
Topical Wound Treatment with a Nitric Oxide-Releasing PDE5 Inhibitor Formulation Enhances Blood Perfusion and Promotes Healing in Mice
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation and Characterization of a TOP-N53 Formulation in a Liquid Hydrogel
2.2. Cell Culture
2.3. MTT Assay
2.4. Measurement of cGMP Levels in Human Platelets
2.5. Animals and Wound Healing Experiments
2.6. Histology
2.7. Immunohistochemistry and Immunofluorescence Staining
2.8. Large-Scale Optoacoustic Microscopy (LSOM)
2.9. Large-Scale Dorsal Skin Imaging
2.10. Automatic Vessel Segmentation and Analysis Algorithm (AVSA) for Skin Vasculature
2.11. Statistical Analysis
3. Results
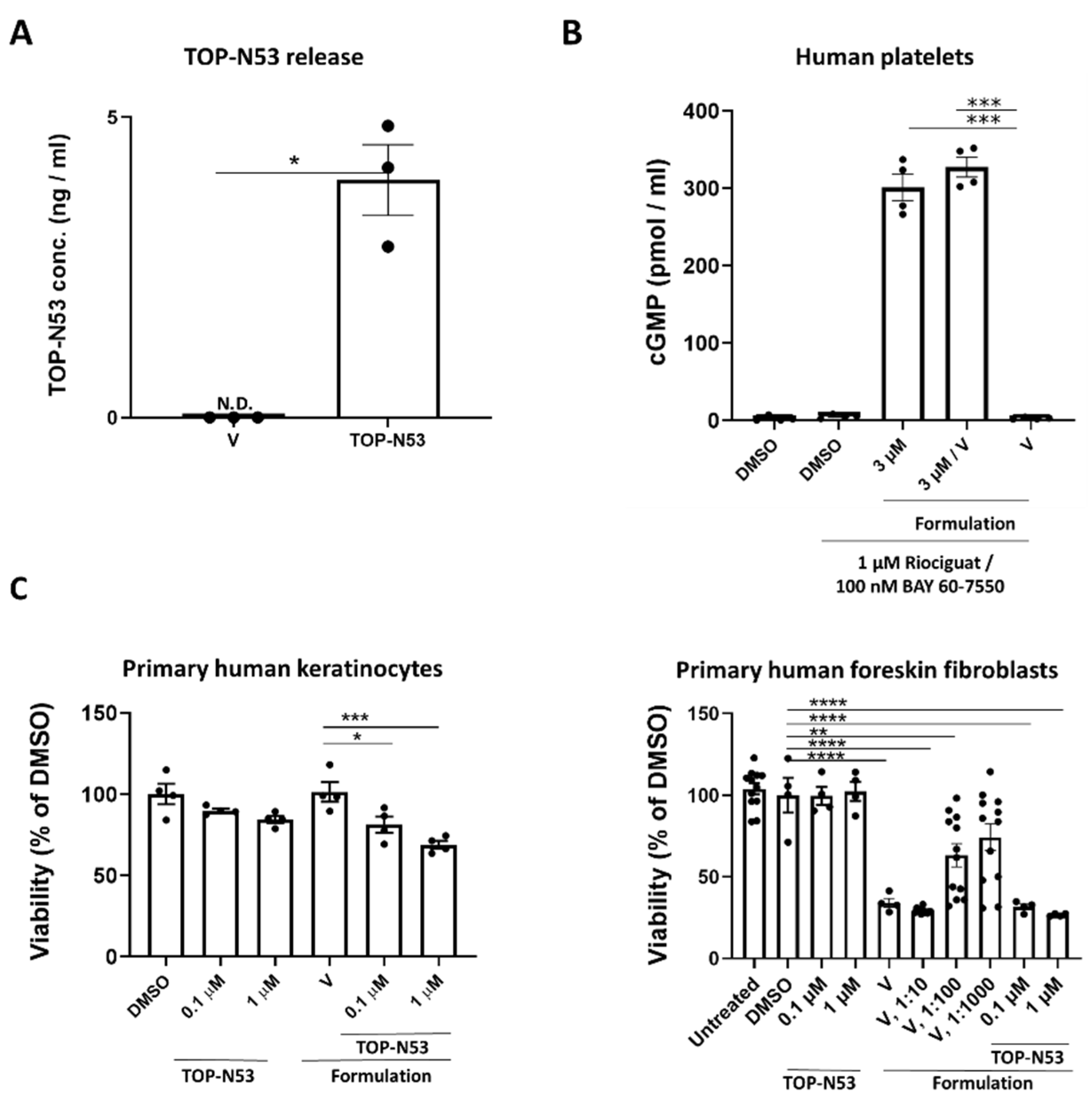
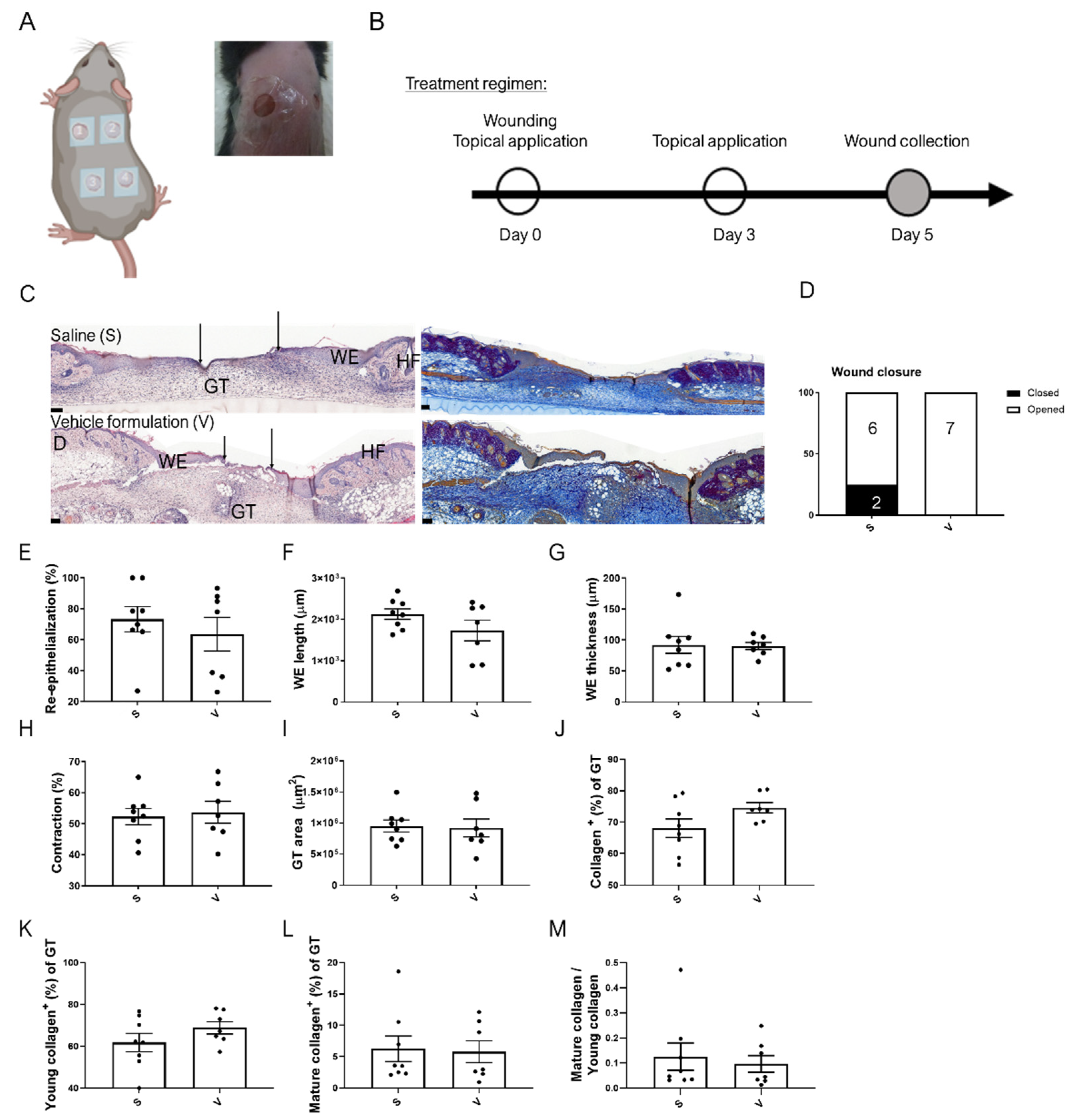
3.1. Preparation of a Non-Toxic TOP-N53 Liquid Hydrogel Formulation, Which Does Not Impair the Wound Healing Process
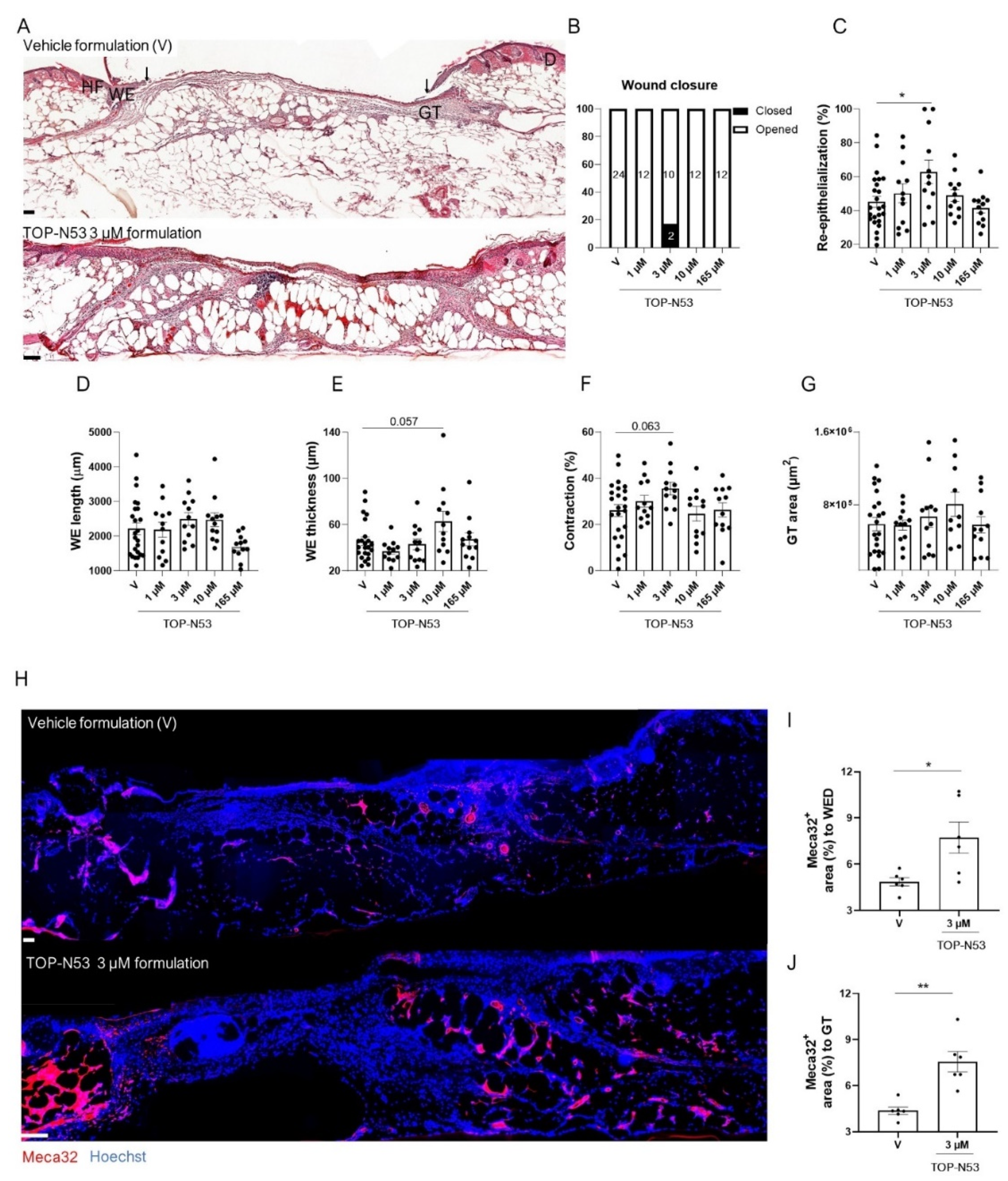
3.2. Topical TOP-N53 Formulation Increases Keratinocyte Proliferation and Wound Angiogenesis in Healthy Mice
3.3. Topical TOP-N53 Formulation Promotes Wound Re-Epithelialization and Angiogenesis in Healing-Impaired Diabetic Mice
3.4. Topical Application of TOP-N53 Liquid Hydrogel Formulation Enhances Wound Blood Flow and Microvascular Network Density in SKH-1 Mice
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Martin, P. Wound healing—Aiming for perfect skin regeneration. Science 1997, 276, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 2014, 6, 265sr266. [Google Scholar] [CrossRef] [Green Version]
