
Advancements in Rectal Drug Delivery Systems: Clinical Trials, and Patents Perspective
 ,
,  , and
, and
Abstract
:1. Introduction
- i.
- have poor gastrointestinal absorption
- ii.
- have low solubility, stability, and permeability
- iii.
- undergo extensive first-pass metabolism
- iv.
- cause irritation to the gastric mucosa
- v.
- are unstable or degradable in the gastrointestinal tract
- vi.
- have localized action in the rectum
- vii.
- could not be administered by any other route [4].
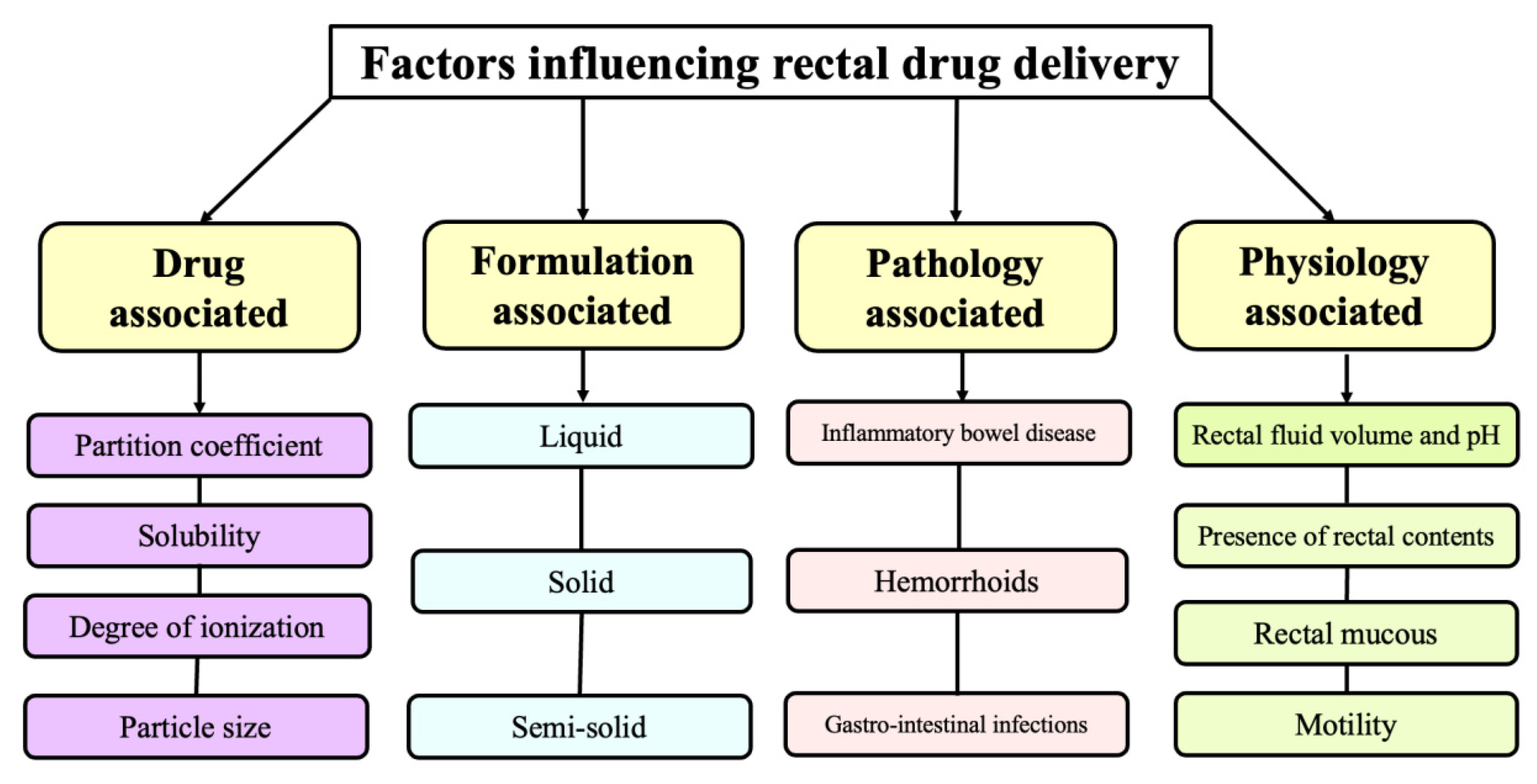
2. Factors Influencing Rectal Drug Delivery
2.1. Drug Associated Factors
2.1.1. Partition Coefficient
2.1.2. Solubility
2.1.3. Dissociation Constant and Degree of Ionization
2.1.4. Particle Size
2.2. Formulation Associated Factors
2.2.1. Liquid Formulations
2.2.2. Solid Formulations
2.2.3. Semi-Solid Dosage Forms
2.3. Physiology Associated Factors
2.3.1. Rectal Fluid Volume and pH
2.3.2. Presence of Rectal Contents
2.3.3. Rectal Mucous
2.3.4. Motility
2.4. Pathology Associated Factors
2.4.1. Inflammatory Bowel Disease (IBD)
2.4.2. Haemorrhoids
2.4.3. Gastro-Intestinal Infections
3. Rectal Diseases
3.1. Perianal Abscess
3.2. Hemorrhoids
3.3. Anal Cancer
3.4. Fissure In-Ano
3.5. Fistula In-Ano
3.6. Anal Abscess
3.7. Anal Warts
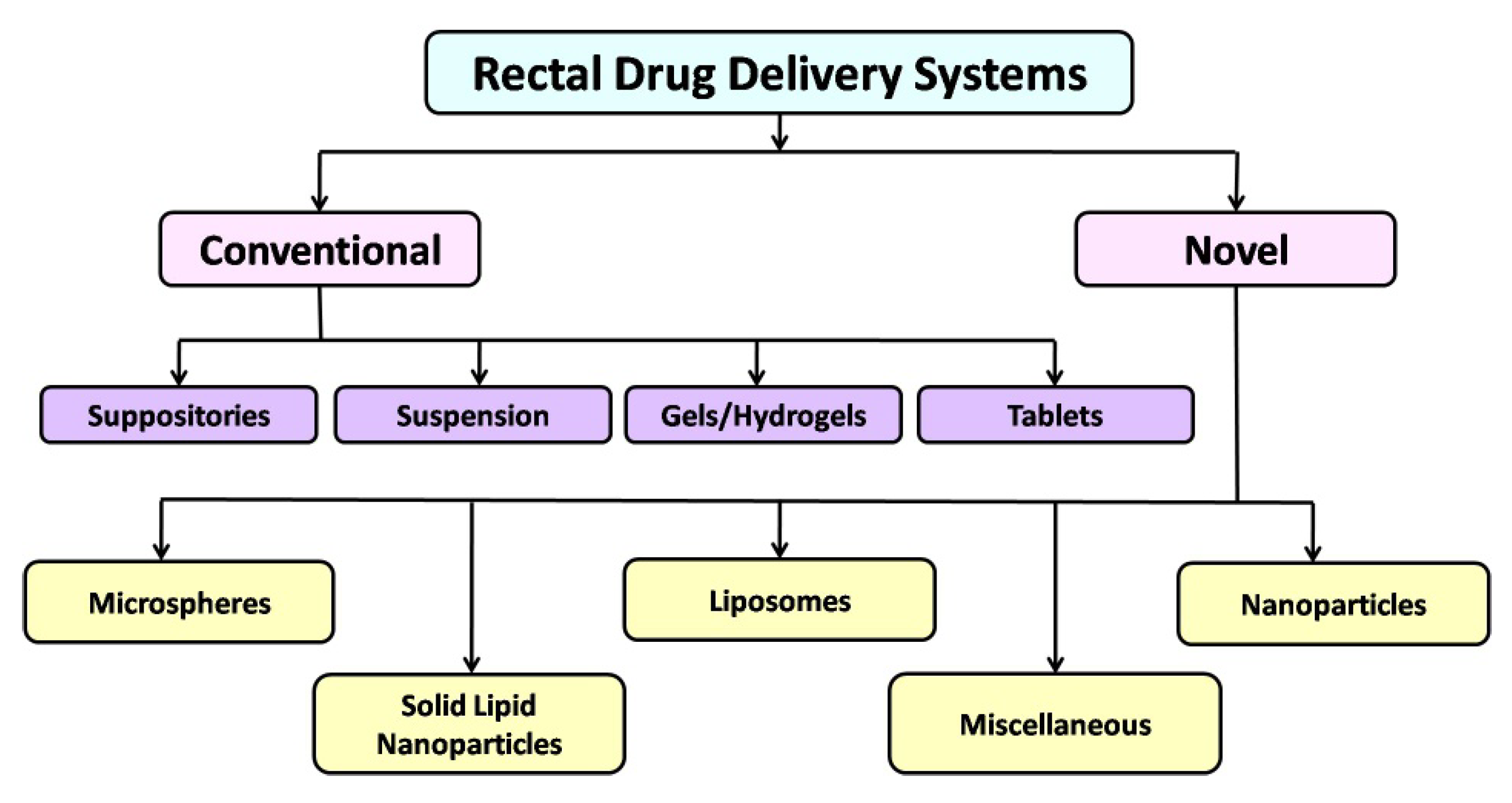
4. Rectal Drug Delivery Systems
4.1. Conventional Rectal Drug Delivery Systems
4.1.1. Suppositories
4.1.2. Rectal Suspension
4.1.3. Tablets
4.1.4. Gels and Hydrogels
4.2. Novel Rectal Drug Delivery Systems
4.2.1. Rectal Microspheres
4.2.2. Nanoparticles
4.2.3. Liposomes
4.2.4. Solid Lipid Nanoparticles
4.2.5. Miscellaneous
5. Rectal Formulations in Clinical Trials
6. Recent Advancements and Patented Formulations in Rectal DDS
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prasanna, J.L.; Deepthi, B.; Rao, N.R. Rectal drug delivery: A promising route for enhancing drug absorption. Asian J. Res. Pharm. Sci. 2012, 2, 143–149. [Google Scholar]
- Purohit, T.J.; Hanning, S.M.; Wu, Z. Advances in Rectal Drug Delivery Systems. Pharm. Dev. Technol. 2018, 23, 942–952. [Google Scholar] [CrossRef] [PubMed]
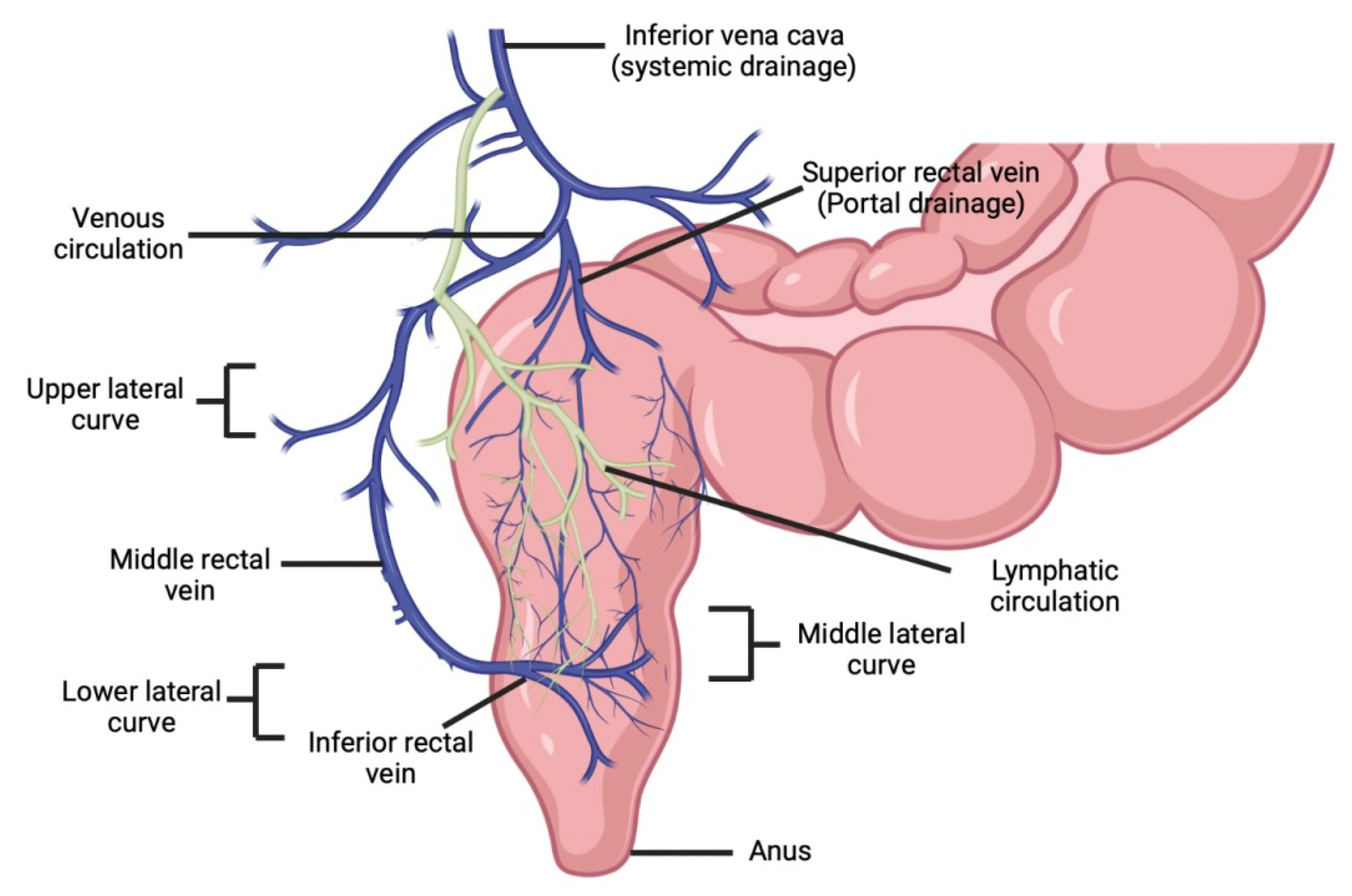
- Mahadevan, V. Anatomy of the rectum and anal canal. Surgery 2020, 38, 7–11. [Google Scholar]
- Jorge, J.M.; Wexner, S.D. Anatomy and physiology of the rectum and anus. Eur. J. Surg. 1997, 163, 723–731. [Google Scholar] [PubMed]
- Baviskar, P.; Bedse, A.; Sadique, S.; Kundea, V.; Jaiswal, S. Drug delivery on rectal absorption: Suppositories. Int. J. Pharm. Sci. Rev. Res. 2013, 21, 70–76. [Google Scholar]
- Savjani, K.T.; Gajjar, A.K.; Savjani, J.K. Drug Solubility: Importance and Enhancement Techniques. ISRN Pharm. 2012, 2012, 195727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, I.; Dastidar, D.G.; Ghosh, D.; Sengupta, A.; Ajala, T.O.; Odeku, O.A.; Singh, B.P.; Sharma, M. Bioadhesive films as drug delivery systems. Drug Deliv. Lett. 2021, 11, 2–15. [Google Scholar] [CrossRef]
- Arévalo-Pérez, R.; Maderuelo, C.; Lanao, J.M. Recent advances in colon drug delivery systems. J. Control. Release 2020, 327, 703–724. [Google Scholar] [CrossRef]
- Amidon, S.; Brown, J.E.; Dave, V.S. Colon-targeted oral drug delivery systems: Design trends and approaches. AAPS PharmSciTech 2015, 16, 731–741. [Google Scholar] [CrossRef]
- Yamamoto, A.; Muranishi, S. Rectal drug delivery systems Improvement of rectal peptide absorption by absorption enhancers, protease inhibitors and chemical modification. Adv. Drug Deliv. Rev. 1997, 28, 275–299. [Google Scholar] [CrossRef]
- Khan, M.S.; Roberts, M.S. Challenges and innovations of drug delivery in older age. Adv. Drug Deliv. Rev. 2018, 135, 3–38. [Google Scholar] [CrossRef]
- Kokate, A.; Marasanapalle, V.; Jasti, B.R.; Li, X. Physiological and biochemical barriers to drug delivery. In Design of Controlled Release Drug Delivery Systems; McGraw-Hill: New York, NY, USA, 2006; pp. 41–73. [Google Scholar]
- Sahnan, K.; Adegbola, S.O.; Tozer, P.J.; Watfah, J.; Phillips, R.K.; Hart, A.; Faiz, O.D. Natural history of anorectal sepsis. JBS 2017, 104, 1857–1865. [Google Scholar] [CrossRef]
- Malik, D.; Singh, I. Formulation and evaluation of press coated tablets of esomeprazole for colonic delivery. Asian J. Pharm. 2012, 6, 252. [Google Scholar]
- Thomson, W.H.F. The nature of haemorrhoids. BJS 1975, 62, 542–552. [Google Scholar] [CrossRef]
- Loder, P.B.; Kamm, M.A.; Nicholls, R.J.; Phillips, R.K. Haemorrhoids: Pathology, pathophysiology and aetiology. BJS 2005, 81, 946–954. [Google Scholar] [CrossRef]
- Avsar, A.F.; Keskin, H.L. Haemorrhoids during pregnancy. J. Obstet. Gynaecol. 2010, 30, 231–237. [Google Scholar] [CrossRef]
- Uronis, H.E.; Bendell, J.C. Anal cancer: An overview. Oncologist 2007, 12, 524–534. [Google Scholar] [CrossRef]
- Hardy, K.J.; Hughes, E.S.; Cuthbertson, A.M. Squamous cell carcinoma of the anal canal and anal margin. Aust. N. Z. J. Surg. 1969, 38, 301–305. [Google Scholar] [CrossRef]
- Johnson, L.G.; Madeleine, M.M.; Newcomer, L.M.; Schwartz, S.M.; Daling, J.R. Anal cancer incidence and survival: The surveillance, epidemiology, and end results experience, 1973–2000. Cancer 2004, 101, 281–288. [Google Scholar] [CrossRef]
