
A Perspective on Imiquimod Microneedles for Treating Warts

 ,
, 
 and
and 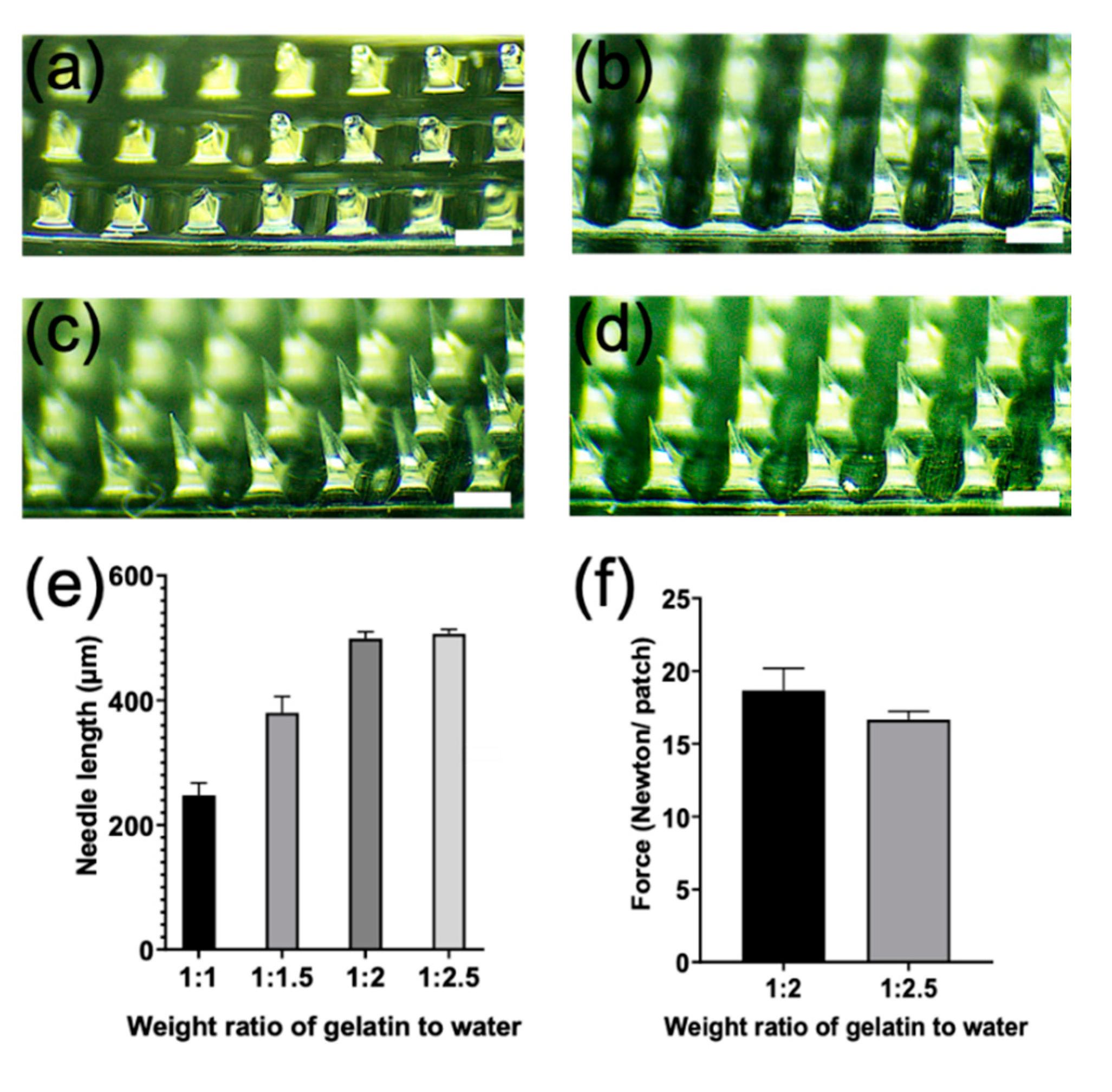{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Imiquimod Microneedle Patch
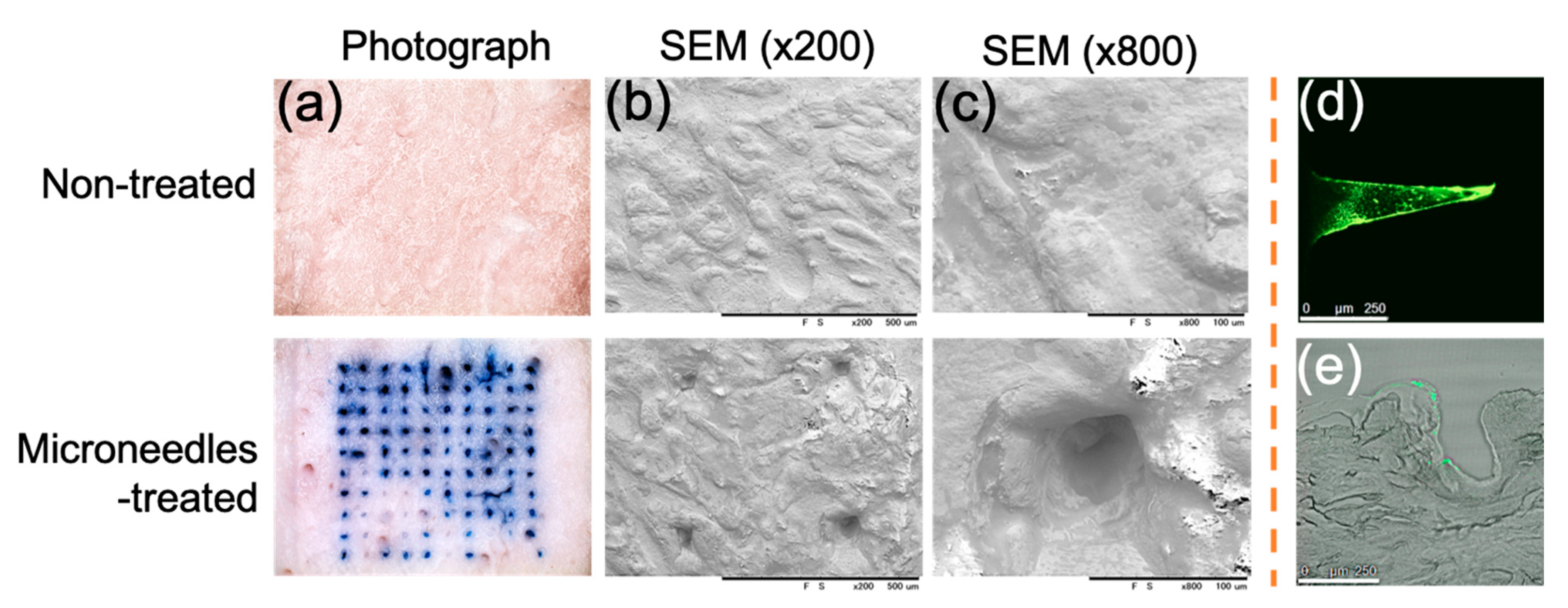
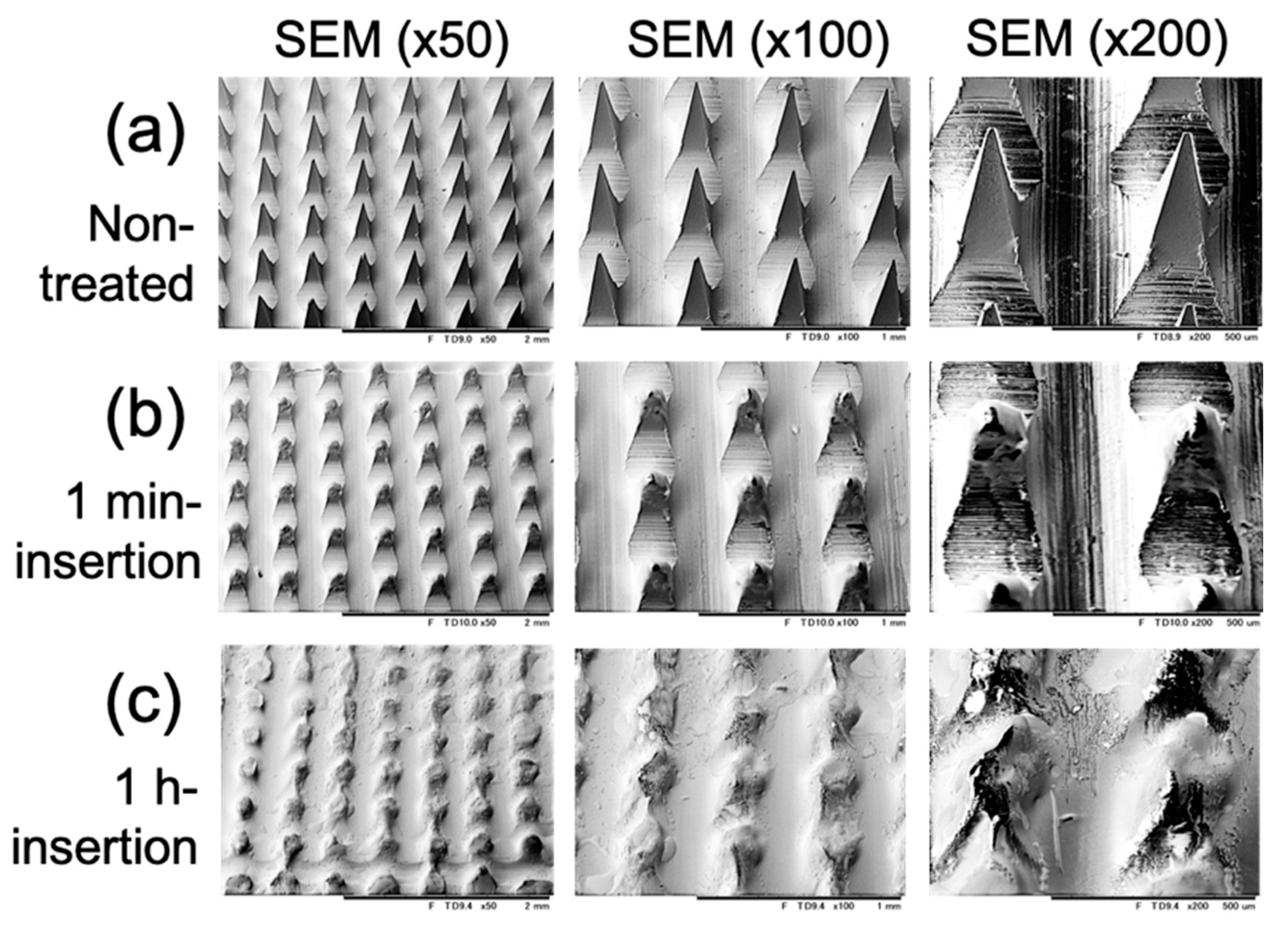
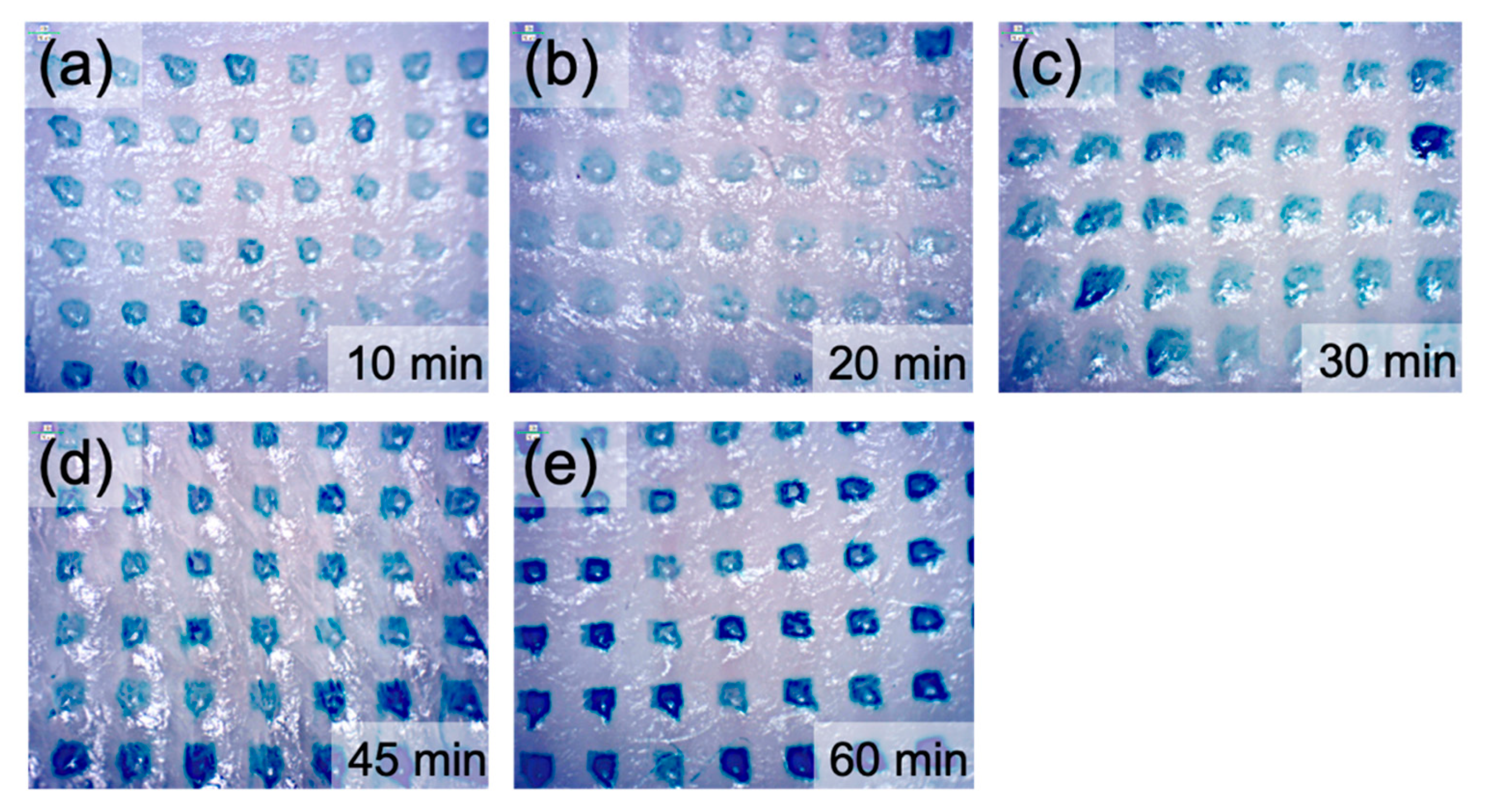
2.2. In Vitro Insertion Capability
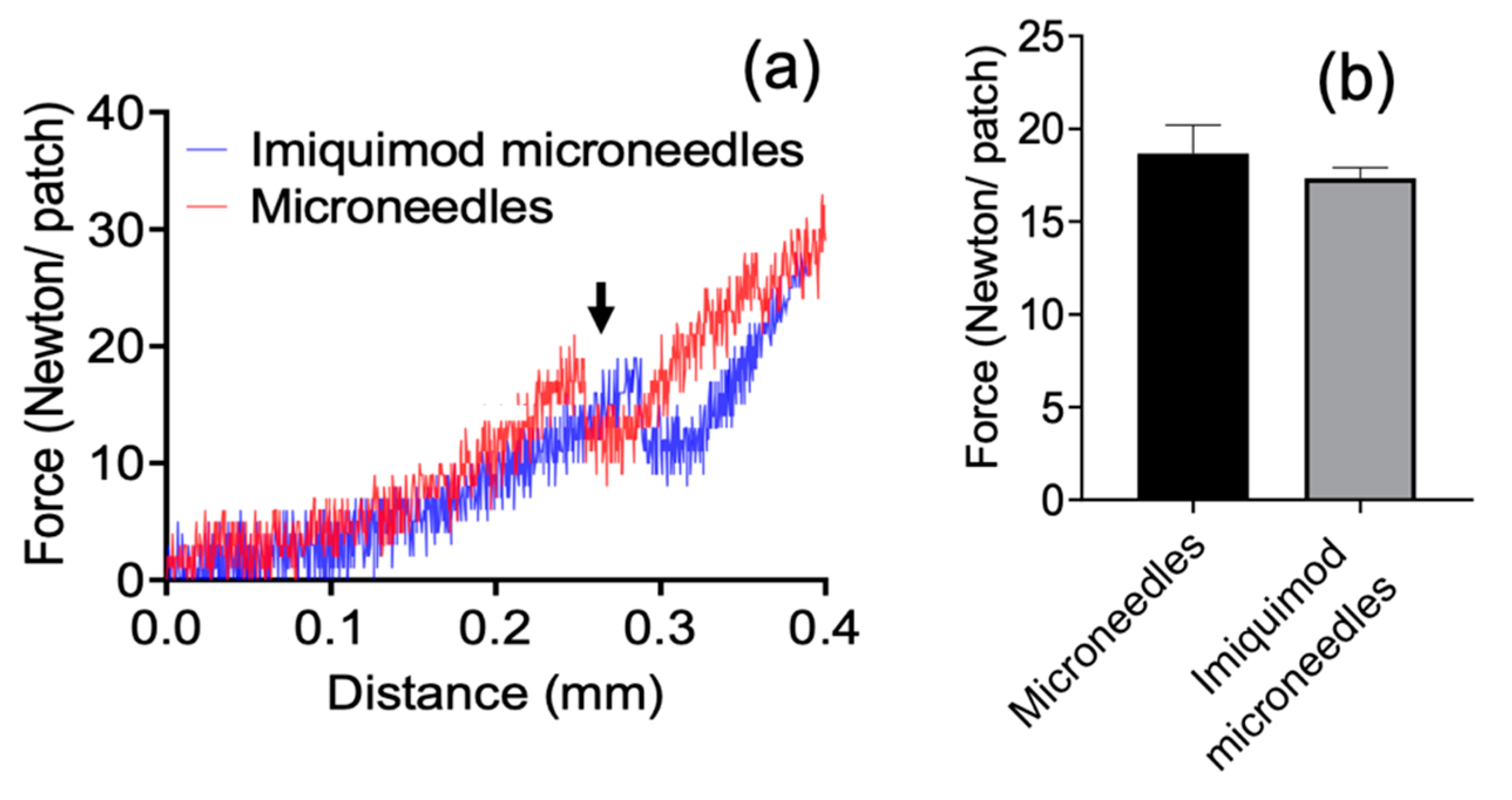
2.3. Mechanical Strength
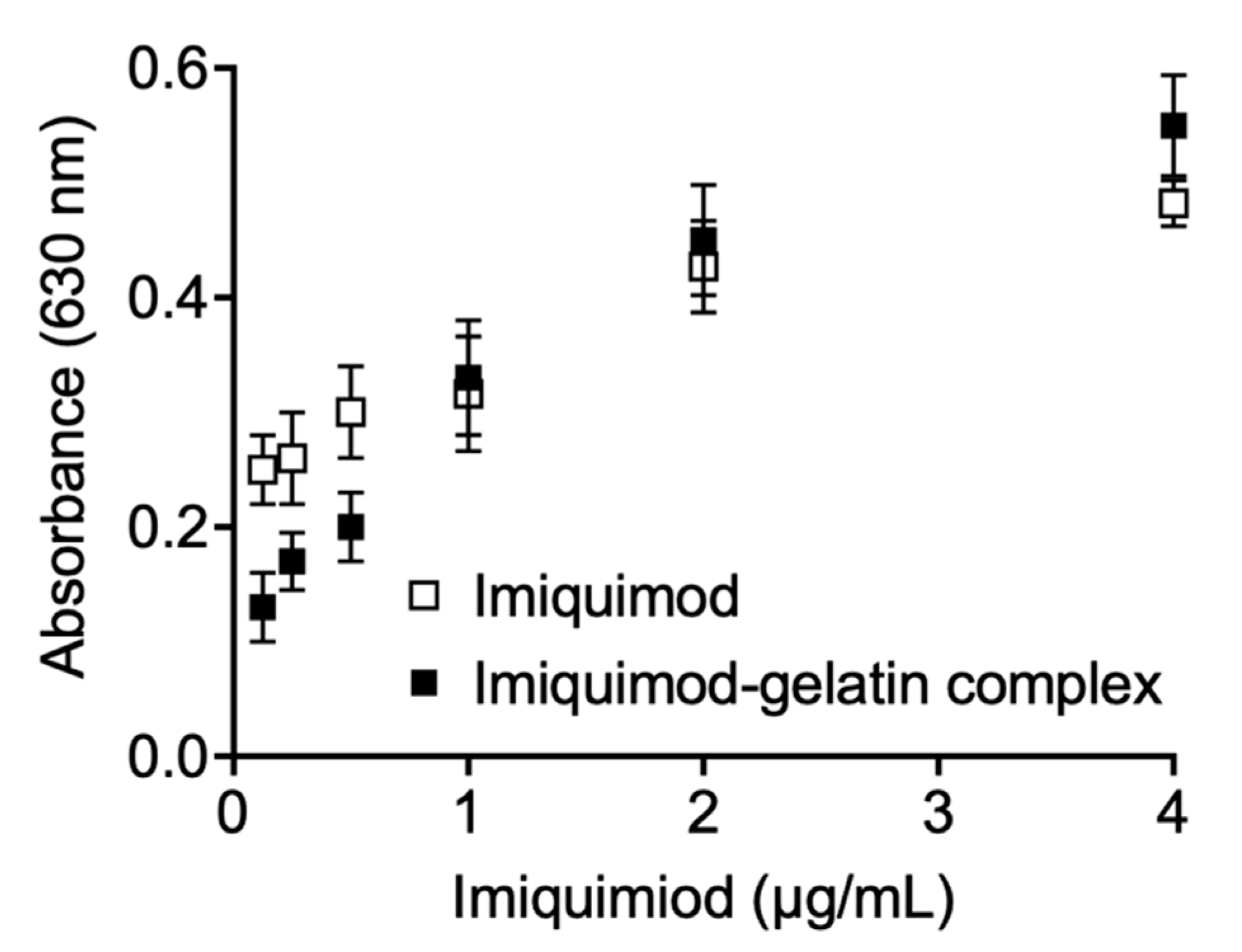
2.4. In-Vitro Immune Response
3. Results
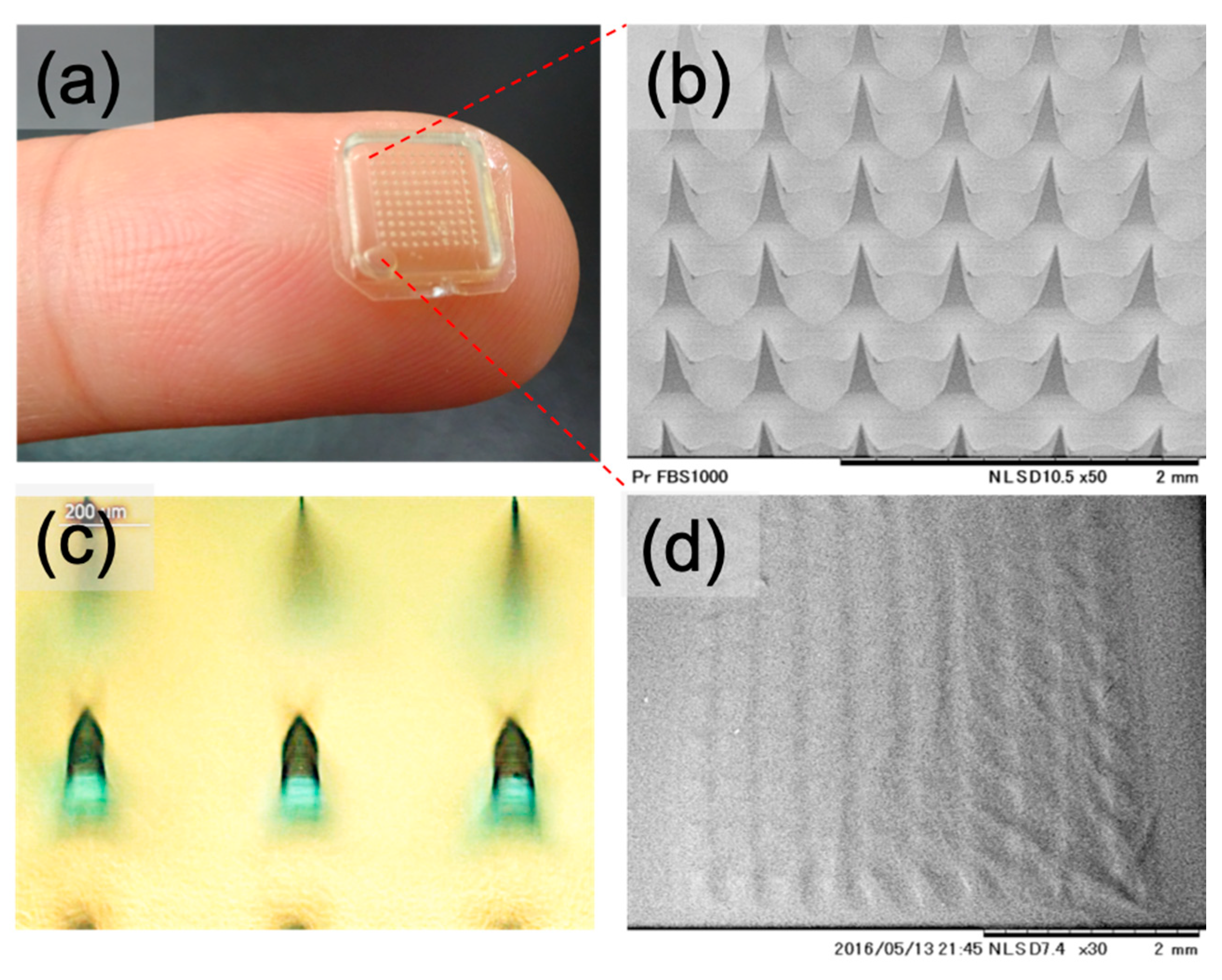
3.1. Preparing and Characterization of Gelatin Microneedle Patch
3.2. Mechanical Strength
3.3. In Vitro Immune Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Y.H.; Su, H.Y.; Hsieh, Y.J. Survey of infectious skin diseases and skin infestations among primary school students of Taitung County, Eastern Taiwan. J. Formos. Med. Assoc. 2000, 99, 128–134. [Google Scholar]
- Berth-Jones, J.; Bourke, J.; Eglitis, H.; Harper, C.; Kirk, P.; Pavord, S.; Rajapakse, R.; Weston, P.; Wiggins, T.; Hutchinson, P.E. Value of a second freeze-thaw cycle in cryotherapy of common warts. Br. J. Dermatol. 