
Cysteamine Eye Drops in Hyaluronic Acid Packaged in Innovative Single-Dose Systems: Stability and Ocular Biopermanence

 , ,
, ,  , , , ,
, , , ,  and
and
Abstract
:
1. Introduction
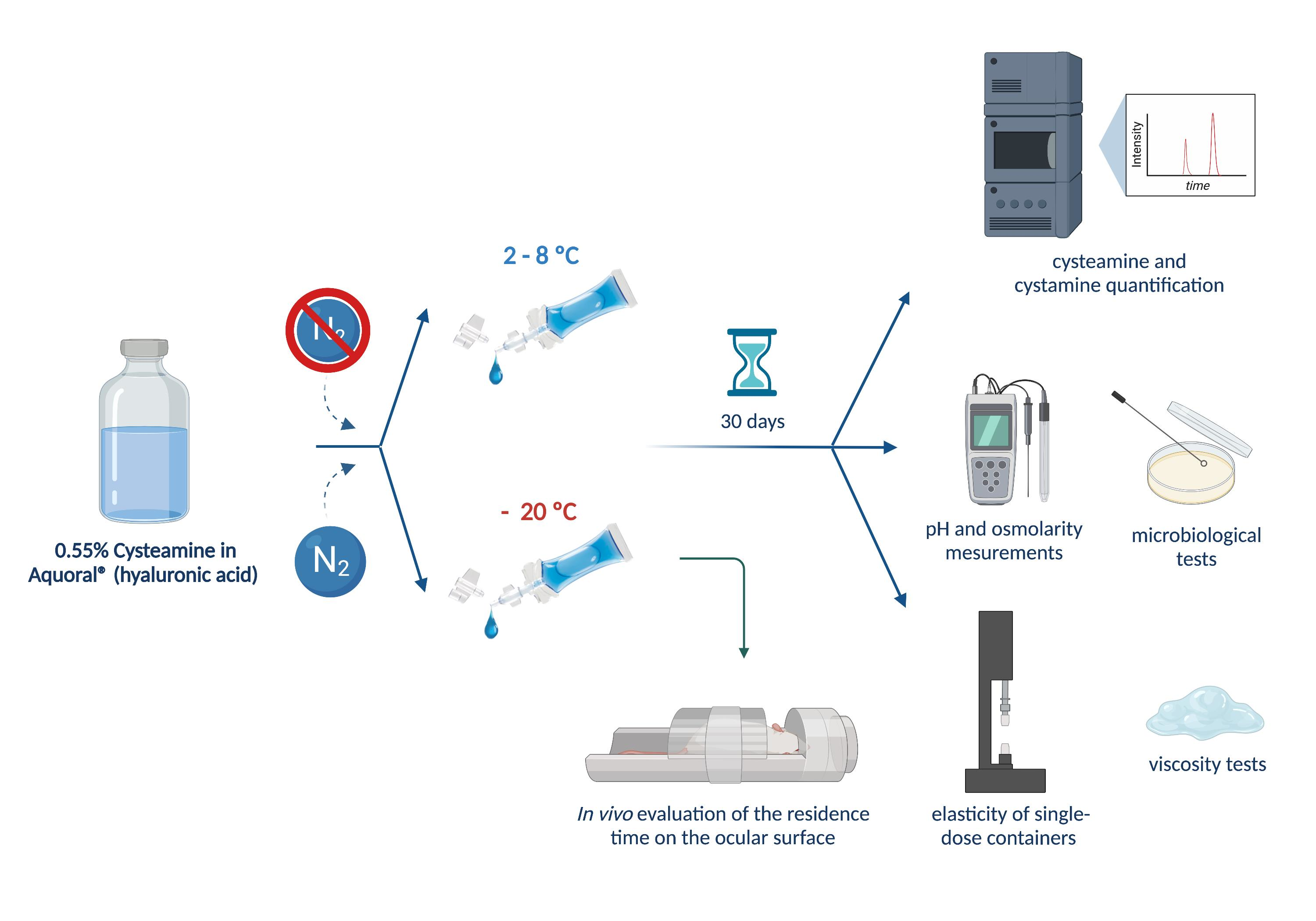
2. Materials and Methods
2.1. Materials
2.2. Elaboration and Packaging of Cysteamine Hydrochloride Sterile Solutions
