
Probing Pharmaceutical Strategies to Promote the Skin Delivery of Asiatic Acid from Hydrogels: Enhancement Effects of Organic Amine Counterions, Chemical Enhancers, and Microneedle Pretreatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Solubility of AA in Different Solvents
2.3. Preparation of AA-Loaded Hydrogels
2.4. Drug Release Experiments
2.5. Skin Penetration Experiments
2.6. Extraction of the Drug from Skin
2.7. HPLC Analysis of AA
2.8. Determination of Rheological Properties
2.9. Scanning Electron Microscope (SEM) Analyses
2.10. Nuclear Magnetic Resonance Spectroscopy (NMR) Analyses
2.11. Histological Study of the Microneedle-Treated Skin
2.12. Statistical Analysis
3. Results and Discussion
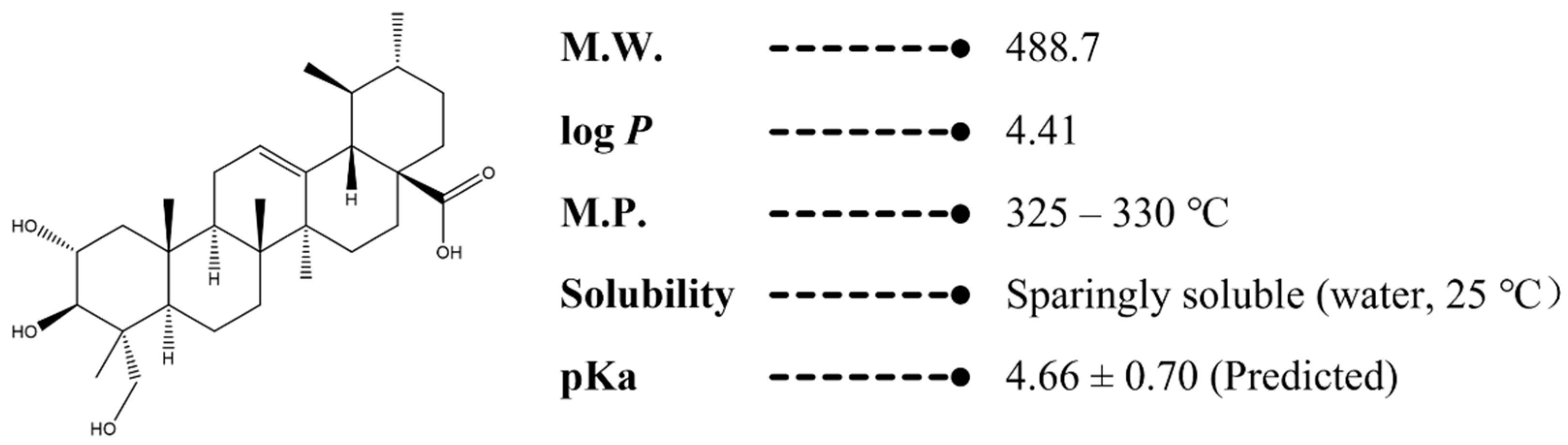
3.1. Solubility of AA in Different Solvents
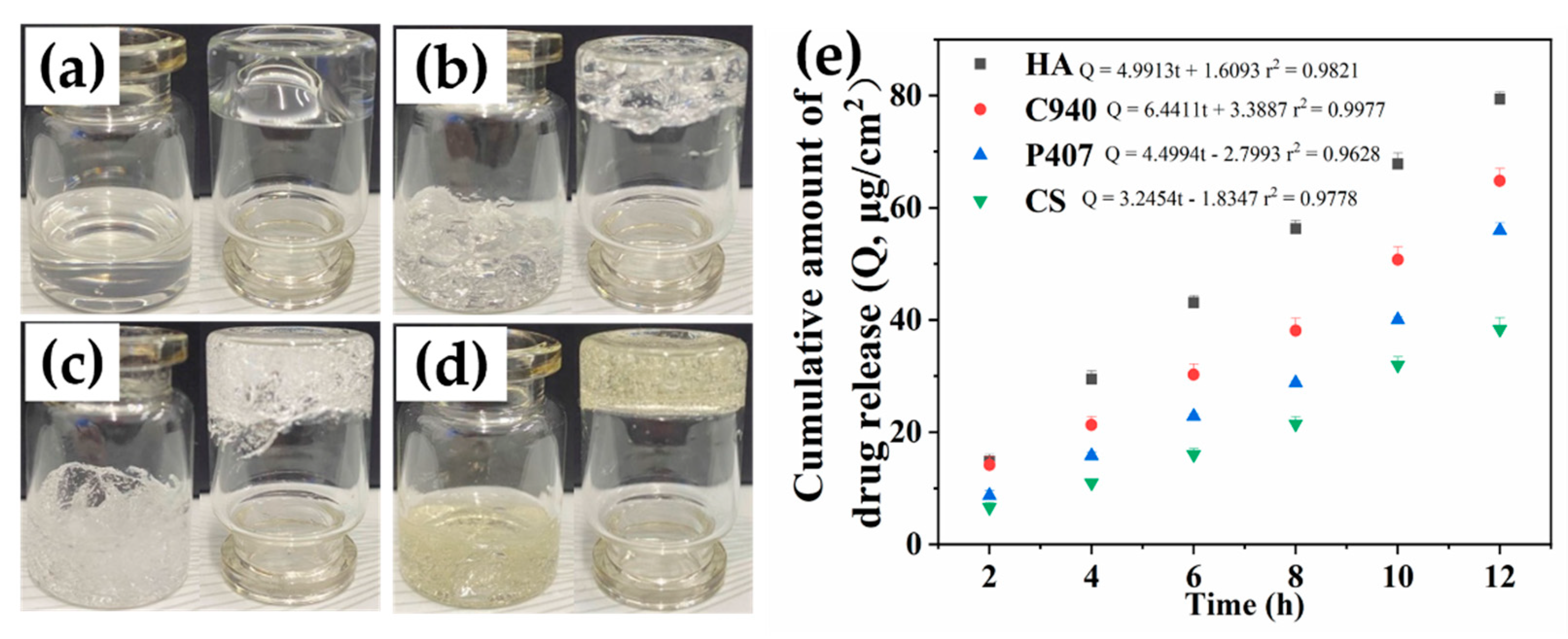
3.2. Effect of Different Base Types on the Release of AA Hydrogels
3.3. Optimization of the Content of HA and AA in the Hydrogels
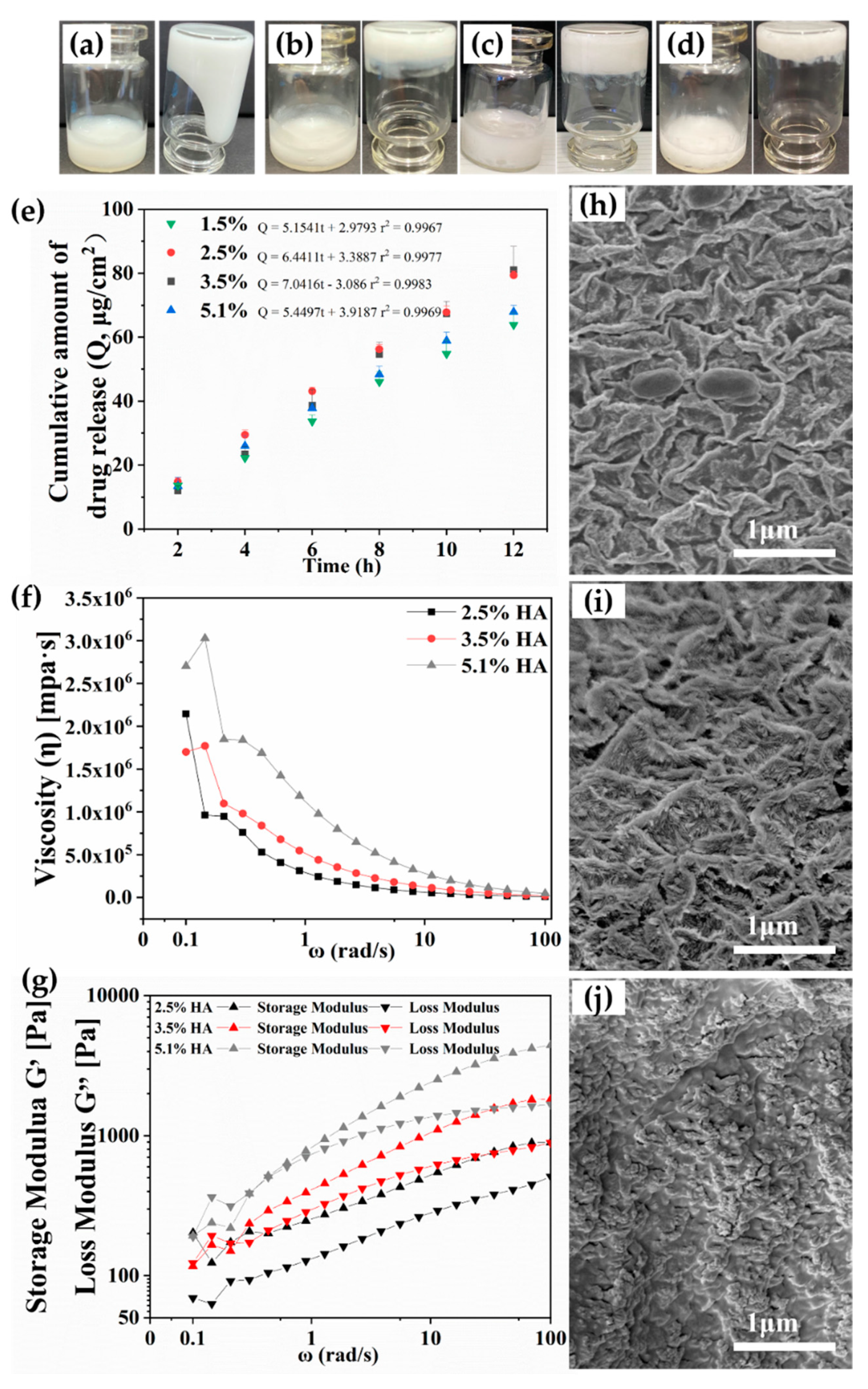
3.3.1. HA Content
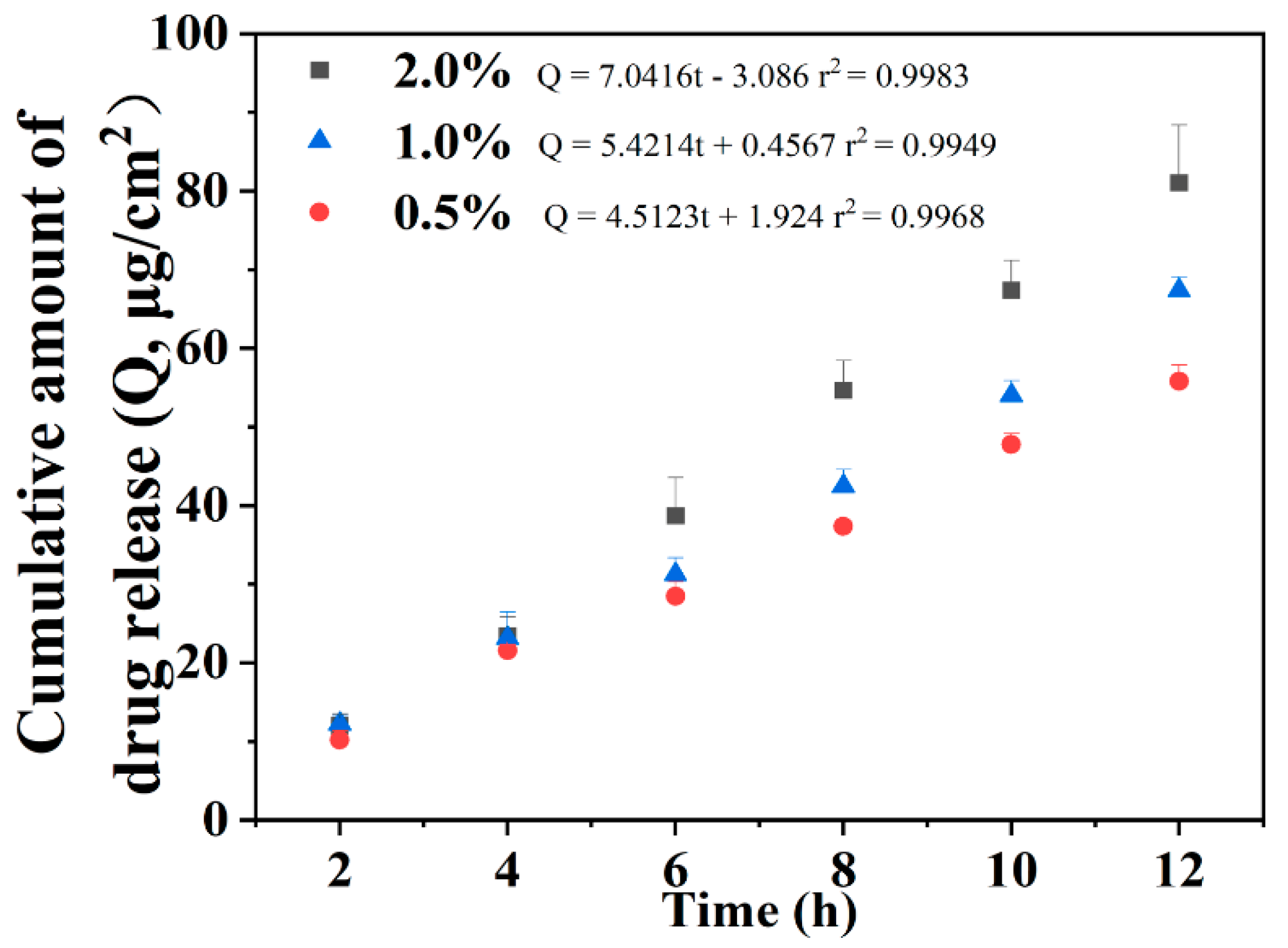
3.3.2. AA Content
3.4. Penetration of AA from Hydrogels into the Skin
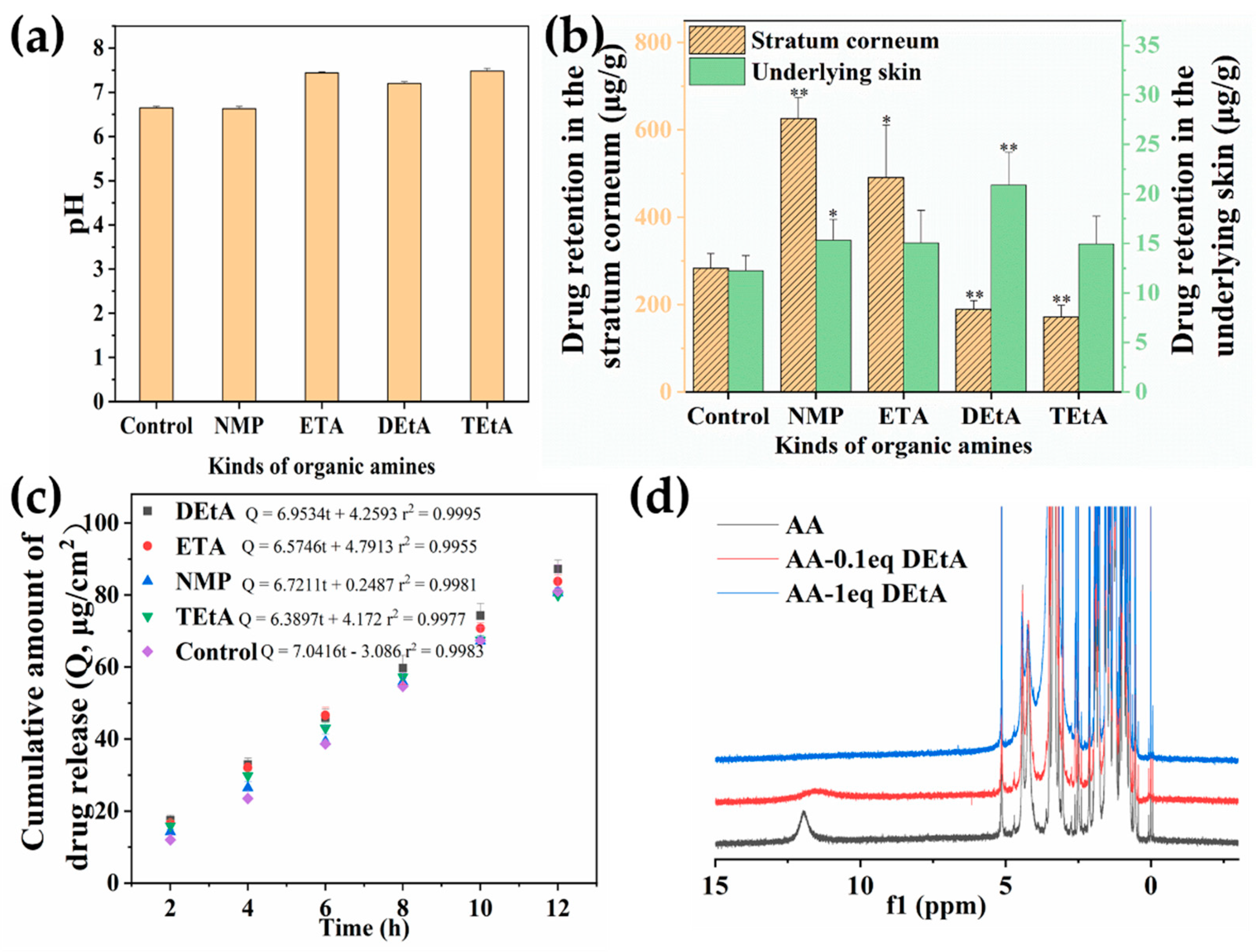
3.4.1. Effects of Organic Amine Counterions
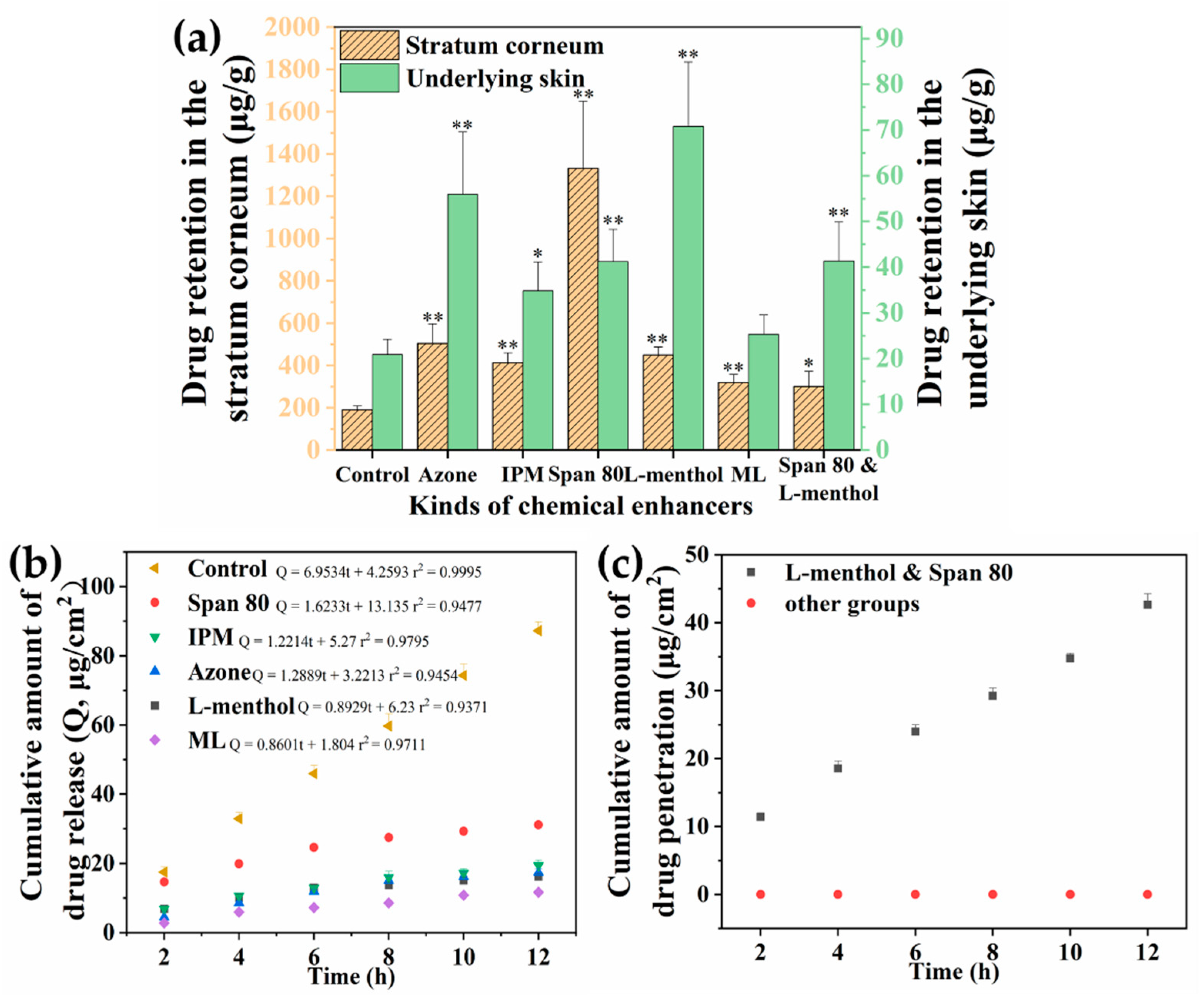
3.4.2. Effects of Chemical Enhancers
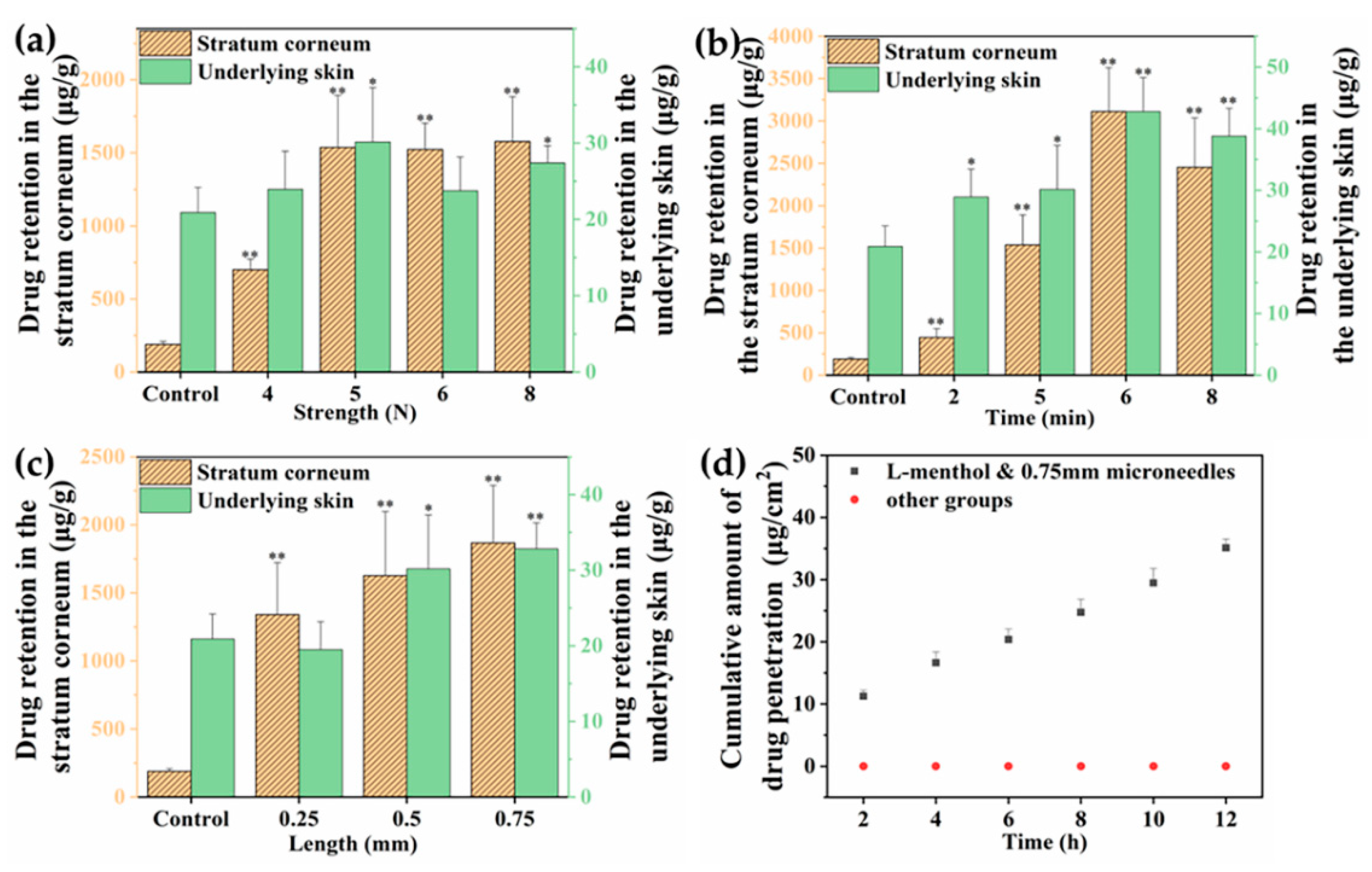
3.4.3. Effects of Microneedle Pretreatment
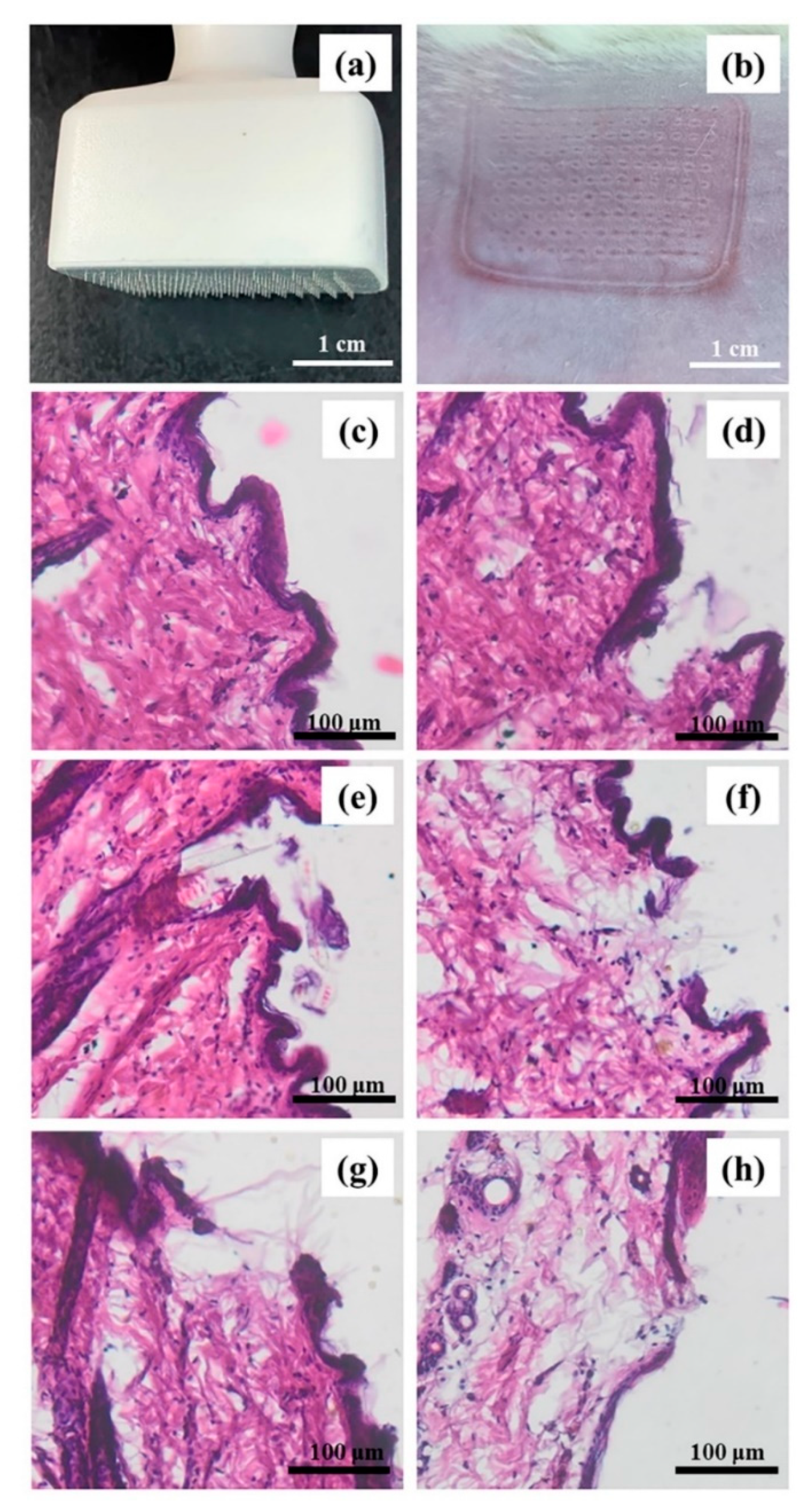
3.5. Histological Study of the Microneedle-Treated Skin
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Razali, N.N.M.; Ng, C.T.; Fong, L.Y. Cardovascular Protective Effects of Centella asiatica and Its Triterpenes: A Review. Planta Med. 2019, 85, 1203–1215. [Google Scholar]
- Meeran, M.F.N.; Goyal, S.N.; Suchal, K.; Sharma, C.; Patil, C.R.; Ojha, S.K. Pharmacological Properties, Molecular Mechanisms, and Pharmaceutical Development of Asiatic Acid: A Pentacyclic Triterpenoid of Therapeutic Promise. Front. Pharmacol. 2018, 9, 892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.S. Pharmacological Effects of Centella asiatica on Skin Diseases: Evidence and Possible Mechanisms. Evid. Based Complement. Altern. Med. 2021, 2021, 5462633. