

Therapies Based on Adipose-Derived Stem Cells for Lower Urinary Tract Dysfunction: A Narrative Review
 , ,
, ,
Abstract
:1. Rational for Focusing on ASCs
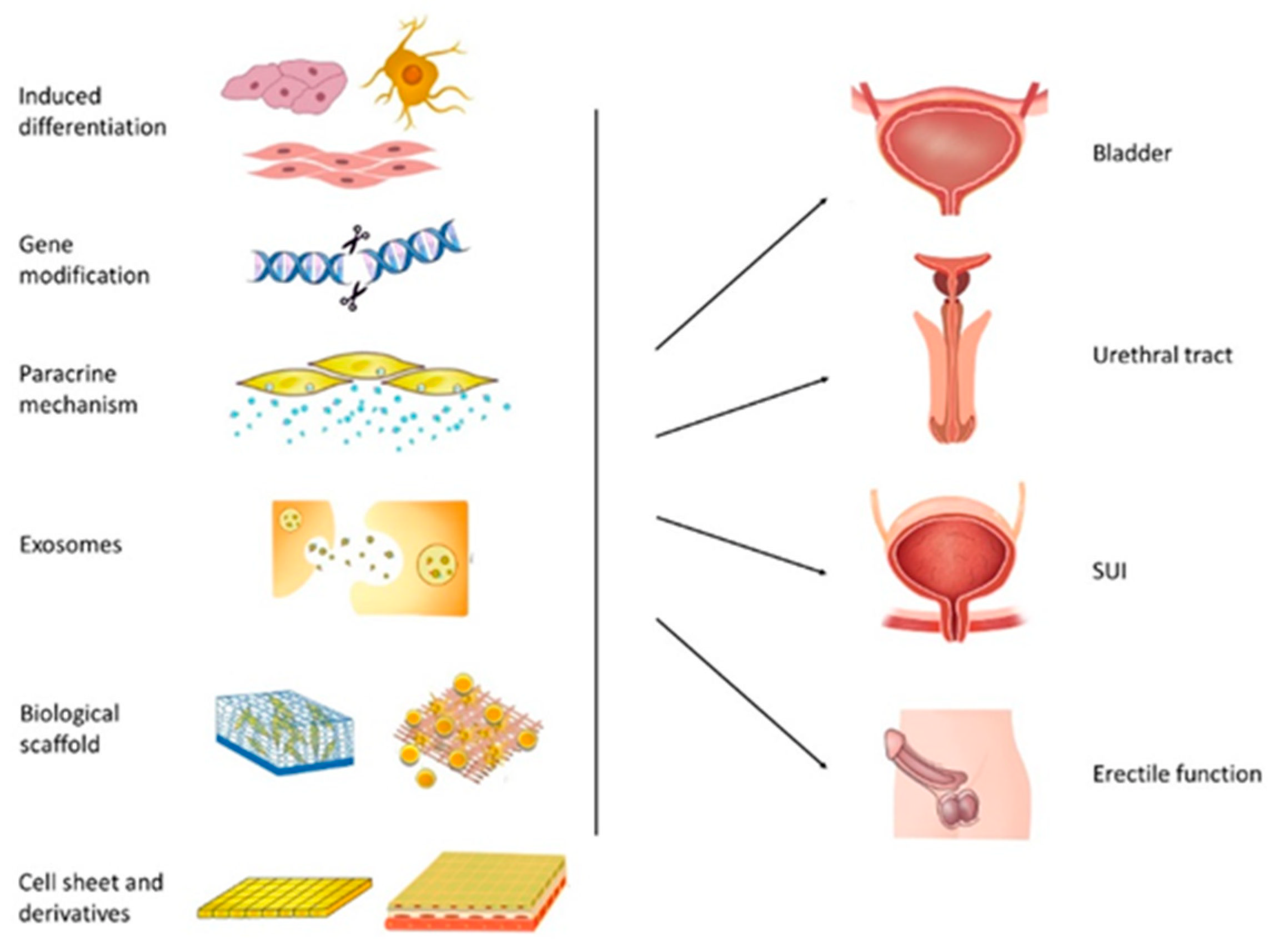
2. Advances in ASCs Therapy for the Lower Urinary Tract
2.1. ASC-Based Therapy for Bladder Reconstruction
2.2. ASC-Based Therapy for Urethral Injuries
2.3. ASC-Based Therapy for Stress Urinary Incontinence (SUI)
2.4. ASC-Based Therapy for Erectile Dysfunction
3. Current Challenges and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Tran, C.; Damaser, M.S. The potential role of stem cells in the treatment of urinary incontinence. Ther. Adv. Urol. 2015, 7, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, H.J.; Song, Y.S. Treatment of Bladder Dysfunction Using Stem Cell or Tissue Engineering Technique. Korean J. Urol. 2014, 55, 228–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillary, C.J.; Roman, S.; MacNeil, S.; Aicher, W.K.; Stenzl, A.; Chapple, C.R. Regenerative medicine and injection therapies in stress urinary incontinence. Nat. Rev. Urol. 2020, 17, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Y.; Xiang, Y.; Ma, J.; Zhang, H.; Dai, J.; Hou, Y.; Yang, Y.; Ma, J.; Li, H. An In Vitro Study on Extracellular Vesicles From Adipose-Derived Mesenchymal Stem Cells in Protecting Stress Urinary Incontinence Through MicroRNA-93/F3 Axis. Front. Endocrinol. 2021, 12, 693977. [Google Scholar] [CrossRef] [PubMed]
- Gallo, F.; Ninotta, G.; Schenone, M.; Cortese, P.; Giberti, C. Advances in stem cell therapy for male stress urinary incontinence. Expert Opin. Biol. Ther. 2019, 19, 293–300. [Google Scholar] [CrossRef]
- Bento, G.; Shafigullina, A.K.; Rizvanov, A.A.; Sardão, V.A.; Macedo, M.P.; Oliveira, P.J. Urine-Derived Stem Cells: Applications in Regenerative and Predictive Medicine. Cells 2020, 9, 573. [Google Scholar] [CrossRef] [PubMed]
- Gimble, J.M.; Katz, A.J.; Bunnell, B.A. Adipose-derived stem cells for regenerative medicine. Circ. Res. 2007, 100, 1249–1260. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Bi, J.; Huang, J.; Tang, Y.; Du, S.; Li, P. Exosome: A Review of Its Classification, Isolation Techniques, Storage, Diagnostic and Targeted Therapy Applications. Int. J. Nanomed. 2020, 15, 6917–6934. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, S.M.; Hensle, T.W. Metabolic consequences and long-term complications of enterocystoplasty in children: A review. J. Urol. 2005, 173, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Husmann, D.A.; Rathbun, S.R. Long-term follow up of enteric bladder augmentations: The risk for malignancy. J. Pediatr. Urol. 2008, 4, 381–385. [Google Scholar] [CrossRef]
- Hensle, T.W.; Gilbert, S.M. A review of metabolic consequences and long-term complications of enterocystoplasty in children. Curr. Urol. Rep. 2007, 8, 157–162. [Google Scholar] [CrossRef]
- Pokrywczynska, M.; Jundzill, A.; Warda, K.; Buchholz, L.; Rasmus, M.; Adamowicz, J.; Bodnar, M.; Marszalek, A.; Helmin-Basa, A.; Michalkiewicz, J.; et al. Does the Mesenchymal Stem Cell Source Influence Smooth Muscle Regeneration in Tissue-Engineered Urinary Bladders? Cell Transplant. 2018, 26, 1780–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamowicz, J.; Pokrywczynska, M.; Van Breda, S.V.; Kloskowski, T.; Drewa, T. Concise Review: Tissue Engineering of Urinary Bladder; We Still Have a Long Way to Go? Stem Cells Transl. Med. 2017, 6, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.D.; Wang, Q.; Yan, H.; Lv, X.G.; Zhao, Y.; Zhou, Z.; Zhang, M.; Sun, Q.; Sun, K.; Li, W.; et al. Adipose-derived stem cells-seeded bladder acellular matrix graft-silk fibroin enhances bladder reconstruction in a rat model. Oncotarget 2017, 8, 86471–86487. [Google Scholar] [CrossRef] [PubMed]
- Zhe, Z.; Jun, D.; Yang, Z.; Mingxi, X.; Ke, Z.; Ming, Z.; Zhong, W.; Mujun, L. Bladder Acellular Matrix Grafts Seeded with Adipose-Derived Stem Cells and Incubated Intraperitoneally Promote the Regeneration of Bladder Smooth Muscle and Nerve in a Rat Model of Bladder Augmentation. Stem Cells Dev. 2016, 25, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Pokrywczynska, M.; Jundzill, A.; Rasmus, M.; Adamowicz, J.; Balcerczyk, D.; Buhl, M.; Warda, K.; Buchholz, L.; Gagat, M.; Grzanka, D.; et al. Understanding the role of mesenchymal stem cells in urinary bladder regeneration-a preclinical study on a porcine model. Stem Cell Res. Ther. 2018, 9, 328. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Shi, C.; Chen, W.; Chen, B.; Jia, W.; Guo, Y.; Ma, C.; Ye, G.; Kang, J.; Dai, J. Transplantation of human adipose-derived mesenchymal stem cells on a bladder acellular matrix for bladder regeneration in a canine model. Biomed. Mater. 2016, 11, 031001. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Manzano, V.; Mellado-Lopez, M.; Morera-Esteve, M.J.; Alastrue-Agudo, A.; Bisbal-Velasco, V.; Forteza-Vila, J.; Serrano-Aroca, A.; Vera-Donoso, C.D. Human adipose-derived mesenchymal stem cells accelerate decellularized neobladder regeneration. Regen. Biomater. 