
Stability Evaluation of Extemporaneously Compounded Vancomycin Ophthalmic Drops: Effect of Solvents and Storage Conditions

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Vancomycin Ophthalmic Drops
2.2. Stability Testing of Vancomycin Ophthalmic Drops
- (a)
- Chemical Analysis of vancomycin using HPLC method
- (b) Microbiological Assay
2.3. Statistical Analysis
3. Results
3.1. Appearance and PH of Vancomycin Ophthalmic Formulations
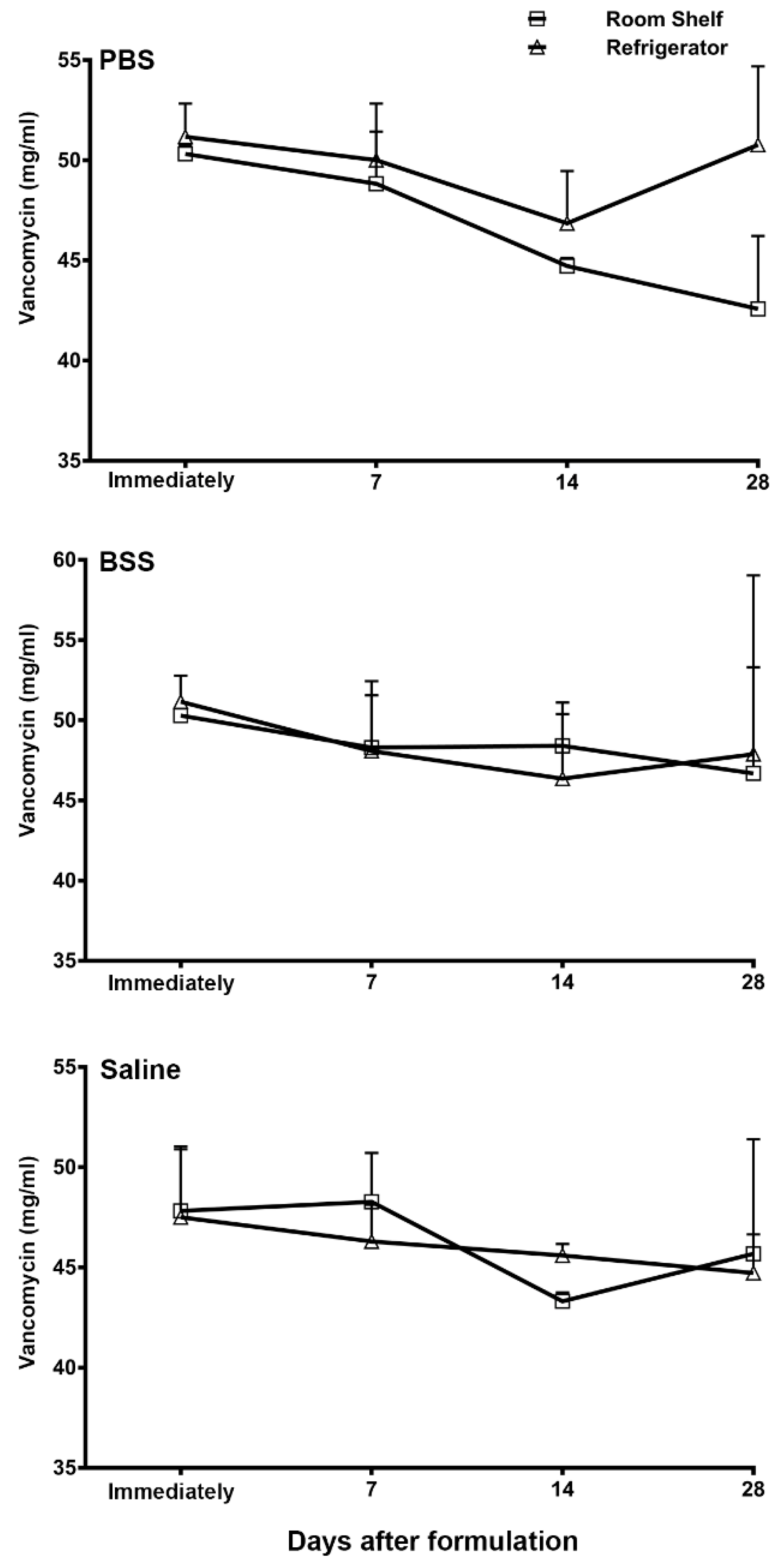
3.2. HPLC Quantification of Vancomycin Ophthalmic Formulations
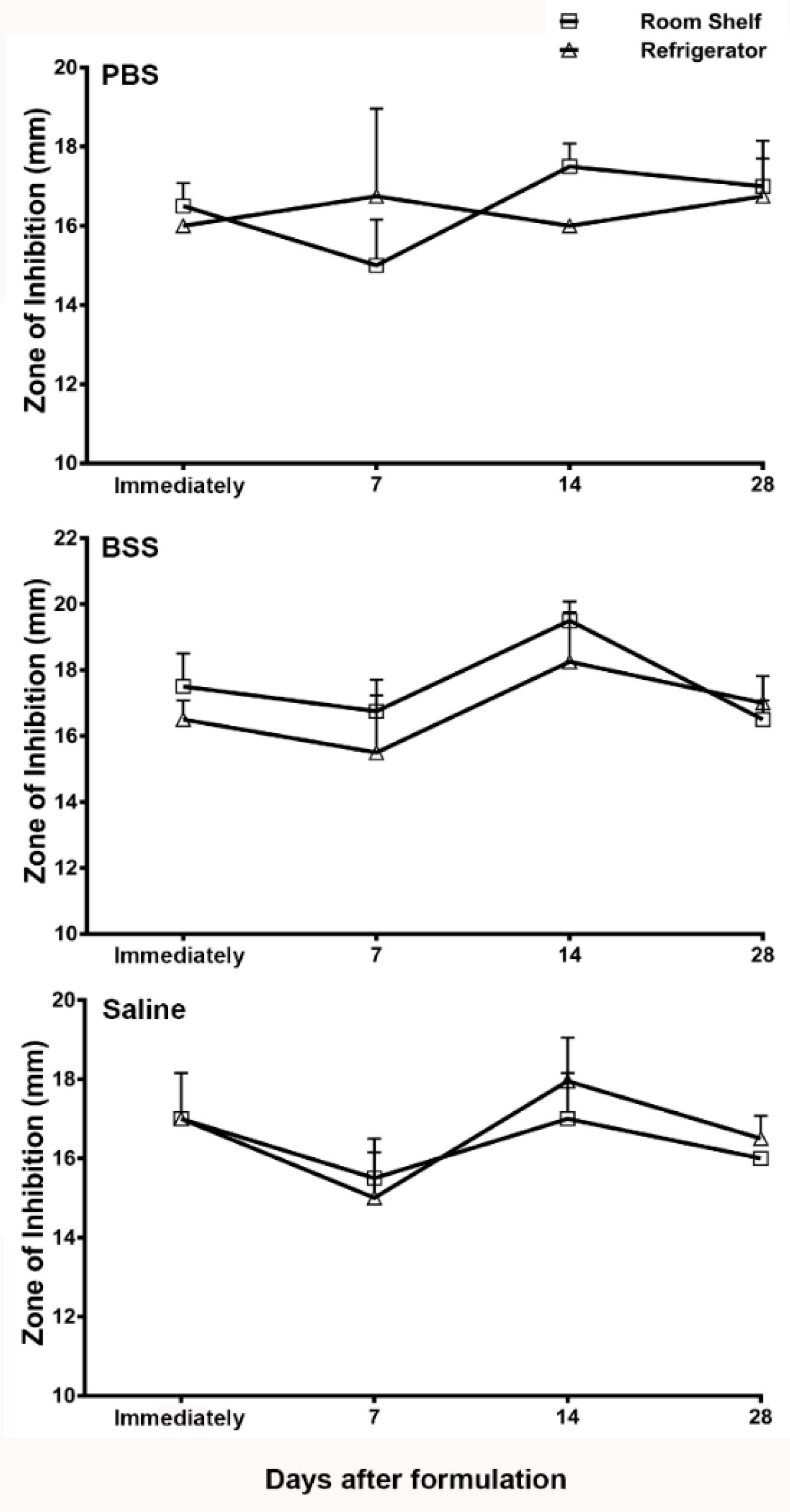
3.3. Microbiology Assay of Vancomycin Ophthalmic Formulations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mah, F.S.; Davidson, R.; Holland, E.J.; Hovanesian, J.; John, T.; Kanellopoulos, J.; Shamie, N.; Starr, C.; Vroman, D.; Kim, T. Current knowledge about and recommendations for ocular methicillin-resistant Staphylococcus aureus. J. Cataract Refract. Surg. 2014, 40, 1894–1908. [Google Scholar] [CrossRef]
- Otri, A.M.; Fares, U.; Al-Aqaba, M.A.; Miri, A.; Faraj, L.A.; Said, D.G.; Maharajan, S.; Dua, H.S. Profile of sight-threatening infectious keratitis: A prospective study. Acta Ophthalmol. 2013, 91, 643–651. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Stein, G.E.; Johnson, L.B. Ceftaroline: A novel cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Clin. Infect. Dis. 2011, 52, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- White, B.P.; Barber, K.E.; Stover, K.R. Ceftaroline for the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Am. J. Health Syst. Pharm. 2017, 74, 201–208. [Google Scholar] [CrossRef]