- Salati, S.A.; Al Kadi, A. Anal cancer–A review. Int. J. Health Sci. 2012, 6, 206. [Google Scholar] [CrossRef]
- Hoots, B.E.; Palefsky, J.M.; Pimenta, J.M.; Smith, J.S. Human papillomavirus type distribution in anal cancer and anal intraepithelial lesions. Int. J. Cancer. 2009, 124, 2375–2383. [Google Scholar] [CrossRef]
- Clark, M.A.; Hartley, A.; Geh, J.I. Cancer of the anal canal. Lancet Oncol. 2004, 5, 149–157. [Google Scholar] [CrossRef]
- Rakinic, J. Anal fissure. Clin. Colon Rectal Surg. 2007, 20, 133–138. [Google Scholar] [CrossRef]
- Cerdán, F.J.; de León, A.R.; Azpiroz, F.; Martín, J.; Balibrea, J.L. Anal sphincteric pressure in fissure-in-ano before and after lateral internal sphincterotomy. Dis. Colon Rectum 1982, 25, 198–201. [Google Scholar] [CrossRef]
- Gupta, P.J. Treatment of fissure in ano-revisited. Afr. Health Sci. 2004, 4, 58–62. [Google Scholar]
- Sangwan, Y.P.; Rosen, L.; Riether, R.D.; Stasik, J.J.; Sheets, J.A.; Khubchandani, I.T. Is simple fistula-in-ano simple? Dis. Colon Rectum 1994, 37, 885–889. [Google Scholar] [CrossRef]
- El-Tawil, A.M. Management of fistula-in-ano: An introduction. World J. Gastroenterol. 2011, 17, 3271. [Google Scholar] [CrossRef]
- Sun, M.R.; Smith, M.P.; Kane, R.A. Current techniques in imaging of fistula in ano: Three-dimensional endoanal ultrasound and magnetic resonance imaging. Semin. Ultrasound CT MRI 2008, 29, 454–471. [Google Scholar] [CrossRef]
- Sneider, E.B.; Maykel, J.A. Anal abscess and fistula. Gastroenterol. Clin. N. Am. 2013, 42, 773–784. [Google Scholar] [CrossRef]
- Pigot, F. Anal abscesses and fistulas treatments. J. Chir. Viscerale. 2015, 152, S22–S28. [Google Scholar] [CrossRef]
- Seow-Choen, F.; Leong, A.F.; Goh, H.S. Results of a policy of selective immediate fistulotomy for primary anal abscess. ANZ J. Surg. 1993, 63, 485–489. [Google Scholar] [CrossRef]
- El-Attar, S.M.; Evans, D.V. Anal warts, sexually transmitted diseases, and anorectal conditions associated with human immunodeficiency virus. Prim. Care 1999, 26, 81. [Google Scholar] [CrossRef]
- Chang, J.; McLemore, E.; Tejirian, T. Anal health care basics. Perm J. 2016, 20, 15–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, A.G.; Moolenaar, F.; De Leede, L.G.J.; Breimer, D.D. Rectal drug administration. Clin. Pharmacokinet. 1982, 7, 285–311. [Google Scholar] [CrossRef] [PubMed]
- Havaldar, V.D.; Yadav, A.V.; Dias, R.J.; Mali, K.K.; Ghorpade, V.S.; Salunkhe, N.H. Rectal suppository as an effective alternative for oral administration. Res. J. Pharm. Technol. 2015, 8, 759–766. [Google Scholar] [CrossRef]
- Gupta, P.J. Suppositories in anal disorders: A review. Eur. Rev. Med. Pharmacol. Sci. 2007, 11, 165. [Google Scholar] [PubMed]
- Choi, H.G.; Jung, J.H.; Ryu, J.M.; Yoon, S.J.; Oh, Y.K.; Kim, C.K. Development of in situ-gelling and mucoadhesive acetaminophen liquid suppository. Int. J. Pharm. 1998, 165, 33–44. [Google Scholar] [CrossRef]
- Gugulothu, D.; Pathak, S.; Suryavanshi, S.; Sharma, S.; Patravale, V. Self-Microemulsifiyng Suppository Formulation of β-Artemether. AAPS PharmSciTech 2010, 11, 1179–1184. [Google Scholar] [CrossRef] [Green Version]
- El-Kamel, A.; El-Khatib, M. Thermally Reversible in situ Gelling Carbamazepine Liquid Suppository. Drug Deliv. 2006, 13, 143–148. [Google Scholar] [CrossRef]
- Idkaidek, N.M.; Amidon, G.L.; Smith, D.E.; Najib, N.M.; Hassan, M.M. Determination of the population pharmacokinetic parameters of sustained-release and enteric-coated oral formulations, and the suppository formulation of diclofenac sodium by simultaneous data fitting using NONMEM. Biopharm. Drug Dispos. 1998, 19, 169–174. [Google Scholar] [CrossRef]
- Kauss, T.; Gaubert, A.; Boyer, C.; Ba, B.B.; Manse, M.; Massip, S.; Gaudin, K. Pharmaceutical development and optimization of azithromycin suppository for paediatric use. Int. J. Pharm. 2013, 441, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Alotaibi, B.S.; Pervaiz, F.; Buabeid, M.; Ashames, A.; Fahelelbom, K.M.; Siddique, S.; Shoukat, H.; Rehman, S.; Noreen, S.; Murtaza, G. Nanostructured lipid carriers based suppository for enhanced rectal absorption of ondansetron: In vitro and in vivo evaluations. Arab. J. Chem. 2021, 14, 103426. [Google Scholar] [CrossRef]
- Gionchetti, P.; Rizzello, F.; Venturi, A.; Ferretti, M.; Brignola, C.; Miglioli, M.; Campieri, M. Comparison of oral with rectal mesalazine in the treatment of ulcerative proctitis. Dis. Colon Rectum 1998, 41, 93–97. [Google Scholar] [CrossRef]
- Lin, H.R.; Tseng, C.C.; Lin, Y.J.; Ling, M.H. A novel in-situ-gelling liquid suppository for site-targeting delivery of anti-colorectal cancer drugs. J. Biomater. Sci. Polym. Ed. 2012, 23, 807–822. [Google Scholar] [CrossRef]
- Alwan, L.A.; Al-Akkam, E.J. Formulation and In vitro Evaluation of Piroxicam Conventional and Hollow Suppositories. Proteins 2019, 6, 7. [Google Scholar] [CrossRef]
- Nief, R.A. Design and in vitro characterization of bisacodyl as a hollow-type suppositories. J. Pharm. Res. 2018, 12, 702–706. [Google Scholar]
- Akl, M.A.; Ismael, H.R.; Abd Allah, F.I.; Kassem, A.A.; Samy, A.M. Tolmetin sodium-loaded thermosensitive mucoadhesive liquid suppositories for rectal delivery; strategy to overcome oral delivery drawbacks. Drug Dev. Ind. Pharm. 2019, 45, 252–264. [Google Scholar] [CrossRef]