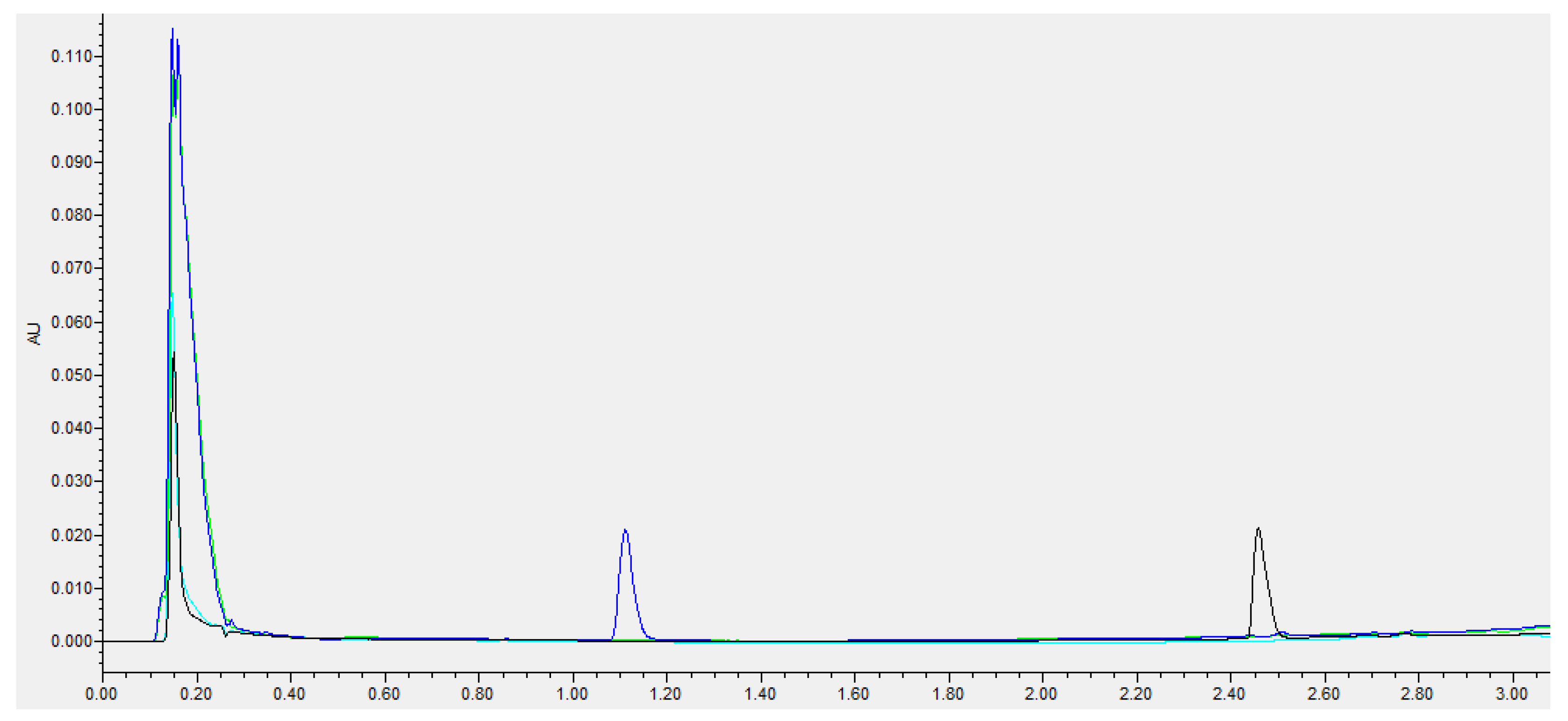
2.3. Cysteamine and Cystamine Quantification
2.4. Storage Stability Study
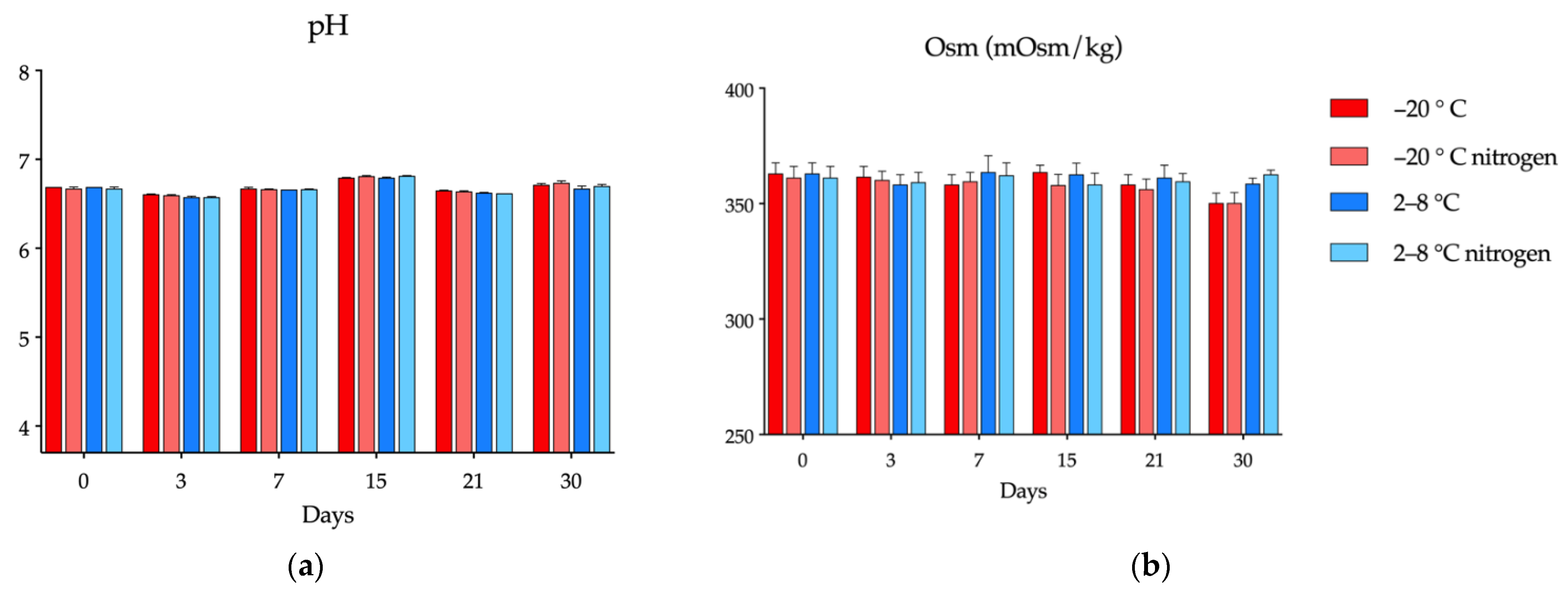
2.4.1. Determination of pH and Osmolarity
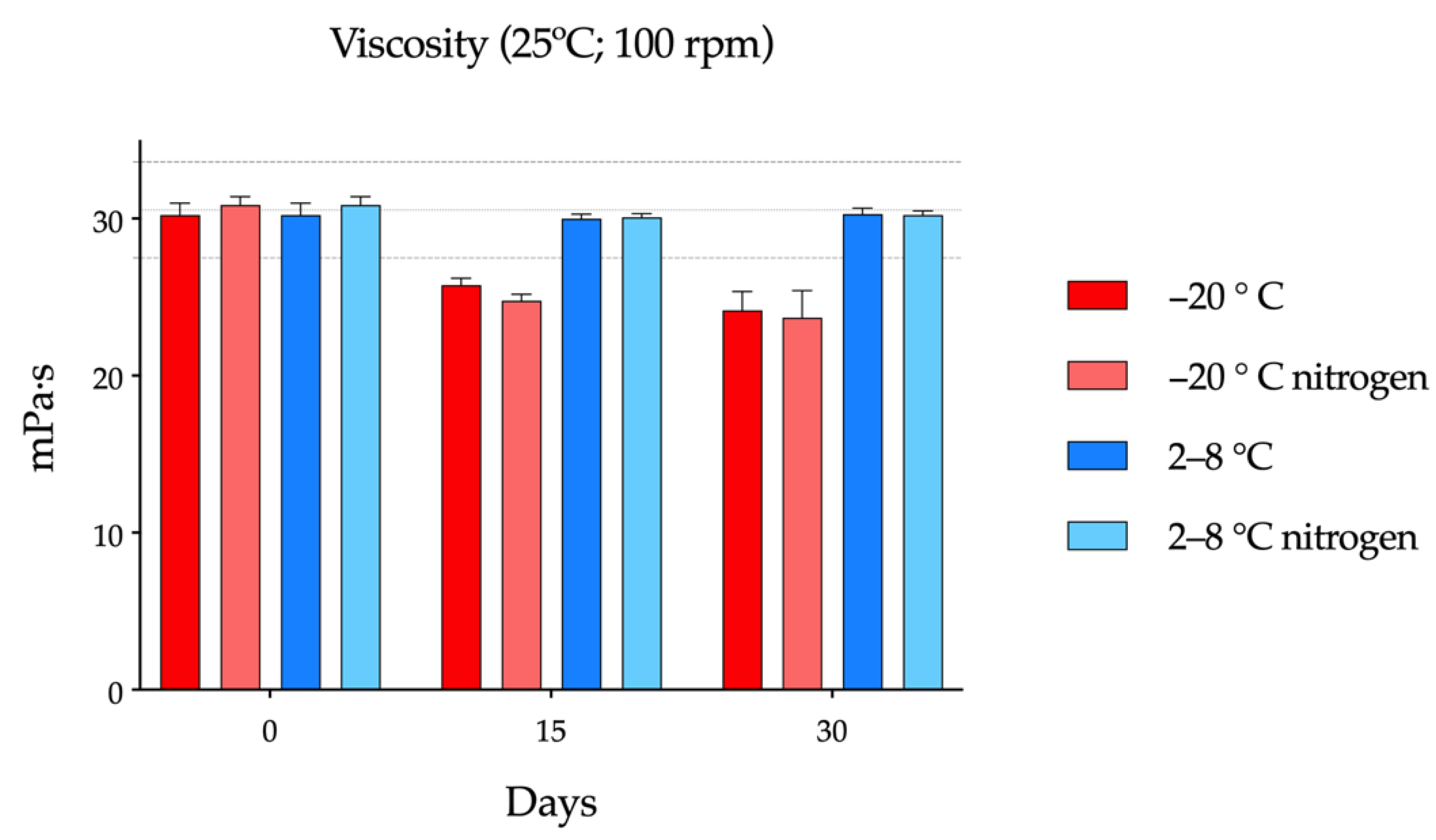
2.4.2. Viscosity Tests
2.4.3. Microbiological Stability
2.4.4. Statistical Analysis
