
Effect of Laparoscopic Sleeve Gastrectomy on the Pharmacokinetics of Oral Omeprazole Using a Population Approach
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Analytical Assay
2.3. Structural PK Model
2.4. Selection of Covariates
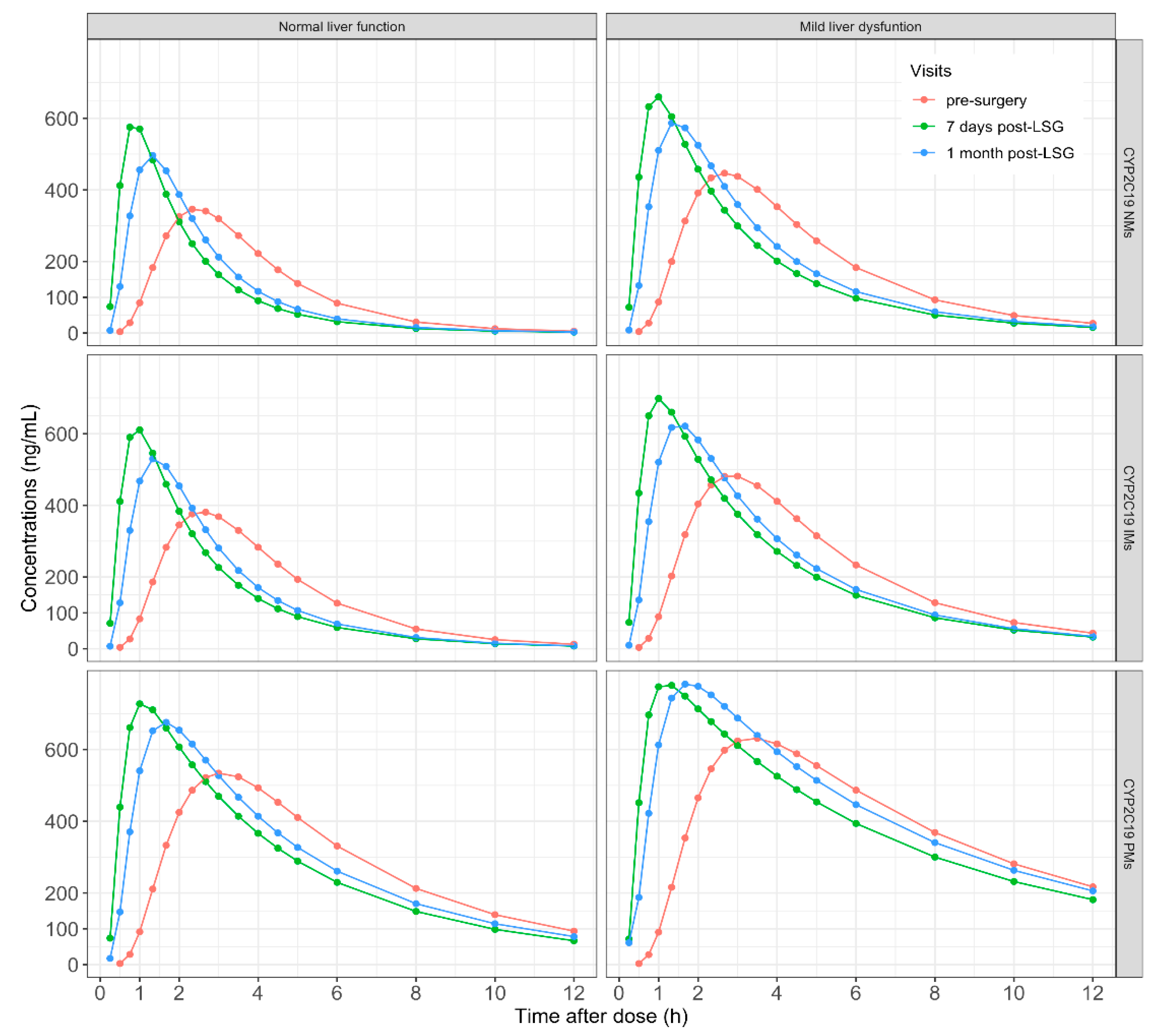
2.5. Monte Carlo Simulations
3. Results
3.1. Subjects and Data
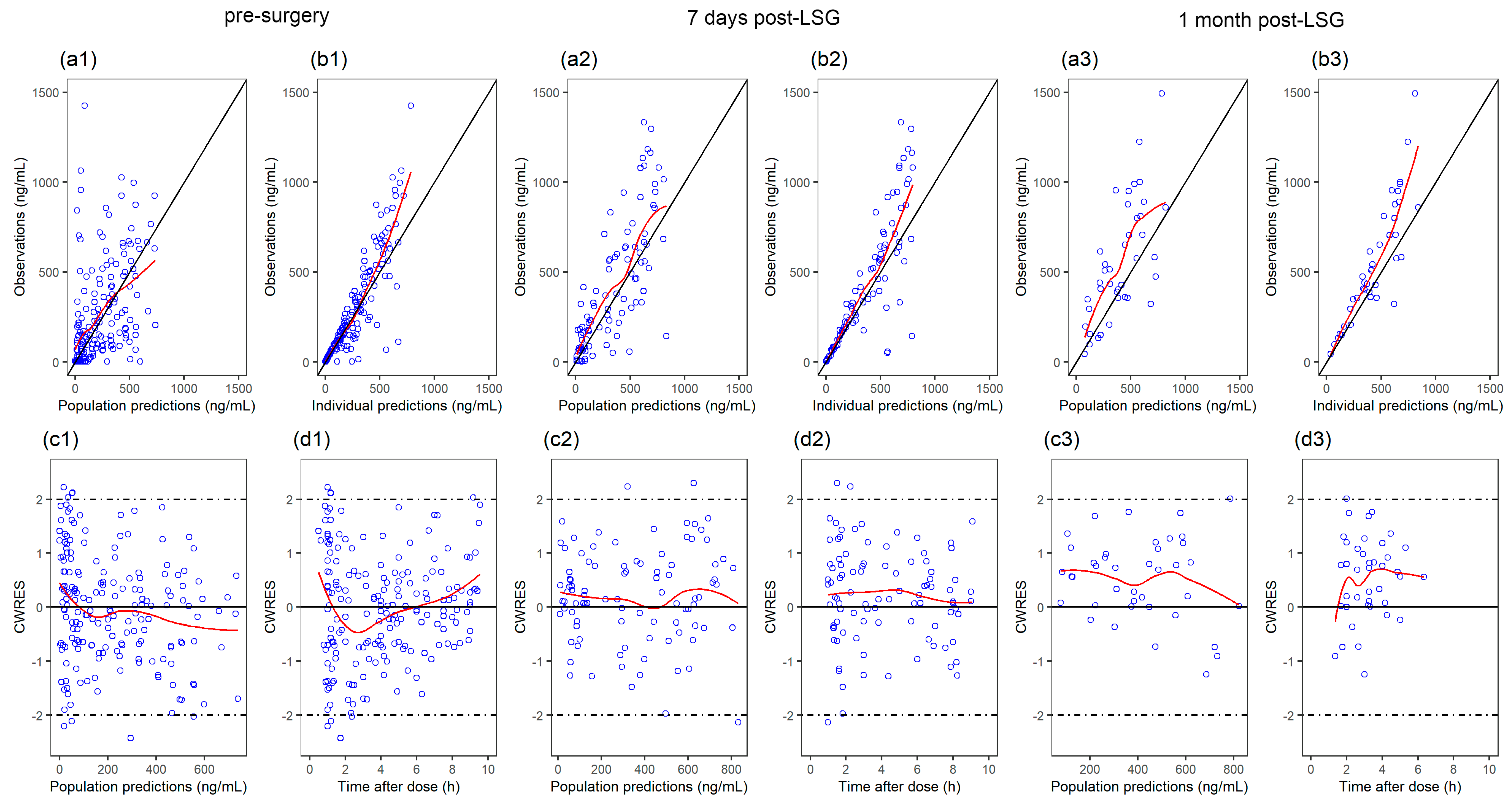
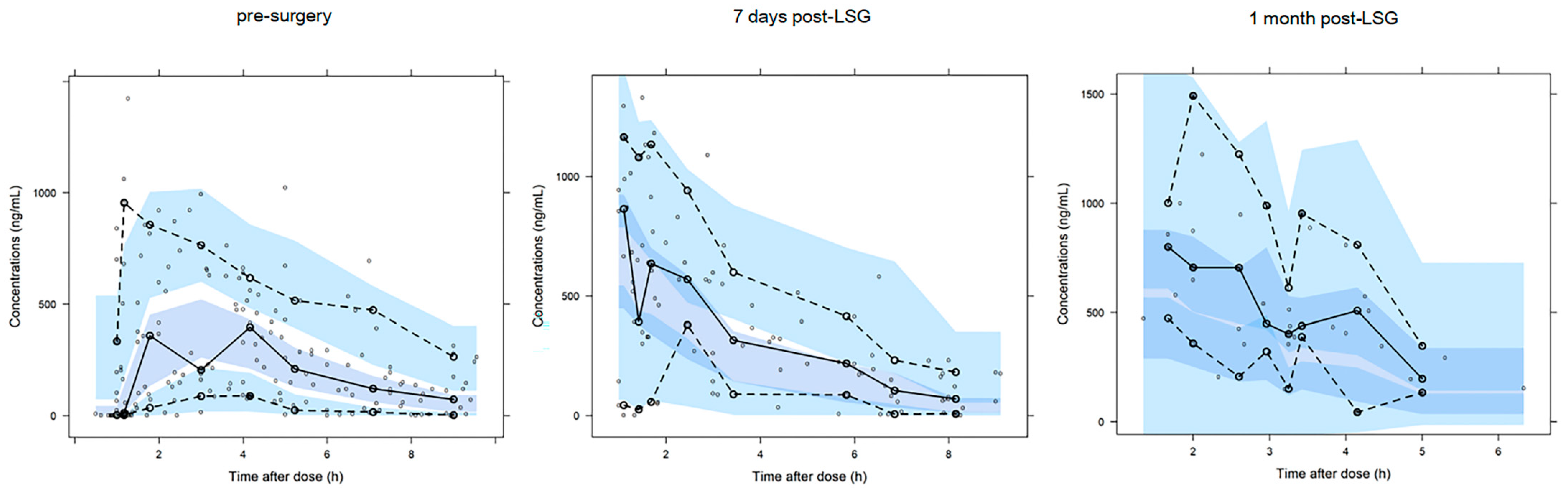
3.2. Population PK Modeling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Obesity and Overweight. Available online: https://www.who.int/health-topics/obesity (accessed on 28 June 2022).
- Singh, A.K.; Singh, R. Pharmacotherapy in obesity: A systematic review and meta-analysis of randomized controlled trials of anti-obesity drugs. Expert Rev. Clin. Pharmacol. 2020, 13, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Haslam, D.W.; James, W.P.T. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef]
- Wadden, T.A.; Webb, V.L.; Moran, C.H.; Bailer, B.A. Lifestyle modification for obesity: New developments in diet, physical activity, and behavior therapy. Circulation 2012, 125, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-H.; Stoll, C.R.T.; Song, J.; Varela, J.E.; Eagon, C.J.; Colditz, G.A. The effectiveness and risks of bariatric surgery: An updated systematic review and meta-analysis, 2003–2012. JAMA Surg. 2014, 149, 275–287. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014, 2014, CD003641. [Google Scholar] [CrossRef]
- IFSO Registry. International Federation for the Surgery of Obesity and Metabolic Disorders. 2019. Available online: https://www.ifso.com/ifso-registry.php (accessed on 28 June 2022).
