
Inhalation Delivery for the Treatment and Prevention of COVID-19 Infection

 , ,
, ,
Abstract
:1. Introduction
2. Compare/Contrast SARS-COV-2 with SARS COV-1/MERS Coronaviruses
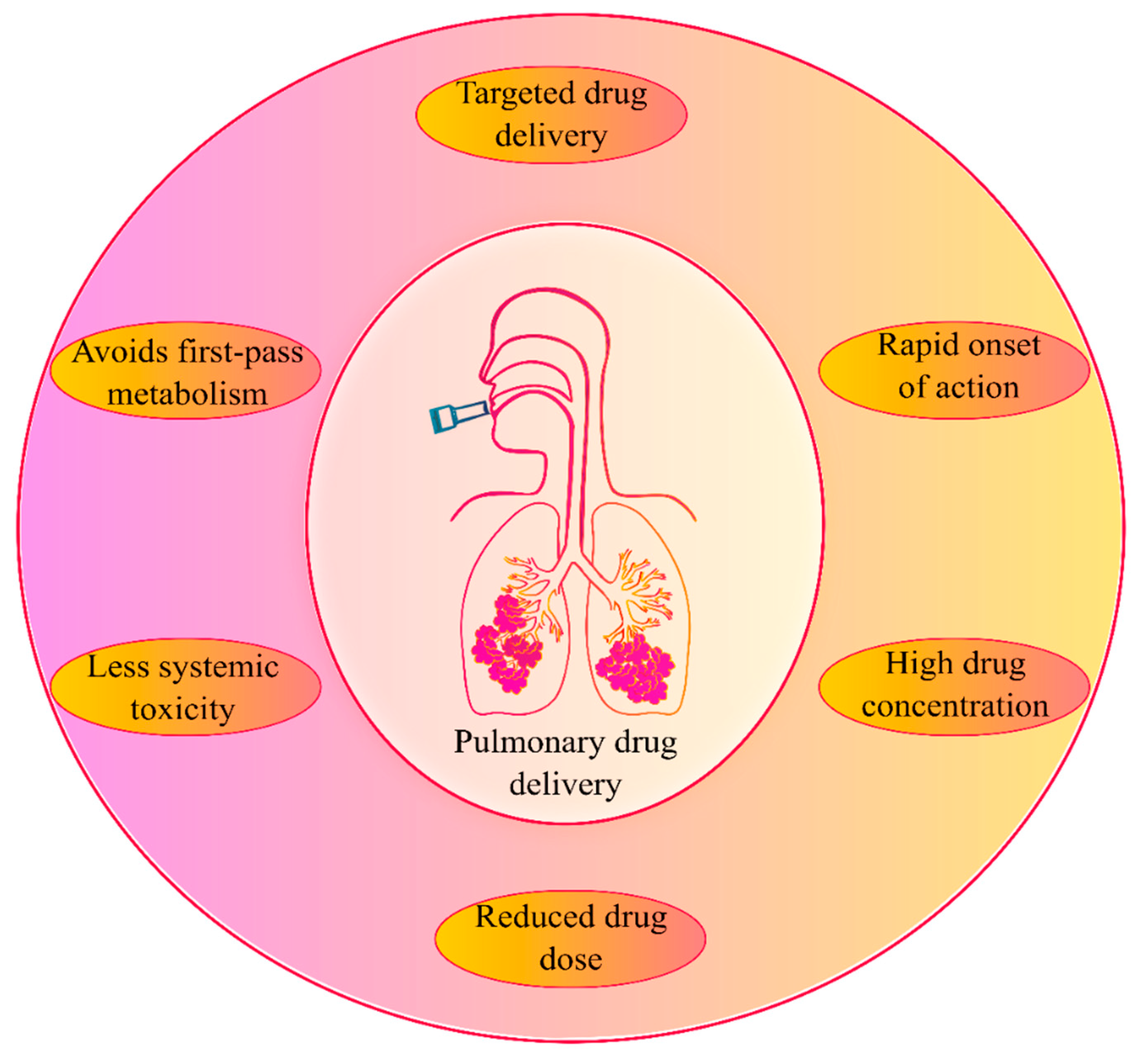
3. Inhalational Drug Administration—An Overview
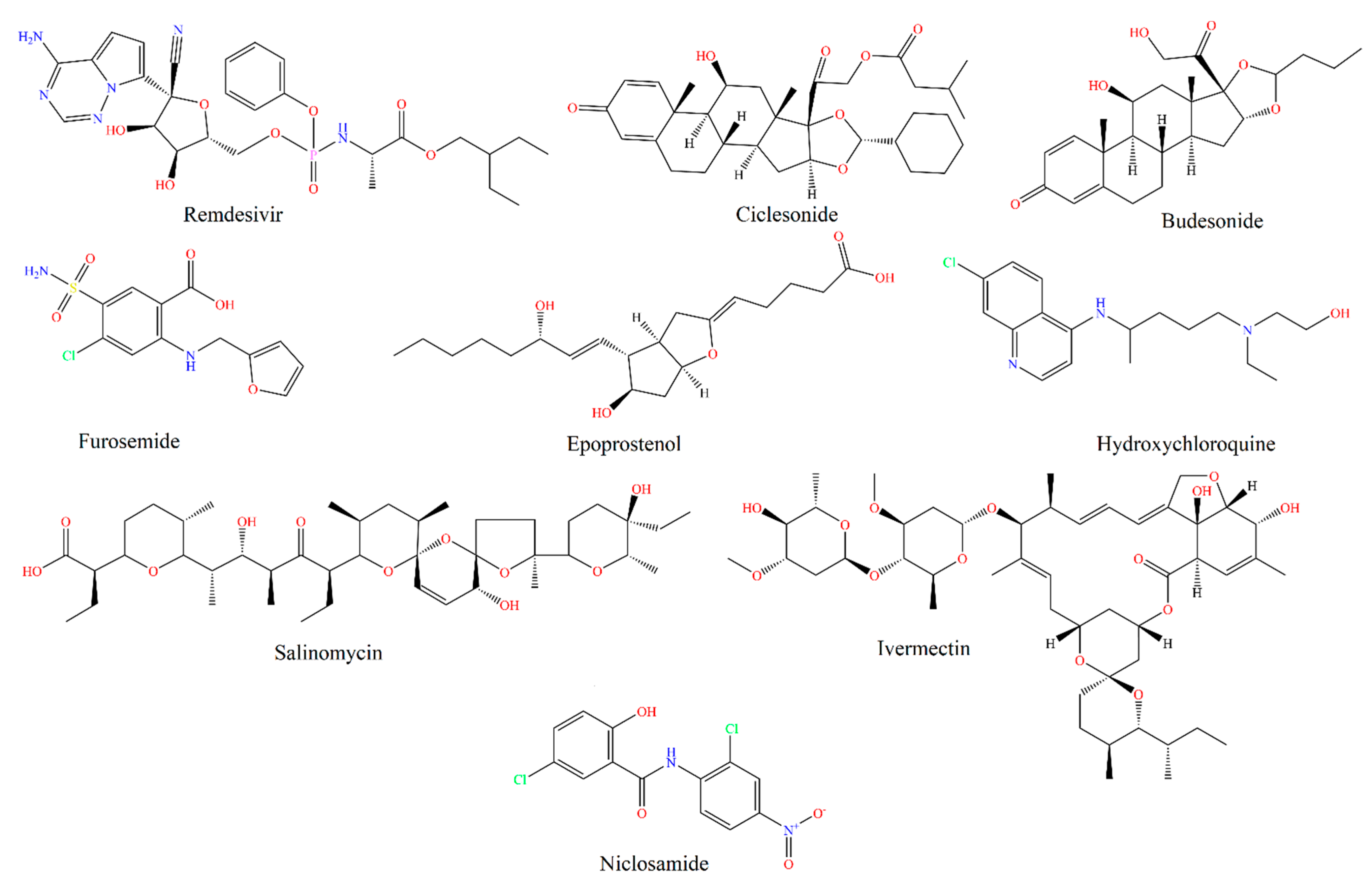
4. Inhaled COVID-19 Therapeutics
4.1. Remdesivir
4.2. Ciclesonide
4.3. Budesonide
4.4. Furosemide
4.5. Nitric Oxide (NO) and Epoprostenol
4.6. Hydroxychloroquine
4.7. Plasminogen
4.8. Modified Angiotensin-Converting Enzyme 2 (ACE2)
4.9. Interferon-β
4.10. Anti-Microbial Colloidal Silver Formulations
4.11. Unfractionated Heparin (UFH)
4.12. Salinomycin
4.13. Ivermectin
4.14. Niclosamide
5. Clinical Trials on Inhaled COVID-19 Therapeutics
6. Inhaled COVID-19 Vaccines and Their Current Clinical Status
6.1. AdCOVID Vaccine
6.2. MV-014-212 Meissa Vaccine
6.3. CoroFlu Vaccine
6.4. CanSinoBio Vaccine
6.5. AstraZeneca COVID19 Vaccine
6.6. COVI-VAC
7. Inhaled Therapy in Long-Haul COVID
8. Conclusions and Future Opportunities
Author Contributions
Funding
Conflicts of Interest
References
- Omolo, C.A.; Soni, N.; Fasiku, V.O.; Mackraj, I.; Govender, T. Update on therapeutic approaches and emerging therapies for SARS-CoV-2 virus. Eur. J. Pharmacol. 2020, 883, 173348. [Google Scholar] [CrossRef]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus Disease (COVID-19) Dashboard. World Health Organization website. Available online: https://covid19.who.int/ (accessed on 18 June 2021).
