
Umbilical Cord, Maternal Milk, and Breastfed Infant Levetiracetam Concentrations Monitoring at Delivery and during Early Postpartum Period


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EURAP—An International Antiepileptic Drugs and Pregnancy Registry. Interim Report, November 2020. Available online: https://eurapinternational.org/wp-content/uploads/2020/01/EurapReport_NOV-2019.pdf (accessed on 19 February 2021).
- Kacirova, I.; Grundmann, M. Trend analysis of the utilization of antiepileptic drugs in pregnant women with epilepsy in Moravian-Silesian region of the Czech Republic. Klin. Farmakol. Farm. 2016, 30, 23–28. [Google Scholar]
- Voinescu, P.E.; Park, S.; Chen, L.Q.; Stowe, Z.N.; Newport, D.J.; Ritchie, J.C.; Pennell, P.B. Antiepileptic drug clearances during pregnancy and clinical implications for women with epilepsy. Neurology 2018, 91, e1228–e1236. [Google Scholar] [CrossRef] [PubMed]
- Tomson, T.; Palm, R.; Källén, K.; Ben-Menachem, E.; Söderfeldt, B.; Danielsson, B.; Johansson, R.; Luef, G.; Öhman, I. Pharmacokinetics of Levetiracetam during Pregnancy, Delivery, in the Neonatal Period, and Lactation. Epilepsia 2007, 48, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Westin, A.A.; Reimers, A.; Helde, G.; Nakken, K.O.; Brodtkorb, E. Serum concentration/dose ratio of levetiracetam before, during and after pregnancy. Seizure 2008, 17, 192–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reisinger, T.; Newman, M.; Loring, D.; Pennell, P.; Meador, K. Antiepileptic drug clearance and seizure frequency during pregnancy in women with epilepsy. Epilepsy Behav. 2013, 29, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannessen, S.I.; Helde, G.; Brodtkorb, E. Levetiracetam Concentrations in Serum and in Breast Milk at Birth and during Lactation. Epilepsia 2005, 46, 775–777. [Google Scholar] [CrossRef]
- Johannessen, S.I.; Helde, G.; Brodtkorb, E. Levetiracetam in pregnancy and lactation: Preliminary observation. Epilepsia 2004, 45 (Suppl. 3), 58. [Google Scholar]
- Dinavitser, N.; Kohn, E.; Berlin, M. Levetiracetam monitoring in breast-milk: High inter-individual variability. Arch. Dis. Child. 2019, 104, 14. [Google Scholar] [CrossRef] [Green Version]
- Bank, A.M.; Stowe, Z.N.; Newport, D.J.; Ritchie, J.C.; Pennell, P.B. Placental passage of antiepileptic drugs at delivery and neonatal outcomes. Epilepsia 2017, 58, e82–e86. [Google Scholar] [CrossRef] [PubMed]
- Ylikotila, P.; Ketola, R.A.; Timonen, S.; Malm, H.; Ruuskanen, J.O. Early pregnancy cerebral venous thrombosis and status epilepticus treated with levetiracetam and lacosamide throughout pregnancy. Reprod. Toxicol. 2015, 57, 204–206. [Google Scholar] [CrossRef]
- López-Fraile, I.P.; Cid, A.O.; Juste, A.O.; Modrego, P.J. Levetiracetam plasma level monitoring during pregnancy, delivery, and postpartum: Clinical and outcome implications. Epilepsy Behav. 2009, 15, 372–375. [Google Scholar] [CrossRef]
- Kramer, G.; Hosli, I.; Glanzmann, R. Levetiracetam accumulation in human breast milk. Epilepsia 2002, 43 (Suppl. 7), 105. [Google Scholar]
- Greenhill, L.; Betts, T.; Yarrow, H. Breast milk levels of levetiracetam after delivery. Epilepsia 2004, 45 (Suppl. 7), 230. [Google Scholar] [CrossRef]
- Kohn, E.; Brandriss, N.; Soback, S.; Bar-Haim, A.; Berkovitch, M. Levetiracetam and lamotrigine excretion in breast milk. Reprod. Toxicol. 2016, 60, 184. [Google Scholar] [CrossRef]
- Paret, N.; Gouraud, A.; Bernard, N. Long-term follow-up of infants exposed to levetiracetam during breastfeeding: Comparison to a control group. Birth Defects Res. Clin. Mol. Teratol. 2014, 100, 537–538. [Google Scholar]
- Birnbaum, A.K.; Meador, K.J.; Karanam, A.; Brown, C.; May, R.C.; Gerard, E.E.; Gedzelman, E.R.; Penovich, P.E.; Kalayjian, L.A.; Cavitt, J.; et al. Antiepileptic Drug Exposure in Infants of Breastfeeding Mothers with Epilepsy. JAMA Neurol. 2020, 77, 441–450. [Google Scholar] [CrossRef] [PubMed]
- The Drug and Lactation Database (LACTMED), a Database of the National Library of Medicine’s TOXNET System. Available online: https://toxnet.nlm.nih.gov/ (accessed on 19 February 2021).
