
Visual Acuity Gain Profiles and Anatomical Prognosis Factors in Patients with Drug-Naive Diabetic Macular Edema Treated with Dexamethasone Implant: The NAVEDEX Study

 , , , , and
, , , , and  add
Show full author list
add
Show full author list
Abstract
:Brief Summary Statement
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Data Collection
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Study Population
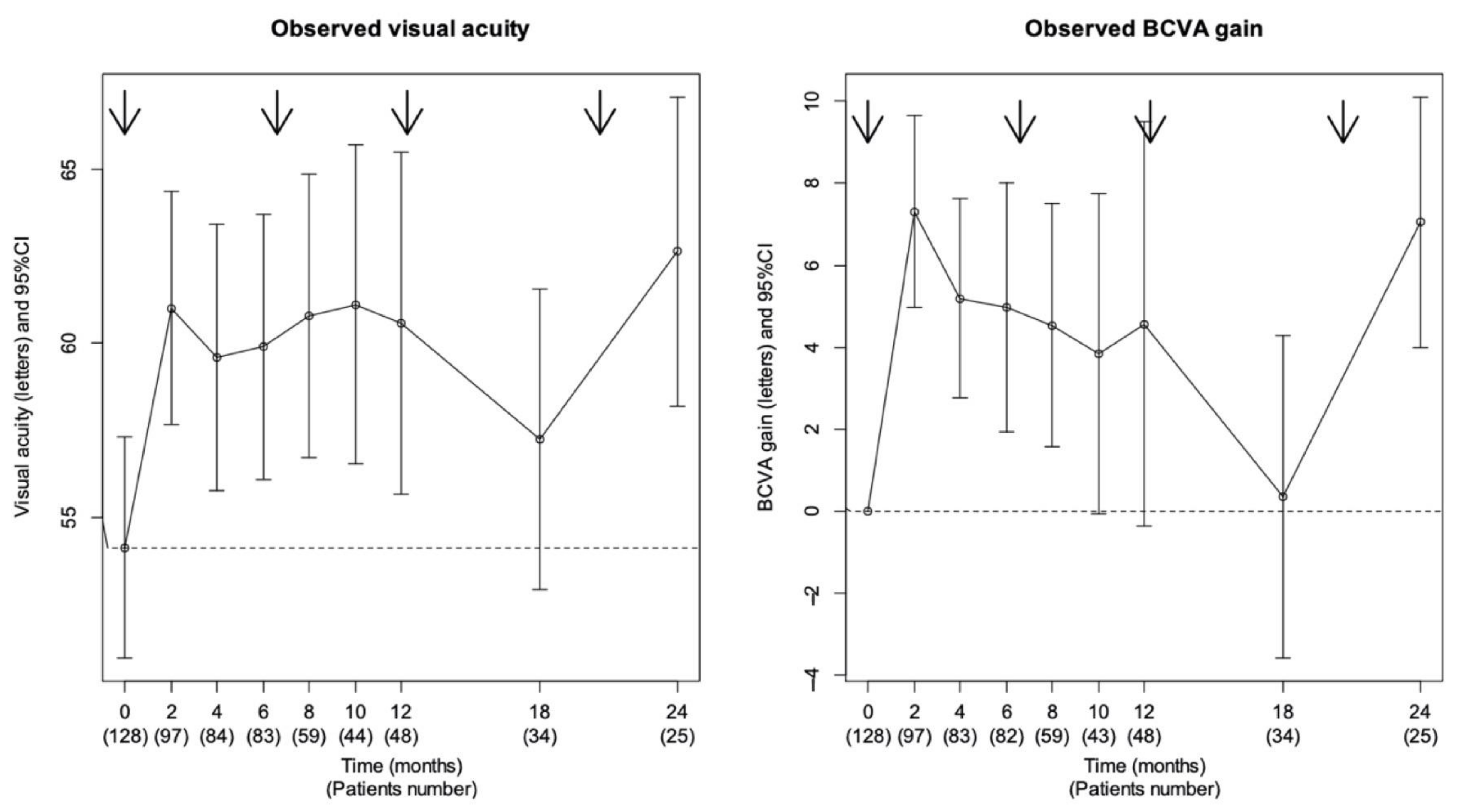
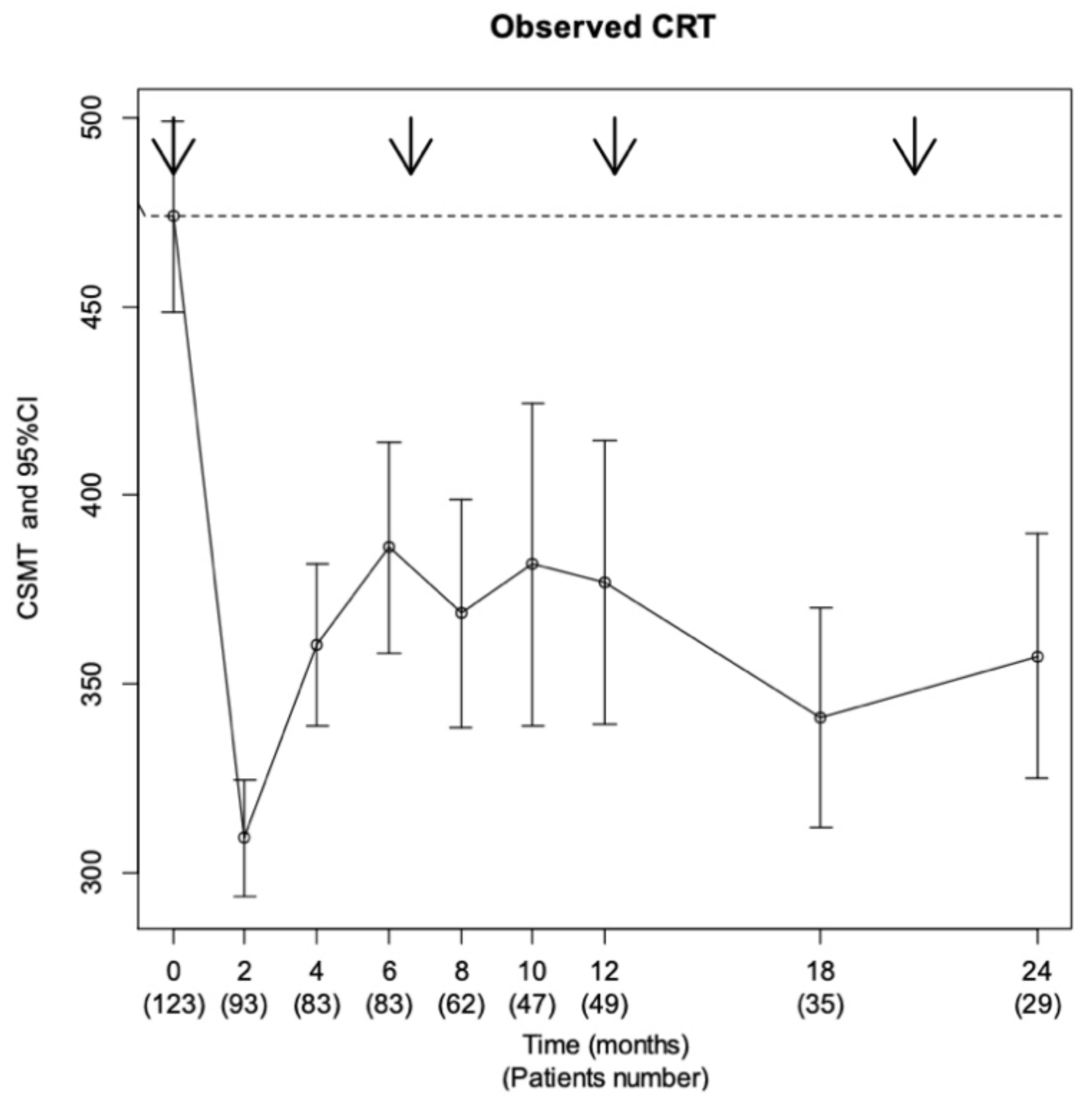
3.2. Overall Functional and Anatomical Efficacy Description
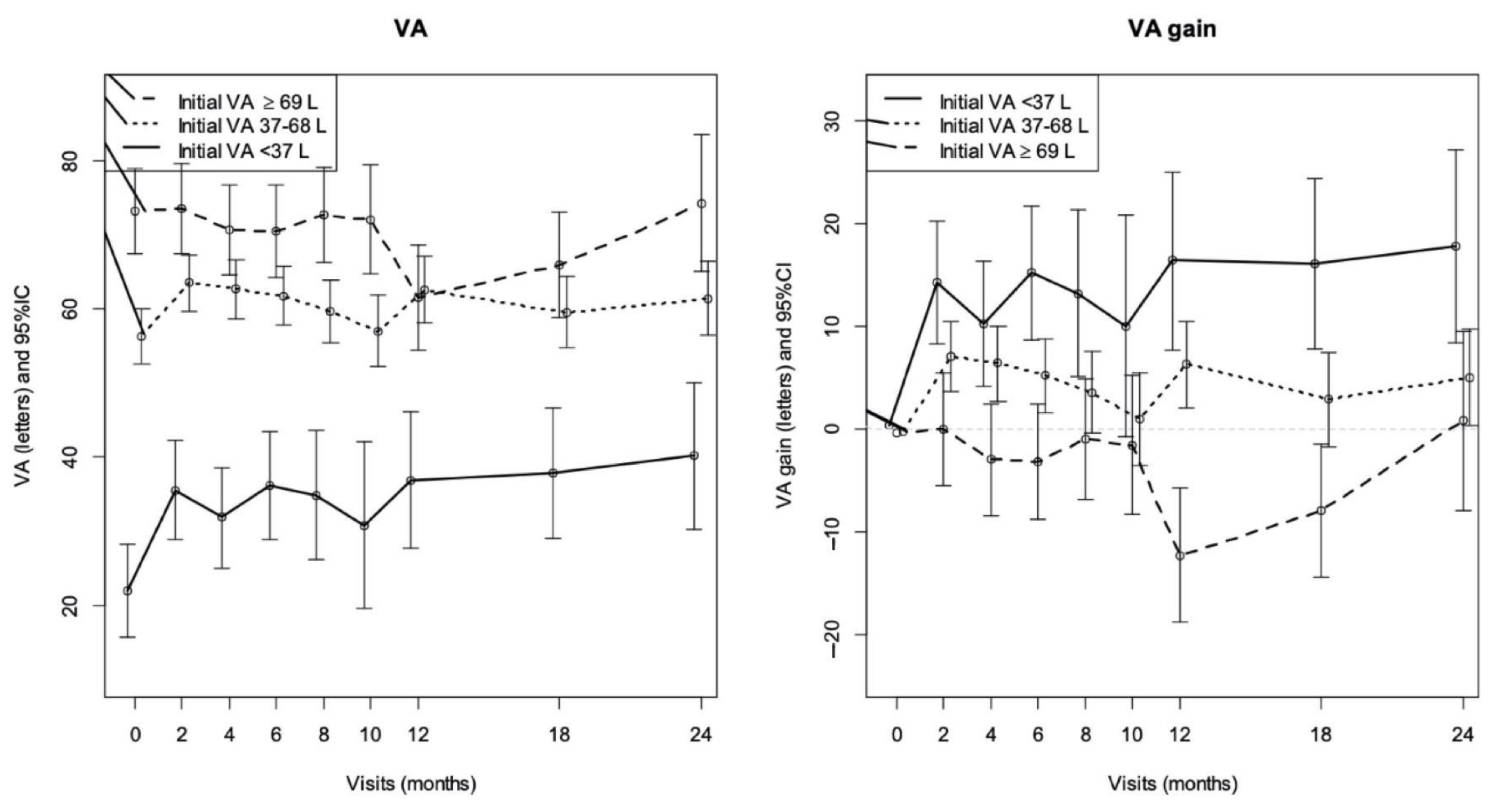
3.3. Analyzes of VA Gain Profiles
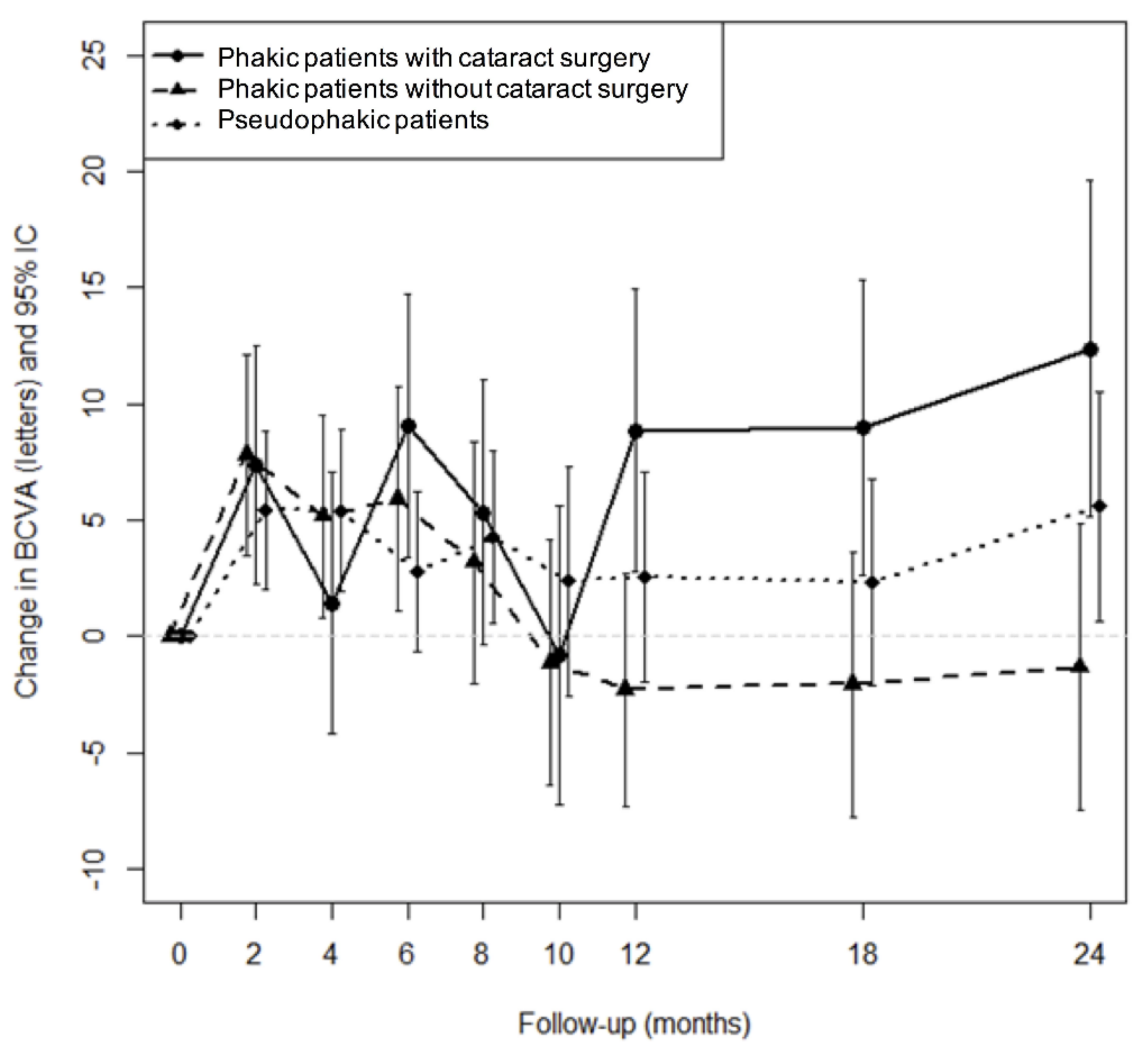
3.4. Anatomical Prognosis Factor for VA Gain
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klein, R.; Klein, B.E.; Moss, S.E.; Davis, M.D.; DeMets, D.L. The Wisconsin Epidemiologic Study of Diabetic Retinopathy. IV. Diabetic Macular Edema. Ophthalmology 1984, 91, 1464–1474. [Google Scholar]
- Miller, K.; Fortun, J.A. Diabetic Macular Edema: Current Understanding, Pharmacologic Treatment Options, and Developing Therapies. Asia-Pac. J. Ophthalmol. Phila. Pa 2018, 7, 28–35. [Google Scholar] [CrossRef]
- Hariprasad, S.M. Current Approaches to the Management of Diabetic Macular Edema. Am. J. Manag. Care 2016, 22, s292–s299. [Google Scholar]
- Tomić, M.; Vrabec, R.; Poljičanin, T.; Ljubić, S.; Duvnjak, L. Diabetic Macular Edema: Traditional and Novel Treatment. Acta Clin. Croat. 2017, 56, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Jansen, M.E.; Hariprasad, S.M.; Singer, M.A. Treatments for Diabetic Macular Edema: Past, Present, and Future. Ophthalmic Surg. Lasers Imaging Retina 2016, 47, 794–800. [Google Scholar] [CrossRef]