- Bhavana, V.; Thakor, P.; Singh, S.B.; Mehra, N.K. COVID-19: Pathophysiology, treatment options, nanotechnology approaches, and research agenda to combating the SARS-CoV2 pandemic. Life Sci. 2020, 261, 118336. [Google Scholar] [CrossRef]
- Edwards, D.; Hickey, A.; Batycky, R.; Griel, L.; Lipp, M.; Dehaan, W.; Clarke, R.; Hava, D.; Perry, J.; Laurenzi, B.; et al. A New natural defense against airborne pathogens. QRB Discov. 2020, 1, e5. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Abdellatif, A.A.H.; Tawfeek, H.M.; Abdelfattah, A.; El-Saber Batiha, G.; Hetta, H.F. Recent updates in COVID-19 with emphasis on inhalation therapeutics: Nanostructured and targeting systems. J. Drug Deliv. Sci. Technol. 2021, 63, 102435. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.P.; Berlinski, A.; Canisius, S.; Cipolla, D.; Dolovich, M.B.; Gonda, I.; Hochhaus, G.; Kadrichu, N.; Lyapustina, S.; Mansour, H.M. Urgent appeal from International Society for Aerosols in Medicine (ISAM) during COVID-19: Clinical decision makers and governmental agencies should consider the inhaled route of administration: A statement from the ISAM regulatory and standardization issues networking group. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.J. Back to the future: Inhaled drug products. J. Pharm. Sci. 2013, 102, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Rau, J.L. The inhalation of drugs: Advantages and problems. Respir. Care 2005, 50, 367–382. [Google Scholar]
- Eedara, B.B.; Tucker, I.G.; Das, S.C. In vitro dissolution testing of respirable size anti-tubercular drug particles using a small volume dissolution apparatus. Int. J. Pharm. 2019, 559, 235–244. [Google Scholar] [CrossRef]
- Eedara, B.B.; Rangnekar, B.; Doyle, C.; Cavallaro, A.; Das, S.C. The influence of surface active l-leucine and 1,2-dipalmitoyl-sn-glycero-3-phosphatidylcholine (DPPC) in the improvement of aerosolization of pyrazinamide and moxifloxacin co-spray dried powders. Int. J. Pharm. 2018, 542, 72–81. [Google Scholar] [CrossRef]
- Eedara, B.B.; Rangnekar, B.; Sinha, S.; Doyle, C.; Cavallaro, A.; Das, S.C. Development and characterization of high payload combination dry powders of anti-tubercular drugs for treating pulmonary tuberculosis. Eur. J. Pharm. Sci. 2018, 118, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Eedara, B.B.; Tucker, I.G.; Das, S.C. Phospholipid-based pyrazinamide spray-dried inhalable powders for treating tuberculosis. Int. J. Pharm. 2016, 506, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Eedara, B.B.; Tucker, I.G.; Zujovic, Z.D.; Rades, T.; Price, J.R.; Das, S.C. Crystalline adduct of moxifloxacin with trans-cinnamic acid to reduce the aqueous solubility and dissolution rate for improved residence time in the lungs. Eur. J. Pharm. Sci. 2019, 136, 104961. [Google Scholar] [CrossRef] [PubMed]
- Rangnekar, B.; Momin, M.A.M.; Eedara, B.B.; Sinha, S.; Das, S.C. Bedaquiline containing triple combination powder for inhalation to treat drug-resistant tuberculosis. Int. J. Pharm. 2019, 570, 118689. [Google Scholar] [CrossRef]
- Tu, Y.-F.; Chien, C.-S.; Yarmishyn, A.A.; Lin, Y.-Y.; Luo, Y.-H.; Lin, Y.-T.; Lai, W.-Y.; Yang, D.-M.; Chou, S.-J.; Yang, Y.-P.; et al. A review of SARS-CoV-2 and the ongoing clinical trials. Int. J. Mol. Sci. 2020, 21, 2657. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.; Jiang, J.; Su, L.; Shu, T.; Liu, H.; Lai, S.; Ghiladi, R.A.; Wang, J. The role of NO in COVID-19 and potential therapeutic strategies. Free Radic. Biol. Med. 2021, 163, 153–162. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, Y.; Vilekar, P.; Yang, S.-P.; Gupta, M.; Oh, M.I.; Meek, A.; Doyle, L.; Villar, L.; Brennecke, A. Small molecule therapeutics for COVID-19: Repurposing of inhaled furosemide. PeerJ 2020, 8, e9533. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, M.; Hamblin, M.R.; Rezaei, N. COVID-19: Transmission, prevention, and potential therapeutic opportunities. Clin. Chim. Acta 2020, 508, 254–266. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 19, 141–154. [Google Scholar] [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.-L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [Green Version]
- Amanat, F.; Krammer, F. SARS-CoV-2 vaccines: Status report. Immunity 2020, 52, 583–589. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Cevik, M.; Tate, M.; Lloyd, O.; Maraolo, A.E.; Schafers, J.; Ho, A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: A systematic review and meta-analysis. Lancet Microbe 2021, 2, e13–e22. [Google Scholar] [CrossRef]
- Stein, S.W.; Thiel, C.G. The history of therapeutic aerosols: A chronological review. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 20–41. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.J. Emerging trends in inhaled drug delivery. Adv. Drug Deliv. Rev. 2020, 157, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Pilcer, G.; Amighi, K. Formulation strategy and use of excipients in pulmonary drug delivery. Int. J. Pharm. 2010, 392, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Alabsi, W.; Al-Obeidi, F.A.; Polt, R.; Mansour, H.M. Organic solution advanced spray-dried microparticulate/nanoparticulate dry powders of lactomorphin for respiratory delivery: Physicochemical characterization, in vitro aerosol dispersion, and cellular studies. Pharmaceutics 2020, 13, 26. [Google Scholar] [CrossRef]
- Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Mansour, H.M. Spray-dried inhalable powder formulations of therapeutic proteins and peptides. AAPS PharmSciTech 2021, 22, 185. [Google Scholar] [CrossRef] [PubMed]
- Sahakijpijarn, S.; Moon, C.; Koleng, J.J.; Christensen, D.J.; Williams III, R.O. Development of remdesivir as a dry powder for inhalation by thin film freezing. Pharmaceutics 2020, 12, 1002. [Google Scholar] [CrossRef] [PubMed]
- Vartak, R.; Patil, S.M.; Saraswat, A.; Patki, M.; Kunda, N.K.; Patel, K. Aerosolized nanoliposomal carrier of remdesivir: An effective alternative for COVID-19 treatment in vitro. Nanomedicine 2021, 16, 1187–1202. [Google Scholar] [CrossRef]
- Matsuyama, S.; Kawase, M.; Nao, N.; Shirato, K.; Ujike, M.; Kamitani, W.; Shimojima, M.; Fukushi, S. The inhaled corticosteroid ciclesonide blocks coronavirus RNA replication by targeting viral NSP15. BioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Iwabuchi, K.; Yoshie, K.; Kurakami, Y.; Takahashi, K.; Kato, Y.; Morishima, T. Therapeutic potential of ciclesonide inhalation for COVID-19 pneumonia: Report of three cases. J. Infect. Chemother. 2020, 26, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.G.; Singh, D.; Hadfield, R.M. Inhaled corticosteroids and COVID-19: A systematic review and clinical perspective. Eur. Respir. J. 2020, 55, 2001009. [Google Scholar] [CrossRef]
- Yamaya, M.; Nishimura, H.; Deng, X.; Sugawara, M.; Watanabe, O.; Nomura, K.; Shimotai, Y.; Momma, H.; Ichinose, M.; Kawase, T. Inhibitory effects of glycopyrronium, formoterol, and budesonide on coronavirus HCoV-229E replication and cytokine production by primary cultures of human nasal and tracheal epithelial cells. Respir. Investig. 2020, 58, 155–168. [Google Scholar] [CrossRef]
