
Management of Patients with Diabetic Macular Edema Switched from Dexamethasone Intravitreal Implant to Fluocinolone Acetonide Intravitreal Implant

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Study Population
3.2. Prior DME Treatment
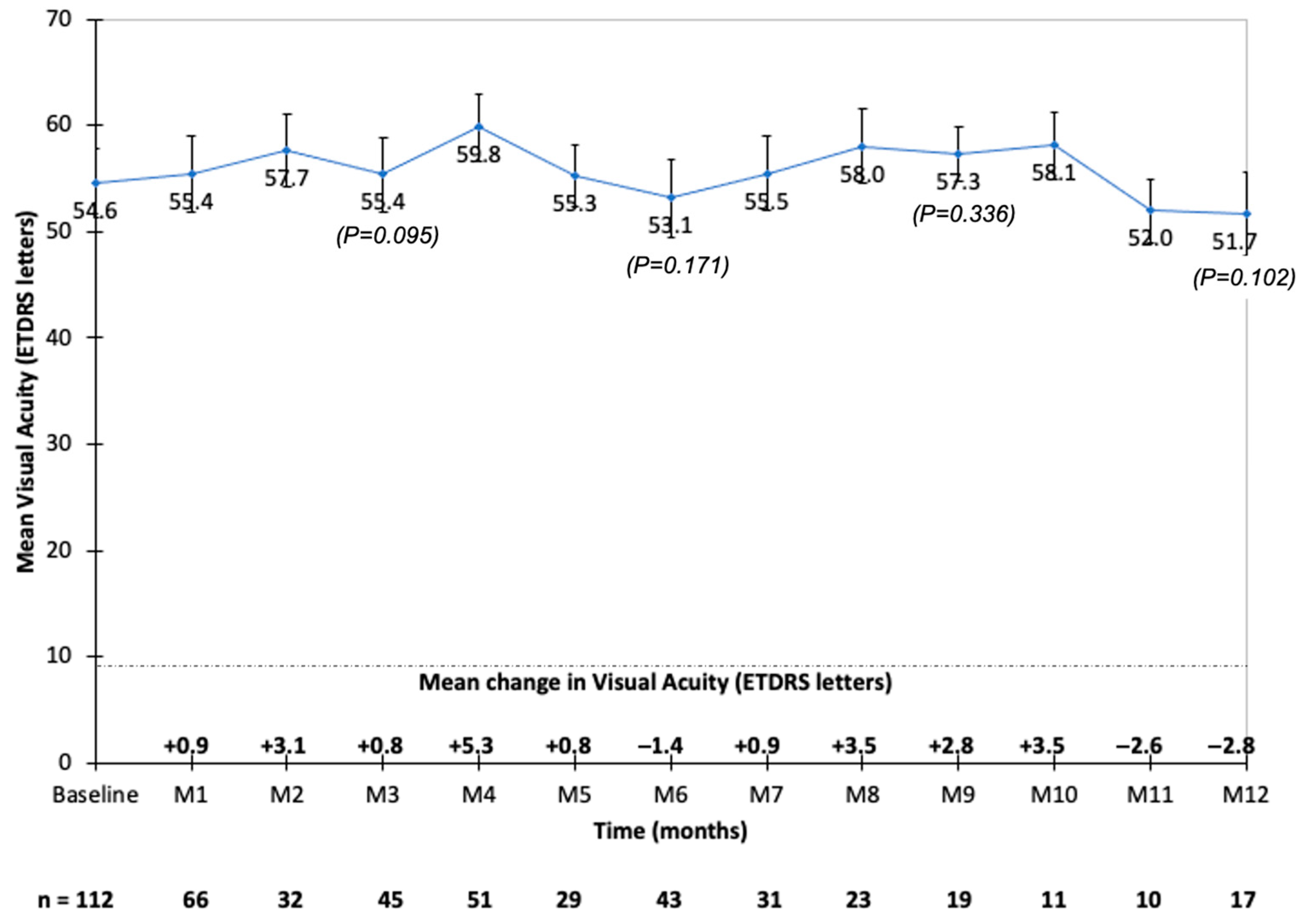
3.3. Visual Acuity
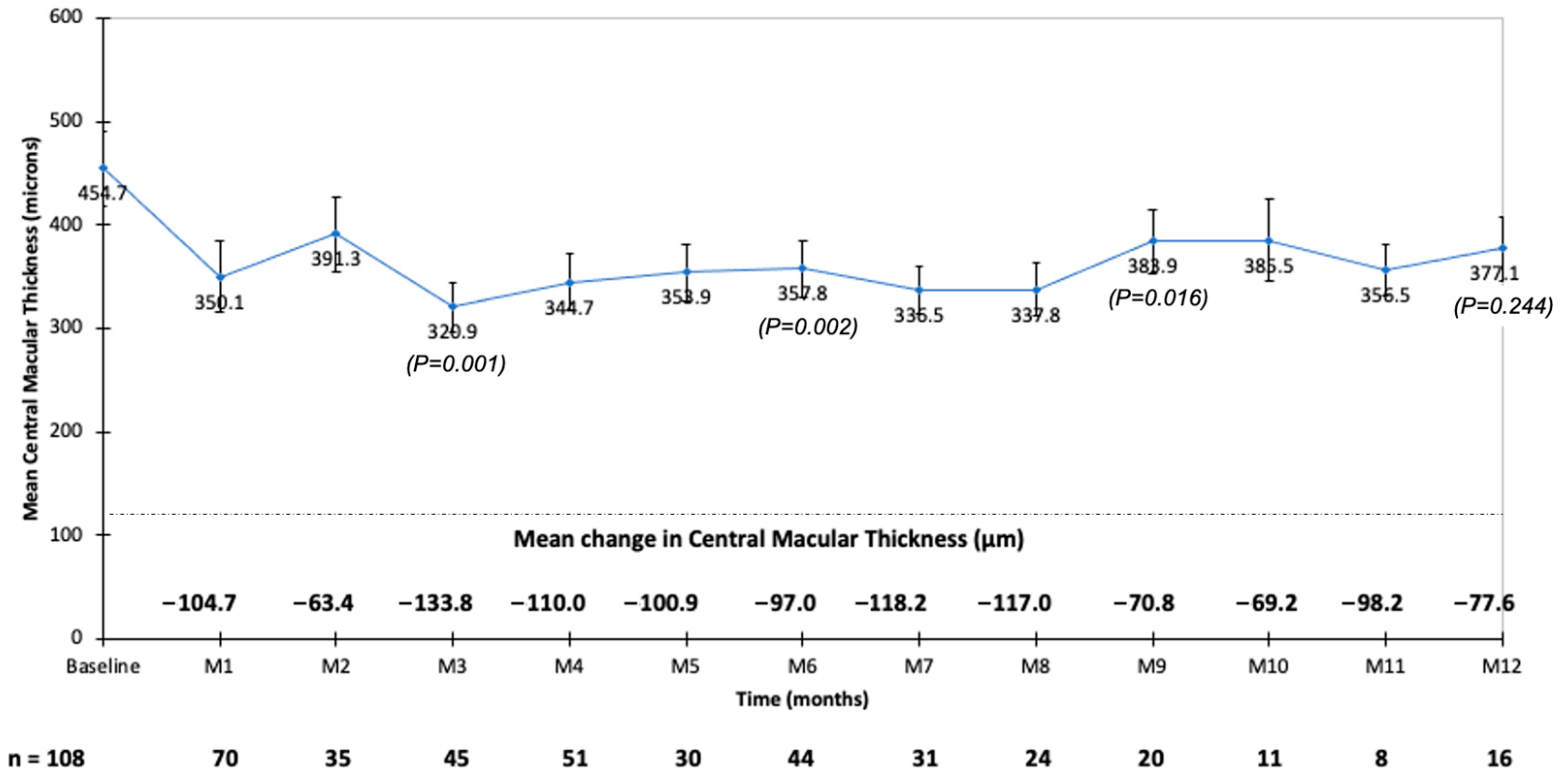
3.4. Retinal Thickness
3.5. Additional Treatments
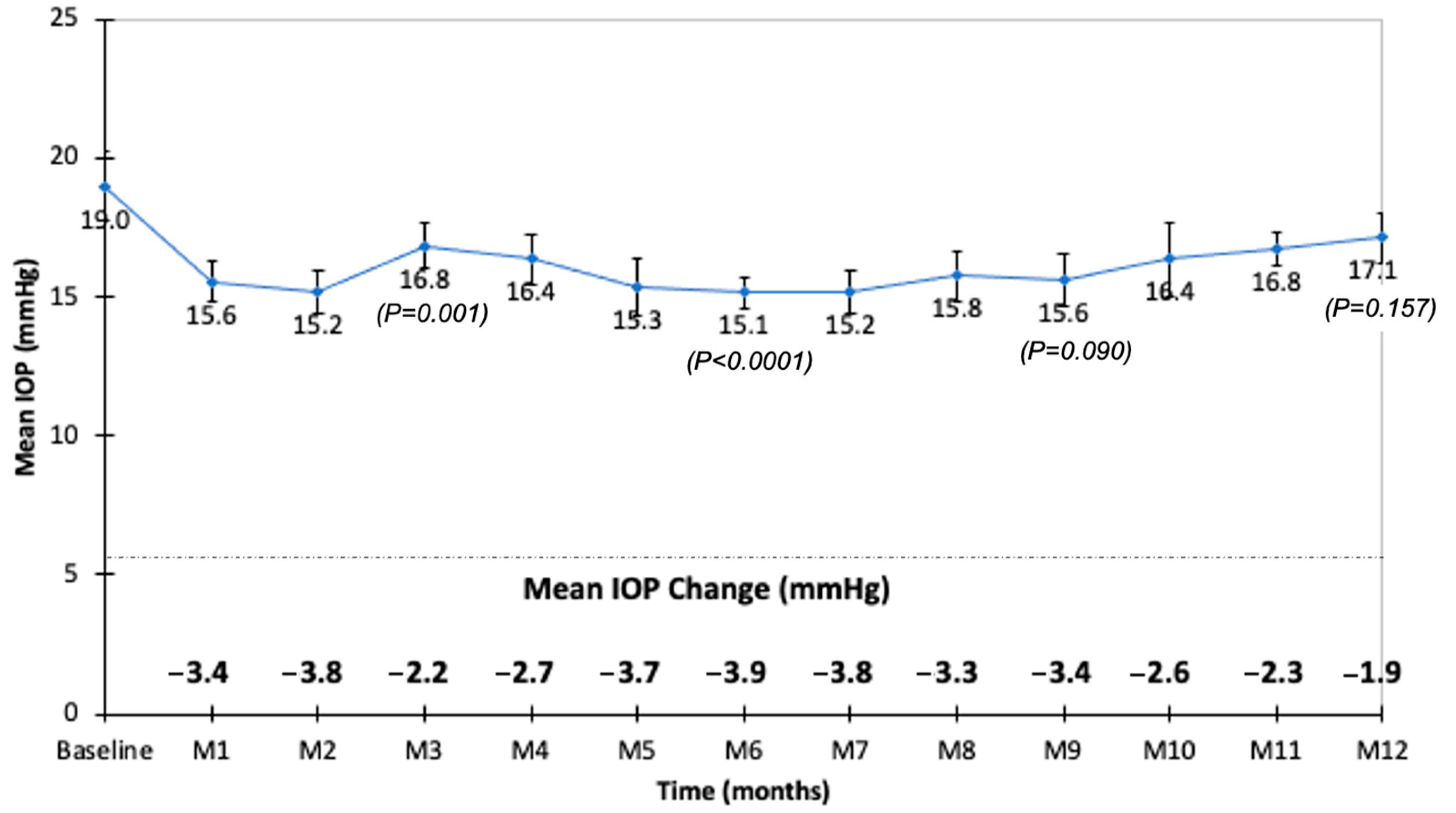
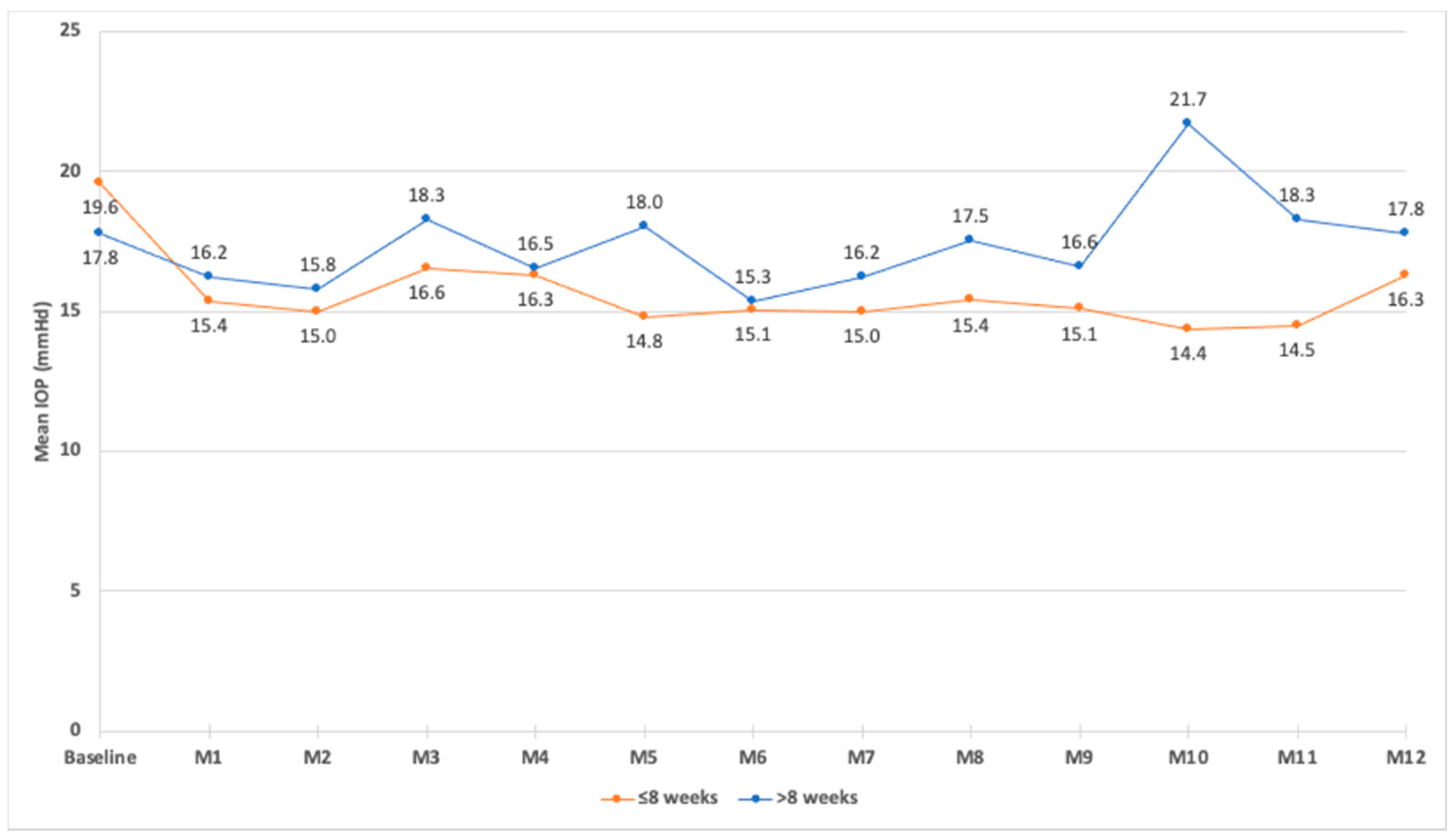
3.6. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solomon, S.D.; Chew, E.; Duh, E.J.; Sobrin, L.; Sun, J.K.; VanderBeek, B.L.; Wykoff, C.C.; Gardner, T.W. Diabetic retinopathy: A position statement by the American Diabetes Association. Diabetes Care 2017, 40, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.; Wong, T.Y.; Sabanayagam, C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015, 2, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yau, J.W.Y.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.; Klein, B.E.; Moss, S.E.; Cruickshanks, K.J. The Wisconsin Epidemiologic Study of Diabetic Retinopathy. XV. The long-term incidence of macular edema. Ophthalmology 1995, 102, 7–16. [Google Scholar] [CrossRef]
- Ferris, F.L.; Patz, A. Macular edema. A complication of diabetic retinopathy. Surv. Ophthalmol. 1984, 28, 52–61. [Google Scholar] [CrossRef]
- Haritoglou, C.; Neubauer, A.S.; Kernt, M. Fluocinolone acetonide and its potential in the treatment of chronic diabetic macular edema. Clin. Ophthalmol. 2013, 7, 503–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Zeng, H.; Bao, S.; Wang, N.; Gillies, M.C. Diabetic macular edema: New concepts in pathophysiology and treatment. Cell Biosci. 2014, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugel, P.U.; Parrish, R. ILUVIEN: A new approach to the treatment of diabetic macular edema. US Ophthalmic. Rev. 2015, 8, 110–115. [Google Scholar] [CrossRef]
- Peto, T. An overview of the clinical outcomes of the fluocinolone acetonide 190μg intravitreal implant clinical evidence study in the United Kingdom (ICE-UK). Curr. Med. Res. Opin. 2017, 33, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Bressler, N.M.; Beaulieu, W.T.; Glassman, A.R.; Blinder, K.J.; Bressler, S.B.; Jampol, L.M.; Melia, M.; Wells, J.A.; Diabetic retinopathy Clinical Research Network. Persistent macular thickening following intravitreous aflibercept, bevacizumab, or ranibizumab for central-Involved diabetic macular edema with vision impairment: A secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2018, 136, 257–269. [Google Scholar] [CrossRef]
