
Lung Targeted Lipopolymeric Microspheres of Dexamethasone for the Treatment of ARDS

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Preparation of Dexamethasone Microspheres and Estimation of Loading and Encapsulation Efficiency
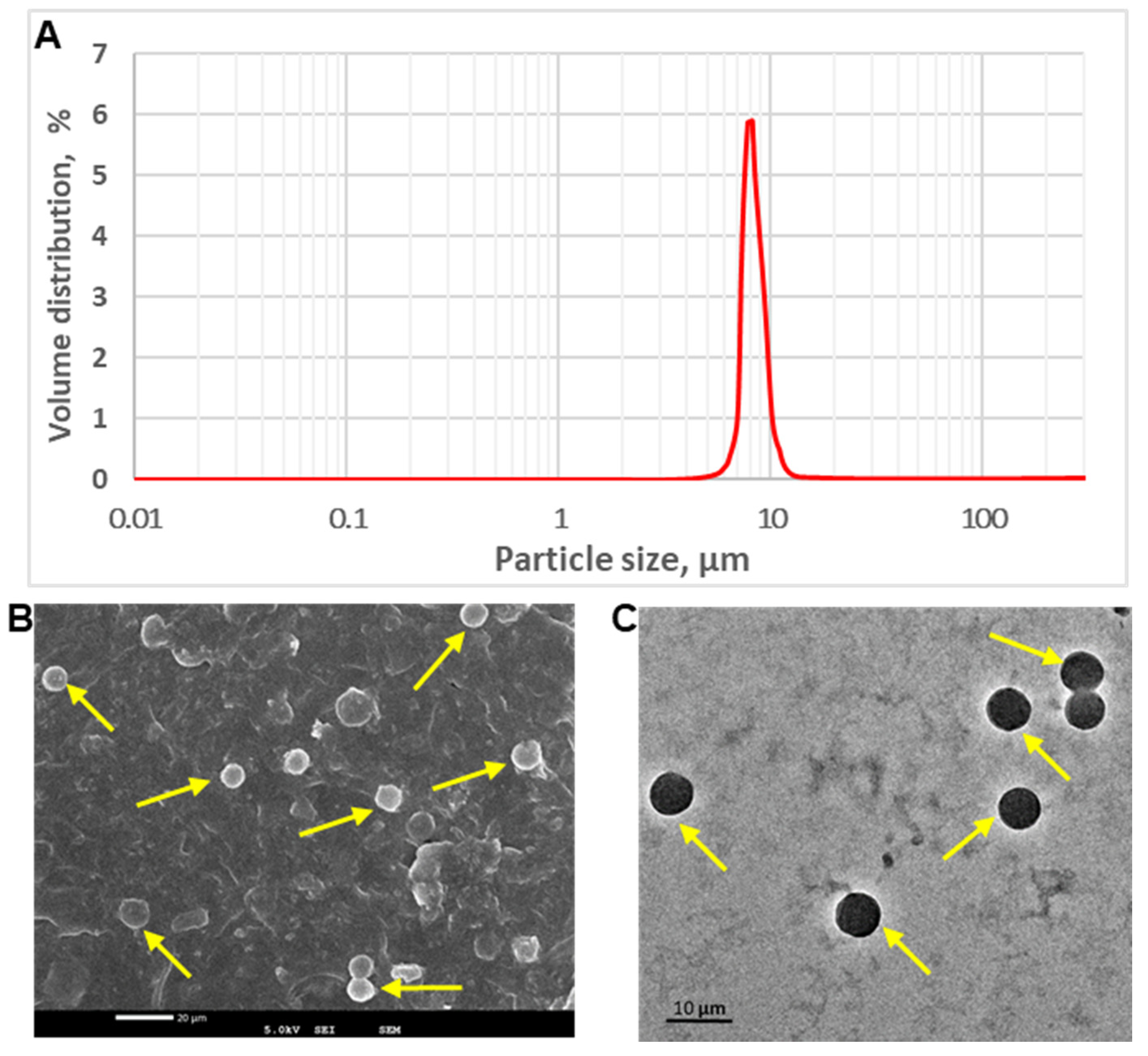
2.2.2. Determination of Particle Size, Distribution and Imaging Using Electron Microscopy
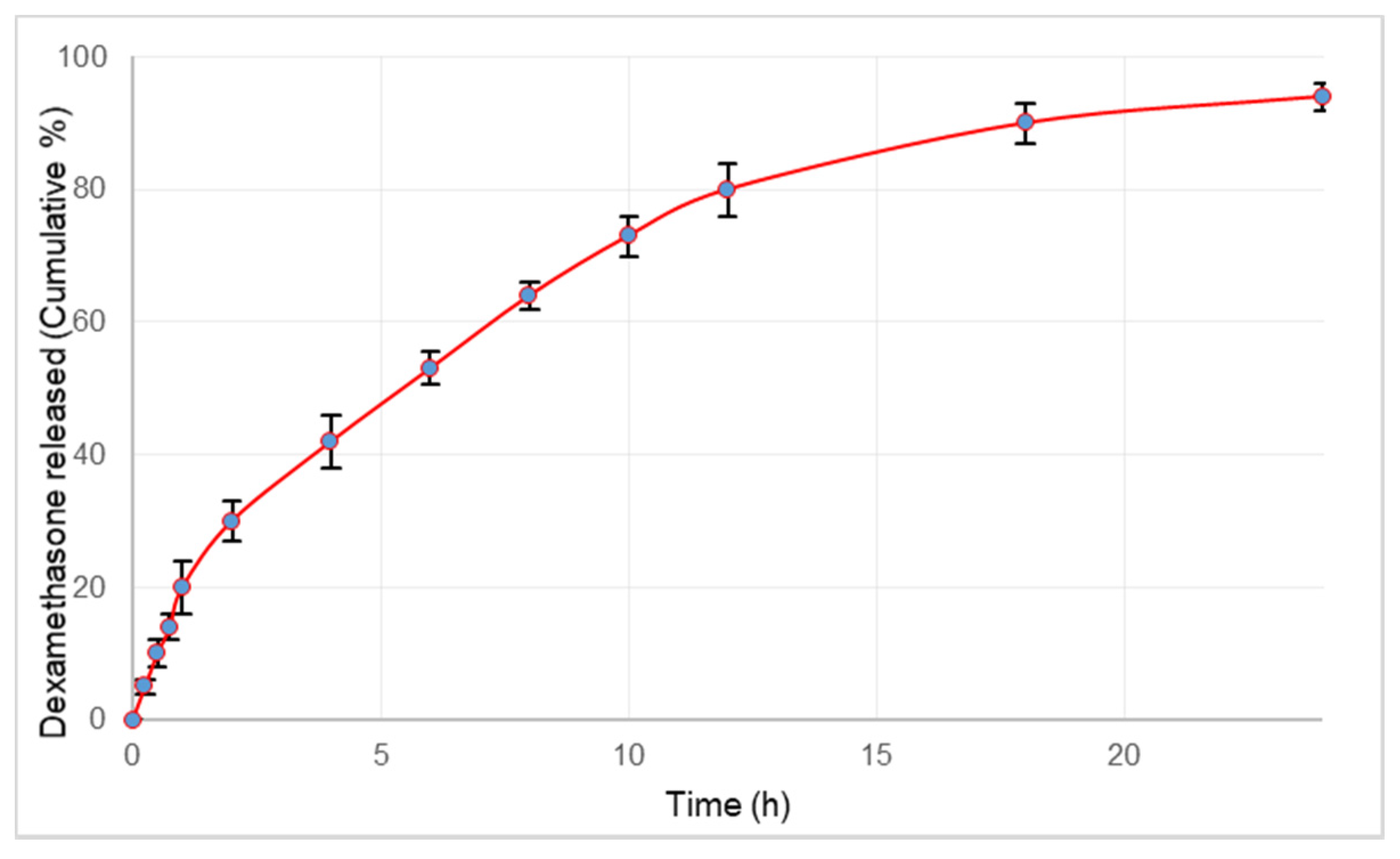
2.2.3. In Vitro Release of Dexamethasone
2.2.4. Analysis of Dexamethasone by HPLC
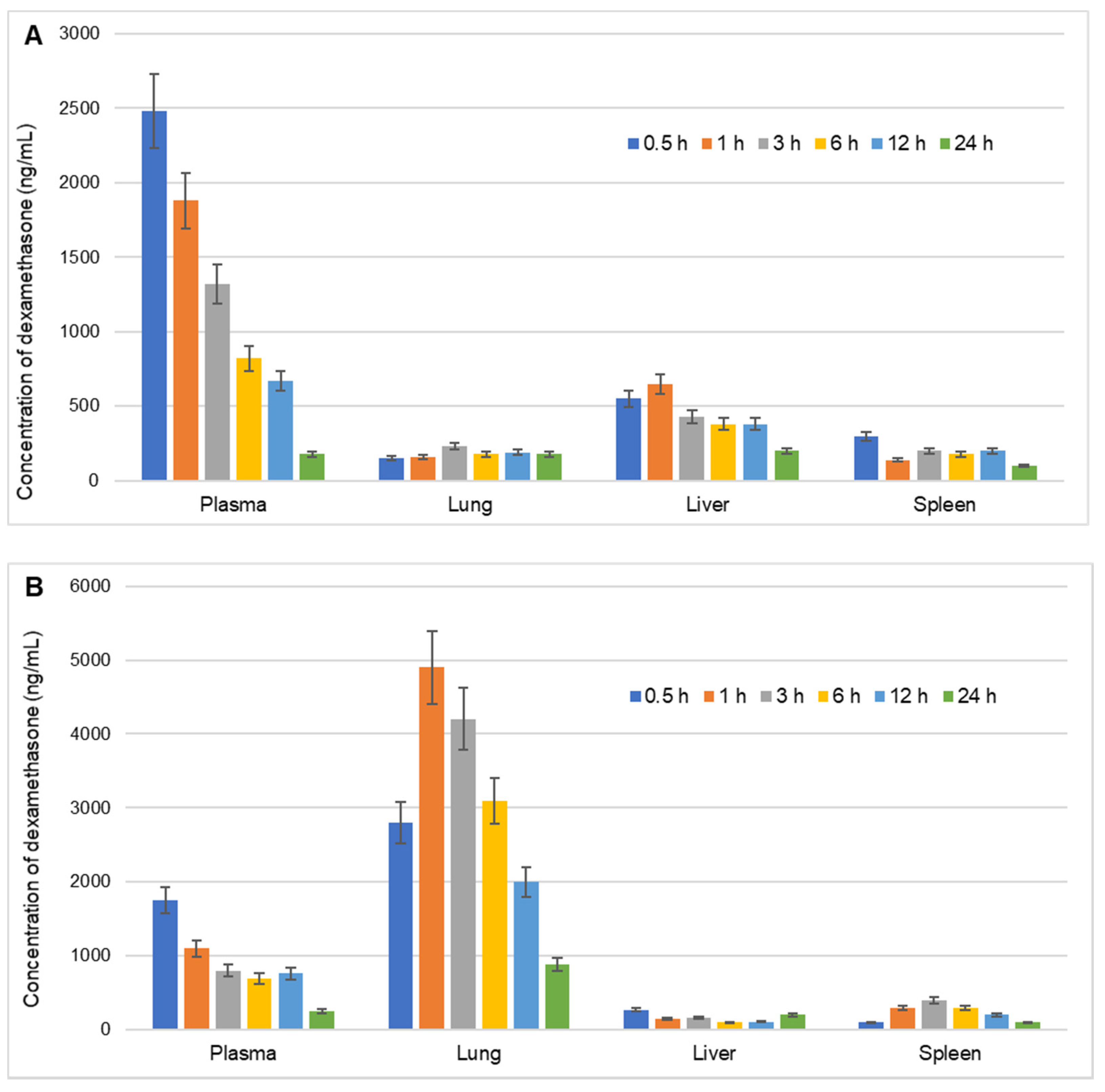
2.2.5. Pharmacokinetic, Biodistribution and Targeting Efficiency
2.2.6. Induction of Lung Inflammation and In Vivo Efficacy Testing
LPS Induced ARDS Model in Rats
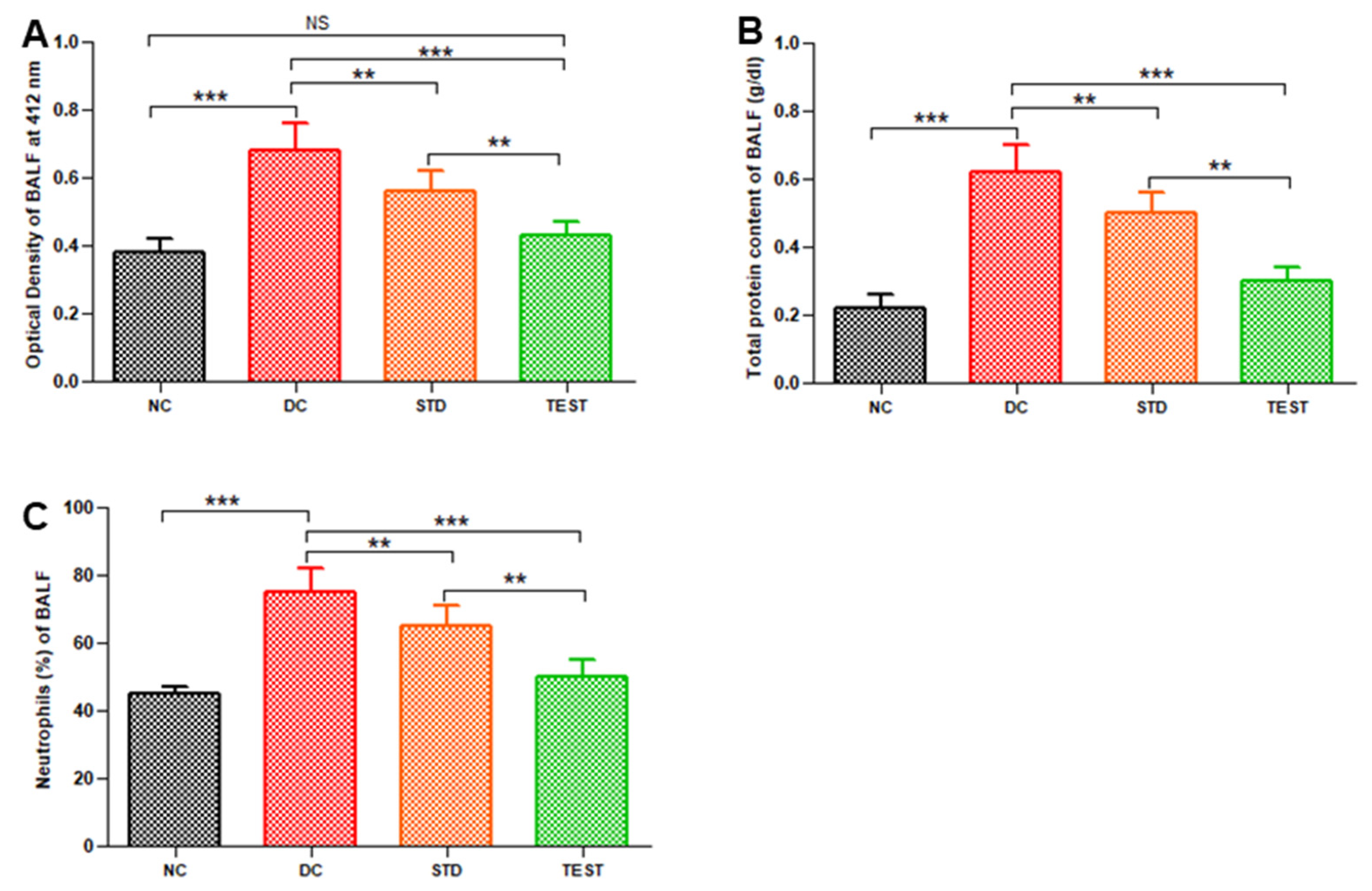
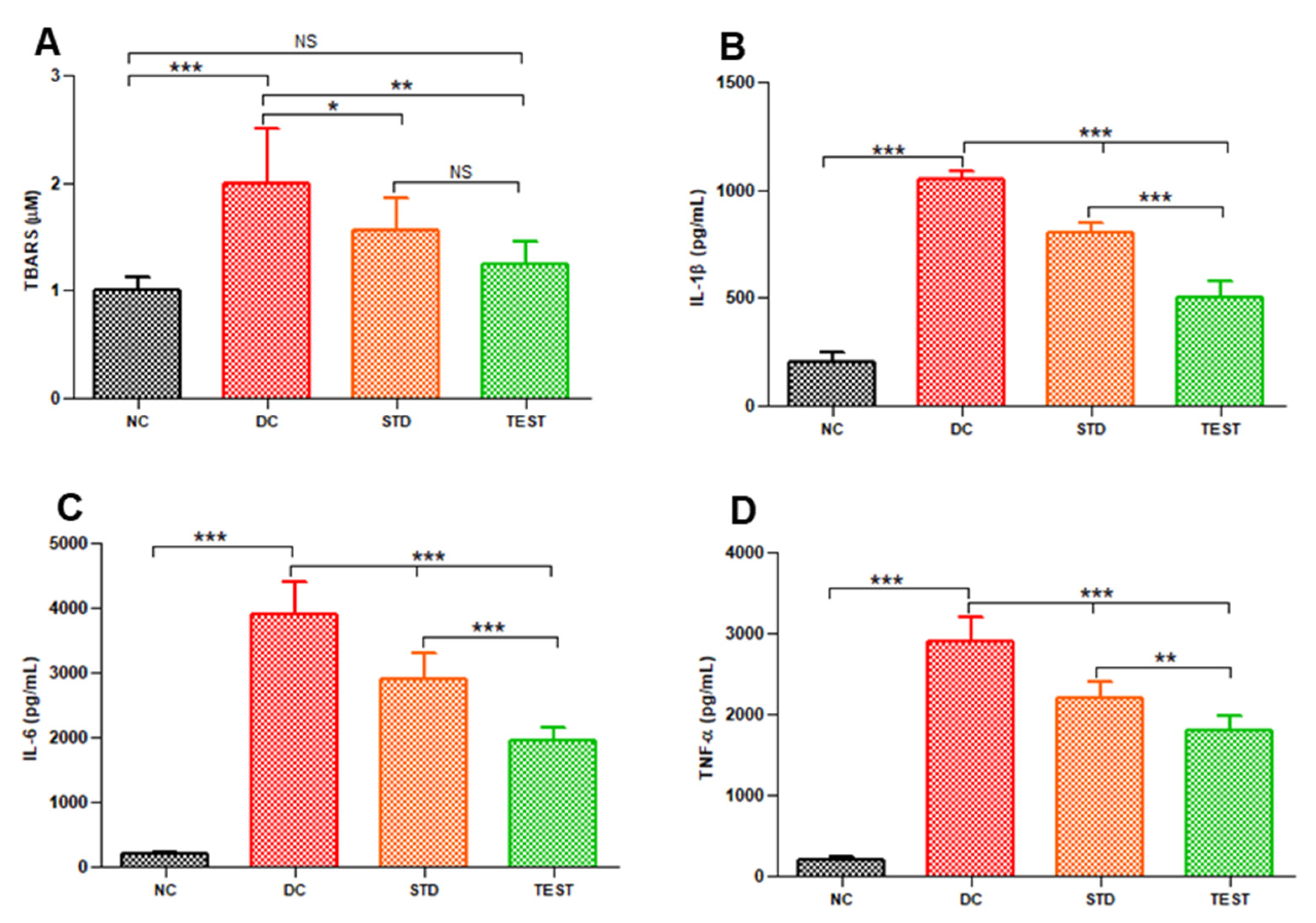
In Vivo Estimation of Inflammation Markers in Bronchoalveolar Lavage Fluid (BAL)
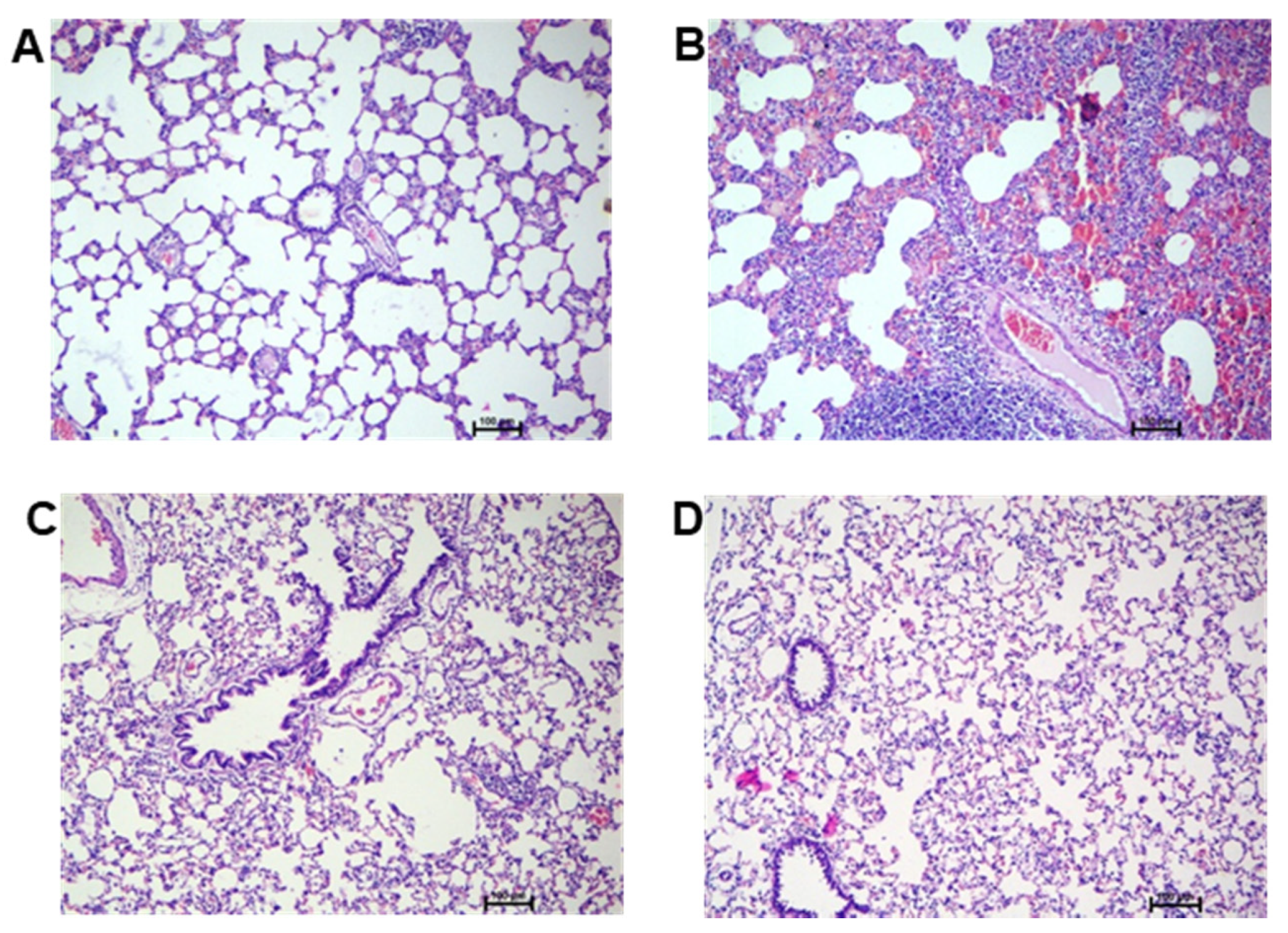
Histopathology of Lungs
2.2.7. Statistical Analysis
3. Results and Discussion
3.1. Determination of Particle Size, Distribution and Imaging Using Electron Microscopy
3.2. In Vitro Release of Dexamethasone
3.3. Pharmacokinetic, Biodistribution and Targeting Efficiency
3.4. In vivo Efficacy in LPS Induced ARDS Model
3.5. Histopathology Studies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marini, J.J.; Gattinoni, L. Management of COVID-19 Respiratory Distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef] [PubMed]
- Kotta, S.; Aldawsari, H.M.; Badr-Eldin, S.M.; Alhakamy, N.A.; Md, S.; Nair, A.B.; Deb, P.K. Combating the Pandemic COVID-19: Clinical Trials, Therapies and Perspectives. Front. Mol. Biosci. 2020, 7, 606393. [Google Scholar] [CrossRef]
