer supported. Br. J. Dermatol. 2021, 185, 435–438. [Google Scholar] [CrossRef]
- Estes, M.L.; Ewing-Wilson, D.; Chou, S.M.; Mitsumoto, H.; Hanson, M.; Shirey, E.; Ratliff, N.B. Chloroquine neuromyotoxicity. Clinical and pathologic perspective. Am. J. Med. 1987, 82, 447–455. [Google Scholar] [CrossRef]
- Martins, A.C.; Cayotopa, A.D.E.; Klein, W.W.; Schlosser, A.R.; da Silva, A.F.; de Souza, M.N.; Andrade, B.W.B.; Filgueira-Júnior, J.A.; Pinto, W.D.J.; da Silva-Nunes, M. Side Effects of Chloroquine and Primaquine and Symptom Reduction in Malaria Endemic Area (Mâncio Lima, Acre, Brazil). Interdiscip. Perspect. Infect. Dis. 2015, 2015, 346853. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Rønne, T.; Rønn, A.; Bygbjerg, I.; Larsen, S.O. Reported side effects to chloroquine, chloroquine plus proguanil, and mefloquine as chemoprophylaxis against malaria in Danish travelers. J. Travel Med. 2000, 7, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Frisk-Holmberg, M.; Bergkvist, Y.; Domeij-Nyberg, B.; Hellström, L.; Jansson, F. Chloroquine serum concentration and side effects: Evidence for dose-dependent kinetics. Clin. Pharmacol. Ther. 1979, 25, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Aghahowa, S.; Obianwu, H.; Isah, A.; Arhewoh, I. Chloroquine-induced Pruritus. Indian J. Pharm. Sci. 2010, 72, 283–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ademowo, O.; Sodeinde, O.; Walker, O. The disposition of chloroquine and its main metabolite desethylchloroquine in volunteers with and without chloroquine-induced pruritus: Evidence for decreased chloroquine metabolism in volunteers with pruritus. Clin. Pharmacol. Ther. 2000, 67, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, N.M.; Nevin, R.L.; Stahl, S.; Block, J.; Shugarts, S.; Wu, A.H.B.; Dominy, S.; Solano-Blanco, M.A.; Kappelman-Culver, S.; Lee-Messer, C.; et al. Prolonged neuropsychiatric effects following management of chloroquine intoxication with psychotropic polypharmacy. Clin. Case Rep. 2015, 3, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Mohan, D.; Mohandas, E.; Rajat, R. Chloroquine psychosis: A chemical psychosis? J. Natl. Med. Assoc. 1981, 73, 1073–1076. [Google Scholar]
- Zou, H.; Yang, Y.; Dai, H.; Xiong, Y.; Wang, J.-Q.; Lin, L.; Chen, Z.-S. Recent Updates in Experimental Research and Clinical Evaluation on Drugs for COVID-19 Treatment. Front. Pharmacol. 2021, 12, 732403. [Google Scholar] [CrossRef]
- Hooks, M.; Bart, B.; Vardeny, O.; Westanmo, A.; Adabag, S. Effects of hydroxychloroquine treatment on QT interval. Heart Rhythm 2020, 17, 1930–1935. [Google Scholar] [CrossRef]
- Concordia Pharmaceuticals Inc. Plaquenil (Hydroxychloroquine Sulfate) [Package Insert]. U.S. Food and Drug Admin-Istration Website. Revised October 2018. Available online: www.accessdata.fda.gov/drugsatfda_docs/label/2018/006002s045lbl.pdf (accessed on 12 November 2021).
- Hansen, M.; Rubinsztein, D.C.; Walker, D.W. Autophagy as a promoter of longevity: Insights from model organisms. Nat. Rev. Mol. Cell Biol. 2018, 19, 579–593. [Google Scholar] [CrossRef]
- Gómez, V.E.; Giovannetti, E.; Peters, G.J. Unraveling the complexity of autophagy: Potential therapeutic applications in Pancreatic Ductal Adenocarcinoma. Semin. Cancer Biol. 2015, 35, 11–19. [Google Scholar] [CrossRef]
- Green, D.R.; Llambi, F. Cell death signaling. Cold Spring Harb. Perspect. Biol. 2015, 7, a006080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boone, B.A.; Zeh, H.J.; Bahary, N. Autophagy Inhibition in Pancreatic Adenocarcinoma. Clin. Color. Cancer 2018, 17, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomé, R.; Lopes, S.C.P.; Costa, F.T.M.; Verinaud, L. Chloroquine: Modes of action of an undervalued drug. Immunol. Lett. 2013, 153, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Sundelin, S.P.; Terman, A. Different effects of chloroquine and hydroxychloroquine on lysosomal function in cultured retinal pigment epithelial cells. APMIS 2002, 110, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Kang, R.; Tang, D. Autophagy in pancreatic cancer pathogenesis and treatment. Am. J. Cancer Res. 2012, 2, 383–396. [Google Scholar]
- Qureshi-Baig, K.; Kuhn, D.; Viry, E.; Pozdeev, V.I.; Schmitz, M.; Rodriguez, F.; Ullmann, P.; Koncina, E.; Nurmik, M.; Frasquilho, S.; et al. Hypoxia-induced autophagy drives colorectal cancer initiation and progression by activating the PRKC/PKC-EZR (ezrin) pathway. Autophagy 2020, 16, 1436–1452. [Google Scholar] [CrossRef] [Green Version]
- Sehgal, A.R.; Konig, H.; Johnson, D.E.; Tang, D.; Amaravadi, R.K.; Boyiadzis, M.; Lotze, M.T. You eat what you are: Autophagy inhibition as a therapeutic strategy in leukemia. Leukemia 2015, 29, 517–525. [Google Scholar] [CrossRef]
- Martinez-Outschoorn, U.; Pavlides, S.; Whitaker-Menezes, D.; Daumer, K.M.; Milliman, J.N.; Chiavarina, B.; Migneco, G.; Witkiewicz, A.K.; Cantarin, M.P.M.; Flomenberg, N.; et al. Tumor cells induce the cancer associated fibroblast phenotype via caveolin-1 degradation: Implications for breast cancer and DCIS therapy with autophagy inhibitors. Cell Cycle 2010, 9, 2423–2433. [Google Scholar] [CrossRef] [Green Version]
- Bigelsen, S. Evidence-based complementary treatment of pancreatic cancer: A review of adjunct therapies including paricalcitol, hydroxychloroquine, intravenous vitamin C, statins, metformin, curcumin, and aspirin. Cancer Manag. Res. 2018, 10, 2003–2018. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Wang, X.; Contino, G.; Liesa, M.; Sahin, E.; Ying, H.; Bause, A.; Li, Y.; Stommel, J.M.; Dell’Antonio, G.; et al. Pancreatic cancers require autophagy for tumor growth. Genes Dev. 2011, 25, 717–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.-C.; Wang, H.-C.; Hou, Y.-C.; Tung, H.-L.; Chiu, T.-J.; Shan, Y.-S. Blockade of autophagy reduces pancreatic cancer stem cell activity and potentiates the tumoricidal effect of gemcitabine. Mol. Cancer 2015, 14, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousquet, G.; El Bouchtaoui, M.; Sophie, T.; Leboeuf, C.; de Bazelaire, C.; Ratajczak, P.; Giacchetti, S.; de Roquancourt, A.; Bertheau, P.; Verneuil, L.; et al. Targeting autophagic cancer stem-cells to reverse chemoresistance in human triple negative breast cancer. Oncotarget 2017, 8, 35205. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-J.; Lei, Y.-H.; Yao, N.; Wang, C.-R.; Hu, N.; Ye, W.-C.; Zhang, D.-M.; Chen, Z.-S. Autophagy and multidrug resistance in cancer. Chin. J. Cancer 2017, 36, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, Y.; Zhang, Z.; Shang, Y.; Jiang, X.; Dong, J.; Yu, P.; Nie, Y.; Zhao, Q. miR-23b-3p regulates the chemoresistance of gastric cancer cells by targeting ATG12 and HMGB2. Cell Death Dis. 2015, 6, e1766. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, D.; Bläuer, M.; Hirota, M.; Ikonen, N.H.; Sand, J.; Laukkarinen, J. Autophagy is needed for the growth of pancreatic adenocarcinoma and has a cytoprotective effect against anticancer drugs. Eur. J. Cancer 2014, 50, 1382–1390. [Google Scholar] [CrossRef]
