
Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research


Abstract
:1. Introduction
2. Materials and Methods
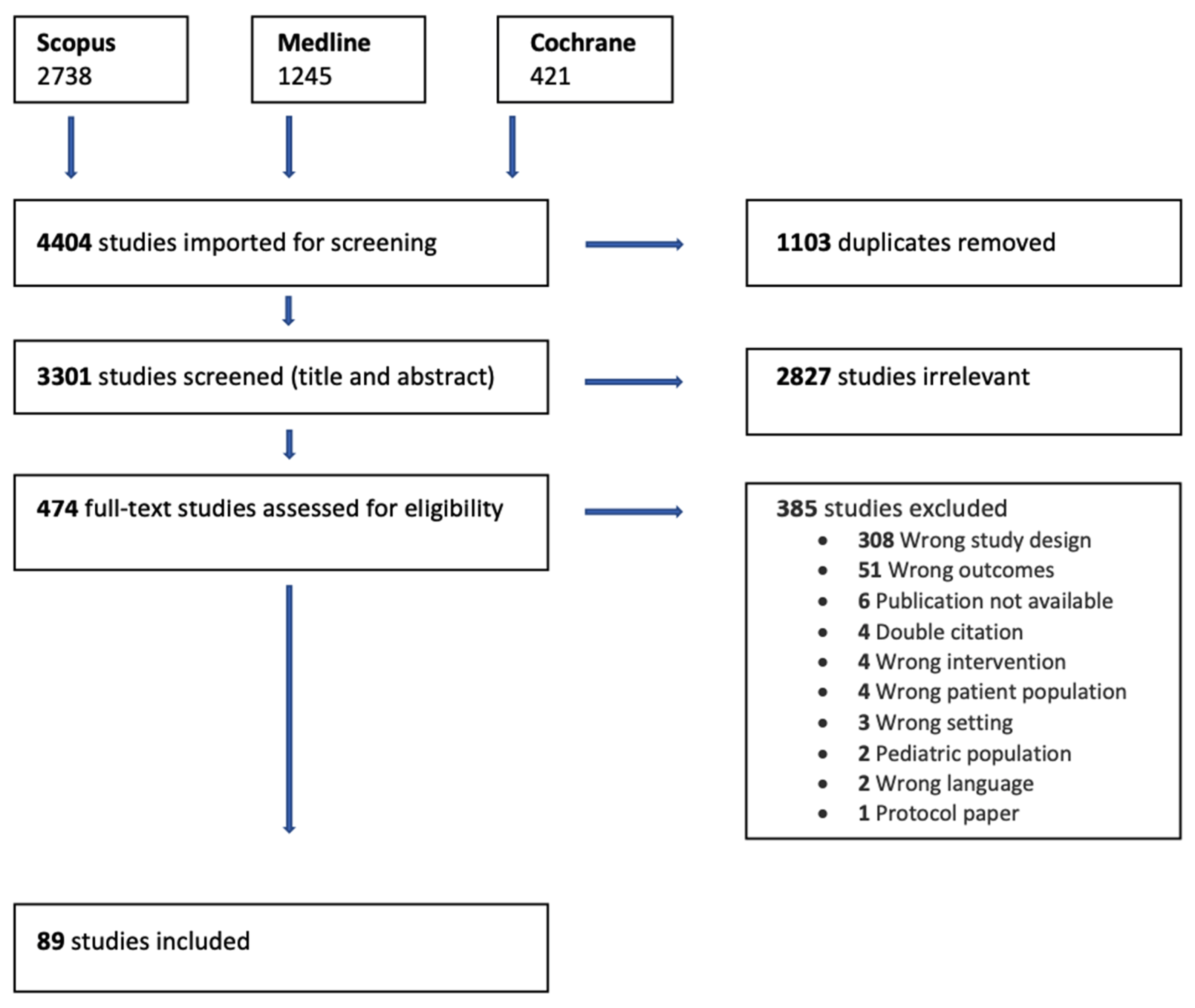
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
3. Results
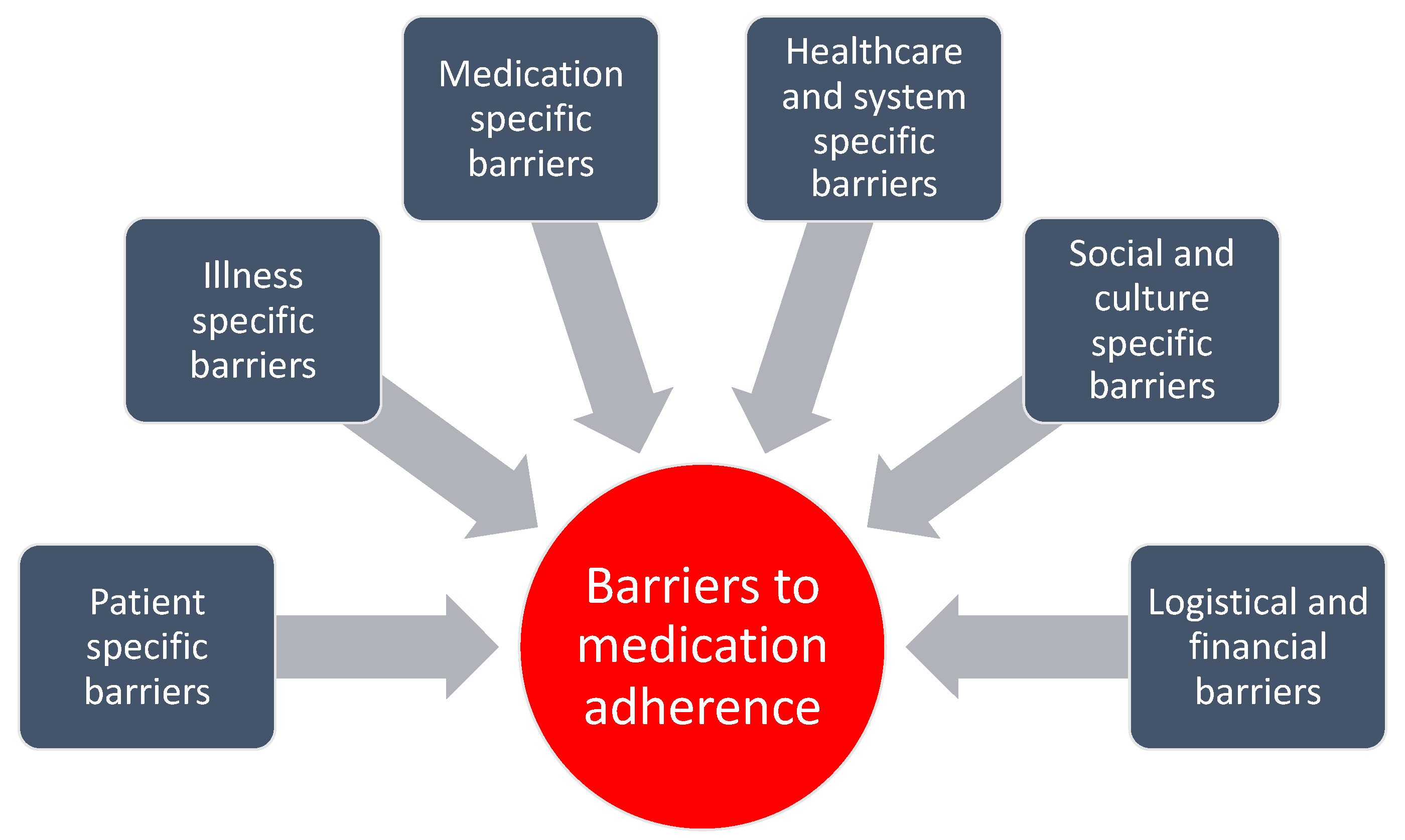
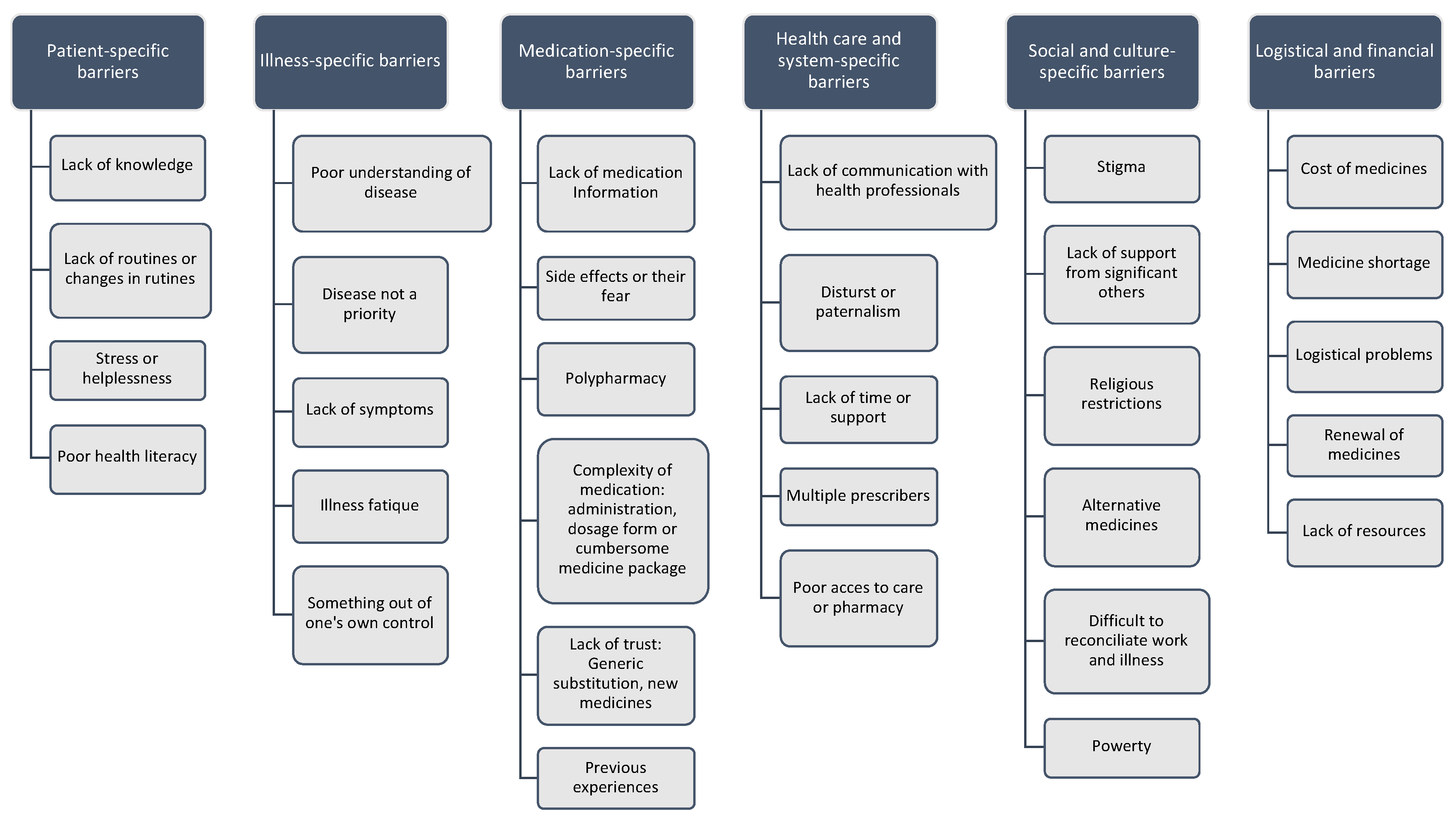
3.1. Barriers to Medication Adherence
3.1.1. Patient-Specific Barriers
3.1.2. Illness-Specific Barriers
3.1.3. Medication-Specific Barriers
3.1.4. Healthcare and System-Specific Barriers
3.1.5. Social and Culture-Specific Barriers
3.1.6. Logistical and Financial Barriers
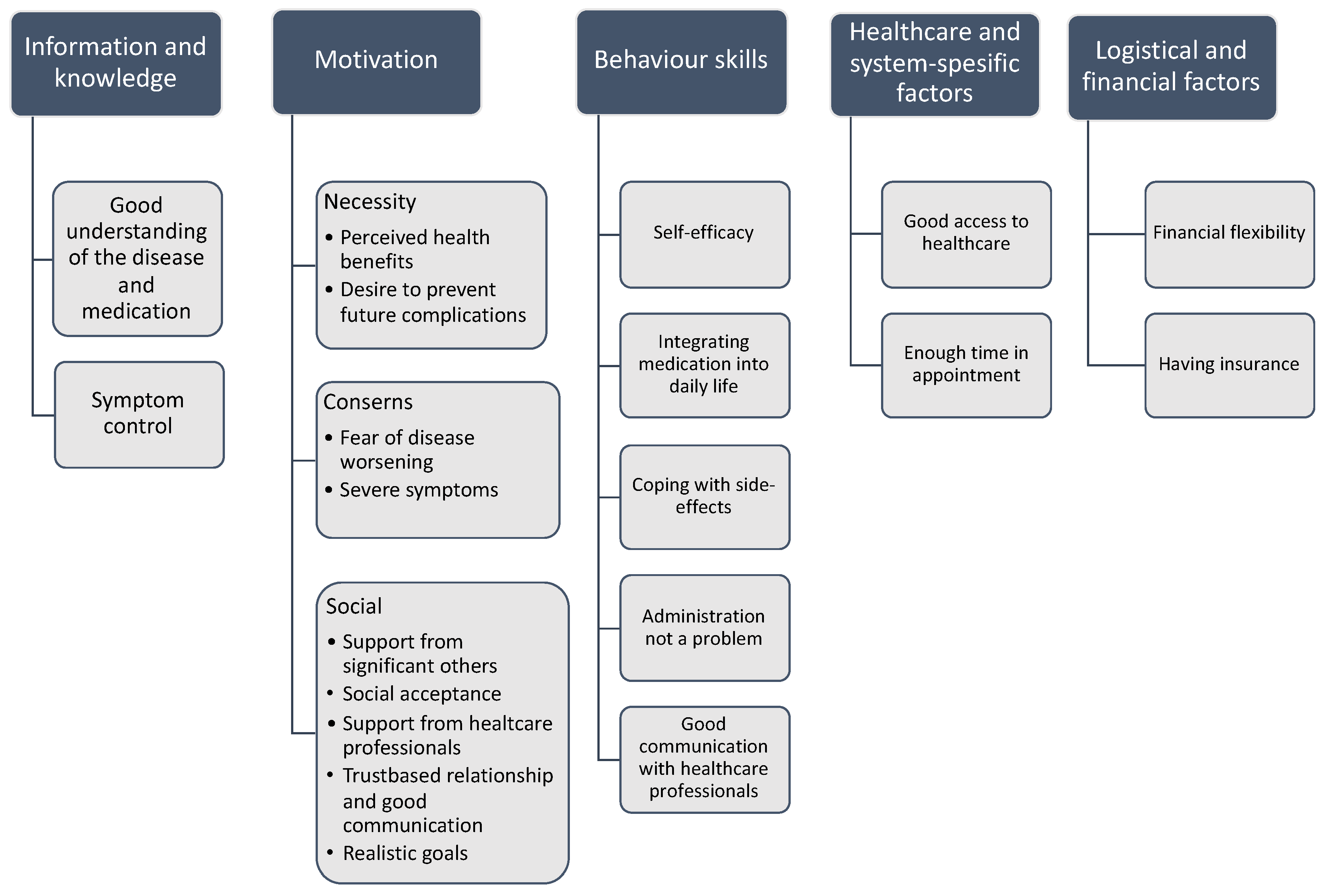
3.2. Facilitators to Medication Adherence
3.2.1. Informational, Motivational and Behavioural Factors
3.2.2. Healthcare and System-Specific Facilitators
3.2.3. Logistical and Financial Factors
3.3. Summary of Findings
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Title | Study Design | Concept | Context | Illness | Country in Which the Study Conducted |
|---|---|---|---|---|---|---|
| Al-Qazaz et al., 2011 | Perception and knowledge of patients with type 2diabetes in Malaysia about their disease and medication: A qualitative study | Individual interviews | Diabetic’ patients’ experience and knowledge about diabetes and its medication and the factors contributing to medication adherence | Diabetic 2 patients’ adherence to medication and knowledge about their illness | Cardiovascular disease | Malaysia |
| AlHamid et al., 2014 | A systematic review of qualitative research on the contributory factors leading to medicine-related problems from the perspectives of adult patients with cardiovascular diseases and diabetes mellitus | Systematic review | To explore and evaluate contributory factors leading to MRPs among adult patients with CVDs and/or DM from their perspectives | Outpatients with diabetes or cardiovascular diseases | DM and cardiovascular disease | 12 countries: Australia, Brazil, Cameroon, Canada, Croatia, Ireland, Malaysia, South Africa, Spain, Taiwan, the UK, and the USA |
| Ali et al., 2019 | Qualitative Analysis of Factors Influencing Patient Persistence and Adherence to Prescribed Overactive Bladder Medication in UK Primary Care | Individual interviews | Non-Adherence has a major impact on health outcomes in long term diseases. | Primary care in the UK | Overactive bladder | UK |
| Alodhaib et al., 2021 | Qualitative Exploration of Barriers to Medication Adherence Among Patients with Uncontrolled Diabetes in Saudi Arabia | Individual interviews | Physicians can rarely identify non-adherent patients | Patients at a diabetes centre in Saudi-Arabia | DM | Saudi-Arabia |
| Alhomoud et al., 2015 | South Asian, and Middle Eastern patients’ perspectives on medicine-related problems in the United Kingdom | Individual interviews | Medication adherence | Outpatients in community pharmacies in London (n = 94) | Not mentioned (patients in general) | UK |
| Axelsson et al., 2015 | Antiretroviral therapy adherence strategies used by patients of a large HIV clinic in Lesotho | Individual interviews | Adherence to ART (outpatients) | Patients receiving ART in their monthly clinical visit | HIV/AIDS | Lesotho |
| Barasa Masaba et al., 2020 | Determinants of Non-Adherence to Treatment Among Patients with Type 2 Diabetes in Kenya: A Systematic Review. (00Review) | Systematic review | Diabetes is the leading non-communicable disease in Kenya | Health care in Kenya | DM2 | Kenya |
| Becker et al., 2020 | Individual, household, and community level barriers to ART adherence among women in rural Eswatini | Focus group | Barriers to ART among woman living with HIV in communities | Rural women living with HIV/AIDS | HIV/AIDS | Eswatini, Africa |
| Bezabhe et al., 2014 | Barriers and Facilitators of Adherence to Antiretroviral Drug Therapy and Retention in Care among Adult HIV-Positive Patients: A Qualitative Study from Ethiopia | Individual interviews | Adherence to ART | Outpatients receiving ART in HIV-clinic, problems in medication taking | HIV/AIDS | Ethiopia |
| Bockwold et al., 2017 | Understanding experiences of diabetes medications among African Americans living with type 2 diabetes | Individual interviews | The contributing factors to non-adherence to diabetic medications in AAs | Hospital-based outpatient diabetes clinic in low-income Chicago | DM2 | United States |
| Chen et al., 2014 | Disease acceptance and adherence to imatinib in Taiwanese chronic myeloid leukaemia outpatients | Individual interviews | Adherence to imatinib, a medication for CML | Outpatient clinic in Taiwan | Chronic myeloid leukaemia | Taiwan |
| Clancy et al., 2020 | Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: A qualitative evidence synthesis | Systematic review | Breast cancer patients’ experiences of adherence | Outpatient setting | Breast cancer | Ireland |
| Dehdari et al., 2019 | The determinants of anti-diabetic medication adherence based on the experiences of type 2 diabetes | Individual interviews | Medication adherence as presented by type 2 DM patients and their families | Secondary care outpatient clinic in Iran | DM2 | Iran |
| Eliasson et al., 2011 | Exploring chronic myeloid leukaemia patients’ reasons for not adhering to the oral anticancer drug imatinib as prescribed | Individual interviews | CML outpatients who have been prescribed imatinib | CML outpatients with prescribed imatinib medication | Chronic myeloid leukaemia | United States |
| Evon et al., 2015 | Adherence during Antiviral Treatment Regimens for Chronic Hepatitis C: A Qualitative Study of Patient-Reported Facilitators and Barriers | Individual interviews | HCV patients’ adherence taking HCV medication as prescribed | Outpatients who receive HCV medication | Chronic Hepatitis C | United States |
| Farinha et al., 2017 | Concerns of patients with systemic lupus erythematosus and adherence to therapy—a qualitative study | Individual interviews | SLE outpatients thoughts and concerns about their illness and medication management | Outpatient clinics | Systemic lupus erythematosus | Portugal |
| Frech et al., 2021 | Patterns and facilitators for the promotion of glaucoma medication adherence-a qualitative study | Individual interviews | Better understanding of patient patterns in glaucoma medication management | Department of Ophthalmology in Germany | Glaucoma | Germany |
| Garavalia et al., 2009 | Exploring Patients’ Reasons for Discontinuance of Heart Medications | Individual interviews | To understand patients’ viewpoints on why they stopped taking their medication | MI outpatients who have stopped to take their prescribed medication (clopidogrel or cholesterol lowering medication) | Cardiovascular disease | United States |
| Garavalia et al., 2011 | Clinician-Patient Discord: Exploring Differences in Perspectives for Discontinuing Clopidogrel | Individual interviews | Why MI outpatients stop to take clopidogrel | Outpatients setting | Cardiovascular disease | United States |
| Gassmann et al., 2016 | Experiences and coping strategies of oncology patients undergoing oral chemotherapy: First steps of a grounded theory study | Individual interviews | Patients’ thoughts about their oral chemotherapy management | Outpatients receiving oral chemotherapy | Oncology patients | Switzerland |
| Goldsmith et al., 2017 | Understanding the patient experience of cost-related non-adherence to prescription medications through typology development and application | Individual interviews | In which situation patients make the decision not to purchase medicines | Outpatients who have not taken their drugs as prescribed because of cost-related problems | Patients who have experiences cost-related-non-adherence | Canada |
| Habte et al., 2017 | Barriers and facilitators to adherence to anti-diabetic medications: Ethiopian patients’ perspectives | Individual interviews | Patients’ anti-diabetic medication-taking experiences | Diabetes 2 patients in public outpatient clinics | DM2 | Ethiopia |
