
Acceptability of Multiparticulate Dosing Using Sympfiny® Delivery System with Children (Age 1–12)

Abstract
:1. Introduction
2. Materials and Methods
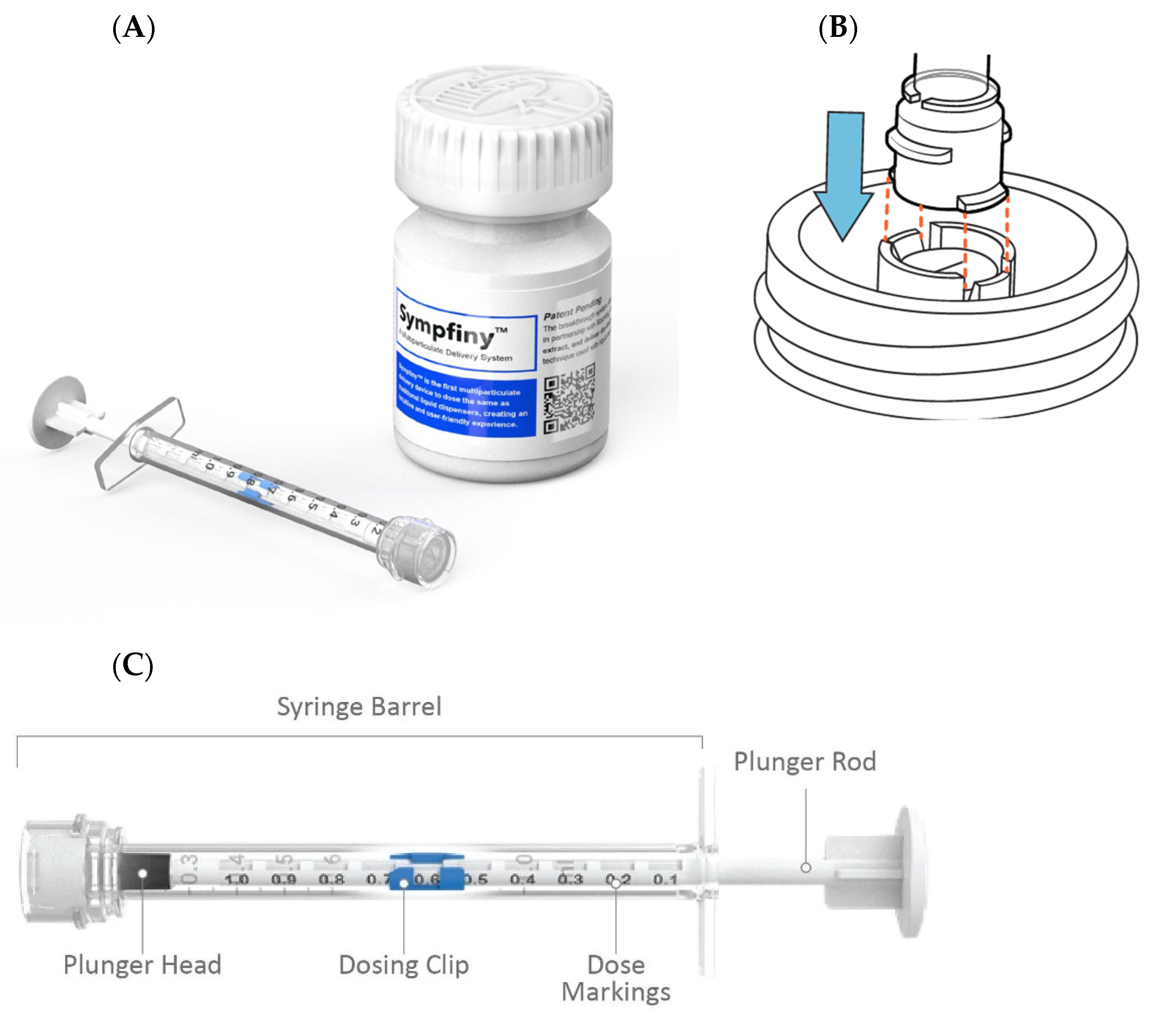
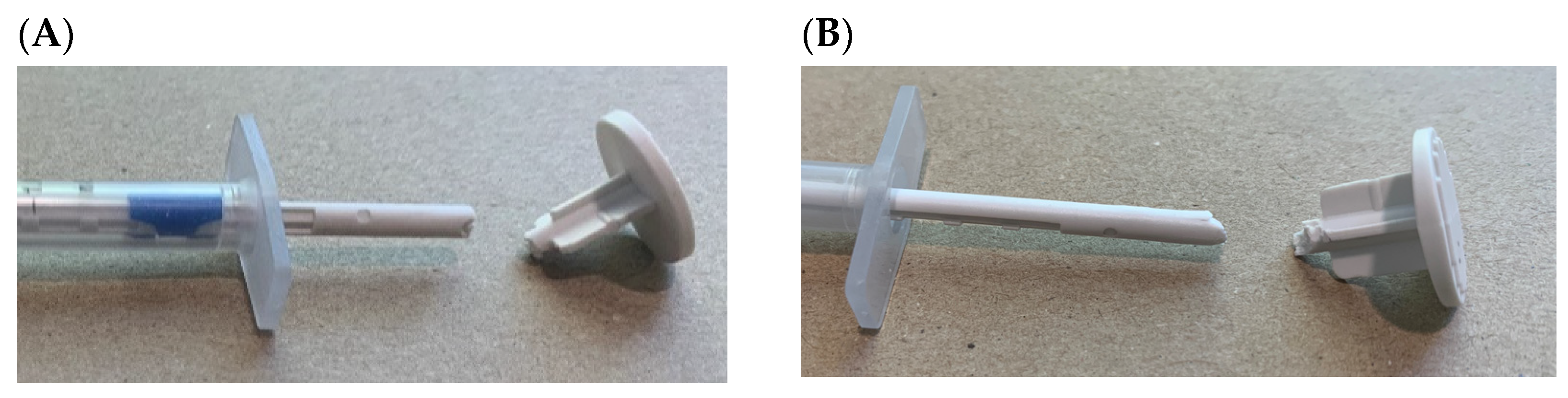
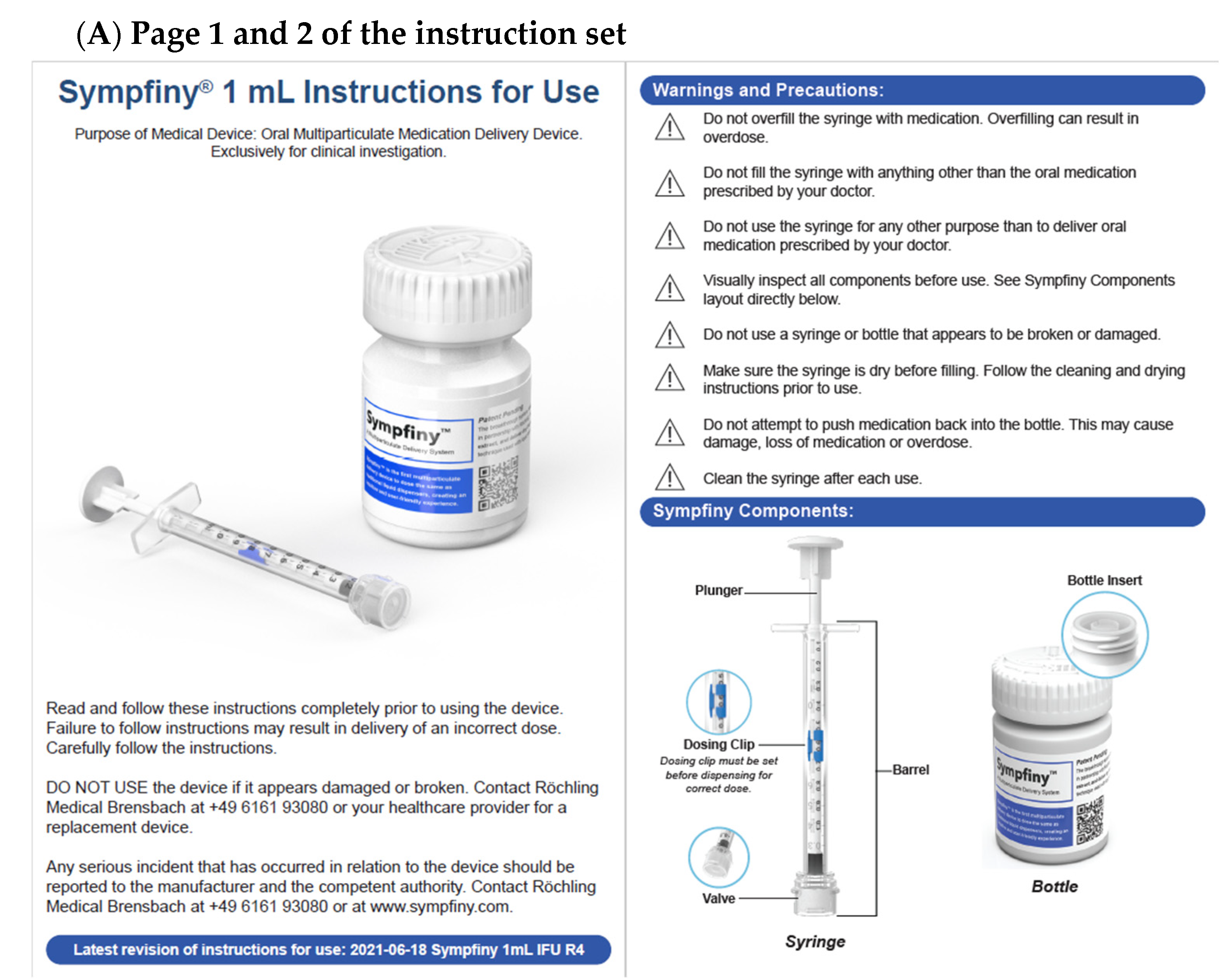
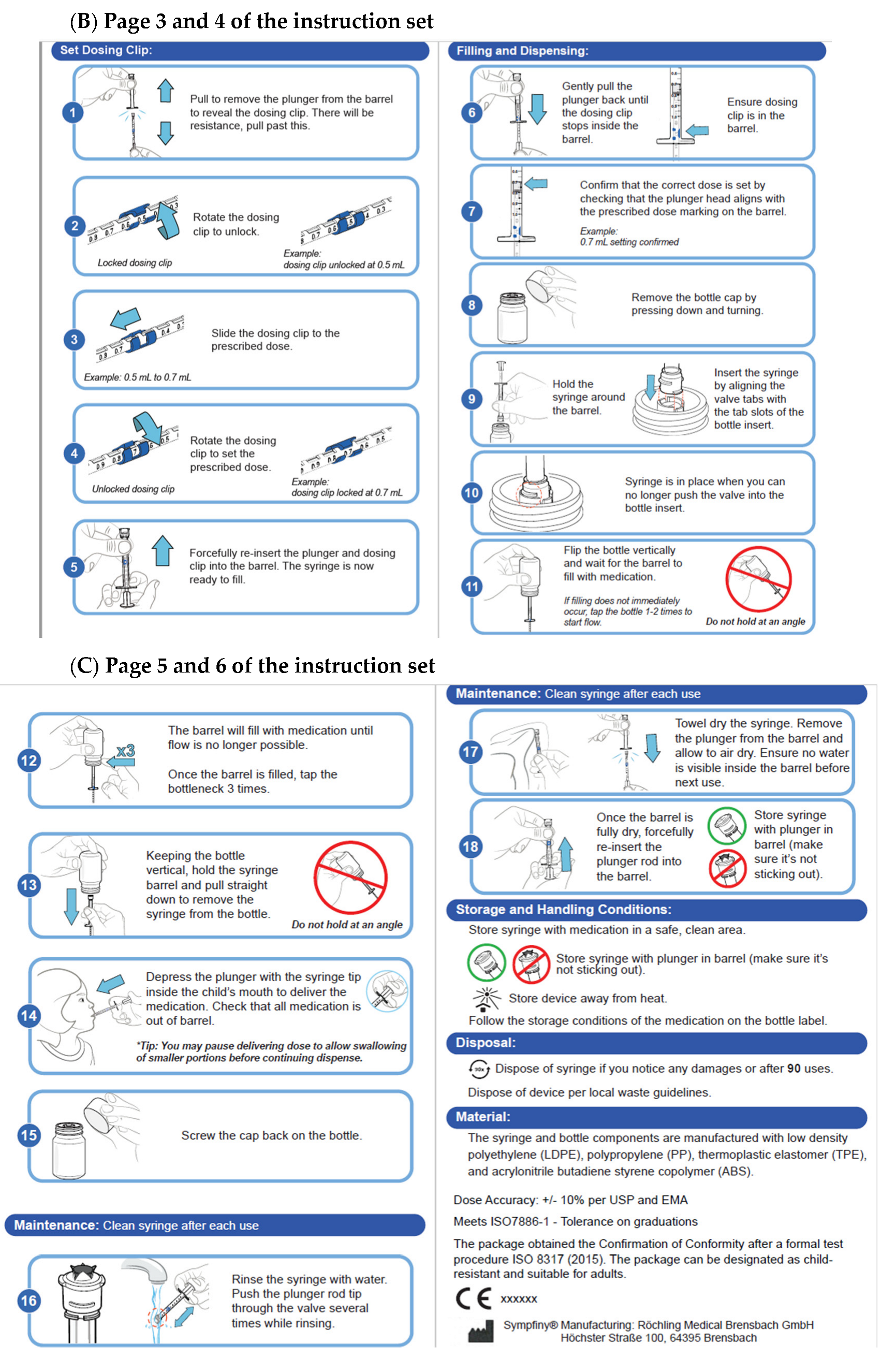
2.1. Sympfiny® System
2.2. Placebo
2.3. Participants
2.4. Methods
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Child Participant Results
3.1.1. Overall Data for Ages 5–12
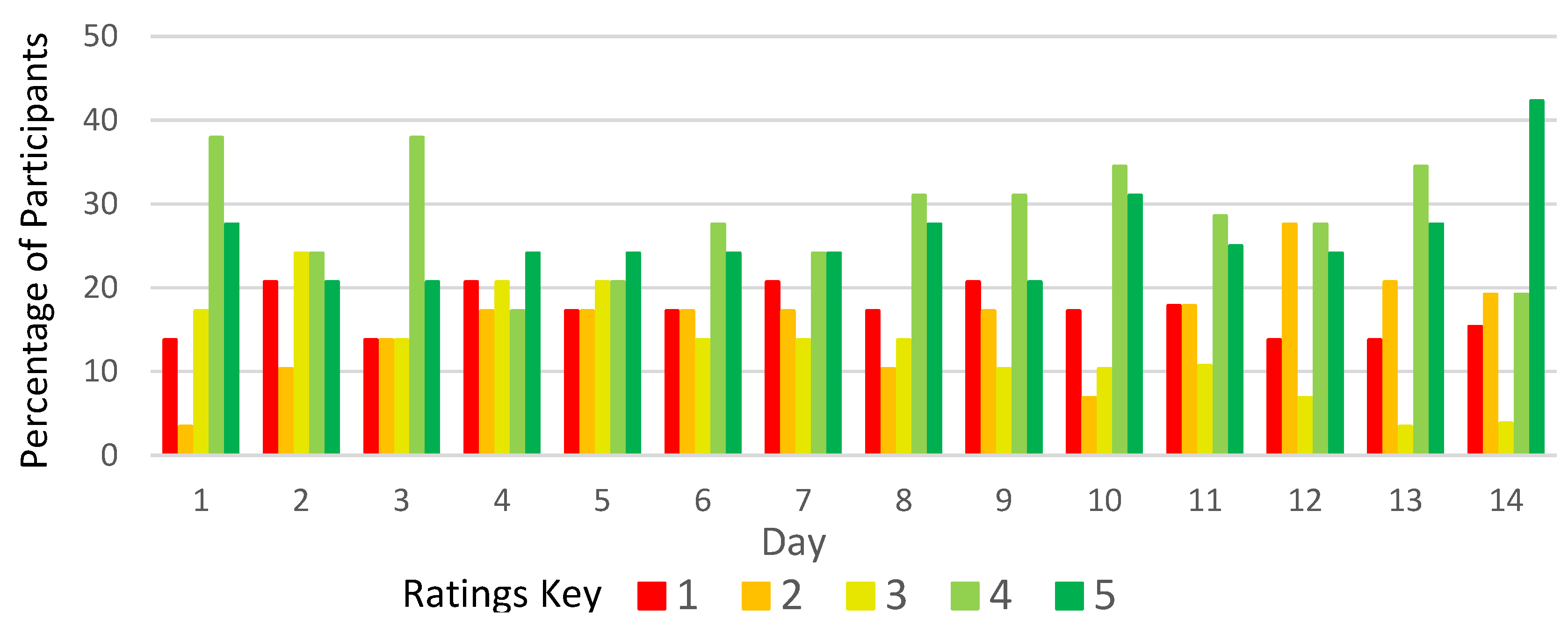
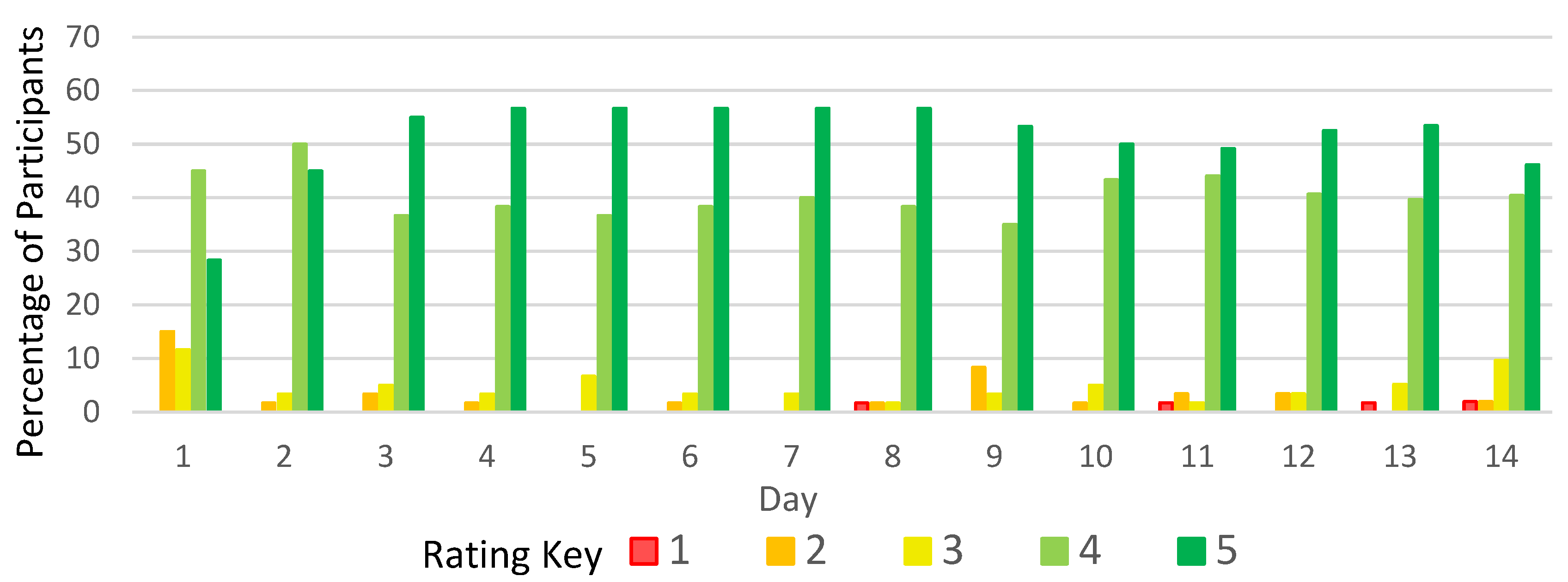
3.1.2. Grittiness of the Sample (Ages 5–12)
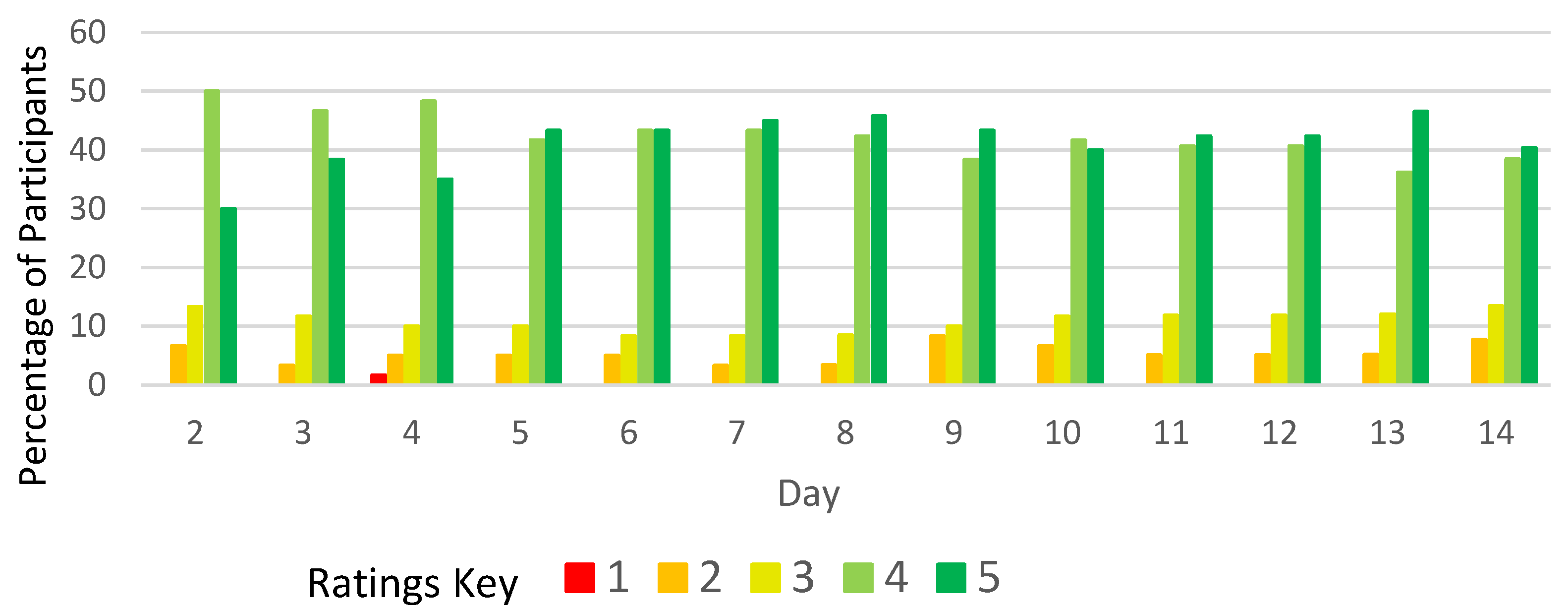
3.1.3. Volume of the Sample (Ages 5–12)
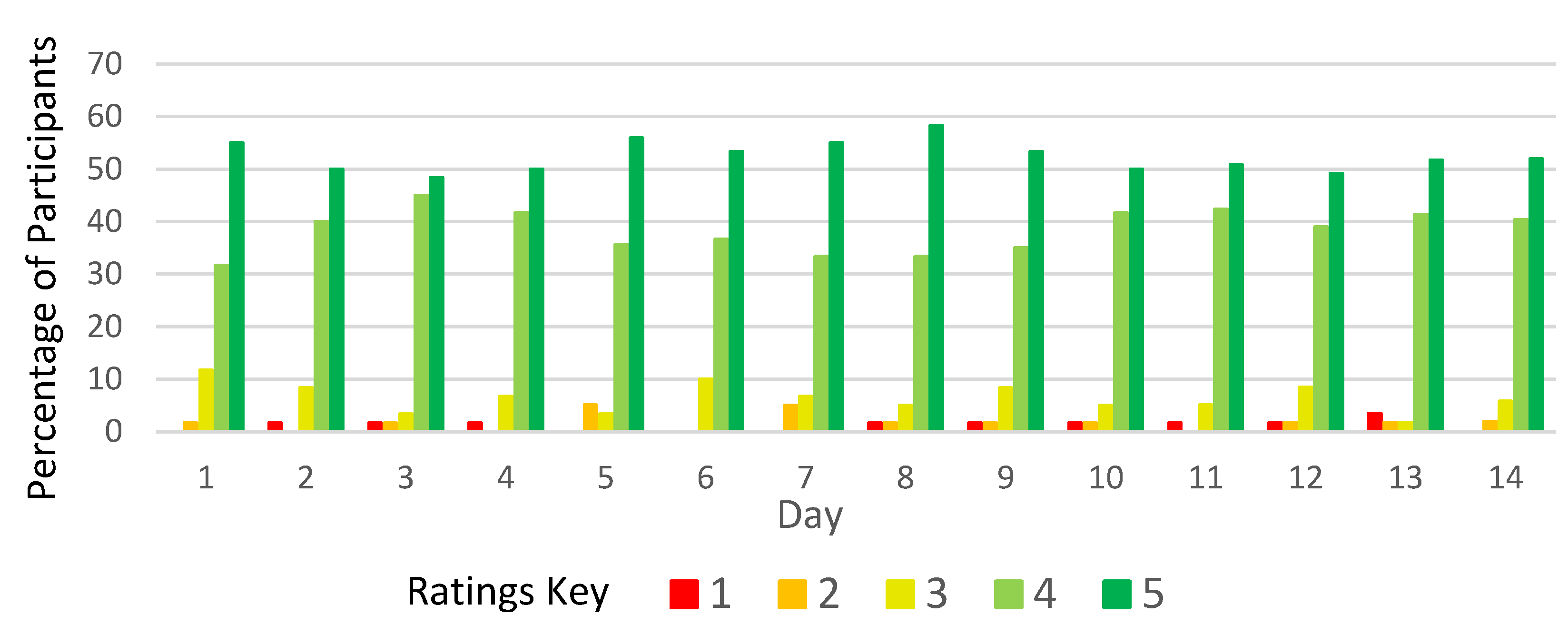
3.1.4. Mouthfeel of Sample (Ages 5–12)
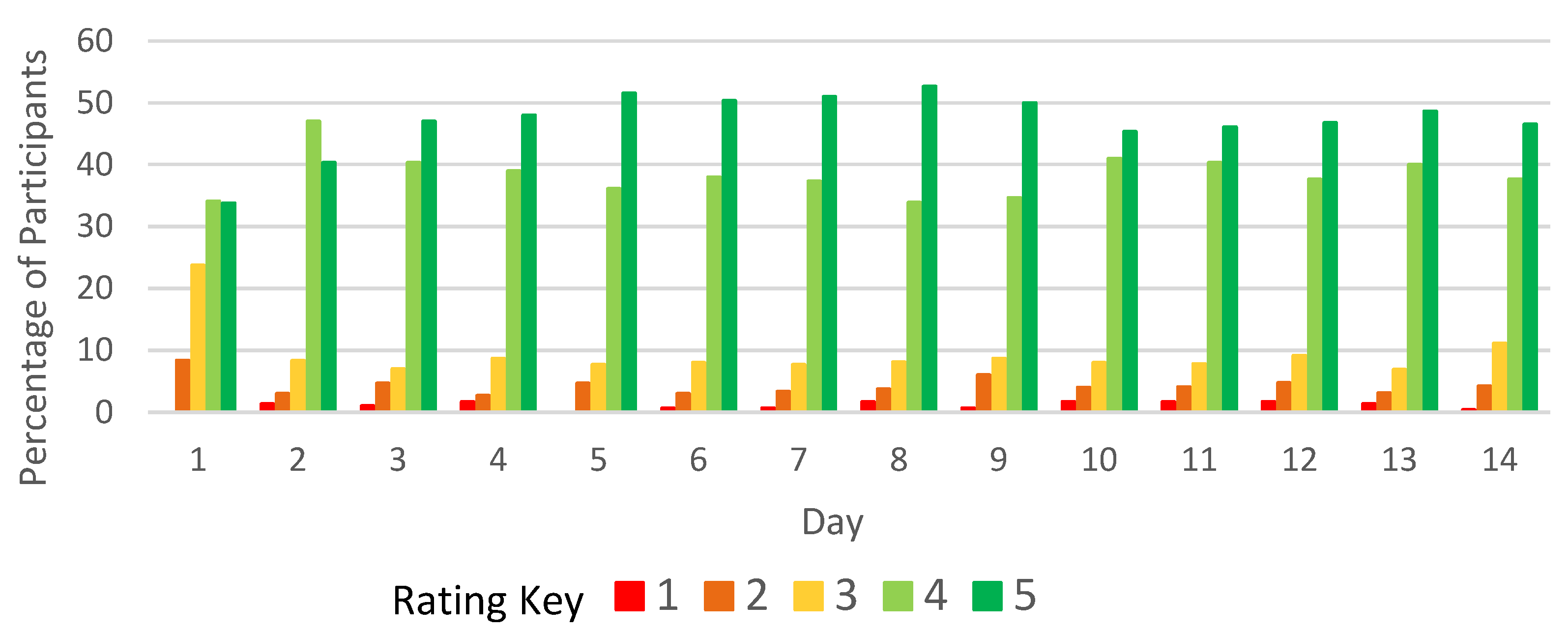
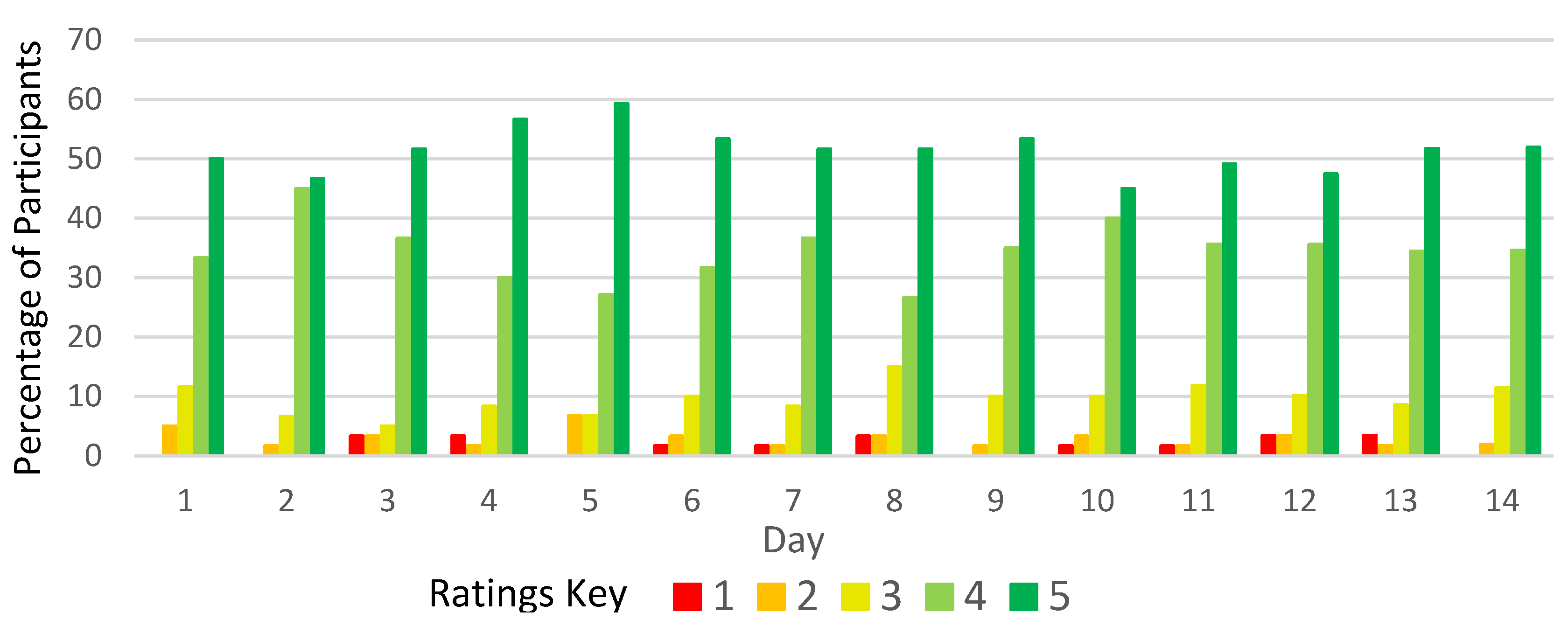
3.1.5. Overall Taste (Ages 5–12)
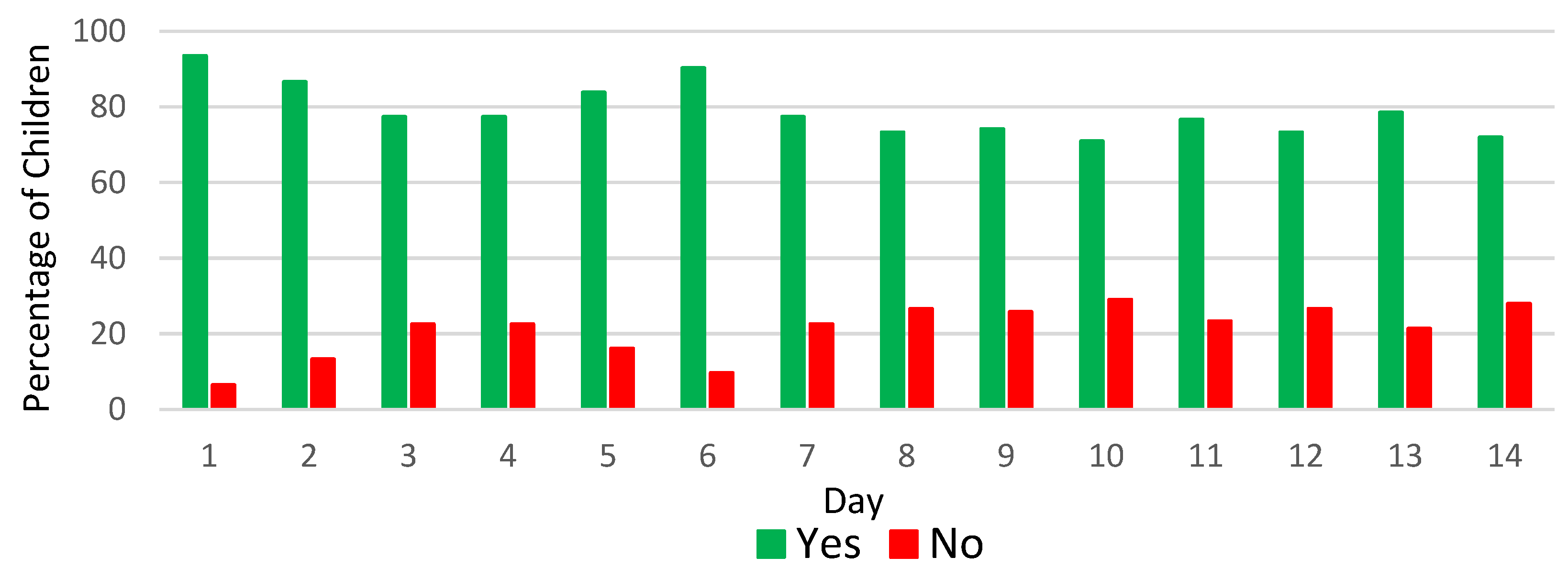
