
Early Negativization of SARS-CoV-2 Infection by Nasal Spray of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial
Abstract
:1. Introduction
2. Methods
2.1. Description of the Trial
2.2. Eligibility Criteria for Participants
- Agreeing to take part within 48 h since testing positive for SARS-CoV-2 at RT-PCR;
- Age >18 years;
- Mild/moderate COVID-19 symptoms or asymptomatic SARS-CoV-2 infection;
- Provision of written informed consent;
- Completion of COVID-19-Q questionnaire (Supplementary File S1) at study entry as well as exit.
2.3. Setting and Location Where the Data Were Collected
2.4. The Interventions by Group
- a treatment arm (receiving standard of care plus nasal spray with Tonimer Lab Panthexyl 800); and
- a control arm (receiving standard of care but nasal spray with Tonimer Lab Panthexyl 800).
2.4.1. Both Treatment and Control Groups
- Section 1: collecting socio-demographic information;
- Section 2: collecting information on COVID-19 vaccination status (number, date and type of vaccine received), comorbidities (diabetes, COPD, heart disorders; renal disorders, other) and lifestyle habits (smoking, alcohol and oral hygiene);
- Section 3: collecting COVID-19 symptoms, which were described using the internationally validated score Sino-Nasal Outcome Test 22 (SNOT-22) regarding smell, taste function, and therapy followed.
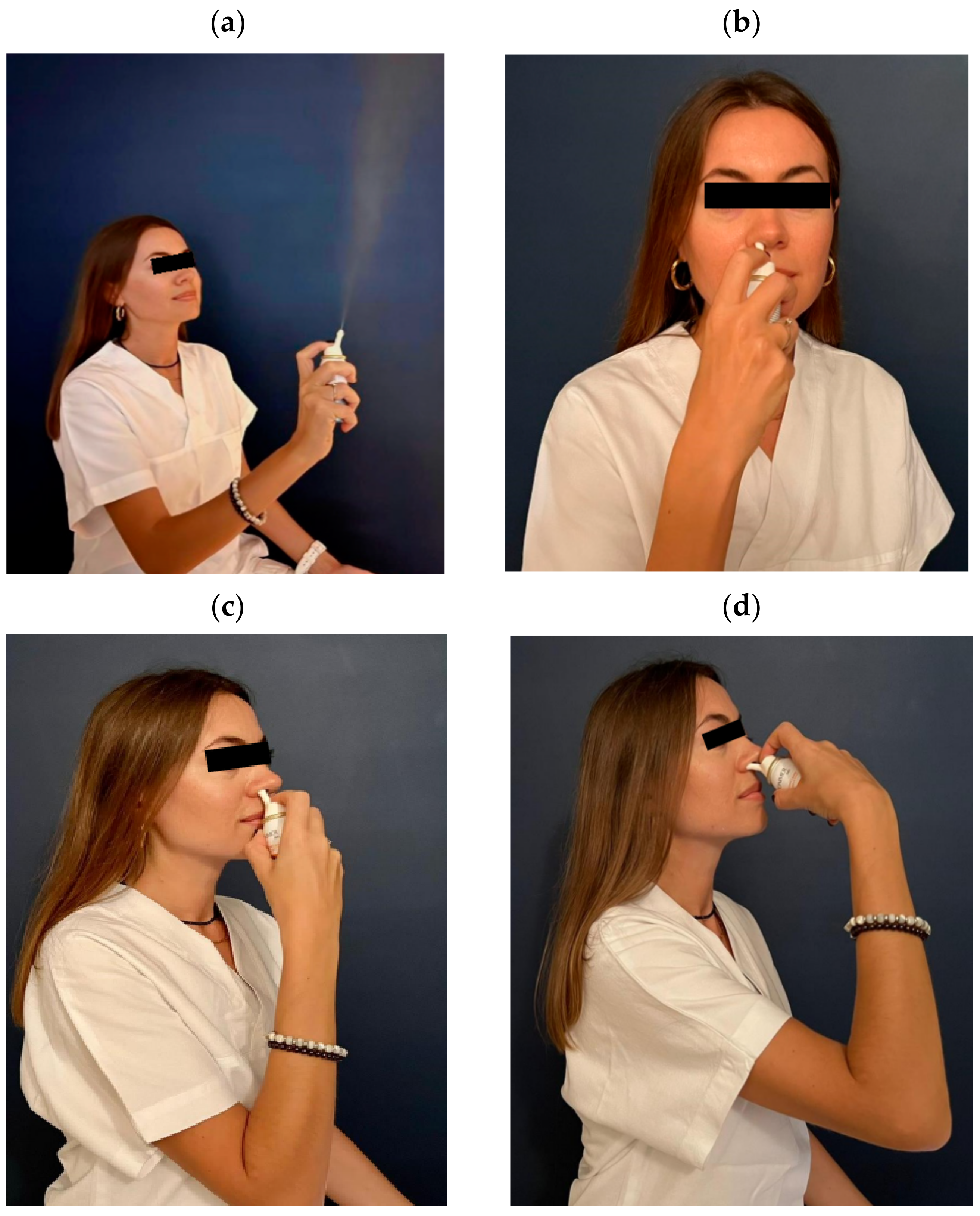
2.4.2. The Treatment Group
2.5. Outcome Measure
2.6. Estimated Sample Size
2.7. Statistical Analysis
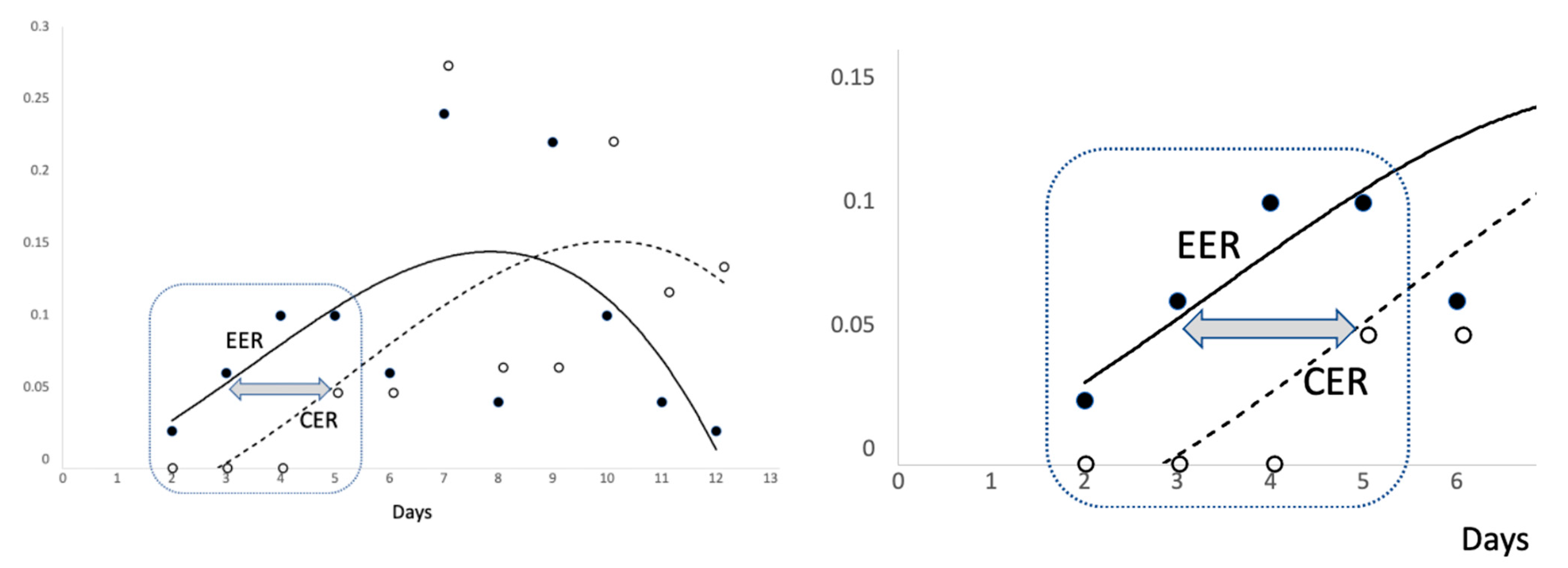
- Rate of events in the experimental arm (EER) = number of events/number of patients in the experimental arm);
- Rate of events in the control arm (CER) = number of events/number of patients in the control arm.
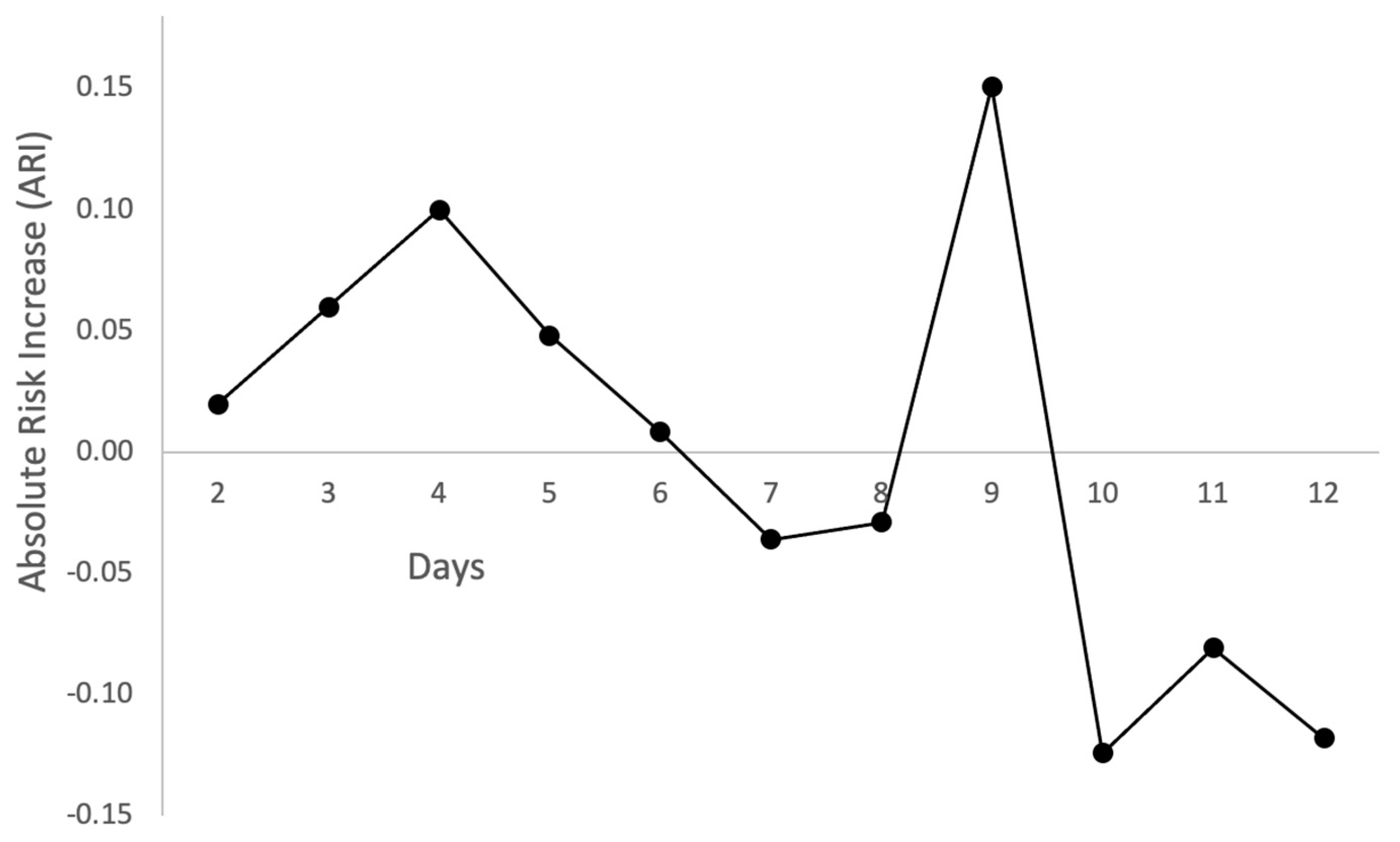
- Absolute risk increase (ARI) = (EER − CER). It expresses, generally in decimal values, the absolute increase in the risk of events in the treated group compared to controls. The sign of ARI is positive when EER > CER and negative otherwise.
- Number needed to treat (NNT) = (1/ARI). NNT represents the expected number of patients required in order to achieve one beneficial outcome event. This estimate is easy to calculate and expresses the benefits of an intervention in the same unit of measurement (number of patients).