- Lim, L.T.; Chia, S.N.; Ah-Kee, E.Y.; Chew, N.; Gupta, M. Advances in the Management of Diabetic Macular Oedema Based on Evidence from the Diabetic Retinopathy Clinical Research Network. Singap. Med. J. 2015, 56, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Kodjikian, L.; Bellocq, D.; Mathis, T. Pharmacological Management of Diabetic Macular Edema in Real-Life Observational Studies. BioMed Res. Int. 2018, 2018, 8289253. [Google Scholar] [CrossRef]
- Pacella, E.; La Torre, G.; Impallara, D.; Malarska, K.; Turchetti, P.; Brillante, C.; Smaldone, G.; De Paolis, G.; Muscella, R.; Pacella, F. Efficacy and Safety of the Intravitreal Treatment of Diabetic Macular Edema with Pegaptanib: A 12-Month Follow-Up. Clin. Ter. 2013, 164, e121–e126. [Google Scholar] [CrossRef]
- Kodjikian, L.; Bellocq, D.; Bandello, F.; Loewenstein, A.; Chakravarthy, U.; Koh, A.; Augustin, A.; de Smet, M.D.; Chhablani, J.; Tufail, A.; et al. First-Line Treatment Algorithm and Guidelines in Center-Involving Diabetic Macular Edema. Eur. J. Ophthalmol. 2019, 1120672119857511. [Google Scholar] [CrossRef]
- Malclès, A.; Dot, C.; Voirin, N.; Vié, A.-L.; Agard, É.; Bellocq, D.; Denis, P.; Kodjikian, L. SAFETY OF INTRAVITREAL DEXAMETHASONE IMPLANT (OZURDEX): The SAFODEX Study. Incidence and Risk Factors of Ocular Hypertension. Retina Phila. Pa 2017, 37, 1352–1359. [Google Scholar] [CrossRef] [Green Version]