- Ciulla, T.A.; Bracha, P.; Pollack, J.; Williams, F.D. Real-world outcomes of anti-vascular endothelial growth factor therapy in diabetic macular edema in the United States. Ophthalmol. Retin. 2018, 2, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Kodjikian, L.; Bellocq, D.; Mathis, T. Pharmacological management of diabetic macular edema in real-life observational studies. Biomed. Res. Int. 2018, 28, 8289253. [Google Scholar] [CrossRef] [PubMed]
- Danis, R.P.; Sadda, S.; Li, X.Y.; Cui, H.; Hashad, Y.; Whitcup, S.M. Anatomical effects of dexamethasone intravitreal implant in diabetic macular oedema: A pooled analysis of 3-year phase III trials. Br. J. Ophthalmol. 2016, 100, 796–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, K.; Khosrof, S.; Bursell, S.E.; Rohan, R.; Murata, T.; Clermont, A.C.; Aiello, L.P.; Ogura, Y.; Adamis, A.P. Prevention of leukostasis and vascular leakage in streptozotocin-induced diabetic retinopathy via intercellular adhesion molecule-1 inhibition. Proc. Natl. Acad. Sci. USA 1999, 96, 10836–10841. [Google Scholar] [CrossRef] [Green Version]
- Joussen, A.M.; Poulaki, V.; Le, M.L.; Koizumi, K.; Esser, C.; Janicki, H.; Schaermeyer, U.; Kociok, N.; Fauser, S.; Kirchhof, B.; et al. A central role for inflammation in the pathogenesis of diabetic retinopathy. FASEB J. 2004, 18, 1450–1452. [Google Scholar] [CrossRef]
- Boyer, D.S.; Yoon, Y.H.; Belfort, R.; Bandello, F.; Maturi, R.K.; Augustin, A.J.; Li, X.Y.; Cui, H.; Hashad, Y.; Whitcup, S.M.; et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology 2014, 121, 1904–1914. [Google Scholar] [CrossRef]
- Whitcup, S.M.; Cidlowski, J.A.; Csaky, K.G.; Ambati, J. Pharmacology of corticosteroids for diabetic macular edema. Invest Opthalmol. Vis. Sci. 2018, 59, 1–12. [Google Scholar] [CrossRef]
- Bucolo, C.; Gozzo, L.; Longo, L.; Mansueto, S.; Vitale, D.C.; Drago, F. Long-term efficacy and safety profile of multiple injections of intravitreal dexamethasone implant to manage diabetic macular edema: A systematic review of real-world studies. J. Pharmacol. Sci. 2018, 138, 219–232. [Google Scholar] [CrossRef]
