
Population Pharmacokinetic/Pharmacodynamic Modelling of Daptomycin for Schedule Optimization in Patients with Renal Impairment

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Population and Study Design
3.2. Population Pharmacokinetic Model
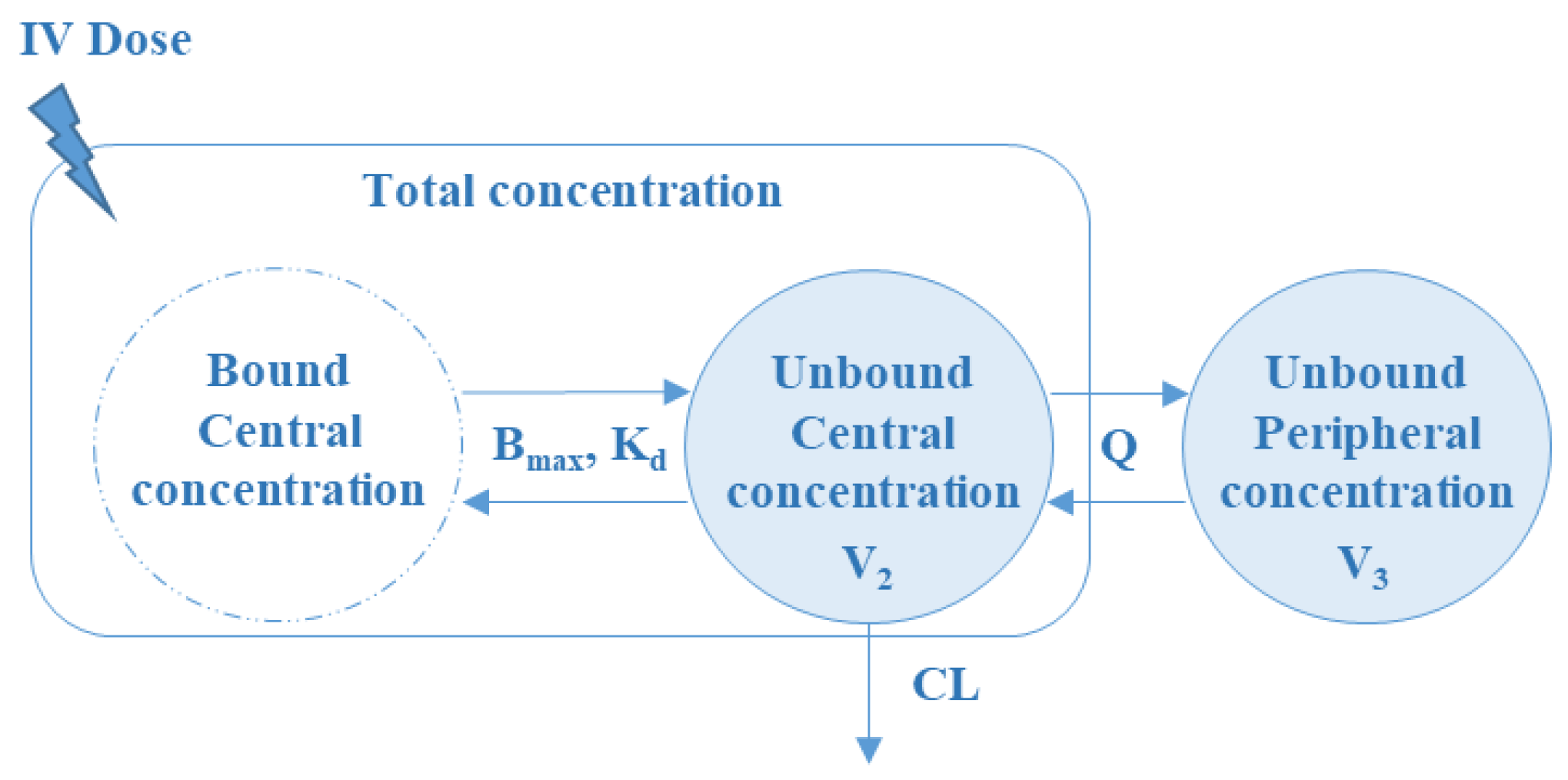
3.2.1. Base Population PK Model
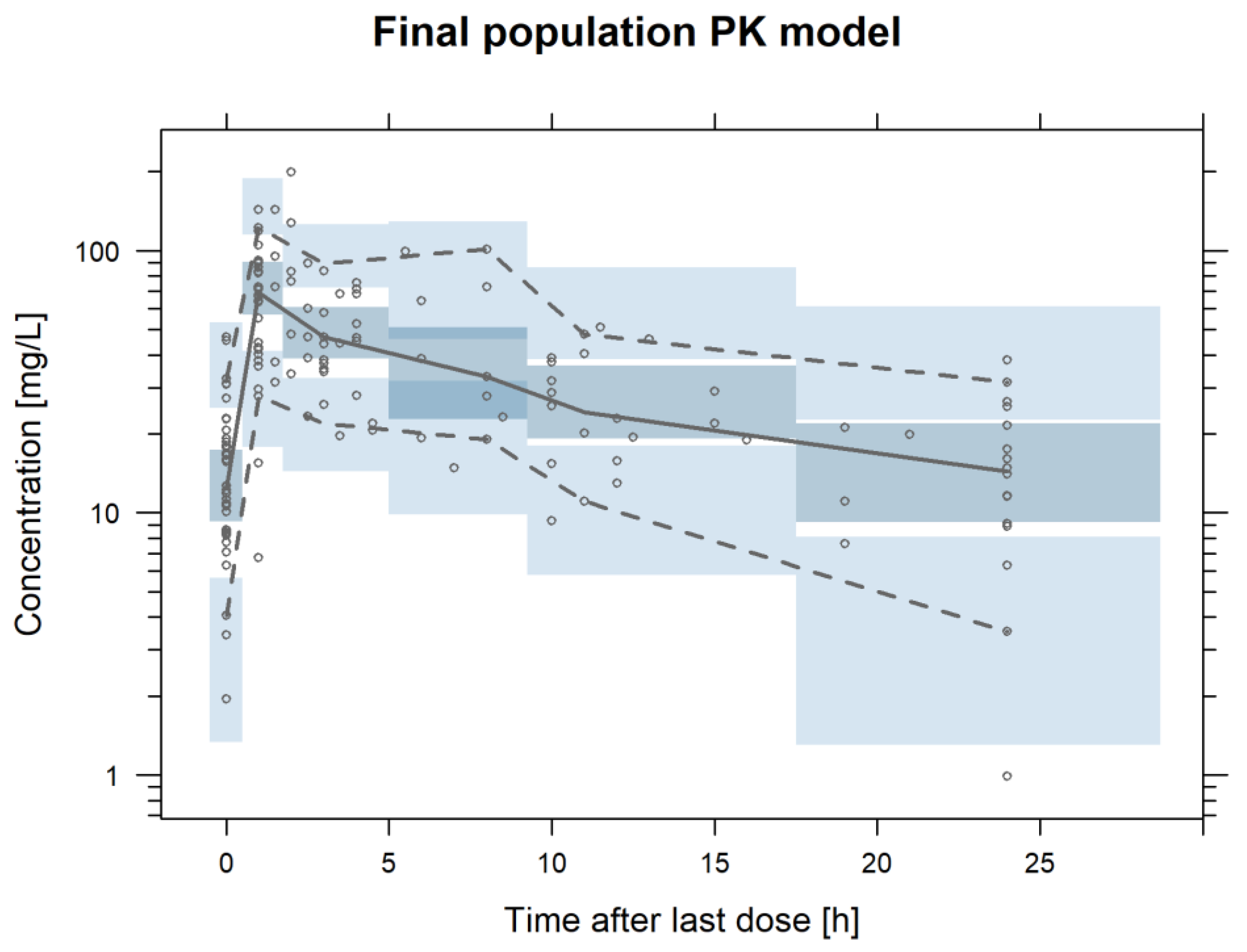
