
Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
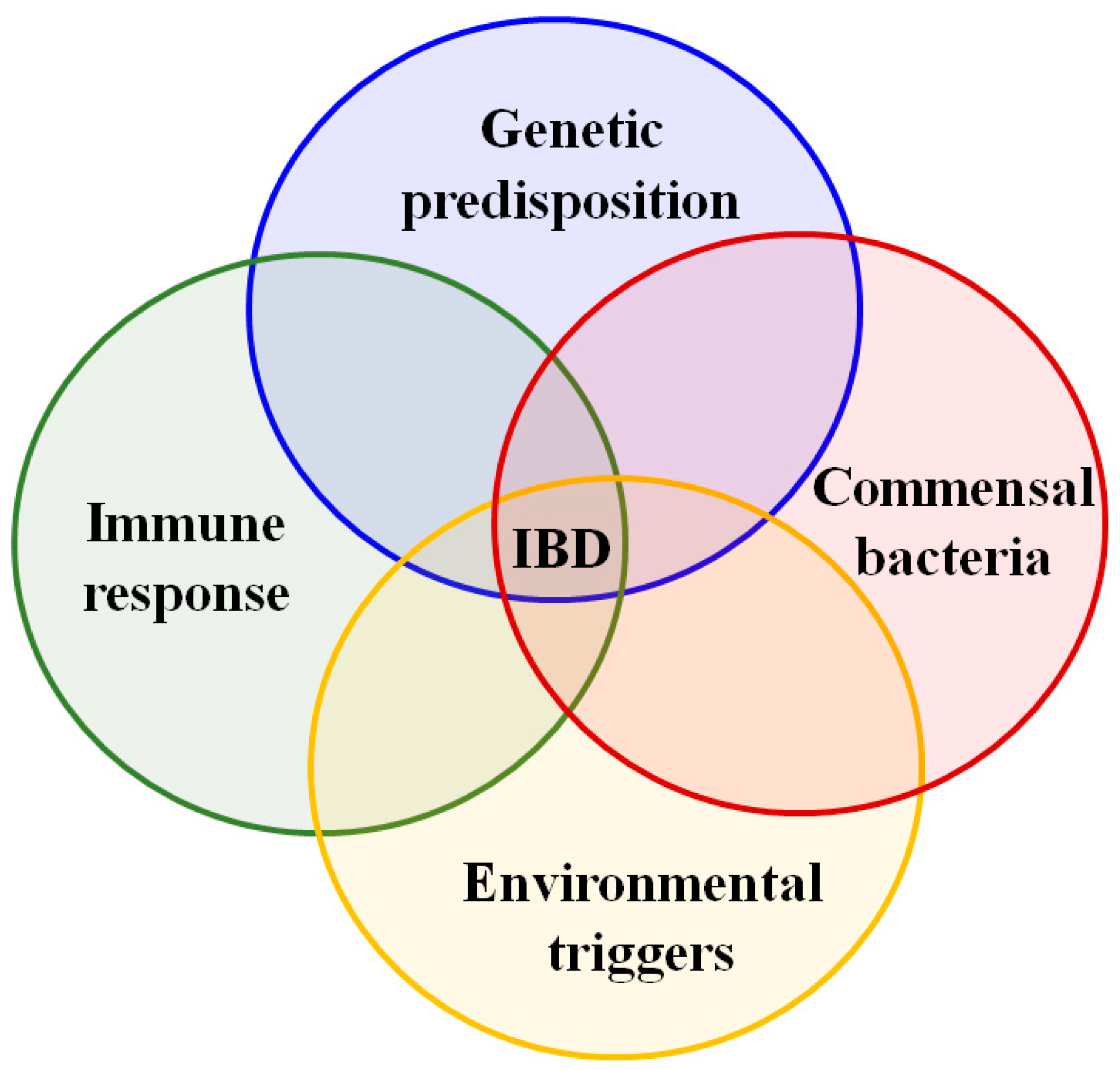
2. Genetics and Pathogenesis of Inflammatory Bowel Disease
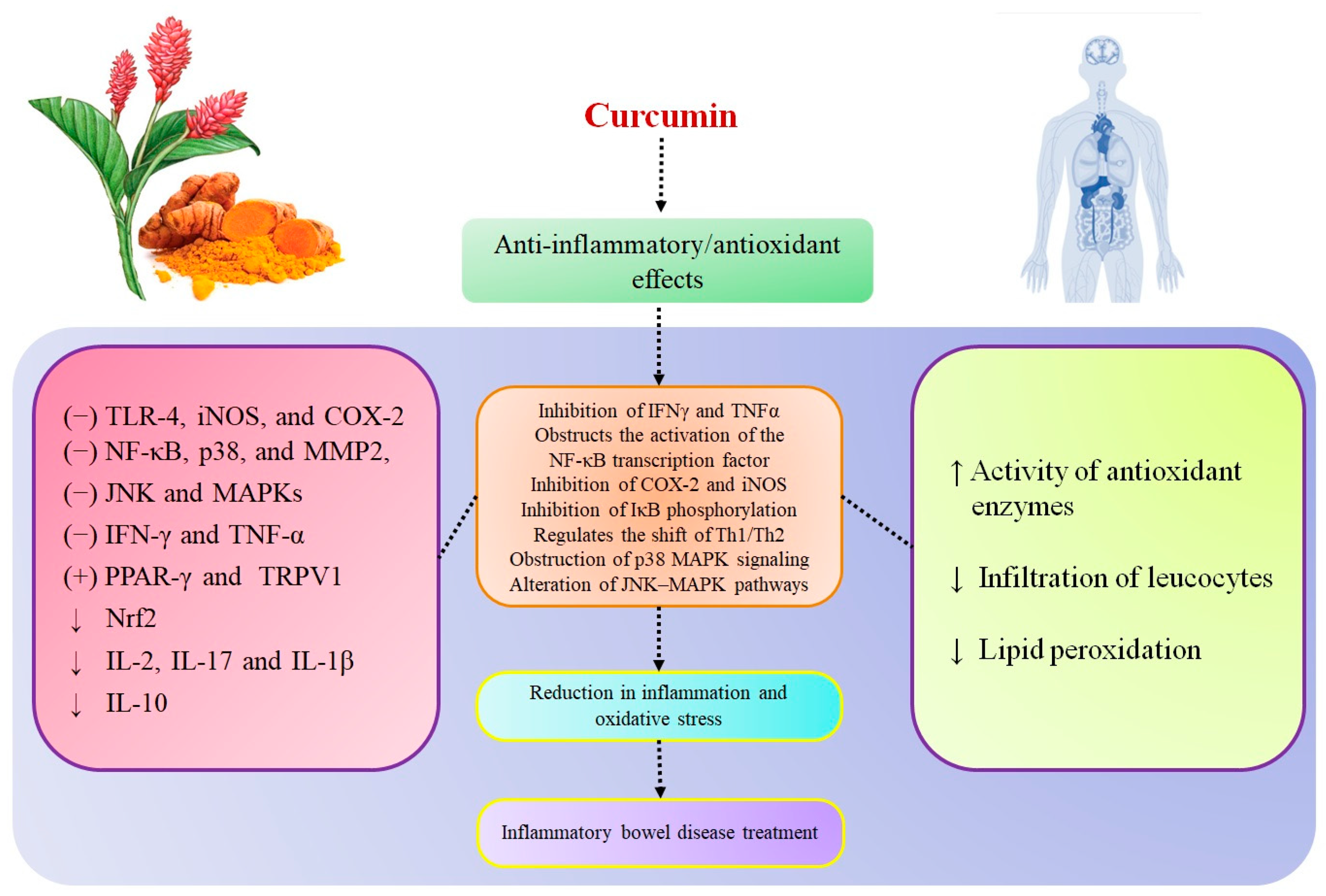
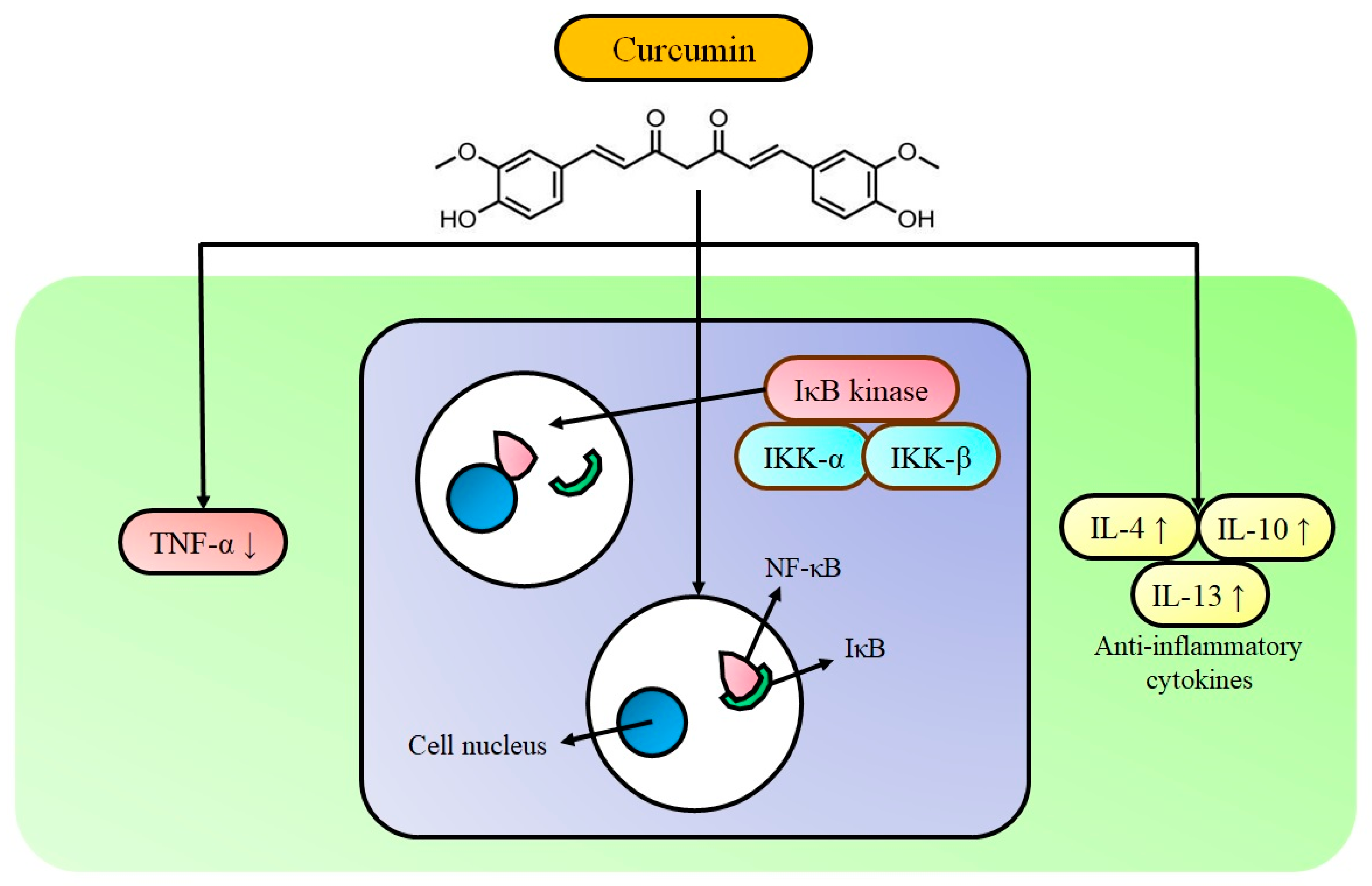
3. Curcumin’s Molecular Targets in Inflammatory Bowel Disease
4. Curcumin in Inflammatory Bowel Disease
5. Curcumin Combinations with Other Therapeutic Molecules and Modified Curcumin Formulations in Inflammatory Bowel Disease
6. Clinical Trials
6.1. Ulcerative Colitis
6.2. Crohn’s Disease
7. Opposing Voices against Curcumin
8. Conclusions and Future Outlook
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Hanauer, S.B. Inflammatory bowel disease: Epidemiology, pathogenesis, and therapeutic opportunities. Inflamm. Bowel Dis. 2006, 12, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Khor, B.; Gardet, A.; Xavier, R.J. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011, 474, 307–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, T.C.; Stappenbeck, T.S. Genetics and Pathogenesis of Inflammatory Bowel Disease. Annu. Rev. Pathol. Mech. 2016, 11, 127–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, F.; De Andrade, K.; Dos Santos, J.; Araujo, O.; Goulart, M. Antioxidant therapy for treatment of inflammatory bowel disease: Does it work? Redox Biol. 2015, 6, 617–639. [Google Scholar] [CrossRef] [Green Version]
- Khare, T.; Palakurthi, S.S.; Shah, B.M.; Palakurthi, S.; Khare, S. Natural product-based nanomedicine in treatment of inflammatory bowel disease. Int. J. Mol. Sci. 2020, 21, 3956. [Google Scholar] [CrossRef]
- Griffiths, A.M. Inflammatory bowel disease. Nutrition 1998, 14, 788–791. [Google Scholar] [CrossRef]
- Siegmund, B.; Fantuzzi, G.; Rieder, F.; Gamboni-Robertson, F.; Lehr, H.A.; Hartmann, G.; Dinarello, C.A.; Endres, S.; Eigler, A. Neutralization of interleukin-18 reduces severity in murine colitis and intestinal IFN-gamma and TNF-alpha production. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 281, R1264–R1273. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.W.; Choi, S.; Kim, S.Y.; Yoon, Y.S.; Kang, J.H.; Oh, S.H. Allyl isothiocyanate ameliorates dextran sodium sulfate-induced colitis in mouse by enhancing tight junction and mucin expression. Int. J. Mol. Sci. 2018, 19, 2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Limbergen, J.; Radford-Smith, G.; Satsangi, J. Advances in IBD genetics. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 372. [Google Scholar] [CrossRef]
- Castro, J.; Ocampo, Y.; Franco, L. Cape gooseberry [Physalis peruviana L.] calyces ameliorate TNBS acid-induced colitis in rats. J. Crohn’s Colitis 2015, 9, 1004–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogler, G.; Michetti, P.F.; Kruger, F.C.; van der Bijl, A.; Kruger, D.S.; Malan, F.; Grouard-Vogel, G.; Dhellin, O.; Fanget, B.; Vandepapeliere, P. T1234 Active Therapeutic Immunization Against TNF With a TNF-Kinoid in Crohn’s Disease Patients: A Phase 1–2 Study. Gastroenterology 2010, 138, S517. [Google Scholar] [CrossRef]
- Stallmach, A.; Hagel, S.; Bruns, T. Adverse effects of biologics used for treating IBD. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A review of its effects on human health. Foods 2017, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, A.; Senthil, N.; Min, T. Nanocurcumin: A promising candidate for therapeutic applications. Front. Pharmacol. 2020, 11, 487. [Google Scholar] [CrossRef] [PubMed]
- Moniruzzaman, M.; Min, T. Curcumin, curcumin nanoparticles and curcumin nanospheres: A review on their pharmacodynamics based on monogastric farm animal, poultry and fish nutrition. Pharmaceutics 2020, 12, 447. [Google Scholar] [CrossRef] [PubMed]
- Beyene, A.M.; Moniruzzaman, M.; Karthikeyan, A.; Min, T. Curcumin Nanoformulations with Metal Oxide Nanomaterials for Biomedical Applications. Nanomaterials 2021, 11, 460. [Google Scholar] [CrossRef] [PubMed]
- Tejada, S.; Manayi, A.; Daglia, M.; Nabavi, S.F.; Sureda, A.; Hajheydari, Z.; Gortzi, O.; Pazoki-Toroudi, H.; Nabavi, S.M. Wound healing effects of curcumin: A short review. Curr. Pharm. Biotechnol. 2016, 17, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.C.; de Freitas Santos, P.D.; do Prado Silva, J.T.; Leimann, F.V.; Bracht, L.; Gonçalves, O.H. Impact of curcumin nanoformulation on its antimicrobial activity. Trends Food Sci. Technol. 2018, 72, 74–82. [Google Scholar] [CrossRef]
- Chang, C.; Meikle, T.G.; Su, Y.; Wang, X.; Dekiwadia, C.; Drummond, C.J.; Conn, C.E.; Yang, Y. Encapsulation in egg white protein nanoparticles protects anti-oxidant activity of curcumin. Food Chem. 2019, 280, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Farhood, B.; Mortezaee, K.; Goradel, N.H.; Khanlarkhani, N.; Salehi, E.; Nashtaei, M.S.; Najafi, M.; Sahebkar, A. Curcumin as an anti-inflammatory agent: Implications to radiotherapy and chemotherapy. J. Cell. Physiol. 2019, 234, 5728–5740. [Google Scholar] [CrossRef]
- Abrahams, S.; Haylett, W.L.; Johnson, G.; Carr, J.A.; Bardien, S. Antioxidant effects of curcumin in models of neurodegeneration, aging, oxidative and nitrosative stress: A review. Neuroscience 2019, 406, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Kunnumakkara, A.B.; Aggarwal, B.B. Curcumin as “Curecumin”. Biochem. Pharmacol. 2008, 75, 787–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.; Davis, J.; Zhang, A.J.; He, X.; Mathews, S.T. Curcumin activates AMPK and suppresses gluconeogenic gene expression in hepatoma cells. Biochem. Biophys. Res. Commun. 2009, 388, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Sreedhar, R.; Arumugam, S.; Thandavarayan, R.A.; Karuppagounder, V.; Watanabe, K. Curcumin as a therapeutic agent in the chemoprevention of inflammatory bowel disease. Drug Discov. Today 2016, 21, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Mazieiro, R.; Frizon, R.R.; Barbalho, S.M.; Goulart, R.d.A. Is curcumin a possibility to treat inflammatory bowel diseases? J. Med. Food 2018, 21, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Kahkhaie, K.R.; Mirhosseini, A.; Aliabadi, A.; Mohammadi, A.; Mousavi, M.J.; Haftcheshmeh, S.M.; Sathyapalan, T.; Sahebkar, A. Curcumin: A modulator of inflammatory signaling pathways in the immune system. Inflammopharmacology 2019, 27, 885–900. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.S.; Acharya, A.; Ray, R.; Agrawal, R.; Raghuwanshi, R.; Jain, P. Cellular and molecular mechanisms of curcumin in prevention and treatment of disease. Crit. Rev. Food. Sci. Nutr. 2020, 60, 887–939. [Google Scholar] [CrossRef]
- Epstein, J.; Sanderson, I.R.; MacDonald, T.T. Curcumin as a therapeutic agent: The evidence from in vitro, animal and human studies. Br. J. Nutr. 2010, 103, 1545–1557. [Google Scholar] [CrossRef] [Green Version]
- Beloqui, A.; Coco, R.; Memvanga, P.B.; Ucakar, B.; des Rieux, A.; Préat, V. pH-sensitive nanoparticles for colonic delivery of curcumin in inflammatory bowel disease. Int. J. Pharm. 2014, 473, 203–212. [Google Scholar] [CrossRef]
- Beloqui, A.; Memvanga, P.B.; Coco, R.; Reimondez-Troitino, S.; Alhouayek, M.; Muccioli, G.G.; Alonso, M.J.; Csaba, N.; de la Fuente, M.; Préat, V. A comparative study of curcumin-loaded lipid-based nanocarriers in the treatment of inflammatory bowel disease. Colloids Surf. B. 2016, 143, 327–335. [Google Scholar] [CrossRef]