- McCluskey, J.D.; Kaufman, P.L.; Wynne, K.; Lewis, G. Early adoption of the fluocinolone acetonide (FAc) intravitreal implant in patients with persistent or recurrent diabetic macular edema (DME). Int. Med. Case. Rep. J. 2019, 12, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Malclès, A.; Dot, C.; Voirin, N.; Agard, E.; Vié, A.L.; Bellocq, D.; Denis, P.; Kodjikian, L. Real-life study in diabetic macular edema treated with dexamethasone implant: The RELDEX study. Retina 2017, 37, 753–760. [Google Scholar] [CrossRef]
- Bellocq, D.; Akesbi, J.; Matonti, F.; Vartin, C.; Despreaux, R.; Comet, A.; Voirin, N.; Denis, P.; Mathis, T.; Kodjikian, L. The pattern of recurrence in diabetic macular edema treated by dexamethasone implant: The PREDIAMEX study. Ophthalmol. Retin. 2018, 2, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Nguyen, Q.D.; Hafiz, G.; Bloom, S.; Brown, D.M.; Busquets, M.; Ciulla, T.; Feiner, L.; Sabates, L.; Billman, K.; et al. Aqueous levels of fluocinolone acetonide after administration of fluocinolone acetonide inserts or fluocinolone acetonide implants. Ophthalmology 2013, 120, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Hafiz, G.; Shah, S.M.; Bloom, S.; Brown, D.M.; Busquets, M.; Ciulla, T.; Feiner, L.; Sabates, L.; Billman, K.; et al. Sustained ocular delivery of fluocinolone acetonide by an intravitreal insert. Ophthalmology 2010, 117, 1393–1399. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Brown, D.M.; Pearson, A.; Chen, S.; Boyer, D.; Ruiz-Moreno, J.; Garretson, B.; Gupta, A.; Hariprasad, S.M.; Bailey, C.; et al. Sustained Delivery Fluocinolone Acetonide Vitreous Inserts Provide Benefit for at Least 3 Years in Patients with Diabetic Macular Edema. Ophthalmology 2012, 119, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Callanan, D.G.; Gupta, S.; Boyer, D.S.; Ciulla, T.A.; Singer, M.A.; Kuppermann, B.D.; Liu, C.C.; Li, X.Y.; Hollander, D.A.; Schiffman, R.M.; et al. Dexamethasone intravitreal implant in combination with laser photocoagulation for the treatment of diffuse diabetic macular edema. Ophthalmology 2013, 120, 1843–1851. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.; Chakravarthy, U.; Lotery, A.; Menon, G.; Talks, J.; Medisoft Audit Group. Extended real-world experience with the ILUVIEN (fluocinolone acetonide) implant in the United Kingdom: 3-year results from the Medisoft audit study. Eye 2022, 36, 1012–1018. [Google Scholar] [CrossRef]
