
Intranasal Administration for Pain: Oxytocin and Other Polypeptides

Abstract
:1. Introduction
2. IN Polypeptides Reach the CSF and Brain
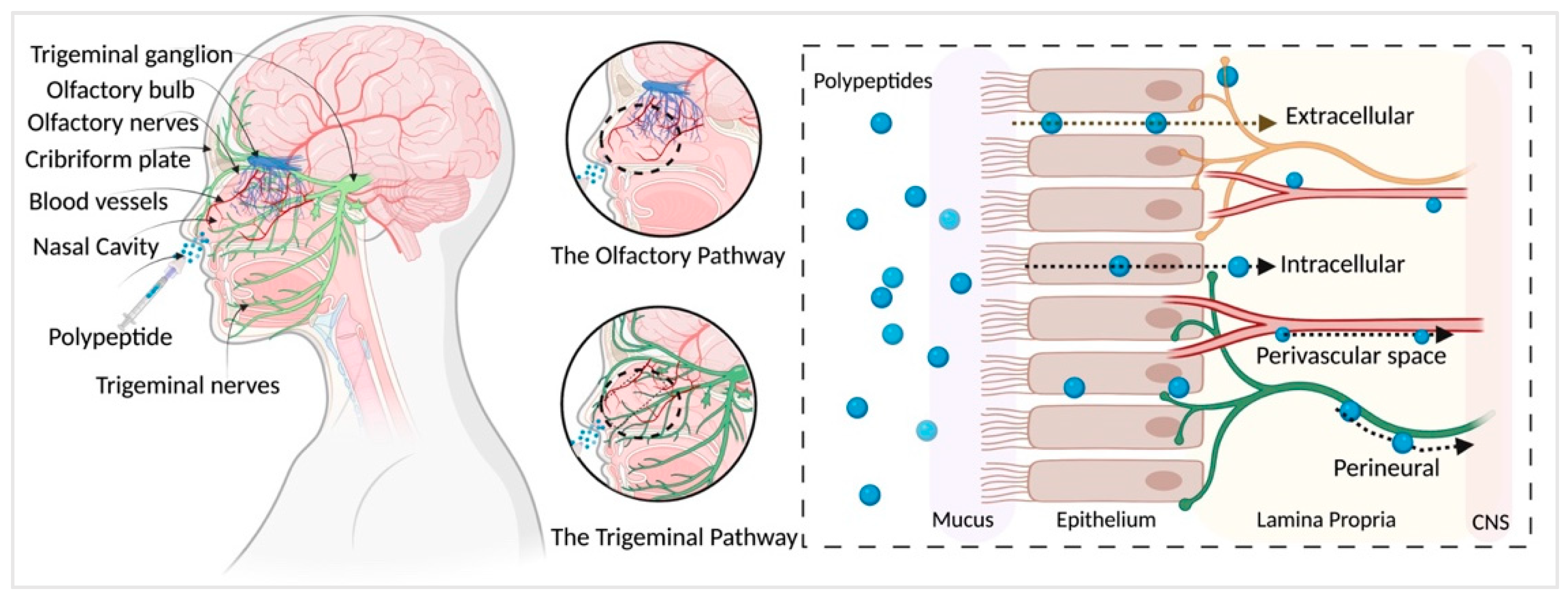
3. Nasal–Cerebral Mechanism
4. Analgesic Effects of Oxytocin
5. Other Polypeptides That Work as Analgesics

{kind=link}
{kind=link}
| Pain Model | Polypeptide | Outcome | References |
|---|---|---|---|
| Chronic pelvic pain | Intranasal oxytocin | Twice-daily administration of oxytocin may represent an adjuvant analgesic for refractory pelvic pain | [57] |
| Thermal pain perception | Intranasal oxytocin | Sex-specific effects of intranasal oxytocin on thermal pain perception, suggesting that oxytocin and endogenous sex hormones may interact to influence noxious stimuli | [61] |
| Migraine | Intranasal oxytocin | Intranasal treatment with oxytocin decreases the frequency of headaches in both chronic and high-frequency episodic migraineurs | [26] |
| Colic pain | Intranasal desmopressin | Complete resolution of colic pain 30 min after IN application of desmopressin in 54% of patients | [63] |
6. Therapeutic Considerations and Delivery Devices
7. Limitations of Intranasal Delivery
8. Future Directions
9. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- van den Pol, A.N. Neuropeptide Transmission in Brain Circuits. Neuron 2012, 76, 98–115. [Google Scholar] [CrossRef] [Green Version]
- Devi, L.A.; Fricker, L.D. Transmitters and Peptides: Basic Principles. In Neuroscience in the 21st Century: From Basic to Clinical; Pfaff, D.W., Volkow, N.D., Eds.; Springer: New York, NY, USA, 2016; pp. 1745–1762. ISBN 978-1-4939-3474-4. [Google Scholar]
- Egleton, R.D.; Davis, T.P. Development of Neuropeptide Drugs That Cross the Blood-Brain Barrier. NeuroRx 2005, 2, 44–53. [Google Scholar] [CrossRef]
- Tiwari, S.K.; Chaturvedi, R.K. Peptide Therapeutics in Neurodegenerative Disorders. Curr. Med. Chem. 2014, 21, 2610–2631. [Google Scholar] [CrossRef]
- Morimoto, B.H. Therapeutic Peptides for CNS Indications: Progress and Challenges. Bioorganic Med. Chem. 2018, 26, 2859–2862. [Google Scholar] [CrossRef] [PubMed]
- Pardridge, W.M. The Blood-Brain Barrier: Bottleneck in Brain Drug Development. Neurotherapeutics 2005, 2, 3–14. [Google Scholar] [CrossRef] [PubMed]
- De Andres, J.; Asensio-Samper, J.M.; Fabregat-Cid, G. Advances in Intrathecal Drug Delivery. Curr. Opin. Anaesthesiol. 2013, 26, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, R.K. Drug Delivery Systems, CNS Protection, and the Blood Brain Barrier. Biomed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Malinowski, M.; Chopra, P.; Varshney, V.; Deer, T.R. Intrathecal Drug Delivery for Pain Management: Recent Advances and Future Developments. Expert Opin. Drug Deliv. 2019, 16, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Dhuria, S.V.; Hanson, L.R.; Frey, W.H. Intranasal Delivery to the Central Nervous System: Mechanisms and Experimental Considerations. J. Pharm. Sci. 2010, 99, 1654–1673. [Google Scholar] [CrossRef]
- Obaidi, M.; Offman, E.; Messina, J.; Carothers, J.; Djupesland, P.G.; Mahmoud, R.A. Improved Pharmacokinetics of Sumatriptan With Breath PoweredTM Nasal Delivery of Sumatriptan Powder. Headache J. Head Face Pain 2013, 53, 1323–1333. [Google Scholar] [CrossRef] [Green Version]