2020, 7, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Gomez, P., 3rd; Gil, E.S.; Lovett, M.L.; Rockwood, D.N.; Di Vizio, D.; Kaplan, D.L.; Adam, R.M.; Estrada, C.R., Jr.; Mauney, J.R. The effect of manipulation of silk scaffold fabrication parameters on matrix performance in a murine model of bladder augmentation. Biomaterials 2011, 32, 7562–7570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesan, J.; Bhatnagar, I.; Manivasagan, P.; Kang, K.H.; Kim, S.K. Alginate composites for bone tissue engineering: A review. Int. J. Biol. Macromol. 2015, 72, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Yan, H.; Wang, Q.; Lv, X.; Zhang, M.; Zhao, Y.; Zhou, Z.; Xu, J.; Sun, Q.; Sun, K.; et al. Trilayer Three-Dimensional Hydrogel Composite Scaffold Containing Encapsulated Adipose-Derived Stem Cells Promotes Bladder Reconstruction via SDF-1alpha/CXCR4 Pathway. ACS Appl. Mater. Interfaces 2017, 9, 38230–38241. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Wang, P.; Zhao, J.; Ling, Z.; An, Z.; Fu, Z.; Fu, W.; Zhang, X. Bi-layer silk fibroin skeleton and bladder acellular matrix hydrogel encapsulating adipose-derived stem cells for bladder reconstruction. Biomater. Sci. 2021, 9, 6169–6182. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, S.; Yang, R.; Zou, Q.; Zhang, K.; Tian, Q.; Zhao, W.; Zong, L.; Fu, Q. Bioengineered bladder patches constructed from multilayered adipose-derived stem cell sheets for bladder regeneration. Acta Biomater. 2019, 85, 131–141. [Google Scholar] [CrossRef]
- Yang, T.; Zhao, F.; Zhou, L.; Liu, J.; Xu, L.; Dou, Q.; Xu, Z.; Jia, R. Therapeutic potential of adipose-derived mesenchymal stem cell exosomes in tissue-engineered bladders. J. Tissue Eng. 2021, 12, 20417314211001545. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Yang, M.; Zhang, M.; Rong, L.; Wang, Y.; Cheng, H.; Sui, X.; Sheikh, S.P.; Lu, M. MicroRNA-126 from stem cell extracellular vesicles encapsulated in a tri-layer hydrogel scaffold promotes bladder angiogenesis by activating CXCR4/SDF-1α pathway. Chem. Eng. J. 2021, 425, 131624. [Google Scholar] [CrossRef]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair. Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Simoes, I.N.; Vale, P.; Soker, S.; Atala, A.; Keller, D.; Noiva, R.; Carvalho, S.; Peleteiro, C.; Cabral, J.M.; Eberli, D.; et al. Acellular Urethra Bioscaffold: Decellularization of Whole Urethras for Tissue Engineering Applications. Sci. Rep. 2017, 7, 41934. [Google Scholar] [CrossRef] [Green Version]
- Feng, Z.; Chen, H.; Fu, T.; Zhang, L.; Liu, Y. miR-21 modification enhances the performance of adipose tissue-derived mesenchymal stem cells for counteracting urethral stricture formation. J. Cell. Mol. Med. 2018, 22, 5607–5616. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Dewulf, K.; Hakim, L.; Weyne, E.; Montorsi, F.; Russo, A.; Boeri, L.; Bivalacqua, T.J.; De Ridder, D.; Joniau, S.; et al. Adipose-derived Stem Cells Counteract Urethral Stricture Formation in Rats. Eur. Urol. 2016, 70, 1032–1041. [Google Scholar] [CrossRef]
- Meng, F.; Henson, R.; Wehbe-Janek, H.; Ghoshal, K.; Jacob, S.T.; Patel, T. MicroRNA-21 regulates expression of the PTEN tumor suppressor gene in human hepatocellular cancer. Gastroenterology 2007, 133, 647–658. [Google Scholar] [CrossRef]
- Krichevsky, A.M.; Gabriely, G. miR-21: A small multi-faceted RNA. J. Cell. Mol. Med. 2009, 13, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, J.; Lei, Y.; Lyu, L.; Zuo, R.; Chen, T. MicroRNA-21 in Skin Fibrosis: Potential for Diagnosis and Treatment. Mol. Diagn. Ther. 2017, 21, 633–642. [Google Scholar] [CrossRef] [PubMed]
- L’Heureux, N.; Pâquet, S.; Labbé, R.; Germain, L.; Auger, F.A. A completely biological tissue-engineered human blood vessel. FASEB J. 1998, 12, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Vallières, K.; Laterreur, V.; Tondreau, M.Y.; Ruel, J.; Germain, L.; Fradette, J.; Auger, F.A. Human adipose-derived stromal cells for the production of completely autologous self-assembled tissue-engineered vascular substitutes. Acta Biomater. 2015, 24, 209–219. [Google Scholar] [CrossRef]
- Magnan, M.; Lévesque, P.; Gauvin, R.; Dubé, J.; Barrieras, D.; El-Hakim, A.; Bolduc, S. Tissue engineering of a genitourinary tubular tissue graft resistant to suturing and high internal pressures. Tissue Eng. Part A 2009, 15, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leto Barone, A.A.; Khalifian, S.; Lee, W.P.; Brandacher, G. Immunomodulatory effects of adipose-derived stem cells: Fact or fiction? BioMed Res. Int. 2013, 2013, 383685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashidbenam, Z.; Jasman, M.H.; Tan, G.H.; Goh, E.H.; Fam, X.I.; Ho, C.C.K.; Zainuddin, Z.M.; Rajan, R.; Rani, R.A.; Nor, F.M.; et al. Fabrication of Adipose-Derived Stem Cell-Based Self-Assembled Scaffold under Hypoxia and Mechanical Stimulation for Urethral Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 3350. [Google Scholar] [CrossRef]