| Harrold et al., 2010 | Patients and providers view gout differently: a qualitative study | Individual interviews | Gout patients views to ULD (urate lowering drugs) | Gout patients’ adherence to long-term urate lowering medication | Gout | United States |
| Hayden et al., 2015 | Patients’ adherence-related beliefs about methotrexate: a qualitative study of the role of written patient information | Individual interviews | How patients’ beliefs and concerns about methotrexate affected their medicine taking | Patients’ decisions about taking methotrexate in outpatients setting | Inflammatory arthritis | UK |
| Hedenrud et al., 2019 | “I did not know it was so important to take it the whole time”—self-reported barriers to medical treatment among individuals with asthma | Individual interviews | Explore self-perceived barriers to medication adherence | Outpatient setting | Asthma | Sweden |
| Ho et al., 2017 | Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: A qualitative study | Individual interviews | Patients’ non-adherence in depression medication | Psychiatric clinic in government-run hospital in Malaysia | Depression | Malaysia |
| Hogan et al., 2014 | Factors affecting nebulised medicine adherence in adult patients with cystic fibrosis: a qualitative study | Individual interviews | Barriers and facilitators of nebulised medicines used for cystic fibrosis | Patients recruited through a patient organisation | Cystic fibrosis | Australia |
| Holtzman et al., 2015 | Mapping patient-identified barriers and facilitators to retention in HIV care and antiretroviral therapy adherence to Andersen’s behavioural model | Individual interviews | HIV medication adherence linked to ABM model | HIV clinics in Philadelphia, USA | HIV/AIDS | United States |
| Huang et al., 2020 | “Why Am I Not Taking Medications?” Barriers and Facilitators of Diabetes Medication Adherence Across Different Health Literacy Levels | Individual interviews | To explore patients’ perceptions of the barriers to and facilitators of medication adherence across different levels of health literacy | how individuals make decisions within an actual real-world situation | DM2 | United States |
| Iacorossi et al., 2019 | Qualitative study of patients with metastatic prostate cancer to adherence of hormone therapy | Individual interviews | Adherence to oral hormone treatment | Outpatient setting | Cancer | Italy |
| Jaffray et al., 2014 | Why do patients discontinue antidepressant therapy early? A qualitative study | Individual interviews | Factors that hinder or facilitate the continuation of AD therapy | Patients treated in general practice in Scotland | Depression | UK |
| Jarab et al., 2018 | A focus group study of patient’s perspective and experiences of type 2 diabetes and its management in Jordan | Focus group | Non-adherence to medication as major barrier to achieve good results in diabetes care | Hospital outpatients in Jordan | DM2 | Jordan |
| Jeragh-Alhaddad et al., 2015 | Barriers to medication taking among Kuwaiti patients with type 2 diabetes: A qualitative study | Individual interviews | Non-adherence to medication remains an unresolved problem | Type 2 DM patients from general practice and hospitals | DM2 | Kuwait |
| Ju et al., 2018 | Patient beliefs and attitudes to taking statins: Systematic review of qualitative studies | Systematic review | Patients’ perspective on statins in primary or secondary prevention of CVD | Systematic review on qualitative studies on patients with statins | Cardiovascular disease | Australia |
| Kassavou et al., 2017 | Reasons for non-adherence to cardiometabolic medications, and acceptability of an interactive voice response intervention in patients with hypertension and type 2 diabetes in primary care: a qualitative study | Individual interviews | Patients’ non-adherence to cardio metabolic medications | General practice patients in the UK | DM2 and/or hypertension | UK |
| Kelly et al., 2014 | Knowledge, attitudes, and beliefs of patients and carersregarding medication adherence: a review of qualitative literature | Systematic review | Systematic qualitative review on factors which can affect medication adherence | Outpatients setting | Not mentioned (patients in general) | Ireland |
| Kelly et al., 2018 | Patients’ Attitudes and Experiences of Disease-Modifying Antirheumatic Drugs in Rheumatoid Arthritis and Spondylarthritis: A Qualitative Synthesis | Systematic review | Non-adherence to antirheumatic drugs | Qualitative studies on adherence to RA drugs | Rheumatoid arthritis and spondylarthritis | Australia |
| King-Shier et al., 2017 | Ethno-Cultural Considerations in Cardiac Patients’ Medication Adherence | Individual interviews | How patients manage to take their cardiac medication | Outpatient setting | Cardiovascular disease | Canada |
| Kobue et al., 2017 | “It’s so hard taking pills when you don’t know what they’re for”: a qualitative study of patients’ medicine taking behaviours and conceptualisation of medicines in the context of rheumatoid arthritis | Individual interviews | To understand RA patients medicine taking behaviour | Patients with Rheumatoid Arthritis (RA) living in South Africa | Rheumatoid arthritis | South Africa |
| Koh et al., 2018 | Access and adherence to medications for the primary and secondary prevention of atherosclerotic cardiovascular disease in Singapore: a qualitative study | Individual interviews | To understand factors influencing patients’ adherence to treatment | Factors impacting on adherence with cardiovascular patients | Cardiovascular disease | Singapore |
| Kucukarslan et al., 2012 | Exploring patient experiences with prescription medicines to identify unmet patient needs: Implications for research and practice | Focus group | Patients’ unmet needs when taking prescribed medicines | Outpatients in the US | Cardiovascular disease | United States |
| Lambert-Kerzner et al., 2015 | Perspectives of patients on factors relating to adherence to post-acute coronary syndrome medical regimens | Individual interviews | Adherence to cardio protective medications after acute coronary syndrome | Patients attending an RCT on multi-faceted intervention to improve cardiac medication adherence | Cardiovascular disease | United States |
| Lyimo et al., 2012 | Determinants of antiretroviral therapy adherence in northern Tanzania: a comprehensive picture from the patient perspective | Individual interviews | Understanding of barriers and facilitators of antiretroviral therapy | Health centres in Tanzania | HIV/AIDS | Tanzania |
| Maffoni et al., 2020 | Medication adherence in the older adults with chronic multimorbidity: a systematic review of qualitative studies on patient’s experience. [Review] | Systematic review | Older patient’s perspective on medication adherence | medication adherence in chronic diseases | Other: hypertension, heart disease, COPD, asthma | Italy, Portugal, and Poland |
| Marshall et al., 2012 | Lay perspectives on hypertension and drug adherence: systematic review of qualitative research | Systematic review | To better understand patients’ perspectives to medication adherence | Qualitative studies on patients using antihypertensive drugs | Cardiovascular disease | UK |
| McDonald et al., 2019 | A theory-driven qualitative study exploring issues relating to adherence to topical glaucoma medications | Individual interviews | Investigating patients’ perceptions of their illness | Two outpatient glaucoma clinics | Glaucoma | UK |
| McKillop et al., 2013 | Patients’ experience and perceptions of polypharmacy in chronic kidney disease and its impact on adherent behaviour | Individual interviews | Polypharmacy is common in chronic kidney disease and associated with medication adherence | Patients at a nephrology clinic | Chronic kidney disease | UK |