- Huang, H.; Song, J.; Liu, Z.; Pan, L.; Xu, G. Autophagy activation promotes bevacizumab resistance in glioblastoma by suppressing Akt/mTOR signaling pathway. Oncol. Lett. 2018, 15, 1487–1494. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.-Q.; Wang, S.-B.; Shao, Y.-F.; Shi, J.-N.; Wang, W.; Chen, W.-Y.; Ye, Z.-Q.; Jiang, J.-Y.; Fang, Q.-X.; Zhang, G.-B.; et al. Hydroxychloroquine potentiates the anti-cancer effect of bevacizumab on glioblastoma via the inhibition of autophagy. Biomed. Pharmacother. 2019, 118, 109339. [Google Scholar] [CrossRef]
- Endo, S.; Nakata, K.; Ohuchida, K.; Takesue, S.; Nakayama, H.; Abe, T.; Koikawa, K.; Okumura, T.; Sada, M.; Horioka, K.; et al. Autophagy Is Required for Activation of Pancreatic Stellate Cells, Associated with Pancreatic Cancer Progression and Promotes Growth of Pancreatic Tumors in Mice. Gastroenterology 2017, 152, 1492–1506.e24. [Google Scholar] [CrossRef] [Green Version]
- Rockel, J.S.; Kapoor, J.S.R.M. Autophagy: Controlling cell fate in rheumatic diseases. Nat. Rev. Rheumatol. 2016, 12, 517–531. [Google Scholar] [CrossRef]
- Delgado-Rizo, V.; Martínez-Guzmán, M.A.; Iñiguez-Gutierrez, L.; García-Orozco, A.; Alvarado-Navarro, A.; Fafutis-Morris, M. Neutrophil Extracellular Traps and Its Implications in Inflammation: An Overview. Front. Immunol. 2017, 8, 81. [Google Scholar] [CrossRef] [Green Version]
- Schrezenmeier, E.; Dörner, T. Mechanisms of action of hydroxychloroquine and chloroquine: Implications for rheumatology. Nat. Rev. Rheumatol. 2020, 16, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Khan, U.; Ghazanfar, H. T Lymphocytes and Autoimmunity. Int. Rev. Cell Mol. Biol. 2018, 341, 125–168. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Puebla, A.; Boya, P. Lysosomal membrane permeabilization as a cell death mechanism in cancer cells. Biochem. Soc. Trans. 2018, 46, 207–215. [Google Scholar] [CrossRef]
- Boya, P.; Gonzalez-Polo, R.-A.; Poncet, D.; Andreau, K.; LA Vieira, H.; Roumier, T.; Perfettini, J.-L.; Kroemer, G. Mitochondrial membrane permeabilization is a critical step of lysosome-initiated apoptosis induced by hydroxychloroquine. Oncogene 2003, 22, 3927–3936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Circu, M.; Cardelli, J.; Barr, M.; O’Byrne, K.; Mills, G.; El-Osta, H. Modulating lysosomal function through lysosome membrane permeabilization or autophagy suppression restores sensitivity to cisplatin in refractory non-small-cell lung cancer cells. PLoS ONE 2017, 12, e0184922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seitz, C.; Hugle, M.; Cristofanon, S.; Tchoghandjian, A.; Fulda, S. The dual PI3K/mTOR inhibitor NVP-BEZ235 and chloroquine synergize to trigger apoptosis via mitochondrial-lysosomal cross-talk. Int. J. Cancer 2013, 132, 2682–2693. [Google Scholar] [CrossRef] [PubMed]
- Enzenmüller, S.; Gonzalez, P.; Debatin, K.-M.; Fulda, S. Chloroquine overcomes resistance of lung carcinoma cells to the dual PI3K/mTOR inhibitor PI103 by lysosome-mediated apoptosis. Anti-Cancer Drugs 2013, 24, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Coban, C. The host targeting effect of chloroquine in malaria. Curr. Opin. Immunol. 2020, 66, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wicht, K.J.; Mok, S.; Fidock, D.A. Molecular Mechanisms of Drug Resistance in Plasmodium falciparum Malaria. Annu. Rev. Microbiol. 2020, 74, 431–454. [Google Scholar] [CrossRef]
- Fidock, D.A.; Nomura, T.; Talley, A.K.; Cooper, R.A.; Dzekunov, S.M.; Ferdig, M.T.; Ursos, L.M.; Sidhu, A.B.S.; Naudé, B.; Deitsch, K.W.; et al. Mutations in the P. falciparum Digestive Vacuole Transmembrane Protein PfCRT and Evidence for Their Role in Chloroquine Resistance. Mol. Cell 2000, 6, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Dunia, D.; Cubitt, B.; de la Torre, J.C. Mechanism of Borna Disease Virus Entry into Cells. J. Virol. 1998, 72, 783–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ros, C.; Burckhardt, C.J.; Kempf, C. Cytoplasmic Trafficking of Minute Virus of Mice: Low-pH Requirement, Routing to Late Endosomes, and Proteasome Interaction. J. Virol. 2002, 76, 12634–12645. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yi, C.; Li, C.; Zhang, F.; Peng, J.; Wang, Q.; Liu, X.; Ye, X.; Li, P.; Wu, M.; et al. Chloroquine inhibits endosomal viral RNA release and autophagy-dependent viral replication and effectively prevents maternal to fetal transmission of Zika virus. Antivir. Res. 2019, 169, 104547. [Google Scholar] [CrossRef]
- Bishop, N.E. Examination of Potential Inhibitors of Hepatitis A Virus Uncoating. Intervirology 1998, 41, 261–271. [Google Scholar] [CrossRef]
- Jiang, M.-C.; Lin, J.-K.; Chen, S.S.-L. Inhibition of HIV-1 Tat-Mediated Transactivation by Quinacrine and Chloroquine. Biochem. Biophys. Res. Commun. 1996, 226, 1–7. [Google Scholar] [CrossRef]
- Ahmad-Nejad, P.; Häcker, H.; Rutz, M.; Bauer, S.; Vabulas, R.M.; Wagner, H. Bacterial CpG-DNA and lipopolysaccharides activate toll-like receptors at distinct cellular compartments. Eur. J. Immunol. 2002, 32, 1958–1968. [Google Scholar] [CrossRef]
- Liu, Y.; Yan, W.; Tohme, S.; Chen, M.; Fu, Y.; Tian, D.; Lotze, M.; Tang, D.; Tsung, A. Hypoxia induced HMGB1 and mitochondrial DNA interactions mediate tumor growth in hepatocellular carcinoma through Toll-like receptor 9. J. Hepatol. 2015, 63, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Tian, J.; Avalos, A.M.; Mao, S.-Y.; Chen, B.; Senthil, K.; Wu, H.; Parroche, P.; Drabic, S.; Golenbock, D.T.; Sirois, C.M.; et al. Toll-like receptor 9–dependent activation by DNA-containing immune complexes is mediated by HMGB1 and RAGE. Nat. Immunol. 2007, 8, 487–496. [Google Scholar] [CrossRef]
- Tai, N.; Wong, F.S.; Wen, L. The role of the innate immune system in destruction of pancreatic beta cells in NOD mice and humans with type I diabetes. J. Autoimmun. 2016, 71, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Tai, N.; Wong, F.S.; Wen, L. TLR9 Deficiency Promotes CD73 Expression in T Cells and Diabetes Protection in Nonobese Diabetic Mice. J. Immunol. 2013, 191, 2926–2937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Peng, J.; Tai, N.; Pearson, J.A.; Hu, C.; Guo, J.; Hou, L.; Zhao, H.; Wong, F.S.; Wen, L. Toll-like receptor 9 negatively regulates pancreatic islet beta cell growth and function in a mouse model of type 1 diabetes. Diabetologia 2018, 61, 2333–2343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutz, M.; Metzger, J.; Gellert, T.; Luppa, P.; Lipford, G.B.; Wagner, H.; Bauer, S. Toll-like receptor 9 binds single-stranded CpG-DNA in a sequence- and pH-dependent manner. Eur. J. Immunol. 2004, 34, 2541–2550. [Google Scholar] [CrossRef]