- Zhou, S.; Yang, R.; Zou, Q.; Zhang, K.; Yin, T.; Zhao, W.; Shapter, J.G.; Gao, G.; Fu, Q. Fabrication of Tissue-Engineered Bionic Urethra Using Cell Sheet Technology and Labeling By Ultrasmall Superparamagnetic Iron Oxide for Full-Thickness Urethral Reconstruction. Theranostics 2017, 7, 2509–2523. [Google Scholar] [CrossRef] [PubMed]
- Sa, Y.; Wang, L.; Shu, H.; Gu, J. Post-transcriptional suppression of TIMP-1 in epithelial-differentiated adipose-derived stem cells seeded bladder acellular matrix grafts reduces urethral scar formation. Artif. Cells Nanomed. Biotechnol. 2018, 46, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Xu, Y.; Xie, H.; Li, C.; Song, L.; Feng, C.; Zhang, Q.; Xie, M.; Wang, Y.; Lv, X. Epithelial-differentiated adipose-derived stem cells seeded bladder acellular matrix grafts for urethral reconstruction: An animal model. Tissue Eng. Part A 2014, 20, 774–784. [Google Scholar] [CrossRef]
- Fu, Q.; Deng, C.L.; Zhao, R.Y.; Wang, Y.; Cao, Y. The effect of mechanical extension stimulation combined with epithelial cell sorting on outcomes of implanted tissue-engineered muscular urethras. Biomaterials 2014, 35, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Z.; Chen, S.; Xie, M.; Huang, J.; Peng, X.; Yang, R.; Wang, H.; Xu, Y.; Feng, C. Structural and functional evaluation of oxygenating keratin/silk fibroin scaffold and initial assessment of their potential for urethral tissue engineering. Biomaterials 2016, 84, 99–110. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, R.E.; Kornitzer, B.S.; Yoo, J.J.; Atala, A. Penile urethra replacement with autologous cell-seeded tubularized collagen matrices. J. Tissue Eng. Regen. Med. 2015, 9, 257–264. [Google Scholar] [CrossRef]
- Kundu, B.; Rajkhowa, R.; Kundu, S.C.; Wang, X. Silk fibroin biomaterials for tissue regenerations. Adv. Drug Deliv. Rev. 2013, 65, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Tian, B.; Song, L.; Liang, T.; Li, Z.; Ye, X.; Fu, Q.; Li, Y. Repair of urethral defects by an adipose mesenchymal stem cellporous silk fibroin material. Mol. Med. Rep. 2018, 18, 209–215. [Google Scholar] [PubMed] [Green Version]
- Wang, L.; Cheng, W.; Zhu, J.; Li, W.; Li, D.; Yang, X.; Zhao, W.; Ren, M.; Ren, J.; Mo, X.; et al. Electrospun nanoyarn and exosomes of adipose-derived stem cells for urethral regeneration: Evaluations in vitro and in vivo. Colloids Surf. B Biointerfaces 2022, 209, 112218. [Google Scholar] [CrossRef]
- Shah, H.N.; Badlani, G.H. Mesh complications in female pelvic floor reconstructive surgery and their management: A systematic review. Indian J. Urol. 2012, 28, 129–153. [Google Scholar]
- Blaivas, J.G.; Purohit, R.S.; Benedon, M.S.; Mekel, G.; Stern, M.; Billah, M.; Olugbade, K.; Bendavid, R.; Iakovlev, V. Safety considerations for synthetic sling surgery. Nat. Rev. Urol. 2015, 12, 481–509. [Google Scholar] [CrossRef]
- Davis, N.F.; Kheradmand, F.; Creagh, T. Injectable biomaterials for the treatment of stress urinary incontinence: Their potential and pitfalls as urethral bulking agents. Int. Urogynecology J. 2013, 24, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Chung, H.Y.; Wang, J.H.; Shih, J.C.; Kuo, M.Y.; Chang, P.C.; Huang, Y.D.; Wang, P.C.; Chang, C.C. Amniotic membrane and adipose-derived stem cell co-culture system enhances bone regeneration in a rat periodontal defect model. J. Formos. Med. Assoc. 2016, 115, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.; Bai, B.; Yao, Y. Progress of co-culture systems in cartilage regeneration. Expert Opin. Biol. Ther. 2018, 18, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Jalali Tehrani, H.; Daryabari, S.S.; Fendereski, K.; Alijani Zirdehi, M.; Kajbafzadeh, A.M. Application of adipose-derived, muscle-derived, and co-cultured stem cells for the treatment of stress urinary incontinence in rat models. Low. Urin. Tract Symptoms 2021, 13, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Guan, R.; Lei, H.; Li, H.; Wang, L.; Gao, Z.; Song, W.; Xin, Z. Therapeutic potential of adipose-derived stem cells-based micro-tissues in a rat model of postprostatectomy erectile dysfunction. J. Sex. Med. 2014, 11, 2439–2448. [Google Scholar] [CrossRef] [PubMed]
- Song, S.Y.; Chung, H.M.; Sung, J.H. The pivotal role of VEGF in adipose-derived-stem-cell-mediated regeneration. Expert Opin. Biol. Ther. 2010, 10, 1529–1537. [Google Scholar] [CrossRef]