- Patsalos, P.N.; Spencer, E.P.; Berry, D.J. Therapeutic Drug Monitoring of Antiepileptic Drugs in Epilepsy: A 2018 Update. Ther. Drug Monit. 2018, 40, 526–548. [Google Scholar] [CrossRef] [PubMed]
- Keizer, R.J.; Jansen, R.S.; Rosing, H.; Thijssen, B.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R. Incorporation of concentration data below the limit of quantification in population pharmacokinetic analyses. Pharmacol. Res. Perspect. 2015, 3, e00131. [Google Scholar] [CrossRef]
- Johnson, E.L.; Stowe, Z.N.; Ritchie, J.C.; Newport, D.J.; Newman, M.L.; Knight, B.; Pennell, P.B. Carbamazepine clearance and seizure stability during pregnancy. Epilepsy Behav. 2014, 33, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.I.; Pennell, P.B. Management of epilepsy during pregnancy: An update. Ther. Adv. Neurol. Disord. 2016, 9, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, C.M.; Capparelli, E.V.; Mower, A.; Farrell, M.J.; Soldin, S.J.; Haas, R.H. A seven-day study of the pharmacokinetics of intravenous levetiracetam in neonates: Marked changes in pharmacokinetics occur during the first week of life. Pediatr. Res. 2012, 72, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merhar, S.L.; Schibler, K.R.; Sherwin, C.M.; Meinzen-Derr, J.; Shi, J.; Balmakund, T.; Vinks, A.A. Pharmacokinetics of Levetiracetam in Neonates with Seizures. J. Pediatr. 2011, 159, 152–154.