- Yasuda, H.; Leelahavanichkul, A.; Tsunoda, S.; Dear, J.W.; Takahashi, Y.; Ito, S.; Hu, X.; Zhou, H.; Doi, K.; Childs, R.; et al. Chloroquine and inhibition of Toll-like receptor 9 protect from sepsis-induced acute kidney injury. Am. J. Physiol. Physiol. 2008, 294, F1050–F1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Kebir, D.; József, L.; Pan, W.; Wang, L.; Filep, J.G. Bacterial DNA Activates Endothelial Cells and Promotes Neutrophil Adherence through TLR9 Signaling. J. Immunol. 2009, 182, 4386–4394. [Google Scholar] [CrossRef] [Green Version]
- Sacre, K.; Criswell, L.A.; McCune, J.M. Hydroxychloroquine is associated with impaired interferon-alpha and tumor necrosis factor-alpha production by plasmacytoid dendritic cells in systemic lupus erythematosus. Arthritis Res. Ther. 2012, 14, R155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kužnik, A.; Benčina, M.; Švajger, U.; Jeras, M.; Rozman, B.; Jerala, R. Mechanism of Endosomal TLR Inhibition by Antimalarial Drugs and Imidazoquinolines. J. Immunol. 2011, 186, 4794–4804. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Zhang, Q.; Wang, F.; Guo, X.; Liu, T.; Zhao, Y.; Gu, B.; Chen, H.; Li, Y. Hydroxychloroquine inhibiting neutrophil extracellular trap formation alleviates hepatic ischemia/reperfusion injury by blocking TLR9 in mice. Clin. Immunol. 2020, 216, 108461. [Google Scholar] [CrossRef]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef]
- Brinkmann, V. Neutrophil Extracellular Traps in the Second Decade. J. Innate Immun. 2018, 10, 414–421. [Google Scholar] [CrossRef]
- Yipp, B.G.; Petri, B.; Salina, D.; Jenne, C.N.; Scott, B.N.V.; Zbytnuik, L.D.; Pittman, K.; Asaduzzaman, M.; Wu, K.; Meijndert, H.C.; et al. Infection-induced NETosis is a dynamic process involving neutrophil multitasking in vivo. Nat. Med. 2012, 18, 1386–1393. [Google Scholar] [CrossRef] [Green Version]
- Berthelot, J.-M.; Le Goff, B.; Neel, A.; Maugars, Y.; Hamidou, M. NETosis: At the crossroads of rheumatoid arthritis, lupus, and vasculitis. Jt. Bone Spine 2016, 84, 255–262. [Google Scholar] [CrossRef]
- Zhou, W.; Guo, S.; Liu, M.; Burow, M.E.; Wang, G. Targeting CXCL12/CXCR4 Axis in Tumor Immunotherapy. Curr. Med. Chem. 2019, 26, 3026–3041. [Google Scholar] [CrossRef]
- Pozzobon, T.; Goldoni, G.; Viola, A.; Molon, B. CXCR4 signaling in health and disease. Immunol. Lett. 2016, 177, 6–15. [Google Scholar] [CrossRef]
- Tachibana, K.; Hirota, S.; Iizasa, H.; Yoshida, H.; Kawabata, K.; Kataoka, Y.; Kitamura, Y.; Matsushima, K.; Yoshida, N.; Nishikawa, S.-I.; et al. The chemokine receptor CXCR4 is essential for vascularization of the gastrointestinal tract. Nature 1998, 393, 591–594. [Google Scholar] [CrossRef]
- Nagasawa, T.; Hirota, S.; Tachibana, K.; Takakura, N.; Nishikawa, S.-I.; Kitamura, Y.; Yoshida, N.; Kikutani, H.; Kishimoto, T. Defects of B-cell lymphopoiesis and bone-marrow myelopoiesis in mice lacking the CXC chemokine PBSF/SDF-1. Nature 1996, 382, 635–638. [Google Scholar] [CrossRef]
- Kruizinga, R.C.; Bestebroer, J.; Berghuis, P.; de Haas, C.J.C.; Links, T.P.; de Vries, E.G.E.; Walenkamp, A.M.E. Role of chemokines and their receptors in cancer. Curr. Pharm. Des. 2009, 15, 3396–3416. [Google Scholar] [CrossRef]
- Domańska, U.M.; Kruizinga, R.C.; Nagengast, W.B.; Timmer-Bosscha, H.; Huls, G.; de Vries, E.G.; Walenkamp, A.M. A review on CXCR4/CXCL12 axis in oncology: No place to hide. Eur. J. Cancer 2013, 49, 219–230. [Google Scholar] [CrossRef]
- Feng, Y.; Broder, C.C.; Kennedy, P.E.; Berger, E.A. HIV-1 Entry Cofactor: Functional cDNA Cloning of a Seven-Transmembrane, G Protein-Coupled Receptor. Science 1996, 272, 872–877. [Google Scholar] [CrossRef]
- Loetscher, P.; Moser, B.; Baggiolini, M. Chemokines and Their Receptors in Lymphocyte Traffic and HIV Infection. Adv. Immunol. 2000, 74, 127–180. [Google Scholar] [CrossRef]
- Mortezaee, K. CXCL12/CXCR4 axis in the microenvironment of solid tumors: A critical mediator of metastasis. Life Sci. 2020, 249, 117534. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, A. CXCL12/CXCR4 signal transduction in diseases and its molecular approaches in targeted-therapy. Immunol. Lett. 2020, 217, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Azad, B.B.; Nimmagadda, S. The Intricate Role of CXCR4 in Cancer. Adv. Cancer Res. 2014, 124, 31–82. [Google Scholar] [CrossRef]
- Han, J.; Li, X.; Luo, X.; He, J.; Huang, X.; Zhou, Q.; Han, Y.; Jie, H.; Zhuang, J.; Li, Y.; et al. The mechanisms of hydroxychloroquine in rheumatoid arthritis treatment: Inhibition of dendritic cell functions via Toll like receptor 9 signaling. Biomed. Pharmacother. 2020, 132, 110848. [Google Scholar] [CrossRef]
- Schols, D.; Hatse, S. CXCL12-CXCR4 Axis in Angiogenesis, Metastasis and Stem Cell Mobilization. Curr. Pharm. Des. 2010, 16, 3903–3920. [Google Scholar] [CrossRef]
- Kim, J.; Yip, M.L.R.; Shen, X.; Li, H.; Hsin, L.-Y.C.; LaBarge, S.; Heinrich, E.L.; Lee, W.; Lu, J.; Vaidehi, N. Identification of Anti-Malarial Compounds as Novel Antagonists to Chemokine Receptor CXCR4 in Pancreatic Cancer Cells. PLoS ONE 2012, 7, e31004. [Google Scholar] [CrossRef] [Green Version]
- Balic, A.; Sørensen, M.D.; Trabulo, S.M.; Sainz, B.; Cioffi, M.; Vieira, C.R.; Miranda-Lorenzo, I.; Hidalgo, M.; Kleeff, J.; Erkan, M.; et al. Chloroquine Targets Pancreatic Cancer Stem Cells via Inhibition of CXCR4 and Hedgehog Signaling. Mol. Cancer Ther. 2014, 13, 1758–1771. [Google Scholar] [CrossRef] [Green Version]
- Yue, D.; Zhang, D.; Shi, X.; Liu, S.; Li, A.; Wang, D.; Qin, G.; Ping, Y.; Qiao, Y.; Chen, X.; et al. Chloroquine Inhibits Stemness of Esophageal Squamous Cell Carcinoma Cells Through Targeting CXCR4-STAT3 Pathway. Front. Oncol. 2020, 10, 311. [Google Scholar] [CrossRef]