2.4.5. Elasticity of Single-Dose Containers
2.5. In-Use Stability Study
2.6. In Vivo Evaluation of the Residence Time on the Ocular Surface
3. Results
3.1. Cysteamine and Cystamine Quantification
3.2. Storage Stability Study
3.2.1. pH and Osmolality
3.2.2. Viscosity tests
3.2.3. Microbiological Stability
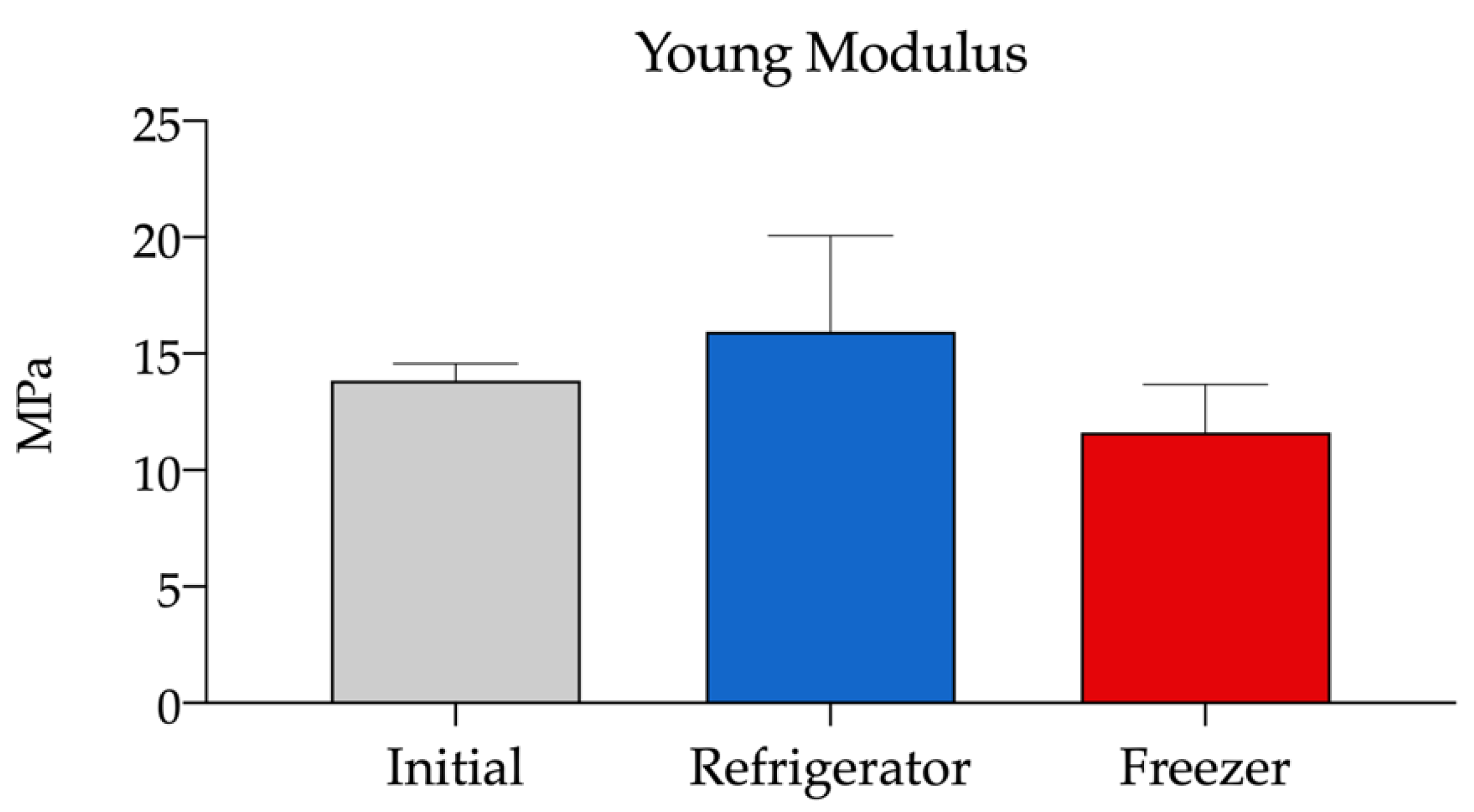