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mruk, A.L.; Garlitz, K.L.; Leung, N.R. Levetiracetam in Neonatal Seizures: A Review. J. Pediatr. Pharmacol. Ther. 2015, 20, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, J.-M.; Bouzom, F.; Hugues, C.; Ungell, A.-L. Oral drug absorption in pediatrics: The intestinal wall, its developmental changes and current tools for predictions. Biopharm. Drug Dispos. 2017, 38, 209–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mothers/Infants | Characteristics | Delivery | 2–4 Days after Delivery | 7–31 Days after Delivery | |||
|---|---|---|---|---|---|---|---|
| N | mean ± SD (range) | N | mean ± SD (range) | N | mean ± SD (range) | ||
| Mothers: | age (years) | 14 | 27 ± 5 (18–37) | 58 | 29 ± 5 (18–41) | 8 | 30 ± 3 (27–34) |
| Concomitant antiseizure medication | lamotrigine (mg/day) | 6 | 300 ± 155 (200–600) | 21 | 371 ± 112 (150–550) | 6 | 275 ± 96 (200–400) |
| valproic acid (mg/day) | 1 | 500 | 2 | 875 ± 530 (500–1250) | 0 | - | |
| topiramate (mg/day) | 1 | 100 | 3 | 183 ± 76 (100–250) | 0 | - | |
| carbamazepine (mg/day) | 0 | - | 6 | 717 ± 184 (400–900) | 1 | 400 | |
| zonisamide (mg/day) | 0 | - | 2 | 525 ± 35 (500–550) | 2 | 525 ± 35 (500–550) | |
| lacosamide (mg/day) | 0 | - | 1 | 200 | 0 | - | |
| Infants: | weight (kg) | 10 | 3.3 ± 0.4 (2.6–3.9) | 51 | 3.2 ± 0.4 (2.0–4.0) | 10 | 3.1 ± 0.5 (2.1–3.7) |