- Hassoun, A.; Linden, P.K.; Friedman, B. Incidence, prevalence, and management of MRSA bacteremia across patient populations—A review of recent developments in MRSA management and treatment. Crit. Care 2017, 21, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballhausen, B.; Kriegeskorte, A.; Schleimer, N.; Peters, G.; Becker, K. The mecA homolog mecC confers resistance against β-lactams in Staphylococcus aureus irrespective of the genetic strain background. Antimicrob. Agents Chemother. 2014, 58, 3791–3798. [Google Scholar] [CrossRef] [Green Version]
- Fuda, C.; Suvorov, M.; Vakulenko, S.B.; Mobashery, S. The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a of methicillin-resistant Staphylococcus aureus. J. Biol. Chem. 2004, 279, 40802–40806. [Google Scholar] [CrossRef] [Green Version]
- Peacock, S.J.; Paterson, G.K. Mechanisms of Methicillin Resistance in Staphylococcus aureus. Annu. Rev. Biochem. 2015, 84, 577–601. [Google Scholar] [CrossRef] [PubMed]
- Llarrull, L.I.; Fisher, J.F.; Mobashery, S. Molecular basis and phenotype of methicillin resistance in Staphylococcus aureus and insights into new beta-lactams that meet the challenge. Antimicrob. Agents Chemother. 2009, 53, 4051–4063. [Google Scholar] [CrossRef] [Green Version]
- Klevens, R.M.; Morrison, M.A.; Nadle, J.; Petit, S.; Gershman, K.; Ray, S.; Harrison, L.H.; Lynfield, R.; Dumyati, G.; Townes, J.M. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA 2007, 298, 1763–1771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, J.C.; Durkee, H.; Miller, D.; Maestre-Mesa, J.; Arboleda, A.; Aguilar, M.C.; Relhan, N.; Flynn, H.W., Jr.; Amescua, G.; Parel, J.M. Molecular epidemiology and resistance profiles among healthcare- and community-associated Staphylococcus aureus keratitis isolates. Infect. Drug Resist. 