- Chakravarthy, U.; Taylor, S.R.; Koch, F.H.J.; Castro de Sousa, J.P.; Bailey, C.; ILUVIEN Registry Safety Study (IRISS) Investigators Group. Changes in intraocular pressure after intravitreal fluocinolone acetonide (ILUVIEN): Real-world experience in three European countries. Br. J. Ophthalmol. 2019, 103, 1072–1077. [Google Scholar] [CrossRef] [Green Version]
- Eaton, A.; Koh, S.S.; Jimenez, J.; Riemann, C.D. The USER Study: A chart review of patients receiving a 0.2 μg/day fluocinolone acetonide implant for diabetic macular edema. Ophthalmol. Ther. 2019, 8, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Kodjikian, L.; Baillif, S.; Creuzot-Garcher, C.; Delyfer, M.N.; Matonti, F.; Weber, M.; Mathis, T. Real-world efficacy and safety of fluocinolone acetonide implant for diabetic macular edema: A systematic review. Pharmaceutics 2021, 13, 72. [Google Scholar] [CrossRef]
- Hussain, R.M.; Ciulla, T.A. Treatment strategies for refractory diabetic macular edema: Switching anti-VEGF treatments, adopting corticosteroid-based treatments, and combination therapy. Expert Opin. Biol. Ther. 2016, 16, 365–374. [Google Scholar] [CrossRef]
- Carneiro, A.; Meireles, A.; Castro Sousa, J.P.; Teixeira, C. Clinical impact of the 0.2 μg/day fluocinolone acetonide intravitreal implant: Outcomes from the ILUVIEN clinical evidence study in Portugal. Ther. Adv. Ophthalmol. 2020, 12, 2515841420917768. [Google Scholar] [CrossRef] [PubMed]
- Kodjikian, L.; Bellocq, D.; Bandello, F.; Loewenstein, A.; Chakravarthy, U.; Koh, A.; Augustin, A.; de Smet, M.D.; Chhablani, J.; Tufail, A.; et al. First-line treatment algorithm and guidelines in center-involving diabetic macular edema. Eur. J. Ophthalmol. 2019, 29, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Rehak, M.; Busch, C.; Unterlauft, J.D.; Jochmann, C.; Wiedemann, P. Outcomes in diabetic macular edema switched directly or after a dexamethasone implant to a fluocinolone acetonide intravitreal implant following anti-VEGF treatment. Acta Diabetol. 2020, 57, 469–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicinelli, M.V.; Rosenblatt, A.; Grosso, D.; Zollet, P.; Capone, L.; Rabiolo, A.; Lattanzio, R.; Loewenstein, A.; Bandello, F.; International Retina Collaborative. Correction: The outcome of fluocinolone acetonide intravitreal implant is predicted by the response to dexamethasone implant in diabetic macular oedema. Eye 2021, 35, 3459. [Google Scholar] [CrossRef] [PubMed]