- Sen, C.K.; Gordillo, G.M.; Roy, S.; Kirsner, R.; Lambert, L.; Hunt, T.K.; Gottrup, F.; Gurtner, G.C.; Longaker, M.T. Human skin wounds: A major and snowballing threat to public health and the economy. Wound Repair. Regen. 2009, 17, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Makrantonaki, E.; Wlaschek, M.; Scharffetter-Kochanek, K. Pathogenesis of wound healing disorders in the elderly. J. Dtsch. Dermatol. Ges. 2017, 15, 255–275. [Google Scholar] [CrossRef]
- Dabiri, G.; Damstetter, E.; Phillips, T. Choosing a wound dressing based on common wound characteristics. Adv. Wound Care 2016, 5, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.G.; Chou, J.J.; Hammond, P. Approaches to modulate the chronic wound environment using localized nucleic acid delivery. Adv. Wound Care 2020, 10, 503–528. [Google Scholar] [CrossRef]
- Hicks, C.W.; Selvarajah, S.; Mathioudakis, N.; Sherman, R.L.; Hines, K.F.; Black III, J.H.; Abularrage, C.J. Burden of infected diabetic foot ulcers on hospital admissions and costs. Ann. Vasc. Surg. 2016, 33, 149–158. [Google Scholar] [CrossRef]
- Jones, R.E.; Foster, D.S.; Longaker, M.T. Management of Chronic Wounds—2018. JAMA 2018, 320, 1481–1482. [Google Scholar] [CrossRef]
- Kang, Y.; Kim, J.; Lee, Y.M.; Im, S.; Park, H.; Kim, W.L. Nitric oxide-releasing polymer incorporated ointment for cutaneous wound healing. J. Control Release 2015, 220, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Witte, M.; Kiyama, T.; Barbul, A. Nitric oxide enhances experimental wound healing in diabetes. Br. J. Surg. 2002, 89, 1594–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Dayyih, W.; Abu Rayyan, W.; Al-Matubsi, H. Impact of sildenafil-containing ointment on wound healing in healthy and experimental diabetic rats. Acta Diabetol. 2020, 57, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Kulshrestha, S.; Chawla, R.; Singh, S.; Yadav, P.; Sharma, N.; Goel, R.; Ojha, H.; Kumar, V.; Adhikari, J.S. Protection of sildenafil citrate hydrogel against radiation-induced skin wounds. Burns 2020, 46, 1157–1169. [Google Scholar] [CrossRef] [PubMed]