| McSharry et al., 2016 | Systematic Review or Meta-analysis Perceptions and experiences of taking oral medications for the treatment of Type 2 diabetes mellitus: a systematic review and meta-synthesis of qualitative studies | Systematic review | DM2 patients’ adherence to diabetes medicines | Outpatients setting | DM2 | UK |
| Meraz et al., 2020 | Medication Non-adherence or Self-care? Understanding the Medication Decision-Making Process and Experiences of Older Adults With Heart Failure | Individual interviews | Understanding the medicine decision-making process | Community setting | Cardiovascular disease | United States |
| Miller et al., 2010 | Why are antiretroviral treatment patients lost to follow-up? A qualitative study from South Africa | Individual interviews | Reasons for non-adherence | HIV/AIDS patients receiving ART | HIV/AIDS | South Africa |
| Ming et al., 2011 | Perspectives of heart failure patients in Malaysia towards medications and disease state management: Findings from a qualitative study | Individual interviews | Patient perspectives in the management of heart failure | General hospital, Malaysia | Cardiovascular disease | Malaysia |
| Mostafavi et al., 2021 | The psychosocial barriers to medication adherence of patients with type 2 diabetes: a qualitative study | Individual interviews | Barriers to medication adherence | Outpatient setting | DM2 | Iran |
| Muiruri et al., 2020 | Why do people living with HIV adhere to antiretroviral therapy and not comorbid cardiovascular disease medications? A qualitative inquiry | Focus groups and individual interviews | HIV-patients adherence to cardiovascular medications | Outpatient setting | Cardiovascular disease | United States |
| Nielsen et al., 2018 | Adherence to medication in patients with chronic kidney disease: a systematic review of qualitative research | Systematic review | Non-adherence to multipharmacological treatment | Nephrology unit in Denmark | Chronic kidney disease | Denmark |
| Oshotse et al., 2018 | Self-Efficacy and Adherence Behaviours in Rheumatoid Arthritis Patients | Other: Focus group and individual interviews | How self-efficacy and adherence is influencing medication taking | RA patients’ self-management | Rheumatoid arthritis | United States |
| Pagès-Puigdemont et al., 2016 | Patients’ Perspective of Medication Adherence in Chronic Conditions: A Qualitative Study | Focus group | Medication adherence in chronic conditions | Patents’ perspectives in medication management in chronic diseases | Chronic diseases | Spain |
| Patel et al., 2015 | Concerns and perceptions about necessity in relation to insulin therapy in an ethnically diverse UK population with type 2 diabetes: a qualitative study focusing mainly on people of South Asian origin | Individual interviews | Accepting insulin as medication to DM2 | Ethnic population living in UK with DM2 and their adherence to insulin | DM2 | UK |
| Peláez et al., 2016 | How can adherence to asthma medication been enhanced? Triangulation of key asthma stakeholders’ perspectives | Focus group | Asthma patients’ adherence to medications | To explore interventions which enhances adherence to asthma medication in long-term | Asthma | Canada |
| Pettersen et al., 2018 | Challenges adhering to a medication regimen following first-time percutaneous coronary intervention: A patient perspective | Individual interviews | Adherence to cardiovascular medication after percutaneous coronary intervention | Cardiology unit in Norway | Cardiovascular disease | Norway |
| Polinski et al., 2014 | A matter of trust: patient barriers to primary medication adherence | Focus group | Patients’ adherence to antihypertensive medications remains suboptimal | Patients who did not pick up the first antihypertensive prescription | Cardiovascular disease | United States |
| Rahmawati et al., 2018 | Understanding untreated hypertension from patients’ point of view: A qualitative study in rural Yogyakarta province, Indonesia | Individual interviews | To explore perspectives from patients who do not take anti-hypertensive medications | Cardiovascular disease | Indonesia | |
| Rashid et al., 2014 | Medication taking in coronary artery disease: A systematic review and qualitative synthesis | Systematic review | Patients’ discontinuation to secondary prevention medication for coronary artery disease | Qualitative research about the medication-taking experiences | Cardiovascular disease | UK |
| Rathbone et al., 2017 | A systematic review and thematic synthesis of patients’ experience of medicines adherence | Systematic review | Phenomenology has a place in studying adherence | Phenomenological papers studying medication adherence | Cardiovascular disease | UK |
| Rezaei et al., 2019 | Barriers of medication adherence in patients with type-2 diabetes: A pilot qualitative study | Individual interviews | Patients with type 2 diabetes have poor adherence to the therapeutic regime | Outpatient setting | DM2 | Iran |
| Richardson et al., 2016 | A joint effort over a period of time: Factors affecting use of urate-lowering therapy for long-Term treatment of gout | Individual interviews | Reasons for non-adherence to gout treatment | GP patients through the UK | Gout | UK |
| Rifkin et al., 2010 | Medication adherence behaviour and priorities among older adults with CKD: A semistructured interview study | Individual interviews | How patients with multiple problems in kidney disease prioritise their medications | Community-dwelling patients with kidney disease | Chronic kidney disease | United States |
| Rowell-Cunsolo et al., 2020 | Barriers to optimal antiretroviral therapy adherence among HIV-infected formerly incarcerated individuals in New York City | Individual interviews | Investigate barriers to ART | Outpatient setting | HIV/AIDS | United States |
| Saleem et al., 2012 | Drug attitude and adherence: A qualitative insight of patients with hypertension | Individual interviews | Patients’ insight to hypertension medication | Outpatient setting | Cardiovascular disease | Pakistan |
| Sapkota et al., 2018 | Nepalese patients’ anti-diabetic medication taking behaviour: an exploratory study | Individual interviews | Diabetes causes a huge burden for low- and middle-income countries | Nepalese type 2 DM patients in Nepal and Australia | DM2 | Nepal and Australia |
| Schatz et al., 2019 | “For us here, we remind ourselves”: strategies and barriers to ART access and adherence among older Ugandans | Individual interviews | Antiretroviral therapy among older Africans | Older adults in Uganda with HIV | HIV/AIDS | Uganda |
| Shalihu et al., 2014 | Namibian prisoners describe barriers to HIV antiretroviral therapy adherence | Individual interviews | Adherence to HIV medication | Patients with AIDS in a Namibian prison | HIV/AIDS | Namibia |
| Shaw et al., 2018 | Rheumatoid arthritis patients’ motivations for accepting or resisting disease-modifying antirheumatic drug treatment regimens | Individual interviews | Patients’ decision to accept or resist disease modifying anti rheumatic drugs | Four rheumatology clinics in Pittsburgh | Rheumatoid arthritis | United States |
| Shiyanbola et al., 2018 | “I did not want to take that medicine”: African-Americans’ reasons for diabetes medication non-adherence and perceived solutions for enhancing adherence | Focus group | Diabetes is disproportionally burdensome among African-Americans (AAs) and medication adherence is important for optimal outcomes. | Community African American type 2 DM patients | DM2 | United States |
| Souter et al., 2014 | Optimisation of secondary prevention of stroke: A qualitative study of stroke patients’ beliefs, concerns and difficulties with their medicines | Individual interviews | Optimisation of secondary prevention of stroke | Patients discharged from stroke rehabilitation | Cardiovascular disease | UK |
