
Topical Administration of Drugs Incorporated in Carriers Containing Phospholipid Soft Vesicles for the Treatment of Skin Medical Conditions


Abstract
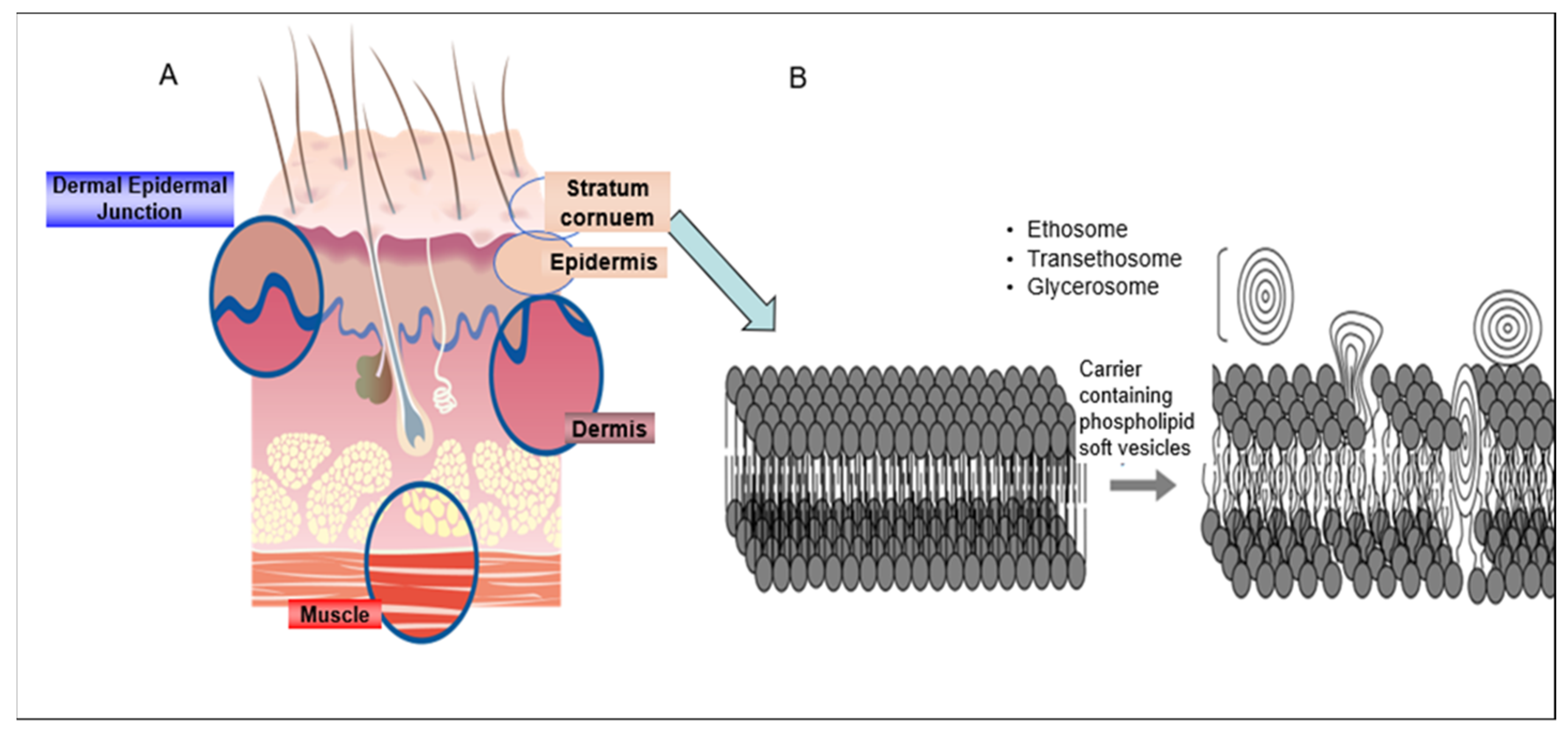
:1. Introduction
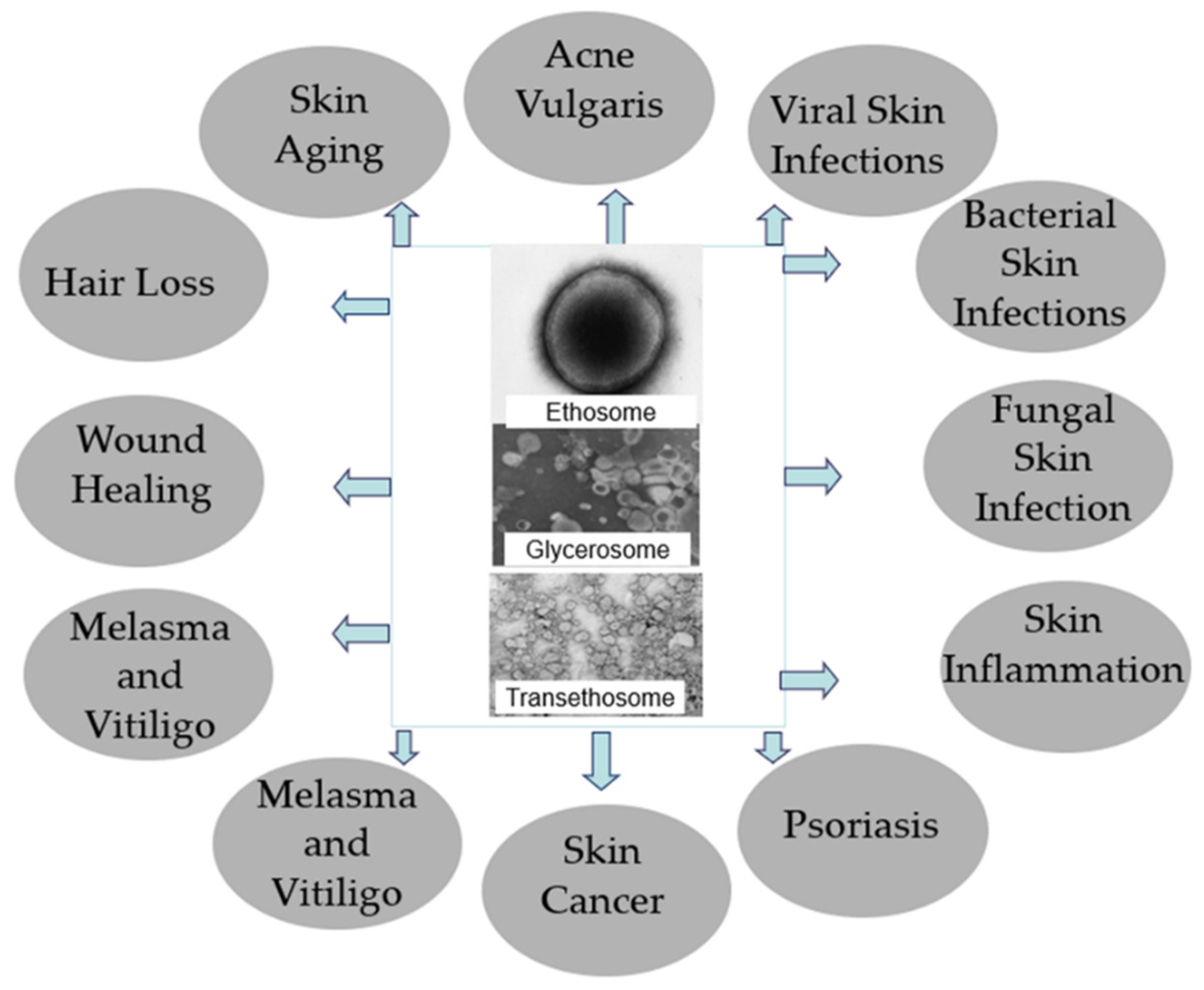
2. Treatment Approaches with Drugs Incorporated in Carriers Containing Phospholipid Soft Vesicles
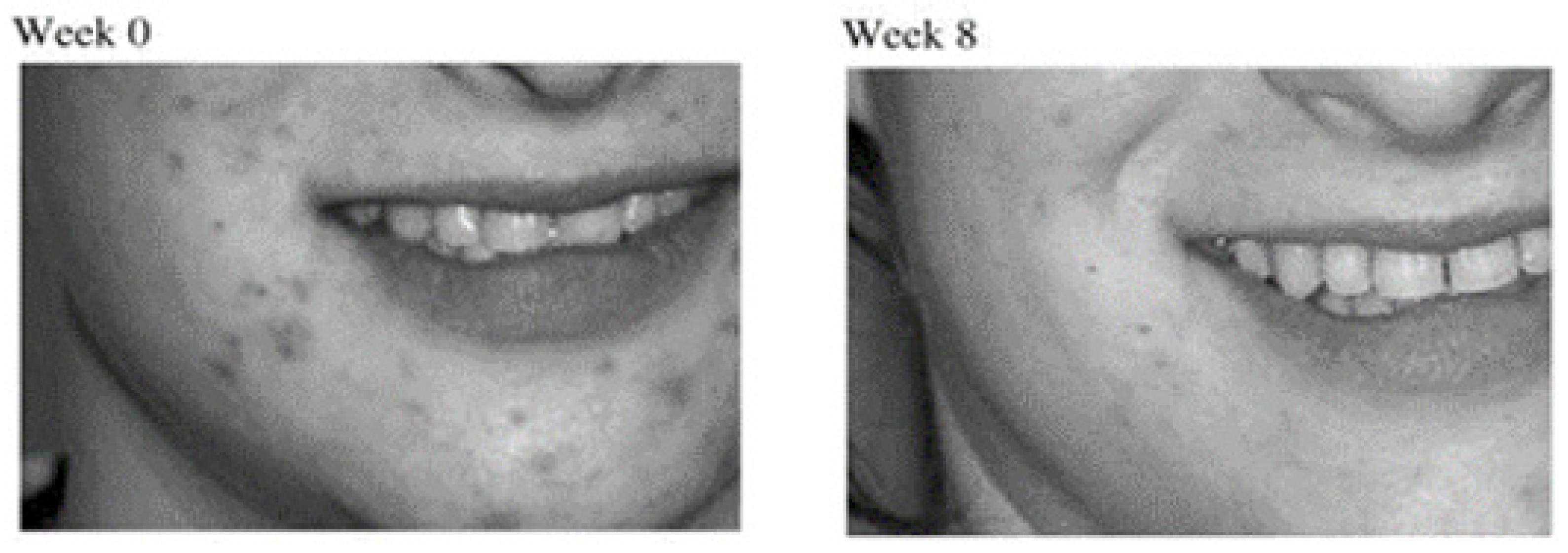
2.1. Treatment of Acne Vulgaris
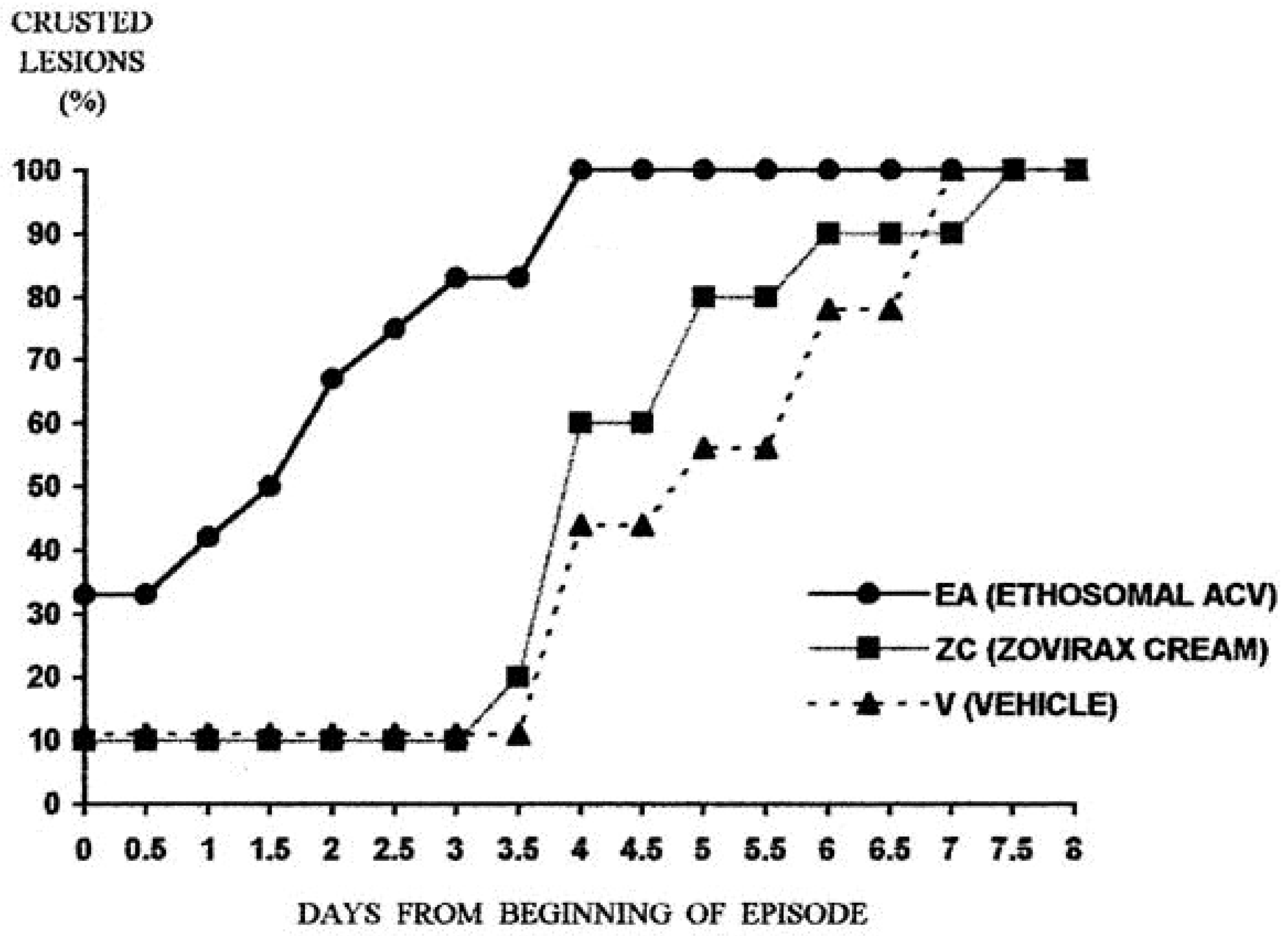
2.2. Treatment of Viral Skin Infections
2.3. Treatment of Bacterial Skin Infections
2.4. Treatment of Fungal Skin Infections
2.5. Treatment of Skin Inflammation
2.6. Treatment of Psoriasis
2.7. Treatment of Skin Cancer
2.8. Treatment of Melasma and Vitiligo
2.9. Wound Healing
2.10. Treatment of Hair Loss
2.11. Treatment of Skin Aging
3. Products Based on Carriers Containing Phospholipid Soft Vesicles
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, M.B.; Martin, G.P.; Jones, S.A.; Akomeah, F.K. Dermal and transdermal drug delivery systems: Current and future prospects. Drug Deliv. 2006, 13, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Brady, R.C.; Bernstein, D.I. Treatment of herpes simplex virus infections. Antivir. Res. 2004, 61, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Wertz, P.W.; van den Bergh, B. The physical, chemical and functional properties of lipids in the skin and other biological barriers. Chem. Phys. Lipids 1998, 91, 85–96. [Google Scholar] [CrossRef]
- Touitou, E.; Barry, B.W. Enhancement in Drug Delivery; CRS Press: Boca Raton, FL, USA; Taylor & Francis Group: London, UK; New York, NY, USA, 2006. [Google Scholar]
- Dragicevic, N.; Maibach, H.I. (Eds.) Percutaneous Penetration Enhancers Chemical Methods in Penetration Enhancement: Nanocarriers; Springer: Berlin/Heidelberg, Germany, 2016; pp. 61–75. [Google Scholar]
- Smith, E.W.; Maibach, H.I. Percutaneous Penetration Enhancers; CRC Press: Boca Raton, FL, USA, 1995. [Google Scholar]
- Smith, E.W.; Maibach, H.I. Penetration Percutaneous Enhancers; Taylor and Francis: London, UK, 2006. [Google Scholar]
- Williams, A.C.; Barry, B.W. Penetration enhancers. Adv. Drug Deliv. Rev. 2004, 56, 603–618. [Google Scholar] [CrossRef]
- Zoabi, A.; Touitou, E.; Margulis, K. Recent Advances in Nanomaterials for Dermal and Transdermal Applications. Colloids Interfaces 2021, 5, 18. [Google Scholar] [CrossRef]
- Touitou, E.; Dayan, N.; Bergelson, L.; Godin, B.; Eliaz, M. Ethosomes- novel vesicular carriers for enhanced delivery: Characterization and skin penetration properties. J. Control. Release 2000, 65, 403–418. [Google Scholar] [CrossRef]
- Touitou, E. Compositions for Applying Active Substances to or through the Skin. U.S. Patent 5,716,638, 10 February 1998. [Google Scholar]
- Song, C.K.; Balakrishnan, P.; Shim, C.K.; Chung, S.J.; Chong, S.; Kim, D.D. A novel vesicular carrier, transethosome, for enhanced skin delivery of voriconazole: Characterization and in vitro/in vivo evaluation. Colloids Surf. B Biointerfaces 2012, 92, 299–304. [Google Scholar] [CrossRef]
- Manca, M.L.; Zaru, M.; Manconi, M.; Lai, F.; Valenti, D.; Sinico, C.; Fadda, A.M. Glycerosomes: A new tool for effective dermal and transdermal drug delivery. Int. J. Pharm. 2013, 455, 66–74. [Google Scholar] [CrossRef]
- Godin, B.; Touitou, E. Mechanism of bacitracin permeation enhancement through the skin and cellular membranes from an ethosomal carrier. J. Control. Release 2004, 94, 365–379. [Google Scholar] [CrossRef]
- Godin, B.; Touitou, E. Erythromycin ethosomal systems: Physicochemical characterization and enhanced antibacterial activity. Curr. Drug Deliv. 2005, 2, 269–275. [Google Scholar] [CrossRef]