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Sharma, A.; Zhang, T.; Wu, Y.; Ding, X. Pharmacological Review on Asiatic Acid and Its Derivatives: A Potential Compound. SLAS Technol. 2018, 23, 111–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somboonwong, J.; Kankaisre, M.; Tantisira, B.; Tantisira, M.H. Wound healing activities of different extracts of Centella asiatica in incision and burn wound models: An experimental animal study. BMC Complement. Altern. Med. 2012, 20, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukula, O.; Kirmizikan, S.; Tiryaki, E.S.; Cicekli, M.N.; Gunaydin, G. Asiatic acid exerts an anti-psoriatic effect in the imiquimod-induced psoriasis model in mice. Immunopharmacol. Immunotoxicol. 2022, 44, 367–372. [Google Scholar] [CrossRef]
- Lee, Y.S.; Jin, D.-Q.; Beak, S.-M.; Lee, E.-S.; Kim, J.-A. Inhibition of ultraviolet-A-modulated signaling pathways by asiatic acid and ursolic acid in HaCaT human keratinocytes. Eur. J. Pharmacol. 2003, 476, 173–178. [Google Scholar]
- Park, B.C.; Bosire, K.O.; Lee, E.-S.; Lee, Y.S.; Kim, J.-A. Asiatic acid induces apoptosis in SK-MEL-2 human melanoma cells. Cancer Lett. 2005, 218, 81–90. [Google Scholar] [CrossRef]
- Anantrao, J.H.; Nath, P.A.; Nivrutti, P.R. Drug Penetration Enhancement Techniques in Transdermal Drug Delivery System: A Review. J. Pharm. Res. Int. 2021, 33, 46–61. [Google Scholar] [CrossRef]
- Chen, Y.; Feng, X.; Meng, S. Site-specific drug delivery in the skin for the localized treatment of skin diseases. Expert Opin. Drug Deli. 2019, 16, 847–867. [Google Scholar] [CrossRef]
- Alkilani, A.Z.; Nasereddin, J.; Hamed, R.; Nimrawi, S.; Hussein, G.; Abo-Zour, H.; Donnelly, R.F. Beneath the skin: A Review of Current Trends and Future Prospects of Transdermal Drug Delivery Systems. Pharmaceutics 2022, 14, 1152. [Google Scholar] [CrossRef] [PubMed]