- Quintana, D.S.; Guastella, A.J.; Westlye, L.T.; Andreassen, O.A. The Promise and Pitfalls of Intranasally Administering Psychopharmacological Agents for the Treatment of Psychiatric Disorders. Mol. Psychiatry 2016, 21, 29–38. [Google Scholar] [CrossRef]
- Warnken, Z.N.; Smyth, H.D.C.; Watts, A.B.; Weitman, S.; Kuhn, J.G.; Williams, R.O. Formulation and Device Design to Increase Nose to Brain Drug Delivery. J. Drug Deliv. Sci. Technol. 2016, 35, 213–222. [Google Scholar] [CrossRef]
- Quintana, D.S.; Lischke, A.; Grace, S.; Scheele, D.; Ma, Y.; Becker, B. Advances in the Field of Intranasal Oxytocin Research: Lessons Learned and Future Directions for Clinical Research. Mol. Psychiatry 2021, 26, 80–91. [Google Scholar] [CrossRef]
- Henschke, N.; Kamper, S.J.; Maher, C.G. The Epidemiology and Economic Consequences of Pain. Mayo Clin. Proc. 2015, 90, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Johnson, Q.; Borsheski, R.R.; Reeves-Viets, J.L. A Review of Management of Acute Pain. Mo. Med. 2013, 110, 74–79. [Google Scholar] [PubMed]
- Seal, K.; Becker, W.; Tighe, J.; Li, Y.; Rife, T. Managing Chronic Pain in Primary Care: It Really Does Take a Village. J. Gen. Intern. Med. 2017, 32, 931–934. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic Pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic Pain: A Review of Its Epidemiology and Associated Factors in Population-Based Studies. Br. J. Anaesth 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Martucci, K.T.; Mackey, S.C. Neuroimaging of Pain: Human Evidence and Clinical Relevance of Central Nervous System Processes and Modulation. Anesthesiology 2018, 128, 1241–1254. [Google Scholar] [CrossRef]
- Yang, S.; Chang, M.C. Chronic Pain: Structural and Functional Changes in Brain Structures and Associated Negative Affective States. Int. J. Mol. Sci. 2019, 20, 3130. [Google Scholar] [CrossRef] [Green Version]
- Chichorro, J.G.; Porreca, F.; Sessle, B. Mechanisms of Craniofacial Pain. Cephalalgia 2017, 37, 613–626. [Google Scholar] [CrossRef]
- Kuner, R.; Kuner, T. Cellular Circuits in the Brain and Their Modulation in Acute and Chronic Pain. Physiol. Rev. 2020, 101, 213–258. [Google Scholar] [CrossRef]
- Veinante, P.; Freund-Mercier, M.-J. Distribution of Oxytocin- and Vasopressin-Binding Sites in the Rat Extended Amygdala: A Histoautoradiographic Study. J. Comp. Neurol. 1997, 383, 305–325. [Google Scholar] [CrossRef]
- Tzabazis, A.; Kori, S.; Mechanic, J.; Miller, J.; Pascual, C.; Manering, N.; Carson, D.; Klukinov, M.; Spierings, E.; Jacobs, D.; et al. Oxytocin and Migraine Headache. Headache J. Head Face Pain 2017, 57, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Pisansky, M.T.; Hanson, L.R.; Gottesman, I.I.; Gewirtz, J.C. Oxytocin Enhances Observational Fear in Mice. Nat. Commun. 2017, 8. [Google Scholar] [CrossRef]