| length (cm) | 10 | 49 ± 2 (45–50) | 51 | 48 ± 3 (37–52) | 10 | 48 ± 3 (42–50) | |
| female | 7 | 33 | 5 | ||||
| male | 2 | 20 | 5 |
| Levetiracetam | Weight (kg) | Dose mg/Day) | Dose/kg (mg/kg) | Cl (L/kg) | M (mg/L) | UC (mg/L) | UC/M Ratio |
|---|---|---|---|---|---|---|---|
| number | 11 | 12 | 11 | 11 | 14 | 14 | 14 |
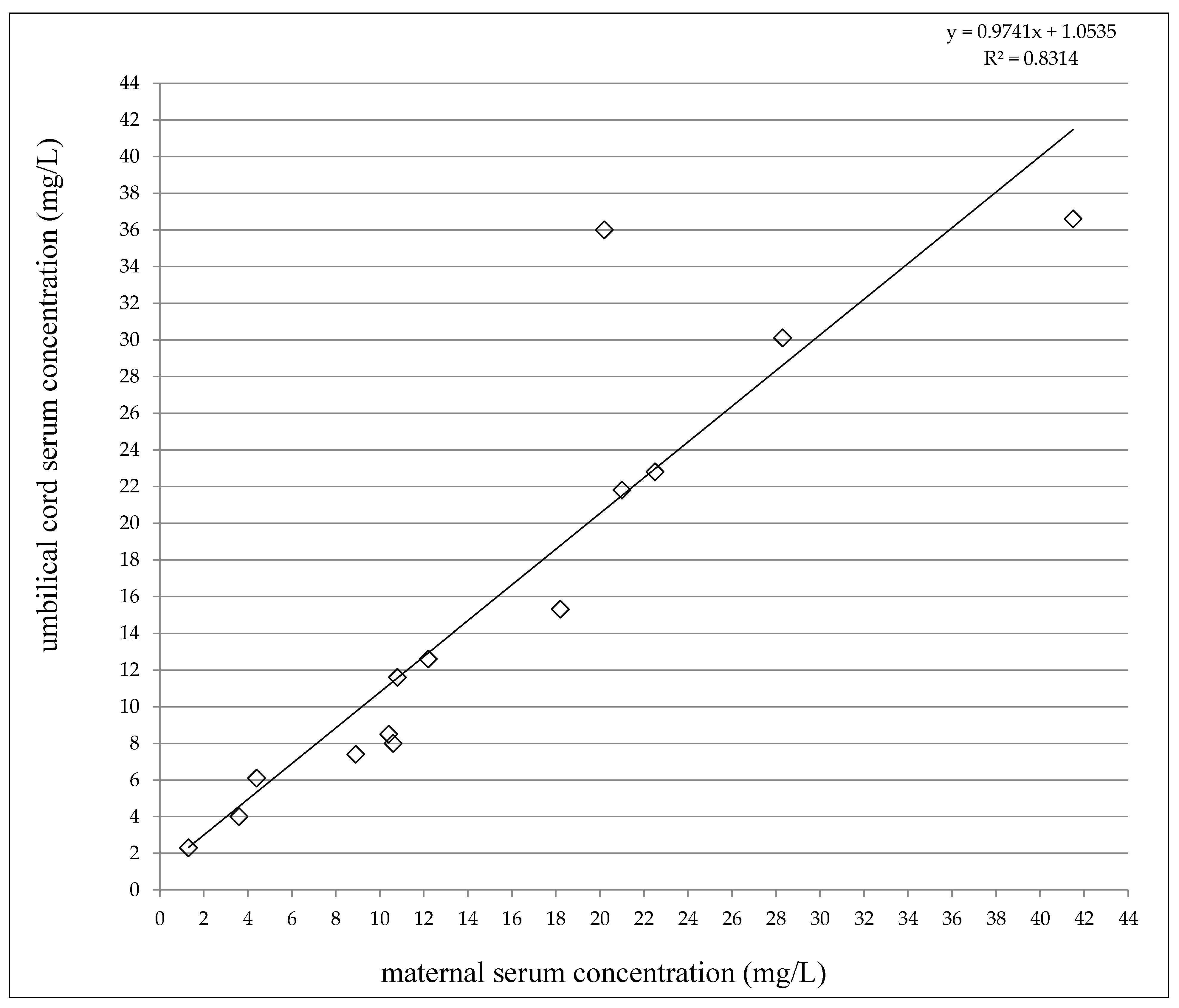
| median range | 75 68–114 | 1500 250–3000 | 17.0 3.7–34.5 | 1.39 0.83–3.37 | 11.5 1.3–41.5 | 12.1 2.3–36.6 | 1.04 0.75–1.78 |
| mean ± SD | 81 ± 15 | 1438 ± 813 | 18.6 ± 10.5 | 1.48 ± 0.69 | * 15.3 ± 10.9 | * 15.9 ± 11.6 | 1.10 ± 0.33 |
| LEV Mono + Neutral Drugs | Weight (kg) | Dose (mg/day) | Dose (mg/kg) | Cl (L/kg) | M (mg/L) | Mi (mg/L) | I (mg/L) | Mi/M Ratio | I/M Ratio | I/Mi Ratio |
|---|---|---|---|---|---|---|---|---|---|---|
| number | 45 | 50 | 44 | 44 | 51 | 47 | 49 | 47 | 45 | 41 |
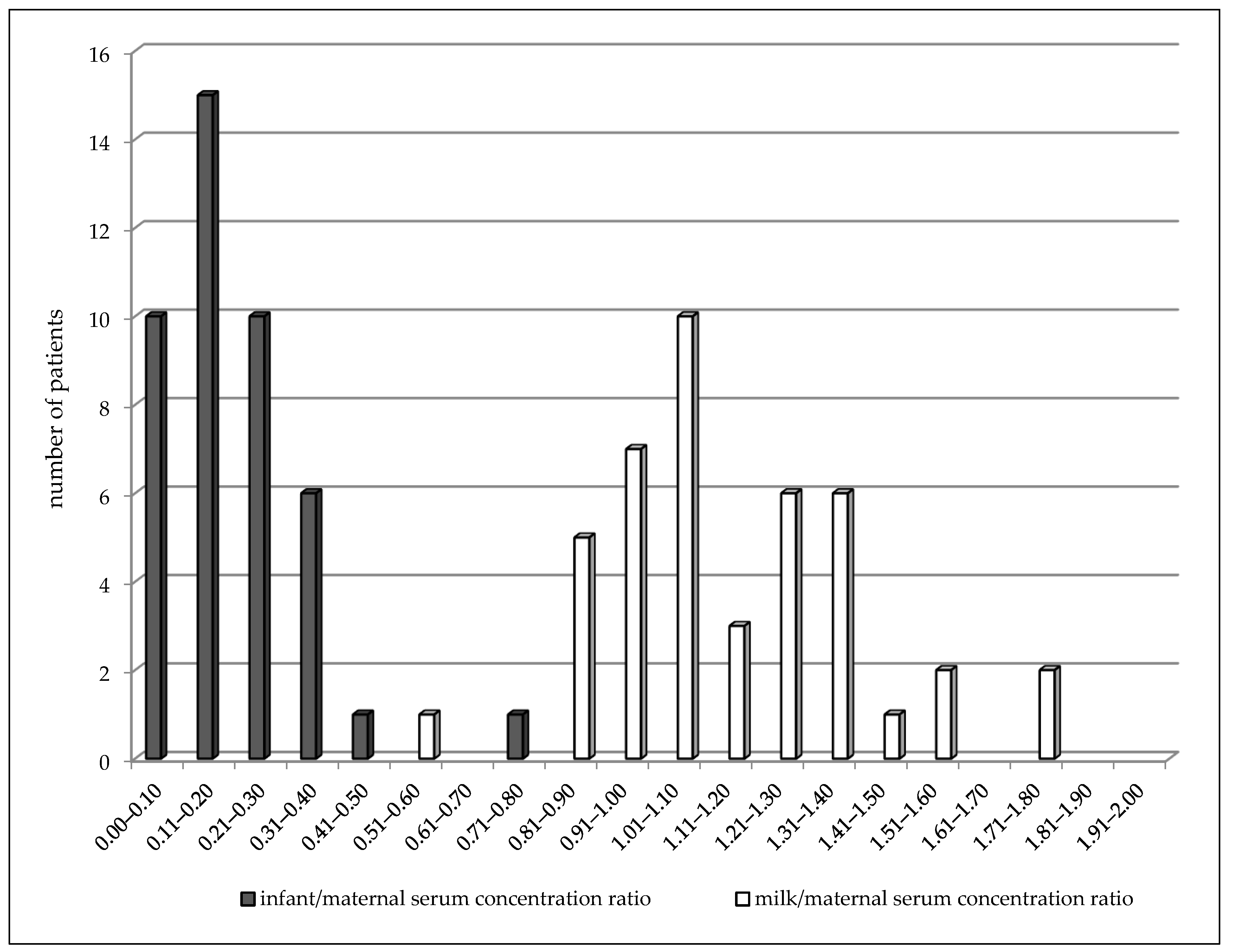
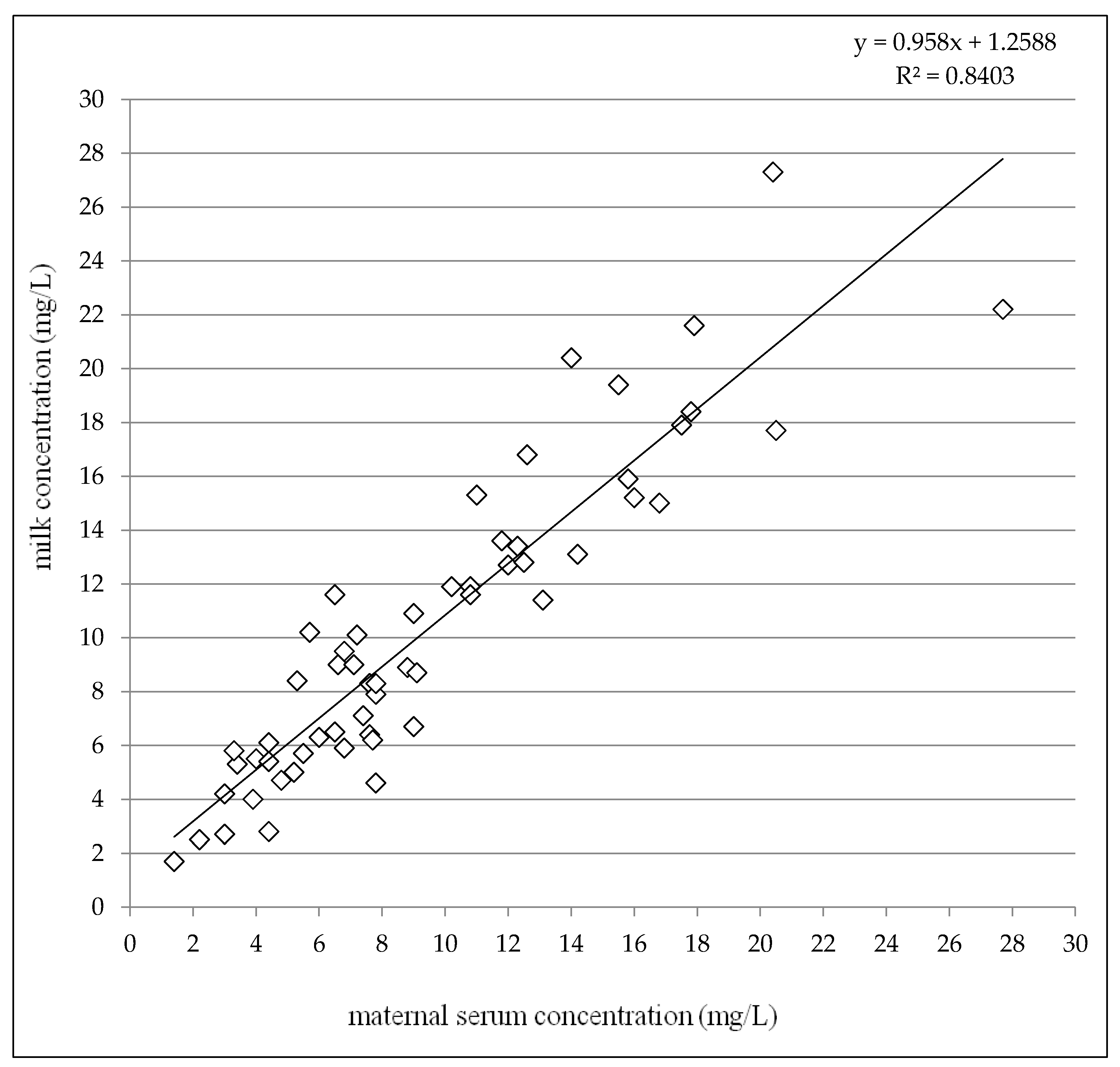
| median range | 73 55–125 | 1500 500–4000 | 17.6 6.8–50.0 | 2.22 1.23–5.38 | 8.8 1.4–35.7 | 9.0 1.7–27.3 | 1.4 0.5–6.3 | 1.09 0.59–1.79 | 0.16 0.03–0.71 | 0.17 0.03–0.52 |
| mean ± SD | 76 ± 14 | 1625 ± 870 | 21.4 ± 12.1 | 2.47 ± 1.03 | 10.1 ± 6.5 | 10.5 ± 5.7 | 1.8 ± 1.4 | 1.16 ± 0.27 | 0.20 ± 0.13 | 0.18 ± 0.12 |
| LEV + CBZ | ||||||||||
| number | 5 | 5 | 5 | 5 | 5 | 4 | 5 | 4 | 4 | 3 |