- Verbaanderd, C.; Maes, H.; Schaaf, M.B.; Sukhatme, V.P.; Pantziarka, P.; Sukhatme, V.; Agostinis, P.; Bouche, G. Repurposing Drugs in Oncology (ReDO)—Chloroquine and hydroxychloroquine as anti-cancer agents. Ecancermedicalscience 2017, 11, 781. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Xie, Y.; Wang, Y.; Peng, Z.-H.; Li, J.; Oupický, D. Chloroquine-Containing HPMA Copolymers as Polymeric Inhibitors of Cancer Cell Migration Mediated by the CXCR4/SDF-1 Chemokine Axis. ACS Macro Lett. 2016, 5, 342–345. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Li, J.; Xie, Y.; Sleightholm, R.L.; Oupický, D. Polymeric chloroquine as an inhibitor of cancer cell migration and experimental lung metastasis. J. Control. Release 2016, 244, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Kang, R.; Zeh, H.J.; Lotze, M.T.; Tang, D. The Beclin 1 network regulates autophagy and apoptosis. Cell Death Differ. 2011, 18, 571–580. [Google Scholar] [CrossRef]
- Xu, T.; Jiang, L.; Wang, Z. The progression of HMGB1-induced autophagy in cancer biology. OncoTargets Ther. 2019, 12, 365–377. [Google Scholar] [CrossRef]
- Schiraldi, M.; Raucci, A.; Muñoz, L.M.; Livoti, E.; Celona, B.; Venereau, E.; Apuzzo, T.; De Marchis, F.; Pedotti, M.; Bachi, A.; et al. HMGB1 promotes recruitment of inflammatory cells to damaged tissues by forming a complex with CXCL12 and signaling via CXCR4. J. Exp. Med. 2012, 209, 551–563. [Google Scholar] [CrossRef] [Green Version]
- Yasinska, I.; Silva, I.G.; Sakhnevych, S.S.; Ruegg, L.; Hussain, R.; Siligardi, G.; Fiedler, W.; Wellbrock, J.; Bardelli, M.; Varani, L.; et al. High mobility group box 1 (HMGB1) acts as an “alarmin” to promote acute myeloid leukaemia progression. OncoImmunology 2018, 7, e1438109. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Cao, L.; Xie, M.; Yu, Y.; Kang, R.; Yang, L.; Zhao, M.; Tang, D. Chloroquine inhibits HMGB1 inflammatory signaling and protects mice from lethal sepsis. Biochem. Pharmacol. 2013, 86, 410–418. [Google Scholar] [CrossRef] [Green Version]
- Chiba, S.; Baghdadi, M.; Akiba, H.; Yoshiyama, H.; Kinoshita, I.; Dosaka-Akita, H.; Fujioka, Y.; Ohba, Y.; Gorman, J.V.; Colgan, J.D.; et al. Tumor-infiltrating DCs suppress nucleic acid–mediated innate immune responses through interactions between the receptor TIM-3 and the alarmin HMGB1. Nat. Immunol. 2012, 13, 832–842. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-P.; Cui, Q.-Y.; Zhang, T.-M.; Yi, Y.; Nie, J.-J.; Xie, G.-H.; Wu, J.-H. Chloroquine pretreatment attenuates ischemia-reperfusion injury in the brain of ob/ob diabetic mice as well as wildtype mice. Brain Res. 2020, 1726, 146518. [Google Scholar] [CrossRef]
- Dai, C.; Xiao, X.; Li, D.; Tun, S.; Wang, Y.; Velkov, T.; Tang, S. Chloroquine ameliorates carbon tetrachloride-induced acute liver injury in mice via the concomitant inhibition of inflammation and induction of apoptosis. Cell Death Dis. 2018, 9, 1164. [Google Scholar] [CrossRef] [Green Version]
- Schierbeck, H.; Wähämaa, H.; Andersson, U.; Harris, H.E. Immunomodulatory Drugs Regulate HMGB1 Release from Activated Human Monocytes. Mol. Med. 2010, 16, 343–351. [Google Scholar] [CrossRef]
- Nosál’, R.; Jančinová, V.; Danihelová, E. Chloroquine: A Multipotent Inhibitor of Human Platelets In Vitro. Thromb. Res. 2000, 98, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Nosál’, R.; Jančinová, V. Cationic amphiphilic drugs and platelet phospholipase A2 (cPLA2). Thromb. Res. 2002, 105, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Nosál, R.; Jančinová, V.; Petríková, M. Chloroquine inhibits stimulated platelets at the arachidonic acid pathway. Thromb. Res. 1995, 77, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Li, M.; Lindberg, M.R.; Kennett, M.J.; Xiong, N.; Wang, Y. PAD4 is essential for antibacterial innate immunity mediated by neutrophil extracellular traps. J. Exp. Med. 2010, 207, 1853–1862. [Google Scholar] [CrossRef] [PubMed]
- Lewis, H.D.; Liddle, J.; Coote, J.E.; Atkinson, S.J.; Barker, M.D.; Bax, B.; Bicker, K.L.; Bingham, R.P.; Campbell, M.; Chen, Y.H.; et al. Inhibition of PAD4 activity is sufficient to disrupt mouse and human NET formation. Nat. Chem. Biol. 2015, 11, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Petri, M. Use of Hydroxychloroquine to Prevent Thrombosis in Systemic Lupus Erythematosus and in Antiphospholipid Antibody–Positive Patients. Curr. Rheumatol. Rep. 2010, 13, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Tincani, A.; Ward, M.M. Response to: “Correspondence on EULAR recommendations for the management of antiphospholipid syndrome in adults” by Gao and Qin. Ann. Rheum. Dis. 2021. [Google Scholar] [CrossRef]
- Rand, J.H.; Wu, X.-X.; Quinn, A.S.; Ashton, A.W.; Chen, P.P.; Hathcock, J.J.; Andree, H.A.M.; Taatjes, D.J. Hydroxychloroquine protects the annexin A5 anticoagulant shield from disruption by antiphospholipid antibodies: Evidence for a novel effect for an old antimalarial drug. Blood 2010, 115, 2292–2299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinola, R.G.; Pierangeli, S.S.; Ghara, A.E.; Harris, E.N. Hydroxychloroquine reverses platelet acti-vation induced by human IgG antiphospholipid antibodies. Thromb. Haemost. 2002, 87, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.H.; Pierangeli, S.; Liu, X.; Barker, J.H.; Anderson, G.; Harris, E.N. Hydroxychloroquine Reverses Thrombogenic Properties of Antiphospholipid Antibodies in Mice. Circulation 1997, 96, 4380–4384. [Google Scholar] [CrossRef] [PubMed]
- Miranda, S.; Billoir, P.; Damian, L.; Thiebaut, P.A.; Schapman, D.; Le Besnerais, M.; Jouen, F.; Galas, L.; Levesque, H.; Le Cam-Duchez, V.; et al. Hydroxychloroquine reverses the prothrombotic state in a mouse model of antiphospholipid syndrome: Role of reduced inflammation and endothelial dysfunction. PLoS ONE 2019, 14, e0212614. [Google Scholar] [CrossRef] [Green Version]
- Urbanski, G.; Caillon, A.; Poli, C.; Kauffenstein, G.; Begorre, M.-A.; Loufrani, L.; Henrion, D.; Belizna, C. Hydroxychloroquine partially prevents endothelial dysfunction induced by anti-beta-2-GPI antibodies in an in vivo mouse model of antiphospholipid syndrome. PLoS ONE 2018, 13, e0206814. [Google Scholar] [CrossRef] [Green Version]
- Pierangeli, S.S.; Vega-Ostertag, M.; Harris, E.N. Intracellular signaling triggered by antiphospholipid antibodies in platelets and endothelial cells: A pathway to targeted therapies. Thromb. Res. 2004, 114, 467–476. [Google Scholar] [CrossRef]
- Rand, J.H.; Wu, X.-X.; Quinn, A.S.; Chen, P.P.; Hathcock, J.J.; Taatjes, D.J. Hydroxychloroquine directly reduces the binding of antiphospholipid antibody–β2-glycoprotein I complexes to phospholipid bilayers. Blood 2008, 112, 1687–1695. [Google Scholar] [CrossRef]
- Müller-Calleja, N.; Hollerbach, A.; Häuser, F.; Canisius, A.; Orning, C.; Lackner, K.J. Antiphospholipid antibody-induced cellular responses depend on epitope specificity: Implications for treatment of antiphospholipid syndrome. J. Thromb. Haemost. 2017, 15, 2367–2376. [Google Scholar] [CrossRef] [Green Version]