- Ainbinder, D.; Touitou, E. A new approach for skin tumor treatment: From delivery system characterization to in vivo evaluation. Drug Deliv. Trans. Res. 2011, 1, 53–65. [Google Scholar] [CrossRef]
- Natsheh, H.; Touitou, E. Phospholipid Vesicles for Dermal/Transdermal and Nasal Administration of Active Molecules: The Effect of Surfactants and Alcohols on the Fluidity of Their Lipid Bilayers and Penetration Enhancement Properties. Molecules 2020, 25, 2959. [Google Scholar] [CrossRef] [PubMed]
- Godin, B.; Touitou, E. Ethosomes: New prospects in transdermal delivery. Crit. Rev. Ther. Drug Carr. Syst. 2003, 20, 63–102. [Google Scholar] [CrossRef]
- Touitou, E.; Godin, B. Ethosomes for skin delivery. J. Drug Deliv. Sci. Technol. 2007, 17, 303–308. [Google Scholar] [CrossRef]
- Lai, F.; Caddeo, C.; Manca, M.L.; Manconi, M.; Sinico, C.; Fadda, A.M. What’s new in the field of phospholipid vesicular nanocarriers for skin drug delivery. Int. J. Pharm. 2020, 583, 119398. [Google Scholar] [CrossRef]
- Das, S.K.; Chakraborty, S.; Roy, C.; Rajabalaya, R.; Mohaimin, A.W.; Khanam, J.; Nanda, A.; David, S.R. Ethosomes as novel vesicular carrier: An overview of the principle, preparation and its applications. Curr. Drug Deliv. 2018, 15, 795–817. [Google Scholar] [CrossRef]
- Esposito, E.; Drechsler, M.; Nastruzzi, C.; Cortesi, R. Cubic phases, cubosomes and ethosomes for cutaneous application. Curr. Pharm. Des. 2016, 22, 5382–5399. [Google Scholar] [CrossRef]
- Esposito, E.; Nastruzzi, C.; Sguizzato, M.; Cortesi, R. Nanomedicines to treat skin pathologies with natural molecules. Curr. Pharm. Des. 2019, 25, 2323–2337. [Google Scholar] [CrossRef]
- Natsheh, H.; Vettorato, E.; Touitou, E. Ethosomes for Dermal Administration of Natural Active Molecules. Curr. Pharm. Des. 2019, 25, 2338–2348. [Google Scholar] [CrossRef] [PubMed]
- Sinico, C.; Fadda, A.M. Vesicular carriers for dermal drug delivery. Expert Opin. Drug Deliv. 2009, 6, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, M.M.; Abdallah, O.Y.; Naggar, V.F.; Khalafallah, N.M. Lipid vesicles for skin delivery of drugs: Reviewing three decades of research. Int. J. Pharm. 2007, 332, 1–16. [Google Scholar] [CrossRef]
- Gollnick, H.P.; Zouboulis, C.C.; Akamatsu, H.; Kurokawa, I.; Schulte, A. Pathogenesis and pathognesis-related treatment of acne. J. Dermatol. 1991, 18, 489–499. [Google Scholar] [CrossRef]
- Leyden, J.J. New understanding of the pathogenesis of acne. J. Am. Acad. Dermatol. 1995, 32, 515–525. [Google Scholar] [CrossRef]
- Gollnick, H.P.; Krautheim, A. Topical treatment in acne: Current status and future aspects. Dermatology 2003, 206, 29–36. [Google Scholar] [CrossRef]
- Strauss, J.S.; Krowchuk, D.P.; Leyden, J.J.; Lucky, A.W.; Shalita, A.R.; Siegfried, E.C.; Thiboutot, D.M.; Van Voorhees, A.S.; Beutner, K.A.; Sieck, C.K.; et al. American Academy of Dermatology/American Academy of Dermatology Association. Guidelines of care for acne vulgaris management. J. Am. Acad. Dermatol. 2007, 56, 651–663. [Google Scholar] [CrossRef]
- Touitou, E.; Godin, B.; Shumilov, M.; Bishouty, N.; Ainbinder, D.; Shouval, R.; Ingber, A.; Leibovici, V. Efficacy and tolerability of clindamycin phosphate and salicylic acid gel in the treatment of mild to moderate acne vulgaris. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 629–631. [Google Scholar] [CrossRef]