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Porat, D.; Markovic, M.; Zur, M.; Fine-Shamir, N.; Azran, C.; Shaked, G.; Czeiger, D.; Vaynshtein, J.; Replyanski, I.; Sebbag, G.; et al. Increased Paracetamol Bioavailability after Sleeve Gastrectomy: A Crossover Pre- vs. Post-Operative Clinical Trial. J. Clin. Med. 2019, 8, 1949. [Google Scholar] [CrossRef]
- Tan, Q.; Gao, Y.; Zhang, P.; Huo, Y.; Lu, Y.; Huang, W. Comparison of Outcomes in Patients with Obesity Between Two Administration Routes of Omeprazole After Laparoscopic Sleeve Gastrectomy: An Open-Label Randomized Clinical Trial. Drug Des. Dev. Ther. 2021, 15, 1569–1576. [Google Scholar] [CrossRef]
- Collares-Pelizaro, R.V.A.; Santos, J.S.; Nonino, C.B.; Gaitani, C.M.; Salgado, W. Omeprazole Absorption and Fasting Gastrinemia after Roux-en-Y Gastric Bypass. Obes. Surg. 2017, 27, 2303–2307. [Google Scholar] [CrossRef]
- Mitrov-Winkelmolen, L.; van Buul-Gast, M.-C.W.; Swank, D.J.; Overdiek, H.W.P.M.; Van Schaik, R.H.N.; Touw, D. The Effect of Roux-en-Y Gastric Bypass Surgery in Morbidly Obese Patients on Pharmacokinetics of (Acetyl)Salicylic Acid and Omeprazole: The ERY-PAO Study. Obes. Surg. 2016, 26, 2051–2058. [Google Scholar] [CrossRef]
- Martínez-Ortega, A.J.; Olveira, G.; Pereira-Cunill, J.L.; Arraiza-Irigoyen, C.; García-Almeida, J.M.; Irles Rocamora, J.A.; Molina-Puerta, M.J.; Molina Soria, J.B.; Rabat-Restrepo, J.M.; Rebollo-Pérez, M.I.; et al. Recommendations Based on Evidence by the Andalusian Group for Nutrition Reflection and Investigation (GARIN) for the Pre- and Postoperative Management of Patients Undergoing Obesity Surgery. Nutrients 2020, 12, 2002. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Marabotto, E.; Zentilin, P.; Furnari, M.; Bodini, G.; De Maria, C.; Pellegatta, G.; Coppo, C.; Savarino, E. Proton pump inhibitors: Use and misuse in the clinical setting. Expert Rev. Clin. Pharmacol. 2018, 11, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef]
- Porat, D.; Vaynshtein, J.; Gibori, R.; Avramoff, O.; Shaked, G.; Dukhno, O.; Czeiger, D.; Sebbag, G.; Dahan, A. Stomach pH before vs. after different bariatric surgery procedures: Clinical implications for drug delivery. Eur. J. Pharm. Biopharm. 2021, 160, 152–157. [Google Scholar] [CrossRef]
- Chen, K.; Lin, Y.; Luo, P.; Yang, N.; Yang, G.; Zhu, L.; Pei, Q. Effect of laparoscopic sleeve gastrectomy on drug pharmacokinetics. Expert Rev. Clin. Pharmacol. 2021, 14, 1481–1495. [Google Scholar] [CrossRef] [PubMed]
- Melissas, J.; Leventi, A.; Klinaki, I.; Perisinakis, K.; Koukouraki, S.; de Bree, E.; Karkavitsas, N. Alterations of global gastrointestinal motility after sleeve gastrectomy: A prospective study. Ann. Surg. 2013, 258, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.I.; Chung, V.; Synold, T.W.; Longmate, J.A.; Suttle, A.B.; Ottesen, L.H.; Lenz, H.-J.; Kummar, S.; Harvey, R.D.; Hamilton, A.L.; et al. Phase I study of pazopanib in patients with advanced solid tumors and hepatic dysfunction: A National Cancer Institute Organ Dysfunction Working Group study. Clin. Cancer Res. 2013, 19, 3631–3639. [Google Scholar] [CrossRef]
- Chen, K.; Luo, P.; Yang, G.; Zhu, S.; Deng, C.; Ding, J.; Lin, Y.; Zhu, L.; Pei, Q. Population pharmacokinetics of omeprazole in obese and normal-weight adults. Expert Rev. Clin. Pharmacol. 2022, 15, 461–471. [Google Scholar] [CrossRef]