| median range | 68 57–76 | 1000 500–2500 | 17.2 6.6–33.8 | 3.65 0.97–4.57 | 4.8 2.2–7.4 | 5.3 2.5–7.1 | 0.5 0.5–0.5 | 0.97 0.87–1.14 | 0.12 0.07–0.23 | 0.11 0.07–0.20 |
| mean ± SD | 67 ± 9 | 1100 ± 822 | 16.5 ± 11.0 | 3.37 ± 1.43 | 5.0 ± 2.1 | 5.1 ± 2.0 | 0.5 ± 0.0 | 0.99 ± 0.11 | 0.13 ± 0.07 | 0.13 ± 0.07 |
| Total | ||||||||||
| number | 50 | 55 | 49 | 49 | 56 | 51 | 54 | 51 | 49 | 44 |
| median range | 72 55–125 | 1500 500–4000 | 17.2 6.6–50.0 | 2.33 0.97–5.38 | * 7.7 1.4–35.7 | * 8.9 1.7–27.3 | 1.2 0.5–6.3 | 1.07 0.59–1.79 | 0.16 0.03–0.71 | 0.17 0.03–0.52 |
| mean ± SD | 75 ± 14 | 1577 ± 872 | 20.9 ± 11.9 | 2.56 ± 1.10 | 9.6 ± 6.4 | 10.1 ± 5.6 | 1.7 ± 1.4 | 1.14 ± 0.27 | 0.19 ± 0.13 | 0.18 ± 0.12 |
| Weight (kg) | Dose (mg/Day) | Dose/kg (mg/kg) | Cl (L/kg) | M (mg/L) | Mi (mg/L) | I (mg/L) | Mi/M Ratio | I/M Ratio | I/Mi Ratio | |
|---|---|---|---|---|---|---|---|---|---|---|
| 7–31 days after delivery | ||||||||||
| number | 6 | 7 | 6 | 6 | 8 | 7 | 10 | 7 | 3 | 2 |
| median range | 70 57–73 | 2000 1000–3000 | 34.1 13.9–52.6 | 3.48 1.78–7.31 | * 10.1 4.4–28.6 | * 10.1 2.8–21.6 | 2.0 0.5–5.1 | 1.06 0.64–1.40 | 0.12 0.11–0.20 | 0.14 0.10–0.18 |
| mean ± SD | 68 ± 6 | 2214 ± 699 | 34.1 ± 13.5 | 4.14 ± 2.30 | 12.9 ± 8.0 | 11.3 ± 6.0 | 2.3 ± 1.4 | 1.04 ± 0.24 | 0.14 ± 0.05 | 0.14 ± 0.06 |
| Total 2–31 days after delivery | ||||||||||
| number | 56 | 62 | 55 | 55 | 64 | 58 | 64 | 58 | 52 | 46 |