- Papanikolaou, I.C.; Tsenempi, X.A. Tropical Lung Diseases. Hunt. Trop. Med. Emerg. Infect. Dis. 2020, 1–7. [Google Scholar] [CrossRef]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e51. [Google Scholar] [CrossRef] [PubMed]
- Máca, J.; Jor, O.; Holub, M.; Sklienka, P.; Burša, F.; Burda, M.; Janout, V.; Ševčík, P. Past and Present ARDS Mortality Rates: A Systematic Review. Respir. Care 2017, 62, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Lee, K.H.; Yoon, S.; Jeong, G.H.; Kim, J.Y.; Han, Y.J.; Hong, S.H.; Ryu, S.; Kim, J.S.; Lee, J.Y.; Yang, J.W.; et al. Efficacy of Corticosteroids in Patients with SARS, MERS and COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2392. [Google Scholar] [CrossRef]
- Romanou, V.; Koukaki, E.; Chantziara, V.; Stamou, P.; Kote, A.; Vasileiadis, I.; Koutsoukou, A.; Rovina, N. Dexamethasone in the Treatment of COVID-19: Primus Inter Pares? J. Pers. Med. 2021, 11, 556. [Google Scholar] [CrossRef]
- Abraham, S.M.; Lawrence, T.; Kleiman, A.; Warden, P.; Medghalchi, M.; Tuckermann, J.; Saklatvala, J.; Clark, A.R. Antiinflammatory effects of dexamethasone are partly dependent on induction of dual specificity phosphatase 1. J. Exp. Med. 2006, 203, 1883–1889. [Google Scholar] [CrossRef] [Green Version]
- Waljee, A.K.; Rogers, M.A.; Lin, P.; Singal, A.G.; Stein, J.D.; Marks, R.M.; Ayanian, J.Z.; Nallamothu, B.K. Short term use of oral corticosteroids and related harms among adults in the United States: Population based cohort study. BMJ (Clin. Res. Ed.) 2017, 357, j1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, J.B.; White, A.G.; Scarpati, L.M.; Wan, G.; Nelson, W.W. Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clin. Ther. 2017, 39, 2216–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ericson-Neilsen, W.; Kaye, A.D. Steroids: Pharmacology, complications, and practice delivery issues. Ochsner J. 2014, 14, 203–207. [Google Scholar] [PubMed]