- Al-Khersan, H.; Hariprasad, S.M.; Chhablani, J. Dex Implant Study Group Early Response to Intravitreal Dexamethasone Implant Therapy in Diabetic Macular Edema May Predict Visual Outcome. Am. J. Ophthalmol. 2017, 184, 121–128. [Google Scholar] [CrossRef]
- Gonzalez, V.H.; Campbell, J.; Holekamp, N.M.; Kiss, S.; Loewenstein, A.; Augustin, A.J.; Ma, J.; Ho, A.C.; Patel, V.; Whitcup, S.M.; et al. Early and Long-Term Responses to Anti-Vascular Endothelial Growth Factor Therapy in Diabetic Macular Edema: Analysis of Protocol I Data. Am. J. Ophthalmol. 2016, 172, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Vujosevic, S.; Torresin, T.; Bini, S.; Convento, E.; Pilotto, E.; Parrozzani, R.; Midena, E. Imaging Retinal Inflammatory Biomarkers after Intravitreal Steroid and Anti-VEGF Treatment in Diabetic Macular Oedema. Acta Ophthalmol. (Copenh.) 2017, 95, 464–471. [Google Scholar] [CrossRef]
- Laird, N.M.; Ware, J.H. Random-Effects Models for Longitudinal Data. Biometrics 1982, 38, 963–974. [Google Scholar]
- Genolini, C.; Alacoque, X.; Sentenac, M.; Arnaud, C. Kml and Kml3d: R Packages to Cluster Longitudinal Data. J. Stat. Softw. 2015, 65, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Pacella, E.; Loffredo, L.; Malvasi, M.; Trovato Battagliola, E.; Messineo, D.; Pacella, F.; Arrico, L. Effects of Repeated Intravitreal Injections of Dexamethasone Implants on Intraocular Pressure: A 4-Year Study. Clin. Ophthalmol. 2020, 14, 3611–3617. [Google Scholar] [CrossRef]
- Dugel, P.U.; Hillenkamp, J.; Sivaprasad, S.; Vögeler, J.; Mousseau, M.-C.; Wenzel, A.; Margaron, P.; Hashmonay, R.; Massin, P. Baseline Visual Acuity Strongly Predicts Visual Acuity Gain in Patients with Diabetic Macular Edema Following Anti-Vascular Endothelial Growth Factor Treatment across Trials. Clin. Ophthalmol. 2016, 10, 1103–1110. [Google Scholar] [CrossRef] [Green Version]