- Bowen, M.T. Does Peripherally Administered Oxytocin Enter the Brain? Compelling New Evidence in a Long-Running Debate. Pharm. Res. 2019, 146, 104325. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Shnitko, T.A.; Blue, S.W.; Kaucher, A.V.; Winchell, A.J.; Erikson, D.W.; Grant, K.A.; Leggio, L. Labeled Oxytocin Administered via the Intranasal Route Reaches the Brain in Rhesus Macaques. Nat. Commun. 2020, 11, 2783. [Google Scholar] [CrossRef]
- Lee, M.R.; Scheidweiler, K.B.; Diao, X.X.; Akhlaghi, F.; Cummins, A.; Huestis, M.A.; Leggio, L.; Averbeck, B.B. Oxytocin by Intranasal and Intravenous Routes Reaches the Cerebrospinal Fluid in Rhesus Macaques: Determination Using a Novel Oxytocin Assay. Mol. Psychiatry 2018, 23, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Rault, J.-L. Effects of Positive and Negative Human Contacts and Intranasal Oxytocin on Cerebrospinal Fluid Oxytocin. Psychoneuroendocrinology 2016, 69, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Mens, W.B.J.; Witter, A.; Van Wimersma Greidanus, T.B. Penetration of Neurohypophyseal Hormones from Plasma into Cerebrospinal Fluid (CSF): Half-Times of Disappearance of These Neuropeptides from CSF. Brain Res. 1983, 262, 143–149. [Google Scholar] [CrossRef]
- Tanaka, A.; Furubayashi, T.; Arai, M.; Inoue, D.; Kimura, S.; Kiriyama, A.; Kusamori, K.; Katsumi, H.; Yutani, R.; Sakane, T.; et al. Delivery of Oxytocin to the Brain for the Treatment of Autism Spectrum Disorder by Nasal Application. Mol. Pharm. 2018, 15, 1105–1111. [Google Scholar] [CrossRef]
- Quintana, D.S.; Westlye, L.T.; Alnæs, D.; Rustan, Ø.G.; Kaufmann, T.; Smerud, K.T.; Mahmoud, R.A.; Djupesland, P.G.; Andreassen, O.A. Low Dose Intranasal Oxytocin Delivered with Breath Powered Device Dampens Amygdala Response to Emotional Stimuli: A Peripheral Effect-Controlled within-Subjects Randomized Dose-Response FMRI Trial. Psychoneuroendocrinology 2016, 69, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.A.; Mazibuko, N.; Zelaya, F.; Vasilakopoulou, S.; Loveridge, J.; Oates, A.; Maltezos, S.; Mehta, M.; Wastling, S.; Howard, M.; et al. Effects of Route of Administration on Oxytocin-Induced Changes in Regional Cerebral Blood Flow in Humans. Nat. Commun. 2020, 11, 1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churchland, P.S.; Winkielman, P. Modulating Social Behavior with Oxytocin: How Does It Work? What Does It Mean? Horm. Behav. 2012, 61, 392–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina, G.; Ji, G.; Grégoire, S.; Neugebauer, V. Nasal Application of Neuropeptide S Inhibits Arthritis Pain-Related Behaviors through an Action in the Amygdala. Mol. Pain 2014, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paloyelis, Y.; Krahé, C.; Maltezos, S.; Williams, S.C.; Howard, M.A.; Fotopoulou, A. The Analgesic Effect of Oxytocin in Humans: A Double-Blind, Placebo-Controlled Cross-Over Study Using Laser-Evoked Potentials. J. Neuroendocr. 2016, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lochhead, J.J.; Davis, T.P. Perivascular and Perineural Pathways Involved in Brain Delivery and Distribution of Drugs after Intranasal Administration. Pharmaceutics 2019, 11, 598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anton, F.; Peppel, P. Central Projections of Trigeminal Primary Afferents Innervating the Nasal Mucosa: A Horseradish Peroxidase Study in the Rat. Neuroscience 1991, 41, 617–628. [Google Scholar] [CrossRef]