3.2.4. Elasticity of Single-Dose Containers
3.3. In-Use Stability Study
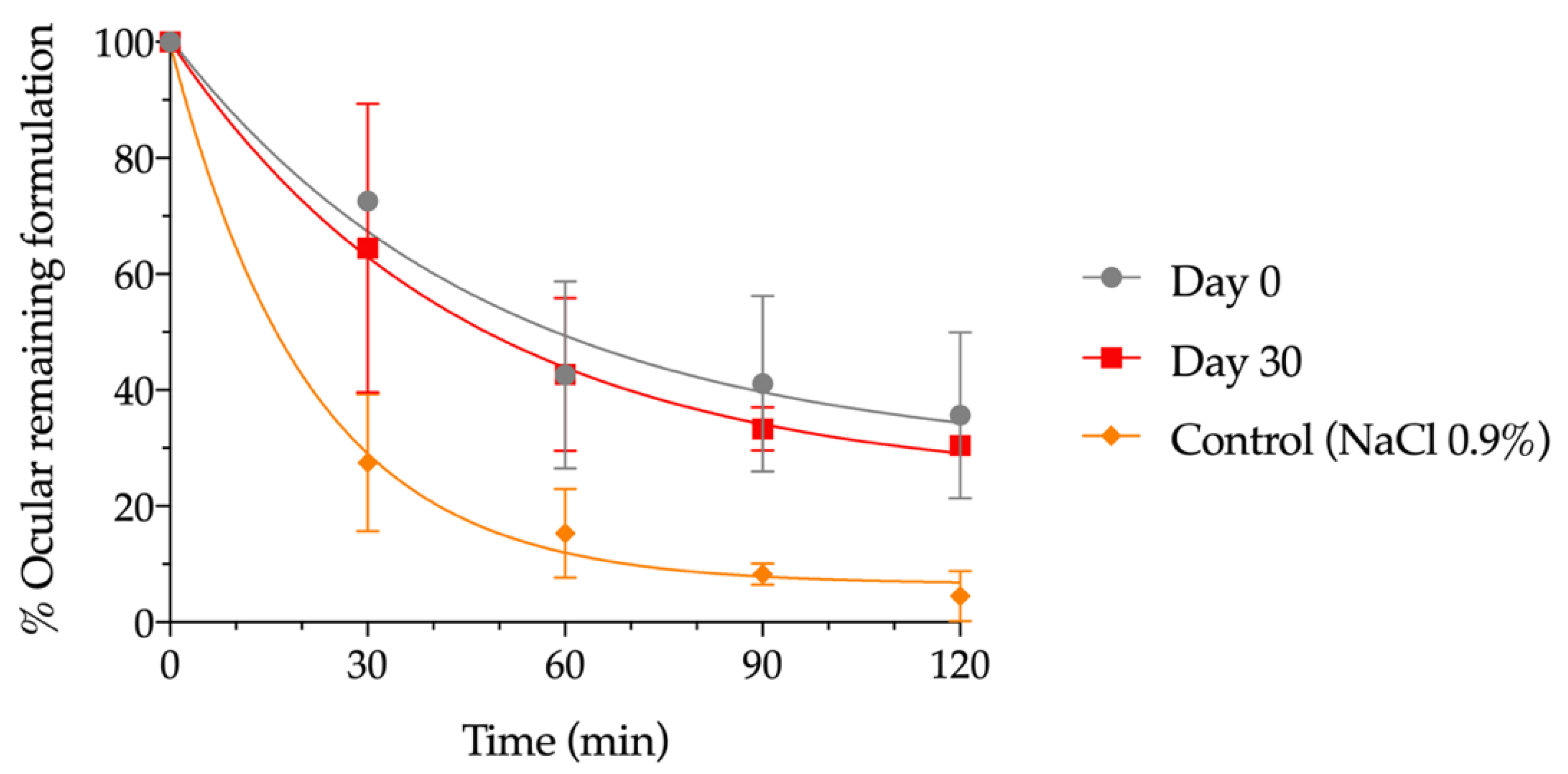
3.4. In Vivo Evaluation of the Residence Time on the Ocular Surface
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orphanet: Cystinosis. Available online: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=213 (accessed on 2 July 2022).