- Bressler, S.B.; Qin, H.; Beck, R.W.; Chalam, K.V.; Kim, J.E.; Melia, M.; Wells, J.A. Diabetic Retinopathy Clinical Research Network Factors Associated with Changes in Visual Acuity and Central Subfield Thickness at 1 Year after Treatment for Diabetic Macular Edema with Ranibizumab. Arch. Ophthalmol. Chic. Ill 1960 2012, 130, 1153–1161. [Google Scholar] [CrossRef]
- Hwang, H.S.; Chae, J.B.; Kim, J.Y.; Kim, D.Y. Association Between Hyperreflective Dots on Spectral-Domain Optical Coherence Tomography in Macular Edema and Response to Treatment. Invest. Ophthalmol. Vis. Sci. 2017, 58, 5958–5967. [Google Scholar] [CrossRef] [Green Version]
- Gerendas, B.S.; Prager, S.; Deak, G.; Simader, C.; Lammer, J.; Waldstein, S.M.; Guerin, T.; Kundi, M.; Schmidt-Erfurth, U.M. Predictive Imaging Biomarkers Relevant for Functional and Anatomical Outcomes during Ranibizumab Therapy of Diabetic Macular Oedema. Br. J. Ophthalmol. 2018, 102, 195–203. [Google Scholar] [CrossRef]
- Das, R.; Spence, G.; Hogg, R.E.; Stevenson, M.; Chakravarthy, U. Disorganization of Inner Retina and Outer Retinal Morphology in Diabetic Macular Edema. JAMA Ophthalmol. 2018, 136, 202–208. [Google Scholar] [CrossRef]