3.2.2. Final Population PK Model
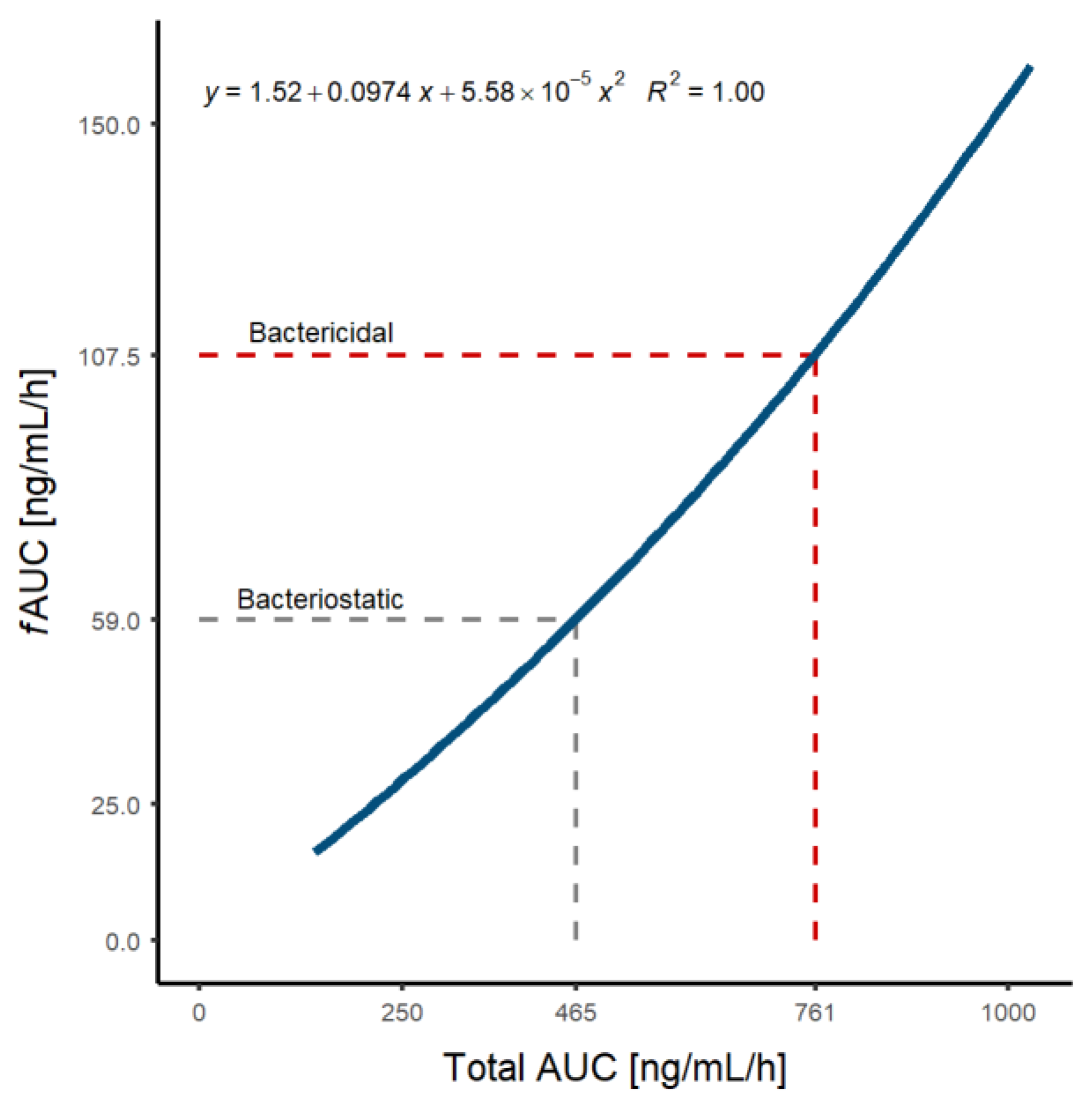
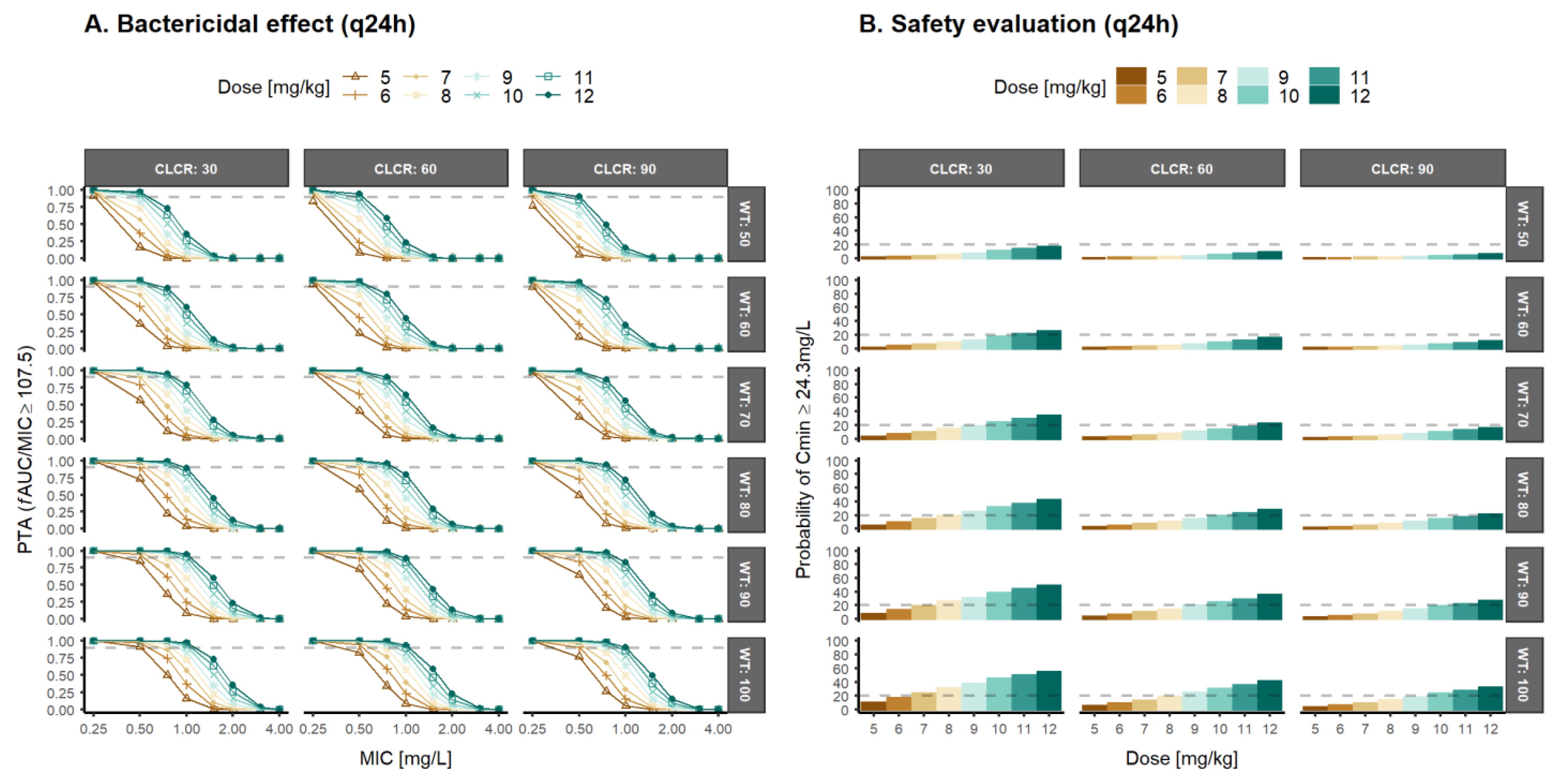
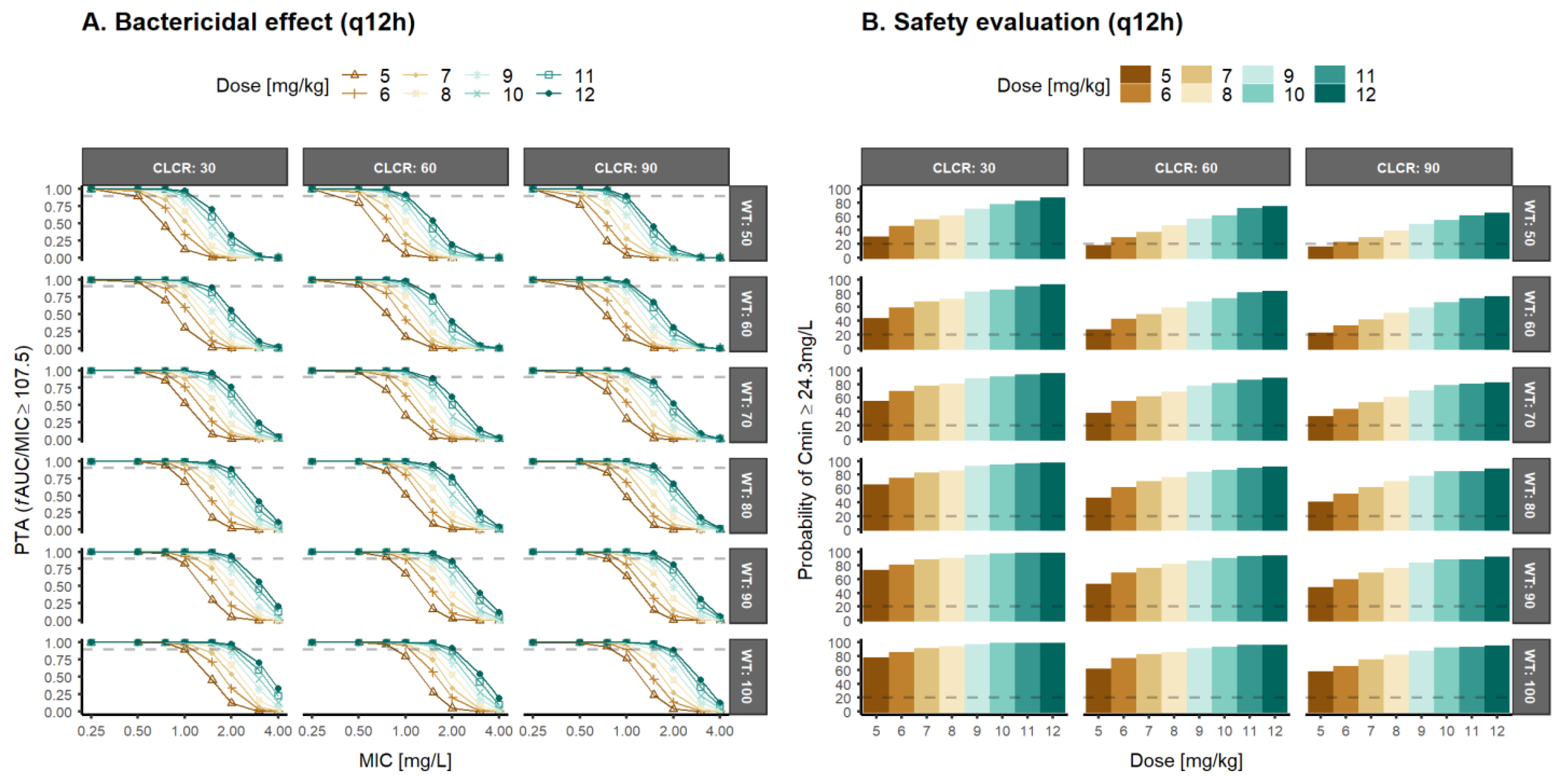
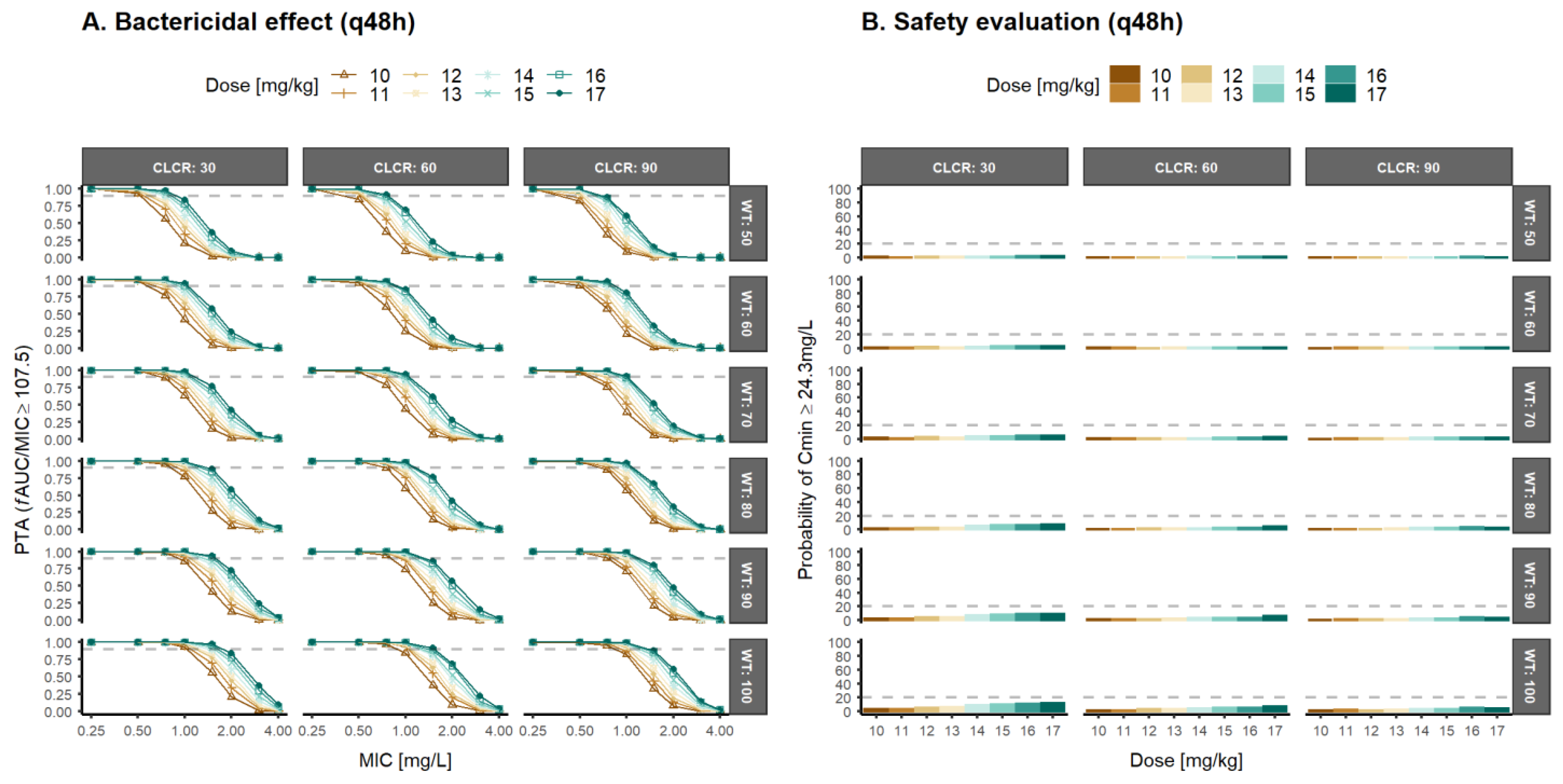
3.3. Population Pharmacokinetic/Pharmacodynamic Simulations and Optimal Dosage Selection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- US FDA Daptomycin (Marketed as Cubicin) Information. 2017. Available online: https://www.Accessdata.Fda.Gov/Drugsatfda_docs/Label/2017/021572s059lbl.Pdf (accessed on 10 April 2022).
- European Medicines Agency. Cubicin: EPAR—Product Information (WC500036049.Pdf); European Medicines Agency: London, UK, 2006.
- European Medicines Agency. Cubicin: EPAR—Scientific Discussion (WC500036046.Pdf); European Medicines Agency: London, UK, 2006.
- Vilhena, C.; Bettencourt, A. Daptomycin: A Review of Properties, Clinical Use, Drug Delivery and Resistance. Mini.-Rev. Med. Chem. 2012, 12, 202–209. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Cubicin (Daptomycin); EMEA/H/C/000637; European Medicines Agency: London, UK, 2006.