- Hui, M.; Quan, P.; Yang, Y.; Fang, L. The effect of ion-pair formation combined with penetration enhancers on the skin permeation of loxoprofen. Drug Deliv. 2016, 23, 5. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.C.; Barry, B.W. Penetration enhancers. Adv. Drug Deliv. Rev. 2012, 64, 128–137. [Google Scholar] [CrossRef]
- Shin, C.I.; Kim, M.; Kim, Y. Delivery of Niacinamide to the Skin Using Microneedle-Like Particles. Pharmaceutics 2019, 11, 326. [Google Scholar] [CrossRef] [Green Version]
- Opatha, S.A.T.; Titapiwatanakun, V.; Boonpisutiinant, K.; Chutoprapat, R. Preparation, Characterization and Permeation Study of Topical Gel Loaded with Transfersomes Containing Asiatic Acid. Molecules 2022, 27, 4865. [Google Scholar] [CrossRef] [PubMed]
- Kesharwani, P.; Bisht, A.; Alexander, A.; Dave, V.; Sharma, S. Biomedical applications of hydrogels in drug delivery system: An update. J. Drug Deliv. Sci. Technol. 2021, 66, 102914. [Google Scholar] [CrossRef]
- Ahsan, A.; Tian, W.-X.; Farooq, M.A.; Khan, D.H. An overview of hydrogels and their role in transdermal drug delivery. Int. J. Polym. Mater. Polym. Biomater. 2020, 70, 574–584. [Google Scholar] [CrossRef]
- Croisfelt, F.M.; Tundisi, L.L.; Ataide, J.A. Modified-release topical hydrogels: A ten-year review. J. Mater. Sci. 2019, 54, 10963–10983. [Google Scholar] [CrossRef]
- Ullah, A.; Lim, S.I. Bioinspired tunable hydrogels: An update on methods of preparation, classification, and biomedical and therapeutic applications. Int. J. Pharm. 2022, 612, 121268. [Google Scholar] [CrossRef]
- Lai, W.-F.; Rogach, A. Hydrogel-Based Materials for Delivery of Herbal Medicines. ACS Appl. Mater. Interfaces 2017, 9, 11309–11320. [Google Scholar] [CrossRef]
- Tavakoli, S.; Klar, A.S. Advanced Hydrogels as Wound Dressings. Biomolecules 2020, 10, 1169. [Google Scholar] [CrossRef] [PubMed]
- Wróblewska, M.; Słyż, J.; Winnicka, K. Rheological and textural properties of hydrogels, containing sulfur as a model drug, made using different polymers types. Polimery 2019, 64, 208–215. [Google Scholar] [CrossRef]