- Ben-Yehuda Greenwald, M.; Tacconi, C.; Jukic, M.; Joshi, N.; Hiebert, P.; Brinckmann, J.; Tenor, H.; Naef, R.; Werner, S. A Dual-Acting Nitric Oxide Donor and Phosphodiesterase 5 Inhibitor Promotes Wound Healing in Normal Mice and Mice with Diabetes. J. Investig. Dermatol. 2021, 141, 415–426. [Google Scholar] [CrossRef]
- Gambaryan, S.; Kobsar, A.; Rukoyatkina, N.; Herterich, S.; Geiger, J.; Smolenski, A.; Lohmann, S.M.; Walter, U. Thrombin and collagen induce a feedback inhibitory signaling pathway in platelets involving dissociation of the catalytic subunit of protein kinase a from an NFκB-IκB complex. J. Biol. Chem. 2010, 285, 18352–18363. [Google Scholar] [CrossRef] [Green Version]
- Herovici, C. Picropolychrome: Histological staining technic intended for the study of normal and pathological connective tissue. Rev. Fr. Etud. Clin. Biol. 1963, 8, 88–89. [Google Scholar]
- Rebling, J.; Ben-Yehuda Greenwald, M.; Wietecha, M.; Werner, S.; Razansky, D. Long-term imaging of wound angiogenesis with large scale optoacoustic microscopy. Adv. Sci. 2021, 8, 2004226. [Google Scholar] [CrossRef]
- Liu, Y.-H.; Brunner, L.M.; Rebling, J.; Ben-Yehuda Greenwald, M.; Werner, S.; Detmar, M.; Razansky, D. Non-invasive longitudinal imaging of VEGF-induced microvascular alterations in skin wounds. Theranostics 2022, 12, 558. [Google Scholar] [CrossRef]
- Naef, R.; Tenor, H. 2-phenyl-3,4-dihydropyrrolo[2,1-f] [1,2,4] Triazinone Derivatives as Phosphodiesterase Inhibitors and Uses Thereof. 2017. Available online: https://patentscope.wipo.int/search/en/detail.jsf?docId=US362945719&_cid=P21-L4MRIT-92997-1 (accessed on 22 February 2022).