- Avolio, A.D.; Pensi, D.; Baietto, L.; Pacini, G.; Di Perri, G.; Francesco, P.; de Rosa, G. Daptomycin Pharmacokinetics and Pharmacodynamics in Septic and Critically Ill Patients. Drugs 2016, 76, 1161–1174. [Google Scholar] [CrossRef]
- Soraluce, A.; Asín-Prieto, E.; Rodríguez-Gascón, A.; Isla, A.; Barrasa, H.; Maynar, J.; Carcelero, E.; Soy, D. Population Pharmacokinetics of Daptomycin in Critically Ill Patients. Int. J. Antimicrob. Agents 2018, 52, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Nakafusa, J.; Misago, N.; Miura, Y.; Kayaba, M.; Tanaka, T.; Narisawa, Y. The Importance of Serum Creatine Phosphokinase Level in the Early Diagnosis, and as a Prognostic Factor, of Vibrio Vulnificus Infection. Br. J. Dermatol. 2001, 145, 280–284. [Google Scholar] [CrossRef] [PubMed]
- DN Gilbert. The Sanford Guide to Antimicrobial Therapy; BI Publications Pvt Ltd.: New Delhi, India, 2006. [Google Scholar]
- Canut, A.; Isla, A.; Betriu, C.; Gascón, A.R. Pharmacokinetic—Pharmacodynamic Evaluation of Daptomycin, Tigecycline, and Linezolid versus Vancomycin for the Treatment of MRSA Infections in Four Western European Countries. Eur. J. Clin. Microbiol. 2012, 31, 2227–2235. [Google Scholar] [CrossRef]
- Ukimura, A.; Oda, K.; Yoshida, M.; Nishihara, M.; Kawanishi, F.; Yamada, T.; Nakano, T.; Ooi, Y.; Uchida, T.; Shibata, Y.; et al. Observational Study to Determine the Optimal Dose of Daptomycin Based on Pharmacokinetic/Pharmacodynamic Analysis. J. Infect. Chemother. 2019, 26, 379–384. [Google Scholar] [CrossRef]
- Gray, D.A.; Wenzel, M. More Than a Pore: A Current Perspective on the In Vivo Mode of Action of the Lipopeptide Antibiotic Daptomycin. Antibiotics 2020, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- EUCAST Daptomycin: Rational for the EUCAST Clinical Breakpoints, Version 2. Mayo 2021. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Rationale_documents/Daptomycin_Rationale_Document_2.0_20210512.pdf (accessed on 31 May 2021).
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current Epidemiology and Antimicrobial Resistance Data for Bacterial Bloodstream Infections in Patients with Hematologic Malignancies: An Italian Multicentre Prospective Survey. Clin. Microbiol. Infect. 2015, 21, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Rolston, K.V.I.; Yadegarynia, D.; Kontoyiannis, D.P.; Raad, I.I.; Ho, D.H. The Spectrum of Gram-Positive Bloodstream Infections in Patients with Hematologic Malignancies, and the in Vitro Activity of Various Quinolones against Gram-Positive Bacteria Isolated from Cancer Patients. Int. J. Infect. Dis. 2006, 10, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Benvenuto, M.; Benziger, D.P.; Yankelev, S.; Vigliani, G. Pharmacokinetics and Tolerability of Daptomycin at Doses up to 12 Milligrams per Kilogram of Body Weight Once Daily in Healthy Volunteers. Antimicrob. Agents Chemother. 2006, 50, 3245–3249. [Google Scholar] [CrossRef]
- Dvorchik, B.; Arbeit, R.D.; Chung, J.; Liu, S.; Knebel, W.; Kastrissios, H. Population Pharmacokinetics of Daptomycin. Antimicrob. Agents Chemother. 2008, 48, 2799–2807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- di Paolo, A.; Tascini, C.; Polillo, M.; Gemignani, G.; Nielsen, E.I.; Bocci, G.; Karlsson, M.O.; Menichetti, F.; Danesi, R. Population Pharmacokinetics of Daptomycin in Patients Affected by Severe Gram-Positive Infections. Int. J. Antimicrob. Agents 2013, 42, 250–255. [Google Scholar] [CrossRef]
- Chaves, R.L.; Chakraborty, A.; Benziger, D.; Tannenbaum, S. Clinical and Pharmacokinetic Considerations for the Use of Daptomycin in Patients with Staphylococcus Aureus Bacteraemia and Severe Renal Impairment. J. Antimicrob. Chemother. 2014, 69, 200–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soon, R.L.; Turner, S.J.; Forrest, A.; Tsuji, B.T.; Brown, J. Pharmacokinetic/Pharmacodynamic Evaluation of the Efficacy and Safety of Daptomycin against Staphylococcus Aureus. Int. J. Antimicrob. Agents 2013, 42, 53–58. [Google Scholar] [CrossRef]
- Xu, X.; Khadzhynov, D.; Peters, H.; Chaves, R.L.; Hamed, K.; Levi, M.; Corti, N. Population Pharmacokinetics of Daptomycin in Adult Patients Undergoing Continuous Renal Replacement Therapy. Br. J. Clin. Pharmacol. 2017, 83, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Xie, F.; Li, S.; Cheng, Z. Population Pharmacokinetics and Dosing Considerations of Daptomycin in Critically Ill Patients Undergoing Continuous Renal Replacement Therapy. J. Antimicrob. Chemother. 2020, 75, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial Therapeutic Drug Monitoring in Critically Ill Adult Patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Liu, Y.; Wang, J.; Cai, L.; He, L.; Yang, X.; Xu, H.; He, X.; Yang, X.; Wei, C.; et al. Population Pharmacokinetics and Individual Analysis of Daptomycin in Kidney Transplant Recipients. Eur. J. Pharm. Sci. 2021, 162, 105818. [Google Scholar] [CrossRef]
