
Recent Advances in Photodynamic Therapy against Fungal Keratitis

 , , ,
, , ,
Abstract
:1. Introduction
2. Fungal Keratitis
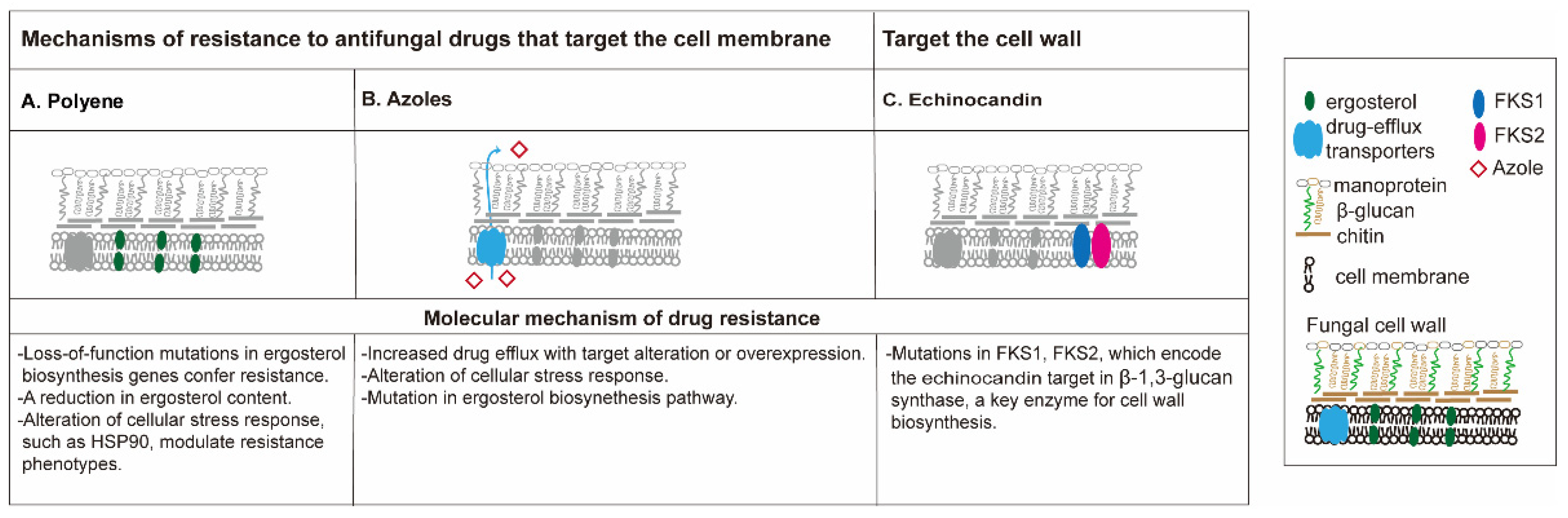
3. Drug Resistance and Biofilm in Fungal Keratitis
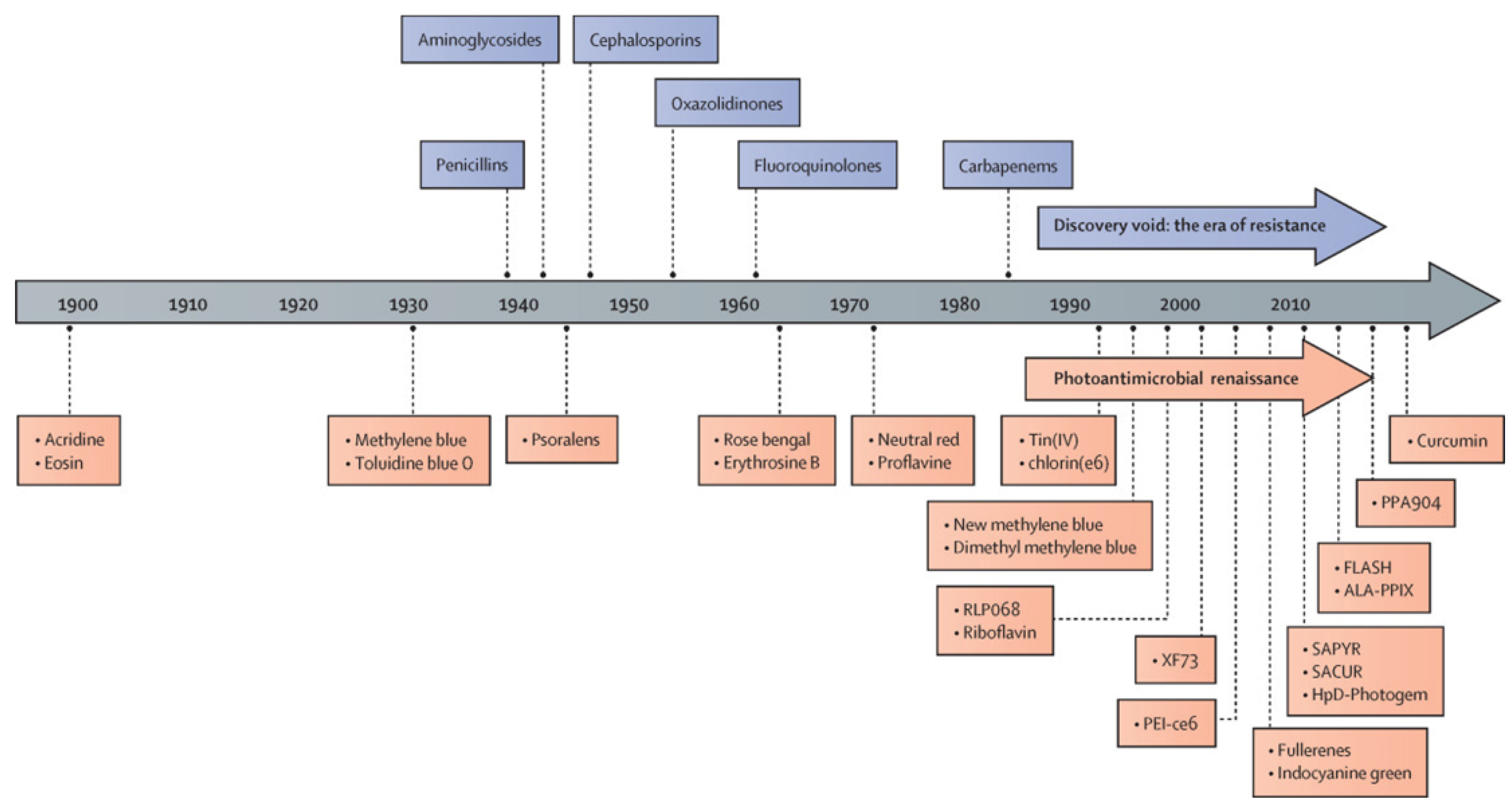
4. The History of Antimicrobial Photodynamic Therapy
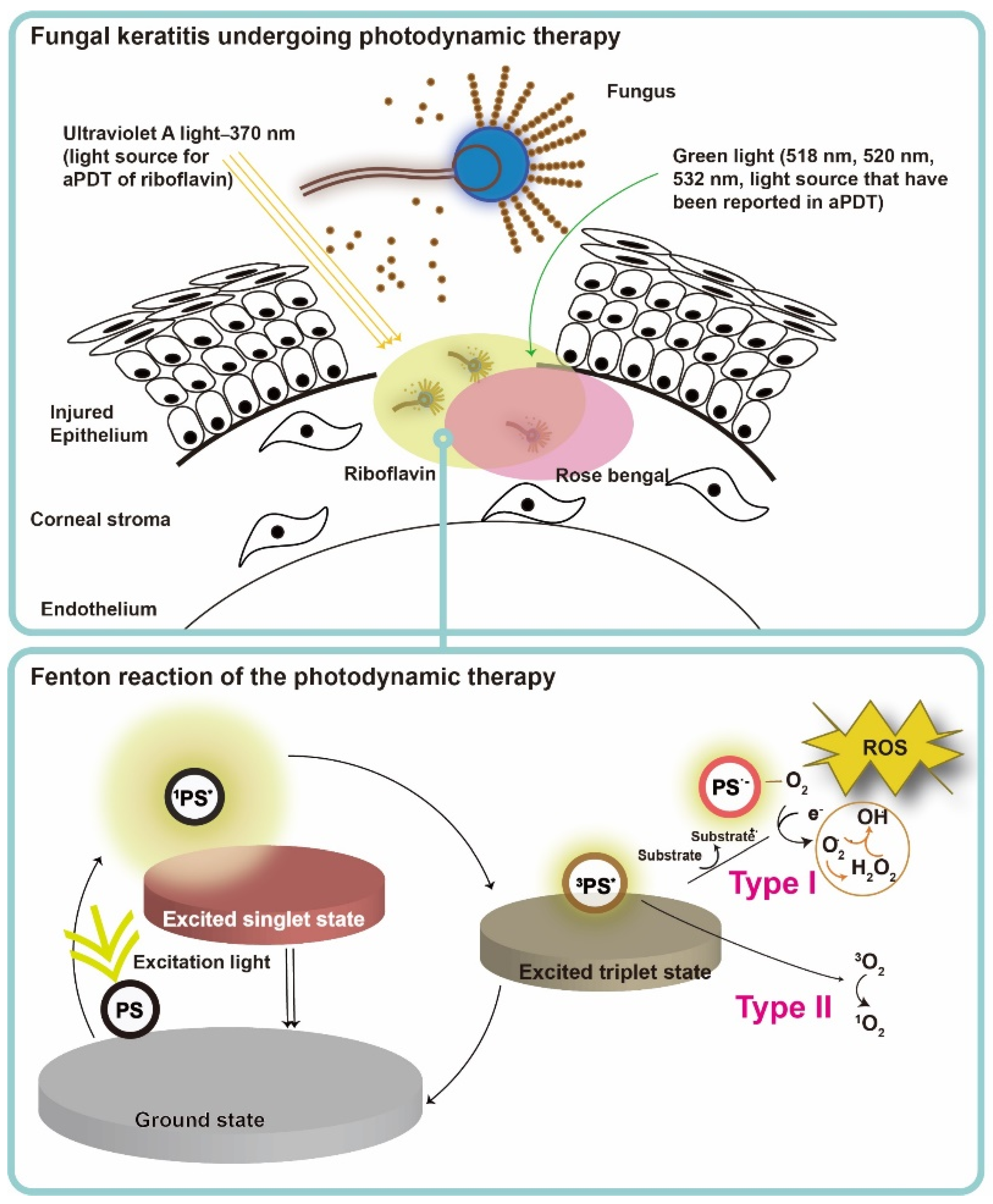
5. Mechanism of the Photodynamic Action in Fungal Infection
6. Antimycotic Photodynamic Therapy
6.1. First-Generation Photosensitizers
Porphyrins
6.2. Second-Generation Photosensitizers
6.2.1. Phenothiaziniums
6.2.2. 5-Aminolevulinic Acid
6.2.3. Phthalocyanines
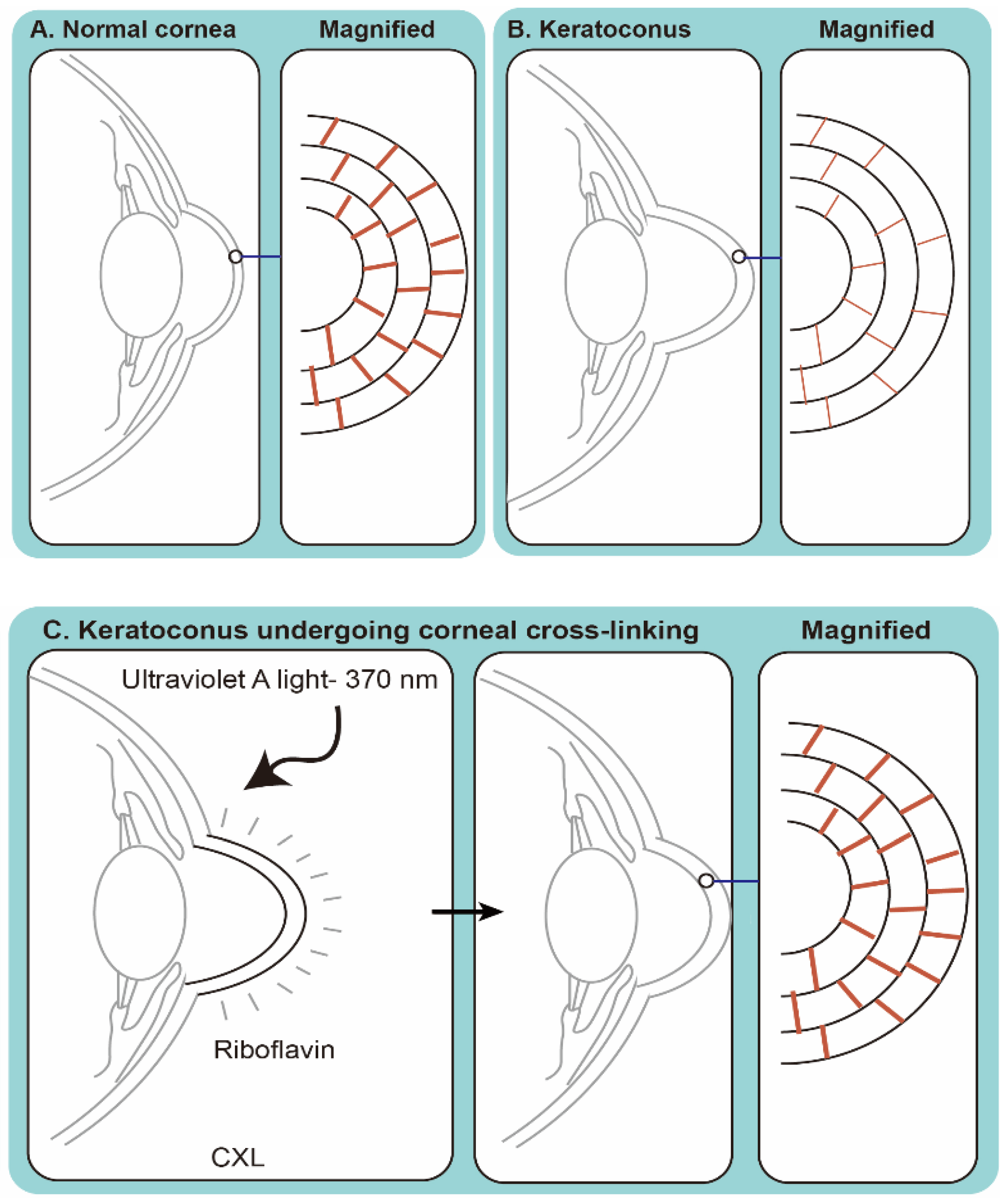
6.2.4. Riboflavin
6.2.5. Rose Bengal
7. aPDT against Fungal Biofilm
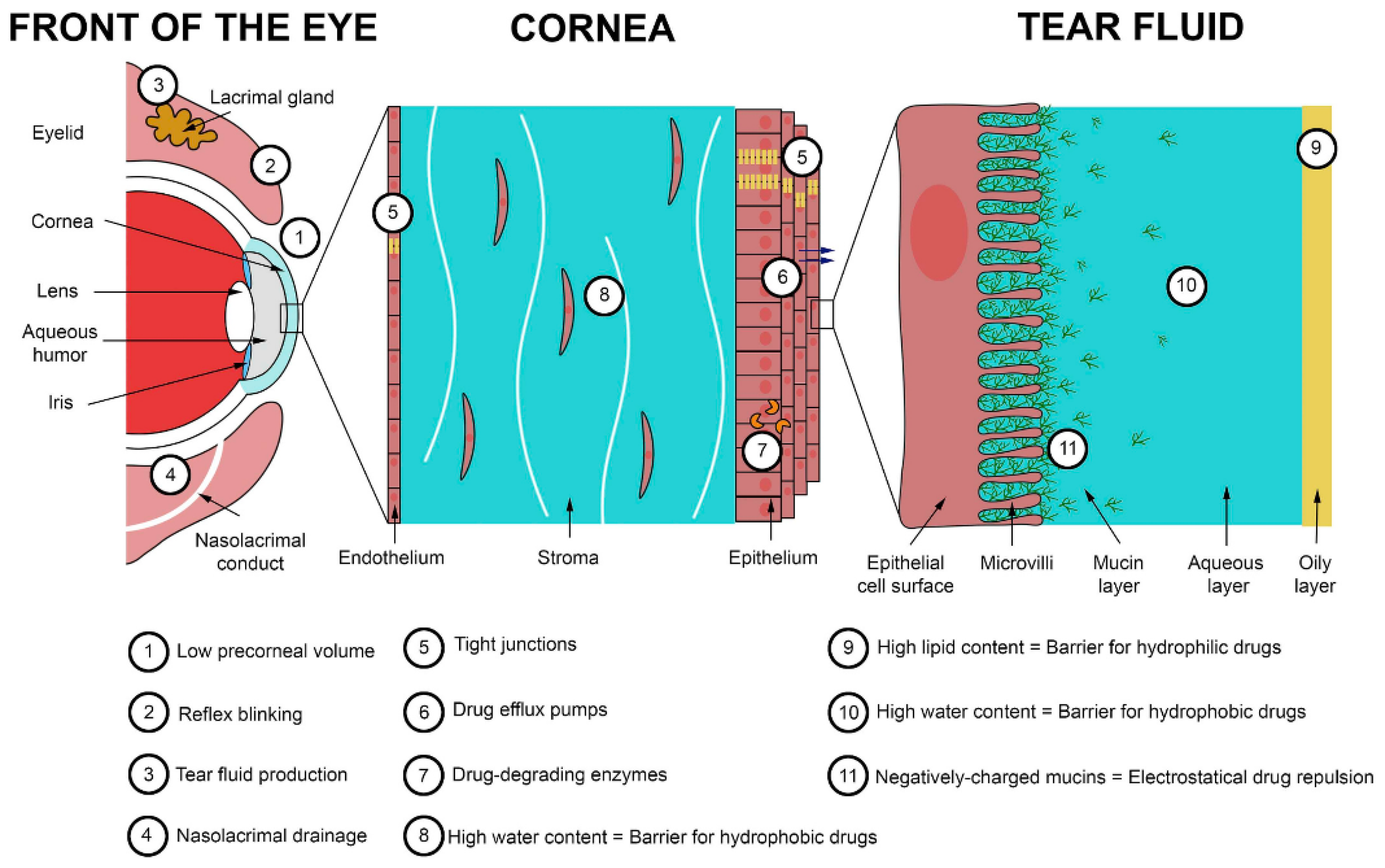
8. Challenges in Trans-Corneal Drug Delivery
9. The Future of aPDT in the Era of Nanomedicine
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ting, D.S.J.; Ho, C.S.; Deshmukh, R.; Said, D.G.; Dua, H.S. Infectious keratitis: An update on epidemiology, causative microorganisms, risk factors, and antimicrobial resistance. Eye 2021, 35, 1084–1101. [Google Scholar] [CrossRef]
- Ung, L.; Bispo, P.J.M.; Shanbhag, S.S.; Gilmore, M.S.; Chodosh, J. The persistent dilemma of microbial keratitis: Global burden, diagnosis, and antimicrobial resistance. Surv. Ophthalmol. 2019, 64, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Khor, W.B.; Prajna, V.N.; Garg, P.; Mehta, J.S.; Xie, L.; Liu, Z.; Padilla, M.D.B.; Joo, C.K.; Inoue, Y.; Goseyarakwong, P.; et al. The Asia Cornea Society Infectious Keratitis Study: A prospective multicenter study of infectious keratitis in Asia. Am. J. Ophthalmol. 2018, 195, 161–170. [Google Scholar] [CrossRef]
- Brown, L.; Leck, A.K.; Gichangi, M.; Burton, M.J.; Denning, D.W. The global incidence and diagnosis of fungal keratitis. Lancet Infect. Dis. 2021, 21, e49–e57. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, J.; Krysan, D.J. Drug resistance and tolerance in fungi. Nat. Rev. Microbiol. 2020, 18, 319–331. [Google Scholar] [CrossRef]
- Xie, L.; Dong, X.; Shi, W. Treatment of fungal keratitis by penetrating keratoplasty. Br. J. Ophthalmol. 2001, 85, 1070–1074. [Google Scholar] [CrossRef] [Green Version]
- Kirkness, C.M.; Ficker, L.A.; Steele, A.D.; Rice, N.S. The role of penetrating keratoplasty in the management of microbial keratitis. Eye 1991, 5 Pt 4, 425–431. [Google Scholar] [CrossRef]
- Tew, T.B.; Chu, H.S.; Hou, Y.C.; Chen, W.L.; Wang, I.J.; Hu, F.R. Therapeutic penetrating keratoplasty for microbial keratitis in Taiwan from 2001 to 2014. J. Formos. Med. Assoc. 2020, 119, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.; Yoon, C.H.; Kim, M.K.; Oh, J.Y. The incidence and outcomes of recurrence of infection after therapeutic penetrating keratoplasty for medically-uncontrolled infectious keratitis. J. Clin. Med. 2020, 9, 3696. [Google Scholar] [CrossRef]
- Vandeputte, P.; Ferrari, S.; Coste, A.T. Antifungal resistance and new strategies to control fungal infections. Int. J. Microbiol. 2012, 2012, 713687. [Google Scholar] [CrossRef] [PubMed]
- Sara, S.; Sharpe, K.; Morris, S. Multidrug-resistant Fusarium keratitis: Diagnosis and treatment considerations. BMJ Case Rep. 2016, 2016, bcr2016215401. [Google Scholar] [CrossRef]
- Lee, C.-N.; Hsu, R.; Chen, H.; Wong, T.-W. Daylight photodynamic therapy: An update. Molecules 2020, 25, 5195. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, M.; Maisch, T.; Nonell, S.; Plaetzer, K.; Almeida, A.; Tegos, G.P.; Hamblin, M.R. Photoantimicrobials—Are we afraid of the light? Lancet Infect. Dis. 2017, 17, e49–e55. [Google Scholar] [CrossRef]
- Cieplik, F.; Deng, D.; Crielaard, W.; Buchalla, W.; Hellwig, E.; Al-Ahmad, A.; Maisch, T. Antimicrobial photodynamic therapy—What we know and what we don’t. Crit. Rev. Microbiol. 2018, 44, 571–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, T.-W.; Liao, S.-Z.; Ko, W.-C.; Wu, C.-J.; Wu, S.B.; Chuang, Y.-C.; Huang, I.H. Indocyanine green-mediated photodynamic therapy reduces Methicillin-resistant Staphylococcus aureus drug resistance. J. Clin. Med. 2019, 8, 411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, D.K. Photodynamic therapy: Current role in the treatment of chorioretinal conditions. Eye 2016, 30, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Wollensak, G.; Spoerl, E.; Seiler, T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am. J. Ophthalmol. 2003, 135, 620–627. [Google Scholar] [CrossRef]
- Iseli, H.P.; Thiel, M.A.; Hafezi, F.; Kampmeier, J.; Seiler, T. Ultraviolet A/riboflavin corneal cross-linking for infectious keratitis associated with corneal melts. Cornea 2008, 27, 590–594. [Google Scholar] [CrossRef] [Green Version]
- Naranjo, A.; Arboleda, A.; Martinez, J.D.; Durkee, H.; Aguilar, M.C.; Relhan, N.; Nikpoor, N.; Galor, A.; Dubovy, S.R.; Leblanc, R.; et al. Rose bengal photodynamic antimicrobial therapy for patients with progressive infectious keratitis: A pilot clinical study. Am. J. Ophthalmol. 2019, 208, 387–396. [Google Scholar] [CrossRef]