| Srimongkon et al., 2018 | Consumer-related factors influencing antidepressant adherence in unipolar depression: a qualitative study | Individual interviews | Adherence at different stages: initiation, implementation, and discontinuation of medication | Outpatient setting | Depression | Australia |
| Stern et al., 2017 | Conceptions of agency and constraint for HIV-positive patients and healthcare workers to support long-term engagement with antiretroviral therapy care in Khayelitsha, South Africa | Individual interviews | Barriers to long-term ART adherence is critical in HIV management | Three HIV clinics in South Africa | HIV/AIDS | South Africa |
| Stryker et al., 2010 | An Exploratory Study of Factors Influencing Glaucoma Treatment Adherence | Individual interviews | Patient adherence to glaucoma treatment regimens is often suboptimal | Veteran Affairs hospital in US | Glaucoma | United States |
| Tong et al., 2011 | The perspectives of kidney transplant recipients on medicine taking: A systematic review of qualitative studies | Systematic review | Non-adherence to medication regimens after kidney transplantation | Qualitative studies using interviews, focus groups, document analysis or observations to explore the perspectives of adult kidney transplant recipients | Kidney transplants | Australia |
| Tordoff et al, 2010 | ‘‘It’s just routine.’’ A qualitative study of medicine-taking amongst older people in New Zealand | Individual interviews | Many older people use large numbers of medicines and are more likely to have problems taking them | Community patients in New Zealand | Not mentioned (patients in general) | New Zealand |
| Tranulis et al., 2011 | Becoming adherent to antipsychotics: a qualitative study of treatment-experienced schizophrenia patients | Individual interviews | Patients’ perspectives on the discontinuation of antipsychotics | Community mental health centre outpatient clinic | Schizophrenia | United States |
| Vaanholt et al., 2018 | Perceived advantages and disadvantages of oral anticoagulants, and the trade-offs patients make in choosing anticoagulant therapy and adhering to their drug regimen | Focus group | Adherence to oral anticoagulants | AF patients in different European countries | Cardiovascular disease | Netherland |
| Van Geffen et al., 2011 | The decision to continue or discontinue treatment: Experiences and beliefs of users of selective serotonin-reuptake inhibitors in the initial months—A qualitative study | Individual interviews | To identify what reasons lead to discontinuation or continuation of treatment | Depression patients in community pharmacies 3 months after starting SSRI treatment | Depression | Netherland |
| Van Tam et al., 2011 | “It is not that I forget, it’s just that I don’t want other people to know”: barriers to and strategies for adherence to antiretroviral therapy among HIV patients in Northern Vietnam | Focus group | Little is known about factors influencing ART adherence among people living with HIV | HIV patients in Vietnam | HIV/AIDS | Vietnam |
| VanLoggerenberg et al., 2015 | A Qualitative Study of Patient Motivation to Adhere to Combination Antiretroviral Therapy in South Africa | Other: Individual interviews and focus groups | Adherence to ART | Patients receiving ART medication at the clinic | HIV/AIDS | South Africa |
| Verbrugghe et al., 2016 | Factors influencing adherence in cancer patients taking oral tyrosine kinase inhibitors | Individual interviews | Non-adherence in cancer patients taking oral anticancer drugs is common | Five hospitals in Belgium | Cancer | Belgium |
| Vipey et al., 2021 | A qualitative study of barriers and facilitators to adherence to secondary prevention medications among French patients suffering from stroke and transient ischemic attack | Individual interviews | TIA patients do not adhere to their secondary prevention medicines | Cohort of TIA patients in France | Cardiovascular disease | France |
| Widayanti et al., 2020 | Medicine taking behaviours of people with type 2 diabetes in Indonesia: a qualitative study | Focus group | Rural and urban communities | People’s medicine-taking behaviours | DM | Indonesia |
| Wu et al., 2015 | Lack of congruence between patients’ and health professionals’ perspectives of adherence to imatinib therapy in treatment of chronic myeloid leukaemia: A qualitative study | Individual interviews | Consistent use of imatinib is critical for treatment success in chronic myeloid leukaemia | Patients in specialised cancer centres (health professionals too) | Chronic myeloid leukaemia | Australia |
| Ågärd et al., 2016 | Diabetes in the shadow of daily life: factors that make diabetes a marginal problem | Individual interviews | Diabetic patients’ challenges in following treatment recommendations | Medical outpatient clinic in Sweden | DM2 | Sweden |
Appendix C
| Study | Title | Country in Which the Study Conducted | Aim of Study | Study Design | Data Sources | Results According to the Research Articles | Population Description | Total Number of Participants |
|---|---|---|---|---|---|---|---|---|
| Al Hamid et al., 2014 | A systematic review of qualitative research on the contributory factors leading to medicine-related problems from the perspectives of adult patients with cardiovascular diseases and diabetes mellitus | 12 countries: Australia, Brazil, Cameroon, Canada, Croatia, Ireland, Malaysia, South Africa, Spain, Taiwan, the UK and the USA | To explore and evaluate contributory factors leading to MRPs among adult patients with CVDs and/or DM from their perspectives. | Systematic review | Pubmed, EMBASE, ISIWeb of Knowledge, PsycInfo, International Pharmaceutical Abstract and PsycExtra | Patient-related factors including socioeconomic factors (beliefs, feeling victimised, history of the condition, lack of finance, lack of motivation, and low self-esteem) and lifestyle factors (diet, lack of exercise/time to see the doctor, obesity, smoking, and stress), medicine-related factors (belief in natural remedies, fear of medicine, lack of belief in medicines, lack of knowledge, non- adherence, and polypharmacy) and condition-related factors (lack of knowledge/understanding, fear of condition and its complications, and lack of control). | Adult patients with cardiovascular disease and/or diabetes | 836 (21 studies) |
| Barasa Masaba et al., 2020 | Determinants of Non-Adherence to Treatment Among Patients with Type 2 Diabetes in Kenya: A Systematic Review. [Review] | Kenya | What are the determinants that contribute to non-adherence to treatment among patients with T2DM in Kenya | Systematic review | Scopus, Web of Science, Science Direct, Cochrane Library, PUBMED, OVID and Google Scholar. | (1) Cost—income, insurance, distance, bills of drugs and food; (2) Patient characteristics—perception of (efficacy, severity, effects of non-adherence), knowledge, co-morbidity, family support, self-unfounded beliefs; and (3) Health system—health education, multiple drugs, evaluations and support, guidelines, and poor perception of system. | Adult patients with type 2 diabetes | 15 studies |
| Clancy et al., 2020 | Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: A qualitative evidence synthesis | Ireland | To synthesise breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy. | Systematic review | Embase, Cinahl, Pubmed, Psychinfo, Proquest, Lenus, Scopus, Web of Science, Rian.ie, EThOS e-theses online, DART Europe. No year limit was set | Three analytic themes were identified (We do not have an option; the side effects are worse than the disease; help us with information and support). Non-adherence and non-persistence were associated with debilitating side effects, inadequate information, and lack of support. | Breast cancer patients | 42 studies |