- Nicolau, D.V.; Bafadhel, M. Inhaled corticosteroids in virus pandemics: A treatment for COVID-19? Lancet. Respir. Med. 2020, 8, 846–847. [Google Scholar] [CrossRef]
- Yu, L.-M.; Bafadhel, M.; Dorward, J.; Hayward, G.; Saville, B.R.; Gbinigie, O.; Van Hecke, O.; Ogburn, E.; Evans, P.H.; Thomas, N.P.; et al. Inhaled budesonide for COVID-19 in people at higher risk of adverse outcomes in the community: Interim analyses from the PRINCIPLE trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Nicolau, D.V.; Langford, B.; Mahdi, M.; Jeffers, H.; Mwasuku, C.; Krassowska, K.; Fox, R.; Binnian, I.; Glover, V.; et al. Inhaled budesonide in the treatment of early COVID-19 illness: A randomised controlled trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Brennecke, A.; Villar, L.; Wang, Z.; Doyle, L.M.; Meek, A.; Reed, M.; Barden, C.; Weaver, D.F. Is inhaled furosemide a potential therapeutic for COVID-19? Am. J. Med. Sci. 2020, 360, 216–221. [Google Scholar] [CrossRef]
- Grogono, J.C.; Butler, C.; Izadi, H.; Moosavi, S.H. Inhaled furosemide for relief of air hunger versus sense of breathing effort: A randomized controlled trial. Respir. Res. 2018, 19, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moosavi, S.H.; Binks, A.P.; Lansing, R.W.; Topulos, G.P.; Banzett, R.B.; Schwartzstein, R.M. Effect of inhaled furosemide on air hunger induced in healthy humans. Respir. Physiol. Neurobiol. 2007, 156, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nishino, T.; Ide, T.; Sudo, T.; Sato, J. Inhaled furosemide greatly alleviates the sensation of experimentally induced dyspnea. Am. J. Respir. Crit. Care Med. 2000, 161, 1963–1967. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z. An update on current therapeutic drugs treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.; Wilson, C.; Weinberg, J.; Gavin, D.; Murphy, J.; Reardon, C.C. Inhaled nitric oxide treatment in spontaneously breathing COVID-19 patients. Ther. Adv. Respir. Dis. 2020, 14. [Google Scholar] [CrossRef]
- Kavanagh, O.; Healy, A.M.; Dayton, F.; Robinson, S.; O’Reilly, N.J.; Mahoney, B.; Arthur, A.; Walker, G.; Farragher, J.P. Inhaled hydroxychloroquine to improve efficacy and reduce harm in the treatment of COVID-19. Med. Hypotheses 2020, 143, 110110. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Klimke, A.; Hefner, G.; Will, B.; Voss, U. Hydroxychloroquine as an aerosol might markedly reduce and even prevent severe clinical symptoms after SARS-CoV-2 infection. Med. Hypotheses 2020, 142, 109783. [Google Scholar] [CrossRef]
- Miles, L.A.; Lighvani, S.; Baik, N.; Parmer, C.M.; Khaldoyanidi, S.; Mueller, B.M.; Parmer, R.J. New insights into the role of Plg-RKT in macrophage recruitment. Int. Rev. Cell Mol. Biol. 2014, 309, 259–302. [Google Scholar]
- Wu, Y.; Wang, T.; Guo, C.; Zhang, D.; Ge, X.; Huang, Z.; Zhou, X.; Li, Y.; Peng, Q.; Li, J. Plasminogen improves lung lesions and hypoxemia in patients with COVID-19. QJM: Int. J. Med. 2020, 113, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Lei, C.; Fu, W.; Qian, K.; Li, T.; Zhang, S.; Ding, M.; Hu, S. Potent neutralization of 2019 novel coronavirus by recombinant ACE2-Ig. BioRxiv 2020. [Google Scholar] [CrossRef]
- Ameratunga, R.; Lehnert, K.; Leung, E.; Comoletti, D.; Snell, R.; Woon, S.-T.; Abbott, W.; Mears, E.; Steele, R.; McKee, J. Inhaled modified angiotensin converting enzyme 2 (ACE2) as a decoy to mitigate SARS-CoV-2 infection. New Zealand Med. J. (Online) 2020, 133, 112–118. [Google Scholar]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]
- Monk, P.D.; Marsden, R.J.; Tear, V.J.; Brookes, J.; Batten, T.N.; Mankowski, M.; Gabbay, F.J.; Davies, D.E.; Holgate, S.T.; Ho, L.-P. Safety and efficacy of inhaled nebulised interferon beta-1a (SNG001) for treatment of SARS-CoV-2 infection: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Respir. Med. 2021, 9, 196–206. [Google Scholar] [CrossRef]
- Yuen, C.K.; Lam, J.Y.; Wong, W.M.; Mak, L.F.; Wang, X.; Chu, H.; Cai, J.P.; Jin, D.Y.; To, K.K.; Chan, J.F.; et al. SARS-CoV-2 nsp13, nsp14, nsp15 and orf6 function as potent interferon antagonists. Emerg. Microbes Infect. 2020, 9, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Djukanović, R.; Harrison, T.; Johnston, S.L.; Gabbay, F.; Wark, P.; Thomson, N.C.; Niven, R.; Singh, D.; Reddel, H.K.; Davies, D.E.; et al. The effect of inhaled IFN-β on worsening of asthma symptoms caused by viral infections. A randomized trial. Am. J. Respir. Crit. Care Med. 2014, 190, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Olsson, M.; Aurell, M.; Lundin, C.; Paraskos, J.; Cavallin, A.; Kjerrulf, M.; Karlsson, K.; Marsden, R.; Malmgren, A.; Gustafson, P.; et al. On-demand inhaled interferon-beta 1a for the prevention of severa asthma exacerbations: Results of the INEXAS phase 2a study. In D12. IMMUNOTHERAPY IN LUNG DISEASE; American Thoracic Society: New York, NY, USA, 2018; p. A6165. [Google Scholar]
- Zachar, O. Formulations for COVID-19 early stage treatment via silver nanoparticles inhalation delivery at home and hospital. Sci. Prepr. 2020. [Google Scholar] [CrossRef]
- Van Haren, F.M.; Page, C.; Laffey, J.G.; Artigas, A.; Camprubi-Rimblas, M.; Nunes, Q.; Smith, R.; Shute, J.; Carroll, M.; Tree, J. Nebulised heparin as a treatment for COVID-19: Scientific rationale and a call for randomised evidence. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef]
- Pindiprolu, S.K.S.; Kumar, C.S.P.; Golla, V.S.K.; Likitha, P.; Chandra, S.; Ramachandra, R. Pulmonary delivery of nanostructured lipid carriers for effective repurposing of salinomycin as an antiviral agent. Med. Hypotheses 2020, 143, 109858. [Google Scholar] [CrossRef]
- Jang, Y.; Shin, J.S.; Yoon, Y.-S.; Go, Y.Y.; Lee, H.W.; Kwon, O.S.; Park, S.; Park, M.-S.; Kim, M. Salinomycin Inhibits Influenza Virus Infection by Disrupting Endosomal Acidification and Viral Matrix Protein 2 Function. J. Virol. 2018, 92, e01441–e01418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, M.; Chang, S.Y.; Byun, S.Y.; Choi, I.; d’Alexandry d’Orengiani, A.-L.P.H.; Shum, D.; Min, J.-Y.; Windisch, M.P. Screening of FDA-approved drugs using a MERS-CoV clinical isolate from South Korea identifies potential therapeutic options for COVID-19. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Caly, L.; Druce, J.D.; Catton, M.G.; Jans, D.A.; Wagstaff, K.M. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antivir. Res. 2020, 178, 104787. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Song, Y.; Xiong, H.; Ci, X.; Li, H.; Yu, L.; Zhang, L.; Deng, X. Inhibitory effects of ivermectin on nitric oxide and prostaglandin E2 production in LPS-stimulated RAW 264.7 macrophages. Int. Immunopharmacol. 2009, 9, 354–359. [Google Scholar] [CrossRef]
- Mittal, N.; Mittal, R. Inhaled route and anti-inflammatory action of ivermectin: Do they hold promise in fighting against COVID-19? Med. Hypotheses 2021, 146, 110364. [Google Scholar] [CrossRef]
- Okasha, K. Ivermectin Nasal Spray for COVID19 Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04510233 (accessed on 19 June 2021).