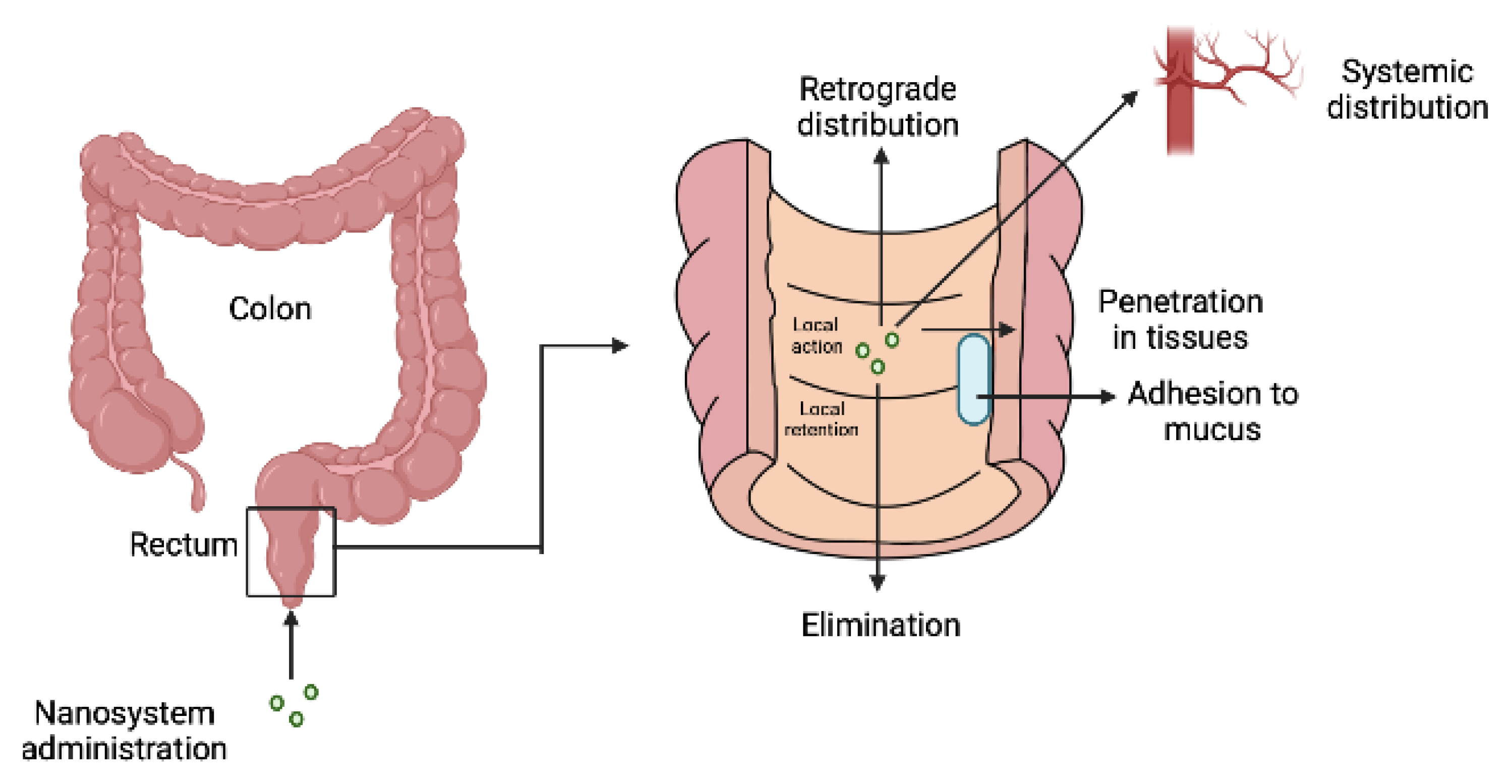
- Melo, M.; Nunes, R.; Sarmento, B.; das Neves, J. Rectal administration of nanosystems: From drug delivery to diagnostics. Mater. Today Chem. 2018, 10, 128–141. [Google Scholar] [CrossRef]
- Davis, M.P.; Walsh, D.; LeGrand, S.B.; Naughton, M. Symptom control in cancer patients: The clinical pharmacology and therapeutic role of suppositories and rectal suspensions. Support. Care Cancer 2002, 10, 117–138. [Google Scholar] [CrossRef]
- Vuong, M.T.; McBride, A.; Mishal, N.; Philipson, G. Topiramate rectal suspensions in pediatric patients. Seizure 2021, 85, 45–47. [Google Scholar] [CrossRef]
- Donnelly, R.F. Stability of Levodopa/Carbidopa Rectal Suspensions. Hosp. Pharm. 2016, 51, 915–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.M.; Liang, J.W.; Wang, Z.; Kou, J.T.; Zhou, Z.X. Effect of preoperative injection of carbon nanoparticle suspension on the outcomes of selected patients with mid-low rectal cancer. Chin. J. Cancer 2016, 35, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, S.B.; Gao, X.S.; Li, H.Z.; Liu, C.X.; Hou, D.L.; Nian, W.D.; Li, X.Y.; Wang, D. Intra-rectal use of epinephrine in radiotherapy of prostate cancer. Cancer Manag. Res. 2019, 11, 4847–4854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moawad, F.A.; Khan, R.U.; El-Refaey, H.; Sharma, S.; Sooranna, D.; Stafford, M. Oral, rectal, and vaginal pharmacokinetics of misoprostol. Obstet. Gynecol. 2004, 103, 866–870. [Google Scholar]
- Shojai, R.; Piéchon, L.; D’Ercole, C.; Boubli, L.; Pontiès, J.E. Rectal Administration of Misoprostol for Delivery Induced Hemorrhage. Preliminary Study. J. Gynecol. Obstet. Biol. Reprod. 2001, 30, 572–575. [Google Scholar]
- Birnbaum, A.K.; Kriel, R.L.; Burkhardt, R.T.; Remmel, R.P. Rectal Absorption of Lamotrigine Compressed Tablets. Epilepsia 2000, 41, 850–853. [Google Scholar] [CrossRef] [Green Version]
- Swamy, P.V.; Ali, M.Y.; Kumar, Y.A.; Prasad, K.; Srinivaslu, N. Design and evaluation of rectal drug delivery systems of non-steroidal anti-inflammatory drug. Int. Pharm. J. 2012, 1, 165–170. [Google Scholar] [CrossRef]
- Mohanty, D.; Bakshi, V.; Simharaju, N.; Haque, M.A.; Sahoo, C.K. A review on in situ gel: A novel drug delivery system. Int. J. Pharm. Sci. Rev. Res. 2018, 50, 175–181. [Google Scholar]
- Edsman, K.; Hägerström, H. Pharmaceutical applications of mucoadhesion for the non-oral routes. J. Pharm. Pharmacol. 2005, 57, 3–22. [Google Scholar] [CrossRef]
- Onaciu, A.; Munteanu, R.A.; Moldovan, A.I.; Moldovan, C.S.; Berindan-Neagoe, I. Hydrogels Based Drug Delivery Synthesis, Characterization and Administration. Pharmaceutics 2019, 11, 432. [Google Scholar] [CrossRef] [Green Version]
- Sri, B.; Ashok, V.; Arkendu, C. As a Review on Hydrogels as Drug Delivery in the Pharmaceutical Field. Int. J. Pharm. Chem. Sci. 2012, 1, 642–661. [Google Scholar]
- Ciolacu, D.E.; Nicu, R.; Ciolacu, F. Cellulose-Based Hydrogels as Sustained Drug-Delivery Systems. Materials 2020, 13, 5270. [Google Scholar] [CrossRef]
- Xu, J.; Tam, M.; Samaei, S.; Lerouge, S.; Barralet, J.; Stevenson, M.M.; Cerruti, M. Mucoadhesive Chitosan Hydrogels as Rectal Drug Delivery Vessels to Treat Ulcerative Colitis. Acta Biomater. 2017, 48, 247–257. [Google Scholar] [CrossRef]
- Nazeri, M.T.; Javanbakht, S.; Shaabani, A.; Ghorbani, M. 5-Aminopyrazole-Conjugated Gelatin Hydrogel: A Controlled 5-Fluorouracil Delivery System for Rectal Administration. J. Drug Deliv. Sci. Technol. 2020, 57, 101669. [Google Scholar] [CrossRef]
- Dabbagh, M.A.; Ameri, A.; Honarmand, M. Preparation of Diazepam Rectal Gel Using Cellulose Polymers. Jundishapur J. Nat. Pharm. Prod. 2007, 2, 34–44. [Google Scholar]
- Fawaz, F.; Koffi, A.; Guyot, M.; Millet, P. Comparative in Vitro–in Vivo Study of Two Quinine Rectal Gel Formulations. Int. J. Pharm. 2004, 280, 151–162. [Google Scholar] [CrossRef]
- Miyazaki, S.; Yokouchi, C.; Nakamura, T.; Hashiguchi, N.; Hou, W.M.; Takada, M. Pluronic F-127 Gels as a Novel Vehicle for Rectal Administration of Indomethacin. Chem. Pharm. Bull. 1986, 34, 1801–1808. [Google Scholar] [CrossRef] [Green Version]
- Cereghino, J.J.; Mitchell, W.G.; Murphy, J.; Kriel, R.L.; Rosenfeld, W.E.; Trevathan, E. Treating Repetitive Seizures with a Rectal Diazepam Formulation: A Randomized Study. Neurology 1998, 51, 1274–1282. [Google Scholar] [CrossRef]
- Parekh, H.B.; Jivani, R.; Jivani, N.P.; Patel, L.D.; Makwana, A.; Sameja, K. Novel insitu polymeric drug delivery system: A review. J. Drug Deliv. Ther. 2012, 2, 136–145. [Google Scholar] [CrossRef]
- Rachmawati, H.; Pradana, A.T.; Safitri, D.; Adnyana, I.K. Multiple Functions of D-α-Tocopherol Polyethylene Glycol 1000 Succinate (TPGS) as Curcumin Nanoparticle Stabilizer: In Vivo Kinetic Profile and Anti-Ulcerative Colitis Analysis in Animal Model. Pharmaceutics 2017, 9, 24. [Google Scholar] [CrossRef]
- Moqejwa, T.; Marimuthu, T.; Kondiah, P.P.; Choonara, Y.E. Development of Stable Nano-Sized Transfersomes as a Rectal Colloid for Enhanced Delivery of Cannabidiol. Pharmaceutics 2022, 14, 703. [Google Scholar] [CrossRef]