- McFadden, R.-M.T.; Larmonier, C.B.; Shehab, K.W.; Midura-Kiela, M.; Ramalingam, R.; Harrison, C.A.; Besselsen, D.G.; Chase, J.H.; Caporaso, J.G.; Jobin, C. The role of curcumin in modulating colonic microbiota during colitis and colon cancer prevention. Inflamm. Bowel Dis. 2015, 21, 2483–2494. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sharma, S.; Wadhwa, J. Improved uptake and therapeutic intervention of curcumin via designing binary lipid nanoparticulate formulation for oral delivery in inflammatory bowel disorder. Artif. Cells. Nanomed. Biotechnol. 2019, 47, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, N.; Cummins, E.; Royle, P.; Kandala, N.; Shyangdan, D.; Arasaradnam, R.; Clar, C.; Johnston, R. Faecal calprotectin testing for differentiating amongst inflammatory and non-inflammatory bowel diseases: Systematic review and economic evaluation. Health Technol. Assess. 2013, 17, 1–211. [Google Scholar] [CrossRef]
- Vecchi Brumatti, L.; Marcuzzi, A.; Tricarico, P.M.; Zanin, V.; Girardelli, M.; Bianco, A.M. Curcumin and inflammatory bowel disease: Potential and limits of innovative treatments. Molecules 2014, 19, 21127–21153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younis, N.; Zarif, R.; Mahfouz, R. Inflammatory bowel disease: Between genetics and microbiota. Mol. Biol. Rep. 2020, 47, 3053–3063. [Google Scholar] [CrossRef]
- Imhann, F.; Vich Vila, A.; Bonder, M.J.; Fu, J.; Gevers, D.; Visschedijk, M.C. Interplay of host genetics and gut microbiota underlying the onset and clinical presentation of infammatory bowel disease. Gut 2018, 67, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Z.; Van Sommeren, S.; Huang, H.; Ng, S.C.; Alberts, R.; Takahashi, A.; Ripke, S.; Lee, J.C.; Jostins, L.; Shah, T. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat. Genet. 2015, 47, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.N.; Park, C.; Park, S.J.; Lee, C.K.; Ye, B.D.; Kim, Y.S.; Lee, S.; Chae, J.; Kim, J.-I.; Kim, Y.-H. Deep resequencing of 131 Crohn’s disease associated genes in pooled DNA confirmed three reported variants and identified eight novel variants. Gut 2016, 65, 788–796. [Google Scholar] [CrossRef] [PubMed]
- Doecke, J.D.; Simms, L.A.; Zhao, Z.Z.; Huang, N.; Hanigan, K.; Krishnaprasad, K.; Roberts, R.L.; Andrews, J.M.; Mahy, G.; Bampton, P. Genetic susceptibility in IBD: Overlap between ulcerative colitis and Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Momozawa, Y.; Dmitrieva, J.; Theatre, E.; Deffontaine, V.; Rahmouni, S.; Charloteaux, B.; Crins, F.; Docampo, E.; Elansary, M.; Gori, A.S.; et al. IBD risk loci are enriched in multigenic regulatory modules encompassing putative causative genes. Nat. Commun. 2018, 9, 2427. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; He, J.; Shen, Y.; Zhang, C.; Wang, J.; Chen, Y. New frontiers in genetics, gut microbiota, and immunity: A rosetta stone for the pathogenesis of inflammatory bowel disease. Biomed. Res. Int. 2017, 2017, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, H.H. Monogenic diseases associated with intestinal inflammation: Implications for the understanding of inflammatory bowel disease. Gut 2013, 62, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- McGovern, D.P.; Kugathasan, S.; Cho, J.H. Genetics of inflammatory bowel diseases. Gastroenterology 2015, 149, 1163–1176.e1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, M.; Burisch, J. Impact of Genes and the Environment on the Pathogenesis and Disease Course of Inflammatory Bowel Disease. Dig. Dis. Sci 2019, 64, 1759–1769. [Google Scholar] [CrossRef] [PubMed]
- Cooney, J.M.; Barnett, M.P.; Dommels, Y.E.; Brewster, D.; Butts, C.A.; McNabb, W.C.; Laing, W.A.; Roy, N.C. A combined omics approach to evaluate the effects of dietary curcumin on colon inflammation in the Mdr1a−/− mouse model of inflammatory bowel disease. J. Nutr. Biochem. 2016, 27, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Kelsen, J.R.; Dawany, N.; Moran, C.J.; Petersen, B.-S.; Sarmady, M.; Sasson, A.; Pauly-Hubbard, H.; Martinez, A.; Maurer, K.; Soong, J. Exome sequencing analysis reveals variants in primary immunodeficiency genes in patients with very early onset inflammatory bowel disease. Gastroenterology 2015, 149, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeissig, S.; Petersen, B.-S.; Tomczak, M.; Melum, E.; Huc-Claustre, E.; Dougan, S.K.; Laerdahl, J.K.; Stade, B.; Forster, M.; Schreiber, S. Early-onset Crohn’s disease and autoimmunity associated with a variant in CTLA-4. Gut 2015, 64, 1889–1897. [Google Scholar] [CrossRef]
- Muise, A.M.; Xu, W.; Guo, C.-H.; Walters, T.D.; Wolters, V.M.; Fattouh, R.; Lam, G.Y.; Hu, P.; Murchie, R.; Sherlock, M. NADPH oxidase complex and IBD candidate gene studies: Identification of a rare variant in NCF2 that results in reduced binding to RAC2. Gut 2012, 61, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Hutchins, A.P.; Diez, D.; Miranda-Saavedra, D. The IL-10/STAT3-mediated anti-inflammatory response: Recent developments and future challenges. Brief Funct. Genom. 2013, 12, 489–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beser, O.F.; Conde, C.D.; Serwas, N.K.; Cokugras, F.C.; Kutlu, T.; Boztug, K.; Erkan, T. Clinical features of interleukin 10 receptor gene mutations in children with very early-onset inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Jostins, L.; Ripke, S.; Weersma, R.K.; Duerr, R.H.; McGovern, D.P.; Hui, K.Y.; Lee, J.C.; Schumm, L.P.; Sharma, Y.; Anderson, C.A. Host-microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature 2012, 491, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keane, J.; Gershon, S.; Wise, R.P.; Mirabile-Levens, E.; Kasznica, J.; Schwieterman, W.D.; Siegel, J.N.; Braun, M.M. Tuberculosis associated with infliximab, a tumor necrosis factor α-neutralizing agent. N. Engl. J. Med. 2001, 345, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Badr-el-Din, S.; Trejdosiewicz, L.; Heatley, R.; Losowsky, M. Local immunity in ulcerative colitis: Evidence for defective secretory IgA production. Gut 1988, 29, 1070–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgart, D.C.; Carding, S.R. Inflammatory bowel disease: Cause and immunobiology. Lancet 2007, 369, 1627–1640. [Google Scholar] [CrossRef]
- Niess, J.H. Role of mucosal dendritic cells in inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 5138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Muñoz, F.; Dominguez-Lopez, A.; Yamamoto-Furusho, J.K. Role of cytokines in inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 4280. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Cho, J.H. Inflammatory Bowel Disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef] [PubMed]
- Matricon, J.; Barnich, N.; Ardid, D. Immunopathogenesis of inflammatory bowel disease. Self/Nonself 2010, 1, 299–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Cheon, J.H. Pathogenesis of inflammatory bowel disease and recent advances in biologic therapies. Immune Netw. 2017, 17, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoneim, A.I.; Abdel-Naim, A.B.; Khalifa, A.E.; El-Denshary, E.S. Protective effects of curcumin against ischaemia/reperfusion insult in rat forebrain. Pharmacol. Res. 2002, 46, 273–279. [Google Scholar] [CrossRef]
- Bishnoi, M.; Chopra, K.; Kulkarni, S.K. Protective effect of Curcumin, the active principle of turmeric (Curcuma longa) in haloperidol-induced orofacial dyskinesia and associated behavioural, biochemical and neurochemical changes in rat brain. Pharmacol. Biochem. Behav. 2008, 88, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, A.M.; Orlando, R.A. Curcumin and resveratrol inhibit nuclear factor-kappaB-mediated cytokine expression in adipocytes. Nutr. Metab. 2008, 5, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soetikno, V.; Sari, F.R.; Veeraveedu, P.T.; Thandavarayan, R.A.; Harima, M.; Sukumaran, V.; Lakshmanan, A.P.; Suzuki, K.; Kawachi, H.; Watanabe, K. Curcumin ameliorates macrophage infiltration by inhibiting NF-κB activation and proinflammatory cytokines in streptozotocin induced-diabetic nephropathy. Nutr. Metab. 2011, 8, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.-M.; Xu, R.; Huang, X.-Y.; Cheng, S.-M.; Huang, M.-F.; Yue, H.-Y.; Wang, X.; Zou, Y.; Lu, A.-P.; Liu, D.-Y. Curcumin suppressed activation of dendritic cells via JAK/STAT/SOCS signal in mice with experimental colitis. Front. Pharmacol. 2016, 7, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.X.; Du, Z.Y.; Wang, W.C.; Song, M.Y.; Sanidad, K.; Sukamtoh, E.; Zheng, J.; Tian, L.; Xiao, H.; Liu, Z.H.; et al. Structure-activity relationship of curcumin: Role of the methoxy group in anti-inflammatory and anticolitis effects of curcumin. J. Agric. Food Chem. 2017, 65, 4509–4515. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yue, Y.; Zheng, X.; Zhang, K.; Chen, S.; Du, Z. Curcumin, inflammation, and chronic diseases: How are they linked? Molecules 2015, 20, 9183–9213. [Google Scholar] [CrossRef] [PubMed]