- Lacroce, E.; Rossi, F. Polymer-based thermoresponsive hydrogels for controlled drug delivery. Expert Opin. Drug Deliv. 2022, 19, 1203–1215. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Mitsui, N.; Hasegawa, T.; Sugibayashi, K.; Morimoto, Y. Potential usefulness of solubility index for prediction of the skin permeation rate of 5-ISMN from pressure-sensitive adhesive tape. J. Control Release 2021, 73, 269–277. [Google Scholar]
- Biondo, N.E.; Argenta, D.F.; Rauber, G.S.; Caon, T. How to define the experimental conditions of skin permeation assays for drugs presenting biopharmaceutical limitations? The experience with testosterone. Int. J. Pharm. 2021, 607, 120987. [Google Scholar] [CrossRef]
- Cilurzo, F.; Musazzi, U.M.; Franzé, S.; Fedele, G.; Minghetti, P. Design of in vitro skin permeation studies according to the EMA guideline on quality of transdermal patches. Eur. J. Pharm. Sci. 2018, 125, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Djekic, L.; Martinović, M.; Dobričić, V.; Čalija, B.; Medarević, Đ.; Primorac, M. Comparison of the Effect of Bioadhesive Polymers on Stability and Drug Release Kinetics of Biocompatible Hydrogels for Topical Application of Ibuprofen. J. Pharm. Sci. 2019, 108, 1326–1333. [Google Scholar] [CrossRef]
- Tiwari, S.; Bahadur, P. Modified hyaluronic acid based materials for biomedical applications. Int. J. Biol. Macromol. 2019, 121, 556–571. [Google Scholar] [CrossRef]
- Zhang, F.; Lubach, J.; Na, W.; Momin, S. Interpolymer Complexation Between Polyox and Carbopl, and Its Effect on Drug Release from Matrix Tablets. J. Pharm. Sci. 2016, 105, 2386–2396. [Google Scholar] [CrossRef]
- Abdeltawab, H.; Svirskis, D.; Sharma, M. Formulation strategies to modulate drug release from poloxamer based in suit gelling systems. Expert Opin. Drug Deliv. 2020, 17, 495–509. [Google Scholar] [CrossRef]
- Zhu, J.; Tang, X.; Jia, Y.; Ho, C.-T.; Huang, Q. Applications and delivery mechanisms of hyaluronic acid used for topical/transdermal delivery—A review. Int. J. Pharm. 2020, 578, 19127. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, J.; Xiong, Y.; Wu, Y.; Yang, F.; Guo, Y.; Chen, Z.; Gao, L.; Deng, W. Ultrashort Peptides and Hyaluronic Acid-Based Injectable Composite Hydrogels for Sustained Drug Release and Chronic Diabetic Wound Healing. ACS Appl. Mater. Interfaces 2021, 13, 58329–58339. [Google Scholar] [CrossRef] [PubMed]