- Liang, H.; Labbé, A.; Baudouin, C.; Plisson, C.; Giordano, V. Long-Term Follow-up of Cystinosis Patients Treated with 0.55% Cysteamine Hydrochloride. Br. J. Ophthalmol. 2020, 105, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Cherqui, S.; Kalatzis, V.; Trugnan, G.; Antignac, C. The Targeting of Cystinosin to the Lysosomal Membrane Requires a Tyrosine-Based Signal and a Novel Sorting Motif*. J. Biol. Chem. 2001, 276, 13314–13321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syres, K.; Harrison, F.; Tadlock, M.; Jester, J.V.; Simpson, J.; Roy, S.; Salomon, D.R.; Cherqui, S. Successful Treatment of the Murine Model of Cystinosis Using Bone Marrow Cell Transplantation. Blood 2009, 114, 2542–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nesterova, G.; Gahl, W.A. Cystinosis: The Evolution of a Treatable Disease. Pediatric Nephrol. 2013, 28, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luaces-Rodríguez, A.; Díaz-Tomé, V.; González-Barcia, M.; Silva-Rodríguez, J.; Herranz, M.; Gil-Martínez, M.; Rodríguez-Ares, M.T.; García-Mazás, C.; Blanco-Mendez, J.; Lamas, M.J.; et al. Cysteamine Polysaccharide Hydrogels: Study of Extended Ocular Delivery and Biopermanence Time by PET Imaging. Int. J. Pharm. 2017, 528, 714–722. [Google Scholar] [CrossRef]
- McKenzie, B.; Kay, G.; Matthews, K.H.; Knott, R.; Cairns, D. Preformulation of Cysteamine Gels for Treatment of the Ophthalmic Complications in Cystinosis. Int. J. Pharm. 2016, 515, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Sarma, P.; Kaur, H.; Prajapat, M.; Shekhar, N.; Bhattacharyya, J.; Kaur, H.; Kumar, S.; Medhi, B.; Ram, J.; et al. Efficacy and Safety of Topical Cysteamine in Corneal Cystinosis: A Systematic Review and Meta- Analysis. Am. J. Ophthalmol. 2020, 223, 275–285. [Google Scholar] [CrossRef]
- Andrzejewska, Z.; Nevo, N.; Thomas, L.; Chhuon, C.; Bailleux, A.; Chauvet, V.; Courtoy, P.J.; Chol, M.; Guerrera, I.C.; Antignac, C. Cystinosin Is a Component of the Vacuolar H+-ATPase-Ragulator-Rag Complex Controlling Mammalian Target of Rapamycin Complex 1 Signaling. J. Am. Soc. Nephrol. 2016, 27, 1678–1688. [Google Scholar] [CrossRef] [Green Version]
- Thoene, J.G.; DelMonte, M.A.; Mullet, J. Microvesicle Delivery of a Lysosomal Transport Protein to Ex Vivo Rabbit Cornea. Mol. Genet. Metab. Rep. 2020, 23, 100587. [Google Scholar] [CrossRef]
- Hollywood, J.A.; Przepiorski, A.; D’Souza, R.F.; Sreebhavan, S.; Wolvetang, E.J.; Harrison, P.T.; Davidson, A.J.; Holm, T.M. Use of Human Induced Pluripotent Stem Cells and Kidney Organoids to Develop a Cysteamine/Mtor Inhibition Combination Therapy for Cystinosis. J. Am. Soc. Nephrol. 2020, 31, 962–982. [Google Scholar] [CrossRef]
- Liu, Z.; Kompella, U.B.; Chauhan, A. Gold Nanoparticle Synthesis in Contact Lenses for Drug-Less Ocular Cystinosis Treatment. Eur. J. Pharm. Biopharm. 2021, 165, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, R.L.; Thoene, J.G.; Christensen, H.N. Detection and Characterization of Carrier-Mediated Cationic Amino Acid Transport in Lysosomes of Normal and Cystinotic Human Fibroblasts. Role in Therapeutic Cystine Removal? J. Biol. Chem. 1985, 260, 4791–4798. [Google Scholar] [CrossRef]
- Gahl, W.A.; Kuehl, E.M.; Iwata, F.; Lindblad, A.; Kaiser-Kupfer, M.I. Corneal Crystals in Nephropathic Cystinosis: Natural History and Treatment with Cysteamine Eyedrops. Mol. Genet. Metab. 2000, 71, 100–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Cystagon® Prescribing Information. 1997. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/cystagon (accessed on 5 August 2022).