- Grégoire, N.; Marchand, S.; Ferrandière, M.; Lasocki, S.; Seguin, P.; Vourc’h, M.; Barbaz, M.; Gaillard, T.; Launey, Y.; Asehnoune, K.; et al. Population Pharmacokinetics of Daptomycin in Critically Ill Patients with Various Degrees of Renal Impairment. J. Antimicrob. Chemother. 2018, 74, 117–125. [Google Scholar] [CrossRef]
- Geriak, M.; Haddad, F.; Rizvi, K.; Rose, W.; Kullar, R.; LaPlante, K.; Yu, M.; Vasina, L.; Ouellette, K.; Zervos, M.; et al. Clinical Data on Daptomycin plus Ceftaroline versus Standard of Care Monotherapy in the Treatment of Methicillin-Resistant Staphylococcus Aureus Bacteremia. Antimicrob. Agents Chemother. 2019, 63, e02483-18. [Google Scholar] [CrossRef]
- Wei, X.; Zhao, M.; Li, X.; Xiao, X. Pharmacokinetic/Pharmacodynamic Analysis of Daptomycin Against Staphylococcus aureus and Enterococcus faecium in Pediatric Patients by Monte Carlo Simulation. J. Clin. Pharmacol. 2020, 60, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Satlin, M.J.; Nicolau, D.P.; Humphries, R.M.; Kuti, J.L.; Campeau, S.A.; Lewis II, J.S.; Weinstein, M.P.; Jorgensen, J.H. Development of Daptomycin Susceptibility Breakpoints for Enterococcus Faecium and Revision of the Breakpoints for Other Enterococcal Species by the Clinical and Laboratory Standards Institute. Clin. Infect. Dis. 2019, 70, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Ogami, C.; Tsuji, Y.; Kasai, H.; Hiraki, Y.; Yamamoto, Y. Evaluation of Pharmacokinetics and the Stability of Daptomycin in Serum at Various Temperatures. Int. J. Infect. Dis. 2017, 57, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cockcroft, D.W.; Gault, H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Tobin, C.M.; Darville, J.M.; Lovering, A.M.; MacGowan, A.P. An HPLC Assay for Daptomycin in Serum. J. Antimicrob. Chemother. 2008, 62, 1462–1463. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, R.; Suzuki, Y.; Goto, K.; Yasuda, N.; Koga, H.; Kai, S.; Ohchi, Y.; Sato, Y.; Kitano, T.; Itoh, H. Development and Validation of Sensitive and Selective Quantification of Total and Free Daptomycin in Human Plasma Using Ultra-Performance Liquid Chromatography Coupled to Tandem Mass Spectrometry. J. Pharm. Biomed. Anal. 2019, 165, 56–64. [Google Scholar] [CrossRef]
- Lindbom, L.; Pihlgren, P.; Jonsson, N. PsN-Toolkit—A Collection of Computer Intensive Statistical Methods for Non-Linear Mixed Effect Modeling Using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef]
- Jun, H.; Rong, Y.; Yih, C.; Ho, J.; Cheng, W.; Kiang, T.K.L. Comparisons of Four Protein-Binding Models Characterizing the Pharmacokinetics of Unbound Phenytoin in Adult Patients Using Non-Linear Mixed-Effects Modeling. Drugs R & D 2020, 20, 343–358. [Google Scholar] [CrossRef]
- Aulin, L.B.S.; de Paepe, P.; Dhont, E.; de Jaeger, A.; vande Walle, J.; Vandenberghe, W.; McWhinney, B.C.; Ungerer, J.P.J.; van Hasselt, J.G.C.; de Cock, P.A.J.G. Population Pharmacokinetics of Unbound and Total Teicoplanin in Critically Ill Pediatric Patients. Clin. Pharmacokinet. 2021, 60, 353–363. [Google Scholar] [CrossRef]
- Charles, B.; Norris, R.; Xiao, X.; Hague, W. Population Pharmacokinetics of Metformin in Late Pregnancy. Ther. Drug Monit. 2006, 28, 67–72. [Google Scholar] [CrossRef]
- Hennig, S.; Norris, R.; Tu, Q.; van Breda, K.; Riney, K.; Foster, K.; Lister, B.; Charles, B. Population Pharmacokinetics of Phenytoin in Critically Ill Children. J. Clin. Pharmacol. 2015, 55, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Toutain, P.L.; Bousquet-Melou, A. Free Drug Fraction vs. Free Drug Concentration: A Matter of Frequent Confusion. J. Vet. Pharmacol. Ther. 2002, 25, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Heine, R.; Kane, S.P.; Huitema, A.D.R.; Krasowski, M.D.; Maarseveen, E.M. Nonlinear Protein Binding of Phenytoin in Clinical Practice: Development and Validation of a Mechanistic Prediction Model. Br. J. Clin. Pharmacol. 2019, 85, 2360–2368. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ohnmacht, C.; Hage, D.S. Studies of Phenytoin Binding to Human Serum Albumin by High-Performance Affinity Chromatography. J. Chromatogr. B 2004, 809, 137–145. [Google Scholar] [CrossRef]
- Musteata, F.M. Calculation of Normalized Drug Concentrations in the Presence of Altered Plasma Protein Binding. Clin. Pharmacokinet. 2012, 51, 55–68. [Google Scholar] [CrossRef]
- Savic, R.M.; Karlsson, M.O. Importance of Shrinkage in Empirical Bayes Estimates for Diagnostics: Problems and Solutions. AAPS J. 2009, 11, 558–569. [Google Scholar] [CrossRef] [Green Version]
- Wade, J.R.; Beal, S.L.; Sambol, N.C. Interaction between Structural, Statistical, and Covariate Models in Population Pharmacokinetic Analysis. J. Pharmacokinet. Biopharm. 1994, 22, 165–177. [Google Scholar] [CrossRef]
- Hooker, A.C.; Staatz, C.E.; Karlsson, M.O. Conditional Weighted Residuals (CWRES): A Model Diagnostic for the FOCE Method. Pharm. Res. 2007, 24, 2187–2197. [Google Scholar] [CrossRef]
- Comets, E.; Brendel, K.; Mentré, F. Computing Normalised Prediction Distribution Errors to Evaluate Nonlinear Mixed-Effect Models: The Npde Add-on Package for R. Comput. Methods Programs Biomed. 2008, 90, 154–166. [Google Scholar] [CrossRef] [Green Version]