- Larmonier, C.B.; Uno, J.K.; Larmonier, N.; Midura, A.J.; Timmermann, B.; Ghishan, F.K.; Kiela, P.R. Protective effects of dietary curcumin in mouse model of chemically induced colitis are strain dependent. Inflamm. Bowel Dis. 2008, 14, 780–793. [Google Scholar] [CrossRef] [Green Version]
- Pan, M.; Lin-Shiau, S.Y.; Lin, J.K. Comparative studies on the suppression of nitric oxide synthase by curcumin and its hydroge ated metabolites through down-regulation of IkappaB kinase and NF-kappaB activation in macrophages. Biochem Pharmcol. 2000, 11, 1665–1676. [Google Scholar] [CrossRef]
- Mouzaoui, S.; Rahim, I.; Djerdjouri, B. Aminoguanidine and curcumin attenuated tumor necrosis factor (TNF)-α-induced oxidative stress, colitis and hepatotoxicity in mice. Int. Immunopharmacol. 2012, 12, 302–311. [Google Scholar] [CrossRef]
- Zhang, M.; Deng, C.S.; Zheng, J.J.; Xia, J. Curcumin regulated shift from Th1 to Th2 in trinitrobenzene sulphonic acid-induced chronic colitis. Acta Pharmacol. Sin. 2006, 1071–1077. [Google Scholar] [CrossRef]
- Jiang, H.; Deng, C.-S.; Zhang, M.; Xia, J. Curcumin-attenuated trinitrobenzene sulphonic acid induces chronic colitis by inhibiting expression of cyclooxygenase-2. World J. Gastroenterol. 2006, 12, 3848. [Google Scholar] [CrossRef] [PubMed]
- Ukil, A.; Maity, S.; Karmakar, S.; Datta, N.; Vedasiromoni, J.; Das, P.K. Curcumin, the major component of food flavour turmeric, reduces mucosal injury in trinitrobenzene sulphonic acid-induced colitis. Br. J. Pharmacol. 2003, 139, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Li, J.; He, S.; Chen, O.; Shi, L. Effect of curcumin on p38MAPK expression in DSS-induced murine ulcerative colitis. Genet. Mol. Res. 2015, 14, 3450–3458. [Google Scholar] [CrossRef] [PubMed]
- Topcu-Tarladacalisir, Y.; Akpolat, M.; Uz, Y.H.; Kizilay, G.; Sapmaz-Metin, M.; Cerkezkayabekir, A.; Omurlu, I.K. Effects of curcumin on apoptosis and oxidoinflammatory regulation in a rat model of acetic acid-induced colitis: The roles of c-Jun N-terminal kinase and p38 mitogen-activated protein kinase. J. Med. Food 2013, 16, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tang, Q.; Duan, P.; Yang, L. Curcumin as a therapeutic agent for blocking NF-κB activation in ulcerative colitis. Immunopharmacol. Immunotoxicol. 2018, 40, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Midura-Kiela, M.T.; Radhakrishnan, V.M.; Larmonier, C.B.; Laubitz, D.; Ghishan, F.K.; Kiela, P.R. Curcumin inhibits interferon-γ signaling in colonic epithelial cells. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G85–G96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atreya, I.; Atreya, R.; Neurath, M.F. NF-kappaB in inflammatory bowel disease. J. Intern. Med. 2008, 263, 591–596. [Google Scholar] [CrossRef]
- Zhao, F.; Gong, Y.; Hu, Y.; Lu, M.; Wang, J.; Dong, J.; Chen, D.; Chen, L.; Fu, F.; Qiu, F. Curcumin and its major metabolites inhibit the inflammatory response induced by lipopolysaccharide: Translocation of nuclear factor-κB as potential target. Mol. Med. Rep. 2015, 11, 3087–3093. [Google Scholar] [CrossRef] [PubMed]
- Bhaumik, S.; Jyothi, M.D.; Khar, A. Differential modulation of nitric oxide production by curcumin in host macrophages and NK cells. FEBS Lett. 2000, 483, 78–82. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Liu, X. Effect of curcumin on immune function of mice. J. Huazhong Univ. Sci. Technol. Med. Sci. 2005, 25, 137–140. [Google Scholar]
- Menon, V.P.; Sudheer, A.R. Antioxidant and anti-inflammatory properties of curcumin. In The molecular Targets and Therapeutic Uses of Curcumin in Health and Disease; Aggarwal, B.B., Surh, Y.-J., Shishodia, S., Eds.; Springer: Boston, MA, USA, 2007; Volume 595, pp. 105–125. [Google Scholar]
- Salh, B.; Assi, K.; Templeman, V.; Parhar, K.; Owen, D.; Gomez-Munoz, A.; Jacobson, K. Curcumin attenuates DNB-induced murine colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, G235–G243. [Google Scholar] [CrossRef]
- Venkataranganna, M.; Rafiq, M.; Gopumadhavan, S.; Peer, G.; Babu, U.; Mitra, S. NCB-02 (standardized Curcumin preparation) protects dinitrochlorobenzene-induced colitis through down-regulation of NF-kB and iNOS. World J. Gastroenterol. 2007, 13, 1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho-Barquero, L.; Villegas, I.; Sánchez-Calvo, J.M.; Talero, E.; Sánchez-Fidalgo, S.; Motilva, V.; de la Lastra, C.A. Curcumin, a Curcuma longa constituent, acts on MAPK p38 pathway modulating COX-2 and iNOS expression in chronic experimental colitis. Int. Immunopharmacol. 2007, 7, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Martelli, L.; Ragazzi, E.; Di Mario, F.; Martelli, M.; Castagliuolo, I.; Dal Maschio, M.; Palù, G.; Maschietto, M.; Scorzeto, M.; Vassanelli, S. A potential role for the vanilloid receptor TRPV1 in the therapeutic effect of curcumin in dinitrobenzene sulphonic acid-induced colitis in mice. Neurogastroenterol. Motil. 2007, 19, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Lubbad, A.; Oriowo, M.; Khan, I. Curcumin attenuates inflammation through inhibition of TLR-4 receptor in experimental colitis. Mol. Cell. Biochem. 2009, 322, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.; Docena, G.; MacDonald, T.T.; Sanderson, I.R. Curcumin suppresses p38 mitogen-activated protein kinase activation, reduces IL-1β and matrix metalloproteinase-3 and enhances IL-10 in the mucosa of children and adults with inflammatory bowel disease. Br. J. Nutr. 2010, 103, 824–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motawi, T.K.; Rizk, S.M.; Shehata, A.H. Effects of curcumin and Ginkgo biloba on matrix metalloproteinases gene expression and other biomarkers of inflammatory bowel disease. J. Physiol. Biochem. 2012, 68, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Thompson, J.K.; MacPherson, M.B.; Beuschel, S.L.; Westbom, C.M.; Sayan, M.; Shukla, A. Curcumin: A double hit on malignant mesothelioma. Cancer Prev. Res. 2014, 7, 330–340. [Google Scholar] [CrossRef] [Green Version]
- McCann, M.J.; Johnston, S.; Reilly, K.; Men, X.; Burgess, E.J.; Perry, N.B.; Roy, N.C. The effect of turmeric (Curcuma longa) extract on the functionality of the solute carrier protein 22 A4 (SLC22A4) and interleukin-10 (IL-10) variants associated with inflammatory bowel disease. Nutrients 2014, 6, 4178–4190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Wang, J.; Yang, C.; Han, H.; Rong, W.; Zhang, G. Oral administration of curcumin attenuates visceral hyperalgesia through inhibiting phosphorylation of TRPV1 in rat model of ulcerative colitis. Mol. Pain 2017, 13. [Google Scholar] [CrossRef]