- Altamirano, D.; Martinez, J.; Leviste, K.D.; Parel, J.M.; Amescua, G. Photodynamic therapy for infectious keratitis. Curr. Ophthalmol. Rep. 2020, 8, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P.A.; Kaliamurthy, J. Mycotic keratitis: Epidemiology, diagnosis and management. Clin. Microbiol. Infect 2013, 19, 210–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoudi, S.; Masoomi, A.; Ahmadikia, K.; Tabatabaei, S.A.; Soleimani, M.; Rezaie, S.; Ghahvechian, H.; Banafsheafshan, A. Fungal keratitis: An overview of clinical and laboratory aspects. Mycoses 2018, 61, 916–930. [Google Scholar] [CrossRef]
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the management of infectious keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef] [PubMed]
- Słowik, M.; Biernat, M.M.; Urbaniak-Kujda, D.; Kapelko-Słowik, K.; Misiuk-Hojło, M. Mycotic Infections of the Eye. Adv. Clin. Exp. Med. 2015, 24, 1113–1117. [Google Scholar] [CrossRef]
- Walther, G.; Stasch, S.; Kaerger, K.; Hamprecht, A.; Roth, M.; Cornely, O.A.; Geerling, G.; Mackenzie, C.R.; Kurzai, O.; von Lilienfeld-Toal, M. Fusarium keratitis in Germany. J. Clin. Microbiol. 2017, 55, 2983–2995. [Google Scholar] [CrossRef] [Green Version]
- Oliveira Dos Santos, C.; Kolwijck, E.; van der Lee, H.A.; Tehupeiory-Kooreman, M.C.; Al-Hatmi, A.M.S.; Matayan, E.; Burton, M.J.; Eggink, C.A.; Verweij, P.E. In vitro activity of chlorhexidine compared with seven antifungal agents against 98 fusarium isolates recovered from fungal keratitis patients. Antimicrob. Agents Chemother. 2019, 63, e02669-18. [Google Scholar] [CrossRef] [Green Version]
- Kalaiselvi, G.; Narayana, S.; Krishnan, T.; Sengupta, S. Intrastromal voriconazole for deep recalcitrant fungal keratitis: A case series. Br. J. Ophthalmol. 2015, 99, 195–198. [Google Scholar] [CrossRef]
- Sun, R.L.; Jones, D.B.; Wilhelmus, K.R. Clinical characteristics and outcome of Candida keratitis. Am. J. Ophthalmol. 2007, 143, 1043–1045. [Google Scholar] [CrossRef] [Green Version]
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The global problem of antifungal resistance: Prevalence, mechanisms, and management. Lancet Infect. Dis. 2017, 17, e383–e392. [Google Scholar] [CrossRef]
- Sponsel, W.E.; Graybill, J.R.; Nevarez, H.L.; Dang, D. Ocular and systemic posaconazole(SCH-56592) treatment of invasive Fusarium solani keratitis and endophthalmitis. Br. J. Ophthalmol. 2002, 86, 829–830. [Google Scholar] [CrossRef] [Green Version]
- Antequera, P.; Garcia-Conca, V.; Martín-González, C.; Ortiz-de-la-Tabla, V. Multidrug resistant Fusarium keratitis. Arch. Soc. Esp. Oftalmol. 2015, 90, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Tupaki-Sreepurna, A.; Al-Hatmi, A.M.; Kindo, A.J.; Sundaram, M.; de Hoog, G.S. Multidrug-resistant Fusarium in keratitis: A clinico-mycological study of keratitis infections in Chennai, India. Mycoses 2017, 60, 230–233. [Google Scholar] [CrossRef]
- Vermitsky, J.-P.; Edlind, T.D. Azole resistance in Candida glabrata: Coordinate upregulation of multidrug transporters and evidence for a Pdr1-like transcription factor. Antimicrob. Agents Chemother. 2004, 48, 3773–3781. [Google Scholar] [CrossRef] [Green Version]
- Costa-de-Oliveira, S.; Rodrigues, A.G. Candida albicans antifungal resistance and tolerance in bloodstream infections: The triad yeast-host-antifungal. Microorganisms 2020, 8, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowen, L.E.; Sanglard, D.; Howard, S.J.; Rogers, P.D.; Perlin, D.S. Mechanisms of antifungal drug resistance. Cold Spring Harb. Perspect. Med. 2014, 5, a019752. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Dodds Ashley, E.S.; Drew, R.H.; Perfect, J.R. Antifungal pharmacotherapy for invasive mould infections. Expert Opin. Pharm. 2003, 4, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Zonios, D.I.; Bennett, J.E. Update on azole antifungals. Semin. Respir. Crit. Care Med. 2008, 29, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical practice guideline for the management of Candidiasis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Denning, D.W. Echinocandin antifungal drugs. Lancet 2003, 362, 1142–1151. [Google Scholar] [CrossRef]
- Kaur, S.; Singh, S. Biofilm formation by Aspergillus fumigatus. Med. Mycol. 2014, 52, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Donlan, R.M. Biofilms: Microbial life on surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Pierce, C.G.; Srinivasan, A.; Uppuluri, P.; Ramasubramanian, A.K.; López-Ribot, J.L. Antifungal therapy with an emphasis on biofilms. Curr. Opin. Pharmacol. 2013, 13, 726–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Córdova-Alcántara, I.M.; Venegas-Cortés, D.L.; Martínez-Rivera, M.; Pérez, N.O.; Rodriguez-Tovar, A.V. Biofilm characterization of Fusarium solani keratitis isolate: Increased resistance to antifungals and UV light. J. Microbiol. 2019, 57, 485–497. [Google Scholar] [CrossRef]