- Tavakoli, S.; Klar, A.S. Advanced Hydrogels as Wound Dressings. Biomolecules 2020, 10, 1169. [Google Scholar] [CrossRef]
- Tsuboi, R.; Rifkin, D.B. Recombinant basic fibroblast growth factor stimulates wound healing in healing-impaired db/db mice. J. Exp. Med. 1990, 172, 245–251. [Google Scholar] [CrossRef]
- Benavides, F.; Oberyszyn, T.M.; VanBuskirk, A.M.; Reeve, V.E.; Kusewitt, D.F. The hairless mouse in skin research. J. Dermatol. Sci. 2009, 53, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciris, P.A.; Qiu, M.; Constable, R.T. Noninvasive MRI measurement of the absolute cerebral blood volume–cerebral blood flow relationship during visual stimulation in healthy humans. Magn. Reson. Med. 2014, 72, 864–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.; Luo, F.; Li, Z.; Zhao, X.; Li, S.J. Transient relationships among BOLD, CBV, and CBF changes in rat brain as detected by functional MRI. Magn. Reson. Med. 2002, 48, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Frykberg, R.G.; Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 2015, 1, 560–582. [Google Scholar] [CrossRef] [Green Version]
- Haensel, D.; Dai, X. Epithelial-to-mesenchymal transition in cutaneous wound healing: Where we are and where we are heading. Dev. Dyn. 2018, 247, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Krischel, V.; Bruch-Gerharz, D.; Suschek, C.; Kröncke, K.-D.; Ruzicka, T.; Kolb-Bachofen, V. Biphasic effect of exogenous nitric oxide on proliferation and differentiation in skin derived keratinocytes but not fibroblasts. J. Investig. Dermatol. 1998, 111, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Dinh, T.; Veves, A. Microcirculation of the diabetic foot. Curr. Pharm. Des. 2005, 11, 2301–2309. [Google Scholar] [CrossRef]