- Sun, J.K.; Lin, M.M.; Lammer, J.; Prager, S.; Sarangi, R.; Silva, P.S.; Aiello, L.P. Disorganization of the Retinal Inner Layers as a Predictor of Visual Acuity in Eyes with Center-Involved Diabetic Macular Edema. JAMA Ophthalmol. 2014, 132, 1309–1316. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.K.; Radwan, S.H.; Soliman, A.Z.; Lammer, J.; Lin, M.M.; Prager, S.G.; Silva, P.S.; Aiello, L.B.; Aiello, L.P. Neural Retinal Disorganization as a Robust Marker of Visual Acuity in Current and Resolved Diabetic Macular Edema. Diabetes 2015, 64, 2560–2570. [Google Scholar] [CrossRef] [Green Version]
- Guigou, S.; Hajjar, C.; Parrat, E.; Merite, P.Y.; Pommier, S.; Matonti, F.; Prost-Magnin, O.; Meyer, F. Multicenter Ozurdex® assessment for diabetic macular edema: MOZART study. J. Fr. Ophtalmol. 2014, 37, 480–485. [Google Scholar] [CrossRef]
- Nguyen-Khoa, B.-A.; Goehring, E.L.; Werther, W.; Fung, A.E.; Do, D.V.; Apte, R.S.; Jones, J.K. Hospitalized Cardiovascular Events in Patients with Diabetic Macular Edema. BMC Ophthalmol. 2012, 12, 11. [Google Scholar] [CrossRef] [Green Version]
- Bonnin, S.; Dupas, B.; Sanharawi, M.E.; Perol, J.; Erginay, A.; Tadayoni, R.; Massin, P. Efficacy of Dexamethasone Intravitreal Implant for the Treatment of Diabetic Macular Edema. Eur. J. Ophthalmol. 2015, 25, 448–453. [Google Scholar] [CrossRef]
- Querques, G.; Darvizeh, F.; Querques, L.; Capuano, V.; Bandello, F.; Souied, E.H. Assessment of the Real-Life Usage of Intravitreal Dexamethasone Implant in the Treatment of Chronic Diabetic Macular Edema in France. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2016, 32, 383–389. [Google Scholar] [CrossRef]