- Logistic regression, expressing the results as odds ratio (OR) with a 95% confidence interval (95%CI). OR is the ratio of the probability of the event in the treatment arm against the probability of the event in the control group. It is expressed in decimal values. OR > 1.00 or < 1.00 expresses, respectively, a beneficial or a detrimental effect of the treatment.
- Cox regression (or proportional hazards regression), expressing the results as hazard ratio (HR) with a 95% confidence interval (95%CI). HR investigates the effect of the treatment on the time until first negative antigenic swab test result. Since this was a beneficial intervention (because treatment stopped viral shedding), a positive HR indicates a protective effect of the associated variable. Cox regression allows the investigation of the effect of multiple variables at the same time. Since all terms displayed in Table 2 were not significant in univariable Cox proportional hazard regression, the analysis was restricted to estimate the treatment effect.
3. Results
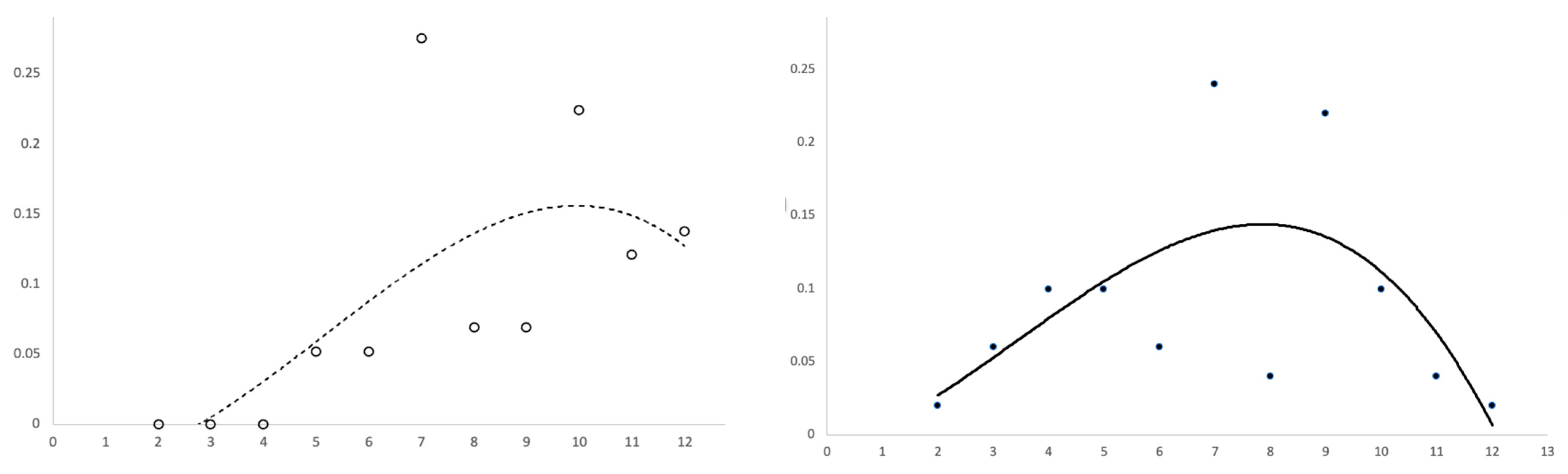
- Number of negative antigenic swab test results (study endpoint) in treatment versus control arm;
- Proportion of endpoint in the experimental (experimental event rate (EER)) versus control (control event rate (CER)) group;
- Absolute risk increase (ARI), computed as the difference between EER and CER.