- Bao, Z.; Xian, C.; Yuan, Q.; Liu, G.; Wu, J. Natural Polymer-Based Hydrogels with Enhanced Mechanical Performances: Preparation, Structure, and Property. Adv. Healthc. Mater. 2019, 8, e1900670. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Jha, k.A.; Harrington, A.D.; Carson, M.C.F.; Jia, X. Hyaluronic Acid-Based Hydrogels: From a Natural Polysaccharide to Complex Networks. Soft Matter. 2012, 8, 3280–3294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombino, S.; Servidio, C.; Curcio, F.; Cassano, R. Strategies for Hyaluronic Acid-Based Hydrogel Design in Drug Delivery. Pharmaceutics 2019, 11, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Li, X.; He, K.; Sheng, X.; Deng, S.; Shen, Y.; Chang, G.; Ye, X. Preparation and properties of redox responsive modified hyaluronic acid hydrogels for drug release. Polym. Adv. Technol. 2017, 28, 1759–1763. [Google Scholar] [CrossRef]
- Sivasankaran, S.; Jonnalagadda, S. Levonorgestrel loaded biodegradable microparticles for injectable contraception: Preparation, characterization and modelling of drug release. Int. J. Pharm. 2022, 624, 121994. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Mano, Y.; Terasaka, S.; Sakurai, T.; Furuya, A.; Urano, H.; Sugibayashi, K. Usefulness of Rat Skin as a Substitute for Human Skin in the in Vitro Skin Permeation Study. Exp. Anim. 2011, 60, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Cilurzo, F.; Minghetti, P.; Alberti, E.; Gennari, C.G.M.; Pallavicini, M.; Valoti, E.; Montanari, L. An Investigation into the Influence of Counterion on the RS-Propranolol and S-Propranolol Skin Permeability. J. Pharm. Sci. 2010, 99, 1217–1224. [Google Scholar] [CrossRef]
- Geng, S.; Liu, X.; Xu, H. Clarithromycin ion pair in a liposomal membrane to improve its stability and reduce its irritation caused by intravenous administration. Expert Opin. Drug Deliv. 2016, 13, 337–348. [Google Scholar] [CrossRef]