- Seo, Y.G.; Kim, D.W.; Yeo, W.H.; Ramasamy, T.; Oh, Y.K.; Park, Y.J.; Kim, J.; Oh, D.H.; Ku, S.K.; Kim, J.K.; et al. Docetaxel-loaded thermosensitive and bioadhesive nanomicelles as a rectal drug delivery system for enhanced chemotherapeutic effect. Pharm. Res. 2013, 30, 1860–1870. [Google Scholar] [CrossRef]
- Vyvyan, H.A.L.; Hanafiah, Z. Patients’ attitudes to rectal drug administration. Anaesthesia 1995, 50, 983–984. [Google Scholar] [CrossRef]
- Singh, S.; Arora, S.; Allawadi, D. Formulation, optimization and evaluation of sustained release microspheres using Taguchi design. J. Pharm. Technol. Res. Manag. 2014, 2, 1–2. [Google Scholar] [CrossRef]
- Sharma, N.; Purwar, N.; Gupta, P.C. Microspheres as Drug Carriers for Controlled Drug Delivery: A Review. Int. J. Pharm. Sci. Res. 2015, 6, 4579. [Google Scholar]
- Ofokansi, K.C.; Adikwu, M.U. Formulation and evaluation of microspheres based on gelatin-mucin admixtures for the rectal delivery of cefuroxime sodium. Trop. J. Pharm. Res. 2007, 6, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Havaldar, V.D.; Yadav, A.V.; Dias, R.J.; Mali, K.K.; Kale, S.S.; Pujari, P.P. Rectal Suppository of Mucoadhesive Microspheres of Alverine Citrate for İrritable Bowel Disease: In vitro Evaluation. Res. J. Pharm. Technol. 2018, 11, 3091–3098. [Google Scholar] [CrossRef]
- El-Leithy, E.S.; Shaker, D.S.; Ghorab, M.K.; Abdel-Rashid, R.S. Evaluation of mucoadhesive hydrogels loaded with diclofenac sodium-chitosan microspheres for rectal administration. AAPS PharmSciTech 2010, 11, 1695–1702. [Google Scholar] [CrossRef]
- Palma, E.; Costa, N.; Molinaro, R.; Francardi, M.; Paolino, D.; Cosco, D.; Fresta, M. Improvement of the therapeutic treatment of inflammatory bowel diseases following rectal administration of mesalazine-loaded chitosan microparticles vs. Asamax®. Carbohydr. Polym. 2019, 212, 430–438. [Google Scholar] [CrossRef]
- Kietzmann, D.; Moulari, B.; Béduneau, A.; Pellequer, Y.; Lamprecht, A. Colonic delivery of carboxyfluorescein by pH-sensitive microspheres in experimental colitis. Eur. J. Biopharm. Pharm. 2010, 76, 290–295. [Google Scholar] [CrossRef]
- Pratt, E.C.; Shaffer, T.M.; Grimm, J. Nanoparticles and radiotracers: Advances toward radionanomedicine. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2016, 8, 872–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelvetro, V.; De Vita, C. Nanostructured Hybrid Materials from Aqueous Polymer Dispersions. Adv. Colloid Interface Sci. 2004, 108–109, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Qiao, Z.A.; Dai, S. Recent advances in carbon nanospheres: Synthetic routes and applications. Chem. Commun. 2015, 51, 9246–9256. [Google Scholar] [CrossRef]
- Neves, J.; Araujo, F.; Andrade, F.; Michiels, J.; Arien, K.K.; Vanham, G.; Amiji, M.; Bahia, M.F.; Sarmento, B. In Vitro and Ex Vivo Evaluation of Polymeric Nanoparticles for Vaginal and Rectal Delivery of the Anti-HIV Drug Dapivirine. Mol. Pharm. 2013, 10, 2793–2807. [Google Scholar] [CrossRef]
- Maisel, K.; Ensign, L.; Reddy, M.; Cone, R.; Hanes, J. Effect of surface chemistry on nanoparticle interaction with gastrointestinal mucus and distribution in the gastrointestinal tract following oral and rectal administration in the mouse. J. Control. Release 2015, 197, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Nunes, R.; Araújo, F.; Barreiros, F.; Bártolo, I.; Segundo, M.A.; Taveira, N.; Sarmento, B.; Neves, J. Noncovalent PEG Coating of Nanoparticle Drug Carriers Improves the Local Pharmacokinetics of Rectal Anti-HIV Microbicides. ACS Appl. Mater. Interfaces 2018, 10, 34942–34953. [Google Scholar] [CrossRef]
- Mahajan, N.; Sakarkar, D.; Manmode, A.; Pathak, V.; Ingole, R.; Dewade, D. Biodegradable nanoparticles for targeted delivery in treatment of ulcerative colitis. Adv. Sci. Lett. 2011, 4, 349–356. [Google Scholar] [CrossRef]
- Sawant, R.R.; Torchilin, V.P. Liposomes as ‘smart’ pharmaceutical nanocarriers. Soft Matter 2010, 6, 4026–4044. [Google Scholar] [CrossRef]
- Jesorka, A.; Orwar, O. Liposomes: Technologies and analytical applications. Annu. Rev. Anal. Chem. 2008, 1, 801–832. [Google Scholar] [CrossRef]
- Zhou, F.; Kraehenbuhl, J.P.; Neutra, M.R. Mucosal IgA response to rectally administered antigen formulated in IgA-coated liposomes. Vaccine 1995, 13, 637–644. [Google Scholar] [CrossRef]
- Gabev, E.E.; Svilenov, D.K.; Poljakova-Krusteva, O.T.; Vassilev, I. Brain, Liver and Spleen Detection of Liposomes after Rectal Administration. J. Microencapsul. 1985, 2, 85–89. [Google Scholar] [CrossRef]
- Scavo, M.P.; Cutrignelli, A.; Depalo, N.; Fanizza, E.; Laquintana, V.; Gasparini, G.; Giannelli, G.; Denora, N. Effectiveness of a controlled 5-FU delivery based on FZD10 antibody-conjugated liposomes in colorectal cancer in vitro models. Pharmaceutics 2020, 12, 650. [Google Scholar] [CrossRef]
- Abdelbary, G.; Fahmy, R.H. Diazepam-loaded solid lipid nanoparticles: Design and characterization. AAPS PharmSciTech 2009, 10, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Hu, P.Y.; Wu, Q.Y.; Xia, M.Y.; Zhang, W.L.; Lei, Z.Q.; Li, D.X.; Zhang, G.S.; Feng, J.F. Preparation, in vitro and in vivo Evaluation of Thermosensitive in situ Gel Loaded with Ibuprofen-Solid Lipid Nanoparticles for Rectal Delivery. Drug Des. Develop. Ther. 2022, 16, 1407. [Google Scholar] [CrossRef]