- Esposito, E.; Menegatti, E.; Cortesi, R. Ethosomes and liposomes as topical vehicles for azelaic acid: A preformulation study. Int. J. Cosmet. Sci. 2004, 55, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Lv, H.; Han, G.; Ma, K. Ethosomes loaded with cryptotanshinone for acne treatment through topical gel formulation. PLoS ONE 2016, 11, e0159967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, S.A.; Qadir, A.; Warsi, M.H.; Mujeeb, M.; Aqil, M.; Mir, S.R.; Sharma, S. Ethosomes-based gel formulation of karanjin for treatment of acne vulgaris: In vitro investigations and preclinical assessment. 3 Biotech 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Horwitz, E.; Pisanty, S.; Czerninski, R.; Helser, M.; Eliav, E.; Touitou, E. A clinical evaluation of a novel liposomal carrier for acyclovir in the topical treatment of recurrent herpes labialis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 87, 700–705. [Google Scholar] [CrossRef]
- Cortesi, R.; Ravani, L.A.; Zaid, A.N.A.; Menegatti, E.A.; Romagnoli, R.A.; Drechsler, M.A.; Esposito, E.A. Ethosomes for the delivery of anti-HSV-1 molecules: Preparation, characterization and in vitro activity. Pharmazie 2010, 65, 743–749. [Google Scholar]
- Cortesi, R.; Ravani, L.; Menegatti, E.; Drechsler, M.; Esposito, E. Colloidal dispersions for the delivery of acyclovir: A comparative study. Indian J. Pharm. Sci. 2011, 73, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Vanti, G.; Ntallis, S.G.; Panagiotidis, C.A.; Dourdouni, V.; Patsoura, C.; Bergonzi, M.C.; Lazari, D.; Bilia, A.R. Glycerosome of Melissa officinalis L. Essential Oil for Effective Anti-HSV Type 1. Molecules 2020, 25, 3111. [Google Scholar] [CrossRef]
- Bagchi, D.; Dutta, S.; Singh, P.; Chaudhuri, S.; Pal, S.K. Essential dynamics of an effective phototherapeutic drug in a nanoscopic delivery vehicle: Psoralen in ethosomes for biofilm treatment. ACS Omega 2017, 2, 1850–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marto, J.; Vitor, C.; Guerreiro, A.; Severino, C.; Eleutério, C.; Ascenso, A.; Simões, S. Ethosomes for enhanced skin delivery of griseofulvin. Colloids Surf. B Biointerfaces 2016, 146, 616–623. [Google Scholar] [CrossRef]
- Shetty, S.; Jose, J.; Kumar, L.; Charyulu, R.N. Novel ethosomal gel of clove oil for the treatment of cutaneous candidiasis. J. Cosmet. Dermatol. 2018, 18, 862–869. [Google Scholar] [CrossRef]
- Faisal, W.; Soliman, G.M.; Hamdan, A.M. Enhanced skin deposition and delivery of voriconazole using ethosomal preparations. J. Liposome Res. 2018, 28, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Utreja, P. Transethosomes of Econazole Nitrate for Transdermal Delivery: Development, In-vitro Characterization, and Ex-vivo Assessment. Pharm. Nanotechnol. 2018, 6, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Patel, N.; Madan, P.; Lin, S. Formulation and rheological evaluation of ethosome-loaded carbopol hydrogel for transdermal application. Drug Dev. Ind. Pharm. 2016, 42, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Paolino, D.; Lucania, G.; Mardente, D.; Alhaique, F.; Fresta, M. Ethosomes for skin delivery of ammonium glycyrrhizinate: In vitro percutaneous permeation through human skin and in vivo anti inflammatory activity on human volunteers. J. Control. Release 2005, 106, 99–110. [Google Scholar] [CrossRef]
- Zhaowu, Z.; Xiaoli, W.; Yangde, Z.; Nianfeng, L. Preparation of matrine ethosome, its percutaneous permeation in vitro and anti- inflammatory activity in vivo in rats. J. Liposome Res. 2009, 19, 155–162. [Google Scholar] [CrossRef]
- Shen, L.N.; Zhang, Y.T.; Wang, Q.; Xu, L.; Feng, N.P. Enhanced in vitro and in vivo skin deposition of apigenin delivered using ethosomes. Int. J. Pharm. 2014, 460, 280–288. [Google Scholar] [CrossRef]