- Elbarky, A.M. Effectiveness and tolerability of the fluocinolone acetonide implant in patients with diabetic macular edema in UAE: 12-Month results. Eur. J. Ophthalmol. 2021, 31, 3196–3202. [Google Scholar] [CrossRef] [PubMed]
- Vaz-Pereira, S.; Castro-de-Sousa, J.P.; Martins, D.; Canelas, J.P.; Reis, P.; Sampaio, A.; Urbano, H.; Kaku, P.; Nascimento, J.; Marques-Neves, C. The outcomes of switching from short- to long-term intravitreal corticosteroid implant therapy in patients with diabetic macular edema. Ophthalmic. Res. 2020, 63, 114–121. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Brown, D.M.; Pearson, A.; Ciulla, T.; Boyer, D.; Holz, F.G.; Tolentino, M.; Gupta, A.; Duarte, L.; Madreperla, S.; et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology 2011, 118, 626–635. [Google Scholar] [CrossRef]
- Augustin, A.J.; Bopp, S.; Fechner, M.; Holz, F.; Sandner, D.; Winkgen, A.M.; Khoramnia, R.; Neuhann, T.; Warscher, M.; Spitzer, M.; et al. Three-year results from the Retro-IDEAL study: Real-world data from diabetic macular edema (DME) patients treated with ILUVIEN® (0.19 mg fluocinolone acetonide implant). Eur. J. Ophthalmol. 2020, 30, 382–391. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C.; Chakravarthy, U.; Lotery, A.; Menon, G.; Talks, J.; Medisoft Audit Group Real-world experience with 0. 2 μg/day fluocinolone acetonide intravitreal implant (ILUVIEN) in the United Kingdom. Eye 2017, 31, 1707–1715. [Google Scholar] [CrossRef] [Green Version]
- Chang-Lin, J.E.; Attar, M.; Acheampong, A.A.; Robinson, M.R.; Whitcup, S.M.; Kuppermann, B.D.; Welty, D. Pharmacokinetics and pharmacodynamics of a sustained-release dexamethasone intravitreal implant. Investig. Ophthalmol. Vis. Sci. 2011, 52, 80–86. [Google Scholar] [CrossRef]
- Kodjikian, L.; Bandello, F.; de Smet, M.; Dot, C.; Zarranz-Ventura, J.; Loewenstein, A.; Sudhalkar, A.; Bilgic, A.; Cunha-Vaz, J.; Dirven, W.; et al. Fluocinolone acetonide implant in diabetic macular edema: International expers’ panel consensus guidelines and treatment algorithm. Eur. J. Ophthalmol. 2022, 10, 11206721221080288. [Google Scholar] [CrossRef] [PubMed]