| median range | 71 55–125 | 1500 500–4000 | 17.9 6.6–52.6 | 2.33 0.97–7.31 | ** 7.8 1.4–35.7 | ** 9.0 1.7–27.3 | 1.4 0.5–6.3 | 1.07 0.59–1.79 | 0.16 0.03–0.71 | 0.17 0.03–0.52 |
| mean ± SD | 74 ± 14 | 1649 ± 873 | 22.3 ± 12.7 | 2.73 ± 1.34 | 10.0 ± 6.7 | 10.2 ± 5.7 | 1.8 ± 1.4 | 1.13 ± 0.26 | 0.19 ± 0.13 | 0.17 ± 0.11 |
| Ref | N | Dose (mg/Day) | M (mg/L) | UC (mg/L) | UC/M Ratio | ||||
|---|---|---|---|---|---|---|---|---|---|
| [4] | 13 | 1000–3000 | 1.9–20.4 | 1.2–31.3 | mean 1.15 range 0.56–2.00 | ||||
| [10] | 10 | 750–5000 | mean 22.75 ± 21.81 range 4.00–76.00 | mean 1.12 ± 0.46 range 0.57–2.17 | |||||
| [12] | 5 | 2000–3000 | 3.5–24.9 | 5.7–29.6 | mean 1.21 range 0.92–1.62 | ||||
| [7] | 4 | 2000–3500 | 11.4–48.3 | 16.5–54.8 | mean 1.14 range 0.97–1.45 | ||||
| [8] | 4 | mean 0.87 range 0.69–1.03 | |||||||
| [11] | 1 | 2000 | 17.0 | 23.0 | 1.35 | ||||
| N | Postpartum time | Dose (mg/day) | M (mg/L) | Mi (mg/L) | Mi/M ratio | N | I (mg/L) | I/M ratio | |
| [17] | 58 | 6–20 weeks | 500–5500 | median 24.0 range 0.3–73.5 | 58 | median 0.9 range 0.9–4.5 | median 0.05 range 0.02–0.20 | ||
| [9] | 14 | 3–22 weeks | mean 2517 | mean 0.88 range 0.23–1.10 | |||||
| [14] | 12 | 4 days 2–3 months | lower than maternal levels | ||||||
| [4] | 11 | 4–23 days | 1000–3000 | mean 15.4 range 4.6–34.2 | mean 16.0 range 5.8–35.7 | mean 1.05 range 0.78–1.55 | 10 | mean 1.9 range 0.7–3.4 | mean 0.13 range 0.07–0.22 |