- Esposito, E.; Drechsler, M.; Huang, N.; Pavoni, G.; Cortesi, R.; Santonocito, D.; Puglia, C. Ethosomes and organogels for cutaneous administration of crocin. Biomed. Microdevices 2016, 18, 108. [Google Scholar] [CrossRef] [Green Version]
- Ghanbarzadeh, S.; Arami, S. Enhanced transdermal delivery of diclofenac sodium via conventional liposomes, ethosomes, and transfersomes. BioMed Res. Int. 2013, 2013, 616810. [Google Scholar] [CrossRef]
- Manca, M.L.; Cencetti, C.; Matricardi, P.; Castangia, I.; Zaru, M.; Sales, O.D.; Nacher, A.; Valenti, D.; Maccioni, A.M.; Fadda, A.M.; et al. Glycerosomes: Use of hydrogenated soy phosphatidylcholine mixture and its effect on vesicle features and diclofenac skin penetration. Int. J. Pharm. 2016, 511, 198–204. [Google Scholar] [CrossRef]
- Manca, M.L.; Manconi, M.; Zaru, M.; Valenti, D.; Peris, J.E.; Matricardi, P.; Maccioni, A.M.; Fadda, A.M. Glycerosomes: Investigation of role of 1, 2-dimyristoyl-sn-glycero-3-phosphatidycholine (DMPC) on the assembling and skin delivery performances. Int. J. Pharm. 2017, 532, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, Y.; Li, Z.; Li, N.; Feng, N. Essential oil-mediated glycerosomes increase transdermal paeoniflorin delivery: Optimization, characterization, and evaluation in vitro and in vivo. Int. J. Nanomed. 2017, 12, 3521–3532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andleeb, M.; Shoaib Khan, H.M.; Daniyal, M. Development, Characterization and Stability Evaluation of Topical Gel Loaded with Ethosomes Containing Achillea millefolium L. Extract. Front. Pharmacol. 2021, 12, 336. [Google Scholar] [CrossRef]
- Zhang, Y.T.; Shen, L.N.; Wu, Z.H.; Zhao, J.H.; Feng, N.P. Comparison of ethosomes and liposomes for skin delivery of psoralen for psoriasis therapy. Int. J. Pharm. 2014, 471, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Aggarwal, G.; Manchanda, S.; Narula, A. Development of topical gel of methotrexate incorporated ethosomes and salicylic acid for the treatment of psoriasis. Pharm. Nanotechnol. 2019, 7, 362–374. [Google Scholar] [CrossRef]
- Fathalla, D.; Youssef, E.M.K.; Soliman, G.M. Liposomal and Ethosomal Gels for the Topical Delivery of Anthralin: Preparation, Comparative Evaluation and Clinical Assessment in Psoriatic Patients. Pharmaceutics 2020, 12, 446. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Lu, J.; Fan, Y.; Zhang, Y.; Yin, S.; Sha, X.; Feng, N. TPGS assists the percutaneous administration of curcumin and glycyrrhetinic acid coloaded functionalized ethosomes for the synergistic treatment of psoriasis. Int. J. Pharm. 2021, 604, 120762. [Google Scholar] [CrossRef]
- Paolino, D.; Celia, C.; Trapasso, E.; Cilurzo, F.; Fresta, M. Paclitaxel-loaded ethosomes®: Potential treatment of squamous cell carcinoma, a malignant transformation of actinic keratoses. Eur. J. Pharm. Biopharm. 2012, 81, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Rady, M.; Gomaa, I.; Afifi, N.; Abdel-Kader, M. Dermal delivery of Fe-chlorophyllin via ultradeformable nanovesicles for photodynamic therapy in melanoma animal model. Int. J. Pharm. 2018, 548, 480–490. [Google Scholar] [CrossRef]
- Md, S.; Alhakamy, N.A.; Aldawsari, H.M.; Husain, M.; Khan, N.; Alfaleh, M.A.; Asfour, H.Z.; Riadi, Y.; Bilgrami, A.L.; Akhter, M.H. Plumbagin-Loaded Glycerosome Gel as Topical Delivery System for Skin Cancer Therapy. Polymers 2021, 13, 923. [Google Scholar] [CrossRef]