- Schneider, J.A. Approval of Cysteamine for Patients with Cystinosis. Pediatric Nephrol. 1995, 9, 254. [Google Scholar] [CrossRef]
- Food and Drug Administration. Cystaran® Prescribing Information. 2012. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/200740s000lbl.pdf (accessed on 20 August 2022).
- Food and Drug Administration. Cystadrops® Prescribing Information. 2012. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/211302s000lbl.pdf (accessed on 20 August 2022).
- European Medicines Agency. Cystadrops® Prescribing Information. 2016. Available online: https://www.ema.europa.eu/en/documents/product-information/cystadrops-epar-product-information_es.pdf (accessed on 20 August 2022).
- Fernández-Ferreiro, A.; Luaces-Rodríguez, A.; Díaz-Tomé, V.; Gil-Martínez, M.; Ares, M.T.R.; Peralba, R.T.; Blanco-Méndez, J.; González-Barcia, M.; Otero-Espinar, F.J.; Lamas, M.J. Cysteamine ophthalmic hydrogel for the treatment of ocular cystinosis. Farm. Hosp. 2017, 41, 678–687. [Google Scholar] [CrossRef]
- Reda, A.; van Schepdael, A.; Adams, E.; Paul, P.; Devolder, D.; Elmonem, M.A.; Veys, K.; Casteels, I.; van den Heuvel, L.; Levtchenko, E. Effect of Storage Conditions on Stability of Ophthalmological Compounded Cysteamine Eye Drops. In JIMD Reports; Springer: Berlin/Heidelberg, Germany, 2017; Volume 42, pp. 47–51. [Google Scholar] [CrossRef]
- Labbé, A.; Baudouin, C.; Deschênes, G.; Loirat, C.; Charbit, M.; Guest, G.; Niaudet, P. A New Gel Formulation of Topical Cysteamine for the Treatment of Corneal Cystine Crystals in Cystinosis: The Cystadrops OCT-1 Study. Mol. Genet. Metab. 2014, 111, 314–320. [Google Scholar] [CrossRef]
- Jimenez, J.; Washington, M.A.; Resnick, J.L.; Nischal, K.K.; Fedorchak, M.V. A Sustained Release Cysteamine Microsphere/Thermoresponsive Gel Eyedrop for Corneal Cystinosis Improves Drug Stability. Drug Deliv. Transl. Res. 2021, 11, 2224–2238. [Google Scholar] [CrossRef]
- Atallah, C.; Charcosset, C.; Greige-Gerges, H. Challenges for Cysteamine Stabilization, Quantification, and Biological Effects Improvement. J. Pharm. Anal. 2020, 10, 499–516. [Google Scholar] [CrossRef]
- Castro-Balado, A.; Mondelo-García, C.; Varela-Rey, I.; Moreda-Vizcaíno, B.; Sierra-Sánchez, J.F.; Rodríguez-Ares, M.T.; Hermelo-Vidal, G.; Zarra-Ferro, I.; González-Barcia, M.; Yebra-Pimentel, E.; et al. Recent Research in Ocular Cystinosis: Drug Delivery Systems, Cysteamine Detection Methods and Future Perspectives. Pharmaceutics 2020, 12, 1177. [Google Scholar] [CrossRef]
- Purkiss, R. Stability of Cysteamine Hydrochloride in Solution. J. Clin. Pharm. Ther. 1977, 2, 199–203. [Google Scholar] [CrossRef]
- Brodrick, A.; Broughton, H.M.; Oakley, R.M. The Stability of an Oral Liquid Formulation of Cysteamine. J. Clin. Hosp. Pharm. 1981, 6, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Dixon, P.; Powell, K.; Chauhan, A. Novel Approaches for Improving Stability of Cysteamine Formulations. Int. J. Pharm. 2018, 549, 466–475. [Google Scholar] [CrossRef]
- Carracedo, G.; Pastrana, C.; Serramito, M.; Rodriguez-Pomar, C. Evaluation of Tear Meniscus by Optical Coherence Tomography after Different Sodium Hyaluronate Eyedrops Instillation. Acta Ophthalmol. 2019, 97, e162–e169. [Google Scholar] [CrossRef] [PubMed]
- Acofarma Fórmulas Magistrales. Distribuidor de Productos para Farmacias Analysis Bulletin—Sodium Hyaluronate. Available online: https://productoquimico.acofarma.com (accessed on 5 August 2022).
- Agencia Española de Medicamentos y Productos Sanitarios. Registro Unificado de Empresas de Sustancias Activas. Available online: https://labofar.aemps.es/labofar/registro/ruesa/consulta.do#nav-no (accessed on 5 August 2022).
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef]
- Olejnik, A.; Goscianska, J.; Zielinska, A.; Nowak, I. Stability determination of the formulations containing hyaluronic acid. Int. J. Cosmet. Sci. 2015, 37, 401–407. [Google Scholar] [CrossRef]
- Falcone, S.J.; Palmeri, D.M.; Berg, R.A. Rheological and cohesive properties of hyaluronic acid. J. Biomed. Mater. Res. Part A 2006, 76A, 721–728. [Google Scholar] [CrossRef]
- Bothner, H.; Wik, O. Rheology of Hyaluronate. Acta Oto-Laryngol. 1987, 104, 25–30. [Google Scholar] [CrossRef]
- Biomed Device-Care in a Revolutionary Way. COL® Video-Kit for the Preparation of Aliquots of Eye Drops with Hemocomponents. Available online: https://www.youtube.com/watch?v=FCorvJXkUZw (accessed on 5 August 2022).
- Biomed Device-Care in a Revolutionary Way. COL® Eye Drops System. Available online: http://col-eyedrops.com/index.php/it/eye-drops-system/col (accessed on 5 August 2022).