- Schaefer, M.L.; Böttger, B.; Silver, W.L.; Finger, T.E. Trigeminal Collaterals in the Nasal Epithelium and Olfactory Bulb: A Potential Route for Direct Modulation of Olfactory Information by Trigeminal Stimuli. J. Comp. Neurol. 2002, 444, 221–226. [Google Scholar] [CrossRef]
- Thorne, R.G.; Pronk, G.J.; Padmanabhan, V.; Frey, W.H. Delivery of Insulin-like Growth Factor-I to the Rat Brain and Spinal Cord along Olfactory and Trigeminal Pathways Following Intranasal Administration. Neuroscience 2004, 127, 481–496. [Google Scholar] [CrossRef] [PubMed]
- Ross, T.M.; Martinez, P.M.; Renner, J.C.; Thorne, R.G.; Hanson, L.R.; Frey, W.H. Intranasal Administration of Interferon Beta Bypasses the Blood-Brain Barrier to Target the Central Nervous System and Cervical Lymph Nodes: A Non-Invasive Treatment Strategy for Multiple Sclerosis. J. Neuroimmunol 2004, 151, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Ross, T.M.; Zuckermann, R.N.; Reinhard, C.; Frey, W.H. Intranasal Administration Delivers Peptoids to the Rat Central Nervous System. Neurosci. Lett. 2008, 439, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Thorne, R.G.; Hanson, L.R.; Ross, T.M.; Tung, D.; Frey, W.H. Delivery of Interferon-Beta to the Monkey Nervous System Following Intranasal Administration. Neuroscience 2008, 152, 785–797. [Google Scholar] [CrossRef]
- Lochhead, J.J.; Thorne, R.G. Intranasal Delivery of Biologics to the Central Nervous System. Adv. Drug Deliv. Rev. 2012, 64, 614–628. [Google Scholar] [CrossRef]
- Kumar, N.N.; Lochhead, J.J.; Pizzo, M.E.; Nehra, G.; Boroumand, S.; Greene, G.; Thorne, R.G. Delivery of Immunoglobulin G Antibodies to the Rat Nervous System Following Intranasal Administration: Distribution, Dose-Response, and Mechanisms of Delivery. J. Control. Release 2018, 286, 467–484. [Google Scholar] [CrossRef]
- Lochhead, J.J.; Kellohen, K.L.; Ronaldson, P.T.; Davis, T.P. Distribution of Insulin in Trigeminal Nerve and Brain after Intranasal Administration. Sci. Rep. 2019, 9, 2621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gizurarson, S. Anatomical and Histological Factors Affecting Intranasal Drug and Vaccine Delivery. Curr. Drug Deliv. 2012, 9, 566–582. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Jin, B.-H.; Chen, Y.-J.; Cao, C.; Zhu, J.-Z.; Zhao, Y.-Z.; Yu, X.-C.; Li, F.-Z. The Involvement of Perivascular Spaces or Tissues in the Facial Intradermal Brain-Targeted Delivery. Drug Deliv. 2019, 26, 393–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal Drug Delivery: Opportunities and Toxicologic Challenges during Drug Development. Drug Deliv. Transl. Res. 2021. [Google Scholar] [CrossRef]
- Inoue, D.; Furubayashi, T.; Tanaka, A.; Sakane, T.; Sugano, K. Effect of Cerebrospinal Fluid Circulation on Nose-to-Brain Direct Delivery and Distribution of Caffeine in Rats. Mol. Pharm. 2020, 17, 4067–4076. [Google Scholar] [CrossRef]