- Partoazar, A.; Kianvash, N.; Darvishi, M.H.; Nasoohi, S.; Rezayat, S.M.; Bahador, A. Ethosomal curcumin promoted wound healing and reduced bacterial flora in second degree burn in rat. Drug Res. 2016, 66, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Kianvash, N.; Bahador, A.; Pourhajibagher, M.; Ghafari, H.; Nikoui, V.; Rezayat, S.M.; Dehpour, A.R.; Partoazar, A. Evaluation of propylene glycol nanoliposomes containing curcumin on burn wound model in rat: Biocompatibility, wound healing, and anti-bacterial effects. Drug Deliv. Transl. Res. 2017, 7, 654–663. [Google Scholar] [CrossRef]
- Fu, X.; Shi, Y.; Wang, H.; Zhao, X.; Sun, Q.; Huang, Y.; Qi, T.; Lin, G. Ethosomal Gel for Improving Transdermal Delivery of Thymosin β-4. Int. J. Nanomed. 2019, 14, 9275–9284. [Google Scholar] [CrossRef] [Green Version]
- Celia, C.; Cilurzo, F.; Trapasso, E.; Cosco, D.; Fresta, M.; Paolino, D. Ethosomes® and transfersomes® containing linoleic acid: Physicochemical and technological features of topical drug delivery carriers for the potential treatment of melasma disorders. Biomed. Microdevices 2012, 14, 119–130. [Google Scholar] [CrossRef]
- Garg, B.J.; Garg, N.K.; Beg, S.; Singh, B.; Katare, O.P. Nanosized ethosomes-based hydrogel formulations of methoxsalen for enhanced topical delivery against vitiligo: Formulation optimization, in vitro evaluation and preclinical assessment. J. Drug Target 2016, 24, 233–246. [Google Scholar] [CrossRef]
- Meidan, V.M.; Touitou, E. Treatments for Androgenetic Alopecia and Alopecia Areata. Drugs 2001, 61, 53–69. [Google Scholar] [CrossRef]
- Rani, D.; Sharma, V.; Manchanda, R.; Chaurasia, H. Formulation, Design and Optimization of Glycerosomes for Topical Delivery of Minoxidil. Res. J. Pharmacol. Technol. 2021, 14, 2367–2374. [Google Scholar] [CrossRef]
- Madhunithya, E.; Venkatesh, G.; Shyamala, G.; Manjari, V.; Ramesh, S.; Karuppaiah, A.; Sankar, V. Development of ethosome comprising combined herbal extracts and its effect on hair growth. Adv. Tradit. Med. 2021, 21, 131–141. [Google Scholar] [CrossRef]
- Touitou, E.; Godin, B. Skin nonpenetrating sunscreens for cosmetic and pharmaceutical formulations. Clin. Dermatol. 2008, 26, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Jeswani, G.; Saraf, S. Topical Delivery of Curcuma longa extract loaded nanosized ethosomes to combat facial wrinkles. J. Pharm. Drug Deliv. Res. 2014, 3, 1–8. [Google Scholar]
- Yücel, Ç.; Şeker Karatoprak, G.; Değim, İ.T. Anti-aging formulation of rosmarinic acid-loaded ethosomes and liposomes. J. Microencapsul. 2019, 36, 180–191. [Google Scholar] [CrossRef]
- Ramdass, P.; Mullick, S.; Farber, H.F. Viral skin diseases. Prim. Care Clin. Off. 2015, 42, 517–567. [Google Scholar] [CrossRef]
- Spruance, S.L.; Crumpacker, C.S. Topical 5% acyclovir in polyethylene-glycol for herpes simplex labialis: Antiviral effect without clinical benefit. Am. J. Med. 1982, 73, 315–319. [Google Scholar] [CrossRef]
- Raborn, G.W.; McGaw, W.T.; Grace, M.; Houle, L. Herpes labialis treatment with acyclovir 5% ointment. J. Can. Dent. Assoc. 1989, 55, 135–137. [Google Scholar]
- Fiddian, A.P.; Ivanyi, L. Topical acyclovir in the management of herpes labialis. Br. J. Dermatol. 1983, 109, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Raborn, G.W.; McGaw, W.T.; Grace, M.; Percy, J.; Samuels, S. Herpes labialis treatment with acyclovir 5% modified aqueous cream: A double blind randomized trial. Oral Surg. Oral Med. Oral Pathol. 1989, 67, 676–679. [Google Scholar] [CrossRef]
- Touitou, E.; Godin, B.; Dayan, N.; Weiss, C.; Piliponsky, A.; Levi-Schaffer, F. Intracellular delivery mediated by an ethosomal carrier. Biomaterials 2001, 22, 3053–3059. [Google Scholar] [CrossRef]
- Naimi, T.S.; LeDell, K.H.; Como-Sabetti, K. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 2003, 290, 2976–2984. [Google Scholar] [CrossRef] [Green Version]