- Müller-Calleja, N.; Manukyan, D.; Canisius, A.; Strand, D.; Lackner, K.J. Hydroxychloroquine inhibits proinflammatory signalling pathways by targeting endosomal NADPH oxidase. Ann. Rheum. Dis. 2017, 76, 891–897. [Google Scholar] [CrossRef]
- De Moreuil, C.; Alavi, Z.; Pasquier, E. Hydroxychloroquine may be beneficial in preeclampsia and recurrent miscarriage. Br. J. Clin. Pharmacol. 2020, 86, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Josephs, S.F.; Ichim, T.E.; Prince, S.M.; Kesari, S.; Marincola, F.M.; Escobedo, A.R.; Jafri, A. Unleashing endogenous TNF-alpha as a cancer immunotherapeutic. J. Transl. Med. 2018, 16, 242. [Google Scholar] [CrossRef] [Green Version]
- Le, N.-T.; Takei, Y.; Izawa-Ishizawa, Y.; Heo, K.-S.; Lee, H.; Smrcka, A.V.; Miller, B.; Ko, K.A.; Ture, S.; Morrell, C.; et al. Identification of Activators of ERK5 Transcriptional Activity by High-Throughput Screening and the Role of Endothelial ERK5 in Vasoprotective Effects Induced by Statins and Antimalarial Agents. J. Immunol. 2014, 193, 3803–3815. [Google Scholar] [CrossRef] [Green Version]
- Dyer, M.R.; Alexander, W.; Hassoune, A.; Chen, Q.; Brzoska, T.; Alvikas, J.; Liu, Y.; Haldeman, S.; Plautz, W.; Loughran, P.; et al. Platelet-derived extracellular vesicles released after trauma promote hemostasis and contribute to DVT in mice. J. Thromb. Haemost. 2019, 17, 1733–1745. [Google Scholar] [CrossRef]
- Fessler, B.J.; Alarcón, G.S.; McGwin, G.; Roseman, J.; Bastian, H.M.; Friedman, A.W.; Baethge, B.A.; Vilá, L.; Reveille, J.D.; LUMINA Study Group. Systemic lupus erythematosus in three ethnic groups: XVI. Association of hydroxychloroquine use with reduced risk of damage accrual. Arthritis Care Res. 2005, 52, 1473–1480. [Google Scholar] [CrossRef]
- Alarcón, G.S.; McGwin, G.; Bertoli, A.M.; Fessler, B.J.; Calvo-Alén, J.; Bastian, H.M.; Vilá, L.M.; Reveille, J.D. Effect of hydroxychloroquine on the survival of patients with systemic lupus erythematosus: Data from LUMINA, a multiethnic US cohort (LUMINA L). Ann. Rheum. Dis. 2007, 66, 1168–1172. [Google Scholar] [CrossRef] [Green Version]
- Rudnicki, R.D.; Gresham, G.E.; Rothfield, N.F. The efficacy of antimalarials in systemic lupus erythematosus. J. Rheumatol. 1975, 2, 323–330. [Google Scholar]
- Canadian Hydroxychloroquine Study Group. A Randomized Study of the Effect of Withdrawing Hydroxychloroquine Sulfate in Systemic Lupus Erythematosus. N. Engl. J. Med. 1991, 324, 150–154. [Google Scholar] [CrossRef]
- Woźniacka, A.; Lesiak, A.; Smigielski, J.; Sysa-Jedrzejowska, A. Chloroquine influence on lipid metabolism and selected laboratory parameters. Prz. Lek. 2005, 62, 855–859. [Google Scholar]
- Sachet, J.; Borba, E.; Bonfá, E.; Vinagre, C.; Silva, V.; Maranhão, R. Chloroquine increases low-density lipoprotein removal from plasma in systemic lupus patients. Lupus 2007, 16, 273–278. [Google Scholar] [CrossRef]
- Meng, J.; Lu, Y.; Dong, X.; Liu, H. Long-term effects of hydroxychloroquine on metabolism of serum lipids and left ventricular structure and function in patients of systemic lupus erythematosus. Zhonghua Yi Xue Za Zhi 2014, 94, 965–968. [Google Scholar]
- Sisó, A.; Ramos-Casals, M.; Bové, A.; Brito-Zerón, P.; Soria, N.; Muñoz, S.; Testi, A.; Plaza, J.; Sentís, J.; Coca, A. Previous antimalarial therapy in patients diagnosed with lupus nephritis: Influence on outcomes and survival. Lupus 2008, 17, 281–288. [Google Scholar] [CrossRef]
- An, Y.; Zhou, Y.; Bi, L.; Liu, B.; Wang, H.; Lin, J.; Xu, D.; Wang, M.; Zhang, J.; Wang, Y.; et al. Combined immunosuppressive treatment (CIST) in lupus nephritis: A multicenter, randomized controlled study. Clin. Rheumatol. 2019, 38, 1047–1054. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Egurbide, M.-V.; Pijoan, J.-I.; Garmendia, M.; Villar, I.; Martinez-Berriotxoa, A.; Erdozain, J.-G.; Aguirre, C. Effect of antimalarials on thrombosis and survival in patients with systemic lupus erythematosus. Lupus 2006, 15, 577–583. [Google Scholar] [CrossRef]
- Kaiser, R.; Cleveland, C.M.; Criswell, L.A. Risk and protective factors for thrombosis in systemic lupus erythematosus: Results from a large, multi-ethnic cohort. Ann. Rheum. Dis. 2009, 68, 238–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wozniacka, A.; Lesiak, A.; Narbutt, J.; McCauliffe, D.P.; Sysa-Jedrzejowska, A. Chloroquine treatment influences proinflammatory cytokine levels in systemic lupus erythematosus patients. Lupus 2006, 15, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.; Kim, M.; Friedman, D.M.; Costedoat-Chalumeau, N.; Clancy, R.; Copel, J.A.; Phoon, C.K.; Cuneo, B.F.; Cohen, R.E.; Robins, K.; et al. Hydroxychloroquine to Prevent Recurrent Congenital Heart Block in Fetuses of Anti-SSA/Ro-Positive Mothers. J. Am. Coll. Cardiol. 2020, 76, 292–302. [Google Scholar] [CrossRef]
- A randomized trial of hydroxychloroquine in early rheumatoid arthritis: The HERA study. Am. J. Med. 1995, 98, 156–168. [CrossRef] [PubMed]
- Clark, P.; Casas, E.; Tugwell, P.; Medina, C.; Gheno, C.; Tenorio, G.; Orozco, J.A. Hydroxychloroquine Compared with Placebo in Rheumatoid Arthritis. A randomized controlled trial. Ann. Intern. Med. 1993, 119, 1067–1071. [Google Scholar] [CrossRef]
- Davis, M.J.; Dawes, P.T.; Fowler, P.D.; Clarke, S.; Fisher, J.; Shadforth, M.F. Should disease-modifying agents be used in mild rheumatoid arthritis? Rheumatology 1991, 30, 451–454. [Google Scholar] [CrossRef]
- Das, S.K.; Pareek, A.; Mathur, D.S.; Wanchu, A.; Srivastava, R.; Agarwal, G.; Chauhan, R.S. Efficacy and Safety of hydroxychloroquine sulphate in rheumatoid arthritis: A randomized, double-blind, placebo controlled clinical trial—An Indian experience. Curr. Med. Res. Opin. 2007, 23, 2227–2234. [Google Scholar] [CrossRef]
- Alam, M.K.; Sutradhar, S.R.; Pandit, H.; Ahmed, S.; Bhattacharjee, M.; Miah, A.H.; Bari, M.A.; Islam, M.Z.; Khan, N.A.; Zannat, K.F.; et al. Comparative study on methotrexate and hydroxychloroquine in the treatment of rheumatoid arthritis. Mymensingh Med. J. 2012, 21, 391–398. [Google Scholar]
- Gubar’, E.E.; Bochkova, A.G.; Bunchuk, N.V. Comparison of efficacy and tolerability of triple combination therapy (methotrexate + sulfasalazine + hydroxychloroquine) with methotrexate monotherapy in patients with rheumatoid ar-thritis. Ter. Arkhiv 2008, 80, 25–30. [Google Scholar]
- Kim, W.-U.; Seo, Y.-I.; Park, S.-H.; Lee, W.-K.; Lee, S.-K.; Paek, S.-I.; Cho, C.-S.; Song, H.-H.; Kim, H.-Y. Treatment with cyclosporin switching to hydroxychloroquine in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2001, 60, 514–517. [Google Scholar] [CrossRef] [Green Version]