- Loganes, C.; Lega, S.; Bramuzzo, M.; Vecchi Brumatti, L.; Piscianz, E.; Valencic, E.; Tommasini, A.; Marcuzzi, A. Curcumin anti-apoptotic action in a model of intestinal epithelial inflammatory damage. Nutrients 2017, 9, 578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.-y.; Zhong, X.; Kim, S.-J.; Kim, D.-H.; Kim, H.S.; Lee, J.-S.; Yum, H.-W.; Lee, J.; Na, H.-K.; Surh, Y.-J. Comparative effects of curcumin and tetrahydrocurcumin on dextran sulfate sodium-induced colitis and inflammatory signaling in mice. J. Cancer Prev. 2018, 23, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, T.; Yang, Y.; Jin, T.; Jiang, W.; Zhou, R. Orchestration of NLRP3 inflammasome activation by ion fluxes. Trends Immunol. 2018, 39, 393–406. [Google Scholar] [CrossRef] [PubMed]
- Yue, W.; Liu, Y.; Li, X.; Lv, L.; Huang, J.; Liu, J. Curcumin ameliorates dextran sulfate sodium-induced colitis in mice via regulation of autophagy and intestinal immunity. Turk. J. Gastroenterol. 2019, 30, 290. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xue, H.; Zhao, G.; Qiao, C.; Sun, X.; Pang, C.; Zhang, D. Curcumin and resveratrol suppress dextran sulfate sodium‑induced colitis in mice. Mol. Med. Rep. 2019, 19, 3053–3060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, C.; Wang, J.-Y.; Xiong, F.; Wu, B.-H.; Luo, M.-H.; Yu, Z.-C.; Liu, T.-T.; Li, D.-F.; Tang, Q.; Li, Y.-X. Curcumin ameliorates DSS‑induced colitis in mice by regulating the Treg/Th17 signaling pathway. Mol. Med. Rep. 2021, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Jian, Y.-T.; Mai, G.-F.; Wang, J.-D.; Zhang, Y.-L.; Luo, R.-C.; Fang, Y.-X. Preventive and therapeutic effects of NF-kappaB inhibitor curcumin in rats colitis induced by trinitrobenzene sulfonic acid. World J. Gastroenterol. 2005, 11, 1747. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Ahmed, B.; Mehta, K.; Kurzrock, R. Liposomal curcumin with and without oxaliplatin: Effects on cell growth, apoptosis, and angiogenesis in colorectal cancer. Mol. Cancer Ther. 2007, 6, 1276–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, V.R.; Suresh, S.; Devi, K.; Yadav, S. Effect of cyclodextrin complexation of curcumin on its solubility and antiangiogenic and anti-inflammatory activity in rat colitis model. AAPS Pharm. Sci. Technol. 2009, 10, 752–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, V.R.; Suresh, S.; Devi, K.; Yadav, S. Novel formulation of solid lipid microparticles of curcumin for anti-angiogenic and anti-inflammatory activity for optimization of therapy of inflammatory bowel disease. J. Pharm. Pharmacol. 2009, 61, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Gugulothu, D.; Kulkarni, A.; Patravale, V.; Dandekar, P. pH-sensitive nanoparticles of curcumin–celecoxib combination: Evaluating drug synergy in ulcerative colitis model. J. Pharm. Sci. 2014, 103, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Sareen, R.; Nath, K.; Jain, N.; Dhar, K. Curcumin loaded microsponges for colon targeting in inflammatory bowel disease: Fabrication, optimization, and in vitro and pharmacodynamic evaluation. Biomed. Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, B.; Si, X.; Zhang, M.; Merlin, D. Oral administration of pH-sensitive curcumin-loaded microparticles for ulcerative colitis therapy. Colloids Surf. B. 2015, 135, 379–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Zhai, W.; Jiang, Q.; Huang, R.; Liu, L.; Dai, J.; Gong, W.; Du, S.; Wu, Q. Curcumin-piperine mixtures in self-microemulsifying drug delivery system for ulcerative colitis therapy. Int. J. Pharm. 2015, 490, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Mutalik, S.; Suthar, N.A.; Managuli, R.S.; Shetty, P.K.; Avadhani, K.; Kalthur, G.; Kulkarni, R.V.; Thomas, R. Development and performance evaluation of novel nanoparticles of a grafted copolymer loaded with curcumin. Int. J. Biol. Macromol. 2016, 86, 709–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sareen, R.; Jain, N.; Rajkumari, A.; Dhar, K. pH triggered delivery of curcumin from Eudragit-coated chitosan microspheres for inflammatory bowel disease: Characterization and pharmacodynamic evaluation. Drug Deliv. 2016, 23, 55–62. [Google Scholar] [CrossRef]
- Blanco-García, E.; Otero-Espinar, F.; Blanco-Méndez, J.; Leiro-Vidal, J.; Luzardo-Alvarez, A. Development and characterization of anti-inflammatory activity of curcumin-loaded biodegradable microspheres with potential use in intestinal inflammatory disorders. Int. J. Pharm. 2017, 518, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Ye, L.; Du, G.; Huang, Y.; Wu, Y.; Ge, S.; Yang, Z.; Zhu, G. Effects of curcumin plus Soy oligosaccharides on intestinal flora of rats with ulcerative colitis. Cell. Mol. Biol. 2017, 63, 20–25. [Google Scholar] [CrossRef]
- Toden, S.; Theiss, A.L.; Wang, X.; Goel, A. Essential turmeric oils enhance anti-inflammatory efficacy of curcumin in dextran sulfate sodium-induced colitis. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohno, M.; Nishida, A.; Sugitani, Y.; Nishino, K.; Inatomi, O.; Sugimoto, M.; Kawahara, M.; Andoh, A. Nanoparticle curcumin ameliorates experimental colitis via modulation of gut microbiota and induction of regulatory T cells. PLoS ONE 2017, 12, e0185999. [Google Scholar] [CrossRef] [Green Version]
- Qiao, H.; Fang, D.; Chen, J.; Sun, Y.; Kang, C.; Di, L.; Li, J.; Chen, Z.; Chen, J.; Gao, Y. Orally delivered polycurcumin responsive to bacterial reduction for targeted therapy of inflammatory bowel disease. Drug Deliv. 2017, 24, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesharwani, S.S.; Ahmad, R.; Bakkari, M.A.; Rajput, M.K.; Dachineni, R.; Valiveti, C.K.; Kapur, S.; Bhat, G.J.; Singh, A.B.; Tummala, H. Site-directed non-covalent polymer-drug complexes for inflammatory bowel disease (IBD): Formulation development, characterization and pharmacological evaluation. J. Control. Release 2018, 290, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Gou, S.; Huang, Y.; Zhou, X.; Li, Q.; Han, M.K.; Kang, Y.; Xiao, B. Facile fabrication of bowl-shaped microparticles for oral curcumin delivery to ulcerative colitis tissue. Colloids Surf. B 2018, 169, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, G.J.; Nagy, L.I.; Berko, A.; Hoffmann, A.; Feher, L.Z.; Bagyanszki, M.; Kari, B.; Balog, J.A.; Hackler, L.; Kanizsai, I. The anti-inflammatory role of mannich curcuminoids; special focus on colitis. Molecules 2019, 24, 1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Gou, S.; Ma, P.; Song, H.; Zhou, X.; Huang, Y.; Han, M.K.; Wan, Y.; Kang, Y.; Xiao, B. Oral administration of colitis tissue-accumulating porous nanoparticles for ulcerative colitis therapy. Int. J. Pharm. 2019, 557, 135–144. [Google Scholar] [CrossRef]
- Yu, S.; Huang, Y.; Huang, G.; Xiong, J.; Wu, Y.; Lei, X. Effects of Curcumin Chitosan Microspheres on the Expression of NF-κB, IL-1β, IL-4 and IL-6 in Rats with Ulcerative Colitis. J. Biomater. Tissue Eng. 2019, 9, 810–815. [Google Scholar] [CrossRef]
- Desai, N.; Momin, M. Colon targeted bioadhesive pellets of curcumin and cyclosporine for improved management of inflammatory bowel disease. Drug Deliv. Transl. Res. 2020, 10, 1288–1301. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.A.; Lee, J.; Naeem, M.; Hasan, N.; Kim, J.; Kim, H.J.; Lee, E.H.; Jung, Y.; Yoo, J.-W. Curcumin Nanocrystal/pH-Responsive Polyelectrolyte Multilayer Core–Shell Nanoparticles for Inflammation-Targeted Alleviation of Ulcerative Colitis. Biomacromolecules 2020, 21, 3571–3581. [Google Scholar] [CrossRef]
- Luo, R.; Lin, M.; Zhang, C.; Shi, J.; Zhang, S.; Chen, Q.; Hu, Y.; Zhang, M.; Zhang, J.; Gao, F. Genipin-crosslinked human serum albumin coating using a tannic acid layer for enhanced oral administration of curcumin in the treatment of ulcerative colitis. Food Chem. 2020, 330, 127241. [Google Scholar] [CrossRef]
- Huang, Y.; Canup, B.S.; Gou, S.; Chen, N.; Dai, F.; Xiao, B.; Li, C. Oral nanotherapeutics with enhanced mucus penetration and ROS-responsive drug release capacities for delivery of curcumin to colitis tissues. J. Mater. Chem. B 2021. [Google Scholar] [CrossRef]