- Sherwin, C.M.T.; Kiang, T.K.L.; Spigarelli, M.G.; Ensom, M.H.H. Fundamentals of Population Pharmacokinetic Modelling. Clin. Pharmacokinet. 2012, 51, 573–590. [Google Scholar] [CrossRef]
- Kiang, T.K.L.; Sherwin, C.M.T.; Spigarelli, M.G.; Ensom, M.H.H. Fundamentals of Population Pharmacokinetic Modelling. Clin. Pharmacokinet. 2012, 51, 515–525. [Google Scholar] [CrossRef]
- Bergstrand, M.; Hooker, A.C.; Wallin, J.E.; Karlsson, M.O. Prediction-Corrected Visual Predictive Checks for Diagnosing Nonlinear Mixed-Effects Models. AAPS J. 2011, 13, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhavnani, S.M.; Rubino, C.M.; Ambrose, P.G.; Drusano, G.L. Daptomycin Exposure and the Probability of Elevations in the Creatine Phosphokinase Level: Data from a Randomized Trial of Patients with Bacteremia and Endocarditis. Clin. Infect. Dis. 2010, 12208, 1568–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of Pharmacokinetic/Pharmacodynamic (PK/PD) Terminology for Anti-Infective Drugs: An Update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukada, H.; Tsuji, Y.; Yamashina, T.; Tsuruta, M.; Hiraki, Y.; Tsuruyama, M.; Ogami, C.; Kawasuji, H.; Sakamaki, I.; Yamamoto, Y. Pharmacokinetics and Pharmacodynamics of Daptomycin in a Clinical Setting. J. Infect. Chemother. 2020, 26, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Safdar, N.; Andes, D.; Craig, W.A. In Vivo Pharmacodynamic Activity of Daptomycin. Antimicrob. Agents Chemother. 2004, 48, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Schneider, E.K.; Huang, J.X.; Carbone, V.; Han, M.; Zhu, Y.; Nang, S.; Khoo, K.K.; Mak, J.; Cooper, M.A.; Li, J.; et al. Plasma Protein Binding Structure-Activity Relationships Related to the N-Terminus of Daptomycin. ACS Infect. Dis. 2017, 3, 249–258. [Google Scholar] [CrossRef]
- Sellers, E.M.; Koch-Weser, J. Clinical Implications of Drug-Albumin Interaction. In Albumin: Structure, Function and Uses; Rosenoer, V.M., Oratz, M., Rothschild, M.A., Eds.; Pergamon Press: Oxford, UK, 1977; pp. 159–182. [Google Scholar]
- Lai, C.-C.; Sheng, W.-H.; Wang, J.-T.; Cheng, A.; Chuang, Y.-C.; Chen, Y.-C.; Chang, S.-C. Safety and Efficacy of High-Dose Daptomycin as Salvage Therapy for Severe Gram-Positive Bacterial Sepsis in Hospitalized Adult Patients. BMC Infect. Dis. 2013, 13, 66. [Google Scholar] [CrossRef] [Green Version]
- Durante-Mangoni, E.; Andini, R.; Parrella, A.; Mattucci, I.; Cavezza, G.; Senese, A.; Trojaniello, C.; Caprioli, R.; Diana, M.V.; Utili, R. Safety of Treatment with High-Dose Daptomycin in 102 Patients with Infective Endocarditis. Int. J. Antimicrob. Agents 2016, 48, 61–68. [Google Scholar] [CrossRef]
- Casapao, A.M.; Kullar, R.; Davis, S.L.; Levine, D.P.; Zhao, J.J.; Potoski, B.A.; Goff, D.A.; Crank, C.W.; Segreti, J.; Sakoulas, G.; et al. Multicenter Study of High-Dose Daptomycin for Treatment of Enterococcal Infections. Antimicrob. Agents Chemother. 2013, 57, 4190–4196. [Google Scholar] [CrossRef]
- Kullar, R.; Casapao, A.M.; Davis, S.L.; Levine, D.P.; Zhao, J.J.; Crank, C.W.; Segreti, J.; Sakoulas, G.; Cosgrove, S.E.; Rybak, M.J. A Multicentre Evaluation of the Effectiveness and Safety of High-Dose Daptomycin for the Treatment of Infective Endocarditis. J. Antimicrob. Chemother. 2013, 68, 2921–2926. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.E.; Lindfield, K.C.; Steenbergen, J.N.; Benziger, D.P.; Blackerby, K.J.; Knapp, A.G.; Martone, W.J. A Pilot Study of High-Dose Short Duration Daptomycin for the Treatment of Patients with Complicated Skin and Skin Structure Infections Caused by Gram-Positive Bacteria. Int. J. Clin. Pract. 2008, 62, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Moise, P.A.; Hershberger, E.; Amodio-Groton, M.I.; Lamp, K.C. Safety and Clinical Outcomes When Utilizing High-Dose (≥8 Mg/Kg) Daptomycin Therapy. Ann. Pharmacother. 2009, 43, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Nicco, E.; Ginocchio, F.; Ansaldi, F.; de Florentiis, D.; Viscoli, C. High-Dose Daptomycin in Documented Staphylococcus Aureus Infections. Int. J. Antimicrob. Agents 2010, 36, 459–461. [Google Scholar] [CrossRef] [Green Version]
- Parra-Ruiz, J.; Peña-Monje, A.; Tomás-Jiménez, C.; Pomares-Mora, J.; Hernández-Quero, J. Eficacia y Seguridad de Daptomicina En Dosis Elevadas (≥8 mg/Kg/Día). Enferm. Infecc. Microbiol. Clin. 2011, 29, 425–427. [Google Scholar] [CrossRef]
- Kullar, R.; Davis, S.L.; Levine, D.P.; Zhao, J.J.; Crank, C.W.; Segreti, J.; Sakoulas, G.; Cosgrove, S.E.; Rybak, M.J. High-Dose Daptomycin for Treatment of Complicated Gram-Positive Infections: A Large, Multicenter, Retrospective Study. Pharmacotherapy 2011, 31, 527–536. [Google Scholar] [CrossRef]
- Gregoire, N.; Chauzy, A.; Buyck, J.; Rammaert, B.; Couet, W.; Marchand, S. Clinical Pharmacokinetics of Daptomycin. Clin. Pharmacokinet. 2020, 60, 271–281. [Google Scholar] [CrossRef]