- Moreland, L.W.; O’Dell, J.R.; Paulus, H.E.; Curtis, J.R.; Bathon, J.M.; St Clair, E.W.; Bridges, S.L., Jr.; Zhang, J.; McVie, T.; Howard, G.; et al. A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: The Treatment of Early Aggressive Rheumatoid Arthritis trial. Arthritis Rheum. 2012, 64, 2824–2835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Dell, J.R.; Mikuls, T.R.; Taylor, T.H.; Ahluwalia, V.; Brophy, M.; Warren, S.R.; Lew, R.A.; Cannella, A.C.; Kunkel, G.; Phibbs, C.S.; et al. Therapies for Active Rheumatoid Arthritis after Methotrexate Failure. N. Engl. J. Med. 2013, 369, 307–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, J.M.; Alvarez-Nemegyei, J.; Saavedra, M.A.; Terán, L.; Galván-Villegas, F.; García-Figueroa, J.; Jara, L.J.; Barile, L.; The GRECIA Group. A Randomized, Double-Blind, Multicenter, Controlled Clinical Trial of Cyclosporine Plus Chloroquine vs. Cyclosporine Plus Placebo in Early-Onset Rheumatoid Arthritis. Arch. Med. Res. 2004, 35, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kravvariti, E.; Koutsogianni, A.; Samoli, E.; Sfikakis, P.P.; Tektonidou, M.G. The effect of hydroxychloroquine on thrombosis prevention and antiphospholipid antibody levels in primary antiphospholipid syndrome: A pilot open label randomized prospective study. Autoimmun. Rev. 2020, 19, 102491. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Tanguy, A.; Voswinkel, J.; Henrion, D.; Subra, J.F.; Loufrani, L.; Rohmer, V.; Ifrah, N.; Belizna, C. Antithrombotic effects of hydroxychloroquine in primary antiphospholipid syndrome patients. J. Thromb. Haemost. 2013, 11, 1927–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tektonidou, M.G.; Laskari, K.; Panagiotakos, D.B.; Moutsopoulos, H.M. Risk factors for thrombosis and primary thrombosis prevention in patients with systemic lupus erythematosus with or without antiphospholipid antibodies. Arthritis Care Res. 2008, 61, 29–36. [Google Scholar] [CrossRef]
- Ruffati, A.; Tonello, M.; Hoxha, A.; Sciascia, S.; Cuadrado, M.J.; Latino, J.O.; Udry, S.; Reshetnyak, T.; Costedoat-Chalumeau, N.; Morel, N.; et al. Effect of Additional Treatments Combined with Conventional Therapies in Pregnant Patients with High-Risk Antiphospholipid Syndrome: A Multicentre Study. Thromb. Haemost. 2018, 118, 639–646. [Google Scholar] [CrossRef]
- Schreiber, K.; Breen, K.; Cohen, H.; Jacobsen, S.; Middeldorp, S.; Pavord, S.; Regan, L.; Roccatello, D.; Robinson, S.E.; Sciascia, S.; et al. HYdroxychloroquine to Improve Pregnancy Outcome in Women with AnTIphospholipid Antibodies (HYPATIA) Protocol: A Multinational Randomized Controlled Trial of Hydroxychloroquine versus Placebo in Addition to Standard Treatment in Pregnant Women with Antiphospholipid Syndrome or Antibodies. Semin. Thromb. Hemost. 2017, 43, 562–571. [Google Scholar] [CrossRef]
- Mekinian, A.; Vicaut, E.; Cohen, J.; Bornes, M.; Kayem, G.; Fain, O. Hydroxychloroquine to obtain pregnancy without adverse obstetrical events in primary antiphospholipid syndrome: French phase II multicenter randomized trial, HYDROSAPL. Gynecol. Obstet. Fertil. Senol. 2018, 46, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Chrisman, O.; Snook, G.; Wilson, T.; Short, J. Prevention of venous thromboembolism by administration of hydroxychloroquine. A preliminary report. J. Bone Jt. Surg. Am. 1976, 58, 918–920. [Google Scholar] [CrossRef]
- Carter, A.E.; Eban, R. Prevention of Postoperative Deep Venous Thrombosis in Legs by Orally administered Hydroxychloroquine Sulphate. BMJ 1974, 3, 94–95. [Google Scholar] [CrossRef] [Green Version]
- Hansen, E.; Jessing, P.; Lindewald, H.; Ostergaard, P.; Olesen, T.; Malver, E. Hydroxychloroquine sulphate in prevention of deep venous thrombosis following fracture of the hip, pelvis, or thoracolumbar spine. J. Bone Jt. Surg. Am. 1976, 58, 1089–1093. [Google Scholar] [CrossRef]
- Cooke, E.D.; Dawson, M.H.; Ibbotson, R.M.; Bowcock, S.A.; Ainsworth, M.E.; Pilcher, M.F. Failure of orally administered hydroxychloroquine sulphate to prevent venous thromboembolism fol-lowing elective hip operations. J. Bone Jt. Surg. Am. 1977, 59, 496–500. [Google Scholar] [CrossRef]
- Johansson, E.; Forsberg, K.; Johnsson, H. Clinical and Experimental Evaluation of the Thromboprophylactic Effect of Hydroxychloroquine Sulfate after Total Hip Replacement. Pathophysiol. Haemost. Thromb. 1981, 10, 89–96. [Google Scholar] [CrossRef]
- Boone, B.A.; Murthy, P.; Miller-Ocuin, J.; Doerfler, W.R.; Ellis, J.T.; Liang, X.; Ross, M.A.; Wallace, C.T.; Sperry, J.L.; Lotze, M.T.; et al. Chloroquine reduces hypercoagulability in pancreatic cancer through inhibition of neutrophil extracellular traps. BMC Cancer 2018, 18, 678. [Google Scholar] [CrossRef] [Green Version]
- Munro, R.; Morrison, E.; McDonald, A.G.; Hunter, J.A.; Madhok, R.; Capell, H.A. Effect of disease modifying agents on the lipid profiles of patients with rheumatoid arthritis. Ann. Rheum. Dis. 1997, 56, 374–377. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.J.; Metzger, A.L.; Stecher, V.J.; Turnbull, B.A.; Kern, P.A. Cholesterol-lowering effect of hydroxychloroquine in patients with rheumatic disease: Reversal of deleterious effects of steroids on lipids. Am. J. Med. 1990, 89, 322–326. [Google Scholar] [CrossRef]
- Mercado, M.V.-D.; Muñoz-Valle, J.F.; Santos, A.; Bernard-Medina, A.G.; Martínez-Bonilla, G.; Paczka, J.A.; Ruiz-García, H.; Orozco-Alcalá, J.; Orozco-Barocio, G.; Quezada-Arellano, D.; et al. Evaluation of lipid profile, macular toxicity and clinical manifestations according to APO E genotype in systemic lupus erythematosus and rheumatoid arthritis patients treated with chloroquine. Scand. J. Rheumatol. 2002, 31, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Garg, R.; Lu, B.; Todd, D.J.; Mercer, E.; Norton, T.; Massarotti, E. Effect of Hydroxychloroquine on Insulin Sensitivity and Lipid Parameters in Rheumatoid Arthritis Patients Without Diabetes Mellitus: A Randomized, Blinded Crossover Trial. Arthritis Care Res. 2014, 66, 1246–1251. [Google Scholar] [CrossRef] [Green Version]
- Araiza-Casillas, R.; Díaz-Molina, R.; González-Ortiz, M.; Robinson-Navarro, O.M. Efecto de la hidroxicloroquina sobre la sensibilidad a la insulina y el perfil de lípidos en pacientes con artritis reumatoide. Rev. Méd. Chile 2013, 141, 1019–1025. [Google Scholar] [CrossRef] [Green Version]
- Pareek, A.; Chandurkar, N.; Thulaseedharan, N.K.; Legha, R.; Agarwal, M.; Mathur, S.L.; Salkar, H.R.; Pednekar, S.; Pai, V.; Sriram, U.; et al. Efficacy and safety of fixed dose combination of atorvastatin and hydroxychloroquine: A randomized, double-blind comparison with atorvastatin alone among Indian patients with dyslipidemia. Curr. Med. Res. Opin. 2015, 31, 2105–2117. [Google Scholar] [CrossRef] [PubMed]