2019, 12, 831–843. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.J.; Huang, Y.C.; Tan, H.Y.; Ma, D.H.; Lin, H.C.; Yeh, L.K.; Chen, P.Y.; Chen, H.C.; Chuang, C.C.; Chang, C.J. Staphylococcus aureus keratitis: A review of hospital cases. PLoS ONE 2013, 8, e80119. [Google Scholar] [CrossRef] [PubMed]
- Blomquist, P.H. Methicillin-resistant Staphylococcus aureus infections of the eye and orbit. Trans. Am. Ophthalmol. Soc. 2006, 104, 322–345. [Google Scholar] [PubMed]
- Freidlin, J.; Acharya, N.; Lietman, T.M.; Cevallos, V.; Whitcher, J.P.; Margolis, T.P. Spectrum of eye disease caused by methicillin-resistant Staphylococcus aureus. Am. J. Ophthalmol. 2007, 144, 313–315. [Google Scholar] [CrossRef]
- Solomon, R.; Donnenfeld, E.D.; Perry, H.D.; Rubinfeld, R.S.; Ehrenhaus, M.; Wittpenn, J.R., Jr.; Solomon, K.D.; Manche, E.E.; Moshirfar, M.; Matzkin, D.C. Methicillin-resistant Staphylococcus aureus infectious keratitis following refractive surgery. Am. J. Ophthalmol. 2007, 143, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Asbell, P.A.; Colby, K.A.; Deng, S.; McDonnell, P.; Meisler, D.M.; Raizman, M.B.; Sheppard, J.D., Jr.; Sahm, D.F. Ocular TRUST: Nationwide antimicrobial susceptibility patterns in ocular isolates. Am. J. Ophthalmol. 2008, 145, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Asbell, P.A.; Sahm, D.F.; Shaw, M.; Draghi, D.C.; Brown, N.P. Increasing prevalence of methicillin resistance in serious ocular infections caused by Staphylococcus aureus in the United States: 2000 to 2005. J. Cataract Refract. Surg. 2008, 34, 814–818. [Google Scholar] [CrossRef]
