
Revisiting the Dissolution of Praziquantel in Biorelevant Media and the Impact of Digestion of Milk on Drug Dissolution


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
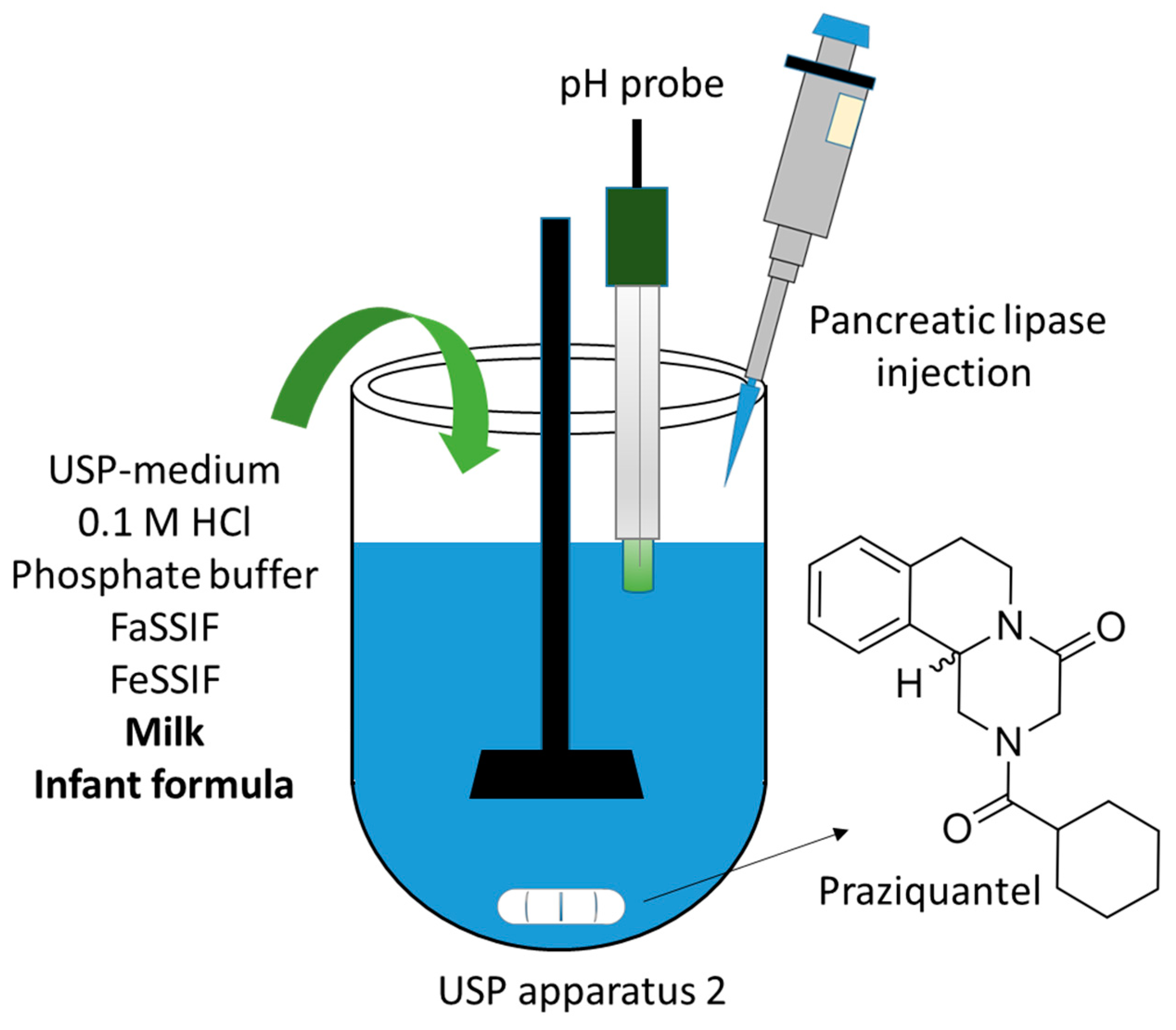
2.2. Dissolution of Praziquantel in USP-Medium and Biorelevant Media
2.3. Dissolution of Praziquantel in Milk, Infant Formula, and the Impact of Digestion
2.4. Solubility of Praziquantel in USP-Medium, Milk, Infant Formula and Biorelevant Media
2.5. Quantification of Praziquantel Using HPLC
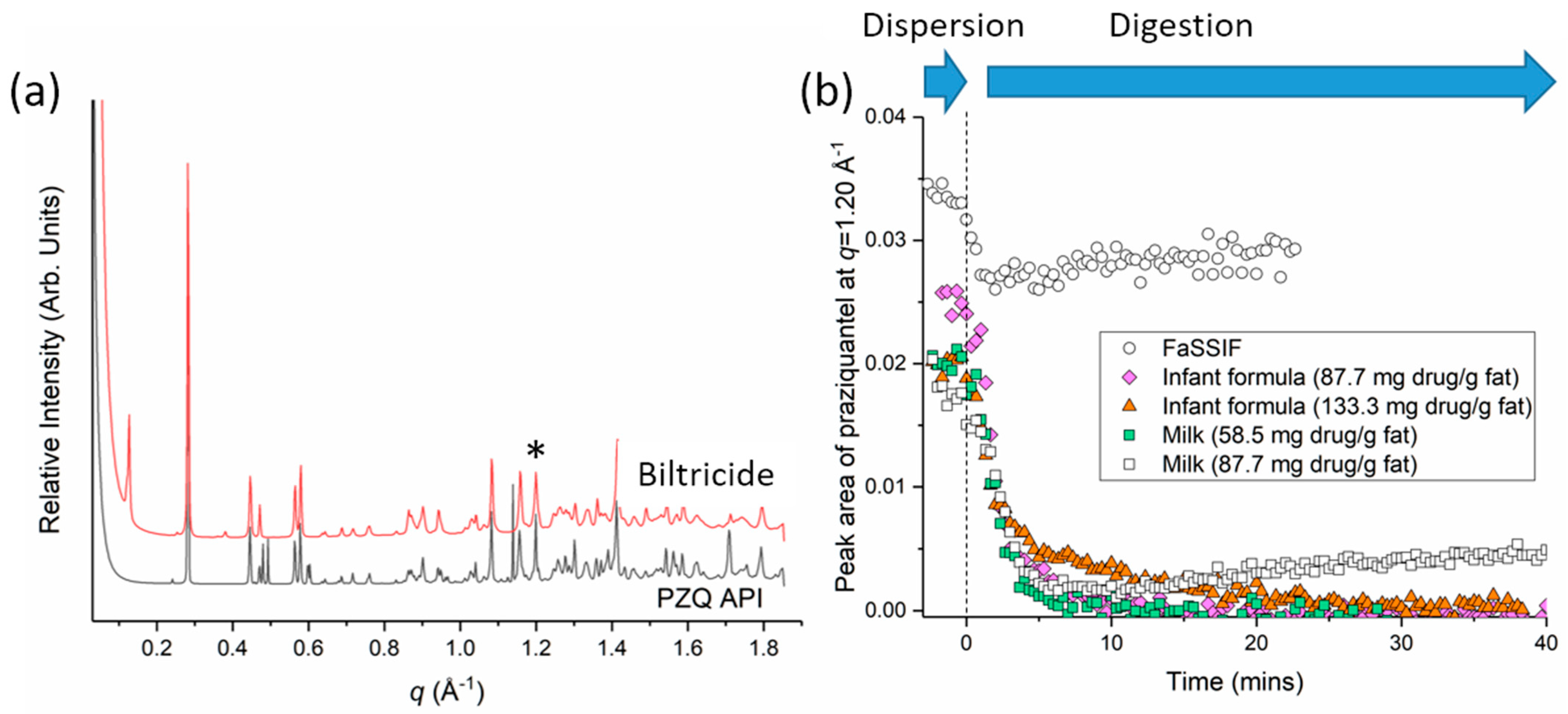
2.6. Dissolution of Praziquantel as Probed Using Small Angle X-ray Scattering (SAXS)
3. Results and Discussion
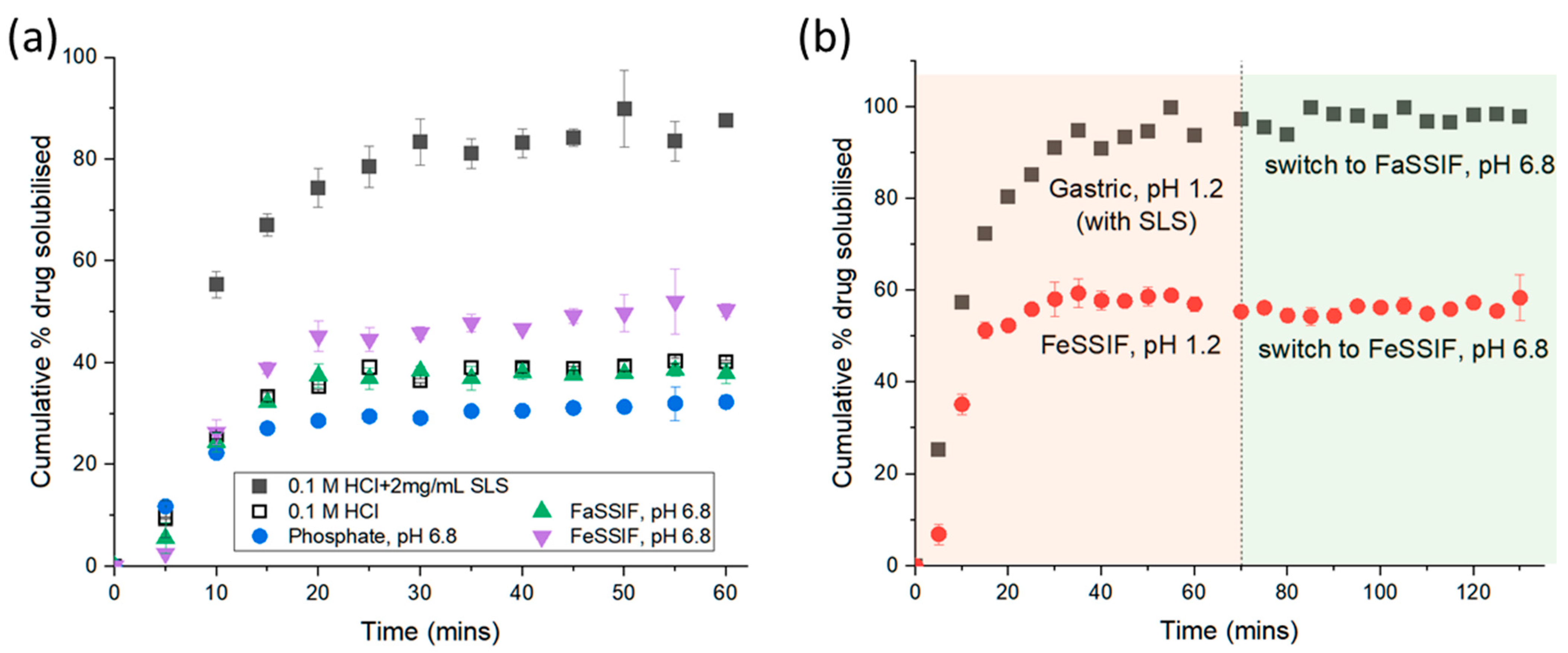
3.1. Dissolution of Praziquantel in Non-Milk Media
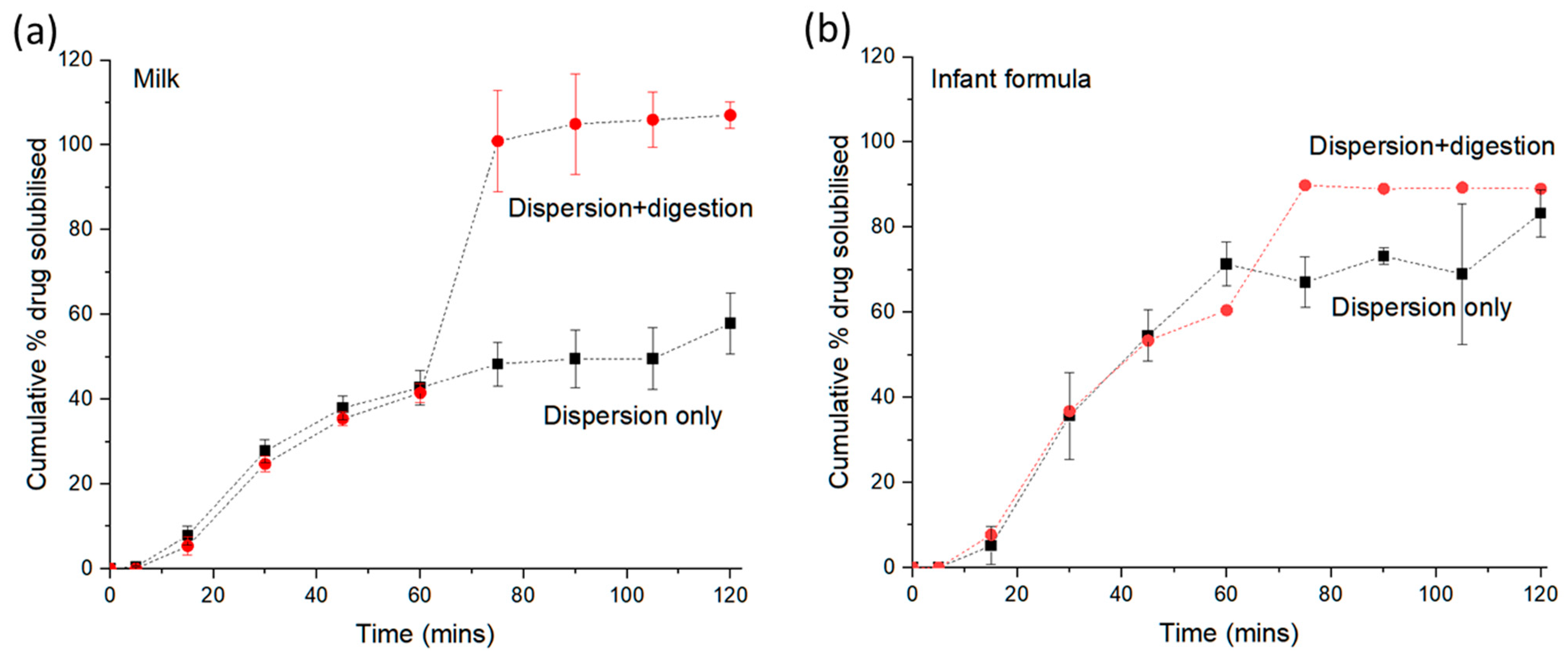
3.2. Dissolution of Praziquantel in Milk-Based Media