4. Discussion
4.1. Key Findings
4.2. Limitations
4.3. Interpretations of Findings
- Inhibition of viral replication. SARS-CoV-2 replication is reportedly dose-dependently inhibited by saline solutions (0.8–1.7% NaCl). Inhibition of viral replication already started from a concentration of 0.6%, increasing up to 50% at 0.9% (isotonic saline solution) and reaching 100% at 1.5% (mildly hypertonic saline solution) [31]. Saline, however, had no direct effect on SARS-CoV-2 itself. Inhibition of viral replication in vitro was arguably due to an intracellular mechanism of membrane depolarization and intracellular energy deprivation efficiently stimulated by hypertonic saline solutions [31].
- Shift of myeloperoxidase (MPO) activity in epithelial or phagocytic cells. This metabolic route yields hypochlorous acid (HOCl). Inhibition of viral replication in presence of chloride and halide salts was first reported in the 1960s [32]. HOCl has the well-known virucidal activity of bleach, effective against all viruses. Nevertheless, HOCl is also cytotoxic and may injure the epithelial cells of human airways. For instance, direct exposure of mucosal cilia to HOCl was found to cause ciliostasis, possibly contributing to discrepant effects of hypertonic saline solutions on the MCC across different studies. Therefore, tight regulation of this metabolic route is recommended [33]. Significantly higher expressions of MPO (≈4 fold, p < 0.05) were found in naso-oropharyngeal samples of SARS-CoV-2 patients. Over-expression of MPO may produce HOCl in excess, thereby damaging nasopharyngeal tissues [34].
4.4. Prospects
- According to the standard behavior of upper respiratory viruses, if symptoms deteriorate in five days after disease onset or persist beyond 10 days, it is likely that there is a secondary bacterial infection requiring clinical evaluation [43].
- The UK Health Security Agency allows healthcare workers (HCWs) to return to work if they test negative on both days 5 and 6 (undertaken 24 h apart) after the date of the initial positive RT-PCR swab test [44].
- Current occupational guidelines by the European Centre for Disease Prevention and Control (ECDC) for HCWs testing positive for SARS-CoV-2 recommend a standard isolation of six days for vaccinated versus 10 days for individuals unvaccinated against COVID-19 [45].
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Clinical Characteristics of COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/clinical (accessed on 4 October 2022).
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Wang, W.; Ma, J.; Wu, S.; Sun, F. Reinfection rates among patients previously infected by SARS-CoV-2: Systematic review and meta-analysis. Chin. Med. J. 2022, 135, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.; Teha, H.S.; Lian, J.; Suah, J.L.; Husin, M.; Hwong, W.Y. SARS-CoV-2 in Malaysia: A surge of reinfection during the predominantly Omicron period. Lancet Reg. Health—Western Pac. 2022, 26, 100572. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, U.; Chakraborty, A.; Naskar, S.; Saha, B.; Bandyapadhyay, B.; Shee, S. Efficacy of Normal Saline Nasal Spray and Gargle on SARS-CoV-2 for Prevention of COVID-19 Pneumonia; Research Square: Durham, NC, USA, 2021. [Google Scholar]
- Cegolon, L.; Javanbakht, M.; Mastrangelo, G. Nasal disinfection for the prevention and control of COVID-19: A scoping review on potential chemo-preventive agents. Int. J. Hyg. Environ. Health 2020, 230, 113605. [Google Scholar] [CrossRef]
- Cegolon, L. Investigating hypothiocyanite against SARS-CoV-2. Int. J. Hyg. Environ. Health 2020, 227, 113520. [Google Scholar] [CrossRef]
- Cegolon, L.; Mirandola, M.; Salaris, C.; Salvati, M.V.; Mastrangelo, G.; Salata, C. Hypothiocyanite and Hypothiocyanite/Lactoferrin Mixture Exhibit Virucidal Activity In Vitro against SARS-CoV-2. Pathogens 2021, 10, 233. [Google Scholar] [CrossRef]
- Ramalingam, S.; Graham, C.; Dove, J.; Morrice, L.; Sheikh, A. Hypertonic saline nasal irrigation and gar-gling should be considered as a treatment option for COVID-19. J. Glob. Health 2020, 10, 010332. [Google Scholar] [CrossRef]