- Vola, M.E.; Moriyama, A.S.; Lisboa, R.; Vola, M.M.; Hirai, F.E.; Bispo, P.J.; Höfling-Lima, A.L. Prevalence and antibiotic susceptibility of methicillin-resistant Staphylococcus aureus in ocular infections. Arq. Bras. Oftalmol. 2013, 76, 350–353. [Google Scholar] [CrossRef] [Green Version]
- Lin, A.; Rhee, M.K.; Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology 2019, 126, 1–55. [Google Scholar] [CrossRef] [Green Version]
- Chang, V.S.; Dhaliwal, D.K.; Raju, L.; Kowalski, R.P. Antibiotic Resistance in the Treatment of Staphylococcus aureus Keratitis: A 20-Year Review. Cornea 2015, 34, 698–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durrani, A.F.; Atta, S.; Bhat, A.K.; Mammen, A.; Dhaliwal, D.; Kowalski, R.P.; Jhanji, V. Methicillin-resistant Staphylococcus aureus keratitis: Initial treatment, risk factors, clinical features, and treatment outcomes. Am. J. Ophthalmol. 2020, 214, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Romanowski, E.G.; Romanowski, J.E.; Shanks, R.M.Q.; Yates, K.A.; Mammen, A.; Dhaliwal, D.K.; Jhanji, V.; Kowalski, R.P. Topical vancomycin 5% is more efficacious than 2.5% and 1.25% for reducing viable methicillin-resistant Staphylococcus aureus in infectious keratitis. Cornea 2020, 39, 250–353. [Google Scholar] [CrossRef]
- Durand, M.L.; Dohlman, C.H. Successful prevention of bacterial endophthalmitis in eyes with the Boston keratoprosthesis. Cornea 2009, 28, 896–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behlau, I.; Martin, K.V.; Martin, J.N.; Naumova, E.N.; Cadorette, J.J.; Sforza, J.T.; Pineda, R., 2nd; Dohlman, C.H. Infectious endophthalmitis in Boston keratoprosthesis: Incidence and prevention. Acta Ophthalmol. 2014, 92, e546–e555. [Google Scholar] [CrossRef]
- Biological tests and assays: Antibiotics, microbial assay. U. S. Pharmacop. 2018, 41, 134–151.