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FDA. Biltricide (Praziquantel) Prescribing Information (Reference ID: 4373219). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/018714s018lbl.pdf (accessed on 28 November 2020).
- WHO. Report of a Meeting to Review the Results of Studies on the Treatment of Schistosomiasis in Preschool-Age Children; WHO: Geneva, Switzerland, 2010; p. 23.
- WHO. Annex 8: Proposal to Waive In Vivo Bioequivalence Requirements for the WHO Model List of Essential Medicines Immediate Release, Solid Dosage Forms; WHO: Geneva, Switzerland, 2006; p. 45.
- Castro, N.; Medina, R.; Sotelo, J.; Jung, H. Bioavailability of praziquantel increases with concomitant administration of food. Antimicrob. Agents Chemother. 2000, 44, 2903–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Geng, Y.; Li, H.; Zhang, Y.; You, J.; Chang, Y. Enhancement the oral bioavailability of praziquantel by incorporation into solid lipid nanoparticles. Pharmazie 2009, 64, 86–89. [Google Scholar] [PubMed]
- Xie, S.; Pan, B.; Shi, B.; Zhang, Z.; Zhang, X.; Wang, M.; Zhou, W. Solid lipid nanoparticle suspension enhanced the therapeutic efficacy of praziquantel against tapeworm. Int. J. Nanomed. 2011, 6, 2367–2374. [Google Scholar] [CrossRef] [Green Version]
- El-Lakkany, N.; Seif el-Din, S.H.; Heikal, L. Bioavailability and in vivo efficacy of a praziquantel–polyvinylpyrrolidone solid dispersion in Schistosoma mansoni-infected mice. Eur. J. Drug Metab. Pharmacokinet. 2012, 37, 289–299. [Google Scholar] [CrossRef] [PubMed]
- González-Esquivel, D.; Rivera, J.; Castro, N.; Yepez-Mulia, L.; Jung Cook, H. In vitro characterization of some biopharmaceutical properties of praziquantel. Int. J. Pharm. 2005, 295, 93–99. [Google Scholar] [CrossRef]
- Boyd, B.J.; Salim, M.; Clulow, A.J.; Ramirez, G.; Pham, A.C.; Hawley, A. The impact of digestion is essential to the understanding of milk as a drug delivery system for poorly water soluble drugs. J. Control. Release 2018, 292, 13–17. [Google Scholar] [CrossRef]
- Salim, M.; Ramirez, G.; Peng, K.-Y.; Clulow, A.J.; Hawley, A.; Ramachandruni, H.; Beilles, S.; Boyd, B.J. Lipid Compositions in Infant Formulas Affect the Solubilization of Antimalarial Drugs Artefenomel (OZ439) and Ferroquine during Digestion. Mol. Pharm. 2020, 17, 2749–2759. [Google Scholar] [CrossRef]
- USP. Dissolution Methods Database. Available online: https://www.usp.org/resources/dissolution-methods-database (accessed on 28 November 2020).