- Li, M.; Li, G.; Lei, H.; Guan, R.; Yang, B.; Gao, Z.; Hui, Y.; Chen, F.; Xin, Z. Therapeutic Potential of Adipose-derived Stem Cell-based Microtissues in a Rat Model of Stress Urinary Incontinence. Urology 2016, 97, 277.e1–277.e7. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, M.; Rahman, M.; Yang, M.; Zhao, W.; Zhou, S.; Gao, G.; Fu, Q. Use of bioactive extracellular matrix fragments as a urethral bulking agent to treat stress urinary incontinence. Acta Biomater. 2020, 117, 156–166. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, S.; Yang, R.; Rahman, M.; Sequeira, R.C.; Cao, N.; Zhang, Y.; Zhao, W.; Fu, Q. Magnetic targeting of super-paramagnetic iron oxide nanoparticle labeled myogenic-induced adipose-derived stem cells in a rat model of stress urinary incontinence. Nanomedicine 2020, 30, 102281. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, C.; Jin, C.; Zhang, Z.; Kong, D.; Xu, W.; Xiu, Y. Periurethral injection of autologous adipose-derived stem cells with controlled-release nerve growth factor for the treatment of stress urinary incontinence in a rat model. Eur. Urol. 2011, 59, 155–163. [Google Scholar] [CrossRef]
- Feng, C.; Hu, J.; Liu, C.; Liu, S.; Liao, G.; Song, L.; Zeng, X. Association of 17-beta Estradiol with Adipose-Derived Stem Cells: New Strategy to Produce Functional Myogenic Differentiated Cells with a Nano-Scaffold for Tissue Engineering. PLoS ONE 2016, 11, e0164918. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, W.; Wang, X.; Wang, Y.; Wang, J.; Fu, Q.; Shi, G. Tissue-engineered sling with adipose-derived stem cells under static mechanical strain. Exp. Ther. Med. 2017, 14, 1337–1342. [Google Scholar] [CrossRef] [Green Version]
- Mirotsou, M.; Jayawardena, T.M.; Schmeckpeper, J.; Gnecchi, M.; Dzau, V.J. Paracrine mechanisms of stem cell reparative and regenerative actions in the heart. J. Mol. Cell Cardiol. 2011, 50, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Herberts, C.A.; Kwa, M.S.; Hermsen, H.P. Risk factors in the development of stem cell therapy. J. Transl. Med. 2011, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kansu, E. Thrombosis in stem cell transplantation. Hematology 2012, 17 (Suppl S1), S159–S162. [Google Scholar] [CrossRef] [PubMed]
- Poulos, J. The limited application of stem cells in medicine: A review. Stem Cell Res. Ther. 2018, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, J.; Li, H.; Zhou, Y.; Gu, B.; Xu, Y.; Fu, Q.; Peng, X.; Cao, N.; Fu, Q.; Jin, M.; et al. Therapeutic Potential of Human Adipose-Derived Stem Cell Exosomes in Stress Urinary Incontinence—An in Vitro and in Vivo Study. Cell Physiol. Biochem. 2018, 48, 1710–1722. [Google Scholar] [CrossRef]
- Liu, X.; Wang, S.; Wu, S.; Hao, Q.; Li, Y.; Guo, Z.; Wang, W. Exosomes secreted by adipose-derived mesenchymal stem cells regulate type I collagen metabolism in fibroblasts from women with stress urinary incontinence. Stem Cell Res. Ther. 2018, 9, 159. [Google Scholar] [CrossRef] [PubMed]
- Gratzke, C.; Angulo, J.; Chitaley, K.; Dai, Y.T.; Kim, N.N.; Paick, J.S.; Simonsen, U.; Uckert, S.; Wespes, E.; Andersson, K.E.; et al. Anatomy, physiology, and pathophysiology of erectile dysfunction. J. Sex. Med. 2010, 7, 445–475. [Google Scholar] [CrossRef]
- Yan, H.; Ding, Y.; Lu, M. Current Status and Prospects in the Treatment of Erectile Dysfunction by Adipose-Derived Stem Cells in the Diabetic Animal Model. Sex. Med. Rev. 2020, 8, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Hou, Q.L.; Ge, M.Y.; Zhang, C.D.; Tian, D.D.; Wang, L.K.; Tian, H.Z.; Wang, W.H.; Zhang, W.D. Adipose tissue-derived stem cell therapy for erectile dysfunction in rats: A systematic review and meta-analysis. Int. Urol. Nephrol. 2017, 49, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Siregar, S.; Adriansjah, R.; Sibarani, J.; Mustafa, A. Effect of Intracorporeal Human Adipose-Derived Stem Cells (hADSCs) on Corpora Cavernosa Transforming Growth Factor beta1 (TGFbeta1) and Collagen Type I Concentration in Wistar Rat Priapism Model. Res. Rep. Urol. 2020, 12, 21–27. [Google Scholar] [PubMed] [Green Version]
- Castiglione, F.; Hedlund, P.; Weyne, E.; Hakim, L.; Montorsi, F.; Bivalacqua, T.J.; De Ridder, D.; Milenkovic, U.; Ralph, D.; Garaffa, G.; et al. Intratunical Injection of Human Adipose Tissue-Derived Stem Cells Restores Collagen III/I Ratio in a Rat Model of Chronic Peyronie’s Disease. Sex. Med. 2019, 7, 94–103. [Google Scholar] [CrossRef]
- Liang, L.; Shen, Y.; Dong, Z.; Gu, X. Photoacoustic image-guided corpus cavernosum intratunical injection of adipose stem cell-derived exosomes loaded polydopamine thermosensitive hydrogel for erectile dysfunction treatment. Bioact. Mater. 2022, 9, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Bai, Z.; Xu, Y.; Sun, J.; Lu, L.; Yang, Y. Effects of Cells Self-aggregation in the Treatment of Neurogenic Erectile Dysfunction With Traditional Single Cell Suspension of Adipose-derived Stem Cells. Urology 2021, 158, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yang, Y.; Zheng, H.; Huang, C.; Zhu, X.; Zhu, Y.; Guan, R.; Xin, Z.; Liu, Z.; Tian, Y. Intracavernous injection of size-specific stem cell spheroids for neurogenic erectile dysfunction: Efficacy and risk versus single cells. EBioMedicine 2020, 52, 102656. [Google Scholar] [CrossRef] [Green Version]