- Okonkwo, U.; DiPietro, L. Diabetes and wound angiogenesis. Int. J. Mol. Sci. 2017, 18, 1419. [Google Scholar] [CrossRef] [Green Version]
- Campbell, L.; Saville, C.R.; Murray, P.J.; Cruickshank, S.M.; Hardman, M.J. Local arginase 1 activity is required for cutaneous wound healing. J. Investig. Dermatol. 2013, 133, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Kolluru, G.K.; Bir, S.C.; Kevil, C.G. Endothelial dysfunction and diabetes: Effects on angiogenesis, vascular remodeling, and wound healing. Int. J. Vasc. Med. 2012, 2012, 918267. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, L.A. Angiogenesis and wound repair: When enough is enough. J. Leukoc. Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cangkrama, M.; Wietecha, M.; Werner, S. Wound Repair, Scar Formation, and Cancer: Converging on Activin. Trends Mol. Med. 2020, 26, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Hiebert, P.; Werner, S. Regulation of wound healing by the NRF2 transcription factor- more than a cytoprotection. Int. J. Mol. Sci. 2019, 20, 3856. [Google Scholar] [CrossRef] [Green Version]
- Naef, R.; Tenor, H.; Koch, G. TOP-N53: A Clinical Drug Candidate for the Treatment of Non-healing Wounds. Chimia 2020, 74, 814–817. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vehicle | 165 µM TOP-N53 | |
|---|---|---|
| Ingredient | (%) (w/w) | (%) (w/w) |
| Polyethylene glycol 400 (PEG 400) | 70 | 70 |
| Benzyl alcohol | 2 | 2 |
| Butylated hydroxytoluene | 0.006 | 0.006 |
| Hydroxyethyl cellulose (HEC) | 0.25 | 0.25 |
| Phosphate buffer 12 mM pH 6.7 | 27.744 | 27.734 |
| TOP-N53 | 0 | 0.01 |