| Ju et al., 2018 | Patient beliefs and attitudes to taking statins: Systematic review of qualitative studies | Australia | To describe patients’ perspectives, experience, and attitudes towards statins | Systematic review | PsycINFO, CINAHL, Embase, MEDLINE, and PhD dissertations from inception to 6 October 2016 | Confidence in prevention (trust in efficacy, minimising long-term catastrophic CVD, taking control, easing anxiety about high cholesterol); routinising into daily life; questioning utility (imperceptible benefits, uncertainties about pharmacological mechanisms); medical distrust (scepticism about overprescribing, pressure to start therapy); threatening health (competing priorities and risks, debilitating side effects, toxicity to body); signifying sickness (fear of perpetual dependence, losing the battle); and financial strain. | cardiovascular patients using statins in different countries | 888 (32 studies) |
| Kelly et al., 2014 | Knowledge, attitudes, and beliefs of patients and carers regarding medication adherence: a review of qualitative literature | Ireland | Knowledge, attitudes, and beliefs of patients and carers regarding medication adherence | Systematic review | CINAHL, Embase, PubMed, and Web of Knowledge from inception to November 2013. | Eight themes were identified: (1) beliefs and experiences of medicines, (2) family support and culture, (3) role of and relationship with healthcare practitioners, (4) factors related to the disease, (5) self-regulation, (6) communication, (7) cost, and (8) access. | Users of medicines (not mentioned, patients in general) | 34 studies |
| Kelly et al., 2018 | Patients’ Attitudes and Experiences of Disease-Modifying Antirheumatic Drugs in Rheumatoid Arthritis and Spondylarthritis: A Qualitative Synthesis | Australia | To describe patients’ attitudes and experiences of DMARDS in RA and spondylarthritis | Systematic review | MEDLINE, Embase, PsycINFO, and CINAHL were searched to January 2016 | Six themes were identifyed with subthemes: intensifying disease identity (severity of sudden pharmacotherapy, signifying deteriorating health, daunting lifelong therapy), distressing uncertainties and consequences (poisoning the body, doubting efficacy, conflicting and confusing advice, prognostic uncertainty with changing treatment regimens), powerful social influences (swayed by others’ experiences, partnering with physicians, maintaining roles, confidence in comprehensive and ongoing care, valuing peer support), privilege and right of access to biologic agents (expensive medications must be better, right to receive a biologic agent, fearing dispossession), maintaining control (complete ownership of decision, taking extreme risks, minimizing life- style intrusion), and negotiating treatment expectations (miraculous recovery, mediocre benefit, reaching the end of the line). | Adults (ages ≥18 years) with rheumatoid arthritis or spondylarthritis | 1383 (56 studies) |
| Maffoni et al., 2020 | Medication adherence in the older adults with chronic multimorbidity: a systematic review of qualitative studies on patient’s experience | Italy, Portugal, Poland | To investigate potential factors associated with medication adherence in the older and chronic population through a PRISMA systematic review of qualitative studies on patients’ experience. | Systematic review | Scopus and Pubmed from 2000 to October 2017 | According to the ABC Taxonomy, Persistence and Implementation were the most often considered phases. Considering the Three Factor model, the most often reported themes were Information and Strategies upon being adherent. The patient’s decisional flowchart describing barriers and facilitators (personal, social and environmental) to adherence was proposed. | Older adults aged 65 or more | 39 studies |
| Marshall et al., 2012 | Lay perspectives on hypertension and drug adherence: systematic review of qualitative research | UK | To examine lay understanding of hypertension and perspectives on drug taking | Systematic review | Medline, Embase, the British Nursing Index, Social Policy and Practice, and PsycInfo from inception to October 2011 | A large proportion of participants thought hypertension was principally caused by stress and produced symptoms, particularly headache, dizziness, and sweating. Participants widely intentionally reduced or stopped treatment without consulting their doctor, commonly perceived that their blood pressure improved when symptoms abated or when they were not stressed, and that treatment was not needed at these times. Participants disliked treatment and its side effects and feared addiction. Participants reported various external factors that prevented adherence: being unable to find time to take the drugs or to see the doctor; having insufficient money to pay for treatment; the cost of appointments and healthy food; a lack of health insurance; and forgetfulness. | A global population with cardiovascular disease | 53 qualitative studies |
| McSharry et al., 2016 | Systematic Review or Meta-analysis Perceptions and experiences of taking oral medications for the treatment of Type 2 diabetes mellitus: a systematic review and meta-synthesis of qualitative studies | UK | To explore patients’ perceptions and experiences of taking oral medications for the pharmacological management of Type 2 diabetes by carrying out a systematic review and qualitative meta-synthesis of published qualitative studies | Systematic review | Cinahl, EMBASE, Medline, and PsycINFO databases were searched in 2014 | Medications for diabetes: a necessary evil, outlines how patients’ negative perceptions of medication risks co-exist with a resounding view that medications are beneficial. Passive patients but active experimenters highlights the contrast between patients’ passive acceptance of medication prescriptions and the urge to actively experiment and adjust doses to optimize medication use in daily life. Finally, Taking oral medication for Type 2 diabetes: a unique context describes features specific to the Type 2 diabetes medication experience, including lack of symptoms and the perceived relationship between medication and diet, which may influence adherence. | Diabetes type 2 patients taking oral medication | 8 studies |
| Nielsen et al., 2018 | Adherence to medication in patients with chronic kidney disease: a systematic review of qualitative research | Denmark | To synthesize findings from qualitative studies of patients’ experiences of factors that facilitate and hinder adherence to medication. | Systematic review | MEDLINE, Embase, and CINAHL | Three analytical themes with the subthemes; (1) logistics (establishing and maintaining routines, and the costs of buying medication), (2) benchmarking the need for medication (absence of effect from a lay perspective, lacking understanding of medication indications and effects and being spurred by emergent symptoms) and (3) the quality of the patient- physician relationship (eliciting patients’ wishes for involvement in decisions concerning medication and lacking information). | Adult patients with chronic kidney disease | 381 (19 studies) |
| Rashid et al., 2014 | Medication taking in coronary artery disease: A systematic review and qualitative synthesis | UK | To understand from a patient perspective the factors that promote medication persistence. | Systematic review | MEDLINE, Embase, Psy- cINFO, SCOPUS, CINAHL, ASSIA, and SSCI | Some patients hold fatalistic beliefs about their disease, whereas others believe they have been cured by interventions; both can lead to failure to take medication. Patients who adapt to being a “heart patient” are positive about medication taking. Some individuals dislike taking tablets generally and are wary of long-term effects. Relationships with prescribing clinicians are of critical importance for patients, with inaccessibility and insensitive terminology negatively affecting patients’ perceptions about treatments. | Adult patients with cardiovascular disease | 391 (17 studies) |