- Cristofoli, M.; Hadgraft, J.; Lane, M.E.; Sil, B.C. A preliminary investigation into the use of amino acids as potential ion pairs for diclofenac transdermal delivery. Int. J. Pharm. 2022, 623, 121906. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Liu, C.; Ruan, J.; Yang, D.; Zhong, T.; Liu, Y.; Fang, L. Effect of the combination of permeation enhancer and ion-pairs strategies on transdermal delivery of tofacitinib. Int. J. Pharm. 2022, 611, 121190. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Liu, C.; Ding, D.; Quan, P.; Fang, L. The molecular design of drug-ionic liquids for transdermal drug delivery: Mechanistic study of counterions structure on complex formation and skin permeation. Int. J. Pharm. 2021, 602, 120560. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, C.; Quan, P.; Wan, X.; Shen, M.; Fang, L. Mechanism study on ion-pair complexes controlling skin permeability: Effect of ion-pair dissociation in the viable epidermis on transdermal permeation of bisoprolol. Int. J. Pharm. 2017, 532, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef]
- Kováčik, A.; Kopečná, M.; Vávrová, K. Permeation enhancers in transdermal drug delivery: Benefits and limitations. Expert Opin. Drug Deliv. 2020, 17, 145–155. [Google Scholar] [CrossRef]
- Ruan, J.; Chao, L.; Wang, J.; Zhong, T.; Quan, P.; Fang, L. Efficacy and safety of permeation enhancers: A kinetic evaluation approach and molecular mechanism study in the skin. Int. J. Pharm. 2022, 626, 122155. [Google Scholar] [CrossRef]
- Chen, L.; Ma, L.; Yang, S.; Wu, X.; Dai, X.; Wang, S.; Shi, X. A multiscale study of the penetration-enhancing mechanism of menthol. J. Tradit. Chin. Med. Sci. 2019, 6, 347–354. [Google Scholar] [CrossRef]
- Trommer, H.; Neube, R.H.H. Overcoming the stratum corneum: The modulation of skin penetration. Skin Pharmacol. Physiol. 2006, 19, 106–121. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Gill, H.S.; Park, J.-H. Microneedles for Drug Delivery. Modif. Release Drug Deliv. 2002, 2, 1295–1309. [Google Scholar]