- Ramalingam, S.; Graham, C.; Dove, J.; Morrice, L.; Sheikh, A. A pilot, open labelled, randomized con-trolled trial of hypertonic saline nasal irrigation and gargling for the common cold. Sci. Rep. 2019, 9, 1015. [Google Scholar] [CrossRef] [Green Version]
- Kanjanawasee, D.; Seresirikachorn, K.; Chitsuthipakorn, W.; Snidvongs, K. Hypertonic saline versus isotonic saline nasal irrigation: Systematic review and meta-analysis. Am. J. Rhinol. Allergy 2018, 32, 269–279. [Google Scholar] [CrossRef]
- Štanfel, D.; Kalogjera, L.; Ryazantsev, S.V.; Hlača, K.; Radtsig, E.Y.; Teimuraz, R.; Hrabač, P. The role of seawater and saline solutions in treatment of upper respiratory conditions. Mar. Drugs 2022, 20, 330. [Google Scholar] [CrossRef] [PubMed]
- Farrell, N.F.; Klatt-Cromwell, C.; Schneider, J.S. Benefits and safety of nasal saline irrigations in a pandemic—Washing COVID-19 away. JAMA Otolaryngol.–Head Neck Surg. 2020, 146, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, S.; Alevizopoulos, K. Nasal Irrigation in the COVID-19 Era. IJCMCR 2021, 13, 004. [Google Scholar]
- Rosati, P.; Giordano, U.; Concato, C. Hypertonic saline nasal irrigation and gargling as an inexpensive practical adjunctive weapon to combat asymptomatic SARS-CoV-2 infections. A case reports. Trends Med. 2020, 20, 1–3. [Google Scholar] [CrossRef]
- Kimura, K.S.; Freeman, M.H.; Wessinger, B.C.; Gupta, V.; Sheng, Q.; Huang, L.C.; von Wahlde, K.; Das, S.; Chowdhury, N.I.; Turner, J.H. Interim analysis of an open-label randomized controlled trial evaluating nasal irrigations in non-hospitalized patients with COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 1325. [Google Scholar] [CrossRef]
- Yildiz, E.; Koca, Y.S.; Kuzu, S.; Günebakan, Ç.; Bucak, A.; Kahveci, O.K. Comparison of the Healing Effect of Nasal Saline Irrigation with Triamcinolone Acetonide Versus Nasal Saline Irrigation alone in COVID-19 Related Olfactory Dysfunction: A Randomized Controlled Study. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–6. [Google Scholar] [CrossRef]
- Varricchio, A.; La, M.I.; Brunese, F.P.; Ciprandi, G. Smell recovery in patients with COVID-19: An experience with nebulized nasal treatment. J. Biol. Regul. Homeost. Agents 2021, 35, 683–686. [Google Scholar]
- Varricchio, A.; La, M.I.; Brunese, F.P.; Varricchio, A.; Ciprandi, G. Viral shedding in symptomatic patients with mild COVID-19: An experience with nebulized nasal treatment. J. Biol. Regul. Homeost. Agents 2021, 35, 1155–1157. [Google Scholar]
- Ciprandi, G.; La, M.I.; Brunese, F.P.; Varricchio, A.; Varricchio, A. Hypertonic saline with xylitol and hyaluronate may shorten the viral shedding duration in asymptomatic COVID-19 positive subjects: A pilot study. J. Biol. Regul. Homeost. Agents 2021, 35, 1151–1154. [Google Scholar]
- Meister, T.L.; Todt, D.; Brüggemann, Y.; Steinmann, J.; Banava, S.; Brill, F.H.H.; Steinmann, J.; Pfaender, S.; Steinmann, E. Virucidal activity of nasal sprays against severe acute respiratory syndrome coronavirus-2. J. Hosp. Infect. 2022, 120, 9–13. [Google Scholar] [CrossRef]
- NCT05458336. A Non-Randomized Controlled Clinical Trial on the Use of Saline Nasal Irrigations to Eradicate Localized Nasal Infection by SARS-CoV-2. Available online: https://clinicaltrials.gov/ct2/show/NCT05458336 (accessed on 16 August 2022).
- Yan, D.; Zhang, X.; Chen, C.; Jiang, D.; Liu, X.; Zhou, Y.; Huang, C.; Zhou, Y.; Guan, Z.; Ding, C.; et al. Characteristics of Viral Shedding Time in SARS-CoV-2 Infections: A systematic review and meta-analysis. Front. Public Health 2021, 9, 652842. [Google Scholar] [CrossRef] [PubMed]
- Spinato, G.; Fabbris, C.; Conte, F.; Menegaldo, A.; Franz, L.; Gaudioso, P.; Cinetto, F.; Agostini, C.; Costantini, G.; Boscolo-Rizzo, P. COVID-Q: Validation of the first COVID-19 questionnaire based on patient-rated symptom gravity. Int. J. Clin. Pract. 2021, 75, e14829. [Google Scholar] [CrossRef] [PubMed]
- University of British Columbia. Clinical Significance Calculator; University of British Columbia: Vancouver, BC, Canada; Available online: https://www.elcomprimido.com/FARHSD/DOC_CD_Curso_Palma_2006/calculadoras/UBC%20Clinical%20Significance%20Calculator.htm (accessed on 16 August 2022).