- Kim, Y.; Na, D.H. Simultaneous Determination of Cysteamine and Cystamine in Cosmetics by Ion-Pairing Reversed-Phase High-Performance Liquid Chromatography. Toxicol. Res. 2019, 35, 161–165. [Google Scholar] [CrossRef]
- Lund, W. The Pharmaceutical Codex: Principles and Practice of Pharmaceutics; The Pharmaceutical Press: London, UK, 1994; ISBN 0-85369-290-4. [Google Scholar]
- Fernández-Ferreiro, A.; Castro-Balado, A.; García Quintanilla, L.; Lamas, M.; Otero-Espinar, F.; Mendez, J.; Gómez-Ulla, F.; Gil-Martínez, M.; Tomé, V.; Luaces-Rodríguez, A.; et al. Formulación Magistral Oftálmica Antiinfecciosa; SEFH Sociedad Española de Farmacia Hospitalaria: Madrid, Spain, 2019; ISBN 978-84-09-10764-3. [Google Scholar]
- Dutescu, R.M.; Panfil, C.; Schrage, N. Osmolarity of Prevalent Eye Drops, Side Effects, and Therapeutic Approaches. Cornea 2015, 34, 560–566. [Google Scholar] [CrossRef]
- Fernández-Ferreiro, A.; Silva-Rodríguez, J.; Otero-Espinar, F.J.; González-Barcia, M.; Lamas, M.J.; Ruibal, A.; Luaces-Rodriguez, A.; Vieites-Prado, A.; Sobrino, T.; Herranz, M.; et al. Positron Emission Tomography for the Development and Characterization of Corneal Permanence of Ophthalmic Pharmaceutical Formulations. Investig. Ophthalmol. Vis. Sci. 2017, 58, 772–780. [Google Scholar] [CrossRef]
- Loening, A.M.; Gambhir, S.S. AMIDE: A Free Software Tool for Multimodality Medical Image Analysis. Mol. Imaging 2003, 2, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Committee for Medicinal Products for Human Use (CHMP). European Medicines Agency Guideline on Bioanalytical Method Validation. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-bioanalytical-method-validation_en.pdf (accessed on 22 September 2022).
- Esteve Aquoral®. Available online: https://aquoral.es/aquoral-lagrimas-artificiales-alivio-rapido-y-duradero/aquoral/ (accessed on 5 August 2022).
- Abbas, N.; Hasan, S.S.; Curley, L.; Babar, Z.-U.-D. Access to Medicines—A Systematic Review of the Literature. Res. Soc. Adm. Pharm. 2020, 16, 1166–1176. [Google Scholar] [CrossRef] [PubMed]
- Pescina, S.; Carra, F.; Padula, C.; Santi, P.; Nicoli, S. Effect of PH and Penetration Enhancers on Cysteamine Stability and Trans-Corneal Transport. Eur. J. Pharm. Biopharm. 2016, 107, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Martín-Sabroso, C.; Alonso-González, M.; Fernández-Carballido, A.; Aparicio-Blanco, J.; Córdoba-Díaz, D.; Navarro-García, F.; Córdoba-Díaz, M.; Torres-Suárez, A.I. Limitations and Challenges in the Stability of Cysteamine Eye Drop Compounded Formulations. Pharmaceuticals 2022, 15, 2. [Google Scholar] [CrossRef]
- Makuloluwa, A.K.; Shams, F. Cysteamine Hydrochloride Eye Drop Solution for the Treatment of Corneal Cystine Crystal Deposits in Patients with Cystinosis: An Evidence-Based Review. Clin. Ophthalmol. 2018, 12, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Bozdag, S.; Gumus, K.; Gumus, O.; Unlu, N. Formulation and in Vitro Evaluation of Cysteamine Hydrochloride Viscous Solutions for the Treatment of Corneal Cystinosis. Eur. J. Pharm. Biopharm. 2008, 70, 260–269. [Google Scholar] [CrossRef]
- U.S. Cysteamine Eye Drop Development. Available online: http://www.cystinosis.com/Documents/EyeDropPaper.html (accessed on 5 August 2022).
- Bastarrachea, L.; Dhawan, S.; Sablani, S.S. Engineering Properties of Polymeric-Based Antimicrobial Films for Food Packaging: A Review. Food Eng. Rev. 2011, 3, 79–93. [Google Scholar] [CrossRef]
- European Medicines Agency. European Public Assessment Report (EPAR) for Cystadrops. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/cystadrops (accessed on 5 August 2022).
- Food and Drug Administration. FDA Drug Approval Package: CYSTADROPS. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/211302Orig1s000TOC.cfm (accessed on 5 August 2022).