- Weinbach, E.C.; Garbus, J. Mechanism of action of reagents that uncouple oxidative phosphorylation. Nature 1969, 221, 1016–1018. [Google Scholar] [CrossRef] [PubMed]
- Frayha, G.J.; Smyth, J.D.; Gobert, J.G.; Savel, J. The mechanisms of action of antiprotozoal and anthelmintic drugs in man. Gen. Pharmacol. Vasc. Syst. 1997, 28, 273–299. [Google Scholar] [CrossRef]
- Xu, J.; Shi, P.-Y.; Li, H.; Zhou, J. Broad Spectrum Antiviral Agent Niclosamide and Its Therapeutic Potential. ACS Infect. Dis. 2020, 6, 909–915. [Google Scholar] [CrossRef]
- New Delivery Method Could Make Niclosamide an Effective Antiviral to Treat COVID-19. Available online: https://news.utexas.edu/2020/04/06/new-delivery-method-could-make-niclosamide-an-effective-antiviral-to-treat-covid-19/ (accessed on 16 June 2021).
- Wu, C.-J.; Jan, J.-T.; Chen, C.-M.; Hsieh, H.-P.; Hwang, D.-R.; Liu, H.-W.; Liu, C.-Y.; Huang, H.-W.; Chen, S.-C.; Hong, C.-F.; et al. Inhibition of severe acute respiratory syndrome coronavirus replication by niclosamide. Antimicrob. Agents Chemother. 2004, 48, 2693–2696. [Google Scholar] [CrossRef] [Green Version]
- Gassen, N.C.; Niemeyer, D.; Muth, D.; Corman, V.M.; Martinelli, S.; Gassen, A.; Hafner, K.; Papies, J.; Mösbauer, K.; Zellner, A.; et al. SKP2 attenuates autophagy through Beclin1-ubiquitination and its inhibition reduces MERS-Coronavirus infection. Nat. Commun. 2019, 10, 5770. [Google Scholar] [CrossRef]
- Jeon, S.; Ko, M.; Lee, J.; Choi, I.; Byun, S.Y.; Park, S.; Shum, D.; Kim, S. Identification of Antiviral Drug Candidates against SARS-CoV-2 from FDA-Approved Drugs. Antimicrob. Agents Chemother. 2020, 64, e00819-00820. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, M.T.; Haugk, K.; McKiernan, J.S.; Gulati, R.; Cheng, H.H.; Maes, J.L.; Dumpit, R.F.; Nelson, P.S.; Montgomery, B.; McCune, J.S. A phase I study of niclosamide in combination with enzalutamide in men with castration-resistant prostate cancer. PLoS ONE 2018, 13, e0198389. [Google Scholar]
- Brunaugh, A.D.; Seo, H.; Warnken, Z.; Ding, L.; Seo, S.H.; Smyth, H.D.C. Development and evaluation of inhalable composite niclosamide-lysozyme particles: A broad-spectrum, patient-adaptable treatment for coronavirus infections and sequalae. PLoS ONE 2021, 16, e0246803. [Google Scholar] [CrossRef]
- Jara, M.O.; Warnken, Z.N.; Sahakijpijarn, S.; Moon, C.; Maier, E.Y.; Christensen, D.J.; Koleng, J.J.; Peters, J.I.; Hackman Maier, S.D.; Williams Iii, R.O. Niclosamide inhalation powder made by thin-film freezing: Multi-dose tolerability and exposure in rats and pharmacokinetics in hamsters. Int. J. Pharm. 2021, 603, 120701. [Google Scholar] [CrossRef] [PubMed]
- Stuart-Harris, N. Nitric Oxide Inhalation Therapy for COVID-19 Infections in the ED (NO COV-ED). Available online: https://ClinicalTrials.gov/show/NCT04338828 (accessed on 10 June 2021).
- Andersson, D.P.; Blennow, O. Inhalation of Ciclesonide For patients with COVID-19: A Randomised Open Treatment Study (HALT COVID-19) (HALT). Available online: https://clinicaltrials.gov/ct2/show/NCT04381364 (accessed on 10 June 2021).
- Ezer, N.; Naderi, N. Inhaled Ciclesonide for Outpatients with COVID19 (CONTAIN). Available online: https://clinicaltrials.gov/ct2/show/NCT04435795 (accessed on 10 June 2021).
- A Study of the Safety and Efficacy of Ciclesonide in the Treatment of Non-Hospitalized COVID-19 Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04377711 (accessed on 10 June 2021).
- Kaprin, A. Inhalation Low Dose Radionuclide Therapy in Treatment COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04724538 (accessed on 10 June 2021).
- Sjöbring, U. Study to Assess the Safety of Ascending Doses of UNI911 INHALATION in Healthy Volunteers in Preparation for Evaluation in Adults with COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04576312 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Efficacy of Aerosol Combination Therapy of 13 Cis Retinoic Acid and Captopril for Treating Covid-19 Patients via Indirect Inhibition of Transmembrane Protease, Serine 2 (TMPRSS2). Available online: https://clinicaltrials.gov/ct2/show/NCT04578236 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Combination of Chemopreventive Agents (all- Trans Retinoic Acid and Tamoxifen) as Potential Treatment for the Lung Complication of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04568096 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Combination Therapy with Isotretinoin and Tamoxifen Expected to Provide Complete Protection Against Severe Acute Respiratory Syndrome Coronavirus (Combination). Available online: https://clinicaltrials.gov/ct2/show/NCT04389580 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Clinical Role of Testosterone and Dihydrotestosterone and which of Them Should be Inhibited in COVID-19 Patients - A Double-Edged Sword? Available online: https://clinicaltrials.gov/ct2/show/NCT04623385 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Efficacy and Safety of Drug Combination Therapy of Isotretinoin and Some Antifungal Drugs as a Potential Aerosol Therapy for COVID-19: An innovative therapeutic approach COVID-19 (isotretinoin). Available online: https://clinicaltrials.gov/ct2/show/NCT04577378 (accessed on 10 June 2021).
- Xia, J. The Efficacy and Safety of Thalidomide Combined with Low-Dose Hormones in the Treatment of Severe COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04273581 (accessed on 10 June 2021).
- Elkazzaz, M.R.M. Aerosol Combination Therapy of All-Trans Retinoic Acid and Isotretinoin as a Novel Treatment for Inducing Neutralizing Antibodies in COVID -19 Infected Patients Better than Vaccine: An Innovative Treatment (Antibodies). Available online: https://clinicaltrials.gov/ct2/show/NCT04396067 (accessed on 10 June 2021).
- Ragab. New Treatment for COVID-19 Using Ethanol Vapor Inhalation. Available online: https://clinicaltrials.gov/ct2/show/NCT04554433 (accessed on 10 June 2021).
- A Clinical Study Evaluating Inhaled Aviptadil on COVID-19 (HOPE). Available online: https://clinicaltrials.gov/ct2/show/NCT04844580 (accessed on 10 June 2021).
- Leuppi, J.D.; Abig, K. Inhaled Aviptadil for the Treatment of COVID-19 in Patients at High Risk for ARDS. Available online: https://clinicaltrials.gov/ct2/show/NCT04536350 (accessed on 10 June 2021).
- Javitt, J.C. Inhaled ZYESAMI™ (Aviptadil Acetate) for the Treatment of Severe COVID-19 (AVICOVID-2). Available online: https://clinicaltrials.gov/ct2/show/NCT04360096 (accessed on 10 June 2021).
- El-Bendary, M. Inhaled Ivermectin and COVID-19 (CCOVID-19). Available online: https://clinicaltrials.gov/ct2/show/study/NCT04681053 (accessed on 10 June 2021).
- Kharma, N. INHALED Iloprost for Suspected COVID-19 Respiratory Failure (ILOCOVID). Available online: https://clinicaltrials.gov/ct2/show/NCT04445246 (accessed on 10 June 2021).
- First in Human SAD and MAD Study of Inhaled TD-0903, a Potential Treatment for ALI Associated with COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04350736 (accessed on 10 June 2021).
- Lanoix, J.-P. Treatment of COVID-19 by Nebulization of Inteferon Beta 1b Efficiency and Safety Study (COV-NI). Available online: https://clinicaltrials.gov/ct2/show/NCT04469491 (accessed on 10 June 2021).
- Varea, S. Inhaled Corticosteroid Treatment of COVID19 Patients with Pneumonia. Available online: https://clinicaltrials.gov/ct2/show/NCT04355637 (accessed on 10 June 2021).
- Bafadhel, M. Steroids in COVID-19 Study (STOIC). Available online: https://clinicaltrials.gov/ct2/show/NCT04416399 (accessed on 10 June 2021).