- Fisher, L.D.; Dixon, D.O.; Herson, J.; Frankowski, R.K.; Hearron, M.S.; Peace, K.E. Intention to treat in clinical trials. In Statistical Issues in Drug Research and Development; Peace, K.E., Ed.; Marcel Dekker: New York, NY, USA, 1990; pp. 331–350. [Google Scholar]
- Wennmacker, S.Z.; van Dijk, A.H.; Drenth, J.P.H.; Donkervoort, S.C.; Boerma, D.; Westert, G.P.; van Laarhoven, C.J.H.M.; Boermeester, M.A.; Dijkgraaf, M.G.W.; de Reuver, P.R. Statistical analysis plan of a randomized controlled trial to compare a restrictive strategy to usual care for the effectiveness of cholecystectomy (SECURE trial). Trials 2018, 19, 604. [Google Scholar] [CrossRef] [PubMed]
- United Stated Environmental Protection Agency (USEPA). About List N: Disinfectants for Corona-Virus (COVID-19). Available online: https://www.epa.gov/coronavirus/about-list-n-disinfectants-coronavirus-covid-19-0 (accessed on 7 November 2022).
- Huijghebaert, S.; Hoste, L.; Vanham, G. Essentials in saline pharmacology for nasal or respiratory hygiene in times of COVID-19. Eur. J. Clin. Pharmacol. 2021, 77, 1275–1293. [Google Scholar] [CrossRef]
- Machado, R.R.G.; Glaser, T.; Araujo, D.B.; Petiz, L.L.; Oliveira, D.B.; Durigon, G.S.; Leal, A.T.; Pinho, J.R.R.; Ferreira, L.C.S.; Ulrich, H.; et al. Inhibition of severe acute respiratory syndrome coronavirus 2 replication by hypertonic saline solution in lung and kidney epithelial cells. ACS Pharmacol. Trans. Sci. 2021, 4, 1514–1527. [Google Scholar] [CrossRef] [PubMed]
- Speir, R.W. Effect of several inorganic salts on the infectivity of Mengo virus. Proc. Soc. Exp. Biol. Med. 1961, 106, 402–404. [Google Scholar] [CrossRef]
- Kasahara, K.; Kawakami, Y.; Kiyono, T.; Yonemura, S.; Kawamura, Y.; Era, S.; Matsuzaki, F.; Goshima, N.; Inagaki, M. Ubiquitin-proteasome system controls ciliogenesis at the initial step of axoneme extension. Nat. Commun. 2014, 5, 5081. [Google Scholar] [CrossRef] [Green Version]
- Akgun, E.; Tuzuner, M.B.; Sahin, B.; Kilercik, M.; Kulah, C.; Cakiroglu, H.N.; Serteser, M.; Unsal, I.; Baykal, A.T. Proteins associated with neutrophil degranulation are upregulated in nasopharyngeal swabs from SARS-CoV-2 patients. PLoS ONE 2020, 15, e0240012. [Google Scholar] [CrossRef]
- Smale, S. Differentiable dynamical systems. Bull. Am. Math. Soc. 1967, 73, 747–817. [Google Scholar] [CrossRef] [Green Version]
- Ashby, M.T. Inorganic chemistry of defensive peroxidases in the human oral cavity. J. Dent. Res. 2008, 87, 900–914. [Google Scholar] [CrossRef] [Green Version]
- Tenovuo, J.; Lehtonen, O.P.; Aaltonen, A.S.; Vilja, P.; Tuohimaa, P. Antimicrobial factors in whole saliva of human infants. Infect. Immun. 1986, 51, 49–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagl, M.; Arnitz, R.; Lackner, M. N-chlorotaurine, a promising future candidate for topical therapy of fungal infections. Mycopathologia 2018, n183, 161–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, N.; Yii, N.; Robinson, D. Xylitol nasal preparations in sinonasal disease: A literature review and meta-analysis. Aust. J. Otolaryngol. 2022, 5, 8. [Google Scholar] [CrossRef]
- Proksch, E.; de Bony, R.; Trapp, S.; Boudon, S. Topical use of dexpanthenol: A 70th anniversary article. J. Dermatol. Treat. 2017, 28, 766–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giarratana, G.; Rajan, B.; Kamala, K.; Mendenhall, M.; Reiner, G. A sprayable Acid-Oxidizing solution containing hypochlorous acid (AOS2020) efficiently and safely inactivates SARS-Cov-2: A new potential solution for upper respiratory tract hygiene. Arch. Otorhinolaryngol. 2021, 278, 3099–3103. [Google Scholar] [CrossRef]
- Liu, Y.; Yan, L.M.; Wan, L.; Xiang, T.X.; Le, A.; Liu, J.M.; Peiris, M.; Poon, L.L.; Zhang, W. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect. Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef] [Green Version]
- Masood, A.; Moumoulidis, I.; Panesar, J. Acute rhinosinusitis in adults: An update on current management. Postgrad. Med. J. 2007, 83, 402–408. [Google Scholar] [CrossRef] [Green Version]
- NHS England Updated UK Health Security Agency (UKHSA) Guidance–Isolation. Available online: https://www.england.nhs.uk/coronavirus/documents/updated-uk-health-security-agency-ukhsa-guidance-isolation/#Self%20isolation%20for%20NHS%20staff (accessed on 14 August 2022).
- European Centre for Disease Prevention and Control (ECDC). Guidance on Quarantine of Close Contacts to COVID-19 Cases and Isolation of COVID-19 Cases, in the Current Epidemiological Situation, 7 January 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/prevention-and-control/quarantine-and-isolation (accessed on 14 August 2022).