| [7] | 7 1–5 | 3–5 days 2 we-10 mon first 8 weeks | 1500–3500 | mean 13.8 range 4.8–29.8 | mean 12.5 range 4.8–26.0 | mean 1.00 range 0.76–1.33 range 0.93–1.22 | 7 1 | <1.7–2.5 2.5–2.9 | |
| [8] | 4 | 3–4 days 2 w-4 mo | mean 0.93 range 0.76–1.04 range 0.93–1.32 | 4 | below limit of quantification | ||||
| [15] | 1 | 2250 3000 | 18.8 21.0 | 16.0–33.6 29.0–51.7 | |||||
| [11] | 1 | 5 days infant day 8 | 2000 | <3.0 | 1 | <3.0 | |||
| [13] | 1 | 1–2 weeks | 5.4 | 16.8 | 3.09 | 1 | 1.0 (96 h after stop of lactation) | ||
| [16] | 1 | 10 days | 3000 | 1 | 2.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kacirova, I.; Grundmann, M.; Brozmanova, H. Umbilical Cord, Maternal Milk, and Breastfed Infant Levetiracetam Concentrations Monitoring at Delivery and during Early Postpartum Period. Pharmaceutics 2021, 13, 398. https://doi.org/10.3390/pharmaceutics13030398
Kacirova I, Grundmann M, Brozmanova H. Umbilical Cord, Maternal Milk, and Breastfed Infant Levetiracetam Concentrations Monitoring at Delivery and during Early Postpartum Period. Pharmaceutics. 2021; 13(3):398. https://doi.org/10.3390/pharmaceutics13030398
Chicago/Turabian StyleKacirova, Ivana, Milan Grundmann, and Hana Brozmanova. 2021. "Umbilical Cord, Maternal Milk, and Breastfed Infant Levetiracetam Concentrations Monitoring at Delivery and during Early Postpartum Period" Pharmaceutics 13, no. 3: 398. https://doi.org/10.3390/pharmaceutics13030398