- Liang, H.; Labbé, A.; Le Mouhaër, J.; Plisson, C.; Baudouin, C. A New Viscous Cysteamine Eye Drops Treatment for Ophthalmic Cystinosis: An Open-Label Randomized Comparative Phase III Pivotal Study. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2275. [Google Scholar] [CrossRef]
- Yang, Y.-J.; Lee, W.-Y.; Kim, Y.-J.; Hong, Y.-P. A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2383. [Google Scholar] [CrossRef]
- Aragona, P.; Simmons, P.A.; Wang, H.; Wang, T. Physicochemical Properties of Hyaluronic Acid-Based Lubricant Eye Drops. Transl. Vis. Sci. Technol. 2019, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Posarelli, C.; Passani, A.; Del Re, M.; Fogli, S.; Toro, M.D.; Ferreras, A.; Figus, M. Cross-Linked Hyaluronic Acid as Tear Film Substitute. J. Ocul. Pharmacol. Ther. 2019, 35, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troiano, P.; Monaco, G. Effect of Hypotonic 0.4% Hyaluronic Acid Drops in Dry Eye Patients: A Cross-over Study. Cornea 2008, 27, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Ang, B.C.H.; Sng, J.J.; Wang, P.X.H.; Htoon, H.M.; Tong, L.H.T. Sodium Hyaluronate in the Treatment of Dry Eye Syndrome: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 9013. [Google Scholar] [CrossRef] [PubMed]
- Sandri, G.; Rossi, S.; Ferrari, F.; Bonferoni, M.C.; Zerrouk, N.; Caramella, C. Mucoadhesive and Penetration Enhancement Properties of Three Grades of Hyaluronic Acid Using Porcine Buccal and Vaginal Tissue, Caco-2 Cell Lines, and Rat Jejunum. J. Pharm. Pharmacol. 2004, 56, 1083–1090. [Google Scholar] [CrossRef]
- Datta, S.; Baudouin, C.; Brignole-Baudouin, F.; Denoyer, A.; Cortopassi, G.A. The Eye Drop Preservative Benzalkonium Chloride Potently Induces Mitochondrial Dysfunction and Preferentially Affects LHON Mutant Cells. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2406–2412. [Google Scholar] [CrossRef] [PubMed]
- Özalp, O.; Atalay, E.; Alataş, İ.Ö.; Küskü Kiraz, Z.; Yıldırım, N. Assessment of Phosphate and Osmolarity Levels in Chronically Administered Eye Drops. Turk. J. Ophthalmol. 2019, 49, 123–129. [Google Scholar] [CrossRef]
- Casey-Power, S.; Ryan, R.; Behl, G.; McLoughlin, P.; Byrne, M.E.; Fitzhenry, L. Hyaluronic Acid: Its Versatile Use in Ocular Drug Delivery with a Specific Focus on Hyaluronic Acid-Based Polyelectrolyte Complexes. Pharmaceutics 2022, 14, 1479. [Google Scholar] [CrossRef]
- Johnson, R.S.; Niedermeier, W.; Bobo, P. The Pseudoplastic Behavior of Aqueous Solutions of Hyaluronic Acid. Biorheology 1971, 7, 177–187. [Google Scholar] [CrossRef]
- Ahumada, L.A.C.; González, M.X.R.; Sandoval, O.L.H.; Olmedo, J.J.S. Evaluation of Hyaluronic Acid Dilutions at Different Concentrations Using a Quartz Crystal Resonator (QCR) for the Potential Diagnosis of Arthritic Diseases. Sensors 2016, 16, 1959. [Google Scholar] [CrossRef]
- García-Abuín, A.; Gómez-Díaz, D.; Navaza, J.M.; Regueiro, L.; Vidal-Tato, I. Viscosimetric Behaviour of Hyaluronic Acid in Different Aqueous Solutions. Carbohydr. Polym. 2011, 85, 500–505. [Google Scholar] [CrossRef]
- Klang, M.G. Sterile Preparation Formulation. In Compounding Sterile Preparations, 4th ed.; American Society of Health-System Pharmacists (ASHP): Bethesda, MD, USA, 2018; pp. 51–66. ISBN 978-1-58528-484-9. [Google Scholar]
- ScienceDirect Topics. Cryoprotective Agent—An Overview. Available online: https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/cryoprotective-agent (accessed on 24 August 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Mobile Phase A (%) | Mobile Phase B (%) |
|---|---|---|
| 0 | 95.0 | 5.0 |
| 0.50 | 95.0 | 5.0 |
| 2.50 | 70.0 | 30.0 |
| 3.20 | 95.0 | 5.0 |
| 6.0 | 95.0 | 5.0 |
| Storage Conditions | K (%/Day) | SDk (%/Day) | r2 |
|---|---|---|---|
| 2–8 °C | 1.414 | 0.05502 | 0.9270 |
| 2–8 °C nitrogen | 1.496 | 0.02904 | 0.9808 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Balado, A.; Bandín-Vilar, E.; Cuartero-Martínez, A.; García-Quintanilla, L.; Hermelo-Vidal, G.; García-Otero, X.; Rodríguez-Martínez, L.; Mateos, J.; Hernández-Blanco, M.; Aguiar, P.; et al. Cysteamine Eye Drops in Hyaluronic Acid Packaged in Innovative Single-Dose Systems: Stability and Ocular Biopermanence. Pharmaceutics 2022, 14, 2194. https://doi.org/10.3390/pharmaceutics14102194
Castro-Balado A, Bandín-Vilar E, Cuartero-Martínez A, García-Quintanilla L, Hermelo-Vidal G, García-Otero X, Rodríguez-Martínez L, Mateos J, Hernández-Blanco M, Aguiar P, et al. Cysteamine Eye Drops in Hyaluronic Acid Packaged in Innovative Single-Dose Systems: Stability and Ocular Biopermanence. Pharmaceutics. 2022; 14(10):2194. https://doi.org/10.3390/pharmaceutics14102194
Chicago/Turabian StyleCastro-Balado, Ana, Enrique Bandín-Vilar, Andrea Cuartero-Martínez, Laura García-Quintanilla, Gonzalo Hermelo-Vidal, Xurxo García-Otero, Lorena Rodríguez-Martínez, Jesús Mateos, Manuela Hernández-Blanco, Pablo Aguiar, and et al. 2022. "Cysteamine Eye Drops in Hyaluronic Acid Packaged in Innovative Single-Dose Systems: Stability and Ocular Biopermanence" Pharmaceutics 14, no. 10: 2194. https://doi.org/10.3390/pharmaceutics14102194