- Xing, R.; Mustapha, O.; Ali, T.; Rehman, M.; Zaidi, S.S.; Baseer, A.; Batool, S.; Mukhtiar, M.; Shafique, S.; Malik, M.; et al. Development, characterization, and evaluation of SLN-loaded thermoresponsive hydrogel system of topotecan as biological macromolecule for colorectal delivery. BioMed Res. Int. 2021, 2021, 9968602. [Google Scholar] [CrossRef]
- Din, F.U.; Jin, S.G.; Choi, H.G. Particle and gel characterization of irinotecan-loaded double-reverse thermosensitive hydrogel. Polymers 2021, 13, 551. [Google Scholar] [CrossRef] [PubMed]
- Ud Din, F.; Mustapha, O.; Kim, D.W.; Rashid, R.; Park, J.H.; Choi, J.Y.; Ku, S.K.; Yong, C.S.; Kim, J.O.; Choi, H.G. Novel dual-reverse thermosensitive solid lipid nanoparticle-loaded hydrogel for rectal administration of flurbiprofen with improved bioavailability and reduced initial burst effect. Eur. J. Pharm. Biopharm. 2015, 94, 64–72. [Google Scholar] [CrossRef]
- Sznitowska, M.; Gajewska, M.; Janicki, S.; Radwanska, A.; Lukowski, G. Bioavailability of Diazepam from Aqueous-Organic Solution, Submicron Emulsion and Solid Lipid Nanoparticles after Rectal Administration in Rabbits. Eur. J. Pharm. Biopharm. 2001, 52, 159–163. [Google Scholar] [CrossRef]
- Kamel, R.; Basha, M.; Abd El-Alim, S.H. Development of a Novel Vesicular System Using a Binary Mixture of Sorbitan Monostearate and Polyethylene Glycol Fatty Acid Esters for Rectal Delivery of Rutin. J. Liposome Res. 2013, 23, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Moawad, F.A.; Ali, A.A.; Salem, F.H. Nanotransfersomes loaded thermosensitive insitu gel as a rectal delivery system of tizanidine HCl: Preparation, invitro and invivo performance. Drug Deliv. 2017, 24, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Maeda, M.; Nakano, Y.; Aoyama, T.; Matsumoto, Y.; Fujito, H. Study on rectal administration of azithromycin by suppository application in children. Int. J. Clin. Pharmacol. Ther. 2016, 54, 263. [Google Scholar] [CrossRef] [PubMed]
- Mpimbaza, A.; Ndeezi, G.; Staedke, S.; Rosenthal, P.J.; Byarugaba, J. Comparison of buccal midazolam with rectal diazepam in the treatment of prolonged seizures in ugandan children: A randomized clinical trial. Pediatrics 2008, 121, E58–E64. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, H.; Khodadoost, M.F. Rectal Diclofenac versus High-Dose Rectal Acetaminophen in Children: A Randomized Clinical Trial. Casp. J. Intern. Med. 2021, 12, 207. [Google Scholar]
- Hussain, A. Comparison of the Efficacy of Postoperative Diclofenac Suppository with Intramuscular Diclofenac in Children Undergoing Inguinal Hernia Surgery. J. Islam. Med. Dent. Coll. 2017, 6, 165–169. [Google Scholar]
- Hagen, I.J.; Haram, E.M.; Laake, K. Absorption of paracetamol from suppositories in geriatric patients with fecal accumulation in the rectum. Aging 1991, 3, 25–29. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov (accessed on 31 August 2022).
- Hua, S. Physiological and Pharmaceutical Considerations for Rectal Drug Formulations. Front. Pharacol. 2019, 10, 1196. [Google Scholar] [CrossRef]
- Ocampo, S.M.; Romero, C.; Aviñó, A.; Burgueño, J.; Gassull, M.A.; Bermúdez, J.; Eritja, R.; Fernandez, E.; Perales, J.C. Functionally enhanced siRNA targeting TNFα attenuates DSS-induced colitis and TLR-mediated immunostimulation in mice. Mol. Ther. 2012, 20, 382–390. [Google Scholar] [CrossRef]
- Sik, K.K. Omeprazole Compositions Designed for Administration in Rectum. CA Patent 2037101A1, 18 March 1997. [Google Scholar]
- Heil, B. Suppository for Rectal, Vaginal or Urethral Administration Containing a Probiotic, an Antibiotic and an Unsaturated Non-Esterified Fatty Acid. U.S. Patent 20120237489A1, 20 September 2012. [Google Scholar]
- Gauthier, C.; Dumoulin, Y.; Powell, D. Mesalamine Suppository. U.S. Patent 8217083B2, 10 July 2012. [Google Scholar]
- Stremmel, W. Phosphatidylcholine as Medication with Protective Effect Large Intestinal Mucosa. U.S. Patent 6677319B1, 13 January 2004. [Google Scholar]
- Metz, C. Suppository Comprising Pantoprazole. WO Patent 2011072861A1, 23 June 2011. [Google Scholar]
- Mikulasik, E.; Szakaly, P. Glycerol-Free Osmotic Laxative Suppository. WO Patent 2010143004A2, 16 December 2010. [Google Scholar]
- Matsui, M.; Ohki, T.; Wada, K. Meloxicam Suppositories Containing e.g., Polyethylenglycol. EP Patent 1492538A1, 5 January 2005. [Google Scholar]
- Purandare, M.S.; Malhotra, G. Pharmaceutical Compositions for Rectal Administration. U.S. Patent 20160002278A1, 7 January 2016. [Google Scholar]
- Shilan, Z. Safety Quick Effective Rectal Suppository Made of Glycerine, Sodium Chloride and Water. CN Patent 1251686C, 19 April 2006. [Google Scholar]
- Lubowski, D. Combination Laxative Compositions Comprising a Colonic Stimulant and a Bulking Laxative. WO Patent 2008141368A1, 27 November 2008. [Google Scholar]
- Bellinvia, S.; Demartis, S.; Viti, F. Compositions for Rectal Administration in the Treatment of Ulcerative Colitis and Methods of Using Same. WO Patent 2017046343A1, 23 March 2017. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Nanosystem | Drug/Moiety | Key Outcomes | Ref. |