- Nobile, C.J.; Johnson, A.D. Candida albicans biofilms and human disease. Annu. Rev. Microbiol. 2015, 69, 71–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, P.K.; Chandra, J.; Yu, C.; Sun, Y.; Pearlman, E.; Ghannoum, M.A. Characterization of fusarium keratitis outbreak isolates: Contribution of biofilms to antimicrobial resistance and pathogenesis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4450–4457. [Google Scholar] [CrossRef] [Green Version]
- Delattin, N.; Cammue, B.P.; Thevissen, K. Reactive oxygen species-inducing antifungal agents and their activity against fungal biofilms. Future Med. Chem. 2014, 6, 77–90. [Google Scholar] [CrossRef]
- Nagy, F.; Tóth, Z.; Daróczi, L.; Székely, A.; Borman, A.M.; Majoros, L.; Kovács, R. Farnesol increases the activity of echinocandins against Candida auris biofilms. Med. Mycol. 2020, 58, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Perez-Laguna, V.; Gilaberte, Y.; Millan-Lou, M.I.; Agut, M.; Nonell, S.; Rezusta, A.; Hamblin, M.R. A combination of photodynamic therapy and antimicrobial compounds to treat skin and mucosal infections: A systematic review. Photochem. Photobiol. Sci. 2019, 18, 1020–1029. [Google Scholar] [CrossRef]
- Sengupta, J.; Saha, S.; Khetan, A.; Sarkar, S.K.; Mandal, S.M. Effects of lactoferricin B against keratitis-associated fungal biofilms. J. Infect. Chemother. 2012, 18, 698–703. [Google Scholar] [CrossRef]
- Zacchino, S.A.; Butassi, E.; Cordisco, E.; Svetaz, L.A. Hybrid combinations containing natural products and antimicrobial drugs that interfere with bacterial and fungal biofilms. Phytomedicine 2017, 37, 14–26. [Google Scholar] [CrossRef]
- Cepas, V.; López, Y.; Gabasa, Y.; Martins, C.B.; Ferreira, J.D.; Correia, M.J.; Santos, L.M.A.; Oliveira, F.; Ramos, V.; Reis, M.; et al. Inhibition of bacterial and fungal biofilm formation by 675 extracts from microalgae and cyanobacteria. Antibiotics 2019, 8, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarro, J.; Rubio, C.; Gené, J.; Cano, J.; Gil, J.; Benito, R.; Moranderia, M.J.; Miguez, E. Case of keratitis caused by an uncommon Fusarium species. J. Clin. Microbiol. 2003, 41, 5823–5826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, E.Y.; McCartney, D.L.; Beatty, R.F.; Springer, K.L.; Levy, J.; Edward, D. Successful treatment of resistant ocular fusariosis with posaconazole (SCH-56592). Am. J. Ophthalmol. 2007, 143, 222–227.e221. [Google Scholar] [CrossRef] [PubMed]
- Proença-Pina, J.; Ssi Yan Kai, I.; Bourcier, T.; Fabre, M.; Offret, H.; Labetoulle, M. Fusarium keratitis and endophthalmitis associated with lens contact wear. Int. Ophthalmol. 2010, 30, 103–107. [Google Scholar] [CrossRef]
- Edelstein, S.L.; Akduman, L.; Durham, B.H.; Fothergill, A.W.; Hsu, H.Y. Resistant Fusarium keratitis progressing to endophthalmitis. Eye Contact Lens 2012, 38, 331–335. [Google Scholar] [CrossRef]
- Vecchio, D.; Dai, T.; Huang, L.; Fantetti, L.; Roncucci, G.; Hamblin, M.R. Antimicrobial photodynamic therapy with RLP068 kills methicillin-resistant Staphylococcus aureus and improves wound healing in a mouse model of infected skin abrasion PDT with RLP068/Cl in infected mouse skin abrasion. J. Biophotonics 2013, 6, 733–742. [Google Scholar] [CrossRef] [Green Version]
- Kashef, N.; Akbarizare, M.; Kamrava, S.K. Effect of sub-lethal photodynamic inactivation on the antibiotic susceptibility and biofilm formation of clinical Staphylococcus aureus isolates. Photodiagn. Photodyn. Ther. 2013, 10, 368–373. [Google Scholar] [CrossRef]
- Ethirajan, M.; Chen, Y.; Joshi, P.; Pandey, R.K. The role of porphyrin chemistry in tumor imaging and photodynamic therapy. Chem. Soc. Rev. 2011, 40, 340–362. [Google Scholar] [CrossRef]
- Jeon, Y.M.; Lee, H.S.; Jeong, D.; Oh, H.K.; Ra, K.H.; Lee, M.Y. Antimicrobial photodynamic therapy using chlorin e6 with halogen light for acne bacteria-induced inflammation. Life Sci. 2015, 124, 56–63. [Google Scholar] [CrossRef]
- Fekrazad, R.; Ghasemi Barghi, V.; Poorsattar Bejeh Mir, A.; Shams-Ghahfarokhi, M. In vitro photodynamic inactivation of Candida albicans by phenothiazine dye (new methylene blue) and indocyanine green (EmunDo®). Photodiagn. Photodyn. Ther. 2015, 12, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Maisch, T.; Eichner, A.; Späth, A.; Gollmer, A.; König, B.; Regensburger, J.; Bäumler, W. Fast and effective photodynamic inactivation of multiresistant bacteria by cationic riboflavin derivatives. PLoS ONE 2014, 9, e111792. [Google Scholar] [CrossRef] [Green Version]
- Maisch, T.; Bosl, C.; Szeimies, R.M.; Lehn, N.; Abels, C. Photodynamic effects of novel XF porphyrin derivatives on prokaryotic and eukaryotic cells. Antimicrob. Agents Chemother. 2005, 49, 1542–1552. [Google Scholar] [CrossRef] [Green Version]