- Sadda, S.R.; Campbell, J.; Dugel, P.U.; Holekamp, N.L.; Kiss, S.; Loewenstein, A.; Augustin, A.J.; Shih, V.; Xu, X.; Wykoff, C.C.; et al. Relationship between duration and extend of oedema and visual acuity outcome with ranibizumab in diabetic macular edema: A post hoc analysis of protocol I data. Eye 2020, 34, 480–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, M.; Osher, J.; Riemann, C.D. Fluocinolone acetonide (0.19 mg) intravitreal implant reduces treatment burden and improves practice resource utilization for patients with diabetic macular edema. BMJ Open Ophthalmol. 2020, 5, e000416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, C.D.; Eaton, A.M.; Cutino, A. Reduction in retinal thickness fluctuations after treatment with fluocinolone acetonide implant for DME: A post-hoc analysis of the USER study. Ophthalmic. Surg. Lasers Imaging Retin. 2020, 51, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Schechet, S.A.; Adams, O.E.; Eichenbaum, D.A.; Hariprasad, S.M. Macular thickness amplitude changes when switching from discontinuous to continuous therapy for diabetic macular oedema. BMJ Open Ophthalmol. 2019, 4, e000271. [Google Scholar] [CrossRef] [PubMed]
- Holden, S.E.; Habib, M.; Currie, C.J. Retinal thickness fluctuations in patients receiving fluocinolone acetonide implant for diabetic macular edema. Curr. Med. Res. Opin. 2020, 36, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Mansour, S.E.; Kiernan, D.F.; Roth, D.B.; Eichenbaum, D.; Holekamp, N.M.; Kaba, S.; Werts, E. Two-year interim safety results of the 0.2 µg/day fluocinolone acetonide intravitreal implant for the treatment of diabetic macular oedema: The observational PALADIN study. Br. J. Ophthalmol. 2021, 105, 414–419. [Google Scholar] [CrossRef]
- Edelman, J.L. Differentiating intraocular glucocorticoids. Ophthalmologica 2010, 224 (Suppl. 1), 25–30. [Google Scholar] [CrossRef]
- Kane, F.E.; Green, K.E. Ocular pharmacokinetics of flu- ocinolone acetonide following Iluvien implantation in the vitreous humor of rabbits. J. Ocul. Pharmacol. Ther. 2015, 31, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Coney, J.M. Fluocinolone acetonide 0.19 mg intravitreal implant improves foveal thickness and reduces treatment burden for up to 1 year in eyes with persistent diabetic macular edema. Int. Med. Case Rep. J. 2019, 12, 161–169. [Google Scholar] [CrossRef]
- Yang, Y.; Bailey, C.; Loewenstein, A.; Massin, P. Intravitreal corticosteroids in diabetic macular edema: Pharmacokinetic considerations. Retina 2015, 35, 2440–2449. [Google Scholar] [CrossRef] [PubMed]