- Reiber, C.; Senn, O.; Müller, D.; Kullak-ublick, G.A. Therapeutic Drug Monitoring of Daptomycin: A Retrospective Monocentric Analysis. Ther. Drug Monit. 2015, 37, 634–640. [Google Scholar] [CrossRef] [Green Version]
- Cojutti, P.G.; Candoni, A.; Ramos-martin, V.; Lazzarotto, D.; Zannier, M.E.; Fanin, R.; Hope, W.; Pea, F.; Carlo, M. Population Pharmacokinetics and Dosing Considerations for the Use of Daptomycin in Adult Patients with Haematological Malignancies. J. Antimicrob. Chemother. 2017, 72, 2342–2350. [Google Scholar] [CrossRef]
- Campos Moreno, E.; Merino Sanjuán, M.; Merino, V.; Nácher, A.; Algarra, R.V.M.; Casabó, V.G. Population Modelling to Describe Pharmacokinetics of Amiodarone in Rats: Relevance of Plasma Protein and Tissue Depot Binding. Eur. J. Pharm. Sci. 2007, 30, 190–197. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, K.; Gras-Colomer, E.; Climente-Martí, M.; Mangas-Sanjuán, V.; Merino-Sanjuán, M. Pharmacometric Characterization of Entero-Hepatic Circulation Processes of Orally Administered Formulations of Amiodarone under Complex Binding Kinetics. Eur. J. Pharm. Sci. 2022, 174, 106198. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 46 Patients Median (IQR)/n (%) | |
|---|---|---|
| Demographics | Sex (Male) (n, %) | 43 (93%) |
| Age (years) | 68 (59–81) | |
| Body weight (kg) | 75 (65–85) | |
| Height (m) | 1.7 (1.6–1.7) | |
| BMI (Kg/m2) | 25.9 (23.4–31.1) | |
| Treatment | Dose (mg) | 675 (500–765) |
| Dose per kilogram (mg/kg) | 9.1 (7.5–10.0) | |
| Treatment duration (days) | 11 (7–15) | |
| Clinical data | Serum albumin (g/dL) | 2.9 (2.4–3.4) |
| Serum protein (g/dL) | 6.0 (5.0–6.4) | |
| Serum cretinine (g/dL) | 0.9 (0.6–1.3) | |
| Creatinine clearance (mL/min/1.73 m2) | 93 (50–136) | |
| Renal function | ||
| >90 mL/min/1.73 m2 | 16 (34.9%) | |
| 60–89 mL/min/1.73 m2 | 13 (28.2%) | |
| 30–59 mL/min/1.73 m2 | 14 (30.4%) | |
| 15–29 mL/min/1.73 m2 | 3 (6.5%) | |
| <15 mL/min/1.73 m2 | 0 (0%) | |
| Pathogenic micro-organism (36/46) | S. aureus | 17 (47.2%) |
| S. epidermidis | 12 (33.3%) | |
| S. hominis | 2 (5.6%) | |
| E. fecalis | 2 (5.6%) | |
| S. sacrophyticus | 2 (5.6%) | |
| S. lugdunensis | 1 (2.7%) | |
| MIC micro-organism | 0.5 (0.25, 0.5) | |
| Population PK Model Estimates | Bootstrap Results | |||||
|---|---|---|---|---|---|---|
| Value | RSE (%) | Shrinkage (%) | Median | RSE * (%) | 95%CI | |
| Fixed-Effect | ||||||
| CL (L/h) | 6.98 | 14 | 7.01 | 15 | [6.63–7.44] | |
| V1 (L) | 0.95 | 9 | 0.97 | 10 | [0.92–1.09] | |
| Q (L/h) | 1.96 | 21 | 1.93 | 19 | [1.43–2.48] | |
| V2 (L/h) | 21 | 19 | 20.5 | 21 | [19.3–22.1] | |
| Bmax (mg/L) | 160 | 26 | 157 | 24 | [129–183] | |
| KD (mg/L) | 3.56 | 15 | 3.61 | 12 | [3.17–3.93] | |
| CrCl on CL | 0.19 | 12 | 0.19 | 13 | [0.18–0.22] | |
| Inter-individual variability | ||||||
| CL (%) | 32 | 11 | 12 | 33 | 10 | [21–42] |
| V2 (%) | 47 | 23 | 17 | 46 | 24 | [52–94] |
| Residual unexplained variability | ||||||
| Additive on Log-scale (%) | 22 | 8 | 5 | 21 | 8 | [18–24] |
| Moderate Renal Impairment (CLCR = 30 mL/min/1.73 m2) | Mild Renal Impairment (CLCR = 60 mL/min/1.73 m2) | Normal Renal Function (CLCR = 90 mL/min/1.73 m2) | Body Weight | |
|---|---|---|---|---|
| MIC ≤ 0.5 mg/L | 10 mg/kg q24h | 11 mg/kg q24h | 12 mg/kg q24h | 50 kg |
| 9 mg/kg q24h | 10 mg/kg q24h | 10 mg/kg q24h | 60 kg | |
| 8 mg/kg q24h | 9 mg/kg q24h | 9 mg/kg q24h | 70 kg | |
| 7 mg/kg q24h | 7 mg/kg q24h | 8 mg/kg q24h | 80 kg | |
| 6 mg/kg q24h | 7 mg/kg q24h | 7 mg/kg q24h | 90 kg | |
| 5 mg/kg q24h | 6 mg/kg q24h | 6 mg/kg q24h | 100 kg | |
| MIC ≤ 1 mg/L | 17 * mg/kg q48h | 17 * mg/kg q48h | 17 * mg/kg q48h | 50 kg |
| 16 mg/kg q48h | 17 * mg/kg q48h | 17 * mg/kg q48h | 60 kg | |
| 14 mg/kg q48h | 16 mg/kg q48h | 17 mg/kg q48h | 70 kg | |
| 12 mg/kg q48h | 14 mg/kg q48h | 15 mg/kg q48h | 80 kg | |
| 11 mg/kg q48h | 12 mg/kg q48h | 13 mg/kg q48h | 90 kg | |
| 10 mg/kg q48h | 11 mg/kg q48h | 12 mg/kg q48h | 100 kg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Martínez, T.; Bellés-Medall, M.D.; García-Cremades, M.; Ferrando-Piqueres, R.; Mangas-Sanjuán, V.; Merino-Sanjuan, M. Population Pharmacokinetic/Pharmacodynamic Modelling of Daptomycin for Schedule Optimization in Patients with Renal Impairment. Pharmaceutics 2022, 14, 2226. https://doi.org/10.3390/pharmaceutics14102226
García-Martínez T, Bellés-Medall MD, García-Cremades M, Ferrando-Piqueres R, Mangas-Sanjuán V, Merino-Sanjuan M. Population Pharmacokinetic/Pharmacodynamic Modelling of Daptomycin for Schedule Optimization in Patients with Renal Impairment. Pharmaceutics. 2022; 14(10):2226. https://doi.org/10.3390/pharmaceutics14102226
Chicago/Turabian StyleGarcía-Martínez, Teresa, María Dolores Bellés-Medall, Maria García-Cremades, Raúl Ferrando-Piqueres, Victor Mangas-Sanjuán, and Matilde Merino-Sanjuan. 2022. "Population Pharmacokinetic/Pharmacodynamic Modelling of Daptomycin for Schedule Optimization in Patients with Renal Impairment" Pharmaceutics 14, no. 10: 2226. https://doi.org/10.3390/pharmaceutics14102226