- Paranjpe, M.; Müller-Goymann, C.C. Nanoparticle-mediated pulmonary drug delivery: A review. Int. J. Mol. Sci. 2014, 15, 5852–5873. [Google Scholar] [CrossRef]
- Pontes, J.F.; Grenha, A. Multifunctional Nanocarriers for Lung Drug Delivery. Nanomaterials 2020, 10, 183. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.A.; Firdous, J.; Choi, Y.J.; Yun, C.H.; Cho, C.S. Design and application of chitosan microspheres as oral and nasal vaccine carriers: An updated review. Int. J. Nanomed. 2012, 7, 6077–6093. [Google Scholar] [CrossRef] [Green Version]
- Gangane, P.; Kawtikwar, P. Development of Donepezil Hydrochloride Loaded Gellan Gum Based Nasal Mucoadhesive Microspheres by Spray Drying Method. Indian J. Pharm. Educ. Res. 2020, 54, 935–945. [Google Scholar] [CrossRef]
- Sangi, S.; SreeHarsha, N.; Bawadekji, A.; Al Ali, M. Chemotherapeutic drug targeting to lungs by way of microspheres after intravenous administration. Drug Des. Dev. Ther. 2018, 12, 3051–3060. [Google Scholar] [CrossRef] [Green Version]
- Huo, D.; Deng, S.; Li, L.; Ji, J. Studies on the poly(lactic-co-glycolic) acid microspheres of cisplatin for lung-targeting. Int. J. Pharm. 2005, 289, 63–67. [Google Scholar] [CrossRef]
- Harsha, S.; Al-Khars, M.; Al-Hassan, M.; Kumar, N.P.; Nair, A.B.; Attimarad, M.; Al-Dhubiab, B.E. Pharmacokinetics and tissue distribution of spray-dried carboplatin microspheres: Lung targeting via intravenous route. Arch. Pharmacal Res. 2014, 37, 352–360. [Google Scholar] [CrossRef]
- SreeHarsha, N.; Venugopala, K.N.; Nair, A.B.; Roopashree, T.S.; Attimarad, M.; Hiremath, J.G.; Al-Dhubiab, B.E.; Ramnarayanan, C.; Shinu, P.; Handral, M.; et al. An Efficient, Lung-Targeted, Drug-Delivery System To Treat Asthma Via Microparticles. Drug Des. Dev. Ther. 2019, 13, 4389–4403. [Google Scholar] [CrossRef] [Green Version]