3.1.6. Willingness to Open Mouth to Receive Sample (Ages 1–4)
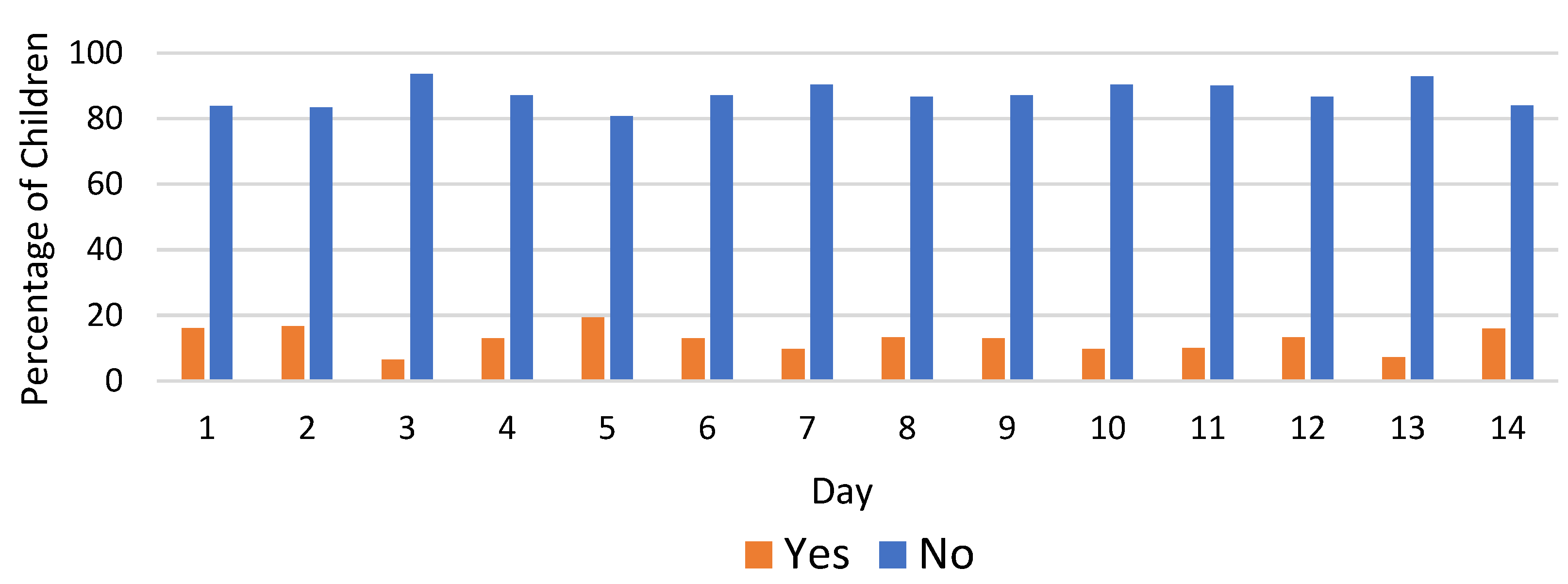
3.1.7. Did the Child Spit out the Placebo? (Ages 1–4)
3.2. Parent Results
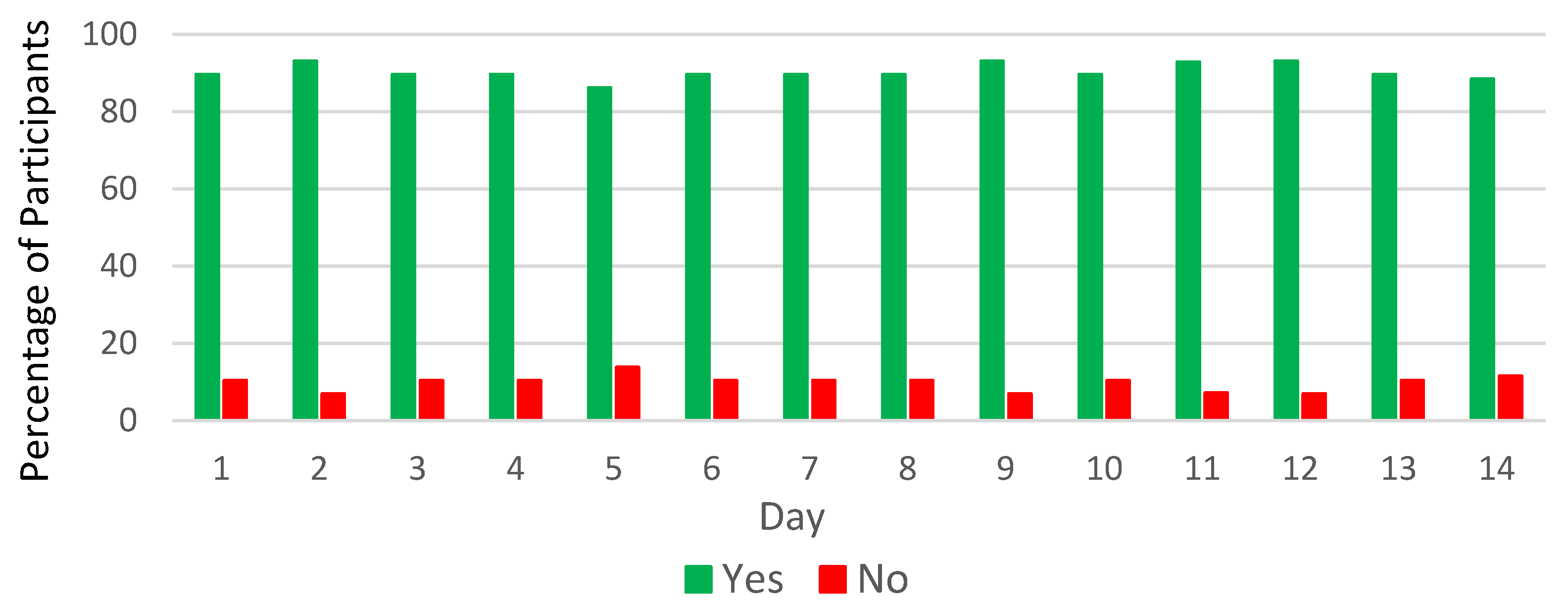
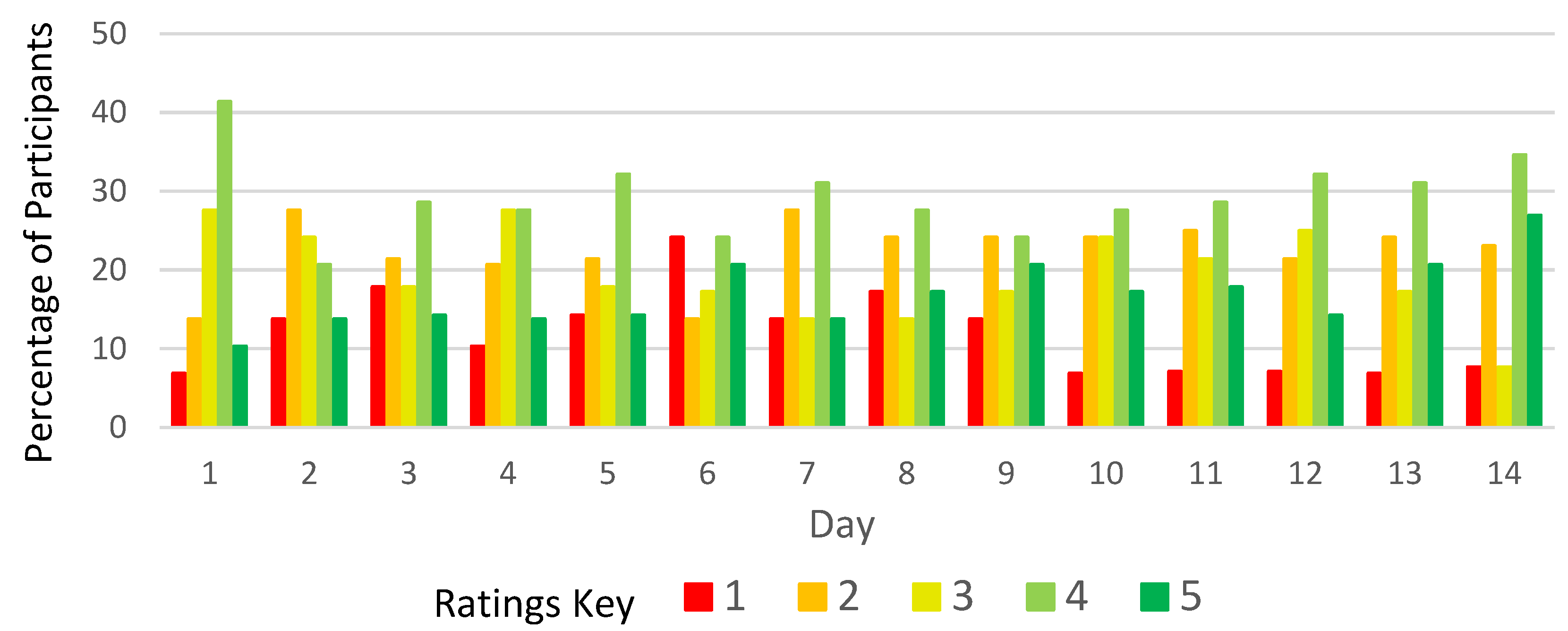
3.2.1. Parents: Overall Results
3.2.2. Setting the Dose
3.2.3. Connecting the Syringe
3.2.4. Dispensing the Multiparticulate
3.2.5. Cleaning
3.2.6. Accuracy of Dose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Survey Question | Assessment Tool |
|---|---|
| Rating for: Setting the dose | 5-point hedonic (Very difficult-very easy) |
| Rating for: Connecting syringe | |
| Rating for: Filling the syringe with MP | |
| Rating for: Dispensing the MP | |
| Rating for: Cleaning syringe | |
| How sure are you that you dispensed an accurate dose? | |
| Did your child have any difficulty receiving or swallowing the dose? (If yes, please explain) | Free text |