- Mizuno, K.; Zhiyentayev, T.; Huang, L.; Khalil, S.; Nasim, F.; Tegos, G.P.; Gali, H.; Jahnke, A.; Wharton, T.; Hamblin, M.R. Antimicrobial photodynamic therapy with functionalized fullerenes: Quantitative structure-activity relationships. J. Nanomed. Nanotechnol. 2011, 2, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Topaloglu, N.; Gulsoy, M.; Yuksel, S. Antimicrobial photodynamic therapy of resistant bacterial strains by indocyanine green and 809-nm diode laser. Photomed. Laser Surg. 2013, 31, 155–162. [Google Scholar] [CrossRef]
- Cieplik, F.; Späth, A.; Regensburger, J.; Gollmer, A.; Tabenski, L.; Hiller, K.A.; Bäumler, W.; Maisch, T.; Schmalz, G. Photodynamic biofilm inactivation by SAPYR--an exclusive singlet oxygen photosensitizer. Free Radic. Biol. Med. 2013, 65, 477–487. [Google Scholar] [CrossRef] [Green Version]
- Tortik, N.; Steinbacher, P.; Maisch, T.; Spaeth, A.; Plaetzer, K. A comparative study on the antibacterial photodynamic efficiency of a curcumin derivative and a formulation on a porcine skin model. Photochem. Photobiol. Sci. 2016, 15, 187–195. [Google Scholar] [CrossRef]
- Ricci Donato, H.A.; Pratavieira, S.; Grecco, C.; Brugnera-Júnior, A.; Bagnato, V.S.; Kurachi, C. Clinical comparison of two photosensitizers for oral cavity decontamination. Photomed. Laser Surg. 2017, 35, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, C.J.; Niu, C.; Foltz, W.; Chen, Y.; Sidorova-Darmos, E.; Eubanks, J.H.; Lilge, L. ALA-PpIX mediated photodynamic therapy of malignant gliomas augmented by hypothermia. PLoS ONE 2017, 12, e0181654. [Google Scholar] [CrossRef] [Green Version]
- Morley, S.; Griffiths, J.; Philips, G.; Moseley, H.; O’Grady, C.; Mellish, K.; Lankester, C.L.; Faris, B.; Young, R.J.; Brown, S.B.; et al. Phase IIa randomized, placebo-controlled study of antimicrobial photodynamic therapy in bacterially colonized, chronic leg ulcers and diabetic foot ulcers: A new approach to antimicrobial therapy. Br. J. Dermatol. 2013, 168, 617–624. [Google Scholar] [CrossRef]
- Lee, H.J.; Kang, S.M.; Jeong, S.H.; Chung, K.H.; Kim, B.I. Antibacterial photodynamic therapy with curcumin and Curcuma xanthorrhiza extract against Streptococcus mutans. Photodiagn. Photodyn. Ther. 2017, 20, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; McCarron, P.A.; Tunney, M.M. Antifungal photodynamic therapy. Microbiol. Res. 2008, 163, 1–12. [Google Scholar] [CrossRef]
- Baltazar, L.M.; Ray, A.; Santos, D.A.; Cisalpino, P.S.; Friedman, A.J.; Nosanchuk, J.D. Antimicrobial photodynamic therapy: An effective alternative approach to control fungal infections. Front. Microbiol. 2015, 6, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, G.; Wei, Z.; Wang, L.; Shen, J.; Baudouin, C.; Labbé, A.; Liang, Q. Evaluation of toluidine blue-mediated photodynamic therapy for experimental bacterial keratitis in rabbits. Transl. Vis. Sci. Technol. 2020, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Shih, M.H.; Huang, F.C. Effects of photodynamic therapy on rapidly growing nontuberculous mycobacteria keratitis. Investig. Ophthalmol. Vis. Sci. 2011, 52, 223–229. [Google Scholar] [CrossRef]
- Halili, F.; Arboleda, A.; Durkee, H.; Taneja, M.; Miller, D.; Alawa, K.A.; Aguilar, M.C.; Amescua, G.; Flynn, H.W., Jr.; Parel, J.M. Rose bengal- and riboflavin-mediated photodynamic therapy to inhibit Methicillin-resistant Staphylococcus aureus keratitis isolates. Am. J. Ophthalmol. 2016, 166, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Arboleda, A.; Miller, D.; Cabot, F.; Taneja, M.; Aguilar, M.C.; Alawa, K.; Amescua, G.; Yoo, S.H.; Parel, J.M. Assessment of rose bengal versus riboflavin photodynamic therapy for inhibition of fungal keratitis isolates. Am. J. Ophthalmol. 2014, 158, 64–70.e62. [Google Scholar] [CrossRef] [Green Version]
- Ito, T. Photodynamic action of hematoporphyrin on yeast cells--a kinetic approach. Photochem. Photobiol. 1981, 34, 521–524. [Google Scholar] [CrossRef]
- Carré, V.; Gaud, O.; Sylvain, I.; Bourdon, O.; Spiro, M.; Biais, J.; Granet, R.; Krausz, P.; Guilloton, M. Fungicidal properties of meso-arylglycosylporphyrins: Influence of sugar substituents on photoinduced damage in the yeast Saccharomyces cerevisiœ. J. Photochem. Photobiol. B Biol. 1999, 48, 57–62. [Google Scholar] [CrossRef]
- Voit, T.; Cieplik, F.; Regensburger, J.; Hiller, K.A.; Gollmer, A.; Buchalla, W.; Maisch, T. Spatial distribution of a porphyrin-based photosensitizer reveals mechanism of photodynamic inactivation of Candida albicans. Front. Med. 2021, 8, 641244. [Google Scholar] [CrossRef]
- Zoładek, T.; Nguyen, B.N.; Jagiełło, I.; Graczyk, A.; Rytka, J. Diamino acid derivatives of porphyrins penetrate into yeast cells, induce photodamage, but have no mutagenic effect. Photochem. Photobiol. 1997, 66, 253–259. [Google Scholar] [CrossRef]
- Baskaran, R.; Lee, J.; Yang, S.-G. Clinical development of photodynamic agents and therapeutic applications. Biomater. Res. 2018, 22, 25. [Google Scholar] [CrossRef]