- Lima, J.J.; Thomas, C.D.; Barbarino, J.; Desta, Z.; Van Driest, S.L.; El Rouby, N.; Johnson, J.A.; Cavallari, L.H.; Shakhnovich, V.; Thacker, D.L.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin. Pharmacol. Ther. 2021, 109, 1417–1423. [Google Scholar] [CrossRef]
- Wasmann, R.E.; Ter Heine, R.; van Dongen, E.P.; Burger, D.M.; Lempers, V.J.; Knibbe, C.A.J.; Brüggemann, R.J. Pharmacokinetics of Anidulafungin in Obese and Normal-Weight Adults. Antimicrob. Agents Chemother. 2018, 62, e00063-18. [Google Scholar] [CrossRef] [Green Version]
- Dosne, A.G.; Bergstrand, M.; Harling, K.; Karlsson, M.O. Improving the estimation of parameter uncertainty distributions in nonlinear mixed effects models using sampling importance resampling. J. Pharmacokinet. Pharmacodyn. 2016, 43, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Savic, R.M.; Jonker, D.M.; Kerbusch, T.; Karlsson, M.O. Implementation of a transit compartment model for describing drug absorption in pharmacokinetic studies. J. Pharmacokinet. Pharmacodyn. 2007, 34, 711–726. [Google Scholar] [CrossRef] [PubMed]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of lean bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef] [PubMed]
- McCarron, M.M.; Devine, B.J. Clinical pharmacy: Case studies: Case number 25 gentamicin therapy. Drug Intell. Clin. Pharm. 1974, 8, 650–655. [Google Scholar] [CrossRef]
- Schwartz, S.N.; Pazin, G.J.; Lyon, J.A.; Ho, M.; Pasculle, A.W. A controlled investigation of the pharmacokinetics of gentamicin and tobramycin in obese subjects. J. Infect. Dis. 1978, 138, 499–505. [Google Scholar] [CrossRef]
- Goday Arno, A.; Farré, M.; Rodríguez-Morató, J.; Ramon, J.M.; Pérez-Mañá, C.; Papaseit, E.; Civit, E.; Langohr, K.; Carbó, M.; Boix, D.B.; et al. Pharmacokinetics in Morbid Obesity: Influence of Two Bariatric Surgery Techniques on Paracetamol and Caffeine Metabolism. Obes. Surg. 2017, 27, 3194–3201. [Google Scholar] [CrossRef]
- Kvitne, K.E.; Krogstad, V.; Wegler, C.; Johnson, L.K.; Kringen, M.K.; Hovd, M.H.; Hertel, J.K.; Heijer, M.; Sandbu, R.; Skovlund, E.; et al. Short- and long-term effects of body weight, calorie restriction and gastric bypass on CYP1A2, CYP2C19 and CYP2C9 activity. Br. J. Clin. Pharmacol. 2022, 88, 4121–4133. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, H.; Meng, L.; Wang, M.; Yuan, H.; Ou, N.; Zhang, H.; Li, Z.; Shi, R. Influence of CYP2C19 on the relationship between pharmacokinetics and intragastric pH of omeprazole administered by successive intravenous infusions in Chinese healthy volunteers. Eur. J. Clin. Pharmacol. 2010, 66, 563–569. [Google Scholar] [CrossRef]
- Zhang, H.-J.; Zhang, X.-H.; Liu, J.; Sun, L.-N.; Shen, Y.-W.; Zhou, C.; Zhang, H.-W.; Xie, L.-J.; Chen, J.; Liu, Y.; et al. Effects of genetic polymorphisms on the pharmacokinetics and pharmacodynamics of proton pump inhibitors. Pharmacol. Res. 2020, 152, 104606. [Google Scholar] [CrossRef]
- Kaartinen, T.J.K.; Tornio, A.; Tapaninen, T.; Launiainen, T.; Isoherranen, N.; Niemi, M.; Backman, J.T. Effect of High-Dose Esomeprazole on CYP1A2, CYP2C19, and CYP3A4 Activities in Humans: Evidence for Substantial and Long-lasting Inhibition of CYP2C19. Clin. Pharmacol. Ther. 2020, 108, 1254–1264. [Google Scholar] [CrossRef]