| Rathbone et al., 2017 | A systematic review and thematic synthesis of patients’ experience of medicines adherence | UK | To explore patients’ lived experiences of medicines adherence reported in the phenomenological literature, through systematic review and thematic synthesis | Systematic review | CINAHL, PsychInfo, Web of Science, Sociological Abstracts, MEDLINE | Descriptive themes identified included (1) dislike for medicines, (2) survival, (3) perceived need, including (a) symptoms and side-effects and (b) cost, and (4) routine. Analytic themes identified were (1) identity and (2) interaction. | Adult patients with cardiovascular disease | 463 (22 studies) |
| Tong et al., 2011 | The perspectives of kidney transplant recipients on medicine taking: A systematic review of qualitative studies | Australia | To summarise and synthesise published qualitative studies on the experiences, perspectives, beliefs and attitudes of kidney transplant recipients on medicine taking. | Systematic review | Medline, PsycINFO, EMBASE, Cochrane Database from inception until Week 3 of January 2010 | (1) attitudes towards medicine taking, its impact on lifestyle, self-image, relationships and outlook on life; (2) inadvertent forgetfulness, preoccupation with life commitments; (3) medication properties; (4) structure of healthcare services, poor access to pharmacy or affordable medications and conflicting medical appointments; (5) personal efforts in managing medications, organizing and devising strategies for taking medicines on time; and (6) availability of external social support | Adult patients with kidney transplants | 207 (7 studies) |
References
- Eduardo, S. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Haynes, R.B.; Ackloo, E.; Sahota, N.; McDonald, H.P.; Yao, X. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Amankwaa, I.; Boateng, D.; Quansah, D.Y.; Akuoko, C.P.; Evans, C. Effectiveness of short message services and voice call interventions for antiretroviral therapy adherence and other outcomes: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0204091. [Google Scholar] [CrossRef]
- Rasmussen, J.N.; Chong, A.; Alter, D.A. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA 2007, 297, 177–186. [Google Scholar] [CrossRef]
- Roebuck, M.C.; Liberman, J.N.; Gemmill-Toyama, M.; Brennan, T.A. Medication adherence leads to lower health care use and costs despite increased drug spending. Health Aff. 2011, 30, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuga, A.O.; McGuire, M.J. Adherence and health care costs. Risk Manag. Healthc. Policy 2014, 7, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauler, S.; Jacquin-Courtois, S.; Haesebaert, J.; Luaute, J.; Coudeyre, E.; Feutrier, C.; Allenet, B.; Decullier, E.; Rode, G.; Janoly-Dumenil, A. Barriers and facilitators for medication adherence in stroke patients: A qualitative study conducted in french neurological rehabilitation units. Eur. Neurol. 2014, 72, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.M.; Juhl, M.F.; Feldt-Rasmussen, B.; Thomsen, T. Adherence to medication in patients with chronic kidney disease: A systematic review of qualitative research. Clin. Kidney J. 2018, 11, 513–527. [Google Scholar] [CrossRef] [Green Version]
- Rezaei, M.; Valiee, S.; Tahan, M.; Ebtekar, F.; Gheshlagh, R.G. Barriers of medication adherence in patients with type-2 diabetes: A pilot qualitative study. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, M.A.; Moles, R.J.; Chen, T.F. Medication-related burden and patients’ lived experience with medicine: A systematic review and metasynthesis of qualitative studies. BMJ Open 2016, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, P.A.; Moncada, L.; Defey, D. Understanding Non-Adherence From the Inside: Hypertensive Patients’ Motivations for Adhering and Not Adhering. Qual. Health Res. 2017, 27, 1023–1034. [Google Scholar] [CrossRef]
- Pagès-Puigdemont, N.; Mangues, M.A.; Masip, M.; Gabriele, G.; Fernández-Maldonado, L.; Blancafort, S.; Tuneu, L. Patients’ Perspective of Medication Adherence in Chronic Conditions: A Qualitative Study. Adv. Ther. 2016, 33, 1740–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, J.D.; Fisher, W.A. Changing AIDS-risk behavior. Psychol Bull. 1992, 111, 455–474. [Google Scholar] [CrossRef]
- Yang, C.; Hui, Z.; Zeng, D.; Liu, L.; Lee, D.T.F. Examining and adapting the information-motivation-behavioural skills model of medication adherence among community-dwelling older patients with multimorbidity: Protocol for a cross-sectional study. BMJ Open 2020, 10, e033431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, D.M.; DeVellis, R.F.; Fisher, E.B.; DeVellis, B.M.; Hogan, S.L.; Jordan, J.M. The effect of conflicting medication information and physician support on medication adherence for chronically ill patients. Patient Educ. Couns. 2010, 81, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Implement. 2021, 19, 3–10. [Google Scholar] [CrossRef]
- Al Hamid, A.; Ghaleb, M.; Aljadhey, H.; Aslanpour, Z. A systematic review of qualitative research on the contributory factors leading to medicine-related problems from the perspectives of adult patients with cardiovascular diseases and diabetes mellitus. BMJ Open 2014, 4. [Google Scholar] [CrossRef]
- Ju, A.; Hanson, C.S.; Banks, E.; Korda, R.; Craig, J.C.; Usherwood, T.; MacDonald, P.; Tong, A. Patient beliefs and attitudes to taking statins: Systematic review of qualitative studies. Br. J. Gen. Pract. 2018, 68, e408–e419. [Google Scholar] [CrossRef]
- Marshall, I.J.; Wolfe, C.D.A.; McKevitt, C. Lay perspectives on hypertension and drug adherence: Systematic review of qualitative research. BMJ 2012, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, M.A.; Edwards, D.; Walter, F.M.; Mant, J. Medication taking in coronary artery disease: A systematic review and qualitative synthesis. Ann. Fam. Med. 2014, 12, 224–232. [Google Scholar] [CrossRef] [Green Version]
- Rathbone, A.P.; Todd, A.; Jamie, K.; Bonam, M.; Banks, L.; Husband, A.K. A systematic review and thematic synthesis of patients’ experience of medicines adherence. Res. Soc. Adm. Pharm. 2017, 13, 403–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellack, A.S.; Bowden, C.L.; Bowie, C.R.; Byerly, M.J.; Carpenter, W.T.; Copeland, L.A.; Dassori, A.M.; Davis, J.M.; Depp, C.A.; Diaz, E.; et al. The expert consensus guideline series: Adherence problems in patients with serious and persistent mental illness. J. Clin. Psychiatry 2009, 70, 1–48. [Google Scholar]
- Barasa Masaba, B.; Mmusi-Phetoe, R.M. Determinants of Non-Adherence to Treatment Among Patients with Type 2 Diabetes in Kenya: A Systematic Review. J. Multidiscip. Healthc. 2020, 13, 2069–2076. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.; Tymms, K.; Tunnicliffe, D.J.; Sumpton, D.; Perera, C.; Fallon, K.; Craig, J.C.; Abhayaratna, W.; Tong, A. Patients’ Attitudes and Experiences of Disease-Modifying Antirheumatic Drugs in Rheumatoid Arthritis and Spondyloarthritis: A Qualitative Synthesis. Arthritis Care Res. 2018, 70, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.; Lynch, J.; OConnor, P.; Dowling, M. Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: A qualitative evidence synthesis. Eur. J. Oncol. Nurs. 2020, 44, 101706. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Howell, M.; Wong, G.; Webster, A.C.; Howard, K.; Craig, J.C. The perspectives of kidney transplant recipients on medicine taking: A systematic review of qualitative studies. Nephrol. Dial. Transplant. 2011, 26, 344–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, M.; McCarthy, S.; Sahm, L.J. Knowledge, attitudes and beliefs of patients and carers regarding medication adherence: A review of qualitative literature. Eur. J. Clin. Pharmacol. 2014, 70, 1423–1431. [Google Scholar] [CrossRef]