- Ornelas, J.; Foolad, N.; Shi, V.; Burney, W.; Sivamani, R.K. Effect of Microneedle Pretreatment on Topical Anesthesia: A Randomized Clinical Trial. Randomized Control. Trial 2016, 152, 476–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arunkumar, S.; Shivakumar, H.N.; Murthy, S.N. Effect of terpenes on transdermal iontophoretic delivery of diclofenac potassium under constant voltage. Pharm. Dev. Technol. 2018, 23, 8. [Google Scholar] [CrossRef] [PubMed]
- Al-Mayahy, M.H.; Sabri, A.H.; Rutland, C.S.; Holmes, A.; Mckenna, J.; Marlow, M.; Scurr, D.J. Insight into imiquimod skin permeation and increased delivery using microneedle pre-treatment. Eur. J. Pharm. Biopharm. 2019, 139, 33–43. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experiments | Polymer | H2O (%) | AA-PG Solution * (%) | pH Regulators # (%) | pH | ||
|---|---|---|---|---|---|---|---|
| Types | Amount (%) | PG (%) | AA (%) | ||||
| Base Types | HA | 2.5 | 62.3 | 33.2 | 2.0 | / | 6.75 |
| CS | 4.4 | 58.9 | 33.7 | 2.0 | 1.0 HAc | 5.93 | |
| C940 | 1.3 | 21.1 | 33.1 | 2.0 | 42.5 TEA (5% aq.) | 7.21 | |
| P407 | 20.1 | 44.8 | 33.1 | 2.0 | / | 7.37 | |
| HA content | 2.5% HA | 2.5 | 62.3 | 33.2 | 2.0 | / | 6.75 |
| 3.5% HA | 3.5 | 61.3 | 33.2 | 2.0 | / | 6.65 | |
| 5.1% HA | 5.1 | 59.6 | 33.3 | 2.0 | / | 6.53 | |
| Drug content | 3.5% HA | 3.5 | 61.3 | 34.7 | 0.5 | / | 7.27 |
| 3.5% HA | 3.5 | 61.3 | 34.2 | 1.0 | / | 6.98 | |
| 3.5% HA | 3.5 | 61.3 | 33.2 | 2.0 | / | 6.65 | |
| Experiments | Organic Amine | Chemical Enhancer | HA (%) | H2O (%) | AA-PG (%) | |||
|---|---|---|---|---|---|---|---|---|
| Types | Amount (mol eq of AA) | Types | Amount (%) | PG | AA | |||
| Organic amine | * DEtA | 0.1 | / | 0 | 3.5 | 61.3 | 33.2 | 2.0 |
| TEtA | 0.1 | / | 0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| NMP | 0.1 | / | 0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| ETA | 0.1 | / | 0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| Chemical enhancer | DEtA | 0.1 | Azone | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 |