- Chhablani, J.; Bansal, P.; Veritti, D.; Sambhana, S.; Sarao, V.; Pichi, F.; Carrai, P.; Massaro, D.; Lembo, A.; Mansour, A.M.; et al. Dexamethasone Implant in Diabetic Macular Edema in Real-Life Situations. Eye Lond. Engl. 2016, 30, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Boyer, D.S.; Yoon, Y.H.; Belfort, R.; Bandello, F.; Maturi, R.K.; Augustin, A.J.; Li, X.-Y.; Cui, H.; Hashad, Y.; Whitcup, S.M.; et al. Three-Year, Randomized, Sham-Controlled Trial of Dexamethasone Intravitreal Implant in Patients with Diabetic Macular Edema. Ophthalmology 2014, 121, 1904–1914. [Google Scholar] [CrossRef]
- Pacella, F.; Romano, M.R.; Turchetti, P.; Tarquini, G.; Carnovale, A.; Mollicone, A.; Mastromatteo, A.; Pacella, E. An Eighteen-Month Follow-up Study on the Effects of Intravitreal Dexamethasone Implant in Diabetic Macular Edema Refractory to Anti-VEGF Therapy. Int. J. Ophthalmol. 2016, 9, 1427–1432. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||
|---|---|---|
| Mean Age, Years (Range) | 65.8 Years (34.9–86.1) | |
| Mean follow-up, months (±SD) | 16.5 (±11.4) | |
| Mean BCVA, ETDRS letters (±SD) | 54.0 (±18.1) | |
| Mean subfield central macular thickness (CSMT), μm (±SD) | 476.4 (±142.6) | |
| Mean IOP, mmHg (±SD) | 14.5 (±3.0) | |
| Eye | Right | Left |
| 54 (42%) | 75 (58%) | |
| Sex | F | M |
| 67 (52%) | 62 (48%) | |
| Lens status | Phakic | Pseudophakic |
| 60 (46%) | 69 (54%) | |
| Diabetes | Type 1 | Type 2 |
| 13 (10%) | 116 (90%) | |
| Number of Patients with (%) | ||
| High blood pressure | 94 (73%) | |
| Glaucoma/HIP | 6 (4.5%) | |
| Vitrectomy | 5 (4%) | |
| Panretinal photocoagulation (PRP) | 73 (56%) | |
| Focal laser | 26 (21%) | |
| Subretinal Fluid (SRF) | 15 (12%) | |
| Central Exudates | 14 (11%) | |