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Larese-Filon, F. SARS-CoV-2 Infection in Health Care Workers of Trieste (North-Eastern Italy), 1 October 2020–7 February 2022: Occupational Risk and the Impact of the Omicron Variant. Viruses 2022, 14, 1663. [Google Scholar] [CrossRef]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | % w/w |
|---|---|
| Panthenol | 5.0 |
| Xylitol | 5.0 |
| Seawater (Maris Aqua) | 10.0 |
| Lactic acid 90% | q.s. pH 4.8–5.0 |
| Purified water | q.s. 100% |
| Total | 100.00 |
| Variables | Categories | Treated (N = 50) N (%) | Controls (N = 58) N (%) | p-Value | |
|---|---|---|---|---|---|
| Sex | Female | 30 (60.0) | 35 (60.3) | 0.971 | |
| Male | 20 (40.0) | 23 (39.7) | |||
| Age (years) | <40 | 19 (42.2) | 22 (38.6) | 0.933 | |
| 40–59 | 20 (44.4) | 27 (47.4) | |||
| 60+ | 6 (13.3) | 8 (14.0) | |||
| Smoking status | Non-smoker | 36 (72.0) | 42 (72.4) | 0.530 | |
| Ex-smoker | 9 (18.0) | 7 (12.1) | |||
| Current smoker | 5 (10.0) | 9 (15.5) | |||
| Alcohol consumption | Non-drinker | 20 (40.0) | 19 (32.8) | 0.285 | |
| Occasional drinker | 29 (58.0) | 34 (58.6) | |||
| Regular drinker | 1 (2.0) | 5 (8.6) | |||
| Number of doses of COVID-19 vaccines | 0 | 5 (10.0) | 1 (1.7) | 0.148 | |
| 1 | 1 (2.0) | 0 | |||
| 2 | 5 (10.0) | 4 (6.9) | |||
| 3 | 39 (78.0) | 53 (91.4) | |||
| Vaccine type | 1st dose | Comirnaty | 36 (80.0) | 47 (82.5) | 0.480 |
| Spikevax | 6 (13.3) | 4 (7.0) | |||
| Vaxzevria | 3 (6.7) | 6 (10.5) | |||
| 2nd dose | Comirnaty | 35 (80.0) | 47 (82.5) | 0.710 | |
| Spikevax | 6 (13.6) | 5 (8.8) | |||
| Vaxzevria | 3 (6.8) | 5 (8.8) | |||
| 3rd dose | Comirnaty | 18 (46.2) | 19 (36.5) | 0.355 | |
| Spikevax | 21 (53.9) | 33 (63.5) | |||
| Vaxzevria | 0 | 0 | |||
| Hypertension (missing: 6) | No | 37 (82.2) | 47 (82.5) | 0.975 | |
| Yes | 8 (17.8) | 10 (17.5) | |||
| Diabetes | No | 49 (98.0) | 57 (98.3) | 0.916 | |
| Yes | 1 (1.8) | 1 (1.7) | |||
| Cardiovascular diseases | No | 50 (100) | 58 (100) | NA | |
| Yes | 0 | 0 | |||
| Cerebrovascular diseases | No | 49 (98.0) | 58 (100) | 0.279 | |
| Yes | 1 (1.8) | 0 | |||
| Cancer | No | 47 (94.0) | 54 (93.1) | 0.850 | |
| Yes | 3 (5.3) | 4 (6.9) | |||
| COPD | No | 42 (84.0) | 52 (89.7) | 0.383 | |
| Yes | 8 (14.0) | 6 (10.3) | |||
| Renal disease | No | 50 (100) | 57 (98.3) | 0.351 | |
| Yes | 0 | 1 (1.7) | |||
| Day | Treated | Controls | EER | CER | ARI | NNT (95%CI) | OR (95%CI) | HR (95%CI) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Daily | Pooled | Daily | Pooled | Daily | Pooled (95%CI) | ||||||
| 2 | 1 | 0 | 0.02 | 0.28 | 0 | 0.05 | 0.02 | 0.23 (0.10; 0.36) | 4 (3;10) | 7.39 (1.83; 29.8) | 6.12 (1.76; 21.32) |
| 3 | 3 | 0 | 0.06 | 0 | 0.06 | ||||||
| 4 | 5 | 0 | 0.1 | 0 | 0.10 | ||||||
| 5 | 5 | 3 | 0.1 | 0.05 | 0.05 | ||||||
| 6 | 3 | 3 | 0.06 | 0.05 | 0.01 | ||||||
| 7 | 12 | 16 | 0.24 | 0.66 | 0.28 | 0.89 | −0.04 | −0.24 (−0.09; −0.38) | NA | 0.22 (0.08; 0.65) | NA |
| 8 | 2 | 4 | 0.04 | 0.07 | −0.03 | ||||||
| 9 | 11 | 4 | 0.22 | 0.07 | 0.15 | ||||||
| 10 | 5 | 13 | 0.10 | 0.22 | −0.12 | ||||||
| 11 | 2 | 7 | 0.04 | 0.12 | −0.08 | ||||||
| 12 + | 1 | 8 | 0.02 | 0.14 | −0.12 | ||||||
| Total | 50 | 58 | |||||||||
| Symptoms and Use of Medicines | Treatment Arm (N = 50) | Control Arm (N = 58) | |||||