| Overall, do you consider this adapted oral syringe to be an acceptable device to administer multiparticulate to children? | Free text |
| What was your child’s mood before administering the dose? | Selection (mad, sad, calm/neutral, happy smiley faces) |
| Did your child willingly open their mouth for the syringe? | Yes/no |
| Did your child: Spit out the placebo, refuse to swallow/hold in mouth, Make a negative facial expression, Cry/Whimper or Other (asked to specify). | Selection/free text |
| What was your child’s mood after administering the dose? | Selection (mad, sad, calm/neutral, happy smiley faces) |
| Survey Question | Assessment Tool |
|---|---|
| Setting the dose | 5-point hedonic (Very difficult-very easy |
| Connecting syringe | |
| Filling the syringe with MP | |
| Dispensing the MP | |
| Cleaning syringe | |
| How sure are you that you dispensed an accurate dose? | |
| Did your child have any difficulty receiving or swallowing the dose? (If yes, please explain) | Free text |
| Overall, do you consider this adapted oral syringe to be an acceptable device to administer multiparticulate to children? | Free text |
| Please rate the grittiness of the sample. (Grittiness means that you feel the ‘bits’ in the sample) | 5-point Hedonic (Dislike very much-Like very much) |
| What did you think of the overall volume of the sample? (Volume means the amount you had to take) | |
| What did you think the overall mouthfeel of the sample? (mouthfeel means how the sam-ple felt in your mouth) | |
| What did you think of the overall taste in your mouth? | |
| Can you still feel any of the ‘bits’ in your mouth? | Yes/no |
| If this was medicine and you were sick, would you be willing to take this every day? | Yes/no |
| Additional comments about the sample or process | Free text |
Appendix B


References