- Herzmann, N.; Salamon, A.; Fiedler, T.; Peters, K. Lipopolysaccharide induces proliferation and osteogenic differentiation of adipose-derived mesenchymal stromal cells in vitro via TLR4 activation. Exp. Cell Res. 2017, 350, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Hwa Cho, H.; Bae, Y.C.; Jung, J.S. Role of toll-like receptors on human adipose-derived stromal cells. Stem Cells 2006, 24, 2744–2752. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Nie, P.; Yang, W.; Ma, X.; Chen, Z.; Wei, H. Lipopolysaccharide-preconditioned allogeneic adipose-derived stem cells improve erectile function in a rat model of bilateral cavernous nerve injury. Basic Clin. Androl. 2022, 32, 5. [Google Scholar] [CrossRef] [PubMed]
- Albersen, M.; Fandel, T.M.; Lin, G.; Wang, G.; Banie, L.; Lin, C.S.; Lue, T.F. Injections of adipose tissue-derived stem cells and stem cell lysate improve recovery of erectile function in a rat model of cavernous nerve injury. J. Sex. Med. 2010, 7, 3331–3340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, G.; Albersen, M.; Harraz, A.M.; Fandel, T.M.; Garcia, M.; McGrath, M.H.; Konety, B.R.; Lue, T.F.; Lin, C.S. Cavernous nerve repair with allogenic adipose matrix and autologous adipose-derived stem cells. Urology 2011, 77, e1501–e1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Yang, R.; Wang, Z.; Lin, G.; Lue, T.F.; Lin, C.S. Adipose tissue-derived stem cells secrete CXCL5 cytokine with neurotrophic effects on cavernous nerve regeneration. J. Sex. Med. 2011, 8, 437–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Zhang, H.; Wang, Z.; Ding, W.; Zeng, Q.; Liu, W.; Huang, C.; He, S.; Wei, A. Adipose-Derived Stem Cell-Derived Exosomes Ameliorate Erectile Dysfunction in a Rat Model of Type 2 Diabetes. J. Sex. Med. 2017, 14, 1084–1094. [Google Scholar] [CrossRef] [PubMed]
- Ying, C.C.; Yang, M.; Wang, Y.; Guo, Y.L.; Hu, W.L.; Zheng, X.M. Neural-like cells from adipose-derived stem cells for cavernous nerve injury in rats. Neural Regen. Res. 2019, 14, 1085–1090. [Google Scholar] [PubMed]
- Zheng, T.; Zhang, T.; Zhang, W.; Lv, K.; Jia, D.; Yang, F.; Sun, Y.; Lian, J.; Wang, R. Icariside II facilitates the differentiation of ADSCs to schwann cells and restores erectile dysfunction through regulation of miR-33/GDNF axis. Biomed. Pharmacother. 2020, 125, 109888. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.; Guo, Y.; Shen, J. IcarisideII facilitates the differentiation of ADSCs to SCs via let-7i/STAT3 axis to preserve erectile function. Biol. Res. 2019, 52, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Li, E.; Li, F.; Luo, L.; Zhao, S.; Kang, R.; Luo, J.; Zhao, Z. Effect of Testosterone on the Phenotypic Modulation of Corpus Cavernosum Smooth Muscle Cells in a Castrated Rat Model. Urology 2017, 103, e271–e273. [Google Scholar] [CrossRef]
- Huang, J.; Wang, T.; Wright, A.C.; Yang, J.; Zhou, S.; Li, L.; Yang, J.; Small, A.; Parmacek, M.S. Myocardin is required for maintenance of vascular and visceral smooth muscle homeostasis during postnatal development. Proc. Natl. Acad. Sci. USA 2015, 112, 4447–4452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mughal, W.; Martens, M.; Field, J.; Chapman, D.; Huang, J.; Rattan, S.; Hai, Y.; Cheung, K.G.; Kereliuk, S.; West, A.R.; et al. Myocardin regulates mitochondrial calcium homeostasis and prevents permeability transition. Cell Death Differ. 2018, 25, 1732–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.B.; Chen, F.Z.; He, S.H.; Liang, Y.B.; Wang, Z.Q.; Wang, L.; Chen, Z.R.; Ding, W.; Zhao, S.C.; Wei, A.Y. In vivo tracking on longer retention of transplanted myocardin gene-modified adipose-derived stem cells to improve erectile dysfunction in diabetic rats. Stem Cell Res. Ther. 2019, 10, 208. [Google Scholar] [CrossRef] [PubMed]
- Kokai, L.E.; Ghaznavi, A.M.; Marra, K.G. Incorporation of double-walled microspheres into polymer nerve guides for the sustained delivery of glial cell line-derived neurotrophic factor. Biomaterials 2010, 31, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Cattin, A.L.; Burden, J.J.; Van Emmenis, L.; Mackenzie, F.E.; Hoving, J.J.; Garcia Calavia, N.; Guo, Y.; McLaughlin, M.; Rosenberg, L.H.; Quereda, V.; et al. Macrophage-Induced Blood Vessels Guide Schwann Cell-Mediated Regeneration of Peripheral Nerves. Cell 2015, 162, 1127–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Chen, Z.; Ma, X.; Ouyang, X.; Fang, J.; Wei, H. Co-overexpression of VEGF and GDNF in adipose-derived stem cells optimizes therapeutic effect in neurogenic erectile dysfunction model. Cell Prolif. 2020, 53, e12756. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, Y.; Zang, G.; Wang, T.; Yu, Z.; Wang, S.; Tang, Z.; Liu, J. Adipose-derived stem cells improve erectile function partially through the secretion of IGF-1, bFGF, and VEGF in aged rats. Andrology 2018, 6, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Yin, Y.; Yang, Y.; Peng, D.; Wei, J.; Yin, G.; Tang, Y. Knockdown of miR-423-5p simultaneously upgrades the eNOS and VEGFa pathways in ADSCs and improves erectile function in diabetic rats. J. Cell. Mol. Med. 2021, 25, 9796–9804. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Sun, J.Y.; Ying, C.C.; Wang, Y.; Guo, Y.L. Adipose-derived stem cells modified by BDNF gene rescue erectile dysfunction after cavernous nerve injury. Neural Regen. Res. 2020, 15, 120–127. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Sun, J.; Ma, T.; Yang, Z.; Wang, X.; Zhang, Z.; Li, J.; Wang, L.; Ii, M.; Yang, J.; et al. Curcumin induces therapeutic angiogenesis in a diabetic mouse hindlimb ischemia model via modulating the function of endothelial progenitor cells. Stem Cell Res. Ther. 2017, 8, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, S.; Luo, C.; Cao, B.; Hu, H.; Wang, S.; Yue, H.; Chen, L.; Zhou, Z. Endothelial Progenitor Cells for Ischemic Stroke: Update on Basic Research and Application. Stem Cells Int. 2017, 2017, 2193432. [Google Scholar] [CrossRef] [Green Version]
- Petrelli, A.; Di Fenza, R.; Carvello, M.; Gatti, F.; Secchi, A.; Fiorina, P. Strategies to reverse endothelial progenitor cell dysfunction in diabetes. Exp. Diabetes Res. 2012, 2012, 471823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, A.L.; Bangalore-Prakash, P.; Rajoria, S.; Suriano, R.; Shanmugam, A.; Mittelman, A.; Tiwari, R.K. Endothelial progenitor cell biology in disease and tissue regeneration. J. Hematol. Oncol. 2011, 4, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gou, X.; He, W.Y.; Xiao, M.Z.; Qiu, M.; Wang, M.; Deng, Y.Z.; Liu, C.D.; Tang, Z.B.; Li, J.; Chen, Y. Transplantation of endothelial progenitor cells transfected with VEGF165 to restore erectile function in diabetic rats. Asian J. Androl. 2011, 13, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Chen, W.; Zhang, C.; Xie, Y.; Gao, Y.; Deng, C.; Sun, X.; Liu, G.; Deng, C. Combined Transplantation of Adipose Tissue-Derived Stem Cells and Endothelial Progenitor Cells Improve Diabetic Erectile Dysfunction in a Rat Model. Stem Cells Int. 2020, 2020, 2154053. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Mi, Y.; Wu, S.; You, X.; Huang, Y.; Zhu, J.; Zhu, L. Exosomes from adipose-derived stem cells protect against high glucose-induced erectile dysfunction by delivery of corin in a streptozotocin-induced diabetic rat model. Regen. Ther. 2020, 14, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, Z.A.; Abboudi, H.; Crawford, R.; Shah, S. Intraurethral bulking agents for the management of female stress urinary incontinence: A systematic review. Int. Urogynecol. J. 2017, 28, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Lin, D.L.; Hanzlicek, B.; Balog, B.; Penn, M.S.; Kiedrowski, M.J.; Hu, Z.; Ye, Z.; Zhu, H.; Damaser, M.S. Mesenchymal stem cells and their secretome partially restore nerve and urethral function in a dual muscle and nerve injury stress urinary incontinence model. American journal of physiology. Ren. Physiol. 2015, 308, F92–F100. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.K.; Dean, A.; Badra, S.; Lankford, S.; Poppante, K.; Badlani, G.; Andersson, K.E. Cell versus Chemokine Therapy in a Nonhuman Primate Model of Chronic Intrinsic Urinary Sphincter Deficiency. J. Urol. 2016, 196, 1809–1815. [Google Scholar] [CrossRef] [PubMed]
- Gill, B.C.; Sun, D.Z.; Damaser, M.S. Stem Cells for Urinary Incontinence: Functional Differentiation or Cytokine Effects? Urology 2018, 117, 9–17. [Google Scholar] [CrossRef]
- Casado-Díaz, A.; Quesada-Gómez, J.M.; Dorado, G. Extracellular Vesicles Derived From Mesenchymal Stem Cells (MSC) in Regenerative Medicine: Applications in Skin Wound Healing. Front. Bioeng. Biotechnol. 2020, 8, 146. [Google Scholar] [CrossRef] [Green Version]
- Xiong, M.; Zhang, Q.; Hu, W.; Zhao, C.; Lv, W.; Yi, Y.; Wu, Y.; Wu, M. Exosomes From Adipose-Derived Stem Cells: The Emerging Roles and Applications in Tissue Regeneration of Plastic and Cosmetic Surgery. Front. Cell Dev. Biol. 2020, 8, 574223. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, H.; Wang, J. Exosomes as a novel pathway for regulating development and diseases of the skin. Biomed. Rep. 2018, 8, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Rinkevich, Y.; Walmsley, G.G.; Hu, M.S.; Maan, Z.N.; Newman, A.M.; Drukker, M.; Januszyk, M.; Krampitz, G.W.; Gurtner, G.C.; Lorenz, H.P.; et al. Skin fibrosis. Identification and isolation of a dermal lineage with intrinsic fibrogenic potential. Science 2015, 348, aaa2151. [Google Scholar] [CrossRef] [Green Version]
- Choumerianou, D.M.; Dimitriou, H.; Kalmanti, M. Stem cells: Promises versus limitations. Tissue Eng. Part B Rev. 2008, 14, 53–60. [Google Scholar] [CrossRef]