- Qu, S.; Dai, C.; Yang, F.; Huang, T.; Xu, T.; Zhao, L.; Li, Y.; Hao, Z. A Comparison of Two Methods for the Preparation Cefquinome-Loaded Gelatin Microspheres for Lung Targeting. Pharm. Res. 2018, 35, 43. [Google Scholar] [CrossRef] [PubMed]
- Ung, K.T.; Rao, N.; Weers, J.G.; Huang, D.; Chan, H.K. Design of spray dried insulin microparticles to bypass deposition in the extrathoracic region and maximize total lung dose. Int. J. Pharm. 2016, 511, 1070–1079. [Google Scholar] [CrossRef]
- Razuc, M.; Piña, J.; Ramírez-Rigo, M.V. Optimization of Ciprofloxacin Hydrochloride Spray-Dried Microparticles for Pulmonary Delivery Using Design of Experiments. AAPS PharmSciTech 2018, 19, 3085–3096. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, X.; Li, B.; Hou, Y.; Cai, Z.; Yang, J.; Li, Y. Paclitaxel-loaded PLGA microspheres with a novel morphology to facilitate drug delivery and antitumor efficiency. RSC Adv. 2018, 8, 3274–3285. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.B.; Shah, J.; Al-Dhubiab, B.E.; Jacob, S.; Patel, S.S.; Venugopala, K.N.; Morsy, M.A.; Gupta, S.; Attimarad, M.; Sreeharsha, N.; et al. Clarithromycin Solid Lipid Nanoparticles for Topical Ocular Therapy: Optimization, Evaluation and In vivo Studies. Pharmaceutics 2021, 13, 523. [Google Scholar] [CrossRef] [PubMed]
- Sreeharsha, N.; Hiremath, J.G.; Kumar, P.R.; Meravanige, G.; Khan, S.; Karnati, R.K.; Attimarad, M.; Al-Dhubiab, B.; Nair, A.B.; Venugopala, K.N. Doxorubicin Hydrochloride Loaded Polyanhydride Nanoformulations and Cytotoxicity. Indian J. Pharm. Educ. Res. 2021, 55, 117–125. [Google Scholar] [CrossRef]