- Rotrekl, D.; Šalamúnová, P.; Paráková, L.; Baďo, O.; Saloň, I.; Štěpánek, F.; Hanuš, J.; Hošek, J. Composites of yeast glucan particles and curcumin lead to improvement of dextran sulfate sodium-induced acute bowel inflammation in rats. Carbohydr. Polym. 2021, 252, 117142. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Iida, T.; Takeuchi, K.; Watanabe, F.; Maruyama, Y.; Andoh, A.; Tsujikawa, T.; Fujiyama, Y.; Mitsuyama, K.; Sata, M. Curcumin maintenance therapy for ulcerative colitis: Randomized, multicenter, double-blind, placebo-controlled trial. Clin. Gastroenterol. Hepatol. 2006, 4, 1502–1506. [Google Scholar] [CrossRef] [PubMed]
- Singla, V.; Pratap Mouli, V.; Garg, S.K.; Rai, T.; Choudhury, B.N.; Verma, P.; Deb, R.; Tiwari, V.; Rohatgi, S.; Dhingra, R. Induction with NCB-02 (curcumin) enema for mild-to-moderate distal ulcerative colitis—A randomized, placebo-controlled, pilot study. J. Crohn’s Colitis 2014, 8, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, A.; Salomon, N.; Wu, J.C.; Kopylov, U.; Lahat, A.; Har-Noy, O.; Ching, J.Y.; Cheong, P.K.; Avidan, B.; Gamus, D. Curcumin in combination with mesalamine induces remission in patients with mild-to-moderate ulcerative colitis in a randomized controlled trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1444–1449.e1. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.T.; Vaughn, A.R.; Sharma, V.; Chopra, D.; Mills, P.J.; Peterson, S.N.; Sivamani, R.K. Effects of Turmeric and Curcumin Dietary Supplementation on Human Gut Microbiota: A Double-Blind, Randomized, Placebo-Controlled Pilot Study. J. Evid. Based Integr. Med. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, N.; Mansoori, A.; Shayesteh, A.; Hashemi, S.J. The effect of curcumin supplementation on clinical outcomes and inflammatory markers in patients with ulcerative colitis. Phytother. Res. 2020, 34, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Pal, P.; Penmetsa, A.; Kathi, P.; Girish, G.; Goren, I.; Reddy, D.N. Novel Bioenhanced Curcumin With Mesalamine for Induction of Clinical and Endoscopic Remission in Mild-to-Moderate Ulcerative Colitis: A Randomized Double-Blind Placebo-controlled Pilot Study. J. Clin. Gastroenterol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Holt, P.R.; Katz, S.; Kirshoff, R. Curcumin therapy in inflammatory bowel disease: A pilot study. Dig. Dis. Sci. 2005, 50, 2191–2193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugimoto, K.; Ikeya, K.; Bamba, S.; Andoh, A.; Yamasaki, H.; Mitsuyama, K.; Nasuno, M.; Tanaka, H.; Matsuura, A.; Kato, M. Highly bioavailable curcumin derivative ameliorates Crohn’s disease symptoms: A randomized, double-blind, multicenter study. J. Crohn’s Colitis 2020, 14, 1693–1701. [Google Scholar] [CrossRef]
- Bommelaer, G.; Laharie, D.; Nancey, S.; Hebuterne, X.; Roblin, X.; Nachury, M.; Peyrin-Biroulet, L.; Fumery, M.; Richard, D.; Pereira, B. Oral curcumin no more effective than placebo in preventing recurrence of Crohn’s disease after surgery in a randomized controlled trial. Clin. Gastroenterol. Hepatol. 2020, 18, 1553–1560.e1. [Google Scholar] [CrossRef]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar] [PubMed]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M. Phase I clinical trial of oral curcumin: Biomarkers of systemic activity and compliance. Clin. Cancer Res. 2004, 10, 6847–6854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kedia, S.; Bhatia, V.; Thareja, S.; Garg, S.; Mouli, V.P.; Bopanna, S.; Tiwari, V.; Makharia, G.; Ahuja, V. Low dose oral curcumin is not effective in induction of remission in mild to moderate ulcerative colitis: Results from a randomized double blind placebo controlled trial. World J. Gastrointest. Pharmacol. Ther. 2017, 8, 147. [Google Scholar] [CrossRef] [PubMed]
- Shapira, S.; Leshno, A.; Katz, D.; Maharshak, N.; Hevroni, G.; Jean-David, M.; Kraus, S.; Galazan, L.; Aroch, I.; Kazanov, D. Of mice and men: A novel dietary supplement for the treatment of ulcerative colitis. Ther. Adv. Gastroenter. 2018, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasyid, A.; Lelo, A. The effect of curcumin and placebo on human gall-bladder function: An ultrasound study. Aliment. Pharmacol. Ther. 1999, 13, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Rasyid, A.; Rahman, A.R.A.; Jaalam, K.; Lelo, A. Effect of different curcumin dosages on human gall bladder. Asia Pac. J. Clin. Nutr. 2002, 11, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Samba-Mondonga, M.; Constante, M.; Fragoso, G.; Calvé, A.; Santos, M.M. Curcumin induces mild anemia in a DSS-induced colitis mouse model maintained on an iron-sufficient diet. PLoS ONE 2019, 14, e0208677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zikaki, K.; Aggeli, I.-K.; Gaitanaki, C.; Beis, I. Curcumin induces the apoptotic intrinsic pathway via upregulation of reactive oxygen species and JNKs in H9c2 cardiac myoblasts. Apoptosis 2014, 19, 958–974. [Google Scholar] [CrossRef]
- Tanwar, V.; Sachdeva, J.; Kishore, K.; Mittal, R.; Nag, T.C.; Ray, R.; Kumari, S.; Arya, D.S. Dose-dependent actions of curcumin in experimentally induced myocardial necrosis: A biochemical, histopathological, and electron microscopic evidence. Cell Biochem. Funct. 2010, 28, 74–82. [Google Scholar] [CrossRef]
- Srivastava, K.; Bordia, A.; Verma, S. Curcumin, a major component of food spice turmeric (Curcuma longa) inhibits aggregation and alters eicosanoid metabolism in human blood platelets. Prostaglandins Leukot. Essent. Fatty Acids 1995, 52, 223–227. [Google Scholar] [CrossRef]
- Srivastava, R.; Dikshit, M.; Srimal, R.; Dhawan, B. Anti-thrombotic effect of curcumin. Thromb. Res. 1985, 40, 413–417. [Google Scholar] [CrossRef]
- Srivastava, R.; Puri, V.; Srimal, R.; Dhawan, B. Effect of curcumin on platelet aggregation and vascular prostacyclin synthesis. Arzneimittel-Forschung 1986, 36, 715–717. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| S. No | Characteristics | Crohn’s Disease | Ulcerative Colitis | References |
|---|---|---|---|---|
| 1 | Lesion site | Infects any part of the gastrointestinal tract | Infection limited to the colon | Waugh et al. [33]; Vecchi Brumatti et al. [34]; Younis et al. [35]. |
| 2 | Spreading type | Patchy | Continuous | |
| 3 | Mucosal inflammation | Entire wall and transmural | Limited to the epithelial mucosa | |
| 4 | Frequently involved site | Ileum | Rectum | |
| 5 | Bloody diarrhea | Less common | Very common | |
| 6 | Perianal complications | Common | Rare | |
| 7 | Cytokine inflammation | IFN-y, IL-12, and TNF-α | IL-1, IL-5, and IL-33 |
| S. No | Major Factors | References |
|---|---|---|
| 1 | Excessive release of IL-6, IL-12, IL-23, and TNF-α | Badr-El-Din et al. [53]; Baumgart and Carding, [54]; Niess, [55]; Sanchez-Munoz et al. [56]; Abraham and Cho, [57]; Matricon [58]; Kim et al. [59]; Younis et al. [35] |
| 2 | Upregulation of Th1, Th2, and Th17 | |
| 3 | Impaired pathogen recognition and epithelial integrity | |
| 4 | Defective macrophages | |
| 5 | Overactive dendritic cells | |
| 6 | Absence of Treg cells |
| S. No | Author/Year | Study Title | Dose, Duration, and Route of Administration | Cell line/Animal Model | Main Findings |
|---|---|---|---|---|---|
| 1 | Salh et al., 2003 [82] | Curcumin attenuates DNB-induced murine colitis | Curcumin (0.25% concentration) supplied in the diet (five days before treatment and five days after induction) | C3H mice/DNBS colitis | Controlled the loss of body weight, reduced the severity of histological parameters and activity of MPO, IL-1β, NF-κB, and p38 MAPK |