- Hartman, O.; Kovanen, P.T.; Lehtonen, J.; Eklund, K.K.; Sinisalo, J. Hydroxychloroquine for the prevention of recurrent cardiovascular events in myocardial infarction patients: Rationale and design of the OXI trial. Eur. Heart J. Cardiovasc. Pharmacother. 2016, 3, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Bartekova, M.; Radosinska, J.; Jelemensky, M.; Dhalla, N.S. Role of cytokines and inflammation in heart function during health and disease. Heart Fail. Rev. 2018, 23, 733–758. [Google Scholar] [CrossRef] [PubMed]
- Ulander, L.; Tolppanen, H.; Hartman, O.; Rissanen, T.T.; Paakkanen, R.; Kuusisto, J.; Anttonen, O.; Nieminen, T.; Yrjölä, J.; Ryysy, R.; et al. Hydroxychloroquine reduces interleukin-6 levels after myocardial infarction: The randomized, double-blind, placebo-controlled OXI pilot trial. Int. J. Cardiol. 2021, 337, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Wasko, M.C.M.; Hubert, H.B.; Lingala, V.B.; Elliott, J.R.; Luggen, M.E.; Fries, J.F.; Ward, M.M. Hydroxychloroquine and Risk of Diabetes in Patients with Rheumatoid Arthritis. JAMA 2007, 298, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasko, M.C.M.; McClure, C.K.; Kelsey, S.F.; Huber, K.; Orchard, T.; Toledo, F.G.S. Antidiabetogenic effects of hydroxychloroquine on insulin sensitivity and beta cell function: A randomised trial. Diabetologia 2015, 58, 2336–2343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pareek, A.; Chandurkar, N.; Thomas, N.; Viswanathan, V.; Deshpande, A.; Gupta, O.P.; Shah, A.; Kakrani, A.; Bhandari, S.; Thulasidharan, N.K.; et al. Efficacy and safety of hydroxychloroquine in the treatment of type 2 diabetes mellitus: A double blind, randomized comparison with pioglitazone. Curr. Med. Res. Opin. 2014, 30, 1257–1266, Erratum in Curr. Med. Res. Opin. 2015, 31, 1087–1092. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Thorpe, K.E.; Taylor, D.W.; Haynes, R.B. The effectiveness of hydroxychloroquine in patients with type 2 diabetes mellitus who are refractory to sulfonylureas—A randomized trial. Diabetes Res. Clin. Pract. 2002, 55, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Toledo, F.G.S.; Miller, R.G.; Helbling, N.L.; Zhang, Y.; DeLany, J.P. The effects of hydroxychloroquine on insulin sensitivity, insulin clearance and inflammation in insulin-resistant adults: A randomized trial. Diabetes Obes. Metab. 2021, 23, 1252–1261. [Google Scholar] [CrossRef]
- Briceño, E.; Reyes, S.; Sotelo, J. Therapy of glioblastoma multiforme improved by the antimutagenic chloroquine. Neurosurg. Focus 2003, 14, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sotelo, J.; Briceño, E.; Lόpez-González, M.A. Adding Chloroquine to Conventional Treatment for Glioblastoma Multiforme: A randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 2006, 144, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, M.R.; Ye, X.; Supko, J.G.; Desideri, S.; Grossman, S.A.; Brem, S.; Mikkelson, T.; Wang, D.; Chang, Y.C.; Hu, J.; et al. A phase I/II trial of hydroxychloroquine in conjunction with radiation therapy and concurrent and adjuvant temozolomide in patients with newly diagnosed glioblastoma multiforme. Autophagy 2014, 10, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- Wolpin, B.M.; Rubinson, D.A.; Wang, X.; Chan, J.A.; Cleary, J.M.; Enzinger, P.C.; Fuchs, C.S.; McCleary, N.J.; Meyerhardt, J.A.; Ng, K.; et al. Phase II and Pharmacodynamic Study of Autophagy Inhibition Using Hydroxychloroquine in Patients with Metastatic Pancreatic Adenocarcinoma. Oncologist 2014, 19, 637–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boone, B.; Bahary, N.; Zureikat, A.H.; Moser, A.J.; Normolle, D.P.; Wu, W.-C.; Singhi, A.D.; Bao, P.; Bartlett, D.L.; Liotta, L.A.; et al. Safety and Biologic Response of Pre-operative Autophagy Inhibition in Combination with Gemcitabine in Patients with Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 4402–4410. [Google Scholar] [CrossRef] [PubMed]
- Zeh, H.J.; Bahary, N.; Boone, B.A.; Singhi, A.D.; Miller-Ocuin, J.L.; Normolle, D.P.; Zureikat, A.H.; Hogg, M.E.; Bartlett, D.L.; Lee, K.K.; et al. A Randomized Phase II Preoperative Study of Autophagy Inhibition with High-Dose Hydroxychloroquine and Gemcitabine/Nab-Paclitaxel in Pancreatic Cancer Patients. Clin. Cancer Res. 2020, 26, 3126–3134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasic, T.B.; O’Hara, M.H.; Loaiza-Bonilla, A.; Reiss, K.A.; Teitelbaum, U.R.; Borazanci, E.; De Jesus-Acosta, A.; Redlinger, C.; Burrell, J.A.; Laheru, D.A.; et al. Effect of Gemcitabine and nab-Paclitaxel with or Without Hydroxychloroquine on Patients with Advanced Pancreatic Cancer. JAMA Oncol. 2019, 5, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Supko, J.G.; Neal, J.W.; Muzikansky, A.; Digumarthy, S.; Fidias, P.; Temel, J.S.; Heist, R.S.; Shaw, A.T.; McCarthy, P.O.; et al. A Phase I Study of Erlotinib and Hydroxychloroquine in Advanced Non–Small-Cell Lung Cancer. J. Thorac. Oncol. 2012, 7, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Arnaout, A.; Robertson, S.J.; Pond, G.R.; Lee, H.; Jeong, A.; Ianni, L.; Kroeger, L.; Hilton, J.; Coupland, S.; Gottlieb, C.; et al. A randomized, double-blind, window of opportunity trial evaluating the effects of chloroquine in breast cancer patients. Breast Cancer Res. Treat. 2019, 178, 327–335. [Google Scholar] [CrossRef]
- Vogl, D.T.; Stadtmauer, E.A.; Tan, K.-S.; Heitjan, D.F.; Davis, L.E.; Pontiggia, L.; Rangwala, R.; Piao, S.; Chang, Y.C.; Scott, E.C.; et al. Combined autophagy and proteasome inhibition: A phase 1 trial of hydroxychloroquine and bortezomib in patients with relapsed/refractory myeloma. Autophagy 2014, 10, 1380–1390. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.; Tan, X. Current Strategies of Antiviral Drug Discovery for COVID-19. Front. Mol. Biosci. 2021, 8, 671263. [Google Scholar] [CrossRef]
- Asai, A.; Konno, M.; Ozaki, M.; Otsuka, C.; Vecchione, A.; Arai, T.; Kitagawa, T.; Ofusa, K.; Yabumoto, M.; Hirotsu, T.; et al. COVID-19 Drug Discovery Using Intensive Approaches. Int. J. Mol. Sci. 2020, 21, 2839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, G.; Joshi, J.; Mandal, R.S.; Shrivastava, N.; Virmani, R.; Sethi, T. Artificial Intelligence in Surveillance, Diagnosis, Drug Discovery and Vaccine Development against COVID-19. Pathogens 2021, 10, 1048. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-P.; Lin, Y.-C.; Chen, T.-C.; Tseng, T.-Y.; Wong, H.-L.; Kuo, C.-Y.; Lin, W.-P.; Huang, S.-R.; Wang, W.-Y.; Liao, J.-H.; et al. A multicenter, randomized, open-label, controlled trial to evaluate the efficacy and tolerability of hydroxychloroquine and a retrospective study in adult patients with mild to moderate coronavirus disease 2019 (COVID-19). PLoS ONE 2020, 15, e0242763. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Semler, M.W.; Leither, L.M.; Casey, J.D.; Angus, D.C.; Brower, R.G.; Chang, S.Y.; Collins, S.P.; Eppensteiner, J.C.; Filbin, M.R.; et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients with COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.; Kilgore, P.; Chaudhry, Z.S.; Jacobsen, G.; Wang, D.D.; Huitsing, K.; Brar, I.; Alangaden, G.J.; Ramesh, M.S.; McKinnon, J.E.; et al. Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. Int. J. Infect. Dis. 2020, 97, 396–403. [Google Scholar] [CrossRef]