- Lochhead, J.J.; Wolak, D.J.; Pizzo, M.E.; Thorne, R.G. Rapid Transport within Cerebral Perivascular Spaces Underlies Widespread Tracer Distribution in the Brain after Intranasal Administration. J. Cereb. Blood Flow Metab. 2015, 35, 371–381. [Google Scholar] [CrossRef]
- Meidahl, A.C.; Eisenried, A.; Klukinov, M.; Cao, L.; Tzabazis, A.Z.; Yeomans, D.C. Intranasal Oxytocin Attenuates Reactive and Ongoing, Chronic Pain in a Model of Mild Traumatic Brain Injury. Headache J. Head Face Pain 2018, 58, 545–558. [Google Scholar] [CrossRef]
- Pfeifer, A.-C.; Schroeder-Pfeifer, P.; Schneider, E.; Schick, M.; Heinrichs, M.; Bodenmann, G.; Ehlert, U.; Herpertz, S.C.; Läuchli, S.; Eckstein, M.; et al. Oxytocin and Positive Couple Interaction Affect the Perception of Wound Pain in Everyday Life. Mol. Pain 2020, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, I.; Schmitgen, M.M.; Boll, S.; Roth, C.; Nees, F.; Usai, K.; Herpertz, S.C.; Wolf, R.C. Oxytocin Modulates Intrinsic Neural Activity in Patients with Chronic Low Back Pain. Eur. J. Pain 2020, 24, 945–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, M.J.; Campbell, T.S.; Robert, M.; Nasr-Esfahani, M.; Rash, J.A. Intranasal Oxytocin as a Treatment for Chronic Pelvic Pain: A Randomized Controlled Feasibility Study. Int. J. Gynaecol. Obstet. 2021, 152, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Boll, S.; de Minas, A.C.A.; Raftogianni, A.; Herpertz, S.C.; Grinevich, V. Oxytocin and Pain Perception: From Animal Models to Human Research. Neuroscience 2018, 387, 149–161. [Google Scholar] [CrossRef]
- Boll, S.; Ueltzhoeffer, K.; Roth, C.; Bertsch, K.; Desch, S.; Nees, F.; Grinevich, V.; Herpertz, S.C. Pain-Modulating Effects of Oxytocin in Patients with Chronic Low Back Pain. Neuropharmacology 2020, 171, 108105. [Google Scholar] [CrossRef]
- García-Boll, E.; Martínez-Lorenzana, G.; Condés-Lara, M.; González-Hernández, A. Inhibition of Nociceptive Dural Input to the Trigeminocervical Complex through Oxytocinergic Transmission. Exp. Neurol. 2020, 323, 113079. [Google Scholar] [CrossRef]
- Tracy, L.M.; Labuschagne, I.; Georgiou-Karistianis, N.; Gibson, S.J.; Giummarra, M.J. Sex-Specific Effects of Intranasal Oxytocin on Thermal Pain Perception: A Randomised, Double-Blind, Placebo-Controlled Cross-over Study. Psychoneuroendocrinology 2017, 83, 101–110. [Google Scholar] [CrossRef]
- Yeomans, D.C.; Klukinov, M. A Rodent Model of Trigeminal Neuralgia. Methods Mol. Biol 2012, 851, 121–131. [Google Scholar] [CrossRef]
- Constantinides, C.; Kapralos, V.; Manousakas, T.; Mitropoulos, D.; Alamanis, C.; Dimopoulos, C. Management of Renal Colic with Intranasal Desmopressin Spray. Acta Urol. Belg. 1998, 66, 1–3. [Google Scholar]
- Lopes, T.; Dias, J.S.; Marcelino, J.; Varela, J.; Ribeiro, S.; Dias, J. An Assessment of the Clinical Efficacy of Intranasal Desmopressin Spray in the Treatment of Renal Colic. BJU Int. 2001, 87, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Hazhir, S.; Badr, Y.A.A.; Darabi, J.N. Comparison of Intranasal Desmopressin and Intramuscular Tramadol versus Pethidine in Patients with Renal Colic. Urol J. 2010, 7, 148–151. [Google Scholar] [PubMed]