- Paardekooper, M.; Van den Broek, P.J.; De Bruijne, A.W.; Elferink, J.G.; Dubbelman, T.M.; Van Steveninck, J. Photodynamic treatment of yeast cells with the dye toluidine blue: All-or-none loss of plasma membrane barrier properties. Biochim. Biophys. Acta 1992, 1108, 86–90. [Google Scholar] [CrossRef]
- de Souza, S.C.; Junqueira, J.C.; Balducci, I.; Koga-Ito, C.Y.; Munin, E.; Jorge, A.O. Photosensitization of different Candida species by low power laser light. J. Photochem. Photobiol. B 2006, 83, 34–38. [Google Scholar] [CrossRef]
- Demidova, T.N.; Hamblin, M.R. Effect of cell-photosensitizer binding and cell density on microbial photoinactivation. Antimicrob. Agents Chemother. 2005, 49, 2329–2335. [Google Scholar] [CrossRef] [Green Version]
- Giroldo, L.M.; Felipe, M.P.; de Oliveira, M.A.; Munin, E.; Alves, L.P.; Costa, M.S. Photodynamic antimicrobial chemotherapy (PACT) with methylene blue increases membrane permeability in Candida albicans. Lasers Med. Sci. 2009, 24, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Güzel Tunçcan, Ö.; Kalkancı, A.; Unal, E.A.; Abdulmajed, O.; Erdoğan, M.; Dizbay, M.; Çağlar, K. The in vitro effect of antimicrobial photodynamic therapy on Candida and Staphylococcus biofilms. Turk. J. Med. Sci. 2018, 48, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, G.; Shankar, A.A. Toluidine blue: A review of its chemistry and clinical utility. J. Oral Maxillofac. Pathol. 2012, 16, 251–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wainwright, M. Photodynamic antimicrobial chemotherapy (PACT). J. Antimicrob. Chemother. 1998, 42, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Wiench, R.; Skaba, D.; Matys, J.; Grzech-Lesniak, K. Efficacy of toluidine blue-mediated antimicrobial photodynamic therapy on Candida spp. a systematic review. Antibiotics 2021, 10, 349. [Google Scholar] [CrossRef]
- Brouillet, N.; Arselin-De Chateaubodeau, G.; Volland, C. Studies on protoporphyrin biosynthetic pathway in Saccharomyces cerevisiae; characterization of the tetrapyrrole intermediates. Biochimie 1975, 57, 647–655. [Google Scholar] [CrossRef]
- Strakhovskaya, M.G.; Shumarina, A.O.; Fraikin, G.Y.; Rubin, A.B. Synthesis of protoporphyrin IX induced by 5-aminolevulinic acid in yeast cells in the presence of 2,2;-dipyridyl. Biochemistry 1998, 63, 725–728. [Google Scholar]
- Monfrecola, G.; Procaccini, E.M.; Bevilacqua, M.; Manco, A.; Calabro, G.; Santoianni, P. In vitro effect of 5-aminolaevulinic acid plus visible light on Candida albicans. Photochem. Photobiol. Sci. 2004, 3, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.T.; Prates, R.A.; Sabino, C.P.; Fuchs, B.B.; Tegos, G.P.; Mylonakis, E.; Hamblin, M.R.; Ribeiro, M.S. Antimicrobial photodynamic inactivation inhibits Candida albicans virulence factors and reduces in vivo pathogenicity. Antimicrob. Agents Chemother. 2013, 57, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Xu, M.; Pan, W.; Wang, M.; Wu, X.; Dai, S.; Li, L.; Zeng, K. Antimicrobial and immunomodulatory responses of photodynamic therapy in Galleria mellonella model. BMC Microbiol. 2020, 20, 196. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Li, J.; Zhang, H.; Zhang, J.; Sun, H. Effect of 5-aminolevulinic acid photodynamic therapy on Candida albicans biofilms: An in vitro study. Photodiagn. Photodyn. Ther. 2016, 15, 40–45. [Google Scholar] [CrossRef]
- Lomax, S.Q. Phthalocyanine and quinacridone pigments: Their history, properties and use. Stud. Conserv. 2005, 50, 19–29. [Google Scholar] [CrossRef]
- Berg, K.; Bommer, J.C.; Moan, J. Evaluation of sulfonated aluminum phthalocyanines for use in photochemotherapy. A study on the relative efficiencies of photoinactivation. Photochem. Photobiol. 1989, 49, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Bertoloni, G.; Rossi, F.; Valduga, G.; Jori, G.; Ali, H.; van Lier, J.E. Photosensitizing activity of water- and lipid-soluble phthalocyanines on prokaryotic and eukaryotic microbial cells. Microbios 1992, 71, 33–46. [Google Scholar]
- Ozturk, I.; Tunçel, A.; Lambrecht, F.; Bıyıklıoğlu, Z.; Ince, M.; Ocakoglu, K. Antifungal photodynamic activities of phthalocyanine derivatives on Candida albicans. Photodiagn. Photodyn. Ther. 2020, 30, 101715. [Google Scholar] [CrossRef]
- Lo, P.C.; Rodriguez-Morgade, M.S.; Pandey, R.K.; Ng, D.K.P.; Torres, T.; Dumoulin, F. The unique features and promises of phthalocyanines as advanced photosensitisers for photodynamic therapy of cancer. Chem. Soc. Rev. 2020, 49, 1041–1056. [Google Scholar] [CrossRef]
- Jeng, B.H.; Farid, M.; Patel, S.V.; Schwab, I.R. Corneal cross-linking for keratoconus: A look at the data, the food and drug administration, and the future. Ophthalmology 2016, 123, 2270–2272. [Google Scholar] [CrossRef] [Green Version]
- Salomão, M.Q.; Hofling-Lima, A.L.; Gomes Esporcatte, L.P.; Correa, F.F.; Lopes, B.; Sena, N., Jr.; Dawson, D.G.; Ambrósio, R., Jr. Ectatic diseases. Exp. Eye Res. 2021, 202, 108347. [Google Scholar] [CrossRef]