- Fung, H.B.; Chang, J.Y.; Kuczynski, S. A practical guide to the treatment of complicated skin and soft tissue infections. Drugs 2003, 63, 1459–1480. [Google Scholar] [CrossRef] [PubMed]
- O’Dell, M.L. Skin and wound infections: An overview. Am. Fam. Physician 1998, 57, 2424–2432. [Google Scholar]
- Nichols, R.L. Optimal treatment of complicated skin and skin structure infections. J. Antimicrob. Chemother. 1999, 44, 19–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, M.L.; Chambers, C.J.; Sharon, V.R.; Thompson, G.R., III. Fungal infections of the skin and nail: New treatment options. Expert Rev. Anti Infect. Ther. 2014, 12, 1389–1405. [Google Scholar] [CrossRef]
- Zhang, L.; Li, X.; Zhu, S.; Zhang, T.; Maimaiti, A.; Ding, M.; Shi, S. Dermal Targeting Delivery of Terbinafine Hydrochloride Using Novel Multi-Ethosomes: A New Approach to Fungal Infection Treatment. Coatings 2020, 10, 304. [Google Scholar] [CrossRef] [Green Version]
- Ferrero-Miliani, L.; Nielsen, O.H.; Andersen, P.S.; Girardin, S.E. Chronic inflammation: Importance of NOD2 and NALP3 in interleukin-1beta generation. Clin. Exp. Immunol. 2007, 147, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, B.E.; Leung, D.Y. Pathophysiology of atopic dermatitis: Clinical implications. Allergy Asthma Proc. 2019, 40, 84. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Tom, W.L.; Berger, T.G.; Krol, A.; Paller, A.S.; Schwarzenberger, K.; Bergman, J.N.; Chamlin, S.L.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 2. Management and treatment of atopic dermatitis with topical therapies. J. Am. Acad. Dermatol. 2014, 71, 116–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.G.; Liu, Y.F.; Gao, T.W. Preparation and anti-inflammatory activity of triptolide ethosomes in an erythema model. J. Liposome Res. 2010, 20, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Gudjonsson, J.E.; Elder, J.T. Psoriasis: Epidemiology. Clin. Dermatol. 2007, 25, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Linares, M.A.; Zakaria, A.; Nizran, P. Skin cancer. Prim. Care 2015, 42, 645–659. [Google Scholar] [CrossRef]
- Diepgen, T.L.; Mahler, V. The epidemiology of skin cancer. Br. J. Dermatol. 2002, 146, 1–6. [Google Scholar] [CrossRef]
- Jerant, A.F.; Johnson, J.T.; Sheridan, C.D.; Caffrey, T.J. Early detection and treatment of skin cancer. Am. Fam. Physician 2000, 62, 357–368. [Google Scholar]
- Rendon, M.; Berneburg, M.; Arellano, I.; Picardo, M. Treatment of melasma. Am. Acad. Dermatol. 2006, 54, S272–S281. [Google Scholar] [CrossRef]
- Taïeb, A.; Picardo, M. Vitiligo. N. Engl. J. Med. 2009, 360, 160–169. [Google Scholar] [CrossRef]
- Sorg, H.; Tilkorn, D.J.; Hager, S.; Hauser, J.; Mirastschijski, U. Skin wound healing: An update on the current knowledge and concepts. Eur. Surg. Res. 2017, 58, 81–94. [Google Scholar] [CrossRef]
- Price, V.H. Treatment of hair loss. N. Engl. J. Med. 1999, 341, 964–973. [Google Scholar] [CrossRef]
- Ainbinder, D.; Touitou, E. Skin photodamage prevention: State of the art and new prospects. In Textbook of Aging Skin; Farage, M.A., Miller, K.W., Maibach, H.I., Eds.; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Sguizzato, M.; Mariani, P.; Spinozzi, F.; Benedusi, M.; Cervellati, F.; Cortesi, R.; Drechsler, M.; Prieux, R.; Valacchi, G.; Esposito, E. Ethosomes for Coenzyme Q10 Cutaneous Administration: From Design to 3D Skin Tissue Evaluation. Antioxidants 2020, 9, 485. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treated Disorder | Investigated Vesicular Carrier | Study | Ref. |
|---|---|---|---|