| Hyperreflective foci | 44 (34%) | |
| Ellipsoid Zone Alterations (EZA) | 40 (31%) | |
| Disorganization of Retinal Inner Layers (DRIL) | 41 (32%) | |
| DRIL or EZA | 58 (45%) | |
| Observations | Group A | Group B | p-Value |
|---|---|---|---|
| n | 96 | 33 | |
| Age (+/−SD) | 66.1 (+/−10.8) | 64.1 (+/−12.6) | 0.428 |
| Baseline BCVA (+/−SD) | 57.9 (+/−16.7) | 43.4 (+/−19.0) | 0.001 |
| Baseline CSMT (+/−SD) | 455.8 (+/−133.6) | 521.2 (+/−161.2) | 0.055 |
| Sex | 0.835 | ||
| Female | 50 (52.6%) | 16 (48.5%) | |
| Male | 45 (47.4%) | 17 (51.5%) | |
| Lens status | 0.103 | ||
| Phakic | 40 (42.1%) | 20 (60.6%) | |
| Pseudophakic | 55 (57.9%) | 13 (39.4%) | |
| Diabetes | 0.921 | ||
| Type 1 | 9 (9.5%) | 4 (12.1%) | |
| Type 2 | 86 (90.5%) | 29 (87.9%) | |
| HBP | 72 (75.8%) | 21 (63.6%) | 0.262 |
| PRP | 55 (57.9%) | 18 (54.5%) | 0.896 |
| Focal laser | 20 (21.1%) | 6 (18.2%) | 0.919 |
| SRF | 10 (10.5%) | 4 (12.1%) | 1 |
| Central Exudates | 10 (10.5%) | 4 (12.1%) | 1 |
| Hyperreflective foci | 34 (35.8%) | 9 (27.3%) | 0.497 |
| EZAs | 33 (34.7%) | 7 (21.2%) | 0.22 |
| DRILs | 31 (32.6%) | 9 (27.3%) | 0.723 |
| DRILs or EZAs | 46 (48.4%) | 11 (33.3%) | 0.194 |
| Observations at 24 Months | Final VA (L) | VA Gain (L) | ||||
|---|---|---|---|---|---|---|
| Baseline BCVA | <37 L | >69 L | p-value | <37 L | >69 L | p-value |
| 39.8 | 75.1 | <0.001 | 17.3 | 1.5 | 0.02 | |
| Yes | No | p-value | Yes | No | p-value | |
| Pseudophakic | 58.3 | 62.5 | 0.39 | 7.15 | 5.3 | 0.52 |
| Panretinal photocoagulation (PRP) | 56.5 | 61.5 | 0.22 | 3.6 | 7.5 | 0.25 |
| Subretinal Fluid (SRF) | 60.8 | 50.8 | 0.12 | 6.6 | 2.64 | 0.40 |