- Dolatabadi, A.A.; Memary, E.; Kariman, H.; Gigloo, K.N.; Baratloo, A. Intranasal Desmopressin Compared with Intravenous Ketorolac for Pain Management of Patients with Renal Colic Referring to the Emergency Department: A Randomized Clinical Trial. Anesth Pain Med. 2017, 7, e43595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fighera, T.M.; Spritzer, P.M. Effect of Intranasal Calcitonin in a Patient with McCune-Albright Syndrome, Fibrous Dysplasia, and Refractory Bone Pain. Case Rep. Endocrinol. 2017, 2017, 7898713. [Google Scholar] [CrossRef] [Green Version]
- Karponis, A.; Rizou, S.; Pallis, D.; Zafeiris, C.P.; Georgiou, D.F.; Galanos, A.; Giannoulis, F.; Lyritis, G.P. Analgesic Effect of Nasal Salmon Calcitonin during the Early Post-Fracture Period of the Distal Radius Fracture. J. Musculoskelet Neuronal. Interact. 2015, 15, 186–189. [Google Scholar]
- Blau, L.A.; Hoehns, J.D. Analgesic Efficacy of Calcitonin for Vertebral Fracture Pain. Ann. Pharm. 2003, 37, 564–570. [Google Scholar] [CrossRef]
- Qin, H.; Cai, J.; Yang, F.S. Could Calcitonin Be a Useful Therapeutic Agent for Trigeminal Neuralgia? Med. Hypotheses 2008, 71, 114–116. [Google Scholar] [CrossRef]
- Eisenberg, E.; Geller, R.; Brill, S. Pharmacotherapy Options for Complex Regional Pain Syndrome. Expert Rev. Neurother 2007, 7, 521–531. [Google Scholar] [CrossRef]
- Wall, G.C.; Heyneman, C.A. Calcitonin in Phantom Limb Pain. Ann. Pharm. 1999, 33, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Appelboom, T. Calcitonin in Reflex Sympathetic Dystrophy Syndrome and Other Painful Conditions. Bone 2002, 30, 84S–86S. [Google Scholar] [CrossRef]
- Meidahl, A.C.; Klukinov, M.; Tzabazis, A.Z.; Sorensen, J.C.; Yeomans, D.C. Nasal Application of HSV Encoding Human Preproenkephalin Blocks Craniofacial Pain in a Rat Model of Traumatic Brain Injury. Gene Ther. 2017, 24, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Gwak, H.S.; Cho, Y.M.; Chun, I.K. Analgesic Effects of Intra-Nasal Enkephalins. J. Pharm. Pharm. 2003, 55, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Kropotova, E.S.; Ivleva, I.S.; Karpenko, M.N.; Mosevitsky, M.I. Design of Enkephalin Modifications Protected from Brain Extracellular Peptidases Providing Long-Term Analgesia. Bioorganic Med. Chem. 2020, 28, 115184. [Google Scholar] [CrossRef]
- Manda, P.; Kushwaha, A.S.; Kundu, S.; Shivakumar, H.N.; Jo, S.B.; Murthy, S.N. Delivery of Ziconotide to Cerebrospinal Fluid via Intranasal Pathway for the Treatment of Chronic Pain. J. Control. Release 2016, 224, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.; Li, Y.; Chen, J.; Zhang, Y.; Tao, X.; Dai, Q.; Wang, Y.; Li, S.; Dong, M. TAT-Modified ω-Conotoxin MVIIA for Crossing the Blood-Brain Barrier. Mar. Drugs 2019, 17, 286. [Google Scholar] [CrossRef] [Green Version]
- Gänger, S.; Schindowski, K. Tailoring Formulations for Intranasal Nose-to-Brain Delivery: A Review on Architecture, Physico-Chemical Characteristics and Mucociliary Clearance of the Nasal Olfactory Mucosa. Pharmaceutics 2018, 10, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourganis, V.; Kammona, O.; Alexopoulos, A.; Kiparissides, C. Recent Advances in Carrier Mediated Nose-to-Brain Delivery of Pharmaceutics. Eur. J. Pharm. Biopharm. 2018, 128, 337–362. [Google Scholar] [CrossRef]