- Harsha, S.N.; Aldhubiab, B.E.; Nair, A.B.; Alhaider, I.A.; Attimarad, M.; Venugopala, K.N.; Srinivasan, S.; Gangadhar, N.; Asif, A.H. Nanoparticle formulation by Büchi B-90 Nano Spray Dryer for oral mucoadhesion. Drug Des. Dev. Ther. 2015, 9, 273–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, J.; Nair, A.B.; Jacob, S.; Patel, R.K.; Shah, H.; Shehata, T.M.; Morsy, M.A. Nanoemulsion Based Vehicle for Effective Ocular Delivery of Moxifloxacin Using Experimental Design and Pharmacokinetic Study in Rabbits. Pharmaceutics 2019, 11, 230. [Google Scholar] [CrossRef] [Green Version]
- Schafroth, N.; Arpagaus, C.; Jadhav, U.Y.; Makne, S.; Douroumis, D. Nano and microparticle engineering of water insoluble drugs using a novel spray-drying process. Colloids Surf. B Biointerfaces 2012, 90, 8–15. [Google Scholar] [CrossRef]
- D’Souza, S.S.; DeLuca, P.P. Development of a dialysis in vitro release method for biodegradable microspheres. AAPS PharmSciTech 2005, 6, E323–E328. [Google Scholar] [CrossRef] [Green Version]
- Morsy, M.A.; Nair, A.B. Prevention of rat liver fibrosis by selective targeting of hepatic stellate cells using hesperidin carriers. Int. J. Pharm. 2018, 552, 241–250. [Google Scholar] [CrossRef]
- Satyavert; Gupta, S.; Choudhury, H.; Jacob, S.; Nair, A.B.; Dhanawat, M.; Munjal, K. Pharmacokinetics and tissue distribution of hydrazinocurcumin in rats. Pharmacol. Rep. PR 2021. [Google Scholar] [CrossRef]
- Luo, L.H.; Zheng, P.J.; Nie, H.; Chen, Y.C.; Tong, D.; Chen, J.; Cheng, Y. Pharmacokinetics and tissue distribution of docetaxel liposome mediated by a novel galactosylated cholesterol derivatives synthesized by lipase-catalyzed esterification in non-aqueous phase. Drug Deliv. 2016, 23, 1282–1290. [Google Scholar] [CrossRef]