| Central Exudates | 59.8 | 56.7 | 0.88 | 6.2 | 4.7 | 0.70 |
| Hyperreflective foci | 62.7 | 52.5 | 0.05 | 8.1 | 2.1 | 0.23 |
| Ellipsoid Zone Alterations (EZAs) | 66.6 | 47.5 | <0.001 | 7.5 | 2.9 | 0.22 |
| Disorganization of Retinal Inner Layers (DRILs) | 64.7 | 46.8 | 0.002 | 6.0 | 5.3 | 0.85 |
| DRILs or EZAs | 66.4 | 53.2 | 0.002 | 6.8 | 4.9 | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, M.; Mathis, T.; Massin, P.; Akesbi, J.; Lereuil, T.; Voirin, N.; Matonti, F.; Fajnkuchen, F.; Conrath, J.; Milazzo, S.; et al. Visual Acuity Gain Profiles and Anatomical Prognosis Factors in Patients with Drug-Naive Diabetic Macular Edema Treated with Dexamethasone Implant: The NAVEDEX Study. Pharmaceutics 2021, 13, 194. https://doi.org/10.3390/pharmaceutics13020194
Pinto M, Mathis T, Massin P, Akesbi J, Lereuil T, Voirin N, Matonti F, Fajnkuchen F, Conrath J, Milazzo S, et al. Visual Acuity Gain Profiles and Anatomical Prognosis Factors in Patients with Drug-Naive Diabetic Macular Edema Treated with Dexamethasone Implant: The NAVEDEX Study. Pharmaceutics. 2021; 13(2):194. https://doi.org/10.3390/pharmaceutics13020194
Chicago/Turabian StylePinto, Mauricio, Thibaud Mathis, Pascale Massin, Jad Akesbi, Théo Lereuil, Nicolas Voirin, Frédéric Matonti, Franck Fajnkuchen, John Conrath, Solange Milazzo, and et al. 2021. "Visual Acuity Gain Profiles and Anatomical Prognosis Factors in Patients with Drug-Naive Diabetic Macular Edema Treated with Dexamethasone Implant: The NAVEDEX Study" Pharmaceutics 13, no. 2: 194. https://doi.org/10.3390/pharmaceutics13020194