- Boddupalli, B.M.; Mohammed, Z.N.K.; Nath, R.A.; Banji, D. Mucoadhesive Drug Delivery System: An Overview. J. Adv. Pharm. Technol. Res. 2010, 1, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Gao, M. Factors Influencing Drug Deposition in the Nasal Cavity upon Delivery via Nasal Sprays. J. Pharm. Investig. 2020, 9, 251–259. [Google Scholar] [CrossRef]
- Harris, A.S.; Ohlin, M.; Lethagen, S.; Nilsson, I.M. Effects of Concentration and Volume on Nasal Bioavailability and Biological Response to Desmopressin. J. Pharm. Sci. 1988, 77, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Laube, B.; Dalby, R. The Effect of Formulation Variables and Breathing Patterns on the Site of Nasal Deposition in an Anatomically Correct Model. Pharm. Res. 2005, 22, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Djupesland, P.G.; Skretting, A.; Winderen, M.; Holand, T. Breath Actuated Device Improves Delivery to Target Sites beyond the Nasal Valve. Laryngoscope 2006, 116, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Quintana, D.S.; Westlye, L.T.; Rustan, Ø.G.; Tesli, N.; Poppy, C.L.; Smevik, H.; Tesli, M.; Røine, M.; Mahmoud, R.A.; Smerud, K.T.; et al. Low-Dose Oxytocin Delivered Intranasally with Breath Powered Device Affects Social-Cognitive Behavior: A Randomized Four-Way Crossover Trial with Nasal Cavity Dimension Assessment. Transl. Psychiatry 2015, 5, e602. [Google Scholar] [CrossRef] [PubMed]
- Hoekman, J.D.; Ho, R.J.Y. Enhanced Analgesic Responses after Preferential Delivery of Morphine and Fentanyl to the Olfactory Epithelium in Rats. Anesth. Analg. 2011, 113, 641–651. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Shao, X.; Zhang, C.; Tan, Y.; Liu, Q.; Wan, X.; Zhang, Q.; Xu, S.; Jiang, X. Intranasal H102 Peptide-Loaded Liposomes for Brain Delivery to Treat Alzheimer’s Disease. Pharm. Res. 2015, 32, 3837–3849. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-S.; Oh, K.T.; Choi, H.-G.; Lim, S.-J. Liposomal Formulations for Nose-to-Brain Delivery: Recent Advances and Future Perspectives. Pharmaceutics 2019, 11, 540. [Google Scholar] [CrossRef] [Green Version]
- Djupesland, P.G. Nasal Drug Delivery Devices: Characteristics and Performance in a Clinical Perspective—A Review. Drug Deliv. Transl. Res. 2013, 3, 42–62. [Google Scholar] [CrossRef] [Green Version]
- Berger, W.E.; Godfrey, J.W.; Slater, A.L. Intranasal Corticosteroids: The Development of a Drug Delivery Device for Fluticasone Furoate as a Potential Step toward Improved Compliance. Expert Opin. Drug Deliv. 2007, 4, 689–701. [Google Scholar] [CrossRef]
- Coe, M.A.; Lofwall, M.R.; Vessels, V.; Nuzzo, P.A.; Walsh, S.L. Evaluation of Tradipitant, a Selective NK1 Antagonist, on Response to Oxycodone in Humans. Psychopharmacology 2021, 238, 1857–1866. [Google Scholar] [CrossRef]
- Li, X.; Hua, G.-C.; Peng, F. Efficacy of Intranasal Ketamine for Acute Pain Management in Adults: A Systematic Review and Meta-Analysis. Eur. Rev. Med. Pharm. Sci. 2021, 25, 3286–3295. [Google Scholar] [CrossRef]