- Shirai, N.; Furuta, T.; Moriyama, Y.; Okochi, H.; Kobayashi, K.; Takashima, M.; Xiao, F.; Kosuge, K.; Nakagawa, K.; Hanai, H.; et al. Effects of CYP2C19 genotypic differences in the metabolism of omeprazole and rabeprazole on intragastric pH. Aliment. Pharmacol. Ther. 2001, 15, 1929–1937. [Google Scholar]
- Hu, X.-P.; Xu, J.-M.; Hu, Y.-M.; Mei, Q.; Xu, X.-H. Effects of CYP2C19 genetic polymorphism on the pharmacokinetics and pharmacodynamics of omeprazole in Chinese people. J. Clin. Pharm. Ther. 2007, 32, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Marier, J.-F.; Dubuc, M.-C.; Drouin, E.; Alvarez, F.; Ducharme, M.P.; Brazier, J.-L. Pharmacokinetics of omeprazole in healthy adults and in children with gastroesophageal reflux disease. Ther. Drug Monit. 2004, 26, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Nagase, M.; Shimada, H.; Nii, M.; Ueda, S.; Higashimori, M.; Ichikawa, K.; Zhang, L.; Zhou, L.; Chen, Y.; Zhou, D.; et al. Population pharmacokinetic analysis of esomeprazole in Japanese subjects with various CYP2C19 phenotypes. J. Clin. Pharm. Ther. 2020, 45, 1030–1038. [Google Scholar] [CrossRef]
- Rodríguez-Morató, J.; Goday, A.; Langohr, K.; Pujadas, M.; Civit, E.; Pérez-Mañá, C.; Papaseit, E.; Ramon, J.M.; Benaiges, D.; Castañer, O.; et al. Short- and medium-term impact of bariatric surgery on the activities of CYP2D6, CYP3A4, CYP2C9, and CYP1A2 in morbid obesity. Sci. Rep. 2019, 9, 20405. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Pre-Surgery (n = 62) | 7 Days Post-LSG (n = 41) | 1 Month Post-LSG (n = 20) |
|---|---|---|---|
| No. (%) of participants by sex | |||
| Female | 43 (69%) | 29 (71%) | 16 (80%) |
| Male | 19 (31%) | 12 (29%) | 4 (20%) |
| No. (%) of participants by CYP2C19 genotype | |||
| Normal metabolizers (NMs) | 26 (42%) | 17 (41.5%) | 4 (20%) |
| Intermediate metabolizers (IMs) | 27 (43.5%) | 18 (44%) | 12 (60%) |
| Poor metabolizers (PMs) | 9 (14.5%) | 6 (14.5%) | 4 (20%) |
| Median (Q1~Q3) values for: | |||
| Age (year) | 31 (27~35) | 28 (25~33) | 28 (23~33) |
| Weight (kg) | 110.8 (91~127) | 114.6 (90.7~124.6) | * 96.2 (82.7~105.8) |
| Height (cm) | 162.5 (158.6~167.5) | 163 (158.5~169) | 160.5 (158.1~166.4) |
| BMI (kg/m2) | 40.3 (35~46) | 41.2 (34.6~45.2) | * 36.1 (31.7~39.5) |
| LBW (kg) | 55.1 (48.9~69.6) | 55.3 (47~68.5) | * 50.9 (46~54) |
| IBW (kg) | 54.8 (50.9~60.6) | 54.8 (50.8~63) | 52.7 (50.5~58.3) |
| ABW (kg) | 78.5 (68.8~89.2) | 79.2 (65.5~84.6) | * 71.7 (64.4~76) |
| No. (%) of participants by liver function | |||
| Normal liver function | 27 (43.5%) | 6 (14.6%) | 7 (35%) |
| Mild liver dysfunction | 35 (56.5%) | 35 (85.4%) | 13 (65%) |
| Parameter | Final Estimates | RSE (%) | SIR (Median) | RSE (%) | 95% CI |
|---|---|---|---|---|---|
| Structural model | |||||
| MTT for visit 1 (h) | 1.91 | 6 | 1.92 | 6 | 1.68–2.13 |
| MTT ratio for visit 2: visit 1 (θ1) | 0.27 | 11.4 | 0.27 | 11.2 | 0.21–0.33 |
| MTT ratio for visit 3: visit 1 (θ2) | 0.45 | 7.6 | 0.45 | 7.6 | 0.38–0.51 |
| CL/F for normal metabolizers with normal liver function (L/h) | 16.7 | 14.9 | 16.7 | 14.4 | 11.9–21.3 |