- Harsha, S.; Al-Dhubiab, B.E.; Nair, A.B.; Al-Khars, M.; Al-Hassan, M.; Rajan, R.; Attimarad, M.; Venugopala, K.N.; Asif, A.H. Novel drying technology of microsphere and its evaluation for targeted drug delivery for lungs. Dry Technol. 2015, 33, 502–512. [Google Scholar] [CrossRef]
- Nair, A.; Morsy, M.A.; Jacob, S. Dose translation between laboratory animals and human in preclinical and clinical phases of drug development. Drug Dev. Res. 2018, 79, 373–382. [Google Scholar] [CrossRef]
- Fiala, A.; Slagle, C.; Legband, N.; Aghabaglou, F.; Buesing, K.; Borden, M.; Harris, S.; Terry, B. Treatment of a Rat Model of LPS-Induced ARDS via Peritoneal Perfusion of Oxygen Microbubbles. J. Surg. Res. 2020, 246, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Shah, J.; Al-Dhubiab, B.E.; Patel, S.S.; Morsy, M.A.; Patel, V.; Chavda, V.; Jacob, S.; Sreeharsha, N.; Shinu, P.; et al. Development of Asialoglycoprotein Receptor-Targeted Nanoparticles for Selective Delivery of Gemcitabine to Hepatocellular Carcinoma. Molecules 2019, 24, 4566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, Q.; Liu, X.; Yang, T.; Cui, K.; Kong, L.; Yang, C.; Zhang, Z. Nanomedicine for acute respiratory distress syndrome: The latest application, targeting strategy, and rational design. Acta Pharm. Sin. B 2021. [Google Scholar] [CrossRef]
- Evora, C.; Soriano, I.; Rogers, R.A.; Shakesheff, K.N.; Hanes, J.; Langer, R. Relating the phagocytosis of microparticles by alveolar macrophages to surface chemistry: The effect of 1,2-dipalmitoylphosphatidylcholine. J. Control. Release Off. J. Control. Release Soc. 1998, 51, 143–152. [Google Scholar] [CrossRef]