| Acne Vulgaris | Clindamycin and salicylic acid ethosomal system | Clinical study on the reduction of acne vulgaris and skin tolerability of the formulation | [31] |
| Azelaic acid ethosomal system | Diffusion study through synthetic membrane | [32] | |
| Cryptotanshinone ethosomal system | In vitro skin permeation and skin deposition; in vivo anti-acne activity on rabbits | [33] | |
| Karanjin ethosomal system | In vitro skin premeation study on excised rats skin; in vivo skin irritation study on rats; in vivo anti-inflammatory and anti- acne studies on rats | [34] | |
| Viral infections | Acyclovir ethosomal system | Two-armed double-blind clinical study on subjects with recurrent herpes labialis | [35] |
| Acyclovir ethosomal system | Antiviral activity against HSV-1 by plaque reduction assay in monolayer cultures of Vero cells | [36,37] | |
| 9-[(2-hydroxyethoxy) methyl]guanine ethosomal system | Antiviral activity against HSV-1 by plaque reduction assay in monolayer cultures of Vero cells | [37] | |
| Ethosomal system of the essential oil of Melissa officinalis L. | In vitro activity against HSV type 1 in mammalian cells | [38] | |
| Bacterial infections | Bacitracin ethosomal system | Intracellular penetration and localization in fibroblasts (3T3); in vitro deposition and permeation through human cadaver skin | [14] |
| Erythromycin ethosomal system | In vivo activity in mice model of deep dermal S. aureus infection | [15] | |
| Psoralen ethosomal system | Photodynamic therapy in biofilms formed in Petri dishes | [39] | |
| Fungal infections | Voriconazole transethosomal system | In vitro skin permeation and deposition studies through mice skin; in vivo deposition study on mice | [12] |
| Griseofulvin ethosomal system | In vitro permeation and deposition study on new-born pig skin | [40] | |
| Clove oil ethosomal system | Ex vivo permeation studies on rat skin; antifungal activity in cup plate test against Candida albicans | [41] | |
| Voriconazole ethosomal system | In vitro anti-fungal activity against Asperigillus flavus colonies. In vitro skin deposition and permeation through abdominal rat skin | [42] | |
| Econazole nitrate transethosomal system | Ex-vivo skin permeation and retention studies followed by in vitro antifungal activity against C. albicans fungus | [43] | |
| Skin inflammation | Diclofenac ethosomal system | In vitro permeation study on rat skin; in vivo anti-inflammatory activity in carrageenan-induced rat paw edema model | [11,44] |
| Ammonium glycyrrhizinate ethosomal system | In vitro permeation through human skin; clinical study to evaluate the anti-inflammatory activity in volunteers with methyl nicotinate erythema | [45] | |
| Matrine ethosomal system | In vitro percutaneous permeation study on rat skin; in vivo anti-inflammatory activity in rat measured by reflection spectrophotometery | [46] | |
| Apigenin ethosomal system | In vitro and in vivo deposition study on rat skin; evaluation of the reduction of cyclooxygenase-2 levels in mouse with skin inflammation | [47] | |
| Crocin ethosomal system | Evaluation of the anti-inflammatory activity on healthy volunteers. | [48] | |
| Diclofenac ethosomal system and Diclofenac transethosomal system | In vitro permeation and deposition studies on rat skin | [49] | |
| Diclofenac glycerosoomal system | In vitro penetration and permeation studies on new-born pig skin | [13,50,51] | |
| Paeoniflorin glycerosomal system | In vitro permeation experiments through excised rat abdominal skin; in vivo deposition in rat synovium | [52] | |