| 2 | Jian et al., 2005 [98] | Preventive and therapeutic effects of NF-κβ inhibitor curcumin in rats colitis induced by trinitrobenzene sulfonic acid. | Curcumin supplied in the diet at 2.0% of concentration, 14 days | SPF Wistar rats/TNBS colitis | Curcumin improved the histological score and attenuated the NF-κB signaling, blockage of IĸB degradation decreased the IL-1 expression level and increased IL-10 level of expression. Effective against TNBS colitis in rats. |
| 3 | Jiang et al. 2006 [71] | Curcumin-attenuated trinitrobenzene sulphonic acid induces chronic colitis by inhibiting the expression of cyclooxygenase-2 | Curcumin (30 and 60 mg/kg) intake every day, intraperitoneal injection, 14 days | Sprague–Dawley rats/TNBS colitis | Reduced the MPO activity and suppressed the COX-2, IFN-α, and TNF-α expression |
| 4 | Camacho-Barquero et al., 2007 [84] | Curcumin, a curcuma longa constituent acts on the MAPK p38 pathway modulating COX-2 and iNOS expression in chronic experimental colitis | Curcumin (50–100 mg/kg) intake every day, 14 days | Wistar rats/TNBS colitis | Curcumin led to the reduction in MAPK activity, which may result in the suppression of COX-2 and iNOS immune signals; no differences were observed in JNK. Effective against TNBS colitis in rats. |
| 5 | Larmonier et al., 2008 [67] | Protective effects of dietary curcumin in mouse model of chemically induced colitis are strain-dependent | Curcumin (2%) supplied in the diet for 14 days | NKT-deficient SJL/J mice (Th1-mediated inflammation) and BALB/c mice (mixed Th1/Th2 response)/TNBS colitis |
The efficacy of curcumin in TNBS colitis varies in BALB/c and SJL/J mouse strains. The exact mechanism governing these differences is unclear, the results suggest that the therapeutic value of curcumin may differ depending on the nature of immune dysregulation in IBD. |
| 6 | Lubbad et al., 2009 [86] | Curcumin attenuates inflammation through inhibition of TLR-4 receptor in experimental colitis | Curcumin (100 mg/kg) supplied in the diet, five days | Sprague-Dawley rats/TNBS colitis | Curcumin suppressed the TLR-4 and NF-κB activity in the inflamed tissue. Effective against TNBS colitis in rats. |
| 7 | Epstein et al., 2010b [87] | Curcumin suppresses p38 mitogen-activated protein kinase activation, reduces IL-1b and matrix metalloproteinase-3, and enhances IL-10 in the the mucosa of children and adults with IBD | Curcumin (5, 10, 20 μM) | Colonic mucosal biopsy and colonic myofibroblast (CMF) cell cultures | Curcumin effectively suppressed the p38 MAPK activity and reduced the IL-1b and matrix metalloproteinase-3, but increased the IL-10 expression in the mucosa of children and adults with IBD |
| 8 | Midura-Kiela et al., 2012 [76] | Curcumin inhibits interferon-gamma signaling in colonic epithelial cells | Curcumin (98.05%; 0, 25, 50, and 75 µM) free of contaminating curcuminoids | T-84 cells and young adult mouse colonocyte cells | Curcumin obstructed the IFN-α signaling and induced the transcription of genes (i.e., CII-TA and MHC-II) and T cell chemokines (CXCL9, CXCL10, and CXCL11) |
| 9 | Motawi et al., 2012 [88] | Effects of curcumin and ginkgo biloba on matrix metalloproteinases gene expression and other biomarkers of inflammatory bowel disease | Curcumin was given at a concentration of 2.0% (wt/wt) (three days before the treatment and five days after induction) | Wistar rats/TNBS colitis | Reduced the MPO activity and pro-inflammatory cytokine TNF-α and attenuated the MMP-1, MMP-3, and TIMP-1 expression. |
| 10 | Miller et al., 2014 [89] | Curcumin: a double hit on malignant mesothelioma | Curcumin (0–50 µM) for 24–72 h | Mouse and human malignant mesothelioma (MM) cells and LP9/TERT-1 | Curcumin effectively suppressed the inflammation-related genes (i.e., NF-κB, TLR, and IL-1β) |
| 11 | McFadden et al., 2015 [31] | The role of curcumin in modulating colonic microbiota during colitis and colon cancer prevention | 98.05% of pure curcumin (8–162 mg/kg/daily, for 0.05% and 1% diets) free of contaminating curcuminoids | Il10−/− mice on 129/SvEv | Curcumin enhanced the survival rate and reduced the colon weight/length ratio while no changes were seen in the control. Besides, curcumin efficiently managed the age-linked reduction in alpha diversity and improved the histology of the colon, bacterial richness, and the lactobacilli level in AOM/Il102/2 |
| 12 | Cooney et al., 2016 [45] | A combined omics approach to evaluate the effects of dietary curcumin on colon inflammation in the Mdr1a −/− mouse model of inflammatory bowel disease | 0.2% of curcumin (≥ 94% curcuminoid content and ≥ 80% curcumin) added to the diet | Mdr1a −/− mouse model | The study showed the activation of α-catenin regulates the anti-inflammatory effects of curcumin in the Mdr1a−/− mouse colon. Curcumin reduced the immune response and improved xenobiotic metabolism and resolution of inflammation by the reduction in neutrophil migration and increase in barrier remodeling. Curcumin effectively downregulated the ERK, FN1, TNFSF12, and PI3K complex activated during inflammation. |
| 13 | Loganes et al., 2017 [92] | Curcumin anti-apoptotic action in a model of intestinal epithelial inflammatory damage | 1 µM curcumin (0–24 h) | HT29 cells | Curcumin treatment of HT29 cells before the inflammatory stimulation of IFN-γ decreased the cell apoptosis rate. Curcumin-induced anti-apoptotic activity was associated with the decrease in the IL-7 secretion in the HT29 cells, but, surprisingly, no effect on the NF-κB signaling pathway was observed. Curcumin exhibited a minor effect on the phosphorylation of proteins in this inflammatory signaling pathway. |
| 14 | Yang et al., 2018 [93] | Comparative effects of curcumin and tetrahydrocurcumin on DSS-induced colitis and inflammatory signaling in mice | Oral administration of curcumin/tetrahydrocurcumin with 0.05% carboxymethyl (0.1 or 0.25 mmol/kg) for seven days | Male ICR mice/DSS colitis | Curcumin was effective against DSS-induced colitis in mice, suppressed the NF-κB and STAT3 activation, and reduced the COX-2 and iNOS expression |
| 16 | Yue et al., 2019 [95] | Curcumin ameliorates dextran sulfate sodium-induced colitis in mice via regulation of autophagy and intestinal immunity | Curcumin (5 mg/kg and 60 mg/kg) added to the diet, eight days | BALB/c mice/ DSS colitis | Curcumin administration effectively controlled the progress of the DSS-induced colitis in mice by regulating cytokine networks and obstructing excessive autophagy |
| 17 | Zhang et al., 2019 [96] | Curcumin and resveratrol suppress dextran sulfate sodium-induced colitis in mice | Curcumin (50 mg/kg) added to the diet, 14 days | BALB/c mice/DSS colitis | Curcumin and resveratrol effectively treat the experimental colitis in mice by attenuating the intestinal inflammatory cascade reaction, decreasing the autophagy, and controlling the signals of SIRT1/mTOR. |
| 18 | Wei et al., 2021 [97] | Curcumin ameliorates DSS‑induced colitis in mice by regulating the Treg/Th17 signaling pathway | Curcumin (100 mg/kg) added to the diet, seven days | Mice/DSS colitis | Curcumin showed the protective effects against DSS colitis in mice by mediating the re-equilibration of Treg/Th17 cells. The regulatory mechanism is possibly associated with IL‑23/Th17. |
| S. No | Author/Year | Study Title | Modified Curcumin Formulations/Curcumin with Other Therapeutic Molecules | Cell Line/Animal Model | Main Findings |
|---|---|---|---|---|---|
| 1 | Li et al., 2007 [99] | Liposomal curcumin with and without oxaliplatin: effects on cell growth, apoptosis, and angiogenesis in colorectal cancer | Liposomal curcumin with oxaliplatin | LoVo and Colo205 cells and nu/nu mice | Liposomal curcumin exhibited a dose-based inhibition in the growth of colon cell lines LoVo and Colo205. The in vivo studies revealed the efficiency of liposomal curcumin by attenuating the CD3 expression, vascular endothelial growth factor, and IL-8 in a mice model. |