- Austin, A.; Schallhorn, J.; Geske, M.; Mannis, M.; Lietman, T.; Rose-Nussbaumer, J. Empirical treatment of bacterial keratitis: An international survey of corneal specialists. BMJ Open Ophthalmol. 2017, 2, e000047. [Google Scholar] [CrossRef] [Green Version]
- Tena, D.; Rodríguez, N.; Toribio, L.; González-Praetorius, A. Infectious Keratitis: Microbiological Review of 297 Cases. Jpn. J. Infect. Dis. 2019, 72, 121–123. [Google Scholar] [CrossRef] [Green Version]
- Akova Budak, B.; Baykara, M.; Kvanç, S.A.; Yilmaz, H.; Cicek, S. Comparing the ocular surface effects of topical vancomycin and linezolid for treating bacterial keratitis. Cutan. Ocul. Toxicol. 2016, 35, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.; Chodosh, J. Infections after keratoprosthesis. Curr. Opin. Ophthalmol. 2016, 27, 373–377. [Google Scholar] [CrossRef]
- Das Gupta, V.; Stewart, K.R.; Nohria, S. Stability of vancomycin hydrochloride in 5% dextrose and 0.9% sodium chloride injections. Am. J. Hosp. Pharm. 1986, 43, 1729–1731. [Google Scholar] [CrossRef]
- Raverdy, V.; Ampe, E.; Hecq, J.D.; Tulkens, P.M. Stability and compatibility of vancomycin for administration by continuous infusion. J. Antimicrob. Chemother. 2013, 68, 1179–1182. [Google Scholar] [CrossRef]
- Peterlini, M.A.; Barbosa, A.; Pedreira, M. Stability of vancomycin hydrochloride solutions in high concentration and extended time of infusion. Intensive Care Med. Exp. 2015, 3 (Suppl. S1), A717. [Google Scholar] [CrossRef] [Green Version]
- Godet, M.; Simar, J.; Closset, M.; Hecq, J.; Braibant, M.; Soumoy, L.; Gillet, P.; Jamart, J.; Bihin, B.; Galanti, L. Stability of Concentrated Solution of Vancomycin Hydrochloride in Syringes for Intensive Care Units. Pharm. Technol. Hosp. Pharm. 2018, 3, 23–30. [Google Scholar] [CrossRef]
- d’Huart, É.; Vigneron, J.; Charmillon, A.; Clarot, I.; Demoré, B. Physicochemical Stability of Vancomycin at High Concentrations in Polypropylene Syringes. Can. J. Hosp. Pharm. 2019, 72, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Masse, M.; Genay, S.; Martin Mena, A.; Carta, N.; Lannoy, D.; Barthélémy, C.; Décaudin, B.; Odou, P. Evaluation of the stability of vancomycin solutions at concentrations used in clinical services. Eur. J. Hosp. Pharm. 2020, 27, e87–e92. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Solvent | Day 0 | Day 7 | Day 14 | Day 28 |
|---|---|---|---|---|
| PBS—RT | 5.0 ± 0 | 4.5 ± 0 | 4.5 ± 0 | 4.5 ± 0 |
| PBS—4 °C | 5.0 ± 0 | 4.5 ± 0 | 4.5 ± 0 | 4.5 ± 0 |
| BSS—RT | 5.5 ± 0 | 5.5 ± 0 | 5.5 ± 0 | 5.5 ± 0 |
| BSS—4 °C | 5.5 ± 0 | 5.5 ± 0 | 5.5 ± 0 | 5.5 ± 0 |
| Saline—RT | 3.0 ± 0 | 3.0 ± 0 | 3.0 ± 0 | 3.0 ± 0 |
| Saline—4 °C | 3.0 ± 0 | 3.0 ± 0 | 3.0 ± 0 | 3.0 ± 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ross, C.; Syed, B.; Pak, J.; Jhanji, V.; Yamaki, J.; Sharma, A. Stability Evaluation of Extemporaneously Compounded Vancomycin Ophthalmic Drops: Effect of Solvents and Storage Conditions. Pharmaceutics 2021, 13, 289. https://doi.org/10.3390/pharmaceutics13020289
Ross C, Syed B, Pak J, Jhanji V, Yamaki J, Sharma A. Stability Evaluation of Extemporaneously Compounded Vancomycin Ophthalmic Drops: Effect of Solvents and Storage Conditions. Pharmaceutics. 2021; 13(2):289. https://doi.org/10.3390/pharmaceutics13020289
Chicago/Turabian StyleRoss, Christopher, Basir Syed, Joanna Pak, Vishal Jhanji, Jason Yamaki, and Ajay Sharma. 2021. "Stability Evaluation of Extemporaneously Compounded Vancomycin Ophthalmic Drops: Effect of Solvents and Storage Conditions" Pharmaceutics 13, no. 2: 289. https://doi.org/10.3390/pharmaceutics13020289