|---|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | ||
| Dry cough | No | 18 | 36 | <0.001 | 23 | 42 | <0.001 |
| Yes | 21 | 2 | 19 | 13 | |||
| Productive cough | No | 30 | 37 | 0.119 | 30 | 41 | 0.047 |
| Yes | 15 | 13 | 12 | 8 | |||
| Ear wadding | No | 31 | 41 | 0.029 | 30 | 45 | 0.003 |
| Yes | 45 | 13 | 12 | 7 | |||
| Stuffy nose | No | 14 | 32 | <0.001 | 13 | 28 | 0.001 |
| Yes | 21 | 24 | 22 | 14 | |||
| Runny nose | No | 13 | 31 | <0.001 | 18 | 36 | <0.001 |
| Yes | 24 | 16 | 24 | 13 | |||
| Frequent sneezing | No | 18 | 39 | <0.001 | 26 | 44 | <0.001 |
| Yes | 22 | 10 | 22 | 10 | |||
| Anosmia/ageusia | No | 37 | 39 | 0.662 | 41 | 43 | 0.710 |
| Yes | 7 | 10 | 7 | 6 | |||
| Lacrimation | No | 37 | 41 | 0.508 | 43 | 54 | 0.006 |
| Yes | 12 | 3 | 7 | 6 | |||
| Hoarseness | No | 16 | 36 | <0.001 | 15 | 40 | <0.001 |
| Yes | 25 | 18 | 24 | 10 | |||
| Feverish sensation | No | 20 | 43 | <0.001 | 20 | 53 | <0.001 |
| Yes | 34 | 4 | 25 | 5 | |||
| Sweating | No | 37 | 43 | 0.227 | 40 | 52 | 0.006 |
| Yes | 16 | 2 | 9 | 4 | |||
| Shivering | No | 29 | 46 | <0.001 | 37 | 54 | 0.002 |
| Yes | 20 | 1 | 18 | 3 | |||
| Headache | No | 22 | 38 | <0.001 | 21 | 47 | <0.001 |
| Yes | 27 | 10 | 17 | 11 | |||
| Throat discomfort | No | 25 | 44 | <0.001 | 16 | 44 | <0.001 |
| Yes | 30 | 12 | 23 | 7 | |||
| Sore throat | No | 27 | 35 | <0.001 | 20 | 50 | <0.001 |
| Yes | 31 | 7 | 20 | 5 | |||
| Aching sinusitis | No | 27 | 35 | 0.083 | 27 | 44 | 0.002 |
| Yes | 21 | 10 | 12 | 11 | |||
| Air hunger | No | 42 | 47 | 0.063 | 50 | 54 | 0.219 |
| Yes | 5 | 3 | 5 | 3 | |||
| Breath shortage | No | 33 | 40 | 0.119 | 43 | 45 | 0.712 |
| Yes | 9 | 6 | 11 | 6 | |||
| Anti-pyretic medications | No | 27 | 32 | 0.323 | 26 | 42 | 0.001 |
| Yes | 18 | 14 | 8 | 15 | |||
| Penicillin intake | No | 47 | 45 | 1.000 | 57 | 58 | 1.000 |
| Yes | 1 | 0 | 1 | 2 | |||
| Inhaling spray for COPD | No | 46 | 48 | 1.000 | 54 | 56 | 0.500 |
| Yes | 2 | 2 | 2 | 2 | |||
| Tablets for COPD | No | 46 | 50 | 0.125 | 56 | 56 | 1.000 |
| Yes | 1 | 1 | 4 | 0 | |||
| Antitussive drugs | No | 38 | 35 | 0.631 | 39 | 40 | 0.071 |
| Yes | 6 | 13 | 3 | 9 | |||
| Eye drop use | No | 49 | 50 | 1.000 | 54 | 56 | 1.000 |
| Yes | 2 | 2 | 1 | 0 | |||
| Nasal spray medications | No | 44 | 10 | 0.180 | 24 | 25 | <0.001 |
| Yes | 4 | 0 | 0 | 1 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cegolon, L.; Mastrangelo, G.; Emanuelli, E.; Camerotto, R.; Spinato, G.; Frezza, D. Early Negativization of SARS-CoV-2 Infection by Nasal Spray of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial. Pharmaceutics 2022, 14, 2502. https://doi.org/10.3390/pharmaceutics14112502
Cegolon L, Mastrangelo G, Emanuelli E, Camerotto R, Spinato G, Frezza D. Early Negativization of SARS-CoV-2 Infection by Nasal Spray of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial. Pharmaceutics. 2022; 14(11):2502. https://doi.org/10.3390/pharmaceutics14112502
Chicago/Turabian StyleCegolon, Luca, Giuseppe Mastrangelo, Enzo Emanuelli, Riccardo Camerotto, Giacomo Spinato, and Daniele Frezza. 2022. "Early Negativization of SARS-CoV-2 Infection by Nasal Spray of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial" Pharmaceutics 14, no. 11: 2502. https://doi.org/10.3390/pharmaceutics14112502