- Afazeli, S. Evaluation of Efficacy of Levamisole and Formoterol+Budesonide in Treatment of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04331470 (accessed on 10 June 2021).
- Taille, C. Protective role of Inhaled Steroids for Covid-19 Infection (INHASCO). Available online: https://clinicaltrials.gov/ct2/show/record/NCT04331054 (accessed on 10 June 2021).
- Levitt, J.; Festic, E.; Wilson, J. Arrest Respiratory Failure from Pneumonia (ARREST). Available online: https://clinicaltrials.gov/ct2/show/NCT04193878 (accessed on 10 June 2021).
- Zykov, K.A. Low-Doses Melphalan Inhalation in Patients with COVID-19 (Coronavirus Disease 2019) Pneumonia (MICOV). Available online: https://clinicaltrials.gov/ct2/show/NCT04380376 (accessed on 10 June 2021).
- Franco, V. VentaProst in Subjects with COVID-19 Requiring Mechanical Ventilation (VPCOVID). Available online: https://clinicaltrials.gov/ct2/show/NCT04452669 (accessed on 10 June 2021).
- Nebulized Heparin for the Treatment of COVID-19 (INHALE-HEP). Available online: https://clinicaltrials.gov/ct2/show/NCT04723563 (accessed on 10 June 2021).
- Haren, F.M.V. Inhaled Heparin for Hospitalised COVID-19 Patients (INHALE-HEP). Available online: https://clinicaltrials.gov/ct2/show/NCT04635241 (accessed on 10 June 2021).
- Qu, J.-M. A Pilot Clinical Study on Inhalation of Mesenchymal Stem Cells Exosomes Treating Severe Novel Coronavirus Pneumonia. Available online: https://clinicaltrials.gov/ct2/show/NCT04276987 (accessed on 10 June 2021).
- Wilkinson, T.; Francis, N. Trial of Inhaled Anti-Viral (SNG001) for SARS-CoV-2 (COVID-19) Infection. Available online: https://clinicaltrials.gov/ct2/show/NCT04385095 (accessed on 10 June 2021).
- Holliday, Z.M.; Schrum, A. Dornase Alfa for ARDS in Patients with Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2) (DORNASESARS2). Available online: https://clinicaltrials.gov/ct2/show/NCT04402970 (accessed on 10 June 2021).
- Porter, J. Nebulised Dornase Alfa for Treatment of COVID-19 (COVASE). Available online: https://clinicaltrials.gov/ct2/show/NCT04359654 (accessed on 10 June 2021).
- Astrelina, T. An Open Randomized Study of Dalargin Effectiveness in Patients with Severe and Critical manifestations of SARS-COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04346693 (accessed on 10 June 2021).
- Amen, R. Sodium Pyruvate Nasal Spray Treatment of COVID-19 and Influenza Infections. Available online: https://clinicaltrials.gov/ct2/show/NCT04824365 (accessed on 10 June 2021).
- Hawari, F. The Potential use of Inhaled hydroxychloroquine for the Treatment of COVID-19 in Cancer Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04731051 (accessed on 10 June 2021).
- El-Sherbiny, I.M. Development and Validation of “Ready-to-Use” Inhalable forms of Hydroxychloroquine for Treatment of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04477083 (accessed on 10 June 2021).
- Bentur, O.S. A Study to Evaluate the Safety, Tolerability and Pharmacokinetics of Orally Inhaled Aerosolized Hydroxychloroquine Sulfate in Healthy Adult Volunteers. Available online: https://clinicaltrials.gov/ct2/show/NCT04461353 (accessed on 10 June 2021).
- Broom, C. The Use of PUL-042 Inhalation Solution to Reduce the Severity of COVID-19 in Adults Positive for SARS-CoV-2 Infection. Available online: https://clinicaltrials.gov/ct2/show/NCT04312997 (accessed on 10 June 2021).
- Incalzi, R.A. Use of Inhaled High-Molecular Weight Hyaluronan in Patients with Severe COVID19: Feasibility and Outcomes (HA-COVID). Available online: https://clinicaltrials.gov/ct2/show/record/NCT04830020 (accessed on 10 June 2021).
- Study in Participants with Early Stage Coronavirus Disease 2019 (COVID-19) to Evaluate the Safety, Efficacy, and Pharmacokinetics of Remdesivir Administered by Inhalation. Available online: https://clinicaltrials.gov/ct2/show/NCT04539262 (accessed on 10 June 2021).
- Study of Ensifentrine or Placebo Delivered via pMDI in Hospitalized Patients with COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04527471 (accessed on 10 June 2021).
- Muscedere, J. Furosemide as Supportive Therapy for COVID-19 Respiratory Failure (FaST-1). Available online: https://clinicaltrials.gov/ct2/show/NCT04588792 (accessed on 10 June 2021).
- Phase 3 Inhaled Novaferon Study in Hospitalized Patients with Moderate to Severe COVID-19 (NOVATION-1). Available online: https://clinicaltrials.gov/ct2/show/NCT04669015 (accessed on 10 June 2021).
- Nebulised Rt-PA for ARDS due to COVID-19 (PACA). Available online: https://clinicaltrials.gov/ct2/show/NCT04356833 (accessed on 10 June 2021).
- Gong, Z. DAS181 for Severe COVID-19: Compassionate USE. Available online: https://clinicaltrials.gov/ct2/show/study/NCT04324489 (accessed on 17 June 2021).
- Sargramostim Use in COVID-19 to Recover Patient Health (SCOPE). Available online: https://clinicaltrials.gov/ct2/show/NCT04707664?term=immunotherapy%2C+inhalation&cond=Covid19&draw=2&rank=3 (accessed on 17 June 2021).
- Inhalon Biopharma Receives $7 Million from USAMRDC to Study Inhaled “Muco-Trapping” Antibody for the Treatment of COVID-19. Available online: https://www.inhalon.com/26may2021 (accessed on 17 June 2021).
- Gomez, A.I.; Acosta, M.F.; Muralidharan, P.; Yuan, J.X.J.; Black, S.M.; Hayes, D.; Mansour, H.M. Advanced spray dried proliposomes of amphotericin B lung surfactant-mimic phospholipid microparticles/nanoparticles as dry powder inhalers for targeted pulmonary drug delivery. Pulm. Pharmacol. Ther. 2020, 64, 101975. [Google Scholar] [CrossRef]
- Safety and Immunogenicity of AdCOVID in Healthy Adults (COVID-19 Vaccine Study). Available online: https://clinicaltrials.gov/ct2/show/NCT04679909 (accessed on 10 June 2021).
- Medzihradsky, O. Safety and Immunogenicity of an Intranasal RSV Vaccine Expressing SARS-CoV-2 Spike Protein (COVID-19 Vaccine) in Adults. Available online: https://clinicaltrials.gov/ct2/show/NCT04798001 (accessed on 10 June 2021).
- Safety and immunogenicity of an intranasal SARS-CoV-2 vaccine (BBV154) for COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04751682 (accessed on 10 June 2021).
- Zhu, F. Phase I/II Clinical Trial of Recombinant novel Coronavirus (COVID-19) Vaccine (Adenovirus Type 5 Vector) for Inhalation. Available online: https://clinicaltrials.gov/ct2/show/NCT04840992 (accessed on 10 June 2021).
- Douglas, A. A Study of Intranasal ChAdOx1 nCOV-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04816019 (accessed on 10 June 2021).
- Bendel, D. Safety and Immunogenicity of COVI-VAC, a Live Attenuated Vaccine Against COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04619628 (accessed on 10 June 2021).