1994, 131, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Leerunyakul, K.; Thammarucha, S.; Suchonwanit, P.; Rutnin, S. A comprehensive review of treatment options for recalcitrant nongenital cutaneous warts. J. Dermatolog. Treat. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Hengge, U.R.; Esser, S.; Schultewolter, T.; Behrendt, C.; Meyer, T.; Stockfleth, E.; Goos, M. Self-administered topical 5% imiquimod for the treatment of common warts and molluscum contagiosum. Br. J. Dermatol. 2000, 143, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Vidal, D.A. Topical imiquimod: Mechanism of action and clinical applications. Min-Rev. Med. Chem. 2006, 6, 499–503. [Google Scholar] [CrossRef]
- Bhatnagar, S.; Gadeela, P.R.; Thathireddy, P.; Venuganti, V.V.K. Microneedle-based drug delivery: Materials of construction. J. Chem. Sci. 2019, 131, 90. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Sanchez, G.; Pavot, V.; Chane-Haong, C.; Handke, N.; Terrat, C.; Gigmes, D.; Trimaille, T.; Verrier, B. Preparation and in vitro evaluation of imiquimod loaded polylactide-based micelles as potential vaccine adjuvants. Pharm. Res. 2015, 32, 311–320. [Google Scholar] [CrossRef]