- Preti, R.A. Bringing safe and effective cell therapies to the bedside. Nat. Biotechnol. 2005, 23, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.; Kriegstein, A.; Grady, D. Clinical trials in stem cell transplantation: Guidelines for scientific and ethical review. Clin. Trials 2008, 5, 517–522. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors and Year | Treatment Strategy | Biological Effect |
|---|---|---|
| Zhe et al., 2016 | ASC-seeded BAMGs | Increases in collagen bundles, myofibroblasts, and nerve cell regeneration. |
| Pokrywczynska et al., 2018 | ASC-seeded BAMGs | ASCs differentiated into smooth muscle. |
| Hou et al., 2016 | ASC-seeded BAMGs | Urothelium, bladder smooth muscle, and capillary vessel regeneration. |
| Moreno-Manzano et al., 2020 | ASC-seeded BAMGs | ASC-seeded BAMGs also accelerated angiogenesis and neuronal regeneration. |
| Xiao et al., 2017 | ASC-seeded BAMGs and silk fibroin | Expression levels of SDF-1α, VEGF, and their receptors were upregulated, and ERK 1/2 phosphorylation was increased. |
| Xiao et al., 2021 | ASC-seeded BAMGs and silk fibroin | ASCs exerted pro-angiogenic effects through the SDF-1α/CXCR4 pathway and its downstream ERK1/2 phosphorylation. |
| Xiao et al., 2017 | ASCs-seeded BAMGs and alginate di-aldehyde-gelatin hydrogel-silk mesh | Smooth muscle regeneration, angiogenesis, and innervation of the bladder were significantly accelerated. |
| Wang et al., 2019 | ASC sheet and porous polyglycolic acid scaffold with ultra-small superparamagnetic iron oxide nanoparticles | ASC sheets promoted urothelial cell, smooth muscle cell, and neurovascular regeneration. |
| Yang et al., 2021 | ASC–exosomes and BAMGs | Angiogenesis was more pronounced with ASC–exosome-stimulated BAMGs. |
| Xiao et al., 2021 | ASC–exosomes and BAMGs alginate dialdehyde-gelatin hydrogel | By upregulating miRNA-12 expression levels, inhibiting RGS16 to activate the CXCR4/SDF-1α pathway ultimately increased VEGF secretion. |
| Author and Year | Treatment Strategy | Biological Effect |
|---|---|---|
| Castiglione et al., 2016 | ASCs | Fibrosis-associated genes were significantly reduced. |
| Feng et al., 2018 | ASCs and miR-21 | MiR-21-modified ASCs increased the expression levels of the angiogenic factors hypoxia inducible factor-1, VEGF, bFGF, stem cell factor, and stromal derived factor-1a. |
| Rashidbenam et al., 2021 | ASC sheet and urothelial and smooth muscle cells | ASC sheet seeded with urothelial and smooth muscle cells was used as a scaffold. |
| Zhou et al., 2017 | ASC sheet and fibroblast and myoblast differentiated cell sheets | ASC sheet for construction of a three-layer bionic urethra. |
| Sa et al., 2018 | Pre-epithelialized ASC-seeded BAMGs | Post-transcriptional inhibition of TIMP-1 by miR-365 in ASCs could further inhibit fibrosis. |
| Li et al., 2014 | Pre-epithelialized ASC-seeded BAMGs | Pre-epithelialized ASC-seeded BAMGs better restored a continuous epithelial layer. |
| Fu et al., 2014 | ASC sheet and oral mucosal epithelium and poly-glycolic acid | Myogenic differentiated ASCs induced by mechanical extension were combined with oral mucosal epithelium to form an artificial urethral substitute with a complete double-layer structure. |
| Tian et al., 2018 | ASCs and silk fibroin | Six to seven layers of urothelial cells were formed on the surface of the silk fibroin, and the numbers of smooth muscle cells and new blood vessels growing along the silk fibroin pores were significantly increased. |
| Wang et al., 2022 | ASCs-exosomes and collagen/poly (L-lactide-cocaprolactone) nanoyarn scaffold | ASC–exosomes nanoyarn scaffold significantly promoted epithelialization and vascularization and accelerated the transition of damaged tissues from an inflammatory state to a regenerative state. |
| Author and Year | Treatment Strategy | Biological Effect |
|---|---|---|
| Tehrani et al., 2021 | ASCs and muscle-derived stem cells | The striated muscle and external sphincter around the urethra were significantly thickened, and the urethral pressure curve was significantly higher. |
| Li et al., 2016 | ASC microtissues | The structure of the external sphincter was more complete, the content of total smooth muscle was increased, and the regeneration of angiogenesis and nerve regeneration was accelerated. |
| Wang et al., 2020 | ECM from ASC sheet | ASC sheet ECM fragments provided a bulking effect and induced muscle regeneration. |
| Wang et al., 2020 | ASCs labeled with superparamagnetic iron oxide | Magnetic targeting can improve the retention rate of stem cells aggregated in the affected area. |
| Zhao et al., 2011 | ASCs and nerve growth factor encapsulated in E2 incorporated poly lac-tic-co-glycolic acid microspheres | Periurethral co-injection of ASCs and controlled-release NGF accelerated muscle and peripheral nerve regeneration. |