- Maffoni, M.; Traversoni, S.; Costa, E.; Midao, L.; Kardas, P.; Kurczewska-Michalak, M.; Giardini, A. Medication adherence in the older adults with chronic multimorbidity: A systematic review of qualitative studies on patient’s experience. Eur. Geriatr. Med. 2020, 11, 369–381. [Google Scholar] [CrossRef]
- Holtzman, C.W.; Shea, J.A.; Glanz, K.; Jacobs, L.M.; Gross, R.; Hines, J.; Mounzer, K.; Samuel, R.; Metlay, J.P.; Yehia, B.R. Mapping patient-identified barriers and facilitators to retention in HIV care and antiretroviral therapy adherence to Andersen’s Behavioral Model. AIDS Care Psychol. Socio-Med. Asp. AIDS/HIV 2015, 27, 817–828. [Google Scholar] [CrossRef] [Green Version]
- Schatz, E.; Seeley, J.; Negin, J.; Weiss, H.A.; Tumwekwase, G.; Kabunga, E.; Nalubega, P.; Mugisha, J. “for us here, we remind ourselves”: Strategies and barriers to ART access and adherence among older Ugandans. BMC Public Health 2019, 19. [Google Scholar] [CrossRef]
- Bockwoldt, D.; Staffileno, B.A.; Coke, L.; Hamilton, R.; Fogg, L.; Calvin, D.; Quinn, L. Understanding Experiences of Diabetes Medications Among African Americans Living With Type 2 Diabetes. J. Transcult. Nurs. 2017, 28, 363–371. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.; Ferguson, E.; Hagger, M.S.; Foss, A.J.E.; King, A.J. A theory-driven qualitative study exploring issues relating to adherence to topical glaucoma medications. Patient Prefer. Adherence 2019, 13, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Pettersen, T.R.; Fridlund, B.; Bendz, B.; Nordrehaug, J.E.; Rotevatn, S.; Schjøtt, J.; Norekvål, T.M.; On behalf of the, C.I. Challenges adhering to a medication regimen following first-time percutaneous coronary intervention: A patient perspective. Int. J. Nurs. Stud. 2018, 88, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, N.; Cordeiro, L.S.; Poudel, K.C.; Sibiya, T.E.; Sayer, A.G.; Sibeko, L.N. Individual, household, and community level barriers to ART adherence among women in rural Eswatini. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Lambert-Kerzner, A.; Havranek, E.P.; Plomondon, M.E.; Fagan, K.M.; McCreight, M.S.; Fehling, K.B.; Williams, D.J.; Hamilton, A.B.; Albright, K.; Blatchford, P.J.; et al. Perspectives of patients on factors relating to adherence to post-acute coronary syndrome medical regimens. Patient Prefer. Adherence 2015, 9, 1053–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucukarslan, S.N.; Lewis, N.J.W.; Shimp, L.A.; Gaither, C.A.; Lane, D.C.; Baumer, A.L. Exploring patient experiences with prescription medicines to identify unmet patient needs: Implications for research and practice. Res. Soc. Adm. Pharm. 2012, 8, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.M.; Pecanac, K.E.; Shiyanbola, O.O. “Why Am I Not Taking Medications?” Barriers and Facilitators of Diabetes Medication Adherence Across Different Health Literacy Levels. Qual. Health Res. 2020, 30, 2331–2342. [Google Scholar] [CrossRef]
- Garavalia, L.; Garavalia, B.; Spertus, J.A.; Decker, C. Exploring patients’ reasons for discontinuance of heart medications. J. Cardiovasc. Nurs. 2009, 24, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garavalia, L.; Ho, P.M.; Garavalia, B.; Foody, J.M.; Kruse, H.; Spertus, J.A.; Decker, C. Clinician-patient discord: Exploring differences in perspectives for discontinuing clopidogrel. Eur. J. Cardiovasc. Nurs. 2011, 10, 50–55. [Google Scholar] [CrossRef]
- Oshotse, C.; Zullig, L.L.; Bosworth, H.B.; Tu, P.; Lin, C. Self-efficacy and adherence behaviors in rheumatoid arthritis patients. Prev. Chronic Dis. 2018, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmawati, R.; Bajorek, B. Understanding untreated hypertension from patients’ point of view: A qualitative study in rural Yogyakarta province, Indonesia. Chronic Illn. 2018, 14, 228–240. [Google Scholar] [CrossRef]
- Meraz, R. Medication Nonadherence or Self-care? Understanding the Medication Decision-Making Process and Experiences of Older Adults With Heart Failure. J. Cardiovasc. Nurs. 2020, 35, 26–34. [Google Scholar] [CrossRef]
- Sapkota, S.; Brien, J.A.E.; Aslani, P. Nepalese patients’ anti-diabetic medication taking behaviour: An exploratory study. Ethn. Health 2018, 23, 718–736. [Google Scholar] [CrossRef] [PubMed]
- Evon, D.M.; Golin, C.E.; Bonner, J.E.; Grodensky, C.; Velloza, J. Adherence during antiviral treatment regimens for chronic Hepatitis C. J. Clin. Gastroenterol. 2015, 49, e41–e50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axelsson, J.M.; Hallager, S.; Barfod, T.S. Antiretroviral therapy adherence strategies used by patients of a large HIV clinic in Lesotho. J. Health Popul. Nutr. 2015, 33. [Google Scholar] [CrossRef] [Green Version]
- Al-Qazaz, H.K.; Hassali, M.A.; Shafie, A.A.; Syed Sulaiman, S.A.; Sundram, S. Perception and knowledge of patients with type 2 diabetes in Malaysia about their disease and medication: A qualitative study. Res. Soc. Adm. Pharm. 2011, 7, 180–191. [Google Scholar] [CrossRef]
- Tranulis, C.; Goff, D.; Henderson, D.C.; Freudenreich, O. Becoming adherent to antipsychotics: A qualitative study of treatment-experienced schizophrenia patients. Psychiatr. Serv. 2011, 62, 888–892. [Google Scholar] [CrossRef]
- Ågärd, A.; Ranjbar, V.; Strang, S. Diabetes in the shadow of daily life: Factors that make diabetes a marginal problem. Pract. Diabetes 2016, 33, 49–53. [Google Scholar] [CrossRef]
- Shaw, Y.; Metes, I.D.; Michaud, K.; Donohue, J.M.; Roberts, M.S.; Levesque, M.C.; Chang, J.C. Rheumatoid Arthritis Patients’ Motivations for Accepting or Resisting Disease-Modifying Antirheumatic Drug Treatment Regimens. Arthritis Care Res. 2018, 70, 533–541. [Google Scholar] [CrossRef]
- Stryker, J.E.; Beck, A.D.; Primo, S.A.; Echt, K.V.; Bundy, L.; Pretorius, G.C.; Glanz, K. An exploratory study of factors influencing glaucoma treatment adherence. J. Glaucoma 2010, 19, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.C.; Jacob, S.A.; Tangiisuran, B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: A qualitative study. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowell-Cunsolo, T.L.; Hu, G. Barriers to optimal antiretroviral therapy adherence among HIV-infected formerly incarcerated individuals in New York City. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.J.K.; Cheng, R.X.; Yap, Y.; Haldane, V.; Tan, Y.G.; Teo, K.W.Q.; Srivastava, A.; Ong, P.S.; Perel, P.; Legido-Quigley, H. Access and adherence to medications for the primary and secondary prevention of atherosclerotic cardiovascular disease in singapore: A qualitative study. Patient Prefer. Adherence 2018, 12, 2481–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarab, A.S.; Mukattash, T.L.; Al-Azayzih, A.; Khdour, M. A focus group study of patient’s perspective and experiences of type 2 diabetes and its management in Jordan. Saudi Pharm. J. 2018, 26, 301–305. [Google Scholar] [CrossRef]
- Gassmann, C.; Kolbe, N.; Brenner, A. Experiences and coping strategies of oncology patients undergoing oral chemotherapy: First steps of a grounded theory study. Eur. J. Oncol. Nurs. 2016, 23, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Habte, B.M.; Kebede, T.; Fenta, T.G.; Boon, H. Barriers and facilitators to adherence to anti-diabetic medications: Ethiopian patients’ perspectives. Afr. J. Prim. Health Care Fam. Med. 2017, 9. [Google Scholar] [CrossRef]
- Harrold, L.R.; Mazor, K.M.; Velten, S.; Ockene, I.S.; Yood, R.A. Patients and providers view gout differently: A qualitative study. Chronic Illn. 2010, 6, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Hogan, A.; Bonney, M.A.; Brien, J.A.; Karamy, R.; Aslani, P. Factors affecting nebulised medicine adherence in adult patients with cystic fibrosis: A qualitative study. Int. J. Clin. Pharm. 2014, 37, 86–93. [Google Scholar] [CrossRef]