| DEtA | 0.1 | IPM | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| DEtA | 0.1 | Span 80 | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| DEtA | 0.1 | L-menthol | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| DEtA | 0.1 | ML | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 | |
| Enhancer combination | DEtA | 0.1 | L-menthol | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 |
| Span 80 | 5.0 | |||||||
| Microneedle pretreatment | DEtA | 0.1 | / | 0 | 3.5 | 61.3 | 33.2 | 2.0 |
| Microneedle & enhancers | DEtA | 0.1 | L-menthol | 5.0 | 3.5 | 61.3 | 33.2 | 2.0 |
| Solvents for Preparation | Solubility (mg/mL) | Solvents for Receptor Fluid | Solubility (mg/mL) |
|---|---|---|---|
| Water | / | PBS | / |
| IPM | 112.41 ± 22.04 | 3% Tween 80/PBS | 644.24 ± 49.54 |
| PG | 5365.38 ± 333.99 | 3% SDS/PBS | 312.75 ± 37.65 |
| * PEG 400 | 3877.34 ± 44.72 | 30% PEG 400/PBS | 128.90 ± 17.08 |
| OA | 522.03 ± 16.19 | ||
| GL | 89.84 ± 12.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Wang, Q.; Chen, N.; Yao, S.; Sun, X.; Quan, P.; Chen, Y. Probing Pharmaceutical Strategies to Promote the Skin Delivery of Asiatic Acid from Hydrogels: Enhancement Effects of Organic Amine Counterions, Chemical Enhancers, and Microneedle Pretreatment. Pharmaceutics 2022, 14, 2532. https://doi.org/10.3390/pharmaceutics14112532
Li M, Wang Q, Chen N, Yao S, Sun X, Quan P, Chen Y. Probing Pharmaceutical Strategies to Promote the Skin Delivery of Asiatic Acid from Hydrogels: Enhancement Effects of Organic Amine Counterions, Chemical Enhancers, and Microneedle Pretreatment. Pharmaceutics. 2022; 14(11):2532. https://doi.org/10.3390/pharmaceutics14112532
Chicago/Turabian StyleLi, Mingming, Qiuyue Wang, Naiying Chen, Sicheng Yao, Xinxing Sun, Peng Quan, and Yang Chen. 2022. "Probing Pharmaceutical Strategies to Promote the Skin Delivery of Asiatic Acid from Hydrogels: Enhancement Effects of Organic Amine Counterions, Chemical Enhancers, and Microneedle Pretreatment" Pharmaceutics 14, no. 11: 2532. https://doi.org/10.3390/pharmaceutics14112532