- European Medicines Agency. Guideline on Pharmaceutical Development of Medicines for Paediatric Use 2013. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 14 November 2022).
- European Medicines Agency. Guideline on the Demonstration of Palatability of Veterinary Medicinal Products 2014. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-demonstration-palatability-veterinary-medicinal-products_en.pdf (accessed on 14 November 2022).
- Kozarewicz, P. Regulatory Perspectives on Acceptability Testing of Dosage Forms in Children. Int. J. Pharm. 2014, 469, 245–248. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Module 5: Acceptability 2018. Available online: https://media.tghn.org/medialibrary/2018/07/WHO_Research_Toolkit_Module_5.pdf (accessed on 14 November 2022).
- Bolger, N.; Davis, A.; Rafaeli, E. Diary Methods: Capturing Life as It Is Lived. Annu. Rev. Psychol. 2003, 54, 579–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lev-On, A.; Lowenstein-Barkai, H. Viewing Diaries in an Age of New Media: An Exploratory Analysis of Mobile Phone App Diaries versus Paper Diaries. Methodol. Innov. 2019, 12, 205979911984444. [Google Scholar] [CrossRef]
- Katarzyna Hofmanová, J.; Bennett, J.; Coupe, A.; Bartlett, J.A.; Monahan, A.; Batchelor, H.K. A Novel Oral Syringe for Dosing and Administration of Multiparticulate Formulations: Acceptability Study in Preschool and School Children. Pharmaceutics 2020, 12, 806. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.W.; Resurreccion, A.V.A.; Paguio, L.P. Age appropriate hedonic scales to measure food preferences of young children. J. Sens. Stud. 1996, 11, 141–163. [Google Scholar] [CrossRef]
- Lawless, H.T.; Heymann, H. Sensory Evaluation of Food: Principles and Practices, Food Science Texts Series; 2nd ed.; Springer: New York, NY, USA, 2010; ISBN 9781441964878. [Google Scholar]