| 2 | Yadav et al., 2009a [100] | Effect of cyclodextrin complexation of curcumin on its solubility and antiangiogenic and anti-inflammatory activity in rat colitis model | Curcumin-cyclodextrin complex | Sprague–Dawley rats, DSS colitis | Curcumin-cyclodextrin complex inhibited the activation of NF-κB and blockade of infiltration of inflammatory cells (CD4 and CD8 T cells). It attenuated DSS-induced colitis in rats. |
| 3 | Yadav et al., 2009b [101] | Novel formulation of solid lipid microparticles of curcumin for anti-angiogenic and anti-inflammatory activity for optimization of therapy of inflammatory bowel disease | Solid lipid microparticles of curcumin (curcumin SLM) | Sprague–Dawley rats, DSS colitis | The increase in body weight and colon length in curcumin SLM-treated rats when compared with native curcumin-treated and DSS control rats. It reduced the number of cells in the mucosa of the colon and effectively reduced the degree of colitis. |
| 4 | Gugulothu et al., 2014 [102] | pH-Sensitive nanoparticles of curcumin-celecoxib combination: evaluating drug synergy in ulcerative colitis model | Curcumin-celecoxib-loaded polymeric nanoparticles (CUR-CelNPs) | Sprague-Dawley rats TNBS colitis | CUR—CelNPs considerably reduced the MPO and LPO activity as well as increased the superoxide dismutase (SOD) activity when compared with curcumin or nanoparticles alone. The synergic effect of curcumin and celecoxib exhibits the better therapeutic effect in treating UC. |
| 5 | Beloqui et al., 2014 [29] | pH-sensitive nanoparticles for colonic delivery of curcumin in inflammatory bowel disease | Curcumin polymeric nanoparticles combining both poly (lactic-co-glycolic) acid (PLGA) and polymethacrylate | Caco-2 cells, C57BL/6 mice, DSS-induced colitis | Curcumin polymeric nanoparticles considerably decreased the secretion of TNF-α in LPS-stimulated macrophages. They effectively reduced the neutrophil infiltration and secretion of TNF-α and helped maintain the colon structure like in the control group in a DSS-induced colitis model. |
| 6 | Li et al., 2015 [105] | Curcumin—piperine mixtures in self-microemulsifying drug delivery system for ulcerative colitis therapy | Curcumin and piperine co-encapsulated into a nanoformulation (CUR-PIP-SMEDDS) | BALB/c mice (pathogen-free), DSS-induced colitis | More stable in colons, increased encapsulation. Use of CUR-PIP-SMEDDS showed a better anti-colitis activity in the inflamed colon region. |
| 7 | Mutalik et al., 2016 [106] | Development and performance evaluation of novel nanoparticles of a grafted copolymer loaded with curcumin | Curcumin polymeric nanoparticles | HCT116 cells Wistar rats, acetic acid-induced colitis | Curcumin polymeric nanoparticles showed a controlled and targeted release of curcumin as well as better absorption than when delivered as free curcumin. They effectively decreased the myeloperoxidase and nitrite levels. Furthermore, they prevented the loss of body weight and attenuated colonicinflammation. |
| 8 | Beloqui et al., 2016 [30] | A comparative study of curcumin-loaded lipid-based nanocarriers in the treatment of IBD | Curcumin—lipid based nanocarriers | J774 murine macrophages and Caco-2 cells, C57BL/6 mice, DSS-induced colitis | Increased curcumin retention at the intestinal site and permeability. Curcumin—lipid-based nanocarriers reduced the infiltration of neutrophils and secretion of TNF-α as well as exhibited efficiency for IBD treatment. |
| 9 | Huang et al., 2017 [109] | Effects of curcumin plus soy oligosaccharides on intestinal flora of rats with ulcerative colitis | Curcumin + soy oligosaccharides | Sprague–Dawley rats, DNCB-induced colitis | Combination of curcumin and soy oligosaccharide attenuated the TNF-α and IL- 8 activity and reduced the colonic mucosa inflammation and tissue damage |
| 10 | Ohno et al., 2017 [111] | Nanoparticle curcumin ameliorates experimental colitis via modulation of gut microbiota and induction of regulatory T cells | Curcumin nanoparticles (theracurmin) | HT29 cells, BALB/c mice, DSS-induced colitis | Curcumin nanoparticles decreased the disease activity index, considerably improved mucosal permeability and the histological colitis score. Furthermore, curcumin nanoparticles suppressed the NF-κB activation. |
| 11 | Qiao et al., 2017 [112] | Orally delivered polycurcumin responsive to bacterial reduction for targeted therapy of inflammatory bowel disease | Curcumin polymeric nanoparticles (polyethylene glycol) (PEG) and curcumin (CUR) linked by a disulfide bond) | Caco-2 cells, C57BL/6 mice, DSS-induced colitis | Better solubility and targeted drug delivery in the inflamed regions of the gut. Enhanced transmembrane permeability and bioavailability. Notably, curcumin nanoparticles reduced the progression of the colon disease and effectively protected mice from IBD. |
| 12 | Kesharwani et al., 2018 [113] | Site-directed non-covalent polymer-drug complexes for IBD: formulation development, characterization, and pharmacological evaluation | Curcumin polymeric nanoparticles (Ora-Curcumin-S) | HCT116 and HT29 cells, BALB/cJ mice, DSS-induced colitis | Ora-Curcumin-S exhibited better solubility and stability. It reduced the colitis-associated symptoms. Controlled the loss of body weight, improved the colon length, colon edema, and spleen weight in DSS-induced colitis. |
| 13 | Chen et al., 2018 [114] | Facile fabrication of bowl-shaped microparticles for oral curcumin delivery to ulcerative colitis tissue | Bowl-shaped microparticles loaded with curcumin | Mice, DSS-induced colitis | Prolonged drug release, better encapsulation efficiency, targeted delivery, and excellent hydrophilicity. Supplementation with BMPs loaded with curcumin alleviates UC well based on the DSS-induced mouse model. |
| 14 | Chen et al., 2019 [116] | Oral administration of colitis tissue-accumulating porous nanoparticles for ulcerative colitis therapy | Porous poly (lactic-co-glycolic acid) nanoparticles and pluronic F127 (PF127) loaded with curcumin | Raw 264.7 macrophages, mice, DSS-induced colitis | Better biocompatibility and cellular uptake rate of curcumin than those of porous curcumin-loaded nanoparticles without PF127 modification (porous nanoparticles). They also effectively obstructed secretion of important proinflammatory cytokines (i.e., IL-6, IL-12, and TNF-α) and ameliorated the symptoms of UC. |
| 15 | Sharma et al., 2019 [32] | Improved uptake and therapeutic intervention of curcumin via designing binary lipid nanoparticulate formulation for oral delivery in inflammatory bowel disorder | Curcumin-loaded solid binary lipid nanoparticles (C-SBLNs) | Guinea pigs, DSS-induced colitis | Control and stable release of curcumin, improved cellular uptake, and targeted delivery. Supplementation with C-SBLNs decreased the infiltration of leucocytes, oxidative stress, and secretion of TNF-α and helped to keep the structure of the colon healthy as compared to free curcumin. |
| 16 | Desai and Monim, 2020 [118] | Colon targeted bioadhesive pellets of curcumin and cyclosporine for improved management of inflammatory bowel disease | Polymeric nanoparticles (bioadhesive pellet cores of curcumin) | Wistar rats, acetic acid-induced colitis | Combining curcumin and cyclosporine exhibited synergistic effects of managing IBD. Controlled the loss of weight and enhanced the clinical response, macroscopic and microscopic parameters of induced colitis when compared to cyclosporine and native curcumin. |