- Kirby, N.M.; Mudie, S.T.; Hawley, A.M.; Cookson, D.J.; Mertens, H.D.T.; Cowieson, N.; Samardzic-Boban, V. A low-background-intensity focusing small-angle X-ray scattering undulator beamline. J. Appl. Crystallogr. 2013, 46, 1670–1680. [Google Scholar] [CrossRef]
- FDA. Dissolution Methods Database. Available online: https://www.accessdata.fda.gov/scripts/cder/dissolution/dsp_getalldata.cfm (accessed on 28 November 2020).
- Dametto, P.R.; Dametto, A.C.; Polese, L.; Ribeiro, C.A.; Chorilli, M.; de Freitas, O. Development and physicochemical characterization of solid dispersions containing praziquantel for the treatment of schistosomiasis. J. Therm. Anal. Calorim. 2017, 127, 1693–1706. [Google Scholar] [CrossRef] [Green Version]
- Clulow, A.J.; Parrow, A.; Hawley, A.; Khan, J.; Pham, A.C.; Larsson, P.; Bergström, C.A.S.; Boyd, B.J. Characterization of Solubilizing Nanoaggregates Present in Different Versions of Simulated Intestinal Fluid. J. Phys. Chem. B 2017, 121, 10869–10881. [Google Scholar] [CrossRef]
- Kamstrup, D.; Berthelsen, R.; Sassene, P.J.; Selen, A.; Mullertz, A. In Vitro Model Simulating Gastro-Intestinal Digestion in the Pediatric Population (Neonates and Young Infants). AAPS PharmSciTech 2017, 18, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Bagchus, W.M.; Bezuidenhout, D.; Harrison-Moench, E.; Kourany-Lefoll, E.; Wolna, P.; Yalkinoglu, O. Relative Bioavailability of Orally Dispersible Tablet Formulations of Levo- and Racemic Praziquantel: Two Phase I Studies. Clin. Transl. Sci. 2019, 12, 66–76. [Google Scholar] [CrossRef] [PubMed]
- FDA. Use of Liquids and/or Soft Foods as Vehicles for Drug Administration: General Considerations for Selection and In Vitro Methods for Product Quality Assessments. Guidance for Industry; FDA: Silver Spring, MD, USA, 2020.