|---|---|---|---|---|
| 1 | Nanoparticle | Curcumin | A seven- fold increase in bioavailability was observed. | [71] |
| 2 | Nano-transferosomes | Cannabidiol | Nano-transferosomes showed improved diffusivity and permeation across excised colorectal membrane. | [72] |
| 3 | Thermosensitive and bioadhesive nano-micelles | Docetaxel | Nanomicelles showed the ability to improve bioavailability and chemotherapeutic potential of Docetaxel in vivo. | [73] |
| 4 | Mucoadhesive microspheres | Ceftriaxone sodium | The in vivo studies in male Wistar rats revealed increase drug release and bioavailability of drug. | [77] |
| 5 | Mucoadhesive microspheres rectal suppository | Alverine Citrate | Sustained drug release was observed and found useful in treating inflammatory bowel syndrome. | [78] |
| 6 | Mucoadhesive hydrogel microsphere | Diclofenac sodium | 34–39% drug release was observed at the end of 6 h and no irritation was observed histopathologically. | [79] |
| 7 | Microparticles | Mesalazine | Microparticles showed efficient drug retention and the in vitro and in vivo studies confirm its mucoadhesion and therapeutic efficacy at a lower dose (13 mg/kg) than marketed formulation (26 mg/kg). | [80] |
| 8 | pH-sensitive microspheres | Carboxyfluorescein | The microspheres led to a higher local drug concentration in the colonic tissue. | [81] |
| 9 | Polymeric nanoparticles | Dapivirine | Increased drug retention was observed on rectal administration than pure drug. | [85] |
| 10 | Mucoadhesive nanoparticle and non-mucoadhesive nanoparticle | - | Nanoparticles administered via rectal route showed increased drug distribution than oral route. | [86] |
| 11 | PEG CoatedNanoparticle | Efavirenz | The efavirenz nanoparticle were found to be safe after once daily administration for 14 days. | [87] |
| 12 | Nanoparticle | Meselamine | The nanoparticles absorbed and retain for much longer time providing systemic drug action. The inflammation produced by UC was also reduced. | [88] |
| 13 | IgA coated Liposomes | - | The coloniclrectal IgA response to liposomal ferritin was significantly enhanced. | [91] |
| 14 | Bangham-type liposomes | - | Rectal administration of liposome showed that blood-brain barrier can be overcome. | [92] |
| 15 | Liposomes | 5-fluorouracil | Enhanced cytotoxic effect of 5-fluorouracil as compared to pure 5-fluorouracil and found to potential carriers for rectal administration. | [93] |
| 16 | In situ gel loaded with solid lipid nanoparticle (ISG-SLN) | Ibuprofen | In comparison with IBU-SLN, IBU-SLN-ISG showed initial burst release followed by sustained release and produced much better absorption of IBU and improved bioavailability in rat with no irritation or damage to rectal tissues, and retained in the rectum for a long time. | [95] |
| 17 | SLN-Loaded Thermoresponsive Hydrogel | Topotecan | In vivo studies in rat rectum showed controlled drug release over extended period of time. The SLNs showed improved bioavailability, plasma concentration, and anti-tumor effect with no toxicity. | [96] |
| 18 | Irinotecan-solid lipid nanoparticles loaded double reverse thermosensitive hydrogel (DRTH) | Irinotecan | The DRTH showed easy administration, fast gelling, and strong gel-forming in the body. | [97] |
| 29 | Dual-reverse thermosensitive solid lipid nanoparticle-loaded hydrogel | Flurbiprofen | Increased drug dissolution rate and plasma concentration were observed. No damage to rectal mucosa with improved bioavailability and reduced initial burst effect was identified. | [98] |
| 20 | Solid lipid nanoparticle | Diazepam | The relative bioavailability of SLN was low (47%) compared to the aqueous organic solution. | [99] |
| 21 | Pro-Niosomes | Rutin | The pro-niosomes showed maximum drug release (up to 98%) and maximum drug deposition in the rectal walls. | [100] |
| 22 | Transferosomes | Tizanidine | 2 times more bioavailability and a longer half-life via rectal route than the oral administered drug in rabbits. | [101] |
| S. No. | Drug | NCT Number | Condition | Status |
|---|---|---|---|---|
| 1 | NRC001 | NCT00857467 | Fecal Incontinence | Completed |
| 2 | NRC001 | NCT01265485 | Fecal Incontinence | Completed |
| 3 | NRC001 | NCT00893607 | Fecal Incontinence | Completed |
| 4 | NRC001 | NCT01175941 | Fecal Incontinence | Completed |
| 5 | Nifedipine | NCT00972907 | Chronic Anal Fissure | Completed |
| 6 | Nifedipine | NCT02023047 | Chronic Anal Fissure | Completed |
| 7 | Budesonide | NCT01966783 | Proctitis | Completed |
| 8 | Mesalamine | NCT01172444 | Proctitis | Terminated |
| 9 | AnucortHC | NCT01913158 | Internal Hemorrhoids | Completed |
| 10 | Hydrocortisone Acetate | NCT03335774 | Internal Hemorrhoids | Completed |
| 11 | Asacol | NCT05091775 | Fissure in Ano Diarrhea | Completed |
| 12 | Hydrocortisone acetate | NCT04469686 | Ulcerative Proctitis | Recruiting |
| 13 | Flucortolone & Lidocaine | NCT03757078 | Acute Hemorrhoids | Completed |
| 14 | MAX-002 | NCT01016262 | Proctitis, Ulcerative | Terminated |
| 15 | Dendrobium Huoshanense | NCT05079438 | Locally Advanced Rectal Cancer | Recruiting |
| 16 | 1R, 2Smethoxamine hydrochloride | NCT01656720 | Faecal Incontinence | Completed |