- King, R.G.; Silva-Sanchez, A.; Peel, J.N.; Botta, D.; Meza-Perez, S.; Allie, S.R.; Schultz, M.D.; Liu, M.; Bradley, J.E.; Qiu, S.; et al. Single-dose intranasal administration of AdCOVID elicits systemic and mucosal immunity against SARS-CoV-2 in mice. bioRxiv 2020. [Google Scholar] [CrossRef]
- Stobart, C.C.; Rostad, C.A.; Ke, Z.; Dillard, R.S.; Hampton, C.M.; Strauss, J.D.; Yi, H.; Hotard, A.L.; Meng, J.; Pickles, R.J.; et al. A live RSV vaccine with engineered thermostability is immunogenic in cotton rats despite high attenuation. Nat. Commun. 2016, 7, 13916. [Google Scholar] [CrossRef]
- Rostad, C.A.; Stobart, C.C.; Gilbert, B.E.; Pickles, R.J.; Hotard, A.L.; Meng, J.; Blanco, J.C.; Moin, S.M.; Graham, B.S.; Piedra, P.A. A recombinant respiratory syncytial virus vaccine candidate attenuated by a low-fusion F protein is immunogenic and protective against challenge in cotton rats. J. Virol. 2016, 90, 7508–7518. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.O.; Kafai, N.M.; Dmitriev, I.P.; Fox, J.M.; Smith, B.K.; Harvey, I.B.; Chen, R.E.; Winkler, E.S.; Wessel, A.W.; Case, J.B. A single-dose intranasal ChAd vaccine protects upper and lower respiratory tracts against SARS-CoV-2. Cell 2020, 183, 169–184. [Google Scholar] [CrossRef]
- Bricker, T.; Darling, T.; Hassan, A.; Harastani, H.; Soung, A.; Jiang, X.; Dai, Y.-N.; Zhao, H.; Adams, L.; Holtzman, M. A single intranasal or intramuscular immunization with chimpanzee adenovirus vectored SARS-CoV-2 vaccine protects against pneumonia in hamsters. bioRxiv 2020. [Google Scholar] [CrossRef]
- Hassan, A.O.; Feldmann, F.; Zhao, H.; Curiel, D.T.; Okumura, A.; Tang-Huau, T.-L.; Case, J.B.; Meade-White, K.; Callison, J.; Chen, R.E.; et al. A single intranasal dose of chimpanzee adenovirus-vectored vaccine protects against SARS-CoV-2 infection in rhesus macaques. Cell Rep. Med. 2021, 2, 100230. [Google Scholar] [CrossRef]
- China Approves Inhaled CanSino Vaccine for Clinical Trials. Available online: https://medicalxpress.com/news/2021-03-china-inhaled-cansino-vaccine-clinical.html (accessed on 16 April 2021).
- Shabong, Y. Oxford to Test Inhaled Version of COVID-19 Vaccine with 30 Volunteers. Available online: https://www.reuters.com/article/us-health-coronavirus-astrazeneca-vaccin-idUSKBN2BH2PS (accessed on 10 June 2021).
- van Doremalen, N.; Purushotham, J.; Schulz, J.; Holbrook, M.; Bushmaker, T.; Carmody, A.; Port, J.; Yinda, K.C.; Okumura, A.; Saturday, G. Intranasal ChAdOx1 nCoV-19/AZD1222 vaccination reduces shedding of SARS-CoV-2 D614G in rhesus macaques. bioRxiv 2021. [Google Scholar] [CrossRef]
- COVI-VAC for SARS-CoV-2 (COVID-19): CODAGENIX INC. Available online: https://codagenix.com/vaccine-programs/covid-19/ (accessed on 10 June 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: Summary of a report of 72,314 cases from the chinese center for disease control and prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent symptoms in patients after acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Fraser, E. Long term respiratory complications of covid-19. BMJ 2020, 370, m3001. [Google Scholar] [CrossRef]
- A Study to Evaluate Ampion in Patients with Prolonged Respiratory Symptoms Due to COVID-19 (long COVID). Available online: https://clinicaltrials.gov/ct2/show/NCT04880161 (accessed on 19 June 2021).
- A Study of Inhaled Ampion in Adults with Respiratory Distress Due to COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04868890 (accessed on 21 June 2021).



{kind=link}
{kind=link}
| Coronavirus | SARS-CoV | MERS-CoV | SARS-CoV-2 |
|---|---|---|---|
| Disease | SARS | MERS | COVID-19 |
| Geographical Origin | Guangdong, China | Saudi Arabia | Hubei, China |
| Latency | 2–7 days | 2–14 days | 11.5 days (97.5% became symptomatic) |
| Contagious Period | 10 days after onset of disease | Once the virus isolated from infected patients | Unknown |
| Fatality Rate | ~10% | ~36% | ~2.3% |
| Reservoir | Bats | Bats | Bats |
| Incidental Host | Masked palm civets | Dromedary camels | Malayan pangolin |
| Transmission |
|
|
|
| Clinical Features | Starts as asymptomatic or mild disease, then acute upper respiratory distress and many organs’ failure leading to death. Individual’s variation. Vomiting and diarrhea are also reported. | ||
| Radiologic Features | Ground-glass opacity was the most common radiologic finding on chest computed tomography. Most patients also developed marked lymphopenia, similar to what was observed in patients with SARS and MERS [22] (Non-specific to distinguish between three different diseases). | ||
| Drug | Category | Chemical Nature | Mode of Action | Inhaled Dose and Formulation/Device |
|---|---|---|---|---|
| Remdesivir | Antiviral | Nucleoside analogue | RNA polymerase inhibitor | 31 mg and 62 mg (nebulizer) |
| Ciclesonide | Anti-inflammatory | Corticosteroid | Anti-inflammatory action | 800 μg/day (MDI, Alvesco) |
| Budesonide | Anti-inflammatory | Corticosteroid | Anti-inflammatory action | 800 µg twice daily for 14 days (DPI, Pulmicort Turbohaler) |
| Furosemide | Loop diuretic | Chlorobenzoic acid | Sodium-potassium-2 chloride (Na+-K+-2 Cl−) cotransporter inhibitor | 40 mg (nebulizer) |
| Nitric Oxide | Pulmonary vasodilator | Oxides of nitrogen | Increases intracellular cGMP | 250 µg/kg IBW/h (INOpulse®) |
| Epoprostenol | Pulmonary vasodilator | Prostaglandins I | Increases intracellular cAMP levels and antagonist of thromboxane A2 | VentaProst (inhaled epoprostenol delivered via a dedicated delivery system) |
| Hydroxychloroquine | Antimalarial | Derivative of chloroquine | Inhibits lysosomal function | 4, 8, 12 mg (nebulized) |
| Up to 50 mg (nebulized) | ||||
| 20 mg (dry powder) | ||||
| Plasminogen | Anticoagulant | Inert protein precursor | Thrombolytic | 10 mg in 2 mL sterile water, twice daily (nebulized) |
| Modified Angiotensin-Converting Enzyme 2 | Antiviral | Metallopeptidase | Regulates renin–angiotensin system and binds the viral spike protein and, thereby, neutralizes SARS-CoV-2 | Not available |
| Interferon-β | Antiviral agent | Signaling proteins | Protease inhibitor | 6 mIU of IFN-β |
| Anti-Microbial Colloidal Silver Formulations | Antimicrobial | Nano sized clusters of silver atoms | Destabilizes the cell membrane | 10 µg/mL (ultrasonic mesh nebulizer) |
| Unfractionated heparin (UFH) | Anticoagulant | Sulfur-rich glycosaminoglycan | Inhibit factor Xa and factor IIa | 25,000 IU/kg (Aeroneb Pro Nebulizer) |
| Salinomycin | Antibacterial agents | Polyketide | Inhibits endosomal acidification | Not available |
| Ivermectin | Antiparasitic drug | Macrocyclic lactone | Nuclear transport inhibitor | 380 mg/m3 (nebulized, dose in rats, no studies in humans) |
| Niclosamide | Antiparasitic agents | Benzamide | SKP2 inhibitor | Not yet released |
| Drug | Title, URL | Clinical Status | Interventions | Locations | References |
|---|---|---|---|---|---|
| Nitric oxide (NO) | Nitric oxide inhalation therapy for COVID-19 infections in the ED (NO COV-ED) | Phase 2 (Active, not recruiting) | Drug: Inhaled NO administered at target inspired concentration 140–300 ppm for 20–30 min Other: Inhaled supplemental oxygen | Massachusetts General Hospital, United States | [78] |
| Ciclesonide | Inhalation of ciclesonide for patients with COVID-19: A randomized open treatment study (HALT COVID-19) (HALT) | Phase 2 (recruiting) | Ciclesonide inhalation aerosol (320 µg) twice daily for 14 days | Karolinska University Hospital, Sweden | [79] |
| Inhaled ciclesonide for outpatients with COVID19 (CONTAIN) | Phase 3 (Recruiting) | Intranasal ciclesonide BID 50 µg BID to each nostril and inhaled ciclesonide 600 µg BID × 14 days | McGill University Health Center Montreal, Canada | [80] | |