- Lopez, F.L.; Mistry, P.; Batchelor, H.K.; Bennett, J.; Coupe, A.; Ernest, T.B.; Orlu, M.; Tuleu, C. Acceptability of Placebo Multiparticulate Formulations in Children and Adults. Sci. Rep. 2018, 8, 9210. [Google Scholar] [CrossRef]


















| Product Name: | APT5136 Placebo Beads |
| Manufacturer: | Adare Pharmaceuticals |
| Coating: | Ethylcellulose |
| Particle size (approx.) | 177–250 microns |
| Batch number: | Pf63410001 |
| Age Group | Multiparticulate Dose Volume Range Per BSA |
|---|---|
| 1–2 years old | 0.2 mL |
| 3–4 years old | 0.3 mL |
| 5–8 years old | 0.4 mL |
| 9–12 years old | 0.5 mL |
| Child Characteristic | Number | Percent (%) |
|---|---|---|
| Gender | ||
| Male | 33 | 55 |
| Female | 27 | 45 |
| Age | ||
| 1–2 | 15 | 25 |
| 3–4 | 16 | 27 |
| 5–8 | 14 | 23 |
| 9–12 | 15 | 25 |
| Parent Characteristic | Number | Percent (%) |
|---|---|---|
| Gender | ||
| Male | 27 | 45 |
| Female | 33 | 55 |
| Race | ||
| White | 43 | 71 |
| Black | 10 | 17 |
| Asian | 7 | 12 |
| Ethnicity | ||
| Hispanic or Latino | 8 | 13 |
| Non-Hispanic or Latino | 52 | 87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abeln, K.; Cox, K.; Haggerty, L.; Privitera, M.B. Acceptability of Multiparticulate Dosing Using Sympfiny® Delivery System with Children (Age 1–12). Pharmaceutics 2022, 14, 2524. https://doi.org/10.3390/pharmaceutics14112524
Abeln K, Cox K, Haggerty L, Privitera MB. Acceptability of Multiparticulate Dosing Using Sympfiny® Delivery System with Children (Age 1–12). Pharmaceutics. 2022; 14(11):2524. https://doi.org/10.3390/pharmaceutics14112524
Chicago/Turabian StyleAbeln, Kate, Kate Cox, Laura Haggerty, and Mary Beth Privitera. 2022. "Acceptability of Multiparticulate Dosing Using Sympfiny® Delivery System with Children (Age 1–12)" Pharmaceutics 14, no. 11: 2524. https://doi.org/10.3390/pharmaceutics14112524