| 17 | Oshi et al., 2020 [119] | Curcumin nanocrystal/pH-responsive polyelectrolyte multilayer core−shell nanoparticles for inflammation-targeted alleviation of ulcerative colitis | Curcumin nanocrystal polyelectrolyte (chitosan/sodium alginate/cellulose acetate phthalate as shells) | Mice, DSS-induced colitis | Targeted delivery of curcumin into the inflamed colon tissue and enhanced biodistribution in the stomach and small intestine. Improved effectiveness in reducing inflammation-associated indicators in a DSS-induced colitis mice model. |
| 18 | Luo et al., 2020 [120] | Genipin-cross-linked human serum albumin coating using a tannic acid layer for enhanced oral administration of curcumin in the treatment of UC | Tannic acid (TA)-coated, genipin (Gnp)-crosslinked human serum albumin (HSA)-encapsulated curcumin nanoparticles (TA/CUR-NPs) | Caco-2 cells, mice, DSS-induced colitis | Controlled curcumin release and increased the curcumin uptake in cells. Oral administration of TA/CUR-NPs obstructed the TLR4-linked NF-κB signaling pathway and reduced the colitis symptoms compared to the controls. |
| 19 | Huang et al., 2021 [121] | Oral nanotherapeutics with enhanced mucus penetration and ROS-responsive drug release capacities for delivery of curcumin to colitis tissues | Hydrogel (chitosan/alginate)-embedding pluronic F127—catalase/curcumin nanoparticles (P-CUR/CAT-NPs) | Raw 264.7 macrophages, FVB male mice, DSS-induced colitis |
Improved the cellular uptake efficiency of macrophage cells, effectively reduced the symptoms, and suppressed secretion of the major proinflammatory cytokines |
| 20 | Rotrekl et al., 2021 [122] | Composites of yeast glucan particles and curcumin lead to improvement of dextran sulfate sodium-induced acute bowel inflammation in rats | Curcumin loaded into yeast glucan particles | Wistar rats, DSS-induced colitis | Curcumin loaded into yeast glucan particles decreased the activity of proinflammatory cytokines (i.e., TNF-α, IL-1β, and IL-6) and MMP activity as compared to native curcumin in DSS-induced colitis rats. |
| S. No | Author/Year | Study Title | Dose and Duration | Population and Study Design | Main Findings |
|---|---|---|---|---|---|
| 1 | Cheng, 2001 [132] | Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-the risk or pre-malignant lesions | 500–8000 mg/day, three months | Twenty-five patients with the risk of premalignant lesions in Taiwan. Patients with resection of bladder cancer, oral leukoplakia, stomach metaplasia, cervical intraepithelial neoplasm, and Bowen’s disease enrolled in this clinical trial. |
|
| 2 | Sharma et al., 2004 [133] | Phase I clinical trial of oral curcumin: biomarkers of systemic activity and compliance | 0.45 to 3.6 g/day, four months | Fifteen patients with colorectal cancer resistant to chemotherapy participated in this clinical trial |
|
| 3 | Holt et al., 2005 [129] | Curcumin therapy in inflammatory bowel disease: a pilot study | Curcumin (550 mg and 360 mg/day) two times for the first month and three times for the second month | Five CD patients; pilot study |
|
| 4 | Hanai et al., 2006 [123] | Curcumin maintenance therapy for ulcerative colitis: randomized, multicenter, double-blind, placebo-controlled trial | Curcumin (capsules) (2 g) + 1.5–3 g 5-ASA or 1–3 g sulfasalazine/day (n = 45) or placebo + 5-ASA/sulfasalazine (n = 44) (six months) | 89 patients participated in this clinical trial. Multicenter, randomized, double-blind, placebo-controlled study |
|
| 5 | Singla et al., 2014 [124] | Induction with NCB-02 (curcumin) enema for mild-to-moderate distal ulcerative colitis—a randomized, placebo-controlled, pilot study | 140 mg NCB-02 (curcumin extract) enema + oral 1.6 g 5-ASA/day (n = 28) or placebo enema + oral 1.6 g5-ASA/day (n = 22), eight weeks | Mild to moderate UC patients (n = 45). Pilot, double-blind, randomized, placebo-controlled study |
|
| 6 | Lang et al., 2015 [125] | Curcumin in combination with mesalamine induces remission in patients with mild-to-moderate ulcerative colitis in a randomized controlled trial | Curcumin (capsules) (3 g) + 4 g 5-ASA/day (n = 26) or placebo + 4 g 5-ASA/day (n = 24), one month | Mild or moderate UC patients (n = 50). Multicenter, randomized, double-blind, placebo-controlled study |
|
| 7 | Kedia et al., 2017 [134] | Low dose oral curcumin is not effective in induction of remission in mild to moderate ulcerative colitis: results from a randomized double a blind placebo-controlled trial | Curcumin (450 mg/day) + 2.4 g 5-ASA/day (n = 29) or placebo + 2.4 g 5-ASA/day (n = 33), eight weeks | Mild or moderate UC patients (n = 62). Single-center, double-blind, randomized, placebo-controlled study |
|
| 8 | Peterson et al., 2018 [126] | Effects of turmeric and curcumin dietary supplementation on human gut microbiota: a double-blind, randomized, placebo-controlled pilot study | Turmeric tablets (C. longa (1000 mg) + piperine (1.25 mg)) and curcumin tablets (curcumin (1000 mg) and piperine (1.25 mg)); the subjects were advised to take three tablets orally with food two times per day (total 6000 mg daily) | UC patients (n = 30). Randomized, double-blind, placebo-controlled study |
|
| 9 | Shapira et al., 2018 [135] | Of mice and men: a novel dietary supplement for the treatment of ulcerative colitis | Two Coltect (500 mg curcumin, 250 mg green tea, and 100 µg selenium) tablets two times daily for eight weeks | Mild or moderate UC patients (n = 20) |
|
| 10 | Sadeghi et al., 2020 [127] | The effect of curcumin supplementation on clinical outcomes and inflammatory markers in patients with ulcerative colitis | Curcumin (1.500 mg/day) + routine drugs (n = 35) or placebo + routine drugs (n = 35), eight weeks | Mild or moderate UC patients (n = 70). Double-blind, randomized, placebo-controlled study |
|
| 11 | Sugimoto et al., 2020 [130] | Highly bioavailable curcumin derivative ameliorates Crohn’s disease symptoms: a randomized, double-blind, multicenter study | Theracurcumin (360 mg/day, n = 20) or placebo (n = 10), 12 weeks | Mild or moderate CD patients (n = 30). Randomized, double-blind, placebo-controlled, multicenter study |
|
| 12 | Bommelaer et al., 2020 [131] | Oral curcumin no more effective than placebo in preventing recurrence of crohn’s disease after surgery in a randomized controlled trial | 2.5 mg/kg azathioprine; subjects were arbitrarily allocated to the oral curcumin (3 g/day; n = 31) group and the placebo (n = 31) group for six months | CD patients (n = 60). Multicenter, randomized, double-blind, placebo-controlled study |
|
| 13 | Banerjee et al., 2020 [128] | Novel bioenhanced curcumin with mesalamine for induction of clinical and endoscopic remission in mild-to-moderate ulcerative colitis: a randomized, double-blind placebo-controlled pilot study | The standard dose of mesalamine was randomized to either 50 mg bio-enhanced curcumin (BEC) or an identical placebo twice daily | Mild or moderately active UC patients (n = 69). Randomized, double-blind, placebo-controlled, pilot study |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karthikeyan, A.; Young, K.N.; Moniruzzaman, M.; Beyene, A.M.; Do, K.; Kalaiselvi, S.; Min, T. Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook. Pharmaceutics 2021, 13, 484. https://doi.org/10.3390/pharmaceutics13040484
Karthikeyan A, Young KN, Moniruzzaman M, Beyene AM, Do K, Kalaiselvi S, Min T. Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook. Pharmaceutics. 2021; 13(4):484. https://doi.org/10.3390/pharmaceutics13040484
Chicago/Turabian StyleKarthikeyan, Adhimoolam, Kim Na Young, Mohammad Moniruzzaman, Anteneh Marelign Beyene, Kyoungtag Do, Senthil Kalaiselvi, and Taesun Min. 2021. "Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook" Pharmaceutics 13, no. 4: 484. https://doi.org/10.3390/pharmaceutics13040484