- Gref, R.; Domb, A.; Quellec, P.; Blunk, T.; Müller, R.H.; Verbavatz, J.M.; Langer, R. The controlled intravenous delivery of drugs using PEG-coated sterically stabilized nanospheres. Adv. Drug Deliv. Rev. 1995, 16, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Salmaso, S.; Caliceti, P. Stealth Properties to Improve Therapeutic Efficacy of Drug Nanocarriers. J. Drug Deliv. 2013, 2013, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Mallampalli, R.K. The Role of Surfactant in Lung Disease and Host Defense against Pulmonary Infections. Ann. Am. Thorac. Soc. 2015, 12, 765–774. [Google Scholar] [CrossRef] [Green Version]
- Tavares Luiz, M.; Delello Di Filippo, L.; Carolina Alves, R.; Sousa Araújo, V.H.; Lobato Duarte, J.; Maldonado Marchetti, J.; Chorilli, M. The use of TPGS in drug delivery systems to overcome biological barriers. Eur. Polym. J. 2021, 142, 110129. [Google Scholar] [CrossRef]
- Emami, F.; Mostafavi Yazdi, S.J.; Na, D.H. Poly(lactic acid)/poly(lactic-co-glycolic acid) particulate carriers for pulmonary drug delivery. J. Pharm. Investig. 2019, 49, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Tan, Z.M.; Lai, G.P.; Pandey, M.; Srichana, T.; Pichika, M.R.; Gorain, B.; Bhattamishra, S.K.; Choudhury, H. Novel Approaches for the Treatment of Pulmonary Tuberculosis. Pharmaceutics 2020, 12, 1196. [Google Scholar] [CrossRef]
- Agnoletti, M.; Rodríguez-Rodríguez, C.; Kłodzińska, S.N.; Esposito, T.V.F.; Saatchi, K.; Mørck Nielsen, H.; Häfeli, U.O. Monosized Polymeric Microspheres Designed for Passive Lung Targeting: Biodistribution and Pharmacokinetics after Intravenous Administration. ACS Nano 2020, 14, 6693–6706. [Google Scholar] [CrossRef]
- Berkland, C.; Kim, K.; Pack, D.W. PLG microsphere size controls drug release rate through several competing factors. Pharm. Res. 2003, 20, 1055–1062. [Google Scholar] [CrossRef]
- Gupta, P.K.; Hung, C.T. Quantitative evaluation of targeted drug delivery systems. Int. J. Pharm. 1989, 56, 217–226. [Google Scholar] [CrossRef]