- Parrish, R.K.; Campochiaro, P.A.; Pearson, P.A.; Green, K.; Traverso, C.E. FAME Study Group. Characterization of intraocular pressure increases and management strategies following treatment with fluocinolone acetonide intravitreal implants in the FAME trials. Ophthalmol. Surg. Lasers Imaging Retin. 2016, 47, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenkranz, M.S.; Haller, J.A.; Kupperman, B.D.; Williams, G.A.; Ip, M.; Davis, M.; Weinberg, D.V.; Chou, C.; Whitcup, S.C. Correlation of visual acuity and macular thickness measured by optical coherence tomography in patients with persistent macular edema. Retina 2010, 30, 1090–1094. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Demographics | n | |
|---|---|---|
| Age, years (mean ± SD) | 69.8 ± 10.2 | 107 |
| Gender, male/female (n (%)) | 55 (48.7)/58 (51.3) | 113 |
| Type of diabetes, n (%) | 108 | |
| Type 2 | 100 (89.3) | |
| Type 1 | 8 (7.1) | |
| Insulin therapy, n (%) | 67 (62.6) | 107 |
| Diabetes duration, years (mean ± SD) | 21.9 ± 12.7 | 93 |
| HbA1c level, mean (%) | 7.4 ± 0.1 | 80 |
| High blood pressure, n (%) | 71 (70.3) | 101 |
| Ocular characteristics | n | |
| Laterality, n (%) | 113 | |
| OD | 61 (54) | |
| OS | 52 (46) | |
| Diabetic macular edema duration, months (mean ± SD [range]) | 71.8 ± 48.2 [15–360] | 104 |
| PDR n (%) | 6 (5.6) | 108 |
| NPDR, n (%) | 32 (29.6) | 108 |
| PRP, n (%) | 70 (64.8) | 108 |
| Pseudophakic, n (%) | 103 (91.2) | 113 |
| IOP-lowering medications, n (%) | 23 (25.6) | 90 |
| Monotherapy | 12 (52.2) | |
| Dual therapy | 9 (39.1) | |
| Triple therapy | 2 (8.7) | |
| Prior vitrectomy, n (%) | 30 (27.3) | 110 |
| Prior ERM peeling, n (%) | 19 (18.1) | 110 |
| ERM, n (%) | 14 (13.3) | 105 |
| BCVA, ETDRS letters (mean ± SD) | 54.1 ± 17.8 | 113 |
| CMT, μm (mean ± SD) | 454.7 ± 196.7 | 108 |
| IOP, mmHg (mean ± SD) | 19.0 ± 4.5 | 74 |
| Prior Treatments | n | |
|---|---|---|
| Intravitreal DEX, n (%) | 113 (100) | 113 |
| Number of DEX injections per eye (mean ± SD [range]) | 6.3 ± 4.5 [1–21] | 113 |
| Time between two DEX injections, weeks (mean ± SD) | 14.8 ± 4.5 | 69 |
| Time between the last DEX injection and the first FAc injection, weeks (mean ± SD [range]) | 11.12 ± 22 [1–163] | 102 |
| Macular laser therapy, n (%) | 27 (26.2) | 103 |
| Intravitreal triamcinolone, n (%) | 13 (11.5) | 113 |
| Peribulbar triamcinolone, n (%) | 5 (4.4) | 113 |
| Intravitreal ranibizumab, n (%) | 72 (63.7) | 113 |