- McCall, A.S.; Kraft, S.; Edelhauser, H.F.; Kidder, G.W.; Lundquist, R.R.; Bradshaw, H.E.; Dedeic, Z.; Dionne, M.J.; Clement, E.M.; Conrad, G.W. Mechanisms of corneal tissue cross-linking in response to treatment with topical riboflavin and long-wavelength ultraviolet radiation (UVA). Investig. Ophthalmol. Vis. Sci. 2010, 51, 129–138. [Google Scholar] [CrossRef]
- Spoerl, E.; Huhle, M.; Seiler, T. Induction of cross-links in corneal tissue. Exp. Eye Res. 1998, 66, 97–103. [Google Scholar] [CrossRef]
- Meek, K.M.; Hayes, S. Corneal cross-linking—A review. Ophthalmic Physiol. Opt. 2013, 33, 78–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, T.C.; Lau, T.W.; Lee, J.W.; Wong, I.Y.; Jhanji, V.; Wong, R.L. Corneal collagen cross-linking for infectious keratitis: An update of clinical studies. Acta Ophthalmol. 2015, 93, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Prajna, N.V.; Radhakrishnan, N.; Lalitha, P.; Austin, A.; Ray, K.J.; Keenan, J.D.; Porco, T.C.; Lietman, T.M.; Rose-Nussbaumer, J. Cross-linking-assisted infection reduction: A randomized clinical trial evaluating the effect of adjuvant cross-linking on outcomes in fungal keratitis. Ophthalmology 2020, 127, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Tabibian, D.; Richoz, O.; Hafezi, F. PACK-CXL: Corneal cross-linking for treatment of infectious keratitis. J. Ophthalmic Vis. Res. 2015, 10, 77–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, S.A.; Combs, J.C.; Noguera, G.; Camacho, W.; Wittmann, P.; Walther, R.; Cano, M.; Dick, J.; Behrens, A. Antimicrobial efficacy of riboflavin/UVA combination (365 nm) in vitro for bacterial and fungal isolates: A potential new treatment for infectious keratitis. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3402–3408. [Google Scholar] [CrossRef] [Green Version]
- Said, D.G.; Elalfy, M.S.; Gatzioufas, Z.; El-Zakzouk, E.S.; Hassan, M.A.; Saif, M.Y.; Zaki, A.A.; Dua, H.S.; Hafezi, F. Collagen cross-linking with photoactivated riboflavin (PACK-CXL) for the treatment of advanced infectious keratitis with corneal melting. Ophthalmology 2014, 121, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Tenkman, L.R.; Schrier, A.; Fairchild, K.M.; Trokel, S.L.; Price, F.W., Jr. Photoactivated riboflavin treatment of infectious keratitis using collagen cross-linking technology. J. Refract. Surg. 2012, 28, 706–713. [Google Scholar] [CrossRef]
- Makdoumi, K.; Mortensen, J.; Sorkhabi, O.; Malmvall, B.E.; Crafoord, S. UVA-riboflavin photochemical therapy of bacterial keratitis: A pilot study. Graefes Arch. Clin. Exp. Ophthalmol. 2012, 250, 95–102. [Google Scholar] [CrossRef]
- Prajna, N.V.; Radhakrishnan, N.; Lalitha, P.; Rajaraman, R.; Narayana, S.; Austin, A.F.; Liu, Z.; Keenan, J.D.; Porco, T.C.; Lietman, T.M.; et al. Cross-linking assisted infection reduction (CLAIR): A randomized clinical trial evaluating the effect of adjuvant cross-linking on bacterial keratitis. Cornea 2020, 40, 837–841. [Google Scholar] [CrossRef] [PubMed]
- Uddaraju, M.; Mascarenhas, J.; Das, M.R.; Radhakrishnan, N.; Keenan, J.D.; Prajna, L.; Prajna, V.N. Corneal cross-linking as an adjuvant therapy in the management of recalcitrant deep stromal fungal keratitis: A randomized trial. Am. J. Ophthalmol. 2015, 160, 131–134.e135. [Google Scholar] [CrossRef]
- Vajpayee, R.B.; Shafi, S.N.; Maharana, P.K.; Sharma, N.; Jhanji, V. Evaluation of corneal collagen cross-linking as an additional therapy in mycotic keratitis. Clin. Exp. Ophthalmol. 2015, 43, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Kasetsuwan, N.; Reinprayoon, U.; Satitpitakul, V. Photoactivated chromophore for moderate to severe infectious keratitis as an adjunct therapy: A randomized controlled trial. Am. J. Ophthalmol. 2016, 165, 94–99. [Google Scholar] [CrossRef]
- Mikropoulos, D.G.; Kymionis, G.D.; Voulgari, N.; Kaisari, E.; Nikolakopoulos, K.A.; Katsanos, A.; Konstas, A.G. Intraoperative photoactivated chromophore for infectious keratitis-corneal cross-linking (PACK-CXL) during penetrating keratoplasty for the management of fungal keratitis in an immunocompromised patient. Ophthalmol. Ther. 2019, 8, 491–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, P.N. The composition of erythrosins, fluorescein, phloxine and rose bengal: A study using thin-layer chromatography and solvent extraction. Histochem. J. 1976, 8, 487–499. [Google Scholar] [CrossRef]
- Feenstra, R.P.; Tseng, S.C. Comparison of fluorescein and rose bengal staining. Ophthalmology 1992, 99, 605–617. [Google Scholar] [CrossRef]
- Lazarova, G. Effect of glutathione on rose bengal photosensitized yeast damage. Microbios 1993, 75, 39–43. [Google Scholar]