- Cu, K.; Bansal, R.; Mitragotri, S.; Fernandez Rivas, D. Delivery strategies for skin: Comparison of nanoliter jets, needles and topical solutions. Ann. Biomed. Eng. 2020, 48, 2028–2039. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Zeng, H.; Sun, J.; Qian, W. Engineering microneedles for therapy and diagnosis: A survey. Micromachines 2020, 11, 271. [Google Scholar] [CrossRef] [Green Version]
- de Groot, A.M.; Platteel, A.C.M.; Kuijt, N.; van Kooten, P.J.S.; Vos, P.J.; Sijts, A.J.A.M.; van der Maaden, K. Nanoporous microneedle arrays effectively induce antibody responses against diphtheria and tetanus toxoid. Front. Immunol. 2017, 8, 1789. [Google Scholar] [CrossRef] [Green Version]
- Queiroz, M.L.B.; Shanmugam, S.; Santos, L.N.S.; Campos, C.A.; Santos, A.M.; Batista, M.S.; Araujo, A.A.S.; Serafini, M.R. Microneedles as an alternative technology for transdermal drug delivery systems: A patent review. Expert Opin. Ther. Pat. 2020, 30, 433–452. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, X.; Fu, Y.; Song, Y. Recent advances of microneedles for biomedical applications: Drug delivery and beyond. Acta Pharm. Sin. B 2019, 9, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, I.; Lai, J.; Ranamukhaarachchi, S.; Schmitt, V.; Lambert, D.; Dutz, J.; Hafeli, U.O.; Stoeber, B. A microneedle-based method for the characterization of diffusion in skin tissue using doxorubicin as a model drug. Biomed. Microdevices 2015, 17, 9967. [Google Scholar] [CrossRef]
- Lee, H.S.; Ryu, H.R.; Roh, J.Y.; Park, J.H. Bleomycin-coated microneedles for treatment of warts. Pharm. Res. 2017, 34, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.R.; Jeong, H.-R.; Seon-Woo, H.-S.; Kim, J.S.; Lee, S.K.; Kim, H.J.; Baek, J.O.; Park, J.-H.; Roh, J.Y. Efficacy of a bleomycin microneedle patch for the treatment of warts. Drug Deliv. Transl. Res. 2017, 8, 273–280. [Google Scholar] [CrossRef]
- Kim, J.S.; Choi, J.A.; Kim, J.C.; Park, H.; Yang, E.; Park, J.S.; Song, M.; Park, J.H. Microneedles with dual release pattern for improved immunological efficacy of Hepatitis B vaccine. Int. J. Pharm. 2020, 591, 119928. [Google Scholar] [CrossRef]