- McCullough, P.A.; Kelly, R.J.; Ruocco, G.; Lerma, E.; Tumlin, J.; Wheelan, K.R.; Katz, N.; Lepor, N.E.; Vijay, K.; Carter, H.; et al. Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection. Am. J. Med. 2021, 134, 16–22. [Google Scholar] [CrossRef]
- Mikami, T.; Miyashita, H.; Yamada, T.; Harrington, M.; Steinberg, D.; Dunn, A.; Siau, E. Risk Factors for Mortality in Patients with COVID-19 in New York City. J. Gen. Intern. Med. 2021, 36, 17–26. [Google Scholar] [CrossRef]
- Mitjà, O.; Corbacho-Monné, M.; Ubals, M.; Alemany, A.; Suñer, C.; Tebé, C.; Tobias, A.; Peñafiel, J.; Ballana, E.; Pérez, C.A.; et al. A Cluster-Randomized Trial of Hydroxychloroquine for Prevention of Covid-19. N. Engl. J. Med. 2021, 384, 417–427. [Google Scholar] [CrossRef]
- Abella, B.S.; Jolkovsky, E.L.; Biney, B.T.; Uspal, J.E.; Hyman, M.C.; Frank, I.; Hensley, S.E.; Gill, S.; Vogl, D.T.; Maillard, I.; et al. Efficacy and Safety of Hydroxychloroquine vs Placebo for Pre-exposure SARS-CoV-2 Prophylaxis Among Health Care Workers. JAMA Intern. Med. 2021, 181, 195. [Google Scholar] [CrossRef]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Barnabas, M.R.V.; Brown, S.E.R.; Bershteyn, A.; Karita, H.C.S.; Johnston, C.; Thorpe, L.E.; Kottkamp, A.; Neuzil, K.M.; Laufer, M.K.; Deming, M.; et al. Hydroxychloroquine as Postexposure Prophylaxis to Prevent Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Randomized Trial. Ann. Intern. Med. 2021, 174, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Rajasingham, R.; Bangdiwala, A.S.; Nicol, M.R.; Skipper, C.P.; Pastick, K.A.; Axelrod, M.L.; Pullen, M.F.; Nascene, A.A.; Williams, D.A.; Engen, N.W.; et al. Hydroxychloroquine as Pre-exposure Prophylaxis for Coronavirus Disease 2019 (COVID-19) in Healthcare Workers: A Randomized Trial. Clin. Infect. Dis. 2021, 72, e835–e843. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.; Boesen, M.E.; Cerchiaro, G.; Doram, C.; Edwards, B.D.; Ganesh, A.; Greenfield, J.; Jamieson, S.; Karnik, V.; Kenney, C.; et al. Assessing the efficacy and safety of hydroxychloroquine as outpatient treatment of COVID-19: A randomized controlled trial. CMAJ Open 2021, 9, E693–E702. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- Piconi, S.; Parisotto, S.; Rizzardini, G.; Passerini, S.; Terzi, R.; Argenteri, B.; Meraviglia, P.; Capetti, A.; Biasin, M.; Trabattoni, D.; et al. Hydroxychloroquine drastically reduces immune activation in HIV-infected, antiretroviral therapy–treated immunologic nonresponders. Blood 2011, 118, 3263–3272. [Google Scholar] [CrossRef] [Green Version]
- Routy, J.-P.; Angel, J.; Patel, M.; Kanagaratham, C.; Radzioch, D.; Kema, I.; Gilmore, N.; Ancuta, P.; Singer, J.; Jenabian, M.-A. Assessment of chloroquine as a modulator of immune activation to improve CD4 recovery in immune nonresponding HIV-infected patients receiving antiretroviral therapy. HIV Med. 2015, 16, 48–56. [Google Scholar] [CrossRef]
- Paton, N.I.; Goodall, R.; Dunn, D.T.; Franzen, S.; Collaco-Moraes, Y.; Gazzard, B.G.; Williams, I.G.; Fisher, M.J.; Winston, A.; Fox, J.; et al. Effects of Hydroxychloroquine on Immune Activation and Disease Progression Among HIV-Infected Patients Not Receiving Antiretroviral Therapy: A randomized controlled trial. JAMA 2012, 308, 353–361. [Google Scholar] [CrossRef]
- Chauhan, A.; Tikoo, A. The enigma of the clandestine association between chloroquine and HIV-1 infection. HIV Med. 2015, 16, 585–590. [Google Scholar] [CrossRef]
- Delvecchio, R.; Higa, L.M.; Pezzuto, P.; Valadão, A.L.; Garcez, P.P.; Monteiro, F.L.; Loiola, E.C.; Dias, A.A.; Silva, F.J.; Aliota, M.T.; et al. Chloroquine, an Endocytosis Blocking Agent, Inhibits Zika Virus Infection in Different Cell Models. Viruses 2016, 8, 322. [Google Scholar] [CrossRef] [Green Version]
- Shiryaev, S.A.; Mesci, P.; Pinto, A.; Fernandes, I.; Sheets, N.; Shresta, S.; Farhy, C.; Huang, C.-T.; Strongin, A.Y.; Muotri, A.R.; et al. Repurposing of the anti-malaria drug chloroquine for Zika Virus treatment and prophylaxis. Sci. Rep. 2017, 7, 15771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smit, J.M.; Moesker, B.; Rodenhuis-Zybert, I.; Wilschut, J. Flavivirus Cell Entry and Membrane Fusion. Viruses 2011, 3, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Bari, A.A. Targeting endosomal acidification by chloroquine analogs as a promising strategy for the treatment of emerging viral diseases. Pharmacol. Res. Perspect. 2017, 5, e00293. [Google Scholar] [CrossRef] [PubMed]
- Pellicelli, A.M.; Morrone, A.; Barbieri, L.; Andreoli, A. Porphyria cutanea tarda in an HCV-positive liver transplant patient: A case report. Ann. Hepatol. 2012, 11, 951–954. [Google Scholar] [CrossRef] [PubMed]
- Vausselin, T.; Calland, N.; Belouzard, S.; Descamps, V.; Douam, F.; Helle, F.; François, C.; Lavillette, D.; Duverlie, G.; Wahid, A.; et al. The antimalarial ferroquine is an inhibitor of hepatitis C virus. Hepatology 2013, 58, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.A.; Vilela, V.S.; Cataldo, M.J.; Ramos, R.C.; Duarte, J.L.; Tura, B.R.; Albuquerque, E.M.; Jesús, N.R. Hydroxychloroquine (HCQ) in lupus pregnancy: Double-blind and placebo-controlled study. Lupus 2001, 10, 401–404. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemann, B.; Puleo, A.; Stout, C.; Markel, J.; Boone, B.A. Biologic Functions of Hydroxychloroquine in Disease: From COVID-19 to Cancer. Pharmaceutics 2022, 14, 2551. https://doi.org/10.3390/pharmaceutics14122551
Niemann B, Puleo A, Stout C, Markel J, Boone BA. Biologic Functions of Hydroxychloroquine in Disease: From COVID-19 to Cancer. Pharmaceutics. 2022; 14(12):2551. https://doi.org/10.3390/pharmaceutics14122551
Chicago/Turabian StyleNiemann, Britney, Amanda Puleo, Conley Stout, Justin Markel, and Brian A. Boone. 2022. "Biologic Functions of Hydroxychloroquine in Disease: From COVID-19 to Cancer" Pharmaceutics 14, no. 12: 2551. https://doi.org/10.3390/pharmaceutics14122551