| Antibody | Source | Dilution | Incubation Conditions | Identifier |
|---|---|---|---|---|
| Rabbit anti-Ki67 | Abcam, Cambridge, UK | 1:200 | 15 min at RT | Cat#Ab15580; RRID: AB_443209 |
| Biotinylated anti-rabbit IgG | Jackson ImmunoResearch | 1:1000 | 30 min at RT | Cat#111-065-003; RRID: AB_2337959 |
| Rat anti-Meca32 | BD Biosciences, Franklin Lakes, NJ | 1:1000 | Overnight at 4 ℃ | Cat#553849; RRID: AB_395086 |
| Mouse anti-α-smooth muscle actin-FITC | Sigma-Aldrich | 1:500 | Overnight at 4 ℃ | Cat#F3777; RRID: AB_476977 |
| Anti-rat-Cy3 | Jackson ImmunoResearch | 1:200 | 30 min at RT | Cat#715-165-150; RRID: AB_2340666 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ben-Yehuda Greenwald, M.; Liu, Y.-H.; Li, W.; Hiebert, P.; Zubair, M.; Tenor, H.; Braun, T.; Naef, R.; Razansky, D.; Werner, S. Topical Wound Treatment with a Nitric Oxide-Releasing PDE5 Inhibitor Formulation Enhances Blood Perfusion and Promotes Healing in Mice. Pharmaceutics 2022, 14, 2358. https://doi.org/10.3390/pharmaceutics14112358
Ben-Yehuda Greenwald M, Liu Y-H, Li W, Hiebert P, Zubair M, Tenor H, Braun T, Naef R, Razansky D, Werner S. Topical Wound Treatment with a Nitric Oxide-Releasing PDE5 Inhibitor Formulation Enhances Blood Perfusion and Promotes Healing in Mice. Pharmaceutics. 2022; 14(11):2358. https://doi.org/10.3390/pharmaceutics14112358
Chicago/Turabian StyleBen-Yehuda Greenwald, Maya, Yu-Hang Liu, Weiye Li, Paul Hiebert, Maria Zubair, Hermann Tenor, Tobias Braun, Reto Naef, Daniel Razansky, and Sabine Werner. 2022. "Topical Wound Treatment with a Nitric Oxide-Releasing PDE5 Inhibitor Formulation Enhances Blood Perfusion and Promotes Healing in Mice" Pharmaceutics 14, no. 11: 2358. https://doi.org/10.3390/pharmaceutics14112358