- Leone, M.; Romeijn, S.; Slutter, B.; O’Mahony, C.; Kersten, G.; Bouwstra, J.A. Hyaluronan molecular weight: Effects on dissolution time of dissolving microneedles in the skin and on immunogenicity of antigen. Eur. J. Pharm. Sci. 2020, 146, 105269. [Google Scholar] [CrossRef]
- Nakaoka, R.; Tabata, Y.; Ikada, Y. Potentiality of gelatin microsphere as immunological adjuvant. Vaccine 1995, 13, 653–661. [Google Scholar] [CrossRef]
- Yasmin, R.; Shah, M.; Khan, S.A.; Ali, R. Gelatin nanoparticles: A potential candidate for medical applications. Nanotechnol. Rev. 2017, 6, 191–207. [Google Scholar] [CrossRef]
- Lutton, R.E.M.; Moore, J.; Larrañeta, E.; Ligett, S.; Woolfson, A.D.; Donnelly, R.F. Microneedle characterisation: The need for universal acceptance criteria and GMP specifications when moving towards commercialisation. Drug Deliv. Transl. Res. 2015, 5, 313–331. [Google Scholar] [CrossRef] [Green Version]
- Yu, R.C.; Abrams, D.C.; Alaibac, M.; Chu, A.C. Morphological and quantitative analyses of normal epidermal Langerhans cells using confocal scanning laser microscopy. Br. J. Dermatol. 1994, 131, 843–848. [Google Scholar] [CrossRef]
- Haj-Ahmad, R.; Khan, H.; Arshad, M.S.; Rasekh, M.; Hussain, A.; Walsh, S.; Li, X.; Chang, M.W.; Ahmad, Z. Microneedle coating techniques for transdermal drug delivery. Pharmaceutics 2015, 7, 486–502. [Google Scholar] [CrossRef] [Green Version]
- Marren, K. Dimethyl sulfoxide: An effective penetration enhancer for topical administration of NSAIDs. Phys. Sportsmed. 2011, 39, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Graziola, F.; Candido, T.M.; Oliveira, C.A.D.; Peres, D.D.A.; Issa, M.G.; Mota, J.; Rosado, C.; Consiglieri, V.O.; Kaneko, T.M.; Velasco, M.V.R.; et al. Gelatin-based microspheres crosslinked with glutaraldehyde and rutin oriented to cosmetics. Braz. J. Pharm. Sci. 2016, 52, 603–612. [Google Scholar] [CrossRef] [Green Version]
- Davis, S.P.; Landis, B.J.; Adams, Z.H.; Allen, M.G.; Prausnitz, M.R. Insertion of microneedles into skin: Measurement and prediction of insertion force and needle fracture force. J. Biomech. 