| A study of the safety and efficacy of ciclesonide in the treatment of non-hospitalized COVID-19 patients | Phase 3 (completed) | 160 µg ciclesonide MDI | University of Buffalo, United States | [81] | |
| 99mTc-pertechnetate | Inhalation low dose radionuclide therapy in treatment COVID-19 | Phase 1 (Recruiting) | 99mTc-pertechnetate aerosol | P. Hertsen Moscow Oncology Research Institute, Russian Federation | [82] |
| UNI911 | Study to assess the safety of ascending doses of UNI911 inhalation in healthy volunteers in preparation for evaluation in adults with COVID-19 | Phase 1 (Active, not recruiting) | UNI911 inhalation (3.4 to 252 mg) | DanTrials, Denmark | [83] |
| Combination of 13 cis retinoic acid and captopril | Efficacy of aerosol combination therapy of 13 cis retinoic acid and captopril for treating COVID-19 patients via indirect inhibition of transmembrane protease, serine 2 (TMPRSS2) | Phase 2 (Not yet recruiting) | 13 cis retinoic acid: gradual dose increases from 0.2 to 4 mg/kg/day for 14 days Captopril: 25 mg for 14 days | Kafrelsheikh University, Egypt | [84] |
| Combination of 13 cis retinoic acid and Tamoxifen | Combination of chemo preventive agents (all-trans retinoic acid and tamoxifen) as potential treatment for the lung complication of COVID-19 | Phase 2 (Not yet recruiting) | 13 cis retinoic acid: gradual dose increases from 0.2 to 4 mg/kg/day for 14 days Tamoxifen: 20 mg orally once daily for 14 days | Kafrelsheikh University, Egypt | [85] |
| Combination therapy with isotretinoin and tamoxifen expected to provide complete protection against severe acute respiratory syndrome coronavirus (combination) | Phase 2 (Not yet recruiting) | 13 cis retinoic acid: gradual dose increases from 0.2 to 4 mg/kg/day for 14 days Tamoxifen: 20 mg orally once daily for 14 days | Kafrelsheikh University, Egypt | [86] | |
| Combination of 13 cis retinoic acid and testosterone | Clinical role of testosterone and dihydrotestosterone and which of them should be inhibited in COVID-19 patients—a double-edged sword? | Phase 4 (Not yet recruiting) | Aerosolized 13 cis retinoic acid: gradual dose increases from 0.2 to 4 mg/kg/day for 14 days Inhaled testosterone: 0.1, 0.2, or 0.3 mg for 14 days | Kafrelsheikh University, Egypt | [87] |
| Combination of 13 cis retinoic acid and itraconazole | Efficacy and safety of drug combination therapy of isotretinoin and some antifungal drugs as a potential aerosol therapy for COVID-19: An innovative therapeutic approach COVID-19 (isotretinoin) | Phase 2 (Not yet recruiting) | 13 cis retinoic acid: gradual dose increases from 0.2 to 4 mg/kg/day for 14 days Itraconazole: 5 mg per day for 14 days | Kafrelsheikh University, Egypt | [88] |
| Combination of thalidomide with low-dose hormones | The efficacy and safety of thalidomide combined with low-dose hormones in the treatment of severe COVID-19 | Phase 2 (Not yet recruiting) | α-interferon: nebulized inhalation, 5 million U or equivalent dose added 2 mL of sterile water for injection, 2 times a day, for 7 days; Abidol, 200 mg, 3 times a day, for 7 days; Methylprednisolone: 40 mg, q12hq12h for 5 days; thalidomide: 100mg, qn, for 14 days. | - | [89] |
| Combination of All-trans Retinoic Acid and Isotretinoin | Aerosol combination therapy of all-trans retinoic acid and isotretinoin as a novel treatment for inducing neutralizing antibodies in COVID -19 infected patients better than vaccine: An innovative treatment (antibodies) | Phase 2 (Not yet recruiting) | Gradual increase in dose of All-trans Retinoic Acid and Isotretinoin from 0.2 to 4 mg/kg/day for 14 days | Kafrelsheikh University, Egypt | [90] |
| Ethanol | New treatment for COVID-19 using ethanol vapor inhalation | Phase 3 (Not yet recruiting) | Controlled ethanol vapor inhalation combined with oral aspirin | Mansoura University, Egypt | [91] |
| Aviptadil | A clinical study evaluating inhaled aviptadil on COVID-19 (HOPE) | Phase 2 (Recruiting) | Inhaled aviptadil 2 times a day, 30 min apart | Centurion Pharma, Turkey | [92] |
| Inhaled aviptadil for the prevention of COVID-19 related ARDS | Phase 1 (Recruiting) | 67 μg nebulized aviptadil 3 times a day for 10 days | Cantonal Hospital Baselland Liestal Liestal, Switzerland | [93] | |
| Inhaled ZYESAMI™ (aviptadil acetate) for the treatment of moderate and severe COVID-19 (AVICOVID-2) | Phase 2 (Recruiting) | Inhaled ZYESAMI™ (aviptadil acetate) 100 μg 3× daily by mesh nebulizer | St. Jude Medical Center Fullerton, United States | [94] | |
| Ivermectin | Ivermectin nasal spray for COVID-19 patients. | Phase 2 (Not yet recruiting) | Ivermectin nasal spray (1 mL) in each nostril BID vs. Ivermectin oral (6 mg) TID vs. SC | Tanta University, Tanta, Egypt | [67] |
| Inhaled ivermectin and COVID-19 (CCOVID-19) | Phase 3 (Recruiting) | Ivermectin inhalation powder (6 mg) BID for 3 days | Mansoura University, Egypt | [95] | |
| Iloprost | Inhaled iloprost for suspected COVID-19 respiratory failure (ILOCOVID) | Phase 2 (Recruiting) | Inhaled iloprost 20 µg every 8 h for 5 days only delivered by nebulization | Hamad Medical Corporation, Qatar | [96] |
| TD-0903 | First in human SAD and MAD study of inhaled TD-0903, a potential treatment for ALI associated with COVID-19 | Phase 1 (Completed) | Inhaled TD-0903 | Theravance Biopharma Investigational Site, United Kingdom | [97] |
| Inteferon Beta 1b | Treatment of COVID-19 by nebulization of inteferon beta 1b efficiency and safety study (COV-NI) | Phase 2 (Recruiting) | Inhaled interferon (9.6 MUI × 2/d for 48 h, then 9.6 MUI ×1/d for 8 to 16 days | Centre Hospitalier Universitaire, France | [98] |
| Budesonide | Inhaled corticosteroid treatment of COVID-19 patients with pneumonia | Phase 4 (Recruiting) | Inhaled budesonide | Infectious Diseases Hospital “Dr. Francisco Javier Muñiz”, Argentina | [99] |
| Steroids in COVID-19 study (STOIC) | Phase 2 (Terminate) | Budesonide inhaled via dry powder inhaler, 400 µg per inhalation, 2 inhalations twice a day | University of Oxford, United Kingdom | [100] | |
| Formoterol + Budesonide and Levamisole | Evaluation of efficacy of levamisole and formoterol + budesonide in treatment of COVID-19 | Phase 2 (Recruiting) | Levamisole Pill (50 mg) + Budesonide + Formoterol inhaler (1–2 puffs every 12 h) | Vali-Asr Hospital Fasa, Fars, Iran | [101] |
| Inhaled Steroids (combination of budesonide and formoterol) | Protective role of inhaled steroids for COVID-19 infection (INHASCO) | Phase 3 (Recruiting) | Symbicort Rapihaler, 2 puffs bid during 30 days by inhalation | Bichat-Claude-Bernard Hospital, Pneumology Department, France | [102] |
| Arrest respiratory failure from pneumonia (ARREST) | Phase 3 (Enrolling by invitation) | Aerosolized doses of budesonide (1.0 mg/2 mL) and formoterol (20 mg/2 mL) twice daily for up to 5 days | Mayo Clinic—Scottsdale, Arizona, United States; University of Arizona, Arizona, United States | [103] | |
| Melphalan | Low-doses melphalan inhalation in patients with COVID-19 (Coronavirus Disease 2019) pneumonia (MICOV) | Phase 2 (Recruiting) | Inhalations with low doses of melphalan for 7–10 consequent days | Kirill Zykov, Russian Federation | [104] |
| Epoprostenol | VentaProst in subjects with COVID-19 requiring mechanical ventilation (VPCOVID) | Phase 2 (Recruiting) | VentaProst delivered for up to 10 days via mechanical ventilation at a dose range that may be up or down titrated to a patient’s clinical condition | Ohio State University, United States | [105] |
| Heparin | Nebulized heparin for the treatment of COVID-19 (INHALE-HEP) | Phase 4 (Enrolling by invitation) | 25,000 units of unfractionated heparin nebulized 4 times daily for the duration of hospitalization | Frederick Health Hospital, United States | [106] |
| Inhaled heparin for hospitalized COVID-19 patients (INHALE-HEP) | Phase 2 Phase 3 (Recruiting) | Inhaled nebulized at a dose 25,000 IU every 6 h for up to 21 days | San Camilo Clinic, Argentina | [107] | |