| Feng et al., 2016 | Pre-myogenic ASCs and poly(L-lactide)/poly(e-caprolactone) nano-scaffold | E2 significantly accelerated stem cell proliferation. Furthermore, α-SMA, calponin, and myosin heavy chain expression was increased in the early, middle, and late stages of differentiation, respectively. |
| Wang et al., 2017 | ASCs and polyglycolic acid fibers | ASCs formed tissue-engineered slings that exhibited improvements in biomechanical properties, and the tissue and collagen structures matured. |
| Ni et al., 2018 | ASCs–exosomes | The signaling proteins carried by ASCs exosomes were closely related to the Wnt, JAK/STAT, and PI3K/AKT pathways. |
| Liu et al., 2018 | ASC–exosomes | ASC–exosomes could upregulate TIMP-1, TIMP-3, and COL1A1 and downregulate MMP-1 and MMP-2 expression levels in fibroblasts, thereby increasing collagen synthesis and decreasing collagen degradation. |
| Wang et al., 2021 | ASC–exosomes | ASC–exosomes could downregulate F3 expression and upregulate PAX7 and MyoD expression in fibroblasts. |
| Author and Year | Treatment Strategy | Biological Effect |
|---|---|---|
| Siregar et al., 2020 | ASCs | ASC injection reduced TGF-β1 and type I collagen expression levels. |
| Castiglione et al., 2019 | ASCs | The expression levels of genes regulating wound recovery, including CXCL13, CXCR4, PLAT, SERPINH1, and TGF-β1, were significantly changed after stem cell treatment. |
| Zheng et al., 2021 | ASC clusters | The retention rate of ASC clusters in the corpus cavernosum was significantly higher than ASC injection. |
| Zhang et al., 2022 | Lipopolysaccharide pre-treated ASCs | Low doses of lipopolysaccharides could improve the survival rate of ASCs, inhibit caspase-3 activation induced by hydrogen peroxide, promote cell migration, and downregulate TGF-β1 expression levels to delay smooth muscle fibrosis. |
| Ying et al., 2019 | Pre-neuralization ASCs | ASC neural-like cell transplantation improved erectile function through increasing the number of neuronal nitric oxide synthase-positive fibers, myelinated axons, and smooth muscle/collagen ratio. |
| Zheng et al., 2020 | ASCs and miR-33 inhibitors (Icariside II) | Icariside II promoted the differentiation of ASCs to Schwann cells via regulating miR-33. |
| Ge et al., 2019 | ASCs and miR-33 inhibitor (Icariside II) | Icariside II can upregulate the expression levels of signal transducer and activator of transcription-3. |
| Zhang et al., 2019 | Myocardin-transfected ASCs | Transfection of MYOCD had no obvious effect on cell apoptosis but inhibited cell proliferation and promoted cell contraction. |
| Yang et al., 2018 | GDNF- and VEGF-overexpressing ASCs | ASCs with both GDNF and VEGF overexpression better improved cavernous nerve repair and vascular endothelium regeneration. |
| Yang et al., 2020 | ASCs | ASCs could increase IGF-1, bFGF, and VEGF expression in penile tissues, the number of cavernous smooth muscle cells, and ICP/MAP of the treated aged rats. |
| Zhou et al., 2021 | miR-423-5p-knock-out ASCs | miR-423-5p-knockout ASCs relieved its inhibition on endothelial NOS1 and VEGFA gene expression with therapeutic benefits. |
| Yang et al., 2020 | BDNF-overexpressing ASCs | ASCs infected with lenti-rBDNF increased the number of nNOS-positive nerve fibers and smooth muscle in the penile tissue, thereby improving ED caused by nerve injury. |
| Yang et al., 2020 | ASCs and endothelial progenitor cells | Stromal-derived factor-1 and VEGF secreted by ASCs increased significantly, which also resulted in endothelial progenitor cells expressing higher levels of 5-ethynyl-2′-deoxyuridine. This promoted repair. |
| Wang et al., 2020 | ASCs–exosomes | After ASC exosome injection, ICP/MAP was increased, nerve and blood vessel regeneration were accelerated, and atrial natriuretic peptide, brain natriuretic peptide, and neuronal nitric oxide synthase expression was inhibited. |
| Liang et al., 2022 | ASCs–exosomes | Polydopamine nanoparticles incorporated in hydrogels could cause ASC–exosomes to exhibit sustained release behavior. Furthermore, they could more effectively promote the regeneration of endothelial and nerve cells by increasing the expression of eNOS and nNOS. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Chen, J.; Cao, N.; Zhao, W.; Gao, G.; Wang, Y.; Fu, Q. Therapies Based on Adipose-Derived Stem Cells for Lower Urinary Tract Dysfunction: A Narrative Review. Pharmaceutics 2022, 14, 2229. https://doi.org/10.3390/pharmaceutics14102229
Liu M, Chen J, Cao N, Zhao W, Gao G, Wang Y, Fu Q. Therapies Based on Adipose-Derived Stem Cells for Lower Urinary Tract Dysfunction: A Narrative Review. Pharmaceutics. 2022; 14(10):2229. https://doi.org/10.3390/pharmaceutics14102229
Chicago/Turabian StyleLiu, Meng, Jiasheng Chen, Nailong Cao, Weixin Zhao, Guo Gao, Ying Wang, and Qiang Fu. 2022. "Therapies Based on Adipose-Derived Stem Cells for Lower Urinary Tract Dysfunction: A Narrative Review" Pharmaceutics 14, no. 10: 2229. https://doi.org/10.3390/pharmaceutics14102229