- Wang, H.M.; Bodenstein, M.; Markstaller, K. Overview of the pathology of three widely used animal models of acute lung injury. Eur. Surg. Res. Eur. Chir. Forschung Rech. Chir. Eur. 2008, 40, 305–316. [Google Scholar] [CrossRef]
- Zioud, F.; Marzaioli, V.; El-Benna, J.; Bachoual, R. Punica granatum and Citrillus colocynthis Aqueous extracts protect mice from LPS-induced lung inflammation and inhibit Metalloproteinases-2 and-9. Indian J. Pharm. Educ. Res. 2019, 53, 503–510. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plasma/Organ | Conventional Dexamethasone Injection te | Dexamethasone Microspheres te | ||
|---|---|---|---|---|
| Plasma | 0.84 | - | - | - |
| Lung | 13.98 | 0.23 | 3.88 | 16.56 |
| Liver | 0.45 | 0.36 | 0.19 | 0.53 |
| Spleen | 1.34 | 0.23 | 0.36 | 1.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotta, S.; Aldawsari, H.M.; Badr-Eldin, S.M.; Binmahfouz, L.S.; Bakhaidar, R.B.; Sreeharsha, N.; Nair, A.B.; Ramnarayanan, C. Lung Targeted Lipopolymeric Microspheres of Dexamethasone for the Treatment of ARDS. Pharmaceutics 2021, 13, 1347. https://doi.org/10.3390/pharmaceutics13091347
Kotta S, Aldawsari HM, Badr-Eldin SM, Binmahfouz LS, Bakhaidar RB, Sreeharsha N, Nair AB, Ramnarayanan C. Lung Targeted Lipopolymeric Microspheres of Dexamethasone for the Treatment of ARDS. Pharmaceutics. 2021; 13(9):1347. https://doi.org/10.3390/pharmaceutics13091347
Chicago/Turabian StyleKotta, Sabna, Hibah Mubarak Aldawsari, Shaimaa M. Badr-Eldin, Lenah S. Binmahfouz, Rana Bakur Bakhaidar, Nagaraja Sreeharsha, Anroop B. Nair, and Chandramouli Ramnarayanan. 2021. "Lung Targeted Lipopolymeric Microspheres of Dexamethasone for the Treatment of ARDS" Pharmaceutics 13, no. 9: 1347. https://doi.org/10.3390/pharmaceutics13091347