| Achillea millefolium L. extract ethosomal system | In vitro permeation strudy through fresh rat skin | [53] | |
| Psoriasis | Psoralen ethosomal system | In vitro permeation and penetration study using Franz diffusion cells and excised rat skin | [54] |
| Methotrexate and Salicylic acid ethosomal system | In vitro retention and permeation study on pig ear skin; in vivo anti-psoriatic activity in mice model with imiquimod-induced psoriasis | [55] | |
| Anthralin ethosomal system | Preparation, comparative evaluation and clinical assessment in psoriatic patients | [56] | |
| Curcumin ethosomal system surface-modified with glycyrrhetinic acid-D-α-tocopherol acid polyethylene glycol succinate | In vitro anti-inflmmatory effect on interleukin-6-induced oxidative stress cell model; in vivo anti-psoriatic activity in mice model with imiquimod-induced psoriasis | [57] | |
| Skin cancer | 5- Fluorouracil ethosomal system containing -decyl methyl sulfoxide (Tumorep) | In vitro anti-tumor effect on five cell lines; in vivo anti-tumor effect in mice model of skin cancer | [16] |
| Paclitaxel ethosomal system | In vitro permeation study on human SC; in vitro antiproliferative effect in squamous carcinoma cells | [58] | |
| Fe-chlorophyllin transethosomal system | In vitro skin permeation and deposition studies through mice skin; in vivo evaluation of the anti-cancer effect in mice | [59] | |
| Plumbagin glycerosomal system | Ex vivo permeation study on rats skin | [60] | |
| Skin injury (wound healing) | Curcumin ethosomal system | In vivo wound healing effect in rats | [61] |
| Curcumin-propylene glycol liposomal system | In vivo wound repair effect is rats with burned skin | [62] | |
| Thymosinβ-4(Tβ-4) ethosomal system | In vitro drug release study on mice skin; in vivo pharmacokinetic and skin irritation studies on mice | [63] | |
| Skin pigmentation disorders | Linoleic acid ethosomal system | In vitro percutaneous permeation through human stratum corneum and viable epidermis membrane | [64] |
| Methoxsalen ethosomal system | Ex vivo release studies and photo- toxicity after exposure to UV light | [65] | |
| Hair loss | Minoxidil ethosomal system Minoxidil glycerosomal system | In vitro penetration and permeation through abdominal nude mice skin | [10,66,67] |
| Ethosomal systems of plant extracts | In vivo effect on hair growth in rats with testosterone induced alopecia | [68] | |
| Skin aging | Vitamin E ethosomal system | In vitro permeation studies through skin and cultured fibroblasts | [69] |
| Curcumin ethosomal system | Clinical trial evaluating skin viscoelasticity, total deformation, biological elasticity and sagginess | [70] | |
| Rosmarinic acid ethosomal system | Ex vivo permeation studies using Franz diffusion cells and mice skin; ex vivo antioxidant activity | [71] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Touitou, E.; Natsheh, H. Topical Administration of Drugs Incorporated in Carriers Containing Phospholipid Soft Vesicles for the Treatment of Skin Medical Conditions. Pharmaceutics 2021, 13, 2129. https://doi.org/10.3390/pharmaceutics13122129
Touitou E, Natsheh H. Topical Administration of Drugs Incorporated in Carriers Containing Phospholipid Soft Vesicles for the Treatment of Skin Medical Conditions. Pharmaceutics. 2021; 13(12):2129. https://doi.org/10.3390/pharmaceutics13122129
Chicago/Turabian StyleTouitou, Elka, and Hiba Natsheh. 2021. "Topical Administration of Drugs Incorporated in Carriers Containing Phospholipid Soft Vesicles for the Treatment of Skin Medical Conditions" Pharmaceutics 13, no. 12: 2129. https://doi.org/10.3390/pharmaceutics13122129