| Number of ranibizumab injections per eye (mean ± SD [range]) | 7.9 ± 5.8 [2–23] | 72 |
| Intravitreal aflibercept, n (%) | 49 (43.4) | 113 |
| Number of aflibercept injections per eye (mean ± SD [range]) | 7.53 ± 8.3 [1–36] | 47 |
| Intravitreal bevacizumab, n (%) | 10 (8.9) | 113 |
| Number of bevacizumab injections per eye (mean ± SD [range]) | 1.6 ± 1.8 [1–6] | 8 |
| Month 1 | Month 3 | Month 6 | Month 12 | |
|---|---|---|---|---|
| Number of eyes | 67 | 46 | 44 | 20 |
| VA gain ≥ 5 ETDRS letters | 36% | 41% | 45% | 40% |
| VA gain ≥ 10 ETDRS letters | 19% | 24% | 32% | 35% |
| VA gain ≥ 15 ETDRS letters | 9% | 15% | 20% | 20% |
| VA stability (±4 ETDRS letters) | 42% | 39% | 27% | 25% |
| VA loss ≥ 5 ETDRS letters | 21% | 17% | 25% | 0% |
| p | |
|---|---|
| Diabetes mellitus duration | 0.009 |
| Diabetic macular edema duration | 0.973 |
| Age | 0.552 |
| Associated high blood pressure | 0.927 |
| HbA1c level | 0.544 |
| Stage of diabetic retinopathy | 0.068 |
| Baseline BCVA (prior to FAc injection) | 0.599 |
| Baseline CMT (prior to FAc injection) | 0.003 |
| Time between the last DEX injection and the first FAc injection | 0.035 |
| Number of prior DEX injections | 0.273 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baillif, S.; Staccini, P.; Weber, M.; Delyfer, M.-N.; Le Mer, Y.; Gualino, V.; Collot, L.; Merite, P.-Y.; Creuzot-Garcher, C.; Kodjikian, L.; et al. Management of Patients with Diabetic Macular Edema Switched from Dexamethasone Intravitreal Implant to Fluocinolone Acetonide Intravitreal Implant. Pharmaceutics 2022, 14, 2391. https://doi.org/10.3390/pharmaceutics14112391
Baillif S, Staccini P, Weber M, Delyfer M-N, Le Mer Y, Gualino V, Collot L, Merite P-Y, Creuzot-Garcher C, Kodjikian L, et al. Management of Patients with Diabetic Macular Edema Switched from Dexamethasone Intravitreal Implant to Fluocinolone Acetonide Intravitreal Implant. Pharmaceutics. 2022; 14(11):2391. https://doi.org/10.3390/pharmaceutics14112391
Chicago/Turabian StyleBaillif, Stéphanie, Pascal Staccini, Michel Weber, Marie-Noëlle Delyfer, Yannick Le Mer, Vincent Gualino, Laurence Collot, Pierre-Yves Merite, Catherine Creuzot-Garcher, Laurent Kodjikian, and et al. 2022. "Management of Patients with Diabetic Macular Edema Switched from Dexamethasone Intravitreal Implant to Fluocinolone Acetonide Intravitreal Implant" Pharmaceutics 14, no. 11: 2391. https://doi.org/10.3390/pharmaceutics14112391