- Fernandes, M.; Schelotto, M.; Doldi, P.M.; Milani, G.; Manzano, A.A.A.; Valdivia, D.P.; Matos, A.M.W.; Abdelrahim, Y.H.; Bek, S.A.H.; Benitez, B.K.; et al. IMPORTANCE Trial: A Provisional Study-Design of a Single-Center, Phase II, Double-Blinded, Placebo-Controlled, Randomized, 4-Week Study to Compare the Efficacy and Safety of Intranasal Esketamine in Chronic Opioid Refractory Pain. F1000Research 2021, 10, 42. [Google Scholar] [CrossRef]
- Khanna, K.; Sharma, N.; Rawat, S.; Khan, N.; Karwasra, R.; Hasan, N.; Kumar, A.; Jain, G.K.; Nishad, D.K.; Khanna, S.; et al. Intranasal Solid Lipid Nanoparticles for Management of Pain: A Full Factorial Design Approach, Characterization & Gamma Scintigraphy. Chem. Phys. Lipids 2021, 236, 105060. [Google Scholar] [CrossRef]
- Yazdani, J.; Khorshidi-Khiavi, R.; Nezafati, S.; Mortazavi, A.; Farhadi, F.; Nojan, F.; Ghanizadeh, M. Comparison of Analgesic Effects of Intravenous and Intranasal Ketorolac in Patients with Mandibular Fracture-A Randomized Clinical Trial. J. Clin. Exp. Dent. 2019, 11, e768–e775. [Google Scholar] [CrossRef]
- Seppänen, S.-M.; Kuuskoski, R.; Mäkelä, K.T.; Saari, T.I.; Uusalo, P. Intranasal Dexmedetomidine Reduces Postoperative Opioid Requirement in Patients Undergoing Total Knee Arthroplasty Under General Anesthesia. J. Arthroplast. 2021, 36, 978–985.e1. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, J.; Lupo, N.; Bernkop-Schnürch, A. Advanced Formulations for Intranasal Delivery of Biologics. Int. J. Pharm. 2018, 553, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Bahadur, S.; Pardhi, D.M.; Rautio, J.; Rosenholm, J.M.; Pathak, K. Intranasal Nanoemulsions for Direct Nose-to-Brain Delivery of Actives for CNS Disorders. Pharmaceutics 2020, 12, 1230. [Google Scholar] [CrossRef] [PubMed]


| Tissue | Mean (nM) ± SE |
|---|---|
| Respiratory epithelium | 731,147 ± 76,889 |
| Olfactory epithelium | 19,348 ± 8141 |
| Trigeminal ganglion | 574 ± 181 |
| Trigeminal maxillary N. | 471 ± 117 |
| Trigeminal mandibular N. | 676 ± 235 |
| Trigeminal ophthalmic N. | 424 ± 235 |
| Dorsal dura | 152 ± 11.6 |
| Ventral dura | 271 ± 43.4 |
| Spinal dura | 31 ± 7.9 |
| Olfactory bulbs | 33 ± 13 |
| Ant. olfactory nucleus | 34 ± 10 |
| Caudate-putamen | 39 ± 10 |
| Septal nucleus | 24 ± 6 |
| Parietal cortex | 29 ± 6 |
| Hippocampus | 15 ± 3 |
| Thalamus | 21 ± 4 |
| Hypothalamus | 21 ± 4 |
| Midbrain | 23 ± 12 |
| Pons | 26 ± 11 |
| Cerebellum | 20 ± 8 |
| Blood | 63 ± 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bharadwaj, V.N.; Tzabazis, A.Z.; Klukinov, M.; Manering, N.A.; Yeomans, D.C. Intranasal Administration for Pain: Oxytocin and Other Polypeptides. Pharmaceutics 2021, 13, 1088. https://doi.org/10.3390/pharmaceutics13071088
Bharadwaj VN, Tzabazis AZ, Klukinov M, Manering NA, Yeomans DC. Intranasal Administration for Pain: Oxytocin and Other Polypeptides. Pharmaceutics. 2021; 13(7):1088. https://doi.org/10.3390/pharmaceutics13071088
Chicago/Turabian StyleBharadwaj, Vimala N., Alexander Z. Tzabazis, Michael Klukinov, Neil A. Manering, and David C. Yeomans. 2021. "Intranasal Administration for Pain: Oxytocin and Other Polypeptides" Pharmaceutics 13, no. 7: 1088. https://doi.org/10.3390/pharmaceutics13071088