- Vaanholt, M.C.W.; Weernink, M.G.M.; von Birgelen, C.; Groothuis-Oudshoorn, C.G.M.; MJ, I.J.; van Til, J.A. Perceived advantages and disadvantages of oral anticoagulants, and the trade-offs patients make in choosing anticoagulant therapy and adhering to their drug regimen. Patient Educ. Couns. 2018, 101, 1982–1989. [Google Scholar] [CrossRef] [PubMed]
- King-Shier, K.M.; Singh, S.; Khan, N.A.; LeBlanc, P.; Lowe, J.C.; Mather, C.M.; Chong, E.; Quan, H. Ethno-Cultural Considerations in Cardiac Patients’ Medication Adherence. Clin. Nurs. Res. 2017, 26, 576–591. [Google Scholar] [CrossRef]
- Van Loggerenberg, F.; Gray, D.; Gengiah, S.; Kunene, P.; Gengiah, T.N.; Naidoo, K.; Grant, A.D. A Qualitative Study of Patient Motivation to Adhere to Combination Antiretroviral Therapy in South Africa. AIDS Patient Care STDs 2015, 29, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, C.; Neame, R.; Tarrant, C. Patients’ adherence-related beliefs about methotrexate: A qualitative study of the role of written patient information. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKillop, G.; Joy, J. Patients’ experience and perceptions of polypharmacy in chronic kidney disease and its impact on adherent behaviour. J. Ren. Care 2013, 39, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Kobue, B.; Moch, S.; Watermeyer, J. “it’s so hard taking pills when you don’t know what they’re for”: A qualitative study of patients’ medicine taking behaviours and conceptualisation of medicines in the context of rheumatoid arthritis. BMC Health Serv. Res. 2017, 17. [Google Scholar] [CrossRef] [Green Version]
- Jeragh-Alhaddad, F.B.; Waheedi, M.; Barber, N.D.; Brock, T.P. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: A qualitative study. Patient Prefer. Adherence 2015, 9, 1491–1503. [Google Scholar] [CrossRef] [Green Version]
- Souter, C.; Kinnear, A.; Kinnear, M.; Mead, G. Optimisation of secondary prevention of stroke: A qualitative study of stroke patients’ beliefs, concerns and difficulties with their medicines. Int. J. Pharm. Pract. 2014, 22, 424–432. [Google Scholar] [CrossRef]
- Bezabhe, W.M.; Chalmers, L.; Bereznicki, L.R.; Peterson, G.M.; Bimirew, M.A.; Kassie, D.M. Barriers and facilitators of adherence to antiretroviral drug therapy and retention in care among adult HIV-positive patients: A qualitative study from Ethiopia. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Saleem, F.; Hassali, M.A.; Shafie, A.A.; Atif, M. Drug attitude and adherence: A qualitative insight of patients with hypertension. J. Young Pharm. 2012, 4, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifkin, D.E.; Laws, M.B.; Rao, M.; Balakrishnan, V.S.; Sarnak, M.J.; Wilson, I.B. Medication adherence behavior and priorities among older adults with CKD: A semistructured interview study. Am. J. Kidney Dis. 2010, 56, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Geffen, E.C.; Hermsen, J.H.; Heerdink, E.R.; Egberts, A.C.; Verbeek-Heida, P.M.; van Hulten, R. The decision to continue or discontinue treatment: Experiences and beliefs of users of selective serotonin-reuptake inhibitors in the initial months--a qualitative study. Res. Soc. Adm. Pharm. 2011, 7, 134–150. [Google Scholar] [CrossRef]
- Alhomoud, F.; Dhillon, S.; Aslanpour, Z.; Smith, F. South Asian and Middle Eastern patients’ perspectives on medicine-related problems in the United Kingdom. Int. J. Clin. Pharm. 2015, 37, 607–615. [Google Scholar] [CrossRef]
- Dehdari, L.; Dehdari, T. The determinants of anti-diabetic medication adherence based on the experiences of patients with type 2 diabetes. Arch. Public Health 2019, 77. [Google Scholar] [CrossRef] [Green Version]
- Alodhaib, G.; Alhusaynan, I.; Mirza, A.; Almogbel, Y. Qualitative Exploration of Barriers to Medication Adherence Among Patients with Uncontrolled Diabetes in Saudi Arabia. Pharmacy 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Lyimo, R.A.; De Bruin, M.; Van Den Boogaard, J.; Hospers, H.J.; Van Der Ven, A.; Mushi, D. Determinants of antiretroviral therapy adherence in northern Tanzania: A comprehensive picture from the patient perspective. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.C.; Chen, T.C.; Huang, Y.B.; Chang, C.S. Disease acceptance and adherence to imatinib in Taiwanese chronic myeloid leukaemia outpatients. Int. J. Clin. Pharm. 2014, 36, 120–127. [Google Scholar] [CrossRef] [Green Version]
- Goldsmith, L.J.; Kolhatkar, A.; Popowich, D.; Holbrook, A.M.; Morgan, S.G.; Law, M.R. Understanding the patient experience of cost-related non-adherence to prescription medications through typology development and application. Soc. Sci. Med. 2017, 194, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Ming, L.C.; Hassali, M.A.; Shafie, A.A.; Awaisu, A.; Hadi, M.A.; Al-Haddad, M. Perspectives of heart failure patients in Malaysia towards medications and disease state management: Findings from a qualitative study. J. Public Health 2011, 19, 569–577. [Google Scholar] [CrossRef]
- Peláez, S.; Bacon, S.L.; Lacoste, G.; Lavoie, K.L. How can adherence to asthma medication be enhanced? Triangulation of key asthma stakeholders’ perspectives. J. Asthma 2016, 53, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Jaffray, M.; Cardy, A.H.; Reid, I.C.; Cameron, I.M. Why do patients discontinue antidepressant therapy early? A qualitative study. Eur. J. Gen. Pract. 2014, 20, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, J.C.; Liddle, J.; Mallen, C.D.; Roddy, E.; Hider, S.; Prinjha, S.; Ziebland, S. A joint effort over a period of time: Factors affecting use of urate-lowering therapy for long-Term treatment of gout. BMC Musculoskelet. Disord. 2016, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| Theory | Medication Therapy | Study |
|---|---|---|
| ABC Taxonomy and Three Factor Model | Hypertension, heart disease, COPD, asthma | Maffoni et al., 2020 |
| Andersen’s Behavioural Model | Antiretroviral therapy Antiretroviral therapy | Holtzman et al., 2015 Schatz et al., 2019 |
| Common-Sense Model of Self-Regulation (CSM) | Glaucoma medication | McDonald et al., 2019 |
| Dowell’s Therapeutic Alliance | Cardio-protective medication | Lambert-Kerzner et al., 2015 |
| Dowell’s Therapeutic Alliance Model and Leventhal’s Common-Sense Model | Use of prescription medicines in general | Kucukarslan et al., 2012 |
| Health Belief Model | Heart medication Clopidogrel Rheumatoid arthritis Hypertension | Garavalia et al., 2009 Garavalia et.al., 2011 Oshotse et.al., 2018 Rahmawati et al., 2018 |
| Health Literacy Pathway Model | Diabetes type 2 medication | Huang et al., 2020 |
| Information-Motivation-Behaviour Skills (IMB) Model of Adherence | Chronic hepatitis C therapy | Evon et al., 2015 |
| Naturalistic Decision-making Model | Heart failure | Meraz et.al., 2020 |
| Roy Adaptation Model | Diabetes type 2 medication | Bockwold et al., 2017 |
| Social Ecological Model | Cardiovascular medication Antiretrovial therapy | Petterssen et al., 2018 Becker et al., 2020 |
| Stages of Change Model | Anti-diabetic medication | Sapkota et al., 2018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kvarnström, K.; Westerholm, A.; Airaksinen, M.; Liira, H. Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research. Pharmaceutics 2021, 13, 1100. https://doi.org/10.3390/pharmaceutics13071100
Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research. Pharmaceutics. 2021; 13(7):1100. https://doi.org/10.3390/pharmaceutics13071100
Chicago/Turabian StyleKvarnström, Kirsi, Aleksi Westerholm, Marja Airaksinen, and Helena Liira. 2021. "Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research" Pharmaceutics 13, no. 7: 1100. https://doi.org/10.3390/pharmaceutics13071100