| CL/F ratio for CYP2C19 intermediate metabolizers: normal metabolizers (θ3) | 0.8 | 12.4 | 0.8 | 12.3 | 0.6–0.98 |
| CL/F ratio for CYP2C19 poor metabolizers: normal metabolizers (θ4) | 0.34 | 17.8 | 0.35 | 17.5 | 0.22–0.45 |
| CL/F ratio for mild liver dysfunction: normal liver function (θ5) | 0.6 | 11.6 | 0.6 | 11.1 | 0.47–0.73 |
| Vd/F (L) | 22.1 | 5.5 | 22.2 | 5.4 | 19.7–24.5 |
| Interindividual variability | |||||
| 2 MTT | 0.16 | 19.7 | 0.16 | 19.1 | 0.1–0.23 |
| 2 CL/F | 0.16 | 22.8 | 0.15 | 21.6 | 0.1–0.22 |
| IOV on CL/F | 0.05 | 39.3 | 0.05 | 38.7 | 0.01–0.09 |
| Residual error | |||||
| σ2 Proportional error | 0.175 | 12.1 | 0.175 | 12.6 | 0.134–0.222 |
| Pre-Surgery (N = 62) | 7 Days Post-LSG (N = 41) | 1 Month Post-LSG (N = 20) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CYP2C19 NMs | CYP2C19 IMs | CYP2C19 PMs | CYP2C19 NMs | CYP2C19 IMs | CYP2C19 PMs | CYP2C19 NMs | CYP2C19 IMs | CYP2C19 PMs | |
| Normal liver function | |||||||||
| Tmax (h) | 2.3 (2~3) | 2.3 (2~3.5) | 2.7 (2~3.5) | * 0.8 (0.5~1) | * 0.8 (0.8~1) | * 0.8 (0.8~1) | * 1.3 (1~1.7) | * 1.3 (1~1.7) | * 1.3 (1~1.7) |
| Cmax (ng/mL) | 470 (386~540) | 512 (427~588) | 663 (595~717) | * 688 (634~738) | * 720 (660~763) | * 804 (771~830) | * 612 (547~674) | * 650 (583~709) | * 767 (720~809) |
| AUC0-inf (ng·h/mL) | 1198 (876~1609) | 1476 (1097~2061) | 3483 (2537~4697) | 1185 (881~1585) | 1540 (1067~2039) | 3470 (2619~4562) | 1156 (894~1613) | 1497 (1128~2054) | 3520 (2560~4725) |
| CL/F (L/h) | 16.7 (12.4~22.8) | 13.5 (9.7~18.2) | 5.7 (4.3~7.9) | 16.9 (12.6~22.7) | 13 (9.8~18.7) | 5.8 (4.4~7.6) | 17.3 (12.4~22.4) | 13.3 (9.7~17.7) | 5.7 (4.2~7.8) |
| Mild liver dysfunction | |||||||||
| Tmax (h) | 2.7 (2~3.5) | 2.7 (2~3.5) | 3 (2.3~3.5) | * 0.8 (0.8~1) | * 0.8 (0.8~1) | * 1 (0.8~1) | * 1.3 (1~1.7) | * 1.3 (1~1.7) | * 1.3 (1~1.7) |
| Cmax (ng/mL) | 571 (501~640) | 606 (533~670) | 740 (682~782) | * 752 (708~789) | * 779 (734~808) | * 840 (817~858) | * 699 (637~744) | * 725 (674~768) | * 835 (788~894) |
| AUC0-inf (ng·h/mL) | 2032 (1484~2654) | 2470 (1828~3242) | 5948 (4376~8081) | 1969 (1482~2654) | 2530 (1882~3443) | 5945 (4358~8258) | 2027 (1519~2680) | 2457 (1880~3345) | 6019 (4399~8085) |
| CL/F (L/h) | 9.8 (7.4~13.5) | 8.1 (6.2~11) | 3.4 (2.5~4.6) | 10.2 (7.5~13.5) | 7.9 (5.8~10.6) | 3.4 (2.4~4.7) | 9.9 (7.5~13.2) | 8.1 (6~10.6) | 3.3 (2.5~4.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.; Luo, P.; Zhu, S.; Lin, Y.; Yang, N.; Huang, S.; Ding, Q.; Zhu, L.; Pei, Q. Effect of Laparoscopic Sleeve Gastrectomy on the Pharmacokinetics of Oral Omeprazole Using a Population Approach. Pharmaceutics 2022, 14, 1986. https://doi.org/10.3390/pharmaceutics14101986
Chen K, Luo P, Zhu S, Lin Y, Yang N, Huang S, Ding Q, Zhu L, Pei Q. Effect of Laparoscopic Sleeve Gastrectomy on the Pharmacokinetics of Oral Omeprazole Using a Population Approach. Pharmaceutics. 2022; 14(10):1986. https://doi.org/10.3390/pharmaceutics14101986
Chicago/Turabian StyleChen, Kaifeng, Ping Luo, Shaihong Zhu, Yaqi Lin, Nan Yang, Shuqi Huang, Qin Ding, Liyong Zhu, and Qi Pei. 2022. "Effect of Laparoscopic Sleeve Gastrectomy on the Pharmacokinetics of Oral Omeprazole Using a Population Approach" Pharmaceutics 14, no. 10: 1986. https://doi.org/10.3390/pharmaceutics14101986