2004, 37, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Loizidou, E.Z.; Williams, N.A.; Barrow, D.A.; Eaton, M.J.; McCrory, J.; Evans, S.L.; Allender, C.J. Structural characterisation and transdermal delivery studies on sugar microneedles: Experimental and finite element modelling analyses. Eur. J. Pharm. Biopharm. 2015, 89, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Tyring, S.K.; Arany, I.I.; Stanley, M.A.; Stoler, M.H.; Tomai, M.A.; Miller, R.L.; Owens, M.L.; Smith, M.H. Mechanism of action of imiquimod 5% cream in the treatment of anogenital warts. Prim. Care Update Ob Gyns 1998, 5, 151–152. [Google Scholar] [CrossRef]
- Telo, I.; Pescina, S.; Padula, C.; Santi, P.; Nicoli, S. Mechanisms of imiquimod skin penetration. Int. J. Pharm. 2016, 511, 516–523. [Google Scholar] [CrossRef]
- Sabri, A.; Ogilvie, J.; McKenna, J.; Segal, J.; Scurr, D.; Marlow, M. Intradermal delivery of an immunomodulator for basal cell carcinoma; expanding the mechanistic insight into solid microneedle-enhanced delivery of hydrophobic molecules. Mol. Pharm. 2020, 17, 2925–2937. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.; Gogoll, K.; Tenzer, S.; Schild, H.; Stevanovic, S.; Langguth, P.; Radsak, M.P. Efficacy of imiquimod-based transcutaneous immunization using a nano-dispersed emulsion gel formulation. PLoS ONE 2014, 9, e102664. [Google Scholar] [CrossRef] [Green Version]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, T.-M.; Hsu, P.-C.; Khan, M.Y.; Lin, C.-A.J.; Lee, C.-H.; Hsu, T.-C.; Chen, M.-H.; Hanagata, N. A Perspective on Imiquimod Microneedles for Treating Warts. Pharmaceutics 2021, 13, 607. https://doi.org/10.3390/pharmaceutics13050607
Chiu T-M, Hsu P-C, Khan MY, Lin C-AJ, Lee C-H, Hsu T-C, Chen M-H, Hanagata N. A Perspective on Imiquimod Microneedles for Treating Warts. Pharmaceutics. 2021; 13(5):607. https://doi.org/10.3390/pharmaceutics13050607
Chicago/Turabian StyleChiu, Tsu-Man, Ping-Chun Hsu, Mohd Yaqub Khan, Cheng-An J. Lin, Chun-Hung Lee, Tsai-Ching Hsu, Min-Hua Chen, and Nobutaka Hanagata. 2021. "A Perspective on Imiquimod Microneedles for Treating Warts" Pharmaceutics 13, no. 5: 607. https://doi.org/10.3390/pharmaceutics13050607