| 17 | Bisacodyl | NCT02609607 | Constipation Fecal Incontinence Multiple Sclerosis | Terminated |
| S. No. | Drug | NCT Number | Condition | Status |
|---|---|---|---|---|
| Microspheres | ||||
| 1 | Irinotecan | NCT03086096 | Colorectal Carcinoma Neoplasm Metastasis | Completed |
| 2 | FOLFOX | NCT00724503 | Colorectal Cancer Colorectal Carcinoma Liver Metastases | Completed |
| 3 | Regorafenib | NCT02195011 | Colorectal Neoplasms | Completed |
| 4 | FOLFOX6m | NCT01721954 | Colorectal Cancer Metastatic | Completed |
| 5 | FOLFOX6, Bevacizumab | NCT00735241 | Colorectal Carcinoma Liver Metastases | Withdrawn |
| 6 | Cetuximab, Irinotecan | NCT00766220 | Colon Cancer Colorectal Cancer | Withdrawn |
| Nanoparticles | ||||
| 7 | AGuIX gadolinium-based nanoparticles | NCT04899908 | Brain Cancer Brain Metastases Melanoma Lung Cancer Breast Cancer HER2-positive Breast Cancer Colorectal Cancer Gastrointestinal Cancer SRS SRT | Recruiting |
| 8 | TKM-080301 | NCT01437007 | Colorectal Cancer with Hepatic Metastases | Completed |
| 9 | Indocyanine green | NCT05092750 | Colorectal Cancer | Not yet recruiting |
| Liposomes | ||||
| 10 | Irinotecan HCl Floxuridine | NCT00361842 | Colorectal Neoplasms | Completed |
| 11 | SN-38 liposome | NCT00311610 | Colorectal Cancer | Completed |
| 12 | Fluorouracil Irinotecan Sucrosofate Leucovorin Calcium Rucaparib | NCT03337087 | Metastatic Colorectal, Carcinoma Stage IVA Colorectal Cancer AJCC v7 Stage IVB Colorectal Cancer AJCC v7 | Recruiting |
| 13 | Bevacizumab, Fluorouracil, Irinotecan hydrochloride leucovorin calcium irinotecan hydrochloride PEP02 Bevacizumab | NCT01375816 | Colorectal Cancer | Terminated |
| 14 | Promitil Capecitabine Bevacizumab | NCT01705002 | Colorectal Cancer | Completed |
| S. No. | Drug | NCT Number | Condition | Status |
|---|---|---|---|---|
| 1 | Lidocaine Hydrochloride | NCT03797703 | Hemorrhoids | Completed |
| 2 | Pico-Salax, fleet enema | NCT05148494 | Colorectal Neoplasms | Recruiting |
| 3 | Niclosamide | NCT03521232 | Ulcerative Colitis Ulcerative Proctitis Ulcerative Proctosigmoiditis | Recruiting |
| 4 | Fleet | NCT02468726 | Colorectal Cancer | Completed |
| 5 | PUR 0110 | NCT01149707 | Left-Sided Ulcerative Colitis Proctosigmoiditis | Completed |
| S. No. | Drug | NCT Number | Condition | Status |
|---|---|---|---|---|
| 1 | Imodium | NCT00933465 | Fecal Incontinence | Withdrawn |
| 2 | Irinotecan | NCT03295084 | Metastatic Colorectal Cancer | Completed |
| 3 | Capecitabine | NCT01493336 | Colorectal Cancer | Completed |
| 4 | Diazepam | NCT04216797 | Levator Ani Syndrome | Recruiting |
| 5 | Regorafenib | NCT03946917 | Colorectal Cancer | - |
| 6 | Imipramine Hydrochloride | NCT03102645 | Fecal Incontinence | Completed |
| 7 | AmoxicillinClavulanate | NCT01012843 | Anal Fistula | Completed |
| 8 | Apatinib Mesylate | NCT03271255 | Colorectal Neoplasms Intestinal Neoplasms Gastrointestinal Neoplasms Digestive System Neoplasms | Recruting |
| 9 | Metronidazole | NCT04264676 | Colorectal Cancer Stage II Colorectal Cancer Stage III | Recruiting |
| 10 | Aspirin and Metformin | NCT05158374 | Colorectal Cancer Colorectal Neoplasms Colorectal Adenoma | Not yet recruiting |
| 11 | Apatinib Mesylate | NCT03743428 | Colorectal Neoplasm | Recruiting |
| 12 | Niclosamide | NCT02519582 | Colorectal Cancer | - |
| 13 | Thalidomide | NCT05266820 | Metastatic Colorectal Cancer | Recruiting |
| 14 | Apatinib | NCT01531777 | Colorectal Cancer | Completed |
| 15 | Regorafenib | NCT01939223 | Colorectal Neoplasms | Terminated |
| 16 | Rifaximin | NCT01345175 | Rectal cancer | Active |
| 17 | Regorafenib | NCT02466009 | Metastatic Colorectal Cancer | Completed |
| 18 | Selinexor, Pembrolizumab, Trifluridine, Tipiracil | NCT04854434 | Metastatic Colorectal Cancer | Active |
| 19 | Pembrolizumab, lenvatinib, regorafenib | NCT04776148 | Colorectal Neoplasms | Active |
| 20 | irinotecan, leucovorin, and 5fluorouracil | NCT00967616 | Colorectal Cancer | Completed |
| 21 | Regorafenib | NCT01103323 | Metastatic Colorectal Cancer | Completed |
| 22 | Clindamycin | NCT02585141 | Anal Fistulas | Completed |
| 23 | Dasatinib, bevacizumab, Oxaliplatin, Capecitabine | NCT00920868 | Metastatic Colorectal Cancer | Completed |
| 24 | Acetylsalicylic acid | NCT02647099 | Colorectal Cancer | Completed |
| 25 | Artesunate | NCT02633098 | Colorectal Cancer Bowel Cancer | Active |
| 26 | Regorafenib | NCT01853319 | Colorectal Neoplasms | Completed |
| 27 | Capecitabine, Perifosine | NCT01097018 | Colorectal Cancer | Completed |
| 28 | Dacomitinib, Docetaxel | NCT02039336 | Colorectal Cancer | - |
| 29 | Lapatinib, trametinib | NCT02230553 | Colorectal Cancer | - |
| 30 | Cabozantinib, Nivolumab | NCT04963283 | Colorectal Adenocarcinoma Colon Cancer Colon Adenocarcinoma Rectum Cancer Rectal Cancer Rectal Adenocarcinoma Colorectal Cancer | Recruiting |
| 31 | Tucatinib | NCT05382364 | Colorectal Cancer | Recruiting |
| S. No. | Drug | Indication | Brand Name | Dosage Form |
|---|---|---|---|---|
| For Local Action | ||||
| 1 | Bisacodyl | Constipation | Dulcolax Bisalax | Suppository Enema |
| 2 | Glycerol | Constipation | Glycerol | Suppository |