| Mesenchymal stem cells (MSCs) | A pilot clinical study on inhalation of mesenchymal stem cells exosomes treating severe novel coronavirus pneumonia | Phase 1 (Completed) | Inhalation of MSCs-derived exosomes (2.0×108 nano vesicles/3 mL at Day 1, Day 2, Day 3, Day 4, Day 5) | Ruijin Hospital, China | [108] |
| SNG001 | Trial of inhaled anti-viral (SNG001) for SARS-CoV-2 (COVID-19) infection | Phase 2 (Active, not recruiting) | SNG001 via inhalation | Belfast City Hospital, United Kingdom | [109] |
| Dornase Alfa | Dornase alfa for ARDS in patients with severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) (DORNASESARS2) | Phase 3 (Completed) | Inhaled/nebulized dornase alfa (Pulmozyme) 2.5 mg twice daily in the ventilator circuit for 3 days | University of Missouri Hospital and Clinics, United States | [110] |
| Nebulized dornase alfa for treatment of COVID-19 (COVASE) | Phase 2 (Recruiting) | Nebulized Dornase alfa 2.5 mg bd for 7 days | University College London Hospital, United Kingdom | [111] | |
| Dalargin | An open randomized study of dalargin effectiveness in patients with severe and critical manifestations of SARS-COVID-19 | Phase 3 (Completed) | inhalation of the drug Dalargin, at a dose of 10 mg daily once per day | Burnasyan Federal Medical Biophysical Center FMBA of Russia, Russian Federation | [112] |
| Sodium Pyruvate | Sodium pyruvate nasal spray treatment of COVID-19 and influenza infections | Phase 3 (Recruiting) | Sodium pyruvate nasal spray 3× daily for 14 days | Family First Medical Research Center, Unites States; Missouri State University, Unites States | [113] |
| Hydroxychloroquine | The potential use of inhaled hydroxychloroquine for the treatment of COVID-19 in cancer patients | Phase 1 Phase 2 (Not yet recruiting) | 2 mL hydroxychloroquine (12.5 mg/mL) twice a day for 5 consecutive days. | King Hussein Cancer Center, Jordan | [114] |
| Development and validation of “ready-to-use” inhalable forms of hydroxychloroquine for treatment of COVID-19 | Not Applicable (Active, not recruiting) | Nebulized hydroxychloroquine Loading dose: day 1, 12 mg TID Maintenance dose: day 2–5, 12 mg BID | Mansoura University Hospital, Egypt | [115] | |
| A study to evaluate the safety, tolerability and pharmacokinetics of orally inhaled aerosolized hydroxychloroquine sulfate in healthy adult volunteers | Phase 1 (Completed) | Sterile aerosolized hydroxychloroquine sulfate 100 mg/mL for inhalation | The Rockefeller University New York, United States | [116] | |
| PUL-042 (a combination of two synthetic Toll-like receptor agonist molecules Pam2 and ODN) | The use of PUL-042 inhalation solution to reduce the severity of COVID-19 in adults positive for SARS-CoV-2 infection | Phase 2 (Recruiting) | 20.3 µg Pam2: 29.8 µg ODN/mL (50 µg PUL-042) PUL-042 inhalation solution | University of California, United States | [117] |
| Hyaluronan | Use of inhaled high-molecular weight hyaluronan in patients with severe COVID19: Feasibility and outcomes (HA-COVID) | Phase 2 (Recruiting) | 5 mL of saline containing 0.3% hyaluronic acid sodium salt via nebulizer b.i.d. | University of Rome Bio-Medical Campus, Italy | [118] |
| Remdesivir | Study in participants with early-stage coronavirus disease 2019 (COVID-19) to evaluate the safety, efficacy, and pharmacokinetics of remdesivir administered by inhalation | Phase 1 (Completed) | Remdesivir (31–62 mg) administered as an aerosolized solution daily for 5 days | The Institute for Liver Health Mesa, United States | [119] |
| Ensifentrine | Study of ensifentrine or placebo delivered via pMDI in hospitalized patients with COVID-19 | Phase 2 (Active, not recruiting) | Ensifentrine delivered twice daily via pMDI | The University of Alabama at Birmingham, United States | [120] |
| Furosemide | Furosemide as supportive therapy for COVID-19 respiratory failure (FaST-1) | Phase 2 (Recruiting) | 40 mg furosemide per dose, given by nebulization (4 mL of 10 mg/mL furosemide in 0.9% saline solution) over 30 min four times daily (Q6h) for up to 28 days | University of Alberta Edmonton, Alberta, Canada | [121] |
| Novaferon | Phase 3 inhaled novaferon study in hospitalized patients with moderate to severe COVID-19 (NOVATION-1) | Phase 3 (Not yet recruiting) | Inhaled Novaferon, given 20 ug BID, daily for 10 days | Cardiovascular Foundation of Colombia, Floridablanco Heart Institute, Colombia | [122] |
| Tissue plasminogen activator (rt-PA) | Nebulized Rt-PA for ARDS due to COVID-19 (PACA) | Phase 2 (Recruiting) | 10 mg rt-PA in 5 mL diluent will be administered by nebulization every 6 h for 14 days | Barnet Hospital, United Kingdom | [123] |
| DAS181 | DAS181 for severe COVID-19: compassionate use | Not applicable | Nebulized DAS181 (4.5 mg BID/day, a total 9 mg/day) for 10 days | Renmin Hospital of Wuhan University, Wuhan, Hubei, China | [124] |
| Sargramostim | Sargramostim use in COVID-19 to recover patient health (SCOPE) | Phase 2 (Recruiting) | 250 µg inhaled sargramostim administered via a vibrating mesh nebulizer once daily for 5 days. | Partner Therapeutics, Inc., United States | [125] |
| IN-006 | Inhaled “muco-trapping” antibody for the treatment of COVID-19 | Phase 1/2a | Not available | Inhalon Biopharma, North Carolina, United States | [126] |
| Sponsor | Product | Vector | Trial ID | Preclinical Results | References |
|---|---|---|---|---|---|
| Altimmune | AdCOVID | Replication deficient adenovirus 5 (RD- Ad5) | NCT04679909 | Strong immune activation after a single intranasal dose: serum neutralizing activity (IgG, IgA and T cell immunity and mucosal immunity. | [128] |
| Meissa vaccine | MV-014-212 | Respiratory syncytial virus (RSV) surface proteins were replaced with the SARS-CoV-2 Spike protein by AttenuBlock platform. | NCT04798001 | IgA and serum neutralization antibodies against spike-expression virus and provided protection against SARS-CoV-2 in the upper and lower respiratory tract | [129] |
| -Bharat Biotech -Precision Virologics -University of Wisconsin | CoroFlu (BBV154) | Chimpanzee Adenovirus based SARS-CoV2 | NCT04751682 | A single intranasal dose of ChAd-SARS-CoV-2 induced neutralizing antibodies and T cell responses and limited or prevented infection in the upper and lower respiratory tract after SARS-CoV-2 challenge. | [130] |
| CanSino Biologics | Ad5-nCoV | Adenovirus type 5 vector that expresses S protein | NCT04840992 | ELISA antibodies and neutralizing antibodies increased significantly at day 14 and peaked 28 days post-vaccination. Specific T-cell response peaked at day 14 post-vaccination for the IM injection. | [131] |
| AstraZeneca | AZD12222 | Defective chimpanzee adenovirus expressing the SARS-CoV-2 surface glycoprotein | NCT04816019 | Significant decrease in viral load in bronchoalveolar lavage and lower respiratory tract tissue | [132] |
| Codagenix Inc. | COVI-VAC | Attenuated wild-type SARS-CoV-2 | NCT04619628 | Designed to produce immunity against all SARS-CoV-2 proteins, not just the spike surface protein. | [133] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Ledford, J.G.; Mansour, H.M. Inhalation Delivery for the Treatment and Prevention of COVID-19 Infection. Pharmaceutics 2021, 13, 1077. https://doi.org/10.3390/pharmaceutics13071077
Eedara BB, Alabsi W, Encinas-Basurto D, Polt R, Ledford JG, Mansour HM. Inhalation Delivery for the Treatment and Prevention of COVID-19 Infection. Pharmaceutics. 2021; 13(7):1077. https://doi.org/10.3390/pharmaceutics13071077
Chicago/Turabian StyleEedara, Basanth Babu, Wafaa Alabsi, David Encinas-Basurto, Robin Polt, Julie G. Ledford, and Heidi M. Mansour. 2021. "Inhalation Delivery for the Treatment and Prevention of COVID-19 Infection" Pharmaceutics 13, no. 7: 1077. https://doi.org/10.3390/pharmaceutics13071077