- Salim, M.; Khan, J.; Ramirez, G.; Clulow, A.J.; Hawley, A.; Ramachandruni, H.; Boyd, B.J. Interactions of Artefenomel (OZ439) with Milk during Digestion: Insights into Digestion-Driven Solubilization and Polymorphic Transformations. Mol. Pharm. 2018, 15, 3535–3544. [Google Scholar] [CrossRef] [Green Version]
- Charkoftaki, G.; Kytariolos, J.; Macheras, P. Novel milk-based oral formulations: Proof of concept. Int. J. Pharm. 2010, 390, 150–159. [Google Scholar] [CrossRef]
- Trastullo, R.; Dolci, L.S.; Passerini, N.; Albertini, B. Development of flexible and dispersible oral formulations containing praziquantel for potential schistosomiasis treatment of pre-school age children. Int. J. Pharm. 2015, 495, 536–550. [Google Scholar] [CrossRef]
- Salim, M.; Fraser-Miller, S.J.; Bērziņš, K.R.; Sutton, J.J.; Ramirez, G.; Clulow, A.J.; Hawley, A.; Beilles, S.; Gordon, K.C.; Boyd, B.J. Low-Frequency Raman Scattering Spectroscopy as an Accessible Approach to Understand Drug Solubilization in Milk-Based Formulations during Digestion. Mol. Pharm. 2020, 17, 885–899. [Google Scholar] [CrossRef] [PubMed]
- Salim, M.; Ramirez, G.; Clulow, A.J.; Zhang, Y.; Ristroph, K.D.; Feng, J.; McManus, S.A.; Hawley, A.; Prud’homme, R.K.; Boyd, B.J. Solid-State Behavior and Solubilization of Flash Nanoprecipitated Clofazimine Particles during the Dispersion and Digestion of Milk-Based Formulations. Mol. Pharm. 2019, 16, 2755–2765. [Google Scholar] [CrossRef] [Green Version]
- Boyd, B.J.; Clulow, A.J. The influence of lipid digestion on the fate of orally administered drug delivery vehicles. Biochem. Soc. Trans. 2021, 49, 1749–1761. [Google Scholar] [CrossRef]
- Clulow, A.J.; Salim, M.; Hawley, A.; Boyd, B.J. A closer look at the behaviour of milk lipids during digestion. Chem. Phys. Lipids 2018, 211, 107–116. [Google Scholar] [CrossRef]
- El-Arini, S.K.; Giron, D.; Leuenberger, H. Solubility Properties of Racemic Praziquantel and Its Enantiomers. Pharm. Dev. Technol. 1998, 3, 557–564. [Google Scholar] [CrossRef]
- Pham, A.C.; Peng, K.Y.; Salim, M.; Ramirez, G.; Hawley, A.; Clulow, A.J.; Boyd, B.J. Correlating Digestion-Driven Self-Assembly in Milk and Infant Formulas with Changes in Lipid Composition. ACS Appl. Bio. Mater. 2020, 3, 3087–3098. [Google Scholar] [CrossRef] [PubMed]
- Bonate, P.L.; Wang, T.; Passier, P.; Bagchus, W.; Burt, H.; Lüpfert, C.; Abla, N.; Kovac, J.; Keiser, J. Extrapolation of praziquantel pharmacokinetics to a pediatric population: A cautionary tale. J. Pharmacokinet. Pharmacodyn. 2018, 45, 747–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salim, M.; Eason, T.; Boyd, B.J. Opportunities for milk and milk-related systems as ‘new’low-cost excipient drug delivery materials. Adv. Drug Deliv. Rev. 2022, 183, 114139. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dissolution Media | Solubility of Praziquantel ± SD (µg/mL) | Solubility of Praziquantel ± SD (mg/g Fat) |
|---|---|---|
| 0.1 M HCl + 2 mg/mL SLS (USP) | 546 ± 138 | - |
| 0.1 M HCl | 297 ± 6 | - |
| Phosphate buffer | 282 ± 149 | - |
| FaSSIF | 289 ± 77 | - |
| FeSSIF | 581 ± 20 | - |
| Milk (3.4% fat) | 372 ± 15 | 10.9 ± 0.4 |
| Digested milk | 1782 ± 1131 | 52.4 ± 33.3 |
| Infant formula (3.4% fat) | 674 ± 11 | 19.8 ± 0.3 |
| Digested infant formula | 1744 ± 781 | 51.3 ± 23.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eason, T.; Ramirez, G.; Clulow, A.J.; Salim, M.; Boyd, B.J. Revisiting the Dissolution of Praziquantel in Biorelevant Media and the Impact of Digestion of Milk on Drug Dissolution. Pharmaceutics 2022, 14, 2228. https://doi.org/10.3390/pharmaceutics14102228
Eason T, Ramirez G, Clulow AJ, Salim M, Boyd BJ. Revisiting the Dissolution of Praziquantel in Biorelevant Media and the Impact of Digestion of Milk on Drug Dissolution. Pharmaceutics. 2022; 14(10):2228. https://doi.org/10.3390/pharmaceutics14102228
Chicago/Turabian StyleEason, Thomas, Gisela Ramirez, Andrew J. Clulow, Malinda Salim, and Ben J. Boyd. 2022. "Revisiting the Dissolution of Praziquantel in Biorelevant Media and the Impact of Digestion of Milk on Drug Dissolution" Pharmaceutics 14, no. 10: 2228. https://doi.org/10.3390/pharmaceutics14102228