| 3 | Saline laxatives | ConstipationBowel | Micolette Microlax | Enema |
| 4 | Mesalazine | Inflammatory bowel disease | Pentasa Salofalk | Suppository Enema Rectal foam |
| 5 | Budesonide | Anti-inflammatory | Budenofalk | Rectal foam |
| 6 | Prednisolone | Anti-inflammatory | Colifoam | Rectal foam |
| 7 | Hydrocortisone | Anti-inflammatory | Predsol Colocort | Suppository Enema |
| 8 | Polystyrene sulfonate resins | Hyperkalemia | Resonium A | Enema |
| 9 | Glyceryl Trinitrate | Anal fissure, haemorrhoids | Rectogesic | Ointment |
| For Systemic Action | ||||
| 10 | Acetaminophen | Pain, fever | Panadol Acephen Fever All | Suppository |
| 11 | Oxycodone | Pain | Proladone | Suppository |
| 12 | Ondansetron | Nausea and vomiting | Zofran | Suppository |
| 13 | Caffeine + ergotamine | Migraine | Migergot | Suppository |
| 14 | Prochlorperazine | Nausea and vomiting | Compro | Suppository |
| 15 | Promethazine | Antihistamine | Phenergan | Suppository |
| 16 | Ibuprofen | Pain, fever | Nurofen | Suppository |
| 17 | Diclofenac | Pain, fever | Voltaren | Suppository |
| 18 | Indomethacin | Pain | Indocin | Suppository |
| 19 | Diazepam | Seizures, sedation | Diazepam rectal solutionDiastatAcuDial | EnemaGel |
| S. No. | Patent | Title | Claim | Ref. |
|---|---|---|---|---|
| 1 | CA2037101C | Omeprazole compositions designed for administration in rectum | A stabilized rectal suppository containing omeprazole as an active ingredient and amino acid as a stabilizer. | [110] |
| 2 | US20120237489A1 | Suppository for rectal, vaginal, or urethral administration containing a probiotic, an antibiotic, and an unsaturated non-esterified fatty acid | A suppository for rectal, vaginal, or urethral administration comprising at least one probiotic, one antibiotic, and one unsaturated, non-esterified fatty acid. | [111] |
| 3 | US8217083B2 | Mesalamine suppository | A mesalamine rectal suppository comprising mesalamine and an oily or fatty base treating active ulcerative proctitis in a patient. | [112] |
| 4 | US6677319B1 | Phosphatidylcholine as medication with protective effect large intestinal mucosa | A method of treating diseases of the colon mucosa, comprising administering a therapeutically effective amount of substrate phosphatidylcholine in a pH-dependent delayed time-release preparation. | [113] |
| 5 | WO2011072861A1 | Suppository comprising pantoprazole | A suppository comprising at least one pellet and suppository base, wherein the pellet comprises a core and an inert layer surrounding the core, wherein the core comprised pantoprazole. | [114] |
| 6 | WO2010143004A2 | Glycerol-free osmotic laxative suppository | Osmotic component, stabilizer, and wetting agent containing laxative suppository, wherein the osmotic component and the stabilizer is PEG 200 and/or a polyethylene glycol with higher molecular weight. | [115] |
| 7 | EP1492538A1 | Meloxicam suppositories containing, e.g., polyethylene glycol | A suppository containing a composition, of meloxicam or a pharmaceutically acceptable excipient, characterized in that at least one of the excipients is a polyalkylene glycol, for the treatment or prevention of polyarthritis, rheumatoid arthritis or inflammation diseases. | [116] |
| 8 | US20160002278A1 | Pharmaceutical composition for rectal Administration | A pharmaceutical composition for rectal administration in the form of a foam comprising fidaxomicin. | [117] |
| 9 | CN1424047A | A Safety quick effective rectal suppository in glycerin, sodium chloride, and water | Glycerol, sodium chlorideandwater were used to prepare the present invention and made a kind of liquid laxative with safety, quick onset of action. | [118] |
| 10 | WO2008141368A1 | Combination laxative compositions comprising a colonic stimulant and a bulking laxative | A method of treating constipation in a subject in need thereof comprising the step of providing to said subject a combination of a colonic stimulant and a bulking laxative. | [119] |
| 11 | WO2017046343A1 | Compositions for rectal administration in the treatment of ulcerative colitis and methods using same | A dry composition for the rectal treatment of IBD comprising an active compound or a pharmaceutically acceptable salt or stereoisomer, an anti-caking agent, and a lubricant, wherein the pH of the dry composition is between about pH 3.0 and about pH 5.0. | [120] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rathi, R.; Sanshita; Kumar, A.; Vishvakarma, V.; Huanbutta, K.; Singh, I.; Sangnim, T. Advancements in Rectal Drug Delivery Systems: Clinical Trials, and Patents Perspective. Pharmaceutics 2022, 14, 2210. https://doi.org/10.3390/pharmaceutics14102210
Rathi R, Sanshita, Kumar A, Vishvakarma V, Huanbutta K, Singh I, Sangnim T. Advancements in Rectal Drug Delivery Systems: Clinical Trials, and Patents Perspective. Pharmaceutics. 2022; 14(10):2210. https://doi.org/10.3390/pharmaceutics14102210
Chicago/Turabian StyleRathi, Ritu, Sanshita, Alpesh Kumar, Vivekanand Vishvakarma, Kampanart Huanbutta, Inderbir Singh, and Tanikan Sangnim. 2022. "Advancements in Rectal Drug Delivery Systems: Clinical Trials, and Patents Perspective" Pharmaceutics 14, no. 10: 2210. https://doi.org/10.3390/pharmaceutics14102210