- Amescua, G.; Arboleda, A.; Nikpoor, N.; Durkee, H.; Relhan, N.; Aguilar, M.C.; Flynn, H.W.; Miller, D.; Parel, J.M. Rose bengal photodynamic antimicrobial therapy: A novel treatment for resistant fusarium keratitis. Cornea 2017, 36, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.C.; Rasteiro, V.M.; Pereira, C.A.; Rossoni, R.D.; Junqueira, J.C.; Jorge, A.O. The effects of rose bengal- and erythrosine-mediated photodynamic therapy on Candida albicans. Mycoses 2012, 55, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Cherfan, D.; Verter, E.E.; Melki, S.; Gisel, T.E.; Doyle, F.J., Jr.; Scarcelli, G.; Yun, S.H.; Redmond, R.W.; Kochevar, I.E. Collagen cross-linking using rose bengal and green light to increase corneal stiffness. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3426–3433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wertheimer, C.M.; Mendes, B.; Pei, Q.; Brandt, K.; Kochevar, I.E. Arginine as an enhancer in rose bengal photosensitized corneal crosslinking. Transl. Vis. Sci. Technol. 2020, 9, 24. [Google Scholar] [CrossRef]
- Santhiago, M.R.; Randleman, J.B. The biology of corneal cross-linking derived from ultraviolet light and riboflavin. Exp. Eye Res. 2021, 202, 108355. [Google Scholar] [CrossRef]
- Fadlallah, A.; Zhu, H.; Arafat, S.; Kochevar, I.; Melki, S.; Ciolino, J.B. Corneal resistance to keratolysis after collagen crosslinking with rose bengal and green light. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6610–6614. [Google Scholar] [CrossRef]
- Martinez, J.D.; Naranjo, A.; Amescua, G.; Dubovy, S.R.; Arboleda, A.; Durkee, H.; Aguilar, M.C.; Flynn, H.W.; Miller, D.; Parel, J.M. Human corneal changes after rose bengal photodynamic antimicrobial therapy for treatment of fungal keratitis. Cornea 2018, 37, e46–e48. [Google Scholar] [CrossRef]
- Peterson, J.C.; Arrieta, E.; Ruggeri, M.; Silgado, J.D.; Mintz, K.J.; Weisson, E.H.; Leblanc, R.M.; Kochevar, I.; Manns, F.; Parel, J.M. Detection of singlet oxygen luminescence for experimental corneal rose bengal photodynamic antimicrobial therapy. Biomed. Opt. Express 2021, 12, 272–287. [Google Scholar] [CrossRef]
- de Melo, W.C.; Avci, P.; de Oliveira, M.N.; Gupta, A.; Vecchio, D.; Sadasivam, M.; Chandran, R.; Huang, Y.Y.; Yin, R.; Perussi, L.R.; et al. Photodynamic inactivation of biofilm: Taking a lightly colored approach to stubborn infection. Expert Rev. Anti-Infect. Ther. 2013, 11, 669–693. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.C.; de Campos Rasteiro, V.M.; Pereira, C.A.; da Silva Hashimoto, E.S.; Beltrame, M., Jr.; Junqueira, J.C.; Jorge, A.O. Susceptibility of Candida albicans and Candida dubliniensis to erythrosine- and LED-mediated photodynamic therapy. Arch. Oral Biol. 2011, 56, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.P.; dos Santos, T.A.; de Barros, P.P.; de Camargo Ribeiro, F.; Junqueira, J.C.; Jorge, A.O. Action of antimicrobial photodynamic therapy on heterotypic biofilm: Candida albicans and Bacillus atrophaeus. Lasers Med. Sci. 2016, 31, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warrier, A.; Mazumder, N.; Prabhu, S.; Satyamoorthy, K.; Murali, T.S. Photodynamic therapy to control microbial biofilms. Photodiagn. Photodyn. Ther. 2021, 33, 102090. [Google Scholar] [CrossRef]
- Akpek, E.K.; Gottsch, J.D. Immune defense at the ocular surface. Eye 2003, 17, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Moiseev, R.V.; Morrison, P.W.J.; Steele, F.; Khutoryanskiy, V.V. Penetration enhancers in ocular drug delivery. Pharmaceutics 2019, 11, 321. [Google Scholar] [CrossRef] [Green Version]
- Jumelle, C.; Gholizadeh, S.; Annabi, N.; Dana, R. Advances and limitations of drug delivery systems formulated as eye drops. J. Control. Release 2020, 321, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Nubile, M.; Calienno, R.; Mattei, P.A.; Pedrotti, E.; Salgari, N.; Mastropasqua, R.; Lanzini, M. Corneal cross-linking: Intrastromal riboflavin concentration in iontophoresis-assisted imbibition versus traditional and transepithelial techniques. Am. J. Ophthalmol. 2014, 157, 623–630.e621. [Google Scholar] [CrossRef]
- Lamy, R.; Chan, E.; Zhang, H.; Salgaonkar, V.A.; Good, S.D.; Porco, T.C.; Diederich, C.J.; Stewart, J.M. Ultrasound-enhanced penetration of topical riboflavin into the corneal stroma. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5908–5912. [Google Scholar] [CrossRef] [Green Version]
- Tefon Aribaş, A.B.; Sarikaya, B.; Bilgihan, K. Iontophoresis-assisted rose bengal and green light corneal cross-linking. Cornea 2020, 39, 1533–1540. [Google Scholar] [CrossRef]
- Wu, H.; Li, L.; Luo, S.; Fang, X.; Shang, X.; Xie, Z.; Xiao, X.; He, H.; Lin, Z.; Liu, Z. Safety and efficacy of repeated crosslinking assisted by transepithelial double-cycle iontophoresis in keratoconus progression after primary corneal crosslinking. Eye 2021, 35, 3020–3027. [Google Scholar] [CrossRef]
- Ustundag Okur, N.; Caglar, E.S.; Siafaka, P.I. Novel ocular drug delivery systems: An update on microemulsions. J. Ocul. Pharmacol. Ther. 2020, 36, 342–354. [Google Scholar] [CrossRef]
- Lalu, L.; Tambe, V.; Pradhan, D.; Nayak, K.; Bagchi, S.; Maheshwari, R.; Kalia, K.; Tekade, R.K. Novel nanosystems for the treatment of ocular inflammation: Current paradigms and future research directions. J. Control. Release 2017, 268, 19–39. [Google Scholar] [CrossRef]
- Ikuta, Y.; Aoyagi, S.; Tanaka, Y.; Sato, K.; Inada, S.; Koseki, Y.; Onodera, T.; Oikawa, H.; Kasai, H. Creation of nano eye-drops and effective drug delivery to the interior of the eye. Sci. Rep. 2017, 7, 44229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucky, S.S.; Soo, K.C.; Zhang, Y. Nanoparticles in photodynamic therapy. Chem. Rev. 2015, 115, 1990–2042. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Han, H.; Chen, Y.; Zhang, X.; Gao, Y.; Li, S.; Jin, Q.; Ji, J.; Yao, K. Antimicrobial nanomedicine for ocular bacterial and fungal infection. Drug Deliv. Transl. Res. 2021, 11, 1352–1375. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. (Year) Citation | Pathogens | Initial VA | Antifungal Drugs | Surgery | Outcome |
|---|---|---|---|---|---|
| Sponsel (2002) [30] | F. solani | Not mentioned | AMB-intravenous, topical KTC-topical NAT-topical POS-PO, topical | PK | VA: 6/30 |
| Guarro (2003) [53] | F. polyphialidicum | 1/200 | AMB-topical | Corneal transplantation | VA: 20/40 (improved) |
| Tu (2007) [54] | F. solani | HM | AMB-IVI, topical FLC-PO ITC-PO NAT-topical POS-PO VRC-intravenous, IVI, PO | PK for 3 times | VA: CF (improved) |
| Fusarium sp. | Not mentioned | AMB-topical FLC-PO NAT-topical VRC-PO, topical POS-PO, topical | PK for 2 times | Resolution of inflammation | |
| Fusarium sp. | Not mentioned | AMB-AC injection, topical CYA-topical FLC-PO NAT-topical POS-PO VRC-IVI, PO, topical | PK, penetrating patch graft | Poor vision, awaiting repeat corneal transplantation | |
| Proença-Pina (2010) [55] | F. solani | HM | AMB-AC irrigation, topical VRC-PO, topical | PK | VA: 20/50 (improved) |
| Edelstein (2012) [56] | F. solani | HM | AMB-ICI, IVI, topical FLC-PO ITC-PO NAT-topical POS-PO VRC-PO, topical | PK for 2 times, pars plana vitrectomies, enucleation | Enucleation |
| Antequera (2015) [31] | F. solani | - | AMB-intravenous CAS-intravenous VRC-intravenous, PO, topical | Enucleation | Enucleation |
| Sara (2016) [12] | F. solani | 6/12 | AMB-IVI NAT-topical VRC-IVI, PO, topical | PK, enucleation | Enucleation |
| Ref. (Year) Citation | Pathogens | Study Type | Case Number | Photosensitizer | Light Source (Wavelength), Irradiance, Irradiation Time or Radiant Exposure | Outcome |
|---|---|---|---|---|---|---|
| Iseli (2008) [19] | Acremonium sp. | Case reports | 1 | 0.1% RFB | UVA 3.0 mW/cm2 30 min | VA: CF after CXL, 20/30 after DALK (8 months after CXL) (improved) |
| Fusarium sp. | 1 | 0.1% RFB | UVA 3.0 mW/cm2 30 min | Corneal infiltrate progressed after CXL → PK | ||
| Uddaraju (2015) [78] | Aspergillus sp., Fusarium sp. | RCT | 6 | 0.1% RFB | UVA (370 nm) 3.0 mW/cm2 30 min | VA: HM (2 out of 6 cases), LP (2 out of 6 cases), 6/60 (2 out of 6 cases) (~20% cases improved; ~20% cases stable disease, ~60% cases worsened) |
| Vajpayee (2015) [79] | Aspergillus sp., Fusarium sp. | Retrospective study. | 20 | 0.1% RFB | UVA (365 nm) 3.0 mW/cm2 30 min | BCVA: 1.13 ± 0.55 (stable disease) |
| Kasetsuwan (2016) [80] | Fusarium sp., Aspergillus sp., Purpureocillium sp., Pythium sp. | RCT | 8 | 0.1% RFB | UVA (365 nm) 3.0 mW/cm2 30 min | Median size of stromal infiltration: 30.2 mm2→ 9.1 mm2 Median size of epithelial defect: 23.7 mm2→ 1.42 mm2 |
| Amescua (2017) [81] | Fusarium sp. | Case reports | 1 | 0.1% RB | Green light LED (518 nm) 0.9 J/cm2→ 1.8 J/cm2 | Clear cornea with fine endothelial function |
| Mikropoulos (2019) [82] | P. lilacinum | Case report | 1 | RFB | UVA 9.0 mW/cm2 30 min (intraoperative) | VA: CF at 1 m (stable disease) |
| Naranjo (2019) [20] | Fusarium sp. | Consecutive case series. | 4 | 0.1% RB | Green light LED 6.0 mW/cm2 15 min | BCVA: 20/100, 20/800, HM, NLP (50% cases improved; 25% cases stable disease, 25% cases worsened) |
| Curvularia sp. | 1 | 0.2% RB | Green light LED 6.0 mW/cm2 15 min | BCVA: 20/50 (improved) | ||
| Prajna (2020) [83] | Aspergillus sp., Bipolaris sp., Colletotrichum sp., Curvularias sp., Exserohilum sp., Fusarium sp., Scedosporium sp. | RCT | 55 | 0.1% RB | UVA (365 nm) 3.0 mW/cm2 30 min | VA: 3.2 Snellen lines worse at 3 months than baseline VA (worsened in all cases) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, J.-H.; Lee, C.-N.; Hsu, H.-W.; Ng, I.-S.; Wu, C.-J.; Yu, C.-K.; Lee, N.-Y.; Chang, Y.; Wong, T.-W. Recent Advances in Photodynamic Therapy against Fungal Keratitis. Pharmaceutics 2021, 13, 2011. https://doi.org/10.3390/pharmaceutics13122011
Hung J-H, Lee C-N, Hsu H-W, Ng I-S, Wu C-J, Yu C-K, Lee N-Y, Chang Y, Wong T-W. Recent Advances in Photodynamic Therapy against Fungal Keratitis. Pharmaceutics. 2021; 13(12):2011. https://doi.org/10.3390/pharmaceutics13122011
Chicago/Turabian StyleHung, Jia-Horung, Chaw-Ning Lee, Huai-Wen Hsu, I-Son Ng, Chi-Jung Wu, Chun-Keung Yu, Nan-Yao Lee, Yun Chang, and Tak-Wah Wong. 2021. "Recent Advances in Photodynamic Therapy against Fungal Keratitis" Pharmaceutics 13, no. 12: 2011. https://doi.org/10.3390/pharmaceutics13122011